
Drug Investigation to Dampen the Comorbidity of Rheumatoid Arthritis and Osteoporosis via Molecular Docking Test



Abstract
:1. Introduction
2. Hypothesis
3. Methods
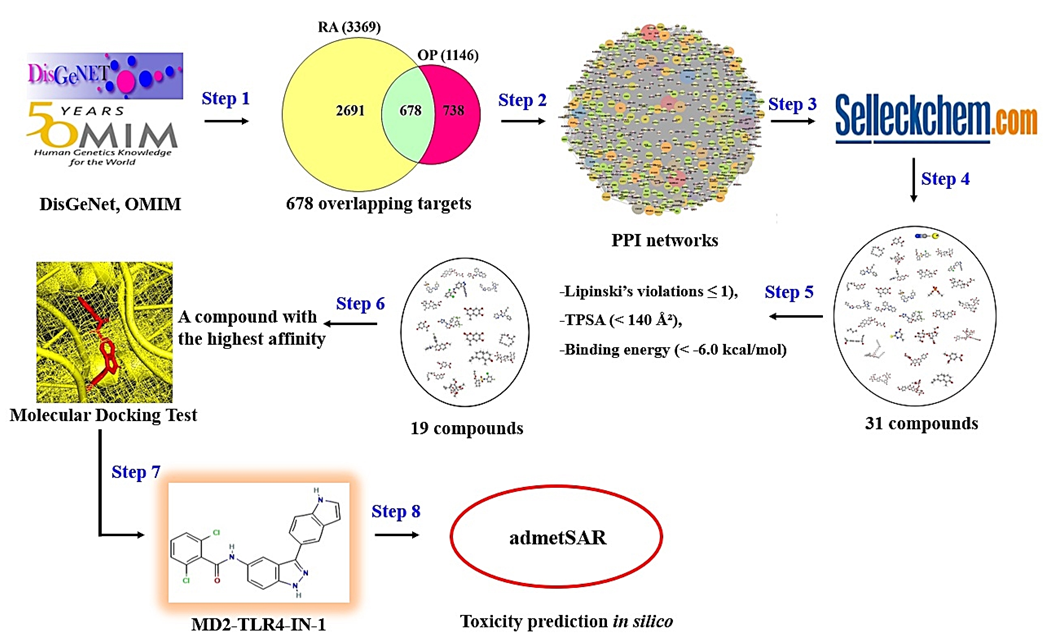
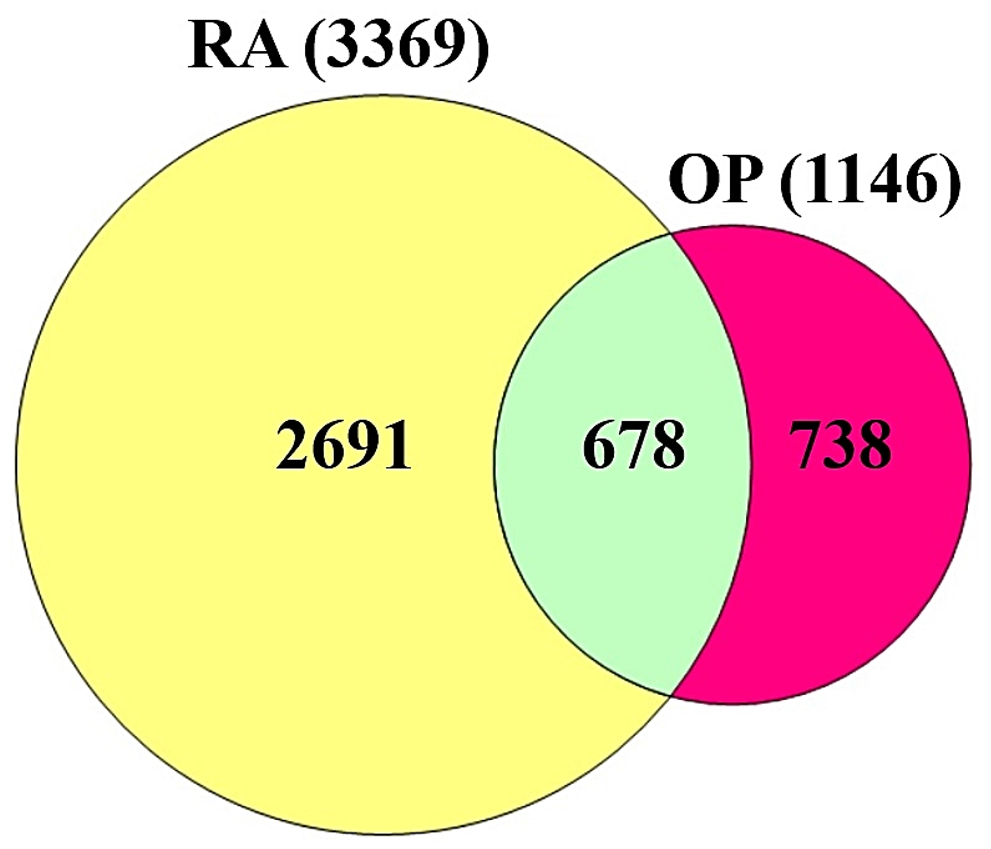
3.1. Retrieval of RA or OP Targets and Identification of Overlapping Targets
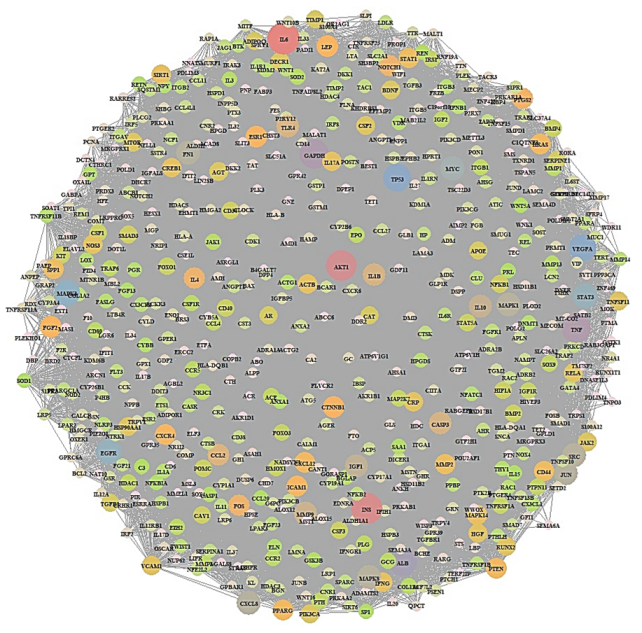
3.2. PPI Network Analysis
3.3. Collection of Ligands
3.4. The Screening of Ligands
3.5. The Preparation of Ligands and a Target for MDT
3.6. The Prediction of Toxicological Properties of the Key Ligand in Silico
4. Results
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
International Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| BMD | Bone mineral density |
| COX | Cyclooxygenase |
| COX-1 | Cyclooxygenase-1 |
| COX-2 | Cyclooxygenase-2 |
| CRP | C-reactive protein |
| DMARDs | Disease-modifying anti-rheumatic drugs |
| IL-1 | Interleukin 1 |
| IL-6 | Interleukin 6 |
| IL-17 | Interleukin 17 |
| NSAIDs | Non-steroidal anti-inflammatory drugs |
| OP | Osteoporosis |
| PPI | Protein–protein interaction |
| RA | Rheumatoid arthritis |
| TCZ | Tocilizumab |
| TPSA | Topological polar surface area |
References
- Llorente, I.; García-Castañeda, N.; Valero, C.; González-Álvaro, I.; Castañeda, S. Osteoporosis in Rheumatoid Arthritis: Dangerous Liaisons. Front. Med. 2020, 802. [Google Scholar] [CrossRef] [PubMed]
- McInnes, I.B.; Schett, G. Pathogenetic insights from the treatment of rheumatoid arthritis. Lancet 2017, 389, 2328–2337. [Google Scholar] [CrossRef] [Green Version]
- Bullock, J.; Rizvi, S.A.A.; Saleh, A.M.; Ahmed, S.S.; Do, D.P.; Ansari, R.A.; Ahmed, J. Rheumatoid Arthritis: A Brief Overview of the Treatment. Med. Princ. Pract. 2019, 27, 501. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, E.S.; Firestein, G.S. Rheumatoid arthritis: Regulation of synovial inflammation. Int. J. Biochem. Cell Biol. 2004, 36, 372–378. [Google Scholar] [CrossRef]
- Jiang, Y.; Zhong, M.; Long, F.; Yang, R.; Zhang, Y.; Liu, T. Network Pharmacology-Based Prediction of Active Ingredients and Mechanisms of Lamiophlomis rotata (Benth.) Kudo Against Rheumatoid Arthritis. Front. Pharmacol. 2019, 1435. [Google Scholar] [CrossRef] [Green Version]
- Smolen, J.S.; Aletaha, D.; Koeller, M.; Weisman, M.H.; Emery, P. New therapies for treatment of rheumatoid arthritis. Lancet 2007, 370, 1861–1874. [Google Scholar] [CrossRef]
- Stevenson, M.; Archer, R.; Tosh, J.; Simpson, E.; Everson-Hock, E.; Stevens, J.; Hernandez, M.; Paisley, S.; Dickinson, K.; Scott, D.; et al. Adalimumab, etanercept, infliximab, certolizumab pegol, golimumab, tocilizumab and abatacept for the treatment of rheumatoid arthritis not previously treated with disease-modifying antirheumatic drugs and after the failure of conventional disease-modifying antirheumatic drugs only: Systematic review and economic evaluation. Health Technol. Assess. 2016, 20, 1–610. [Google Scholar] [CrossRef] [Green Version]
