
Novel Strategies for Cancer Combat: Drug Combination Using Repurposed Drugs Induces Synergistic Growth Inhibition of MCF-7 Breast and HT-29 Colon Cancer Cells




Abstract
:1. Introduction
2. Materials and Methods
2.1. Reagents
2.2. Cell Culture
2.3. Drug Treatment
2.4. Microscopic Observation
2.5. Viability Assay
2.6. Data Analysis
2.7. Synergism Evaluation
2.8. Statistical Analysis
3. Results
3.1. Combination of Antineoplastic Drugs with Quetiapine and Edaravone for Breast and Colon Cancer Therapy
3.1.1. MCF-7 Results
3.1.2. HT-29 Results
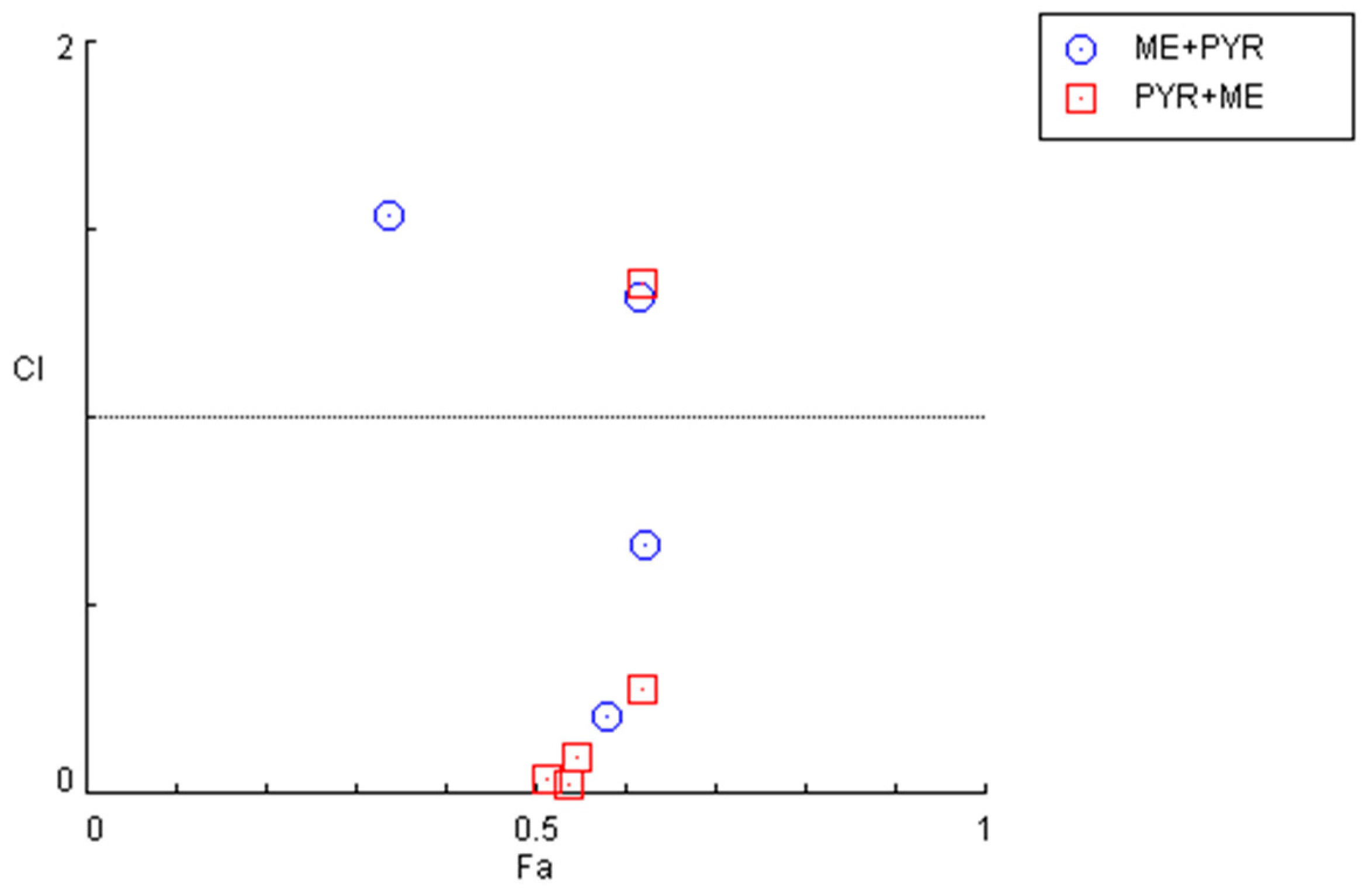
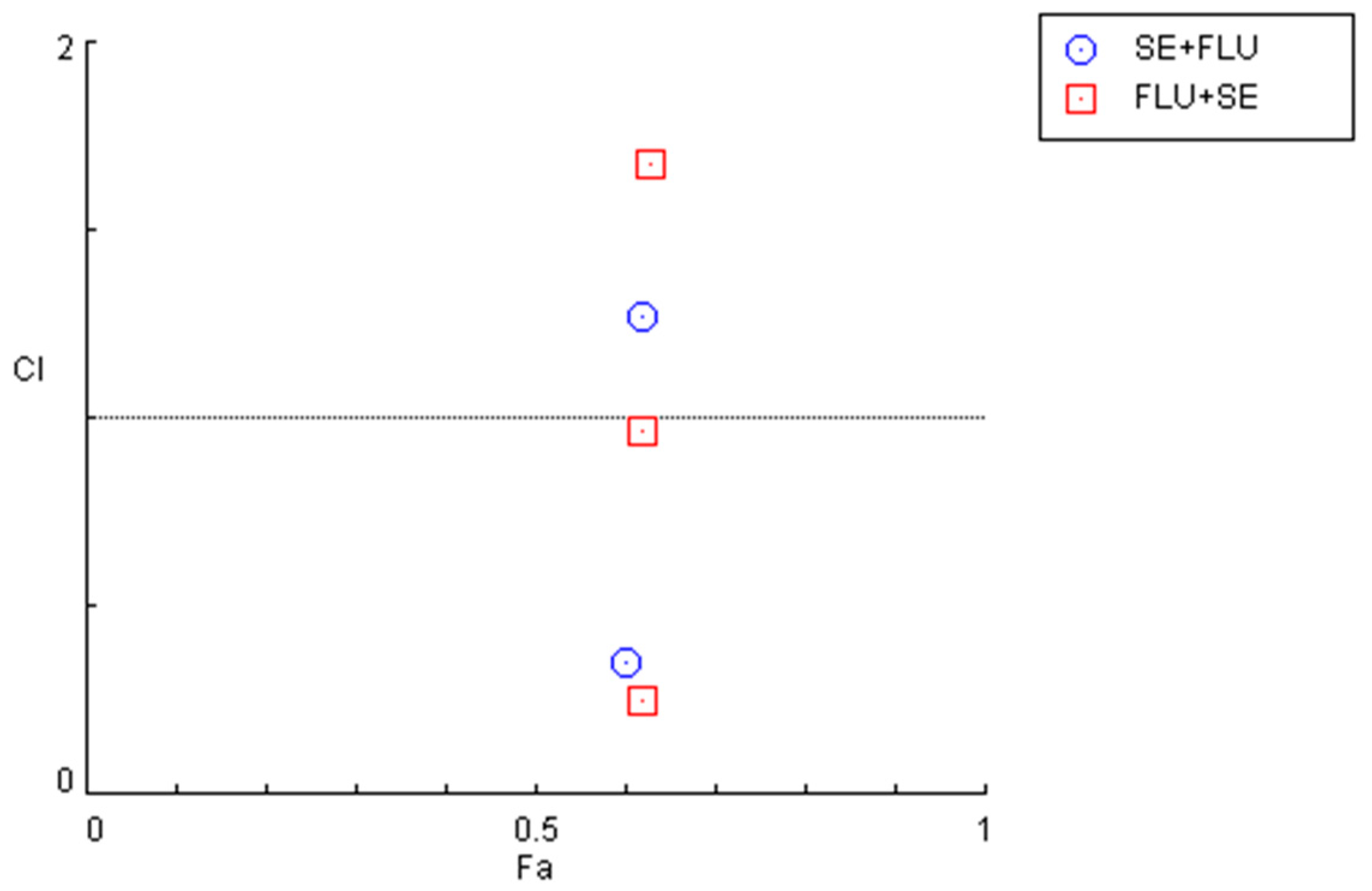
3.2. Combination of Repurposed Drugs for Breast and Colon Cancer Therapy
3.2.1. MCF-7 Results
3.2.2. HT-29 Results
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2022. Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Entezar-Almahdi, E.; Mohammadi-Samani, S.; Tayebi, L.; Farjadian, F. Recent Advances in Designing 5-Fluorouracil Delivery Systems: A Stepping Stone in the Safe Treatment of Colorectal Cancer. Int. J. Nanomed. 2020, 15, 5445–5458. [Google Scholar] [CrossRef]
- Ben-Hamo, R.; Zilberberg, A.; Cohen, H.; Bahar-Shany, K.; Wachtel, C.; Korach, J.; Aviel-Ronen, S.; Barshack, I.; Barash, D.; Levanon, K.; et al. Resistance to Paclitaxel Is Associated with a Variant of the Gene BCL2 in Multiple Tumor Types. NPJ Precis. Oncol. 2019, 3, 12. [Google Scholar] [CrossRef] [Green Version]
- Thorn, C.F.; Oshiro, C.; Marsh, S.; Hernandez-Boussard, T.; McLeod, H.; Klein, T.E.; Altman, R.B. Doxorubicin Pathways. Pharm. Genom. 2011, 21, 440–446. [Google Scholar] [CrossRef]
- Ben-Aharon, I.; Bar-Joseph, H.; Tzarfaty, G.; Kuchinsky, L.; Rizel, S.; Stemmer, S.M.; Shalgi, R. Doxorubicin-Induced Ovarian Toxicity. Reprod. Biol. Endocrinol. 2010, 8, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niringiyumukiza, J.D.; Cai, H.; Chen, L.; Li, Y.; Wang, L.; Zhang, M.; Xu, X.; Xiang, W. Protective Properties of Glycogen Synthase Kinase-3 Inhibition against Doxorubicin-Induced Oxidative Damage to Mouse Ovarian Reserve. Biomed. Pharmacother. 2019, 116, 108963. [Google Scholar] [CrossRef] [PubMed]
