
Development of Post-Stroke Cognitive and Depressive Disturbances: Associations with Neurohumoral Indices
 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
- -
- For 45 patients (33 men/12 women) in the acute period after stroke;
- -
- For 41 patients (32 men/9 women) in the acute period and 30 days after stroke;
- -
- For 33 patients (27 men/6 women) in the acute period, 30 days, and 180 days after stroke;
- -
- For 29 patients (24 men/5 women) in the acute period, 30 days, 180 days, and 365 days after stroke;
- -
- For control group participants (HC).
2.2. Clinical Examination
2.3. Laboratory Examination
2.3.1. Serum and Blood Plasma
2.3.2. Saliva
2.3.3. Hair Cortisol
2.4. Statistical Analysis
3. Results
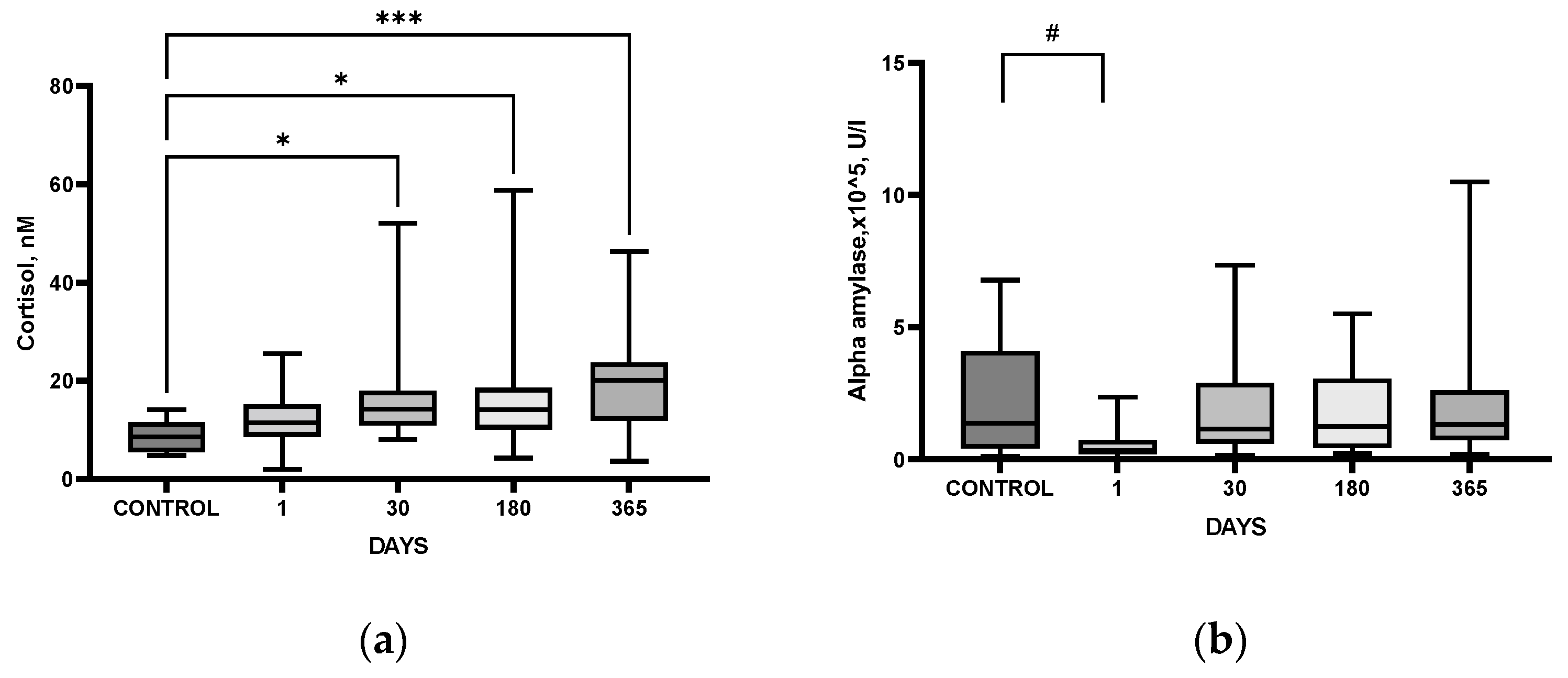
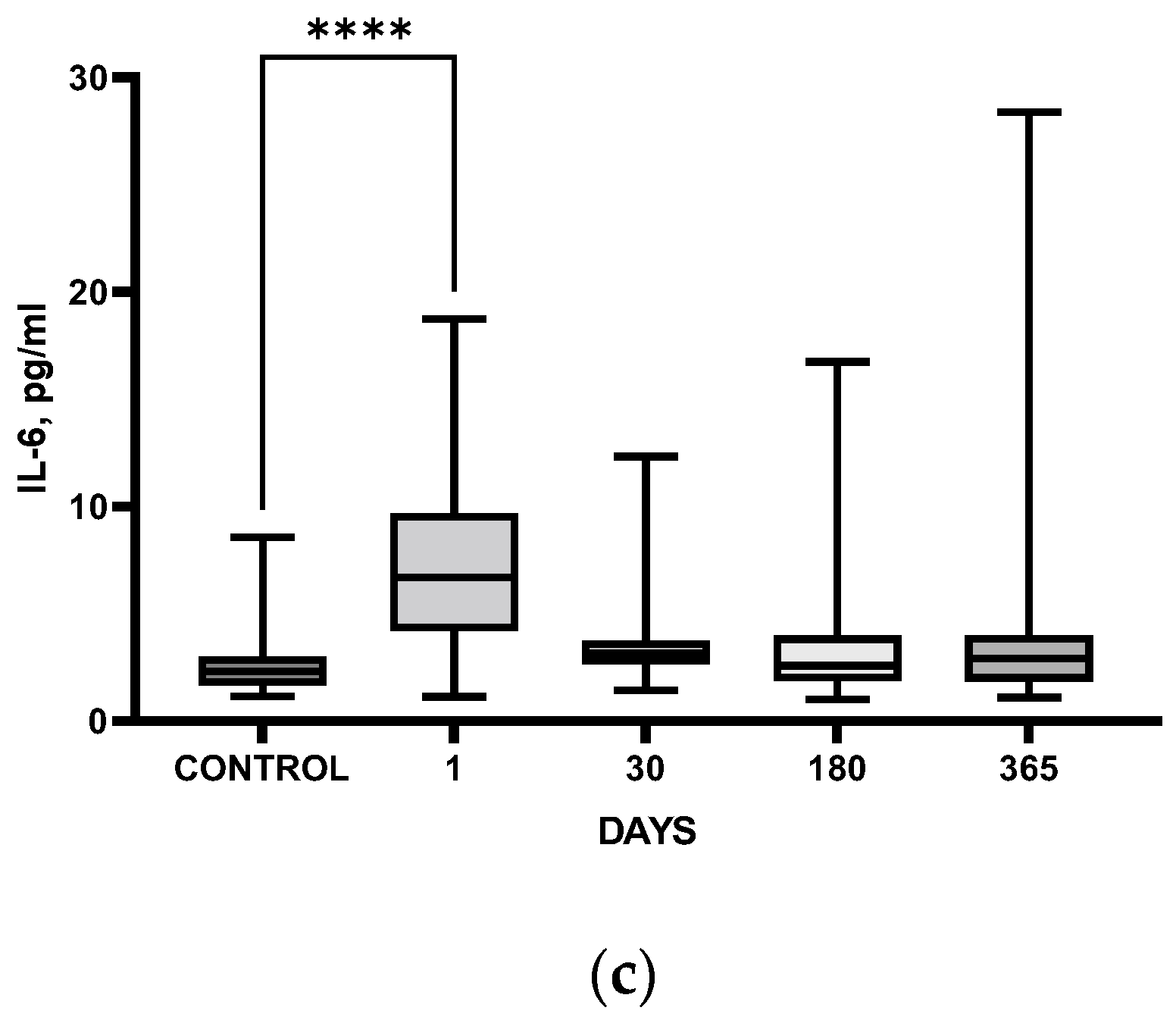
3.1. Time Course of Laboratory Markers after IS: Comparison with HC
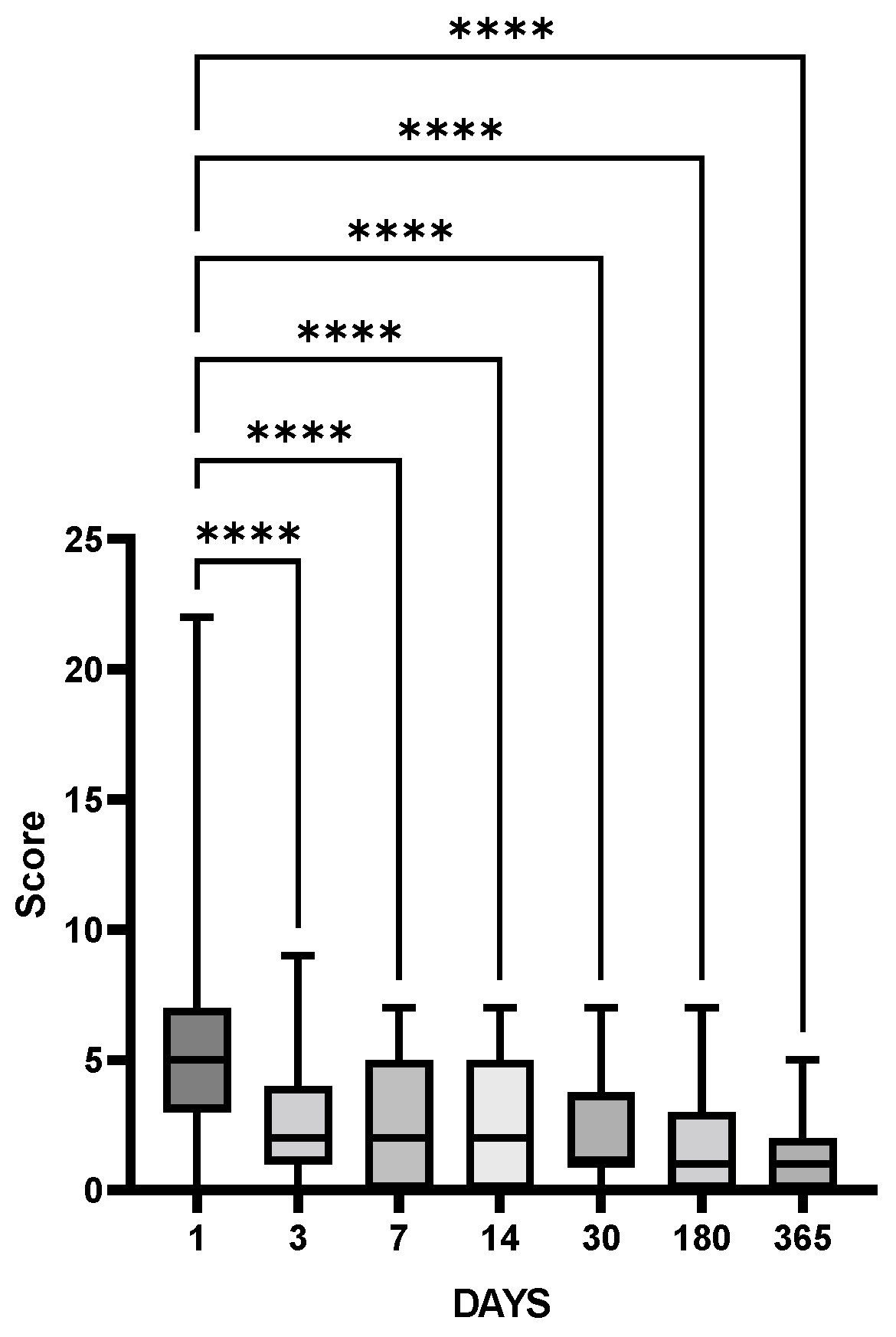
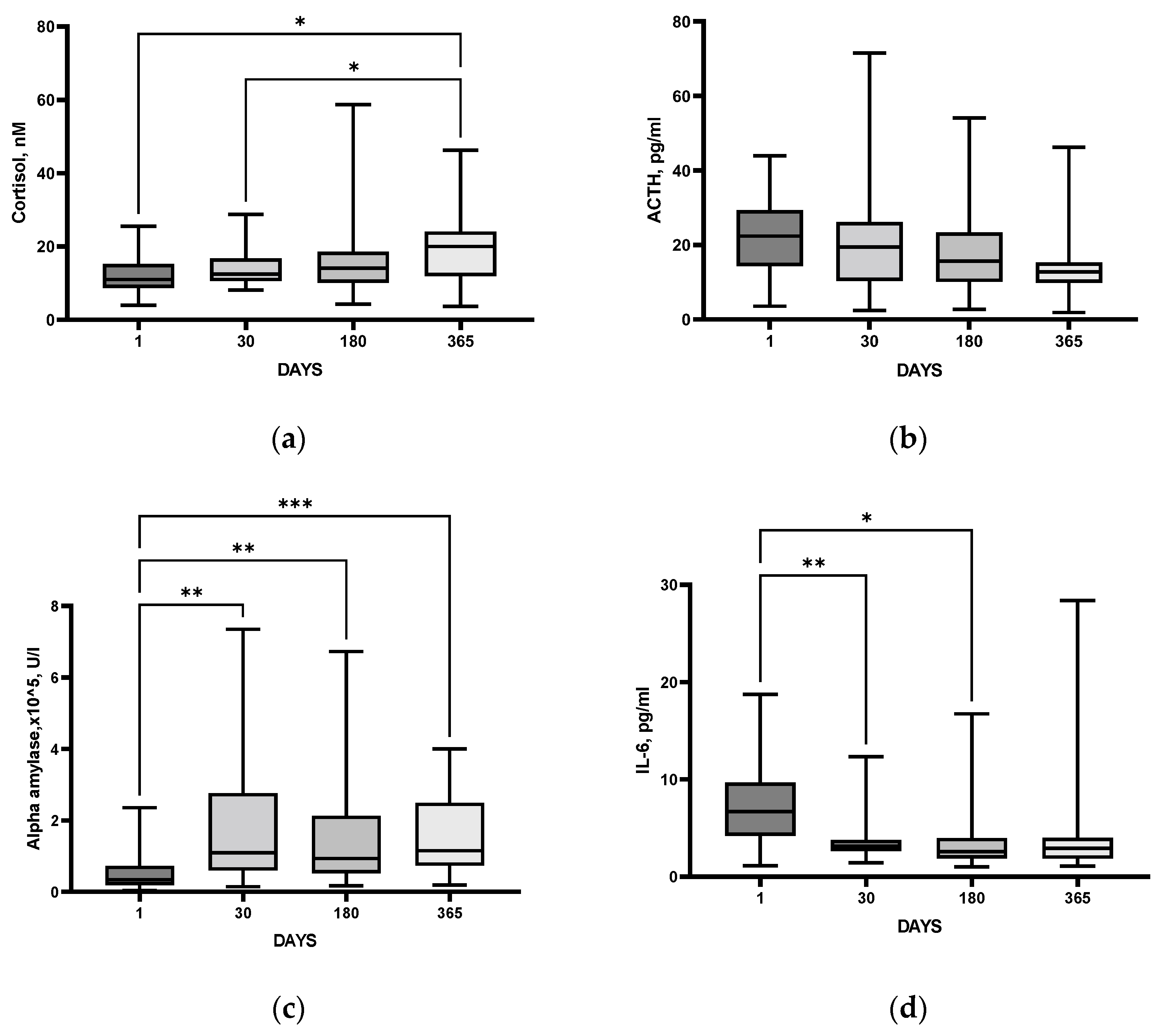
3.2. Time Course of Clinical Indices and Laboratory Markers after IS
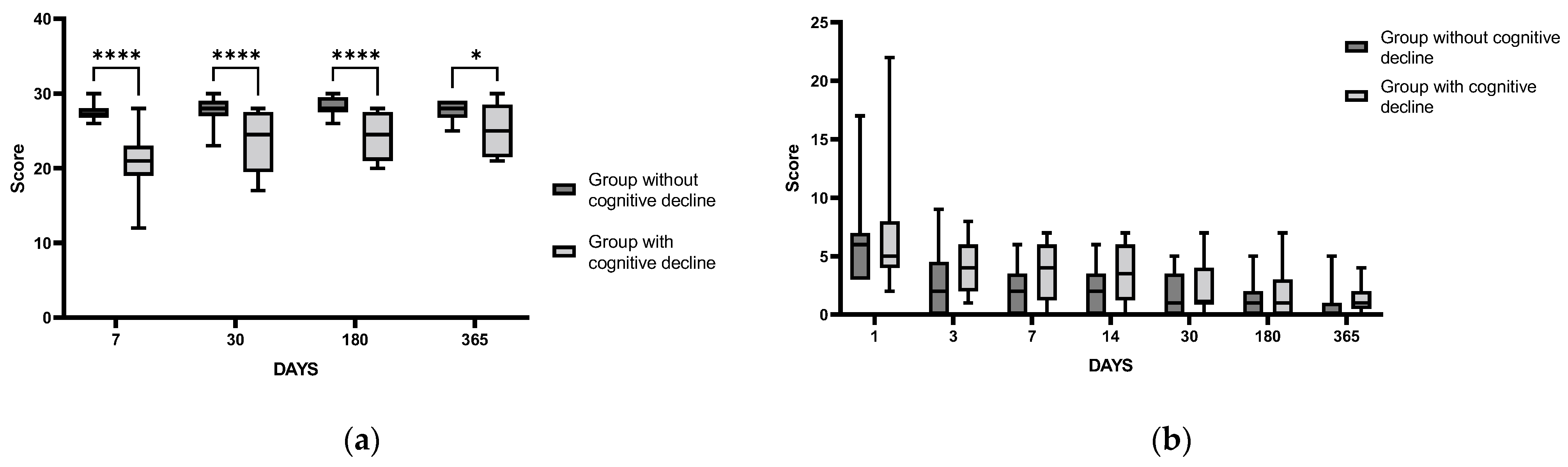
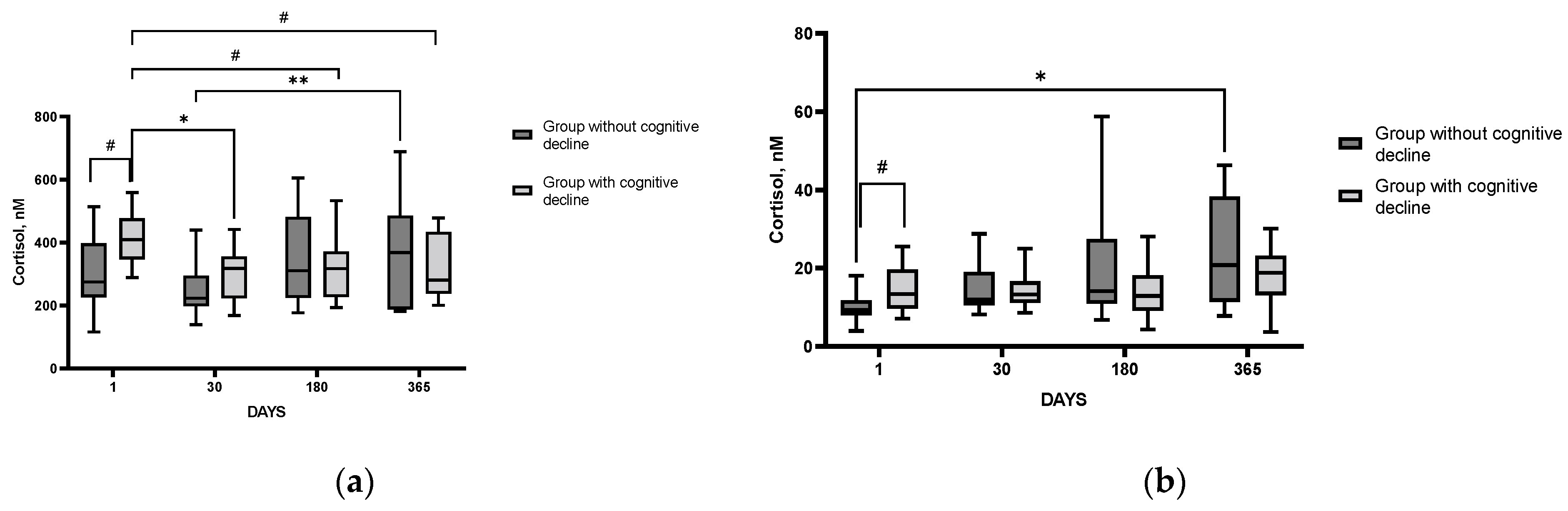
3.3. Time Course of Clinical Indices and Laboratory Markers after IS in Patients with and without Cognitive Impairment (PSCI)
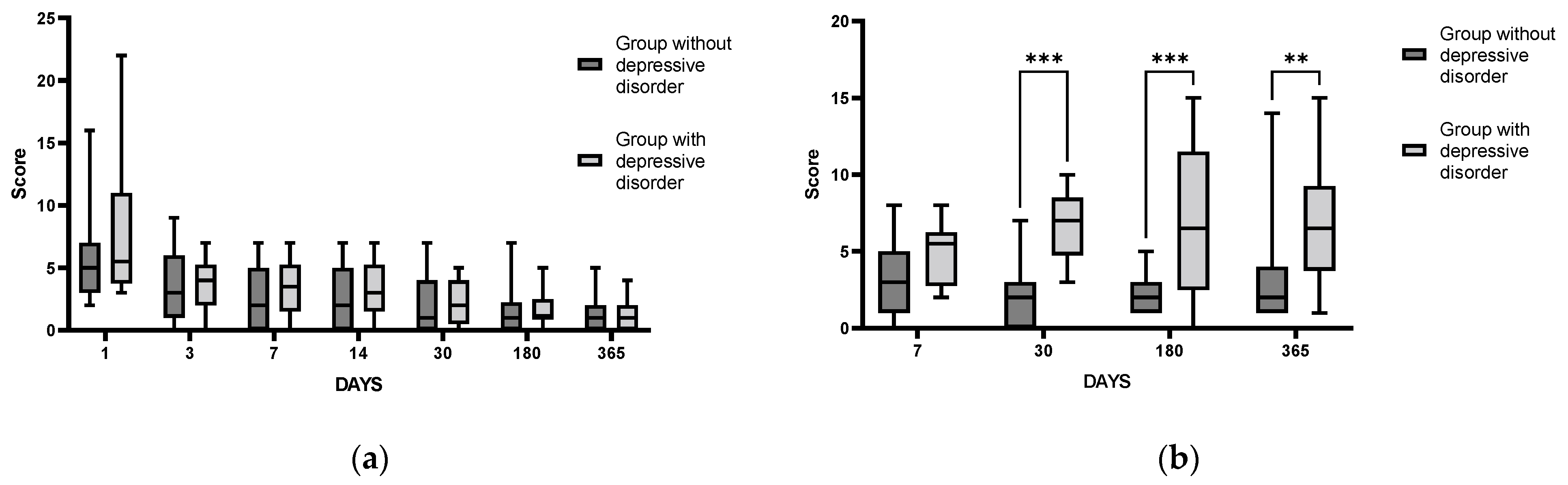
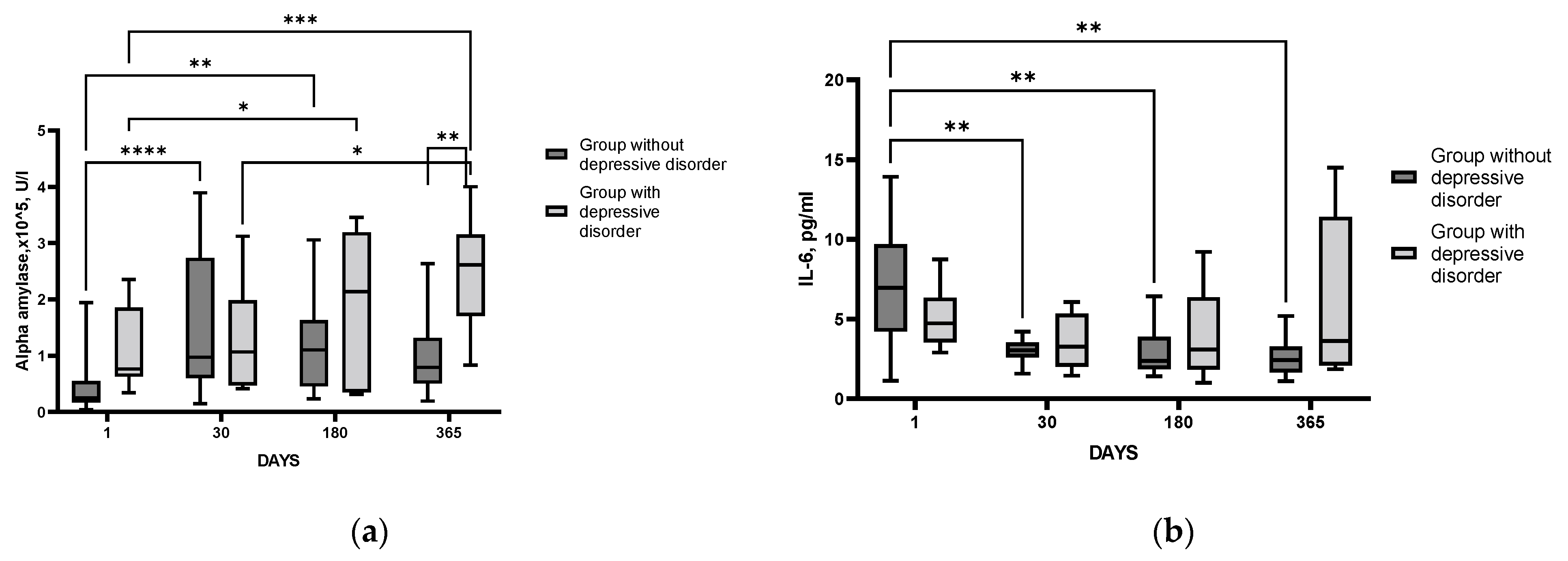
3.4. Time Course of Changes in Clinical and Laboratory Parameters after IS in Patients with and without Depressive Disorder
4. Discussion
4.1. Delayed Post-Stroke Cognitive and Emotional Disturbances
4.2. Involvement of HPA Axis in IS consequences
4.3. Involvement of SAMS in IS Consequences
4.4. Involvement of Inflammatory Response in IS Consequences
5. Conclusions
6. Limitations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: A systematic analysis for the Global Burden if Disease Study 2019. Lancet Neurol. 2021, 20, 79–82. [Google Scholar] [CrossRef]
- Droś, J.; Klimkowicz-Mrowiec, A. Current view on post-stroke dementia. Psychogeriatrics 2021, 21, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Medeiros, G.C.; Roy, D.; Kontos, N.; Beach, S.R. Post-stroke depression: A 2020 updated review. Gen. Hosp. Psychiatry 2020, 66, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Gorelick, P.B.; Nyenhuis, D. Stroke and Cognitive Decline. JAMA 2015, 314, 29–30. [Google Scholar] [CrossRef]
