
Serum Levels of VEGF-A and Its Receptors in Patients in Different Phases of Hemorrhagic and Ischemic Strokes

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Subjects
2.2. Blood Samples and ELISA Technique
2.3. Statistical Analysis
2.4. Power Calculation
3. Results
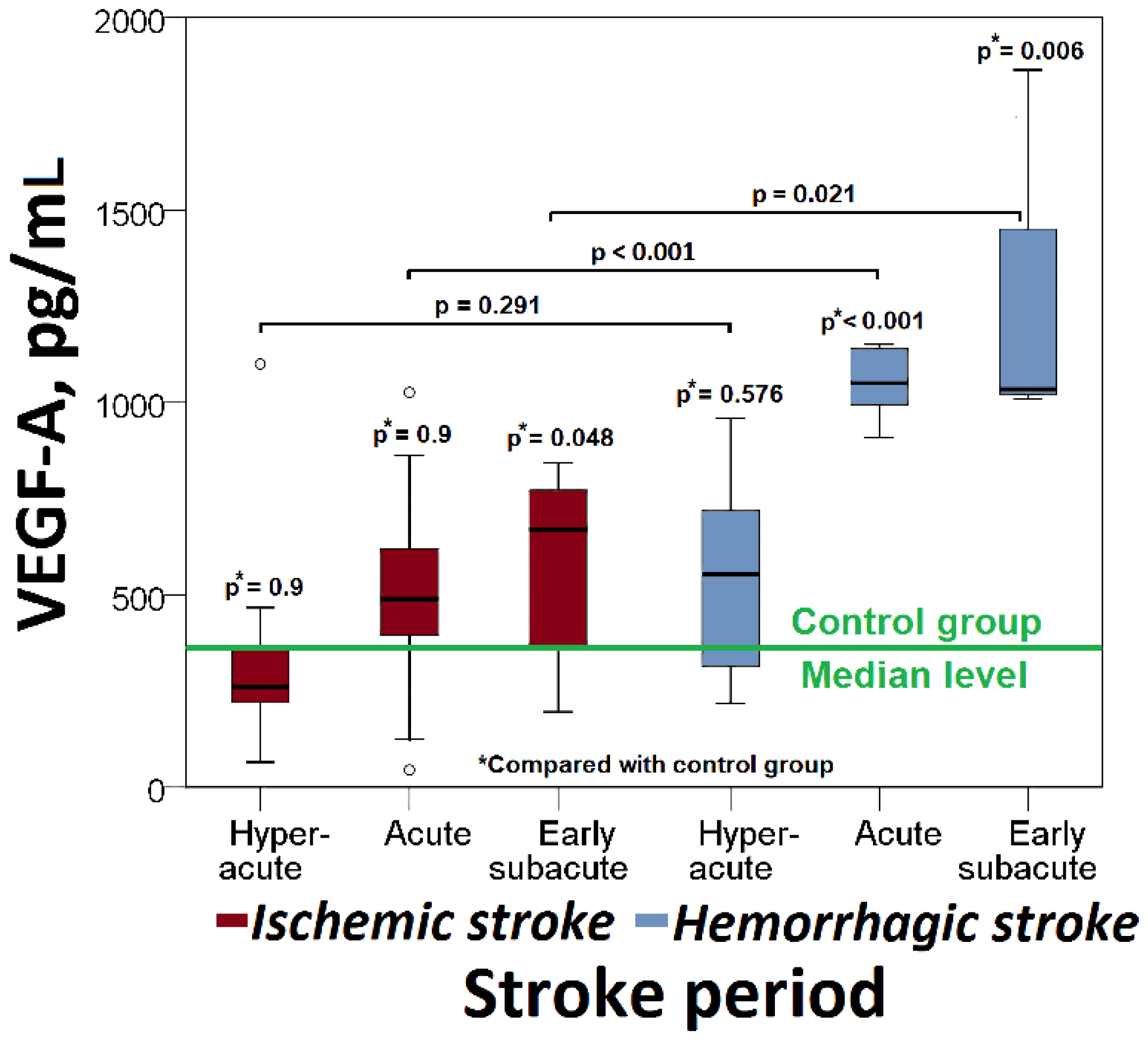
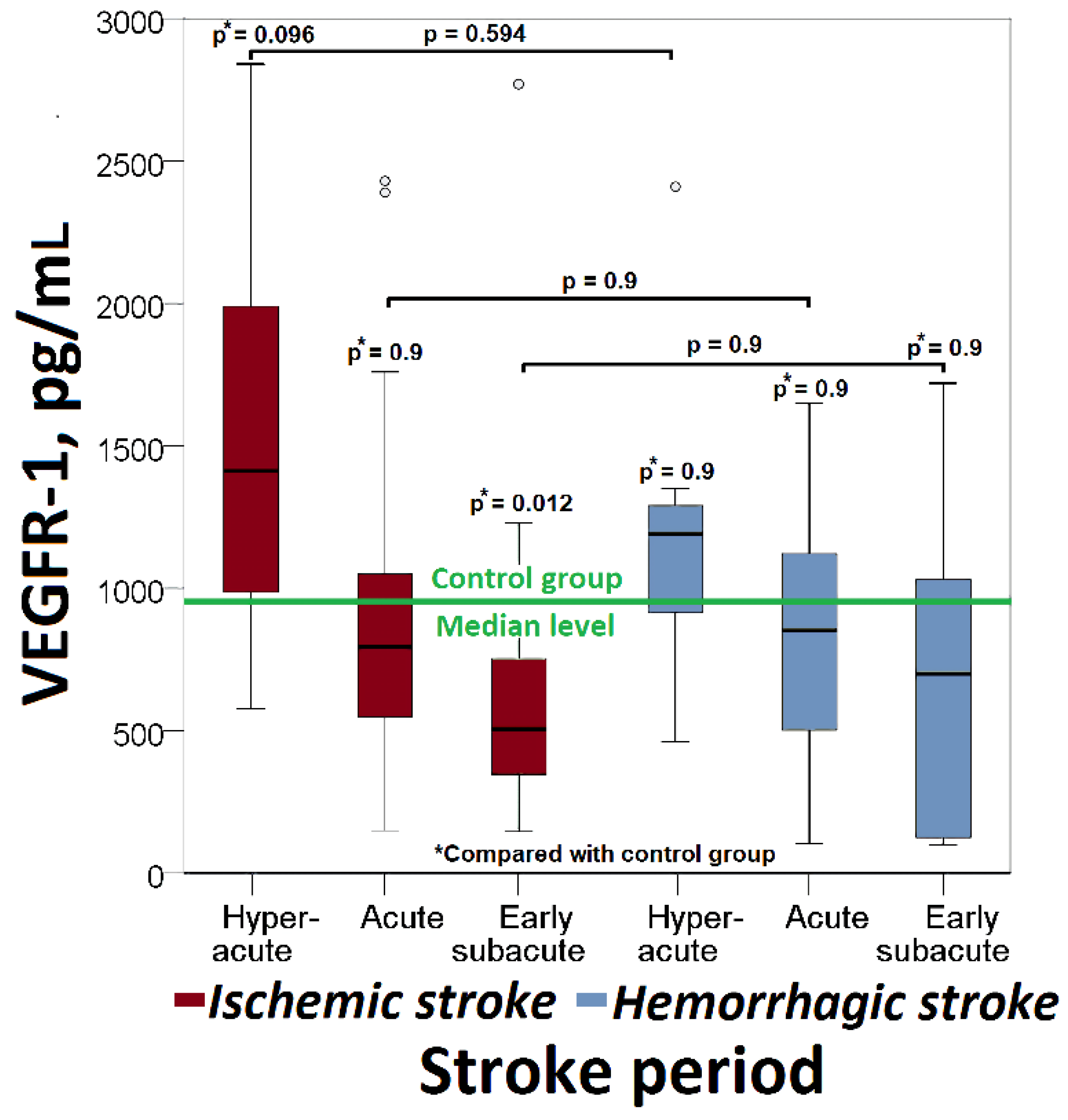
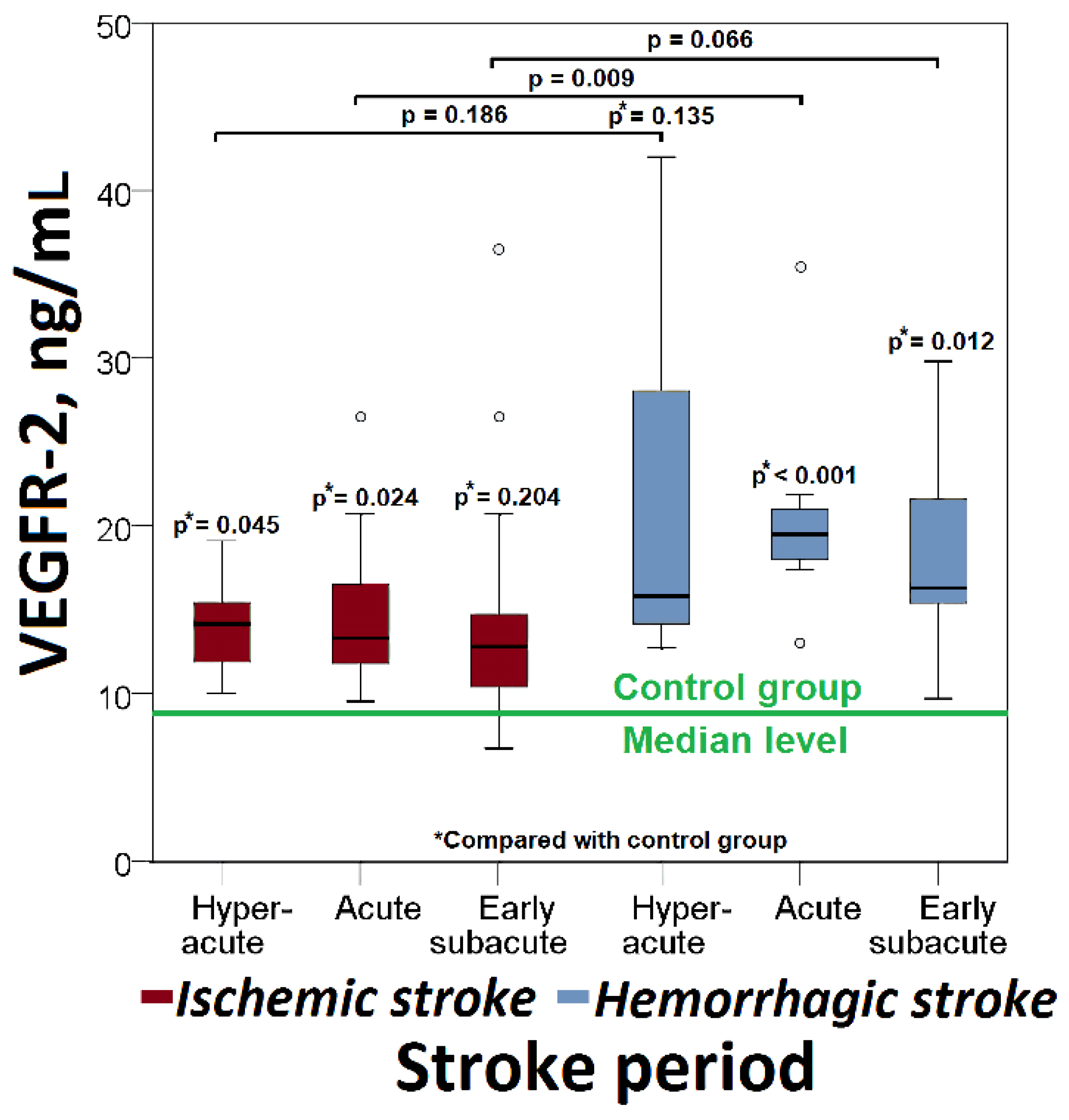
3.1. VEGF-A, VEGFR-1, VEGFR-2 in Different Phases of Ischemic Stroke
3.2. VEGF-A, VEGFR-1, VEGFR-2 in Different Phases of Hemorrhagic Stroke
3.3. VEGF-A, VEGFR-1, VEGFR-2 in Different Types of Stroke