- Tossetta, G.; Fantone, S.; Montanari, E.; Marzioni, D.; Goteri, G. Role of NRF2 in Ovarian Cancer. Antioxidants 2022, 11, 663. [Google Scholar] [CrossRef] [PubMed]
- Pantziarka, P.; Sukhtame, V.; Meheus, L.; Sukhatme, V.P.V.V.; Bouche, G.; Meheus, L.; Sukhatme, V.P.V.V.; Bouche, G. Repurposing Non-Cancer Drugs in Oncology—How Many Drugs Are out There? bioRxiv 2017, 1, 197434. [Google Scholar] [CrossRef] [Green Version]
- Antoszczak, M.; Markowska, A.; Markowska, J.; Huczyński, A. Old Wine in New Bottles: Drug Repurposing in Oncology. Eur. J. Pharmacol. 2020, 866, 172784. [Google Scholar] [CrossRef]
- Verbaanderd, C.; Meheus, L.; Huys, I.; Pantziarka, P. Repurposing Drugs in Oncology: Next Steps. Trends Cancer 2017, 3, 543–546. [Google Scholar] [CrossRef]
- Mohammad Jafari, R.; Sheibani, M.; Nezamoleslami, S.; Shayesteh, S.; Jand, Y.; Dehpour, A.R. Drug Repositioning: A Review. J. Iran. Med. Counc. 2018, 1, 7–10. [Google Scholar]
- Ashburn, T.T.; Thor, K.B. Drug Repositioning: Identifying and Developing New Uses for Existing Drugs. Nat. Rev. Drug Discov. 2004, 3, 673–683. [Google Scholar] [CrossRef] [PubMed]
- Sleire, L.; Førde-Tislevoll, H.E.; Netland, I.A.; Leiss, L.; Skeie, B.S.; Enger, P.Ø. Drug Repurposing in Cancer. Pharmacol. Res. 2017, 124, 74–91. [Google Scholar] [CrossRef] [PubMed]
- Hu, Q.; Sun, W.; Wang, C.; Gu, Z. Recent Advances of Cocktail Chemotherapy by Combination Drug Delivery Systems. Adv. Drug Deliv. Rev. 2016, 98, 19–34. [Google Scholar] [CrossRef] [Green Version]
- Wu, Y.; Zhang, D.; Wu, B.; Quan, Y.; Liu, D.; Li, Y.; Zhang, X. Synergistic Activity of an Antimetabolite Drug and Tyrosine Kinase Inhibitors against Breast Cancer Cells. Chem. Pharm. Bull. 2017, 65, 768–775. [Google Scholar] [CrossRef] [Green Version]
- Miskimins, W.K.; Ahn, H.J.; Kim, J.Y.; Ryu, S.; Jung, Y.-S.; Choi, J.Y. Synergistic Anti-Cancer Effect of Phenformin and Oxamate. PLoS ONE 2014, 9, e85576. [Google Scholar] [CrossRef] [Green Version]