- Betts, K.A.; Griffith, J.; Ganguli, A.; Li, N.; Douglas, K.; Wu, E.Q. Economic Burden and Treatment Patterns of Cycling between Conventional Synthetic Disease-modifying Antirheumatic Drugs among Biologic-treated Patients with Rheumatoid Arthritis. Clinical Therapeutics 2016, 38, 1205–1216. [Google Scholar] [CrossRef]
- Tanaka, Y. Managing Osteoporosis and Joint Damage in Patients with Rheumatoid Arthritis: An Overview. J. Clin. Med. 2021, 10, 1241. [Google Scholar] [CrossRef]
- Osterhoff, G.; Morgan, E.F.; Shefelbine, S.J.; Karim, L.; McNamara, L.M.; Augat, P. Bone mechanical properties and changes with osteoporosis. Injury 2016, 47, S11. [Google Scholar] [CrossRef] [Green Version]
- Alexandru, D.; So, W. Evaluation and Management of Vertebral Compression Fractures. Perm. J. 2012, 16, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, M.-X.; Yu, Q. Primary osteoporosis in postmenopausal women. Chronic Dis. Transl. Med. 2015, 1, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sözen, T.; Özışık, L.; Başaran, N.Ç. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46. [Google Scholar] [CrossRef] [PubMed]
- Ginaldi, L.; Di Benedetto, M.C.; Martinis, M. De Osteoporosis, inflammation and ageing. Immun. Ageing I A 2005, 2, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hardy, R.; Cooper, M.S. Bone loss in inflammatory disorders. J. Endocrinol. 2009, 201, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Tella, S.H.; Gallagher, J.C. Biological agents in management of osteoporosis. Eur. J. Clin. Pharmacol. 2014, 70, 1291–1301. [Google Scholar] [CrossRef] [PubMed]
- Lewiecki, E.M. New targets for intervention in the treatment of postmenopausal osteoporosis. Nat. Rev. Rheumatol. 2011, 7, 631–638. [Google Scholar] [CrossRef]
- Ginosyan, K.; Jndoyan, Z.; Ghazinyan, I.; Vardanyan, V. Benefits and disadvantages of biologic agents in chronic inflammatory arthritis. Int. J. Clin. Rheumatol. 2020, 15, 6–9. [Google Scholar] [CrossRef]
- Thong, B.Y.-H.; Tan, T.-C. Epidemiology and risk factors for drug allergy. Br. J. Clin. Pharmacol. 2011, 71, 684–700. [Google Scholar] [CrossRef]
- Parker, S.E.; Davey, P.; Davey, P.G. Pharmacoeconomics of intravenous drug administration. Pharm. 1992, 1, 103–115. [Google Scholar] [CrossRef]
