

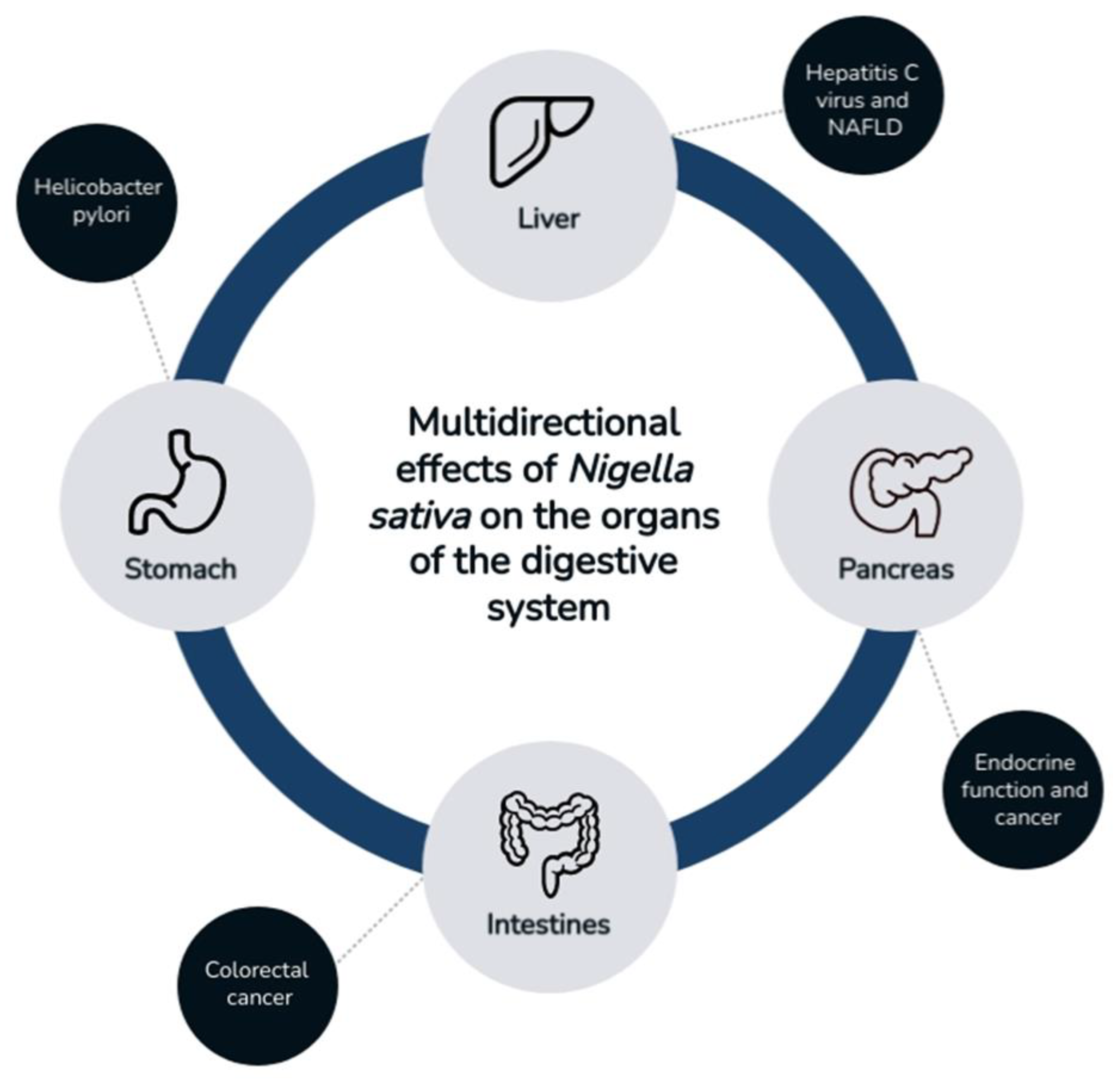
Effect of Nigella sativa on Selected Gastrointestinal Diseases
 , , , and
, , , and
Abstract
:1. Introduction
2. Chemical Composition of Nigella sativa
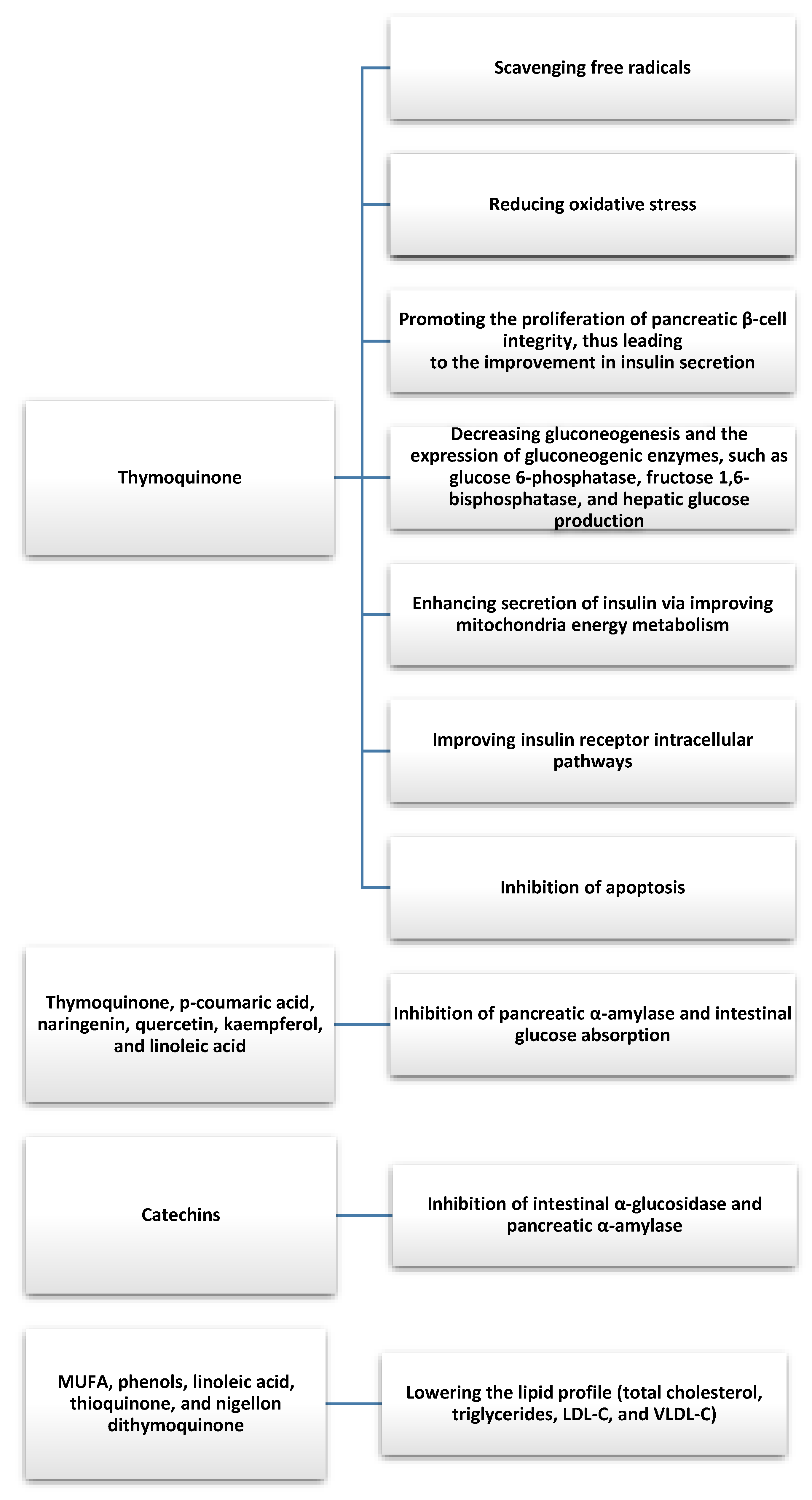
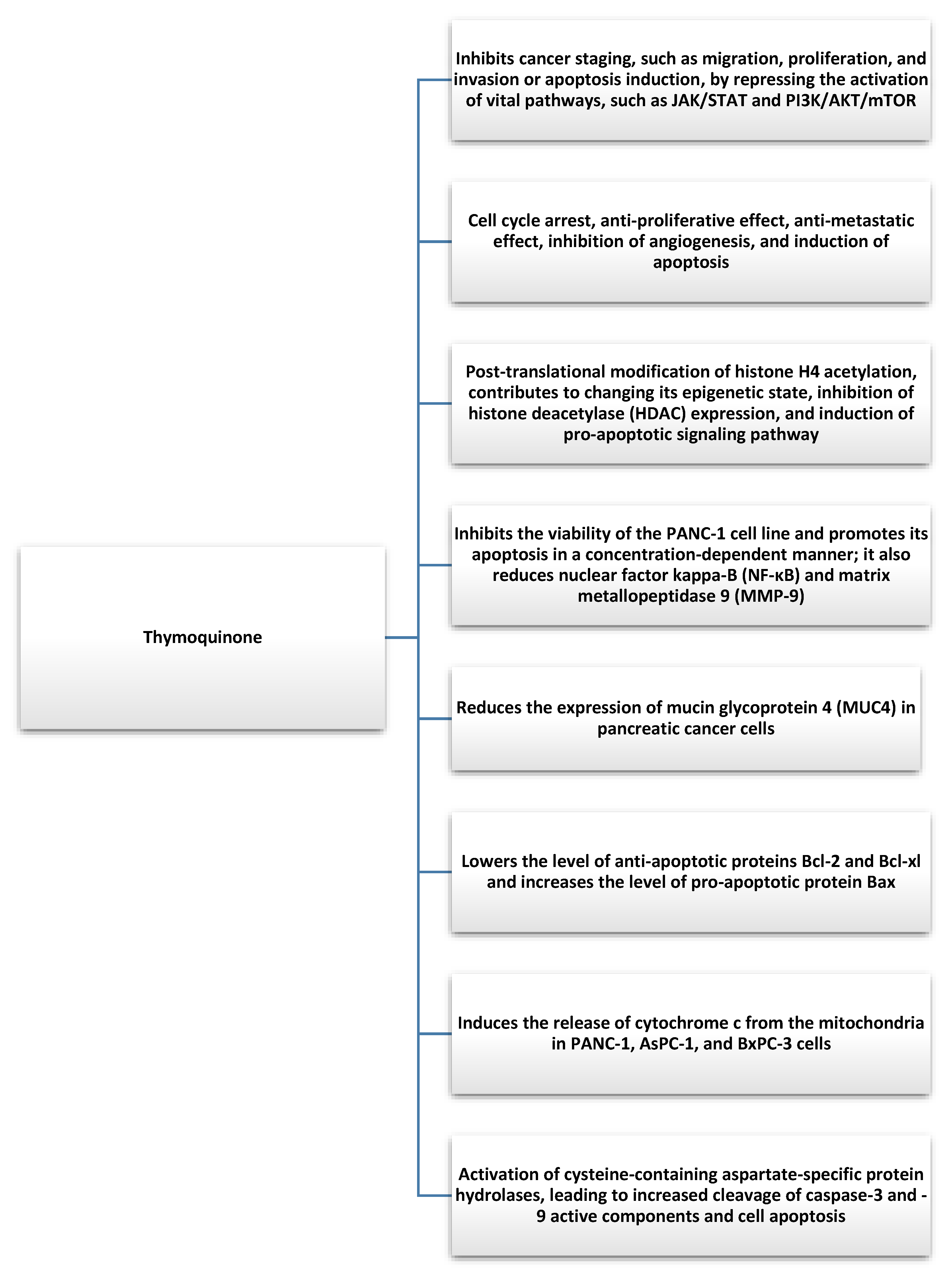
3. Effects of Nigella sativa on the Pancreas
Pancreatic Cancer
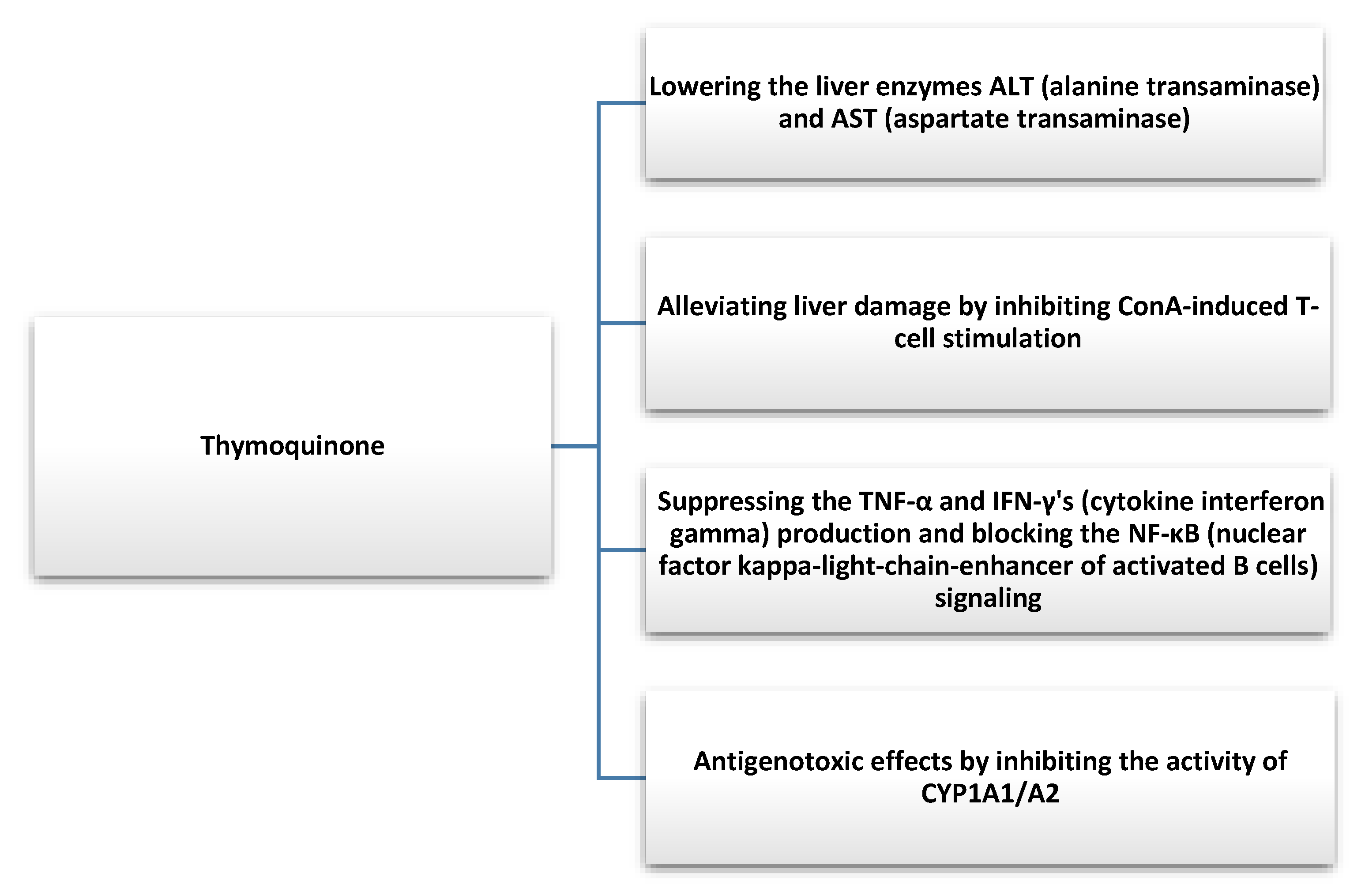
4. Effects of Nigella sativa on the Liver
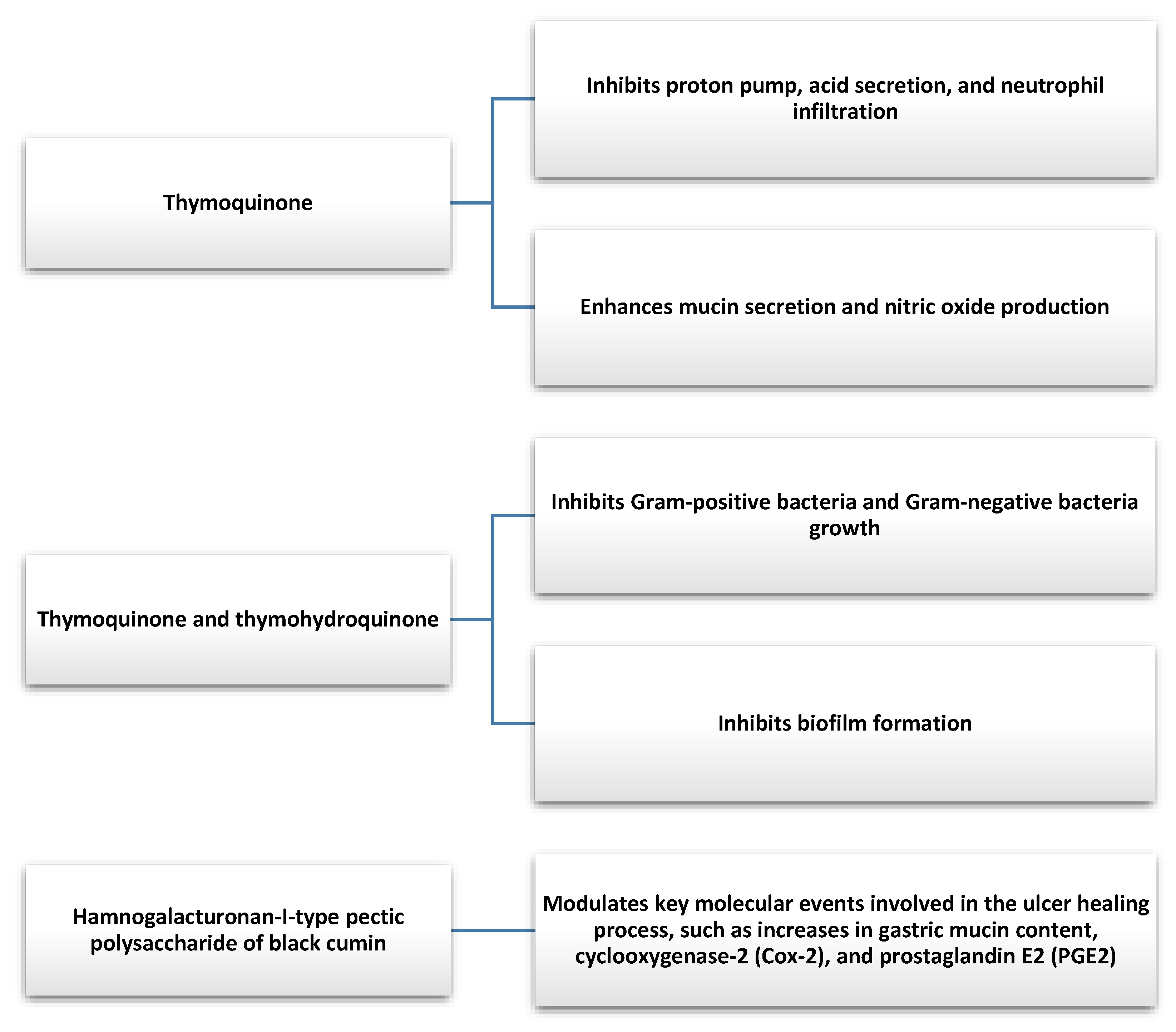
5. Effects of Nigella sativa on the Stomach
6. Effects of Nigella sativa on the Intestines
7. Safety
8. Drug Interactions
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oskouei, Z.; Akaberi, M.; Hosseinzadeh, H. A glance at black cumin (Nigella sativa) and its active constituent, thymoquinone, in ischemia: A review. Iran. J. Basic Med. Sci. 2018, 21, 1200–1209. [Google Scholar] [CrossRef] [PubMed]
- Dalli, M.; Bekkouch, O.; Azizi, S.; Azghar, A.; Gseyra, N.; Kim, B. Nigella sativa L. Phytochemistry and pharmacological activities: A review (2019–2021). Biomolecules 2021, 23, 20. [Google Scholar] [CrossRef]
- Kooti, W.; Hasanzadeh-Noohi, Z.; Sharafi-Ahvazi, N.; Asadi-Samani, M.; Ashtary-Larky, D. Phytochemistry, pharmacology, and therapeutic uses of black seed (Nigella sativa). Chin. J. Nat. Med. 2016, 14, 732–745. [Google Scholar] [CrossRef]
- Leong, X.; Rais Mustafa, M.; Jaarin, K. Nigella sativa and its protective role in oxidative stress and hypertension. Evid. Based Complement. Alternat. Med. 2013, 2013, 120732. [Google Scholar] [CrossRef] [PubMed]
- Emamat, H.; Mousavi, S.H.; Kargar Shouraki, J.; Hazrati, E.; Mirghazanfari, S.M.; Samizadeh, E.; Hosseini, M.; Hadi, V.; Hadi, S. The effect of Nigella sativa oil on vascular dysfunction assessed by flow-mediated dilation and vascular-related biomarkers in subject with cardiovascular disease risk factors: A randomized controlled trial. Phytother. Res. 2022, 36, 2236–2245. [Google Scholar] [CrossRef] [PubMed]
- Enayatfard, L.; Mohebbati, R.; Niazmand, S.; Hosseini, M.; Shafei, M. The standardized extract of Nigella sativa and its major ingredient, thymoquinone, ameliorates angiotensin II-induced hypertension in rats. J. Basic. Clin. Physiol. Pharm. 2018, 19, 51–58. [Google Scholar] [CrossRef]
- Hadi, S.; Daryabeygi-Khotbehsara, R.; Mirmiran, P.; McVicar, J.; Hadi, V.; Soleimani, D.; Askari, G. Effect of Nigella sativa oil extract on cardiometabolic risk factors in type 2 diabetes: A randomized, double-blind, placebo-controlled clinical trial. Phytother. Res. 2021, 35, 3747–3755. [Google Scholar] [CrossRef]
- Mahomoodally, M.F.; Aumeeruddy, M.Z.; Legoabe, L.J.; Montesano, D.; Zengin, G. Nigella sativa L. and its active compound thymoquinone in the clinical management of diabetes: A systematic review. Int. J. Mol. Sci. 2022, 11, 12111. [Google Scholar] [CrossRef]
- Namazi, N.; Larijani, B.; Ayati, M.H.; Abdollahi, M. The effects of Nigella sativa L. on obesity: A systematic review and meta-analysis. J. Ethnopharmacol. 2018, 12, 173–181. [Google Scholar] [CrossRef]
- Hussain, A.; Ahmed, M.; Ahmed, S.; Manogaran, P.; Platanias, L.; Alvi, S.; Al-Kuraya, K.; Uddin, S. Thymoquinone suppresses growth and induces apoptosis via generation of reactive oxygen species in primary effusion lymphoma. Free Radic. Biol. Med. 2011, 15, 978–987. [Google Scholar] [CrossRef]
- Badr, G.; Mohany, M.; Abu-Tarboush, F. Thymoquinone decreases F-actin polymerization and the proliferation of human multiple myeloma cells by suppressing STAT3 phosphorylation and Bcl2/Bcl-XL expression. Lipids Health Dis. 2011, 16, 236. [Google Scholar] [CrossRef] [Green Version]
- Lotfi, M.; Kazemi, S.; Ebrahimpour, A.; Pourabdolhossein, F.; Satarian, L.; Eghbali, A.; Moghadamnia, A. Thymoquinone improved nonylphenol-induced memory deficit and neurotoxicity through its antioxidant and neuroprotective effects. Mol. Neurobiol. 2022, 59, 3600–3616. [Google Scholar] [CrossRef]