- Mei, L.; Chen, Y.; Wang, Z.; Wang, J.; Wan, J.; Yu, C.; Liu, X.; Li, W. Synergistic Anti-Tumour Effects of Tetrandrine and Chloroquine Combination Therapy in Human Cancer: A Potential Antagonistic Role for P21. Br. J. Pharmacol. 2015, 172, 2232–2245. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Xiao, X.; Zhang, C.; Yu, W.; Guo, W.; Zhang, Z.; Li, Z.; Feng, X.; Hao, J.; Zhang, K.; et al. Melatonin Synergizes the Chemotherapeutic Effect of 5-Fluorouracil in Colon Cancer by Suppressing PI3K/AKT and NF-ΚB/INOS Signaling Pathways. J. Pineal Res. 2017, 62, e12380. [Google Scholar] [CrossRef]
- Palmer, A.C.; Chidley, C.; Sorger, P.K. A Curative Combination Cancer Therapy Achieves High Fractional Cell Killing through Low Cross-Resistance and Drug Additivity. Elife 2019, 8, e50036. [Google Scholar] [CrossRef]
- Sun, W.; Sanderson, P.E.; Zheng, W. Drug Combination Therapy Increases Successful Drug Repositioning. Drug Discov. Today 2016, 21, 1189–1195. [Google Scholar] [CrossRef] [Green Version]
- Correia, A.S.; Gärtner, F.; Vale, N. Drug Combination and Repurposing for Cancer Therapy: The Example of Breast Cancer. Heliyon 2021, 7, e05948. [Google Scholar] [CrossRef] [PubMed]
- Duarte, D.; Cardoso, A.; Vale, N. Synergistic Growth Inhibition of HT-29 Colon and MCF-7 Breast Cancer Cells with Simultaneous and Sequential Combinations of Antineoplastics and CNS Drugs. Int. J. Mol. Sci. 2021, 22, 7408. [Google Scholar] [CrossRef] [PubMed]
- Duarte, D.; Vale, N. New Trends for Antimalarial Drugs: Synergism between Antineoplastics and Antimalarials on Breast Cancer Cells. Biomolecules 2020, 10, 1623. [Google Scholar] [CrossRef] [PubMed]
- Duarte, D.; Rêma, A.; Amorim, I.; Vale, N. Drug Combinations: A New Strategy to Extend Drug Repurposing and Epithelial-Mesenchymal Transition in Breast and Colon Cancer Cells. Biomolecules 2022, 12, 190. [Google Scholar] [CrossRef] [PubMed]
