
Megalin Expression in Primary Oral Squamous Cell Carcinoma Is Associated with the Presence of Lymph Node Metastases, Vascular Invasion, and Lower Overall Survival

Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Tissue Specimens
2.2. Immunohistochemistry
2.3. Immunofluorescence
2.4. Quantification of Megalin-Positive Cells
2.5. Statistical Analysis
2.6. Ethical Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Chi, A.C.; Day, T.A.; Neville, B.W. Oral cavity and oropharyngeal squamous cell carcinoma—An update. CA A Cancer J. Clin. 2015, 65, 401–421. [Google Scholar] [CrossRef] [PubMed]
- D’Cruz, A.K.; Vaish, R.; Kapre, N.; Dandekar, M.; Gupta, S.; Hawaldar, R.; Agarwal, J.P.; Pantvaidya, G.; Chaukar, D.; Deshmukh, A.; et al. Head and Neck Disease Management Group. Elective versus Therapeutic Neck Dissection in Node-Negative Oral Cancer. N. Engl. J. Med. 2015, 373, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Blanchard, P.; Belkhir, F.; Temam, S.; El Khoury, C.; De Felice, F.; Casiraghi, O.; Patrikidou, A.; Mirghani, H.; Levy, A.; Even, C.; et al. Outcomes and prognostic factors for squamous cell carcinoma of the oral tongue in young adults: A single-institution case-matched analysis. Eur. Arch. Otorhinolaryngol. 2017, 274, 1683–1690. [Google Scholar] [CrossRef] [PubMed]
- Colevas, A.D.; Yom, S.S.; Pfister, D.G.; Spencer, S.; Adelstein, D.; Adkins, D.; Brizel, D.M.; Burtness, B.; Busse, P.M.; Caudell, J.J.; et al. NCCN Guidelines Insights: Head and Neck Cancers, Version 1.2018. J. Natl. Compr. Cancer Netw. 2018, 16, 479–490. [Google Scholar] [CrossRef] [Green Version]
- Christensen, E.I.; Birn, H. Megalin and cubilin: Multifunctional endocytic receptors. Nat. Rev. Mol. Cell Biol. 2002, 3, 258–267. [Google Scholar] [CrossRef]
- Christensen, E.I.; Birn, H. Megalin and cubilin: Synergistic endocytic receptors in renal proximal tubule. Am. J. Physiol. Renal. Physiol. 2001, 280, F562–F573. [Google Scholar] [CrossRef] [Green Version]
- Gomes, J.R.; Lobo, A.; Nogueira, R.; Terceiro, A.F.; Costelha, S.; Lopes, I.M.; Magalhães, A.; Summavielle, T.; Saraiva, M.J. Neuronal megalin mediates synaptic plasticity-a novel mechanism underlying intellectual disabilities in megalin gene pathologies. Brain Commun. 2020, 2, fcaa135. [Google Scholar] [CrossRef]
- Li, Y.; Cong, R.; Biemesderfer, D. The COOH terminus of megalin regulates gene expression in opossum kidney proximal tubule cells. Am. J. Physiol. Cell Physiol. 2008, 295, C529–C537. [Google Scholar] [CrossRef] [Green Version]