- Lees, R.; Stott, D.J. Feasibility and diagnostic accuracy of early mood screening to diagnose persisting clinical depression/anxiety disorder after stroke. Cerebrovasc. Dis. 2014, 37, 323–329. [Google Scholar] [CrossRef]
- Yu, K.H.; Cho, S.J. Cognitive impairment evaluated with Vascular Cognitive Impairment Harmonization Standards in a multicenter prospective stroke cohort in Korea. Stroke 2013, 44, 786–788. [Google Scholar] [CrossRef]
- Kapoor, A.; Lanctot, K. Screening for Post-Stroke Depression andCognitive Impairment at Baseline Predicts Long-Term Patient-Centered Outcomes After Stroke. J. Geriatr. Psychiatry Neurol. 2019, 32, 40–48. [Google Scholar] [CrossRef]
- Ayerbe, L.; Ayis, S. Natural history, predictors and outcomes of depression after stroke: Systematic review and meta-analysis. Br. J. Psychiatry 2013, 202, 14–21. [Google Scholar] [CrossRef] [Green Version]
- Hackett, M.L.; Pickles, K. Part I: Frequency of depression after stroke: An updated systematic review and meta-analysis of observational studies. Int. J. Stroke 2014, 9, 1017–1025. [Google Scholar] [CrossRef]
- Tene, O.; Shenhar-Tsarfaty, S. Depressive symptoms following stroke and transient ischemic attack: Is it time for a more intensive treatment approach? Results from the TABASCO cohort study. J. Clin. Psychiatry 2016, 77, 673–680. [Google Scholar] [CrossRef]
- Gulyaeva, N.V. Biochemical Mechanisms and Translational Relevance of Hippocampal Vulnerability to Distant Focal Brain Injury: The Price of Stress Response. Biochemistry 2019, 86, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Bolshakov, A.P.; Tret’yakova, L.V. Glucocorticoids: Dr. Jekyll and Mr. Hyde of Hippocampal Neuroinflammation. Biochemistry 2021, 86, 156–167. [Google Scholar] [CrossRef] [PubMed]
- Gulyaeva, N.V. Functional Neurochemistry of the Ventral and Dorsal Hippocampus: Stress, Depression, Dementia and Remote Hippocampal Damage. Neurochem. Res. 2019, 44, 1306–1322. [Google Scholar] [CrossRef] [PubMed]