- Chou, T.C. Drug Combination Studies and Their Synergy Quantification Using the Chou-Talalay Method. Cancer Res. 2010, 70, 440–446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roell, K.R.; Reif, D.M.; Motsinger-Reif, A.A. An Introduction to Terminology and Methodology of Chemical Synergy—Perspectives from Across Disciplines. Front. Pharmacol. 2017, 8, 158. [Google Scholar] [CrossRef] [Green Version]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef]
- Pantziarka, P.; Verbaanderd, C.; Huys, I.; Bouche, G.; Meheus, L. Repurposing Drugs in Oncology: From Candidate Selection to Clinical Adoption. Semin. Cancer Biol. 2020, 68, 186–191. [Google Scholar] [CrossRef]
- Gupta, S.C.; Sung, B.; Prasad, S.; Webb, L.J.; Aggarwal, B.B. Cancer Drug Discovery by Repurposing: Teaching New Tricks to Old Dogs. Trends Pharmacol. Sci. 2013, 34, 508–517. [Google Scholar] [CrossRef]
- Webster, R.M. Combination Therapies in Oncology. Nat. Rev. Drug Discov. 2016, 15, 81–82. [Google Scholar] [CrossRef]
- Bailly, C. Potential Use of Edaravone to Reduce Specific Side Effects of Chemo-, Radio- and Immuno-Therapy of Cancers. Int. Immunopharmacol. 2019, 77, 105967. [Google Scholar] [CrossRef] [PubMed]
- Dash, R.P.; Babu, R.J.; Srinivas, N.R. Two Decades-Long Journey from Riluzole to Edaravone: Revisiting the Clinical Pharmacokinetics of the Only Two Amyotrophic Lateral Sclerosis Therapeutics. Clin. Pharmacokinet. 2018, 57, 1385–1398. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.K.; Baker, D.E. Formulary Drug Review: Edaravone. Hosp. Pharm. 2017, 52, 732–736. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Teng, C.; Wu, F.; Ge, L.; Xiao, J.; Zhang, H.; Chen, D. Edaravone Attenuates Traumatic Brain Injury through Anti-Inflammatory and Anti-Oxidative Modulation. Exp. Ther. Med. 2019, 18, 467–474. [Google Scholar] [CrossRef] [Green Version]
- Szczesny-Malysiak, E.; Stojak, M.; Campagna, R.; Grosicki, M.; Jamrozik, M.; Kaczara, P.; Chlopicki, S. Bardoxolone Methyl Displays Detrimental Effects on Endothelial Bioenergetics, Suppresses Endothelial ET-1 Release, and Increases Endothelial Permeability in Human Microvascular Endothelium. Oxid. Med. Cell. Longev. 2020, 2020, 4678252. [Google Scholar] [CrossRef]