- Gomes, E.; Demoly, P. Epidemiology of hypersensitivity drug reactions. Curr. Opin. Allergy Clin. Immunol. 2005, 5, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Crofford, L.J. Use of NSAIDs in treating patients with arthritis. Arthritis Res. Ther. 2013, 15, S2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, P.; Emery, P.; Evans, J.F.; Fenner, H.; Hawkey, C.J.; Patrono, C.; Smolen, J.; Breedveld, F.; Day, R.; Dougados, M.; et al. Interpreting the clinical significance of the differential inhibition of cyclooxygenase-1 and cyclooxygenase-2. Rheumatology 1999, 38, 779–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lisowska, B.; Kosson, D.; Domaracka, K. Positives and negatives of nonsteroidal anti-inflammatory drugs in bone healing: The effects of these drugs on bone repair. Drug Des. Dev. Ther. 2018, 12, 1809. [Google Scholar] [CrossRef]
- Gaubitz, M. Osteoporose–häufige Komorbidität bei Rheumapatienten. Z. Für Rheumatol. 2019, 78, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Schneeweiss, S.; Liu, J.; Daniel, G.W.; Chang, C.-L.; Garneau, K.; Solomon, D.H. Risk of osteoporotic fracture in a large population-based cohort of patients with rheumatoid arthritis. Arthritis Res. Ther. 2010, 12, R154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Castañeda, S.; Garcés-Puentes, M.V.; Bernad Pineda, M. Pathophysiology of osteoporosis in chronic inflammatory joint diseases. Rev. De Osteoporos. Y Metab. Miner. 2021, 13, 32–38. [Google Scholar] [CrossRef]
- Pushpakom, S.; Iorio, F.; Eyers, P.A.; Escott, K.J.; Hopper, S.; Wells, A.; Doig, A.; Guilliams, T.; Latimer, J.; McNamee, C.; et al. Drug repurposing: Progress, challenges and recommendations. Nat. Rev. Drug Discov. 2018, 18, 41–58. [Google Scholar] [CrossRef]
- Somolinos, F.J.; León, C.; Guerrero-Aspizua, S. Drug repurposing using biological networks. Processes 2021, 9, 1057. [Google Scholar] [CrossRef]
- Rudrapal, M.; Khairnar, S.J.; Jadhav, A.G. Drug Repurposing (DR): An Emerging Approach in Drug Discovery. In Drug Repurposing-Hypothesis, Molecular Aspects and Therapeutic Applications; IntechOpen: London, UK, 2020. [Google Scholar] [CrossRef]
- Gil, C.; Martinez, A. Is drug repurposing really the future of drug discovery or is new innovation truly the way forward? Expert Opin. Drug Discov. 2021, 16, 829–831. [Google Scholar] [CrossRef]
- Hodos, R.A.; Kidd, B.A.; Shameer, K.; Readhead, B.P.; Dudley, J.T. Computational Approaches to Drug Repurposing and Pharmacology. Wiley Interdiscip. Reviews. Syst. Biol. Med. 2016, 8, 186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, G.; Wang, W.; Wang, X.; Xu, M.; Zhang, L.; Ding, L.; Guo, R.; Shi, Y. Network pharmacology-based strategy to investigate pharmacological mechanisms of Zuojinwan for treatment of gastritis. BMC Complementary Altern. Med. 2018, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Yip, K.W.; Liu, F.-F. Small Molecule Screens. Encycl. Cancer 2011, 3451–3455. [Google Scholar] [CrossRef]
- Zhang, M.-Q.; Wilkinson, B. Drug discovery beyond the “rule-of-five”. Curr. Opin. Biotechnol. 2007, 18, 478–488. [Google Scholar] [CrossRef]