- Nater, U.M.; La Marca, R. Stress-induced changes in human salivary alpha-amylase activity—Associations with adrenergic activity. Psychoneuroendocrinology 2006, 31, 49–58. [Google Scholar] [CrossRef]
- Lyden, P. Using the National Institutes of Health Stroke Scale: A Cautionary Tale. Stroke 2017, 48, 513–519. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Beck, A.T.; Ward, C.H. An inventory for measuring depression. Arch. Gen. Psychiatry 1961, 4, 561–571. [Google Scholar] [CrossRef] [Green Version]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [Green Version]
- Chan, S.F.; La Greca, A.M. Percieved Stress Scale (PSS). In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, USA, 2013; pp. 1454–1455. [Google Scholar] [CrossRef]
- Holmes, T.H.; Rahe, R.H. The Social Readjustment Rating Scale. J. Psychosom. Res. 1967, 11, 213–218. [Google Scholar] [CrossRef]
- Patel, N.; Rao, V.A. Simple and reliable determination of the modified rankin scale score in neurosurgical and neurological patients: The mRS-9Q. Neurosurgery 2012, 71, 971–975. [Google Scholar] [CrossRef] [PubMed]
- Quinn, T.J.; Langhorne, P. Barthel index for stroke trials: Development, properties, and application. Stroke 2011, 42, 1146–1151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stroop, J.R. Studies of interference in serial verbal reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- Thomas, S.A.; Russell, L.A. Luria memory words test and Wechsler memory scale: Comparison of utility in discriminating neurologically impaired from controls. J. Clin. Psychol. 1990, 46, 190–193. [Google Scholar] [CrossRef]
- Lauren, R.D.; Mahone, E.M. Assosiations of postural knowledge and basic motor skill with dyspraxia in autism: Implicatin for abnormalities in distributed connectivity and motor learning. Neuropsychology 2009, 23, 563–570. [Google Scholar] [CrossRef] [Green Version]
- Shin, M.-S.; Park, S.-Y. Clinical and empirical applications of the Rey-Osterrieth Complex Figure Test. Nat. Protoc. 2006, 1, 892–899. [Google Scholar] [CrossRef] [PubMed]