- Shah, M.; Baterina, O.Y., Jr.; Taupin, V.; Farquhar, M.G. ARH directs megalin to the endocytic recycling compartment to regulate its proteolysis and gene expression. J. Cell Biol. 2013, 202, 113–127. [Google Scholar] [CrossRef] [Green Version]
- Christensen, E.I.; Birn, H.; Storm, T.; Weyer, K.; Nielsen, R. Endocytic receptors in the renal proximal tubule. Physiology 2012, 27, 223–236. [Google Scholar] [CrossRef] [Green Version]
- Li, Y.; Cam, J.; Bu, G. Low-density lipoprotein receptor family: Endocytosis and signal transduction. Mol. Neurobiol. 2001, 23, 53–67. [Google Scholar]
- Spuch, C.; Ortolano, S.; Navarro, C. LRP-1 and LRP-2 receptors function in the membrane neuron. Trafficking mechanisms and proteolytic processing in Alzheimer’s disease. Front. Physiol. 2012, 3, 269. [Google Scholar] [CrossRef] [Green Version]
- Holt, S.K.; Karyadi, D.M.; Kwon, E.M.; Stanford, J.L.; Nelson, P.S.; Ostrander, E.A. Association of megalin genetic polymorphisms with prostate cancer risk and prognosis. Clin. Cancer Res. 2008, 14, 3823–3831. [Google Scholar] [CrossRef] [Green Version]
- Zang, X.; Zheng, F.; Hong, H.J.; Jiang, Y.; Song, Y.; Xia, Y. Neutrophil gelatinase-associated lipocalin protects renal tubular epithelial cells in hypoxia-reperfusion by reducing apoptosis. Int. Urol. Nephrol. 2014, 46, 1673–1679. [Google Scholar] [CrossRef]
- Jobst-Schwan, T.; Knaup, K.X.; Nielsen, R.; Hackenbeck, T.; Buettner-Herold, M.; Lechler, P.; Kroening, S.; Goppelt-Struebe, M.; Schloetzer-Schrehardt, U.; Fürnrohr, B.G.; et al. Renal uptake of the antiapoptotic protein survivin is mediated by megalin at the apical membrane of the proximal tubule. Am. J. Physiol. Renal. Physiol. 2013, 305, F734–F744. [Google Scholar] [CrossRef] [Green Version]
- Andersen, R.K.; Hammer, K.; Hager, H.; Christensen, J.N.; Ludvigsen, M.; Honoré, B.; Thomsen, M.B.; Madsen, M. Melanoma tumors frequently acquire LRP2/megalin expression, which modulates melanoma cell proliferation and survival rates. Pigment. Cell Melanoma Res. 2015, 28, 267–280. [Google Scholar] [CrossRef]
- Zulijani, A.; Dekanić, A.; Ćabov, T.; Jakovac, H. Metallothioneins and Megalin Expression Profiling in Premalignant and Malignant Oral Squamous Epithelial Lesions. Cancers 2021, 13, 4530. [Google Scholar] [CrossRef]
- El-Naggar, A.K.; Chan, J.K.C.; Grandis, J.R.; Takata, T.; Slootweg, P.J. WHO Classification of Head and Neck Tumours, 4th ed.; IARC Press: Lyon, France, 2017; pp. 105–115. [Google Scholar]