- Fanoudi, S.; Alavi, M.; Hosseini, M.; Sadeghnia, H. Nigella sativa and thymoquinone attenuate oxidative stress and cognitive impairment following cerebral hypoperfusion in rats. Metab. Brain Dis. 2019, 34, 1001–1010. [Google Scholar] [CrossRef]
- Herlina Aziz, S.; Kurniawati, A.; Faridah, D. Changes of thymoquinone, thymol, and malondialdehyde content of black cumin (Nigella sativa L.) in response to Indonesia tropical. J. Biosci. 2017, 24, 156–161. [Google Scholar] [CrossRef]
- Ansary, J.; Giampieri, F.; Forbes-Hernandez, T.; Regolo, L.; Quinzi, D. Nutritional value and preventive role of Nigella sativa L. and its main component thymoquinone in cancer: An evidenced-based review of preclinical and clinical studies. Molecules 2021, 7, 2108. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, A.; Mishra, R.; Vyawahare, A.; Kumar, A. Thymoquinone (2-Isoprpyl-5-methyl-1, 4-benzoquinone) as a chemopreventive/anticancer agent: Chemistry and biological effects. Saudi Pharm. J. 2019, 27, 1113–1126. [Google Scholar] [CrossRef]
- Ahmad, A.; Husain, A.; Mujeeb, M.; Khan, S.; Najmi, A.; Siddique, N.; Damanhouri, Z.; Anwar, F. A review on therapeutic potential of Nigella sativa: A miracle herb. Asian Pac. J. Trop. Biomed. 2013, 3, 337–352. [Google Scholar] [CrossRef] [Green Version]
- Greenish, H. Contribution to the chemistry of Nigella sativa. Pharmac. J. Trans. 1880, 10, 909–911. [Google Scholar]
- Albakry, Z.; Karrar, E.; Ahmed, I.A.M.; Oz, E.; Proestos, C.; El Sheikha, A.F.; Oz, F.; Wu, G.; Wang, X. Nutritional composition and volatile compounds of black cumin (Nigella sativa L.) seed, fatty acid composition and tocopherols, polyphenols, and antioxidant activity of its essential oil. Horticulturae 2022, 8, 575. [Google Scholar] [CrossRef]
- Yimer, E.; Tuem, K.; Karim, A.; Ur-Rehman, N.; Anwar, F. Nigella sativa L. (Black Cumin): A promising natural remedy for wide range of illnesses. Evid.-Based Complement. Altern. Med. 2019, 12, 1528635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pop, R.; Trifa, A.; Popolo, A.; Chedea, V.; Militaru, C.; Bocsan, I.; Buzoianu, A. Nigella sativa: Valuable perspective in the management of chronic diseases. Iran. J. Basic Med. Sci. 2020, 23, 699–713. [Google Scholar] [CrossRef]
- Cheikh-Rouhou, S.; Besbes, S.; Hentati, B.; Blecker, C.; Deroanne, C.; Attia, H. Nigella sativa L.: Chemical composition and physicochemical characteristics of lipid fraction. Food Chem. 2007, 101, 673–681. [Google Scholar] [CrossRef]
- Akram, K.M.; Afzal, M. Chemical composition of Nigella sativa Linn: Part 2 recent advances. Inflammopharmacology 2016, 24, 67–79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannan, M.A.; Rahman, M.A.; Sohag AA, M.; Uddin, M.J.; Dash, R.; Sikder, M.H.; Rahman, M.S.; Timalsina, B.; Munni, Y.A.; Sarker, P.P.; et al. Black Cumin (Nigella sativa L.): A comprehensive review on phytochemistry, health benefits, molecular pharmacology, and safety. Nutrients 2021, 24, 1784. [Google Scholar] [CrossRef] [PubMed]
- Karpińska, M.; Czauderna, M. Pancreas-its functions, disorders, and physiological impact on the mammals’ organism. Front. Physiol. 2022, 30, 807632. [Google Scholar] [CrossRef] [PubMed]
- Hamdan, A.; Haji, I.R.; Mokhtar, M. Effects of Nigella sativa on type-2 diabetes mellitus: A systematic review. Int. J. Environ. Res. Public Health 2019, 5, 4911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahmad, M.; Ahmad, F.; Ashraf, H.; Saad, H.; Wahab, S.; Khan, M.; Ali, M.; Mohan, S.; Hakeem, K.; Athar, M. An updated knowledge of Black seed (Nigella sativa L.): Review of phytochemical constituents and pharmacological properties. J. Herb. Med. 2021, 25, 100404. [Google Scholar] [CrossRef]
- Heshmati, J.; Namazi, N. Effects of black seed (Nigella sativa) on metabolic parameters in diabetes mellitus: A systematic review. Complement. Ther. Med. 2015, 23, 275–282. [Google Scholar] [CrossRef]