- Stephen, M.R.; Deborah, L.H. Distributed Neural Systems Underlying the Timing of Movements. J. Neurosci. 1997, 17, 5528–5535. [Google Scholar] [CrossRef] [Green Version]
- Pochigaeva, K.; Druzhkova, T.; Yakovlev, A.; Onufriev, M.; Grishkina, M.; Chepelev, A.; Guekht, A.; Gulyaeva, N. Hair cortisol as a marker of hypothalamic-pituitary-adrenal Axis activity in female patients with major depressive disorder. Metab. Brain Dis. 2017, 32, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Melkas, S.; Jokinen, H.; Hietanen, M.; Erkinjuntti, T. Poststroke cognitive impairment and dementia: Prevalence, diagnosis, and treatment. Degener. Neurol. Neuromuscul. Dis. 2014, 4, 21–27. [Google Scholar] [CrossRef]
- Robinson, R.G.; Jorgeбю, R.E. Post-Stroke Depression: A Review. Am. J. Psychiatry. 2016, 173, 221–231. [Google Scholar] [CrossRef] [Green Version]
- Khedr, E.M.; Abdelrahman, A.A.; Desoky, T.; Zaki, A.F.; Gamea, A. Post-stroke depression: Frequency, risk factors, and impact on quality of life among 103 stroke patients—Hospital-based study. Egypt. J. Neurol. Psychiatry Neurosurg. 2020, 56, 66. [Google Scholar] [CrossRef]
- Guo, J.; Wang, J.; Sun, W.; Liu, X. The advances of post-stroke depression: 2021 update. J. Neurol. 2022, 269, 1236–1249. [Google Scholar] [CrossRef] [PubMed]
- Gulyaeva, N.V.; Onufriev, M.V.; Moiseeva, Y.V. Ischemic Stroke, Glucocorticoids, and Remote Hippocampal Damage: A Translational Outlook and Implications for Modeling. Front. Neurosci. 2021, 15, 781964. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Iqbaal, H. Serum-cortisol levels in severity of stroke. Internat. J. Med. Biomed. Stud. 2020, 4, 2. [Google Scholar] [CrossRef] [Green Version]
- Jnanendrappa, K.H. A Study on Correlation between Serum Cortisol and Stroke Severity with Serum Cortisol. Acad. J. Med. 2020, 2, 179–181. [Google Scholar] [CrossRef]
- Barugh, A.J.; Gray, P.; Shenkin, S.D.; MacLullich, A.M.; Mead, G.E. Cortisol levels and the severity and outcomes of acute stroke: A systematic review. J. Neurol. 2014, 261, 533–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iranmanesh, F.; Sedighi, B.; Ziaadini, B. Prognostic Value of Cortisol in Patients with Acute Ischemic Stroke. Zahedan J. Res. Med. Sci. 2017, 19, e6187. [Google Scholar] [CrossRef] [Green Version]