- Habib, E.; Linher-Melville, K.; Lin, H.X.; Singh, G. Expression of XCT and Activity of System Xc(-) Are Regulated by NRF2 in Human Breast Cancer Cells in Response to Oxidative Stress. Redox Biol. 2015, 5, 33–42. [Google Scholar] [CrossRef] [Green Version]
- Emanuelli, M.; Sartini, D.; Molinelli, E.; Campagna, R.; Pozzi, V.; Salvolini, E.; Simonetti, O.; Campanati, A.; Offidani, A. The Double-Edged Sword of Oxidative Stress in Skin Damage and Melanoma: From Physiopathology to Therapeutical Approaches. Antioxidants 2022, 11, 612. [Google Scholar] [CrossRef]
- Kokura, S.; Yoshida, N.; Sakamoto, N.; Ishikawa, T.; Takagi, T.; Higashihara, H.; Nakabe, N.; Handa, O.; Naito, Y.; Yoshikawa, T. The Radical Scavenger Edaravone Enhances the Anti-Tumor Effects of CPT-11 in Murine Colon Cancer by Increasing Apoptosis via Inhibition of NF-ΚB. Cancer Lett. 2005, 229, 223–233. [Google Scholar] [CrossRef]
- Nonogawa, M.; Arai, T.; Endo, N.; Pack, S.P.; Kodaki, T.; Makino, K. Reactive Oxygen Species Generation through NADH Oxidation by Pterin Derivatives. Nucleic Acids Symp. Ser. 2008, 52, 567–568. [Google Scholar] [CrossRef] [Green Version]
- Arai, T.; Nonogawa, M.; Makino, K.; Endo, N.; Mori, H.; Miyoshi, T.; Yamashita, K.; Sasada, M.; Kakuyama, M.; Fukuda, K. The Radical Scavenger Edaravone (3-Methyl-1-Phenyl-2-Pyrazolin-5-One) Reacts with a Pterin Derivative and Produces a Cytotoxic Substance That Induces Intracellular Reactive Oxygen Species Generation and Cell Death. J. Pharmacol. Exp. Ther. 2008, 324, 529–538. [Google Scholar] [CrossRef]
- Suzuki, R.; Gopalrao, R.K.; Maeda, H.; Rao, P.; Yamamoto, M.; Xing, Y.; Mizobuchi, S.; Sasaguri, S. MCI-186 Inhibits Tumor Growth through Suppression of EGFR Phosphorylation and Cell Cycle Arrest. Anticancer Res. 2005, 25, 1131–1138. [Google Scholar] [PubMed]
