
Downregulation of Tumour Necrosis Factor α Gene Expression in Peripheral Blood Mononuclear Cells Cultured in the Presence of Tofacitinib Prior to Therapy Is Associated with Clinical Remission in Patients with Rheumatoid Arthritis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethics Statement
2.2. Patients
2.3. Demographic, Clinical, and Immunological Evaluations
2.4. Peripheral Blood Fractionation
2.5. Cell Viability Test
2.6. Peripheral Blood Mononuclear Cells Culture
2.7. Total Ribonucleic Acid (RNA) Isolation and Reverse Transcriptase (RT) Reaction
2.8. Real-Time Quantitative Polymerase Chain Reaction (PCR)
2.9. Statistical Analysis
3. Results
3.1. Clinical and Immunological Characteristics and Therapeutic Response in Patients with Rheumatoid Arthritis at Baseline and after Three Months of Tofacitinib Therapy
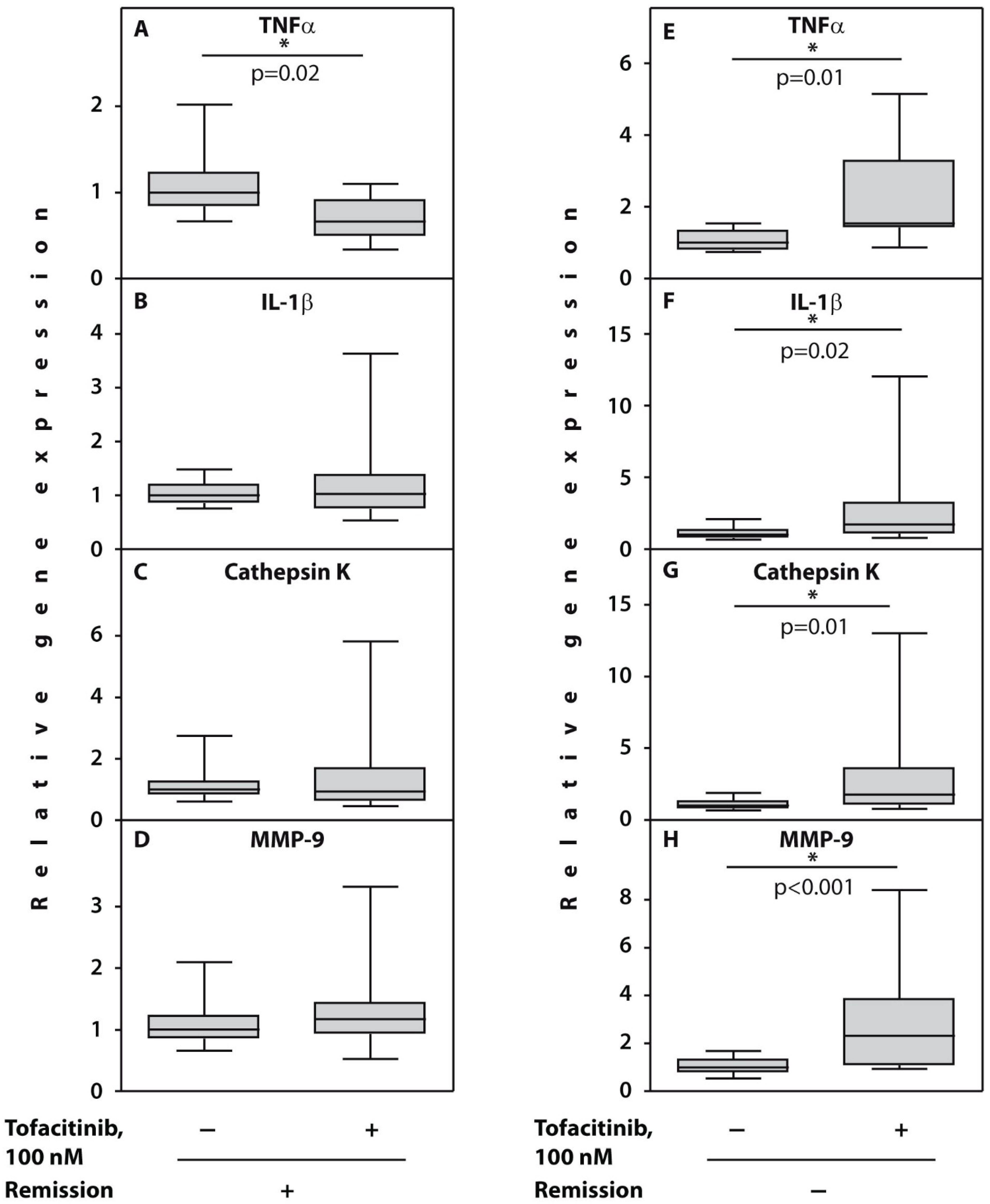
3.2. Gene Expression Analyses in the Peripheral Blood Mononuclear Cells Cultured with Tofacitinib Prior to Therapy
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- McInnes, I.B.; Schett, G. The pathogenesis of rheumatoid arthritis. N. Engl. J. Med. 2011, 365, 2205–2219. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komatsu, N.; Takayanagi, H. Inflammation and bone destruction in arthritis: Synergistic activity of immune and mesenchymal cells in joints. Front. Immunol. 2012, 3, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bartok, B.; Firestein, G.S. Fibroblast-like synoviocytes: Key effector cells in rheumatoid arthritis. Immunol. Rev. 2010, 233, 233–255. [Google Scholar] [CrossRef] [PubMed]
- Smolen, J.S.; Aletaha, D.; McInnes, I.B. Rheumatoid arthritis. Lancet 2016, 388, 2023–2038. [Google Scholar] [CrossRef]
- Atzeni, F.; Sarzi-Puttini, P.; Gorla, R.; Marchesoni, A.; Caporali, R. Switching rheumatoid arthritis treatments: An update. Autoimmun. Rev. 2011, 10, 397–403. [Google Scholar] [CrossRef]
- Winthrop, K.L. The emerging safety profile of JAK inhibitors in rheumatic disease. Nat. Rev. Rheumatol. 2017, 13, 234–243. [Google Scholar] [CrossRef]
- Strand, V.; Kremer, J.M.; Gruben, D.; Krishnaswami, S.; Zwillich, S.H.; Wallenstein, G.V. Tofacitinib in combination with conventional disease-modifying antirheumatic drugs in patients with active rheumatoid arthritis: Patient-reported outcomes from a phase III randomized controlled trial. Arthritis Care Res. 2017, 69, 592–598. [Google Scholar] [CrossRef] [Green Version]
- Gadina, M.; Le, M.T.; Schwartz, D.M.; Silvennoinen, O.; Nakayamada, S.; Yamaoka, K.; O’Shea, J.J. Janus kinases to Jakinibs: From basic insights to clinical practice. Rheumatology 2019, 58, i4–i16. [Google Scholar] [CrossRef]
- Tsuchiya, H.; Fujio, K. The current status of the search for biomarkers for optimal therapeutic drug selection for patients with rheumatoid arthritis. Int. J. Mol. Sci. 2021, 22, 9534. [Google Scholar] [CrossRef]