- Matsson, P.; Kihlberg, J. How Big Is Too Big for Cell Permeability? J. Med. Chem. 2017, 60, 1662–1664. [Google Scholar] [CrossRef] [Green Version]
- Shityakov, S.; Förster, C. In silico predictive model to determine vector-mediated transport properties for the blood–brain barrier choline transporter. Adv. Appl. Bioinform. Chem. AABC 2014, 7, 23. [Google Scholar] [CrossRef] [Green Version]
- Khanal, P.; Patil, B.M.; Chand, J.; Naaz, Y. Anthraquinone Derivatives as an Immune Booster and their Therapeutic Option Against COVID-19. Nat. Prod. Bioprospecting 2020, 10, 325. [Google Scholar] [CrossRef]
- Yang, H.; Lou, C.; Sun, L.; Li, J.; Cai, Y.; Wang, Z.; Li, W.; Liu, G.; Tang, Y. admetSAR 2.0: Web-service for prediction and optimization of chemical ADMET properties. Bioinformatics 2019, 35, 1067–1069. [Google Scholar] [CrossRef]
- Boulanger, M.J.; Chow, D.-c.; Brevnova, E.E.; Garcia, K.C. Hexameric structure and assembly of the interleukin-6/IL-6 alpha-receptor/gp130 complex. Science (New York N.Y.) 2003, 300, 2101–2104. [Google Scholar] [CrossRef]
- Somers, W.; Stahl, M.; Seehra, J.S. 1.9 A crystal structure of interleukin 6: Implications for a novel mode of receptor dimerization and signaling. EMBO J. 1997, 16, 989–997. [Google Scholar] [CrossRef] [Green Version]
- Yokota, T.; Arai, N.; De Vries, J.; Spits, H.; Banchereau, J.; Zlotnik, A.; Rennick, D.; Howard, M.; Takebe, Y.; Miyatake, S.; et al. Molecular Biology of Interleukin 4 and Interleukin 5 Genes and Biology of their Products that Stimulate B Cells, T Cells and Hemopoietic Cells. Immunol. Rev. 1988, 102, 137–187. [Google Scholar] [CrossRef] [PubMed]
- Gelinas, A.D.; Davies, D.R.; Edwards, T.E.; Rohloff, J.C.; Carter, J.D.; Zhang, C.; Gupta, S.; Ishikawa, Y.; Hirota, M.; Nakaishi, Y.; et al. Crystal Structure of Interleukin-6 in Complex with a Modified Nucleic Acid Ligand. J. Biol. Chem. 2014, 289, 8720. [Google Scholar] [CrossRef] [Green Version]
- Hashizume, M.; Mihara, M. The roles of interleukin-6 in the pathogenesis of rheumatoid arthritis. Arthritis 2011, 2011, 765624. [Google Scholar] [CrossRef]
- Scheller, J.; Chalaris, A.; Schmidt-Arras, D.; Rose-John, S. The pro- and anti-inflammatory properties of the cytokine interleukin-6. Biochim. Et Biophys. Acta (BBA)-Mol. Cell Res. 2011, 1813, 878–888. [Google Scholar] [CrossRef] [Green Version]
- Ogata, A.; Kato, Y.; Higa, S.; Yoshizaki, K. IL-6 inhibitor for the treatment of rheumatoid arthritis: A comprehensive review. Mod. Rheumatol. 2019, 29, 258–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Zhou, Z.; Zhang, Y.; Yang, H. IL-6 Contributes to the Defective Osteogenesis of Bone Marrow Stromal Cells from the Vertebral Body of the Glucocorticoid-Induced Osteoporotic Mouse. PLoS ONE 2016, 11, 154677. [Google Scholar] [CrossRef] [Green Version]