- Amin, M.B.; Edge, S.B.; Greene, F.L.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C.; et al. AJCC Cancer Staging Manual, 8th ed.; Springer: New York, NY, USA, 2017; pp. 79–94. [Google Scholar]
- Jakovac, H.; Stašić, N.; Krašević, M.; Jonjić, N.; Radošević-Stašić, B. Expression profiles of metallothionein-I/II and megalin/LRP-2 in uterine cervical squamous lesions. Virchows Arch. 2021, 478, 735–746. [Google Scholar] [CrossRef]
- Pedersen, M.Ø.; Hansen, P.B.; Nielsen, S.L.; Penkowa, M. Metallothionein-I + II and receptor megalin are altered in relation to oxidative stress in cerebral lymphomas. Leuk. Lymphoma. 2010, 51, 314–328. [Google Scholar] [CrossRef]
- Schuetz, A.N.; Yin-Goen, Q.; Amin, M.B.; Moreno, C.S.; Cohen, C.; Hornsby, C.D.; Yang, W.L.; Petros, J.A.; Issa, M.M.; Pattaras, J.G.; et al. Molecular classification of renal tumors by gene expression profiling. J. Mol. Diagn. 2005, 7, 206–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ammar, H.; Closset, J.L. Clusterin activates survival through the phosphatidylinositol 3-kinase/Akt pathway. J. Biol. Chem. 2008, 283, 12851–12861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pedersen, M.Ø.; Jensen, R.; Pedersen, D.S.; Skjolding, A.D.; Hempel, C.; Maretty, L.; Penkowa, M. Metallothionein-I+II in neuroprotection. Biofactors 2009, 35, 315–325. [Google Scholar] [CrossRef] [PubMed]
- Chung, R.S.; Hidalgo, J.; West, A.K. New insight into the molecular pathways of metallothionein-mediated neuroprotection and regeneration. J. Neurochem. 2008, 104, 14–20. [Google Scholar] [CrossRef]
- Jakovac, H.; Grubić Kezele, T.; Radošević-Stašić, B. Expression Profiles of Metallothionein I/II and Megalin in Cuprizone Model of De- and Remyelination. Neuroscience 2018, 388, 69–86. [Google Scholar] [CrossRef]
- Subash, A.; Sinha, P.; Singh, A. Revisiting the role of depth of invasion in clinical TNM staging. Oral. Oncol. 2020, 109, 104680. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Clinicopathological Characteristic | N | Percentage of Megalin-Positive Cells (Median, Range) | p-Value |
|---|---|---|---|
| N = 63 | |||
| Gender | |||
| Male | 39 | 40.0 (6.50–99.30) | 0.1082 |
| Female | 24 | 24.95 (2.90–96.3) | |
| Age | |||
| ≤65 | 34 | 29.40 (5.90–96.60) | 0.2495 |
| >65 | 29 | 40.00 (2.90–99.30) | |
| Smoking | |||
| Yes | 35 | 38.60 (7.10–96.30) | 0.4849 |
| No | 28 | 28.70 (2.90–99.30) | |
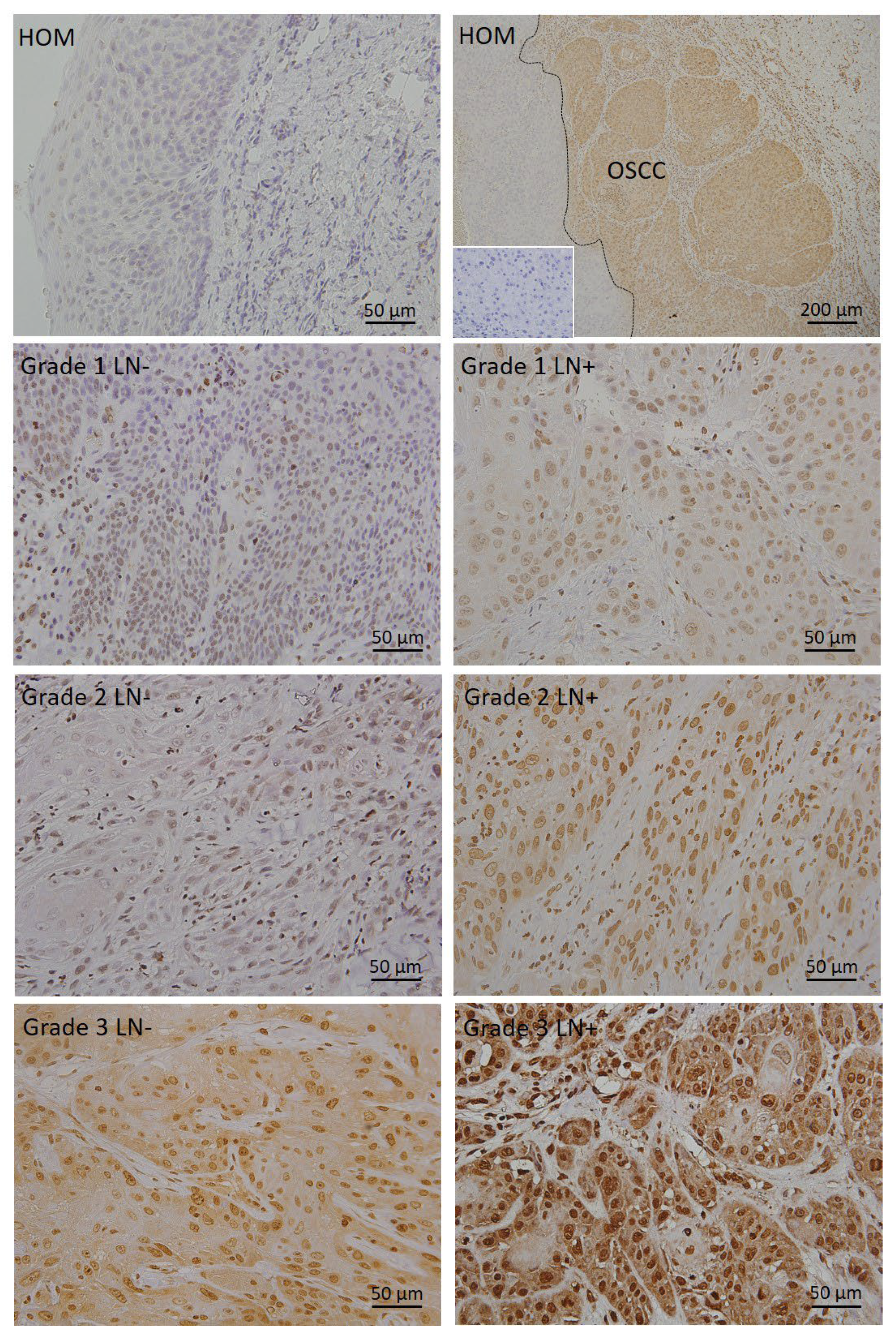