- Tchetina, E.V.; Satybaldyev, A.M.; Markova, G.A.; Samarkina, E.Y.; Lila, A.M. Putative association between low baseline gene expression in the peripheral blood and clinical remission in rheumatoid arthritis patients treated with tofacitinib. Life 2021, 11, 1385. [Google Scholar] [CrossRef]
- Grassi, F.; Cristino, S.; Toneguzzi, S.; Piacentini, A.; Facchini, A.; Lisignoli, G. CXCL12 chemokine up-regulates bone resorption and MMP-9 release by human osteoclasts: CXCL12 levels are increased in synovial and bone tissue of rheumatoid arthritis patients. J. Cell. Physiol. 2004, 199, 244–251. [Google Scholar] [CrossRef]
- Brömme, D.; Lecaille, F. Cathepsin K inhibitors for osteoporosis and potential off-target effects. Expert Opin. Investig. Drugs 2009, 18, 585–600. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, K.S.; Choi, H.M.; Lee, Y.A.; Choi, I.A.; Lee, S.H.; Hong, S.J.; Yang, H.I.; Yoo, M.C. Expression levels and association of gelatinases MMP-2 and MMP-9 and collagenases MMP-1 and MMP-13 with VEGF in synovial fluid of patients with arthritis. Rheumatol. Int. 2011, 31, 543–547. [Google Scholar] [CrossRef] [PubMed]
- Burrage, P.S.; Mix, K.S.; Brinckerhoff, C.F. Matrix metalloproteinases: Role in arthritis. Front. Biosci. 2006, 11, 529–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Richardson, V.J. Divergent and synergistic regulation of matrix metalloprotease production by cytokines in combination with C-C chemokines. Int. J. Immunopathol. Pharmacol. 2010, 23, 715–726. [Google Scholar] [CrossRef] [Green Version]
- Kong, R.; Sun, L.; Li, H.; Wang, D. The role of NLRP3 inflammasome in the pathogenesis of rheumatic disease. Autoimmunity 2022, 55, 1–7. [Google Scholar] [CrossRef]
- Furst, D.E.; Emery, P. Rheumatoid arthritis pathophysiology: Update on emerging cytokine and cytokine-associated cell targets. Rheumatology 2014, 53, 1560–1569. [Google Scholar] [CrossRef] [Green Version]
- Huang, J.L.; Wu, S.Y.; Xie, X.J.; Wang, M.X.; Zhu, S.; Gu, J.R. Inhibiting effects of Leflunomide metabolite on overexpression of CD147, MMP-2 and MMP-9 in PMA differentiated THP-1 cells. Eur. J. Rharmacol. 2011, 670, 304–310. [Google Scholar] [CrossRef]
- Vandooren, B.; Kruithof, E.; Yu, D.T.Y.; Rihl, M.; Gu, J.; De Rycke, L.; Van Den Bosch, F.; Veys, E.M.; De Keyser, F.; Baeten, D. Involvement of matrix metalloproteinases and their inhibitors in peripheral synovitis and down-regulation by tumor necrosis factor alpha blockade in spondylarthropathy. Arthritis Rheum. 2004, 50, 2942–2953. [Google Scholar] [CrossRef]
- Matsushita, I.; Uzuki, M.; Matsuno, H.; Sugiyama, E.; Kimura, T. Rheumatoid nodulosis during methotrexate therapy in a patient with rheumatoid arthritis. Mod. Rheumatol. 2006, 16, 401–403. [Google Scholar] [CrossRef]