- Roodman, G.D. Perspectives: Interleukin-6: An osteotropic factor? J. Bone Miner. Res. 1992, 7, 475–478. [Google Scholar] [CrossRef] [PubMed]
- Ohshima, S.; Saeki, Y.; Mima, T.; Sasai, M.; Nishioka, K.; Nomura, S.; Kopf, M.; Katada, Y.; Tanaka, T.; Suemura, M.; et al. Interleukin 6 plays a key role in the development of antigen-induced arthritis. Proc. Natl. Acad. Sci. USA 1998, 95, 8222–8226. [Google Scholar] [CrossRef] [Green Version]
- Denya, I.; Malan, S.F.; Joubert, J. Indazole derivatives and their therapeutic applications: A patent review (2013–2017). Expert Opin. Ther. Pat. 2018, 28, 441–453. [Google Scholar] [CrossRef]
- Zhang, S.-G.; Liang, C.-G.; Zhang, W.-H. Recent Advances in Indazole-Containing Derivatives: Synthesis and Biological Perspectives. Molecules 2018, 23, 2783. [Google Scholar] [CrossRef] [Green Version]
- Cheekavolu, C.; Muniappan, M. In vivo and In vitro Anti-Inflammatory Activity of Indazole and Its Derivatives. J. Clin. Diagn. Res. JCDR 2016, 10, FF01. [Google Scholar] [CrossRef] [PubMed]
- Cerecetto, H.; Gerpe, A.; González, M.; Arán, V.J.; De Ocáriz, C.O. Pharmacological properties of indazole derivatives: Recent developments. Mini Rev. Med. Chem. 2005, 5, 869–878. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Target | Degrees of Value |
|---|---|---|
| 1 | IL-6 | 432 |
| 2 | INS | 317 |
| 3 | AKT1 | 312 |
| 4 | TNF | 289 |
| 5 | GAPDH | 288 |
| 6 | TP53 | 267 |
| 7 | VEGFA | 266 |
| 8 | MAPK3 | 242 |
| 9 | EGFR | 237 |
| 10 | STAT3 | 236 |
| 11 | CXCL8 | 216 |
| 12 | JUN | 216 |
| 13 | MAPK1 | 215 |
| 14 | SRC | 215 |
| 15 | MMP9 | 215 |
| 16 | IGF1 | 209 |
| 17 | IL-10 | 206 |
| 18 | CASP3 | 195 |
| 19 | IL-1B | 195 |
| 20 | TLR4 | 194 |
| Compounds | Lipinski Rules | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| MW | HBA | HBD | MLogP | Lipinski’s violations | Bioavailability Score | TPSA | Compound Classification | ||
| No. | <500 | <10 | ≤5 | ≤4.15 | ≤1 | >0.1 | <140 Å2 | ||
| 1 | Forsythoside B | 756.70 | 19 | 11 | −3.93 | 3 | 0.17 | 304.21 | Oligosaccharides |
| 2 | Pectolinarin | 622.57 | 15 | 7 | −3.03 | 3 | 0.17 | 227.20 | Flavonoid-7-O-glycosides |
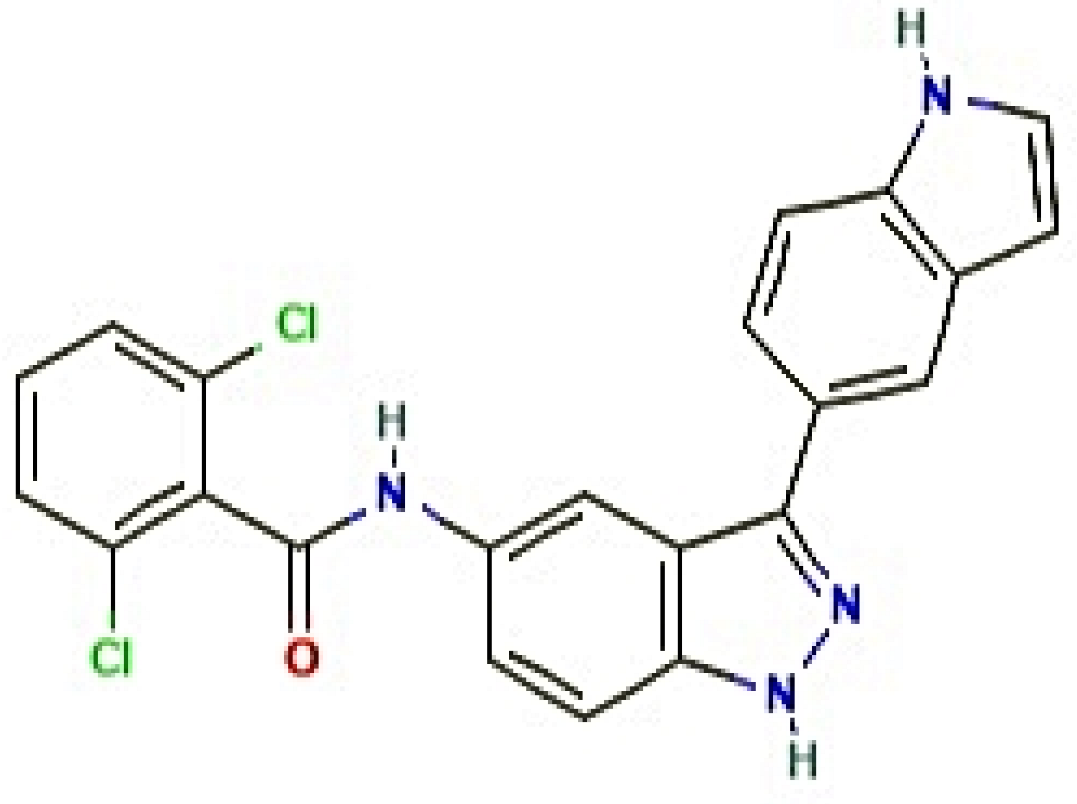
| 3 | MD2-TLR4-IN-1 | 421.28 | 2 | 3 | 4.01 | 0 | 0.55 | 73.57 | Indazole |
| 4 | Aprepitant | 534.43 | 12 | 2 | 4.05 | 1 | 0.55 | 83.24 | Phenylmorpholines |
| 5 | Mulberroside A | 568.52 | 14 | 10 | −2.97 | 3 | 0.17 | 239.22 | Stilbene glycosides |
| 6 | Homoplantaginin | 462.40 | 11 | 6 | −1.89 | 2 | 0.17 | 179.28 | Flavonoid-7-O-glycosides |
| 7 | NE 52-QQ57 | 416.52 | 6 | 1 | 3.46 | 0 | 0.55 | 81.14 | Pyrazolo[1,5-a]pyrimidines |
| 8 | Madecassic acid | 504.70 | 6 | 5 | 3.33 | 1 | 0.55 | 118.22 | Triterpenoids |
| 9 | GSK583 | 398.45 | 5 | 2 | 3.36 | 0 | 0.55 | 96.12 | Aminoquinolines and derivatives |
| 10 | IQ 3 | 341.32 | 6 | 0 | 2 | 0 | 0.55 | 77.58 | Quinoxalines |