- Hoda, F.; Khanam, A.; Thareja, M.; Arshad, M.; Ahtar, M.; Najmi, A. Effect of Nigella sativa in improving blood glucose level in T2DM: Systematic literature review of randomized control rrials. Drug Res. 2023, 73, 17–22. [Google Scholar] [CrossRef]
- Faisal Lutfi, M.; Abdel-Moneim, A.; Alsharidah, A.; Mobark, M.; Abdellatif, A.; Saleem, I.; Al Rugaie, O.; Mohany, K.; Alsharidah, M. Thymoquinone lowers blood glucose and reduces oxidative stress in a rat model of diabetes. Molecules 2021, 17, 2348. [Google Scholar] [CrossRef]
- El-Shemi, A.; Kensara, O.; Alsaegh, A.; Mukhtar, M. Pharmacotherapy with thymoquinone improved pancreatic β-cell integrity and functional activity, enhanced islets revascularization, and alleviated metabolic and hepato-renal disturbances in streptozotocin-induced diabetes in rats. Pharmacology 2018, 101, 9–21. [Google Scholar] [CrossRef]
- Khan, S.; Zaidi, K. Protective effect of Nigella sativa seed extract and its bioactive compound thymoquinone on streptozotocin-induced diabetic rats. Cardiovasc. Hematol. Agents Med. Chem. 2022. E-pub Ahead of Print. [Google Scholar] [CrossRef] [PubMed]
- Dalli, M.; Daoudi, N.; Azizi, S.; Benouda, H.; Bnouham, M.; Gseyra, N. Chemical composition analysis using HPLC-UV/GC-MS and inhibitory activity of different Nigella sativa fractions on pancreatic α-amylase and intestinal glucose absorption. Biomed. Res. Int. 2021, 26, 9979419. [Google Scholar] [CrossRef]
- Varghese, L.; Mehrotra, N. α-amylase inhibitory activity of microencapsulated Nigella sativa L. and herb-drug interaction: An in vitro analysis. Ann. Fitomed. Int. J. 2020, 9, 107–112. [Google Scholar] [CrossRef]
- Tiji, S.; Bouhrim, M.; Addi, M.; Drouet, S.; Lorenzo, J.; Hano, C.; Bnouham, M.; Mimouni, M. Linking the phytochemicals and the α-glucosidase and α-amylase enzyme inhibitory effects of Nigella sativa seed extracts. Foods 2021, 6, 1818. [Google Scholar] [CrossRef]
- Hannan, J.; Ansari, P.; Haque, A.; Sanju, A.; Huzaifa, A.; Rahman, A.; Ghosh, A.; Azam, S. Nigella sativa stimulates insulin secretion from isolated rat islets and inhibits the digestion and absorption of (CH2O)n in the gut. Biosci. Rep. 2019, 23, BSR20190723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alshahrani, S.; Anwer, T.; Alam, M.; Ahmed, R.; Khan, G.; Sivakumar, S.; Shoaib, A.; Alam, P.; Azam, F. Effect of thymoquinone on high fat diet and STZ-induced experimental type 2 diabetes: A mechanistic insight by in vivo and in silico studies. J. Food Biochem. 2021, 21, e13807. [Google Scholar] [CrossRef] [PubMed]
- Aboul-Mahasen, L.; Abdulrahman, A.R. The possible protective effects of virgin olive oil and Nigella sativa seeds on the biochemical and histopathological changes in pancreas of hyperlipidaemic rats. Folia Morphol. 2019, 78, 762–772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shehata, T.; Almostafa, M.; Elsewedy, H. Development and optimization of Nigella sativa nanoemulsion loaded with pioglitazone for hypoglycemic effect. Polymers 2022, 26, 3021. [Google Scholar] [CrossRef]
- Badar, A.; Kaatabi, H.; Bamosa, A.; Al-Elq, A.; Abou-Hozaifa, B.; Lebda, F.; Alkhadra, S.; Al-Almaie, S. Effect of Nigella sativa supplementation over a one-year period on lipid levels, blood pressure and heart rate in type-2 diabetic patients receiving oral hypoglycemic agents: Nonrandomized clinical trial. Ann. Saudi Med. 2017, 37, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Kooshki, A.; Tofighiyan, T.; Rastgoo, N.; Rakhshani, M.; Miri, M. Effect of Nigella sativa oil supplement on risk factors for cardiovascular diseases in patients with type 2 diabetes mellitus. Phytother. Res. 2020, 34, 2706–2711. [Google Scholar] [CrossRef] [PubMed]