- Gyawali, P.; Chow, W.Z.; Hinwood, M.; Kluge, M.; English, C.; Ong, L.K.; Nilsson, M.; Walker, F.R. Opposing Associations of Stress and Resilience With Functional Outcomes in Stroke Survivors in the Chronic Phase of Stroke: A Cross-Sectional Study. Front. Neurol. 2020, 11, 230. [Google Scholar] [CrossRef] [Green Version]
- Marklund, N.; Peltonen, M.; Nilsson, T.K.; Olsson, T. Low and high circulating cortisol levels predict mortality and cognitive dysfunction early after stroke. J. Intern. Med. 2004, 256, 15–21. [Google Scholar] [CrossRef]
- Qiu, Q.; Zhou, X.; Wu, L.; Zhang, Y.; Yu, Z.; Wang, M.; Huang, H.; Luo, X.; Pan, D. Serum Cortisol Is Associated With Cerebral Small Vessel Disease-Related Brain Changes and Cognitive Impairment. Front. Aging Neurosci. 2022, 13, 809684. [Google Scholar] [CrossRef]
- Wang, J.; Guan, Q.; Sheng, Y.; Yang, Y.; Guo, L.; Li, W.; Gu, Y.; Han, C. The potential predictive value of salivary cortisol on the occurrence of secondary cognitive impairment after ischemic stroke. Neurosurg. Rev. 2021, 44, 1103–1108. [Google Scholar] [CrossRef] [PubMed]
- Ben Assayag, E.; Tene, O. High hair cortisol concentrations predict worse cognitive outcome after stroke: Results from the TABASCO prospective cohort study. Psychoneuroendocrinology 2017, 82, 133–139. [Google Scholar] [CrossRef] [PubMed]
- Tene, O.; Hallevi, H. The Price of Stress: High Bedtime Salivary Cortisol Levels Are Associated with Brain Atrophy and Cognitive Decline in Stroke Survivors. Results from the TABASCO Prospective Cohort Study. J. Alzheimers Dis. 2018, 65, 1365–1375. [Google Scholar] [CrossRef]
- Lupien, S.J.; Maheu, F. The effects of stress and stress hormones on human cognition: Implications for the field of brain and cognition. Brain Cogn. 2007, 65, 209–237. [Google Scholar] [CrossRef] [Green Version]