| 11 | Methylprednisolone | 374.47 | 5 | 3 | 1.52 | 0 | 0.55 | 94.83 | 21-Hydroxysteroids |
| 12 | Hydrocortisone hemisuccinate | 462.53 | 8 | 3 | 1.29 | 0 | 0.55 | 138.20 | Gluco/mineralocorticoids, progestogens, and derivatives |
| 13 | 20(S)-Ginsenoside Rh1 | 638.87 | 9 | 7 | 1.77 | 2 | 0.17 | 160.07 | Triterpene saponins |
| 14 | Stylopine | 323.34 | 5 | 0 | 2.56 | 0 | 0.55 | 323.34 | Protoberberine alkaloids and derivatives |
| 15 | Methylprednisolone Acetate | 416.51 | 6 | 2 | 1.86 | 0 | 0.55 | 100.90 | Gluco/mineralocorticoids, progestogens, and derivatives |
| 16 | Gardenoside | 404.37 | 11 | 6 | −2.62 | 2 | 0.11 | 175.37 | Iridoid O-glycosides |
| 17 | 4-Methylesculetin | 192.17 | 4 | 2 | 0.76 | 0 | 0.55 | 70.67 | 6,7-Dihydroxycoumarins |
| 18 | Auraptene | 298.38 | 3 | 0 | 3.51 | 0 | 0.55 | 39.44 | Terpene lactones |
| 19 | AX-024 HCl | 375.86 | 4 | 0 | 3.86 | 0 | 0.55 | 21.70 | Neoflavenes |
| 20 | APX-115 free base | 279.34 | 2 | 1 | 2.66 | 0 | 0.55 | 50.68 | Pyrazolylpyridines |
| 21 | Resatorvid | 361.82 | 5 | 1 | 2.44 | 0 | 0.55 | 80.85 | Sulfanilides |
| 22 | Myrislignan | 374.43 | 6 | 2 | 1.97 | 0 | 0.55 | 77.38 | Lignans, neolignans, and related compounds |
| 23 | Muscone | 238.41 | 1 | 0 | 3.92 | 0 | 0.55 | 17.07 | Cyclic ketones |
| 24 | 2′,5′-Dihydroxyacetophenone | 152.15 | 3 | 2 | 0.51 | 0 | 0.55 | 57.53 | Alkyl-phenylketones |
| 25 | α-Cyperone | 218.33 | 1 | 0 | 3.46 | 0 | 0.55 | 17.07 | Eudesmane, isoeudesmane, or cycloeudesmane sesquiterpenoids |
| 26 | Veratric acid | 182.17 | 4 | 1 | 1.06 | 0 | 0.85 | 55.76 | P-methoxybenzoic acids and derivatives |
| 27 | Triolein | 885.43 | 6 | 0 | 9.49 | 2 | 0.17 | 78.90 | Triacylglycerols |
| 28 | Methylthiouracil | 142.18 | 1 | 2 | −0.35 | 0 | 0.55 | 80.74 | Pyrimidones |
| 29 | Falcarindiol | 260.37 | 2 | 2 | 3.33 | 0 | 0.55 | 40.46 | Long-chain fatty alcohols |
| 30 | Diethyl phosphate | 154.10 | 4 | 1 | −0.43 | 0 | 0.85 | 65.57 | Dialkyl phosphates |
| 31 | Sodium thiocyanate | 81.07 | 1 | 0 | −1.01 | 0 | 0.55 | 23.79 | Metal thiocyanates |
| Grid Box | Hydrogen Bond Interactions | Hydrophobic Interactions | |||||
|---|---|---|---|---|---|---|---|
| Protein | Ligand | PubChem ID | Binding Energy (kcal/mol) | Center | Dimension | Amino Acid Residue | Amino Acid Residue |
| IL6 (PDB ID: 4NI9) | Forsythoside B | 23928102 | −11.4 | x = 11.213 | size_x = 40 | Asp34,Tyr31,Glu110 | Gly35,Gln111,Ala114 |
| y = 33.474 | size_y = 40 | ||||||
| z = 11.162 | size_z = 40 | ||||||
| Pectolinarin | 168849 | −10.4 | x = 11.213 | size_z = 41 | Asp34,Gln111 | Ala38 | |
| y = 33.474 | size_z = 42 | ||||||
| z = 11.162 | size_z = 43 | ||||||
| (*) MD2-TLR4-IN-1 | 138454798 | −9.9 | x = 11.213 | size_z = 44 | N/A | Glu110,Ala114 | |
| y = 33.474 | size_z = 45 | ||||||
| z = 11.162 | size_z = 46 | ||||||