- Moustafa, H.; El Wakeel, L.; Halawa, M.; Sabri, N.; El-Bahy, A.; Singab, A. Effect of Nigella sativa oil versus metformin on glycemic control and biochemical parameters of newly diagnosed type 2 diabetes mellitus patients. Endocrine 2019, 65, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Jangjo-Borazjani, S.; Dastgheib, M.; Kiyamarsi, E.; Jamshidi, R.; Rahmati-Ahmadabad, S.; Helalizadeh, M.; Iraji, R.; Cornish, S.M.; Mohammadi-Darestani, S.; Khojasteh, Z.; et al. Effects of resistance training and Nigella sativa on type 2 diabetes: Implications for metabolic markers, low-grade inflammation and liver enzyme production. Arch. Physiol. Biochem. 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mostafa, T.; Hegazy, S.; Elnaidany, S.; Shehabeldin, W.; Sawan, E. Nigella sativa as a promising intervention for metabolic and inflammatory disorders in obese prediabetic subjects: A comparative study of Nigella sativa versus both lifestyle modification and metformin. J. Diabetes Complicat. 2021, 35, 107947. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Liu, L.; Li, S.; Hou, X.; Yang, J. Advances in research on the relationship between thymoquinone and pancreatic cancer. Front. Oncol. 2023, 4, 1092020. [Google Scholar] [CrossRef]
- Mizrahi, J.; Surana, R.; Valle, J.; Shroff, R. Pancreatic cancer. Lancet 2020, 27, 2008–2020. [Google Scholar] [CrossRef]
- Sharifi-Rad, M.; Anil Kumar, N.V.; Zucca, P.; Varoni, E.M.; Dini, L.; Panzarini, E.; Rajkovic, J.; Tsouh Fokou, P.V.; Azzini, E.; Peluso, I.; et al. Lifestyle, oxidative stress, and antioxidants: Back and forth in the pathophysiology of chronic diseases. Front. Physiol. 2020, 2, 694. [Google Scholar] [CrossRef]
- Almajali, B.; Al-Jamal, H.; Taib, W.; Ismail, I.; Johan, M.; Doolaanea, A.; Ibrahim, W. Thymoquinone, as a novel therapeutic candidate of cancers. Pharmaceuticals 2021, 16, 369. [Google Scholar] [CrossRef]
- Imran, M.; Rauf, A.; Khan, I.A.; Shahbaz, M.; Qaisrani, T.B.; Fatmawati, S.; Abu-Izneid, T.; Imran, A.; Rahman, K.U.; Gondal, T.A. Thymoquinone: A novel strategy to combat cancer: A review. Biomed. Pharmacother. 2018, 106, 390–402. [Google Scholar] [CrossRef]
- Relles, D.; Chipitsyna, G.; Gong, Q.; Yeo, C.; Arafat, H. Thymoquinone promotes pancreatic cancer cell death and reduction of tumor size through combined inhibition of histone deacetylation and induction of histone acetylation. Adv. Prev. Med. 2016, 2016, 1407840. [Google Scholar] [CrossRef] [Green Version]
- Tan, M.; Norwood, A.; May, M.; Tucci, M.; Benghuzzi, H. Effects of (-)epigallocatechin gallate and thymoquinone on proliferation of a PANC-1 cell line in culture. Biomed. Sci. Instrum. 2006, 42, 363–371. [Google Scholar] [PubMed]
- Wu, Z.; Chen, Z.; Shen, Y.; Huang, L.; Jiang, P. Anti-metastasis effect of thymoquinone on human pancreatic cancer. Yao Xue Xue Bao 2011, 46, 910–914. [Google Scholar] [PubMed]
- Narayanan, P.; Farghadani, R.; Nyamathulla, S.; Rajarajeswaran, J.; Thirugnanasampandan, R.; Bhuwaneswari, G. Natural quinones induce ROS-mediated apoptosis and inhibit cell migration in PANC-1 human pancreatic cancer cell line. J. Biochem. Mol. Toxicol. 2022, 36, e23008. [Google Scholar] [CrossRef]
- Torres, M.P.; Ponnusamy, M.P.; Chakraborty, S.; Smith, L.M.; Das, S.; Arafat, H.A.; Batra, S.K. Effects of thymoquinone in the expression of mucin 4 in pancreatic cancer cells: Implications for the development of novel cancer therapies. Mol. Cancer Ther. 2010, 9, 1419–1431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mu, G.; Zhang, L.; Li, H.; Liao, Y.; Yu, H. Thymoquinone pretreatment overcomes the insensitivity and potentiates the antitumor effect of gemcitabine through abrogation of Notch1, PI3K/Akt/mTOR regulated signaling pathways in pancreatic cancer. Dig. Dis. Sci. 2015, 60, 1067–1080. [Google Scholar] [CrossRef]
- Djamgoz, M.; Jentzsch, V. Integrative management of pancreatic cancer (PDAC): Emerging complementary agents and modalities. Nutr. Cancer 2022, 74, 1139–1162. [Google Scholar] [CrossRef]