- Ennis, G.E.; An, Y. Long-term cortisol measures predict Alzheimer disease risk. Neurology 2017, 88, 371–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, C.W.; Lui, C.C. Elevated basal cortisol level predicts lower hippocampal volume and cognitive decline in Alzheimer’s disease. J. Clin. Neurosci. 2009, 16, 1283–1286. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.F.; Zou, W.; Yang, Y. Effects of IL-6 and cortisol fluctuations in post-stroke depression. J. Huazhong Univ. Sci. Technolog. Med. Sci. 2016, 36, 732–735. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Feng, T. Expression of serum cortisol levels in post-stroke depression patients before and after treatment and its correlation with depression. J. Clin. Med. Pract. 2019, 23, 34–36. [Google Scholar] [CrossRef]
- Kwon, O.J.; Kim, M.; Lee, H.S.; Sung, K.K.; Lee, S. The Cortisol Awakening Response in Patients with Poststroke Depression Is Blunted and Negatively Correlated with Depressive Mood. Biomed. Res. Int. 2015, 2015, 709230. [Google Scholar] [CrossRef]
- Terroni, L.; Amaro, E., Jr.; Iosifescu, D.; Mattos, P.; Yamamoto, F.; Tinone, G.; Conforto, A.; Sobreiro, M.; Guajardo, V.; De Lucia, M.; et al. The association of post-stroke anhedonia with salivary cortisol levels and stroke lesion in hippocampal/parahippocampal region. Neuropsychiatr. Dis. Treat. 2015, 11, 233–242. [Google Scholar] [CrossRef] [Green Version]
- Het, S.; Wolf, O.T. Mood changes in response to psychosocial stress in healthy young women: Effects of pretreatment with cortisol. Behav. Neurosci. 2007, 121, 11–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nater, U.M.; Rohleder, N. Salivary alpha-amylase as a non-invasive biomarker for the sympathetic nervous system: Current state of research. Psychoneuroendocrinology 2009, 34, 486–496. [Google Scholar] [CrossRef] [PubMed]
- Özdemir, A.; Sağkan, R.; Karahan, A.; Ordahan, B. Evaluation of salivary alpha-amylase activity after stroke. Med. Sci. 2019, 8, 852. [Google Scholar] [CrossRef]