- Iguchi, T.; Nishikawa, M.; Chang, B.; Muroya, O.; Sato, E.; Nakatani, T.; Inoue, M. Edaravone Inhibits Acute Renal Injury and Cyst Formation in Cisplatin-Treated Rat Kidney. Free Radic. Res. 2004, 38, 333–341. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Kumar, A. Protective Effect of Edaravone on Cyclophosphamide Induced Oxidative Stress and Neurotoxicity in Rats. Curr. Drug Saf. 2019, 14, 209. [Google Scholar] [CrossRef] [PubMed]
- Ikegami, E.; Fukazawa, R.; Kanbe, M.; Watanabe, M.; Abe, M.; Watanabe, M.; Kamisago, M.; Hajikano, M.; Katsube, Y.; Ogawa, S. Edaravone, a Potent Free Radical Scavenger, Prevents Anthracycline-Induced Myocardial Cell Death. Circ. J. 2007, 71, 1815–1820. [Google Scholar] [CrossRef] [Green Version]
- Arvanitis, L.A.; Miller, B.G. Multiple Fixed Doses of “seroquel” (Quetiapine) in Patients with Acute Exacerbation of Schizophrenia: A Comparison with Haloperidol and Placebo. Biol. Psychiatry 1997, 42, 233–246. [Google Scholar] [CrossRef]
- Wang, Y.; Huang, N.; Li, H.; Liu, S.; Chen, X.; Yu, S.; Wu, N.; Bian, X.W.; Shen, H.Y.; Li, C.; et al. Promoting Oligodendroglial-Oriented Differentiation of Glioma Stem Cell: A Repurposing of Quetiapine for the Treatment of Malignant Glioma. Oncotarget 2017, 8, 37511–37524. [Google Scholar] [CrossRef]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Combination (Drug A + Drug B) | Dose A | Dose B | Fractional Effect (Fa) | CI Value |
|---|---|---|---|---|
| DOX + edaravone | IC50 | 0.01 | 0.389 | >10 |
| 0.1 | 0.393 | >10 | ||
| 1 | 0.343 | >10 | ||
| 10 | 0.381 | >10 | ||
| 50 | 0.370 | >10 | ||
| 100 | 0.376 | >10 | ||
| PTX + edaravone | IC50 | 0.01 | 0.255 | >10 |
| 0.1 | 0.307 | >10 | ||
| 1 | 0.240 | >10 | ||
| 10 | 0.247 | >10 | ||
| 50 | 0.240 | >10 | ||
| 100 | 0.274 | >10 | ||
| DOX + quetiapine | IC50 | 0.01 | 0.399 | 0.528 |
| 0.1 | 0.464 | 0.363 | ||
| 1 | 0.451 | 0.390 | ||
| 10 | 0.530 | 0.252 | ||
| 50 | 0.554 | 0.231 | ||
| 100 | 0.562 | 0.232 | ||
| PTX + quetiapine | IC50 | 0.01 | 0.173 | 0.182 |
| 0.1 | 0.264 | 0.049 | ||
| 1 | 0.283 | 0.043 | ||