- Pandita, A.; Kumar, B.; Manvati, S.; Vaishnavi, S.; Singh, S.; Bamezai, R. Synergistic combination of gemcitabine and dietary molecule induces apoptosis in pancreatic cancer cells and down regulates PKM2 expression. PLoS ONE 2014, 9, e107154. [Google Scholar] [CrossRef]
- Pandita, A.; Manvati, S.; Singh, S.; Vaishnavi, S.; Bamezai, R. Combined effect of microRNA, nutraceuticals and drug on pancreatic cancer cell lines. Chem. Biol. Interact. 2015, 233, 56–64. [Google Scholar] [CrossRef]
- Karki, N.; Aggarwal, S.; Laine, R.; Greenway, F.; Losso, J. Cytotoxicity of juglone and thymoquinone against pancreatic cancer cells. Chem. Biol. Interact. 2020, 327, 109142. [Google Scholar] [CrossRef]
- El-Far, A.; Al Jaouni, S.; Li, W.; Mousa, S. Protective roles of Thymoquinone nanoformulations: Potential nanonutraceuticals in human diseases. Nutrients 2018, 10, 1369. [Google Scholar] [CrossRef] [Green Version]
- Liu, D.; Zhang, H.; Fontana, F.; Hirvonen, J.; Santos, H. Current developments and applications of microfluidic technology toward clinical translation of nanomedicines. Adv. Drug Deliv. Rev. 2018, 128, 54–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanter, M.; Meral, I.; Dede, S.; Gunduz, H.; Cemek, M.; Ozbek, H.; Uygan, I. Effects of Nigella sativa L. and Urtica dioica L. on lipid peroxidation, antioxidant enzyme systems and some liver enzymes in CCl4-treated rats. J. Vet. Med. A Physiol. Pathol. Clin. Med. 2003, 50, 264–268. [Google Scholar] [CrossRef] [PubMed]
- Fadishei, M.; Ghasemzadeh Rahbardar, M.; Imenshahidi, M.; Mohajeri, A.; Razavi, B.; Hosseinzadeh, H. Effects of Nigella sativa oil and thymoquinone against bisphenol A-induced metabolic disorder in rats. Phytother. Res. 2021, 35, 2005–2024. [Google Scholar] [CrossRef] [PubMed]
- Hussain, M.; Tunio, A.; Akhtar, L.; Shaikh, G. Effects of Nigella sativa on various parameters in Patients of non-alcoholic fatty liver disease. J. Ayub. Med. Coll. Abbottabad. 2017, 29, 403–407. [Google Scholar] [PubMed]
- Rashidmayvan, M.; Mohammadshahi, M.; Seyedian, S.; Haghighizadeh, M. The effect of Nigella sativa oil on serum levels of inflammatory markers, liver enzymes, lipid profile, insulin and fasting blood sugar in patients with non-alcoholic fatty liver. J. Diabetes Metab. Disord. 2019, 18, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Darand, M.; Darabi, Z.; Yari, Z.; Saadati, S.; Hedayati, M.; Khoncheh, A.; Hosseini-Ahangar, B.; Alavian, S.; Hekmatdoost, A. Nigella sativa and inflammatory biomarkers in patients with non-alcoholic fatty liver disease: Results from a randomized, double-blind, placebo-controlled, clinical trial. Complement. Ther. Med. 2019, 44, 204–209. [Google Scholar] [CrossRef]
- Razmpoosh, E.; Safi, S.; Abdollahi, N.; Nadjarzadeh, A.; Nazari, M.; Fallahzadeh, H.; Mazaheri, M.; Salehi-Abargouei, A. The effect of Nigella sativa on the measures of liver and kidney parameters: A systematic review and meta-analysis of randomized-controlled trials. Pharmacol. Res. 2020, 156, 104767. [Google Scholar] [CrossRef]
- Khonche, A.; Huseini, H.; Gholamian, M.; Mohtashami, R.; Nabati, F.; Kianbakht, S. Standardized Nigella sativa seed oil ameliorates hepatic steatosis, aminotransferase and lipid levels in non-alcoholic fatty liver disease: A randomized, double-blind and placebo-controlled clinical trial. J. Ethnopharmacol. 2019, 234, 106–111. [Google Scholar] [CrossRef]
- Mohtashamian, A.; Ebrahimzadeh, A.; Shamekhi, Z.; Sharifi, N. Nigella sativa supplementation and non-alcoholic fatty liver disease: A systematic review of clinical trials. Avicenna J. Phytomed. 2023, 13, 18–33. [Google Scholar] [CrossRef]
- Azizi, N.; Amini, M.; Djafarian, K.; Shab-Bidar, S. The effects of Nigella sativa supplementation on liver enzymes levels: A systematic review and meta-analysis of randomized controlled trials. Clin. Nutr. Res. 2021, 10, 72–82. [Google Scholar] [CrossRef]