- Bassi, A.; Bozzali, M. Potential Interactions between the Autonomic Nervous System and Higher Level Functions in Neurological and Neuropsychiatric Conditions. Front. Neurol. 2015, 6, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robinson, R.G.; Spalletta, G.; Jorge, R.E.; Bassi, A.; Colivicchi, F.; Ripa, A.; Caltagirone, C. Decreased heart rate variability is associated with poststroke depression. Am. J. Geriatr. Psychiatry 2008, 16, 867–873. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauduin, S.E.E.C.; van Noorden, M.S.; van der Werff, S.J.A.; de Leeuw, M.; van Hemert, A.M.; van der Wee, N.J.A.; Giltay, E.J. Elevated salivary alpha-amylase levels at awakening in patients with depression. Psychoneuroendocrinology 2018, 97, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Labudda, K.; Wolf, O. Decision-making and neuroendocrine responses in pathological gamblers. Psychiatry Res. 2007, 153, 233–243. [Google Scholar] [CrossRef]
- Moret, C.; Briley, M. The importance of norepinephrine in depression. Neuropsychiatr. Dis. Treat. 2011, 7 (Suppl. 1), 9–13. [Google Scholar] [CrossRef]
- Valdizan, E.M.; Diez-Alarcia, R. α₂-Adrenoceptor functionality in postmortem frontal cortex of depressed suicide victims. Biol. Psychiatry 2010, 68, 869–872. [Google Scholar] [CrossRef] [PubMed]
- Klimek, V.; Stockmaier, C. Reduced Levels of Norepinphrine Transporters in the Locus Coeruleus in Major Depression. J. Neurosci. 1997, 17, 8451–8458. [Google Scholar] [CrossRef] [Green Version]
- Pawluk, H.; Woźniak, A.; Grześk, G.; Kołodziejska, R.; Kozakiewicz, M.; Kopkowska, E.; Grzechowiak, E.; Kozera, G. The Role of Selected Pro-Inflammatory Cytokines in Pathogenesis of Ischemic Stroke. Clin. Interv. Aging 2020, 15, 469–484. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, H.; Hu, S.; Li, Y.; Sun, Y.; Xiong, X.; Hu, X.; Chen, J.; Qiu, S. Interleukins and Ischemic Stroke. Front. Immunol. 2022, 13, 828447. [Google Scholar] [CrossRef] [PubMed]
- Zeng, L.; Wang, Y.; Liu, J.; Wang, L.; Weng, S.; Chen, K.; Domino, E.F.; Yang, G.Y. Pro-inflammatory cytokine network in peripheral inflammation response to cerebral ischemia. Neurosci. Lett. 2013, 548, 4–9. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, J.; Pan, Y.; Wang, M.; Lin, J.; Meng, X.; Liao, X.; Wang, Y. Interleukin-6 as Predictor of One-Year Cognitive Function After Ischemic Stroke or TIA. Neuropsychiatr. Dis. Treat. 2022, 18, 391–399. [Google Scholar] [CrossRef]