| (*) Aprepitant | 135413536 | −9.6 | x = 11.213 | size_z = 47 | N/A | Tyr31,Asp34,Gly35 | |
| y = 33.474 | size_z = 48 | Gln111 | |||||
| z = 11.162 | size_z = 49 | ||||||
| Mulberroside A | 6443484 | −9.5 | x = 11.213 | size_z = 50 | Glu110,Ser37,Asp34 | Ala114,Gln111 | |
| y = 33.474 | size_z = 51 | Tyr31 | |||||
| z = 11.162 | size_z = 52 | ||||||
| Homoplantaginin | 5318083 | −9.5 | x = 11.213 | size_z = 53 | Asp34,Gln111 | Ala38 | |
| y = 33.474 | size_z = 54 | ||||||
| z = 11.162 | size_z = 55 | ||||||
| (*) NE 52-QQ57 | 68379135 | −9.4 | x = 11.213 | size_z = 56 | Ser37 | Asp34,Tyr31,Ala114 | |
| y = 33.474 | size_z = 57 | Gln111 | |||||
| z = 11.162 | size_z = 58 | ||||||
| (*) Madecassic acid | 73412 | −9.4 | x = 11.213 | size_z = 59 | Glu110 | Ala114,Tyr31 | |
| y = 33.474 | size_z = 60 | ||||||
| z = 11.162 | size_z = 61 | ||||||
| (*) GSK583 | 67469084 | −9.0 | x = 11.213 | size_z = 62 | N/A | Gln111,Ala38 | |
| y = 33.474 | size_z = 63 | ||||||
| z = 11.162 | size_z = 64 | ||||||
| (*) IQ 3 | 777728 | −9.0 | x = 11.213 | size_z = 65 | N/A | Tyr31,Glu110 | |
| y = 33.474 | size_z = 66 | ||||||
| z = 11.162 | size_z = 67 | ||||||
| (*) Methylprednisolone | 6741 | −9.0 | x = 11.213 | size_z = 68 | N/A | Tyr31,Glu110 | |
| y = 33.474 | size_z = 69 | ||||||
| z = 11.162 | size_z = 70 | ||||||
| (*) Hydrocortisone hemisuccinate | 16623 | −8.9 | x = 11.213 | size_z = 71 | N/A | Glu110,Ala114,Gln111 | |
| y = 33.474 | size_z = 72 | ||||||
| z = 11.162 | size_z = 73 | ||||||
| 20(S)-Ginsenoside Rh1 | 12855920 | −8.8 | x = 11.213 | size_z = 74 | Gln111 | Asp34,Tyr31 | |
| y = 33.474 | size_z = 75 | ||||||
| z = 11.162 | size_z = 76 | ||||||
| Stylopine | 6770 | −8.8 | x = 11.213 | size_z = 77 | N/A | Gln111,Ala114,Glu110 | |
| y = 33.474 | size_z = 78 | ||||||
| z = 11.162 | size_z = 79 | ||||||
| (*) Methylprednisolone Acetate | 5877 | −8.6 | x = 11.213 | size_z = 80 | N/A | Gln111,Tyr31,Ala114 | |
| y = 33.474 | size_z = 81 | Glu110 | |||||
| z = 11.162 | size_z = 82 | ||||||
| Gardenoside | 24721095 | −7.8 | x = 11.213 | size_z = 83 | Tyr31,Asp34,Gln111 | N/A | |
| y = 33.474 | size_z = 84 | ||||||
| z = 11.162 | size_z = 85 | ||||||
| (*) 4-Methylesculetin | 5319502 | −7.6 | x = 11.213 | size_z = 86 | Arg24,Arg16 | Pro18 | |
| y = 33.474 | size_z = 87 | ||||||
| z = 11.162 | size_z = 88 | ||||||
| (*) Auraptene | 1550607 | −7.6 | x = 11.213 | size_z = 89 | N/A | Asp34,Glu110,Ala114 | |
| y = 33.474 | size_z = 90 | Tyr31 | |||||
| z = 11.162 | size_z = 91 | ||||||
| (*) AX-024 HCl | 129909862 | −7.5 | x = 11.213 | size_z = 92 | N/A | Gln111,Tyr31,Ala114 | |
| y = 33.474 | size_z = 93 | ||||||
| z = 11.162 | size_z = 94 | ||||||
| (*) APX-115 free base | 51036475 | −7.2 | x = 11.213 | size_z = 95 | Tyr31 | Glu110,Gln111,Asp34 | |