- Barakat, E.; El Wakeel, L.; Hagag, R. Effects of Nigella sativa on outcome of hepatitis C in Egypt. World J. Gastroenterol. 2013, 19, 2529–2536. [Google Scholar] [CrossRef]
- Abdel-Moneim, A.; Morsy, B.; Mahmoud, A.; Abo-Seif, M.; Zanaty, M. Beneficial therapeutic effects of Nigella sativa and/or Zingiber officinale in HCV patients in Egypt. Excli. J. 2013, 12, 943–955. [Google Scholar]
- Ahmed, A.; Zahoor, A.; Ibrahim, M.; Younus, M.; Nawaz, S.; Naseer, R.; Akram, Q.; Deng, C.; Ojha, S. Enhanced efficacy of direct-acting antivirals in Hepatitis C patients by coadministration of Black Cumin and ascorbate as antioxidant adjuvants. Oxid. Med. Cell Longev. 2020, 2020, 7087921. [Google Scholar] [CrossRef]
- Kathem, S.; Abdulsahib, W.; Zalzala, M. Berbamine and thymoquinone exert protective effects against immune-mediated liver injury via NF-κB dependent pathway. Front. Vet. Sci. 2022, 9, 960981. [Google Scholar] [CrossRef]
- Hossen, M.; Yang, W.; Kim, D.; Aravinthan, A.; Kim, J.; Cho, J. Thymoquinone: An IRAK1 inhibitor with in vivo and in vitro anti-inflammatory activities. Sci. Rep. 2017, 7, 42995. [Google Scholar] [CrossRef] [Green Version]
- Seronello, S.; Sheikh, M.; Choi, J. Redox regulation of hepatitis C in nonalcoholic and alcoholic liver. Free Radic. Biol. Med. 2007, 43, 869–882. [Google Scholar] [CrossRef] [Green Version]
- Forouzanfar, F.; Bazzaz, B.; Hosseinzadeh, H. Black cumin (Nigella sativa) and its constituent (thymoquinone): A review on antimicrobial effects. Iran. J. Basic Med. Sci. 2014, 17, 929–938. [Google Scholar]
- Shahin, Y.R.; Elguindy, N.M.; Abdel Bary, A.; Balbaa, M. The protective mechanism of Nigella sativa against diethylnitrosamine-induced hepatocellular carcinoma through its antioxidant effect and EGFR/ERK1/2 signaling. Environ. Toxicol. 2018, 33, 885–898. [Google Scholar] [CrossRef]
- Saddiq, A.A.; El-Far, A.H.; Mohamed Abdullah, S.A.; Godugu, K.; Almaghrabi, O.A.; Mousa, S.A. Curcumin, thymoquinone, and 3,3’-diindolylmethane combinations attenuate lung and liver cancers progression. Front Pharmacol. 2022, 13, 936996. [Google Scholar] [CrossRef]
- Usmani, A.; Mishra, A.; Arshad, M.; Jafri, A. Development and evaluation of doxorubicin self nanoemulsifying drug delivery system with Nigella sativa oil against human hepatocellular carcinoma. Artif. Cells Nanomed. Biotechnol. 2019, 47, 933–944. [Google Scholar] [CrossRef] [Green Version]
- Tadros, S.; Attia, Y.; Maurice, N.; Fahim, S.; Abdelwahed, F.; Ibrahim, S.; Badary, O. Thymoquinone suppresses angiogenesis in DEN-Induced hepatocellular carcinoma by targeting miR-1-3p. Int. J. Mol. Sci. 2022, 23, 15904. [Google Scholar] [CrossRef]
- Magdy, M.A.; Hanan, E.-A.; Nabila, E.-M. Thymoquinone: Novel gastroprotective mechanisms. Eur. J. Pharmacol. 2012, 697, 126–131. [Google Scholar] [CrossRef] [PubMed]
- Pop, R.M.; Sabin, O.; Suciu, S.; Vesa, S.; Socaci, S.; Chedea, V.; Bocsan, I.; Buzoianu, A. Nigella sativa’s anti-Inflammatory and antioxidative effects in experimental inflammation. Antioxidants 2020, 9, 921. [Google Scholar] [CrossRef] [PubMed]
- Manjegowda, S.; Rajagopal, H.; Dharmesh, S. Polysaccharide of Black cumin (Nigella sativa) modulates molecular signaling cascade of gastric ulcer pathogenesis. Int. J. Biol. Macromol. 2017, 101, 823–836. [Google Scholar] [CrossRef]
- Aleem, U.; Rehman, A.; Shah, R.; Jan, T.; Jan, M.; Jan, R. Effects of thymoquinone obtained from seeds of Nigella sativa on volume & Acidity of stimulated gastric secretion. Pak. J. Med. Health Sci. 2020, 14, 49–50. [Google Scholar]
- Saleem, N.; Howden, C. Update on the management of Helicobacter pylori Infection. Curr. Treat. Options Gastroenterol. 2020, 18, 476–487. [Google Scholar] [CrossRef]
- Piscione, M.; Mazzone, M.; Di Marcantonio, M.; Muraro, R.; Mincione, G. Eradication of Helicobacter pylori and gastric cancer: A controversial relationship. Front. Microbiol. 2021, 12, 630852. [Google Scholar] [CrossRef]