- Tchetina, E.V.; Poole, A.R.; Zaitseva, E.M.; Sharapova, E.P.; Kashevarova, N.G.; Taskina, E.A.; Alekseeva, L.I.; Semyonova, L.A.; Glukhova, S.I.; Kuzin, A.N.; et al. Differences in mammalian target of rapamycin gene expression in the peripheral blood and articular cartilages of osteoarthritic patients and disease activity. Arthritis 2013, 2013, 461486. [Google Scholar] [CrossRef] [PubMed]
- Scherer, H.U.; Dorner, T.; Burmester, G.R. Patient–tailored therapy in rheumatoid arthritis: An editorial review. Curr. Opin. Rheumatol. 2010, 22, 237–245. [Google Scholar] [CrossRef] [PubMed]
- Verweij, C.L. Transcript profiling towards personalised medicine in rheumatoid arthritis. Neth. J. Med. 2009, 67, 364–371. [Google Scholar] [PubMed]
- Ghoreschi, K.; Jessson, M.I.; Li, X.; Lee, J.L.; Ghosh, S.; Alsup, J.W.; Warner, J.D.; Tanaka, M.; Steward-Tharp, S.C.; Gadina, M.; et al. Modulation of innate and adaptive immune response by tofacitinib (CP-690,550). J. Immunol. 2011, 186, 4234–4243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isailovic, N.; Ceribelli, A.; Cincinelli, G.; Vecellio, M.; Guidelli, G.M.; Caproli, M.; Luciano, N.; Motta, F.; Selmi, C.; De Santis, M. Lymphocyte modulation by tofacitinib in patients with rheumatoid arthritis. Clin. Exp. Immunol. 2021, 205, 142–149. [Google Scholar] [CrossRef]
- Meyer, D.M.; Jesson, M.I.; Li, X.; Elrick, M.M.; Funckes-Shippy, C.L.; Warner, J.D.; Gross, C.J.; Martin E Dowty, M.E.; Ramaiah, S.K.; Hirsch, J.L.; et al. Anti-inflammatory activity and neutrophil reductions mediated by the JAK1/JAK3 inhibitor, CP-690,550, in rat adjuvant-induced arthritis. J. Inflamm. 2010, 7, 41. [Google Scholar] [CrossRef] [Green Version]
- Yarilina, A.; Xu, K.; Chan, C.; Ivashkiv, L.B. Regulation of inflammatory responses in tumor necrosis factor-activated and rheumatoid arthritis synovial macrophages by JAK inhibitors. Arthritis Rheum. 2012, 64, 3856–3866. [Google Scholar] [CrossRef] [Green Version]
- Kothari, P.; Pestana, R.; Mesraoua, R.; Elchaki, R.; Khan, K.M.F.; Dannenberg, A.J.; Falcone, D.J. Il-6-mediated induction of matrix metalloproteinase-9 is modulated by JAK-dependent IL-10 expression in macrophages. J. Immunol. 2014, 192, 349–351. [Google Scholar] [CrossRef] [Green Version]
- Kondo, N.; Kuroda, T.; Kobayashi, D. Cytokine Networks in the Pathogenesis of Rheumatoid Arthritis. Int. J. Mol. Sci. 2021, 22, 10922. [Google Scholar] [CrossRef]
- Ram, M.; Sherer, Y.; Shoenfeld, Y. Matrix metalloproteinase-9 and autoimmune diseases. J. Clin. Immunol. 2006, 26, 299–307. [Google Scholar] [CrossRef]
- Salminen-Mankonen, H.J.; Morko, J.; Vuorio, E. Role of cathepsin K in normal joints and in the development of arthritis. Curr. Drug Targets 2007, 8, 315–323. [Google Scholar] [CrossRef] [PubMed]