| Histopathological grade * | |||
| I | 34 | 16.901 (2.90–44.60) | 0.000001 |
| II | 22 | 65.102 (14.80–85.40) | |
| III | 7 | 94.903 (70.50–99.30) | |
| Lymph node metastases | |||
| Yes | 28 | 43.05 (6.50–99.30) | 0.0495 |
| No | 35 | 23.90 (2.90–96.30) | |
| Perineural invasion | |||
| Yes | 15 | 38.60 (7.10–85.40) | 0.5519 |
| No | 43 | 28.70 (2.90–99.30) | |
| Vascular invasion | |||
| Yes | 15 | 46.20 (10.60–94.90) | 0.0249 |
| No | 36 | 25.80 (2.90–89.80) | |
| Depth of invasion | |||
| ≤5 mm | 19 | 19.70 (2.90–99.30) | 0.1953 |
| >5 mm | 38 | 39.30 (6.50–89.80) | |
| TNM * | |||
| I | 16 | 26.85 (2.90–80.10) | 0.1853 |
| II | 8 | 18.65 (8.00–96.30) | |
| III | 17 | 32.90 (6.50–96.60) | |
| IV | 22 | 41.00 (10.60–99.30) |
| Clinicopathological Parameter | Overall Survival (Chi-Squared) | p-Value |
|---|---|---|
| Gender (male/female) | 2.6169 | 0.1057 |
| Age (<median value/≥median value) | 0.9908 | 0.3195 |
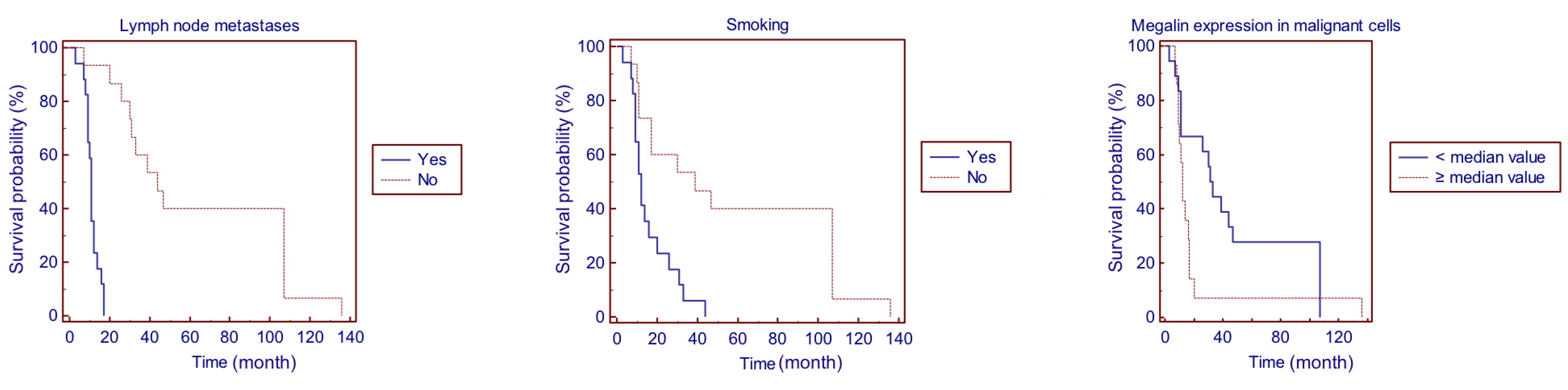
| Smoking (yes/no) | 9.8976 | 0.0017 |
| Lymph node metastases (yes/no) | 27.4622 | 0.0001 |
| Perineural invasion (yes/no) | 1.1767 | 0.2780 |
| Vascular invasion (yes/no) | 13.6816 | 0.0011 |
| Depth of invasion (≤5 mm/>5 mm) | 2.8700 | 0.0902 |
| Histopathological grade (I/II/III) | 2.2211 | 0.3294 |
| TNM (I/II/III/IV) | 15.6181 | 0.0014 |
| Percentage of megalin-expressing cells (<median value/≥median value) | 3.9729 | 0.0462 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zulijani, A.; Milardović, A.; Kovač, Z.; Perić, B.; Jakovac, H. Megalin Expression in Primary Oral Squamous Cell Carcinoma Is Associated with the Presence of Lymph Node Metastases, Vascular Invasion, and Lower Overall Survival. Curr. Issues Mol. Biol. 2023, 45, 2757-2766. https://doi.org/10.3390/cimb45040180
Zulijani A, Milardović A, Kovač Z, Perić B, Jakovac H. Megalin Expression in Primary Oral Squamous Cell Carcinoma Is Associated with the Presence of Lymph Node Metastases, Vascular Invasion, and Lower Overall Survival. Current Issues in Molecular Biology. 2023; 45(4):2757-2766. https://doi.org/10.3390/cimb45040180
Chicago/Turabian StyleZulijani, Ana, Ana Milardović, Zoran Kovač, Berislav Perić, and Hrvoje Jakovac. 2023. "Megalin Expression in Primary Oral Squamous Cell Carcinoma Is Associated with the Presence of Lymph Node Metastases, Vascular Invasion, and Lower Overall Survival" Current Issues in Molecular Biology 45, no. 4: 2757-2766. https://doi.org/10.3390/cimb45040180