- Hanafy, M.; Hatem, M. Studies on the antimicrobial activity of Nigella sativa seed (black cumin). J. Ethnopharmacol. 1991, 34, 275–278. [Google Scholar] [CrossRef]
- Halawani, E. Antibacterial activity of thymoquinone and thymohydroquinone of Nigella sativa L. and their interaction with some antibiotics. Adv. Biol. Res. 2009, 3, 148–152. [Google Scholar]
- Salman, M.; Khan, R.; Shukla, I. Antimicrobial activity of Nigella sativa seed oil against multi-drug resistant bacteria from clinical isolates. Nat. Prod. Radiance 2008, 7, 10–14. [Google Scholar]
- Salem, E.; Yar, T.; Bamosa, A.; Al-Quorain, A.; Yasawy, M.; Alsulaiman, R.; Randhawa, M. Comparative study of Nigella sativa and triple therapy in eradication of Helicobacter Pylori in patients with non-ulcer dyspepsia. Saudi J. Gastroenterol. 2010, 16, 207–214. [Google Scholar] [CrossRef] [PubMed]
- Hashem-Dabaghian, F.; Agah, S.; Taghavi-Shirazi, M.; Ghobadi, A. Combination of Nigella sativa and honey in eradication of gastric Helicobacter pylori infection. Iran. Red. Crescent. Med. J. 2016, 18, e23771. [Google Scholar] [CrossRef] [Green Version]
- Mohtashami, R.; Huseini, H.; Heydari, M.; Amini, M.; Sadeqhi, Z.; Ghaznavi, H.; Mehrzadi, S. Efficacy and safety of honey based formulation of Nigella sativa seed oil in functional dyspepsia: A double blind randomized controlled clinical trial. J. Ethnopharmacol. 2015, 175, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Alizadeh-Naini, M.; Yousefnejad, H.; Hejazi, N. The beneficial health effects of Nigella sativa on Helicobacter pylori eradication, dyspepsia symptoms, and quality of life in infected patients: A pilot study. Phytother. Res. 2020, 34, 1367–1376. [Google Scholar] [CrossRef]
- Shahid, F.; Farooqui, Z.; Khan, A.; Khan, F. Oral Nigella sativa oil and thymoquinone administration ameliorates the effect of long-term cisplatin treatment on the enzymes of carbohydrate metabolism, brush border membrane, and antioxidant defense in rat intestine. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2018, 391, 145–157. [Google Scholar] [CrossRef] [PubMed]
- Shahid, F.; Farooqui, Z.; Rizwan, S.; Abidi, S.; Parwez, I.; Khan, F. Oral administration of Nigella sativa oil ameliorates the effect of cisplatin on brush border membrane enzymes, carbohydrate metabolism and antioxidant system in rat intestine. Exp. Toxicol. Pathol. 2017, 69, 299–306. [Google Scholar] [CrossRef] [PubMed]
- Venkataraman, B.; Almarzooqi, S.; Raj, V.; Alhassani, A.T.; Alhassani, A.S.; Ahmed, K.J.; Subramanian, V.S.; Ojha, S.K.; Attoub, S.; Adrian, T.E.; et al. Thymoquinone, a aietary bioactive compound, exerts anti-Inflammatory effects in colitis by stimulating expression of the colonic epithelial PPAR-γ transcription factor. Nutrients 2021, 13, 1343. [Google Scholar] [CrossRef]
- El-Sheikh, A.; Morsy, M.; Hamouda, A. Protective mechanisms of thymoquinone on methotrexate-induced intestinal toxicity in rats. Pharmacogn. Mag. 2016, 12, S76–S81. [Google Scholar] [CrossRef] [Green Version]
- Orhon, Z.; Uzal, C.; Kanter, M.; Erboga, M.; Demiroglu, M. Protective effects of Nigella sativa on gamma radiation-induced jejunal mucosal damage in rats. Pathol. Res. Pract. 2016, 212, 437–443. [Google Scholar] [CrossRef] [PubMed]
- El-Far, A.; Godugu, K.; Noreldin, A.; Saddiq, A.; Almaghrabi, O.; Al Jaouni, S.; Mousa, S. Thymoquinone and costunolide induce apoptosis of both proliferative and doxorubicin-induced-senescent colon and breast cancer cells. Integr. Cancer Ther. 2021, 20, 15347354211035450. [Google Scholar] [CrossRef]
- Akinrinde, A.; Adekanmbi, A.; Olojo, F. Nigella sativa oil protects against cadmium-induced intestinal toxicity via promotion of anti-inflammatory mechanisms, mucin expression and microbiota integrity. Avicenna J. Phytomed. 2022, 12, 241–256. [Google Scholar] [CrossRef] [PubMed]