| 10 | 0.231 | 0.186 | ||
| 50 | 0.287 | 0.295 | ||
| 100 | 0.567 | 0.027 |
| Combination (Drug A + Drug B) | Dose A | Dose B | Fractional Effect (Fa) | CI Value |
|---|---|---|---|---|
| 5-FU + edaravone | IC50 | 0.01 | 0.261 | >10 |
| 0.1 | 0.406 | >10 | ||
| 1 | 0.367 | >10 | ||
| 10 | 0.529 | >10 | ||
| 50 | 0.458 | >10 | ||
| 100 | 0.645 | >10 | ||
| 5-FU + quetiapine | IC50 | 0.01 | 0.307 | 0.095 |
| 0.1 | 0.398 | 0.072 | ||
| 1 | 0.374 | 0.102 | ||
| 10 | 0.654 | 0.036 | ||
| 50 | 0.643 | 0.061 | ||
| 100 | 0.775 | 0.026 |
| Drug | HT-29 | MCF-7 | |
|---|---|---|---|
| IC50 (µM) | IC50 (µM) | ||
| CNS | Fluphenazine | 1.86 | 2.68 |
| Fluoxetine | 6.12 | 7.78 | |
| Benztropine | 18.23 | 21.71 | |
| Thioridazine | 4.26 | 5.72 | |
| Sertraline | 2.45 | 2.22 | |
| Entacapone | 40.89 | ND | |
| Tolcapone | 35.47 | ND | |
| Edaravone | >50 | >50 | |
| Quetiapine | 15.19 | >50 | |
| Antimalarials | Artesunate | 17.88 | 11.60 |
| Chloroquine | 32.13 | N.D. | |
| Mefloquine | 2.18 | 1.24 | |
| Cycloguanil | N.D. | 20.30 | |
| Piperazine | N.D. | 3.24 | |
| Primaquine | N.D. | 29.90 | |
| Pyronaridine | 2.43 | 1.39 | |
| Tafenoquine | N.D. | 2.60 |
| Combination (Drug A + Drug B) | Dose A | Dose B | Fractional Effect (Fa) | CI Value |
|---|---|---|---|---|
| Mefloquine + Pyronaridine | IC50 | 0.01 | 0.204 | >10 |
| 0.1 | 0.242 | 7.063 | ||
| 1 | 0.339 | 1.537 | ||
| 10 | 0.582 | 0.205 | ||
| 50 | 0.623 | 0.664 | ||
| 100 | 0.618 | 1.324 | ||
| Pyronaridine + Mefloquine | IC50 | 0.01 | 0.538 | 0.025 |
| 0.1 | 0.514 | 0.038 | ||
| 1 | 0.547 | 0.096 | ||
| 10 | 0.621 | 0.279 | ||
| 50 | 0.619 | 1.358 | ||
| 100 | 0.632 | 2.272 |
| Combination (Drug A + Drug B) | Dose A | Dose B | Fractional Effect (Fa) | CI Value |
|---|---|---|---|---|
| Sertraline + Fluphenazine | IC50 | 0.01 | 0.192 | 8.434 |
| 0.1 | 0.177 | >10 | ||
| 1 | 0.255 | 5.102 | ||
| 10 | 0.601 | 0.351 | ||
| 50 | 0.618 | 1.269 | ||
| 100 | 0.629 | 2.197 | ||
| Fluphenazine + Sertraline | IC50 | 0.01 | 0.156 | >10 |
| 0.1 | 0.196 | >10 | ||