| y = 33.474 | size_z = 96 | ||||||
| z = 11.162 | size_z = 97 | ||||||
| (*) Resatorvid | 11703255 | −7.1 | x = 11.213 | size_z = 98 | Tyr31,Gln111 | Glu110,Asp34 | |
| y = 33.474 | size_z = 99 | ||||||
| z = 11.162 | size_z = 100 | ||||||
| (*) Myrislignan | 21636106 | −7.1 | x = 11.213 | size_z = 101 | Gln111 | Tyr31,Gly35,Asp34 | |
| y = 33.474 | size_z = 102 | ||||||
| z = 11.162 | size_z = 103 | ||||||
| (*) Muscone | 10947 | −6.7 | x = 11.213 | size_z = 104 | N/A | N/A | |
| y = 33.474 | size_z = 105 | ||||||
| z = 11.162 | size_z = 106 | ||||||
| (*) 2′,5′-Dihydroxyacetophenone | 10279 | −6.5 | x = 11.213 | size_z = 107 | N/A | Gln17,Pro18 | |
| y = 33.474 | size_z = 108 | ||||||
| z = 11.162 | size_z = 109 | ||||||
| (*) α-Cyperone | 6452086 | −6.3 | x = 11.213 | size_z = 110 | N/A | Gln111,Glu110 | |
| y = 33.474 | size_z = 111 | ||||||
| z = 11.162 | size_z = 112 | ||||||
| (*) Veratric acid | 7121 | −6.1 | x = 11.213 | size_z = 113 | Arg16 | Gln17,Pro18 | |
| y = 33.474 | size_z = 114 | ||||||
| z = 11.162 | size_z = 115 | ||||||
| Triolein | 5497163 | −5.5 | x = 11.213 | size_z = 116 | N/A | N/A | |
| y = 33.474 | size_z = 117 | ||||||
| z = 11.162 | size_z = 118 | ||||||
| Methylthiouracil | 667493 | −5.4 | x = 11.213 | size_z = 119 | N/A | Arg24 | |
| y = 33.474 | size_z = 120 | ||||||
| z = 11.162 | size_z = 121 | ||||||
| Falcarindiol | 5281148 | −5.2 | x = 11.213 | size_z = 122 | Glu110 | Ala114,Tyr31,Gln111 | |
| y = 33.474 | size_z = 123 | Glu110 | |||||
| z = 11.162 | size_z = 124 | ||||||
| Diethyl phosphate | 654 | −4.9 | x = 11.213 | size_z = 125 | N/A | Arg16,Gln17 | |
| y = 33.474 | size_z = 126 | ||||||
| z = 11.162 | size_z = 127 | ||||||
| Sodium thiocyanate | 516871 | −2.6 | x = 11.213 | size_z = 128 | N/A | Arg16,Gln17 | |
| y = 33.474 | size_z = 129 | ||||||
| z = 11.162 | size_z = 130 | ||||||
| Parameters | Compound |
|---|---|
| MD2-TLR4-IN-1 | |
| Ames toxicity | NAT |
| Carcinogens | NC |
| Acute oral toxicity | Ⅲ |
| Rat acute toxicity | 2.2347 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oh, K.-K.; Adnan, M.; Cho, D.-H. Drug Investigation to Dampen the Comorbidity of Rheumatoid Arthritis and Osteoporosis via Molecular Docking Test. Curr. Issues Mol. Biol. 2022, 44, 1046-1061. https://doi.org/10.3390/cimb44030069
Oh K-K, Adnan M, Cho D-H. Drug Investigation to Dampen the Comorbidity of Rheumatoid Arthritis and Osteoporosis via Molecular Docking Test. Current Issues in Molecular Biology. 2022; 44(3):1046-1061. https://doi.org/10.3390/cimb44030069
Chicago/Turabian StyleOh, Ki-Kwang, Md. Adnan, and Dong-Ha Cho. 2022. "Drug Investigation to Dampen the Comorbidity of Rheumatoid Arthritis and Osteoporosis via Molecular Docking Test" Current Issues in Molecular Biology 44, no. 3: 1046-1061. https://doi.org/10.3390/cimb44030069