- Zhang, J.C.; Yao, W.; Dong, C.; Yang, C.; Ren, Q.; Ma, M.; Hashimoto, K. Blockade of interleukin-6 receptor in the periphery promotes rapid and sustained antidepressant actions: A possible role of gut-microbiota-brain axis. Transl. Psychiatry 2017, 7, e1138. [Google Scholar] [CrossRef] [Green Version]
- Korostynski, M.; Hoinkis, D.; Piechota, M.; Golda, S.; Pera, J.; Slowik, A.; Dziedzic, T. Toll-like receptor 4-mediated cytokine synthesis and post-stroke depressive symptoms. Transl. Psychiatry 2021, 11, 246. [Google Scholar] [CrossRef]
- Dowlati, Y.; Herrmann, N. A meta-analysis of cytokines in major depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef]
- Nemeroff, C.B.; Vale, W.W. The neurobiology of depression: Inroads to treatment and new drug discovery. J. Clin. Psychiatry 2005, 66 (Suppl. 7), 5–13. [Google Scholar] [PubMed]
- Rudilosso, S.; Rodríguez-Vázquez, A.; Urra, X.; Arboix, A. The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. Int. J. Mol. Sci. 2022, 23, 1497. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhanina, M.Y.; Druzhkova, T.A.; Yakovlev, A.A.; Vladimirova, E.E.; Freiman, S.V.; Eremina, N.N.; Guekht, A.B.; Gulyaeva, N.V. Development of Post-Stroke Cognitive and Depressive Disturbances: Associations with Neurohumoral Indices. Curr. Issues Mol. Biol. 2022, 44, 6290-6305. https://doi.org/10.3390/cimb44120429
Zhanina MY, Druzhkova TA, Yakovlev AA, Vladimirova EE, Freiman SV, Eremina NN, Guekht AB, Gulyaeva NV. Development of Post-Stroke Cognitive and Depressive Disturbances: Associations with Neurohumoral Indices. Current Issues in Molecular Biology. 2022; 44(12):6290-6305. https://doi.org/10.3390/cimb44120429
Chicago/Turabian StyleZhanina, Marina Y., Tatyana A. Druzhkova, Alexander A. Yakovlev, Elena E. Vladimirova, Sofia V. Freiman, Natalia N. Eremina, Alla B. Guekht, and Natalia V. Gulyaeva. 2022. "Development of Post-Stroke Cognitive and Depressive Disturbances: Associations with Neurohumoral Indices" Current Issues in Molecular Biology 44, no. 12: 6290-6305. https://doi.org/10.3390/cimb44120429