| 1 | 0.218 | >10 | ||
| 10 | 0.619 | 0.250 | ||
| 50 | 0.621 | 0.967 | ||
| 100 | 0.630 | 1.676 |
| Combination (Drug A + Drug B) | Dose A | Dose B | Fractional Effect (Fa) | CI Value |
|---|---|---|---|---|
| Mefloquine + Pyronaridine | IC50 | 0.01 | 0.891 | 0.164 |
| 0.1 | 0.889 | 0.169 | ||
| 1 | 0.891 | 0.192 | ||
| 10 | 0.893 | 0.439 | ||
| 50 | 0.904 | 1.426 | ||
| 100 | 0.907 | 2.643 | ||
| Pyronaridine + Mefloquine | IC50 | 0.01 | 0.385 | 0.373 |
| 0.1 | 0.219 | 0.654 | ||
| 1 | 0.600 | 0.263 | ||
| 10 | 0.850 | 0.256 | ||
| 50 | 0.875 | 0.777 | ||
| 100 | 0.877 | 1.460 |
| Combination (Drug A + Drug B) | Dose A | Dose B | Fractional Effect (Fa) | CI Value |
|---|---|---|---|---|
| Sertraline + Fluphenazine | IC50 | 0.01 | 0.784 | 0.081 |
| 0.1 | 0.789 | 0.083 | ||
| 1 | 0.786 | 0.122 | ||
| 10 | 0.815 | 0.451 | ||
| 50 | 0.840 | 1.749 | ||
| 100 | 0.838 | 3.464 | ||
| Fluphenazine + Sertraline | IC50 | 0.01 | 0.319 | 0.322 |
| 0.1 | 0.399 | 0.262 | ||
| 1 | 0.542 | 0.230 | ||
| 10 | 0.805 | 0.380 | ||
| 50 | 0.831 | 1.466 | ||
| 100 | 0.836 | 2.814 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duarte, D.; Guerreiro, I.; Vale, N. Novel Strategies for Cancer Combat: Drug Combination Using Repurposed Drugs Induces Synergistic Growth Inhibition of MCF-7 Breast and HT-29 Colon Cancer Cells. Curr. Issues Mol. Biol. 2022, 44, 4930-4949. https://doi.org/10.3390/cimb44100335
Duarte D, Guerreiro I, Vale N. Novel Strategies for Cancer Combat: Drug Combination Using Repurposed Drugs Induces Synergistic Growth Inhibition of MCF-7 Breast and HT-29 Colon Cancer Cells. Current Issues in Molecular Biology. 2022; 44(10):4930-4949. https://doi.org/10.3390/cimb44100335
Chicago/Turabian StyleDuarte, Diana, Inês Guerreiro, and Nuno Vale. 2022. "Novel Strategies for Cancer Combat: Drug Combination Using Repurposed Drugs Induces Synergistic Growth Inhibition of MCF-7 Breast and HT-29 Colon Cancer Cells" Current Issues in Molecular Biology 44, no. 10: 4930-4949. https://doi.org/10.3390/cimb44100335