- Crowson, C.S.; Rahman, M.U.; Matteson, E.L. Which measure of inflammation to use? A comparison of erythrocyte sedimentation rate and C-reactive protein measurements from randomized clinical trials of golimumab in rheumatoid arthritis. J. Rheumatol. 2009, 36, 1606–1610. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Subgroup 1 Patients Who Achieved Remission (n = 6) DAS28 < 2.6 | p | Subgroup 2 Other Examined Patients with RA (n = 6) | p | p′ Prior to Therapy | |||
|---|---|---|---|---|---|---|---|
| Baseline (n = 6) Me [IQR] | After 3 Months (n = 6) Me [IQR] | Baseline (n = 6) Me [IQR] | After 3 Months (n = 6) Me [IQR] | ||||
| Age, years # | 46.5 [29.5; 59.5] | 60 [41.5; 69] | 0.18 | ||||
| Disease duration, months # | 30 [16.5; 108] | 21 [6; 39] | 0.42 | ||||
| IgM RF, mU/L # | 13 [8; 18] | 48 [12; 75] | 0.07 | ||||
| ACPA, U/mL # | 30 [14; 74.5] | 35.5 [25.5; 40] | 0.69 | ||||
| CRP, mg/mL | 18.6 [2.4; 98] | 3.9 [0.25; 8.6] | 0.06 | 17.5 [8.7; 83.2] | 5.2 [1; 28.5] | 0.31 | 0.93 |
| ESR, mm | 30 [14; 74.5] | 13 [8; 18] | 0.12 | 35.5 [25.5; 40] | 48.0 [12; 75] | 0.43 | 0.69 |
| DAS 28 | 4.85 [3.6; 6.2] | 1.95 [1.3; 2.2] | 0.03 * | 6.2 [5.3; 7.0] | 4.8 [3.9; 5.4] | 0.03 * | 0.09 |
| ΔDAS 28 # | 2.77 [1.9;4.2] | 1.4 [0.9; 2.1] | 0.01 * | ||||
| Number of swollen joints | 5.5 [3; 11.5] | 0 [0; 0.5] | 0.03 * | 12.5 [7; 17] | 2 [1; 8.5] | 0.03 * | 0.06 |
| Number of tender joints | 4 [2.5; 10.5] | 0 [0; 0] | - | 13.5 [7; 20.5] | 6.5 [1.5; 15.5] | 0.06 | 0.04 # |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tchetina, E.V.; Markova, G.A.; Satybaldyev, A.M.; Lila, A.M. Downregulation of Tumour Necrosis Factor α Gene Expression in Peripheral Blood Mononuclear Cells Cultured in the Presence of Tofacitinib Prior to Therapy Is Associated with Clinical Remission in Patients with Rheumatoid Arthritis. Curr. Issues Mol. Biol. 2022, 44, 1941-1949. https://doi.org/10.3390/cimb44050132
Tchetina EV, Markova GA, Satybaldyev AM, Lila AM. Downregulation of Tumour Necrosis Factor α Gene Expression in Peripheral Blood Mononuclear Cells Cultured in the Presence of Tofacitinib Prior to Therapy Is Associated with Clinical Remission in Patients with Rheumatoid Arthritis. Current Issues in Molecular Biology. 2022; 44(5):1941-1949. https://doi.org/10.3390/cimb44050132
Chicago/Turabian StyleTchetina, Elena V., Galina A. Markova, Azamat M. Satybaldyev, and Aleksandr M. Lila. 2022. "Downregulation of Tumour Necrosis Factor α Gene Expression in Peripheral Blood Mononuclear Cells Cultured in the Presence of Tofacitinib Prior to Therapy Is Associated with Clinical Remission in Patients with Rheumatoid Arthritis" Current Issues in Molecular Biology 44, no. 5: 1941-1949. https://doi.org/10.3390/cimb44050132