- Maideen, N.M.P. Antidiabetic activity of Nigella sativa (Black Seeds) and its active constituent (Thymoquinone): A review of human and experimental animal studies. Chonnam. Med. J. 2021, 57, 169–175. [Google Scholar] [CrossRef] [PubMed]
- Mashayekhi-Sardoo, H.; Rezaee, R.; Karimi, G. An overview of in vivo toxicological profile of thymoquinone. Toxin. Rev. 2020, 39, 115–122. [Google Scholar] [CrossRef]
- Al-Ali, A.; Alkhawajah, A.; Randhawa, M.; Shaikh, N. Oral and intraperitoneal LD50 of thymoquinone, an active principle of Nigella sativa, in mice and rats. J. Ayub. Med. Coll. Abbottabad 2008, 20, 25–27. [Google Scholar] [PubMed]
- Tavakkoli, A.; Mahdian, V.; Razavi, B.; Hosseinzadeh, H. Review on clinical trials of black seed (Nigella sativa) and its active constituent, thymoquinone. J. Pharmacopunct. 2017, 20, 179–193. [Google Scholar] [CrossRef]
- Thomas, J.; Mohan, M.; Prabhakaran, P.; Das, S.; Maliakel, B.; Krishnakumar, I. A phase I clinical trial to evaluate the safety of thymoquinone-rich black cumin oil (BlaQmax®) on healthy subjects: Randomized, double-blinded, placebo-controlled prospective study. Toxicol. Rep. 2022, 9, 999–1007. [Google Scholar] [CrossRef]
- Mesonero, F.; Fernández, C.; Sánchez-Rodrígue, E.; García-García, P.A.; Senosiain, C.; Albillos, A.; López-Sanromán, A. Polypharmacy in patients with inflammatory bowel disease: Prevalence and outcomes in a single-center series. J. Clin. Gastroenterol. 2022, 56, e189–e195. [Google Scholar] [CrossRef]
- Pazan, F.; Wehling, M. Polypharmacy in older adults: A narrative review of definitions, epidemiology and consequences. Eur. Geriatr. Med. 2021, 12, 443–452. [Google Scholar] [CrossRef]
- Albassam, A.; Ahad, A.; Alsultan, A.; Al-Jenoobi, F. Inhibition of cytochrome P450 enzymes by thymoquinone in human liver microsomes. Saudi Pharm. J. 2018, 26, 673–677. [Google Scholar] [CrossRef]
- Schwab, M.; Klotz, U. Pharmacokinetic considerations in the treatment of inflammatory bowel disease. Clin. Pharmacokinet. 2001, 40, 723–751. [Google Scholar] [CrossRef]
- Berends, S.; Strik, A.; Löwenberg, M.; D’Haens, G.; Mathôt, R. Clinical pharmacokinetic and pharmacodynamic considerations in the treatment of ulcerative colitis. Clin. Pharmacokinet. 2019, 58, 15–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Jenoobi, F.; Al-Suwayeh, S.; Muzaffar, I.; Alam, M.; Al-Kharfy, K.; Korashy, H.; Al-Mohizea, A.; Ahad, A.; Raish, M. Effects of Nigella sativa and Lepidium sativum on cyclosporine pharmacokinetics. Biomed. Res. Int. 2013, 2013, 953520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alrashedi, M.; Ali, A.; Ali, A.; Khan, L. Impact of thymoquinone on cyclosporine a pharmacokinetics and toxicity in rodents. J. Pharm. Pharmacol. 2018, 70, 1332–1339. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Organs | Disease | Effects of Black Cumin | Conclusion |
|---|---|---|---|
| Stomach | Peptic ulcer disease |
|
|
| Pancreas | Type 2 diabetes |
|
|
| Pancreatic cancer |
|
| |
| Liver | Nonalcoholic fatty liver disease (NAFLD) |
|
|
| Hepatitis C (HCV) |
|
| |
| Intestines | Overall impact |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jarmakiewicz-Czaja, S.; Zielińska, M.; Helma, K.; Sokal, A.; Filip, R. Effect of Nigella sativa on Selected Gastrointestinal Diseases. Curr. Issues Mol. Biol. 2023, 45, 3016-3034. https://doi.org/10.3390/cimb45040198
Jarmakiewicz-Czaja S, Zielińska M, Helma K, Sokal A, Filip R. Effect of Nigella sativa on Selected Gastrointestinal Diseases. Current Issues in Molecular Biology. 2023; 45(4):3016-3034. https://doi.org/10.3390/cimb45040198
Chicago/Turabian StyleJarmakiewicz-Czaja, Sara, Magdalena Zielińska, Kacper Helma, Aneta Sokal, and Rafał Filip. 2023. "Effect of Nigella sativa on Selected Gastrointestinal Diseases" Current Issues in Molecular Biology 45, no. 4: 3016-3034. https://doi.org/10.3390/cimb45040198