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Mazilina, A.N.; Skalny, A.V.; Fesyun, A.D.; Yakovlev, M.Y.; Savko , S.A.; Namiot , E.D. Review of the Elemental Status in Blood Serum in Patients with Ischemic Stroke. Bull. Rehabil. Med. 2022, 21, 104–113. [Google Scholar] [CrossRef]
- Tokshilykova, A.; Kabdrakhmanova, G.; Sarkulova, Z.; Utepkaliyeva, A.; Khamidulla, A.; Urasheva, Z. Modern Aspects of Etiopathogenesis, Diagnosis and Treatment of Hemorrhagic Stroke NcJSC; West Kazakhstan Marat Ospanov Medical University: Aktobe city, Kazakhstan, 2020. [Google Scholar]
- Wijerathne, H.; Witek, M.A.; Baird, A.E.; Soper, S.A. Liquid biopsy markers for stroke diagnosis. Expert Rev. Mol. Diagn. 2020, 20, 771–788. [Google Scholar] [CrossRef]
- Simpkins, A.N.; Janowski, M.; Oz, H.S.; Roberts, J.; Bix, G.; Doré, S.; Stowe, A.M. Biomarker Application for Precision Medicine in Stroke. Transl. Stroke Res. 2020, 11, 615–627. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brunkhorst, R.; Pfeilschifter, W.; Foerch, C. Astroglial proteins as diagnostic markers of acute intracerebral hemorrhage—Pathophysiological background and clinical findings. Transl. Stroke Res. 2010, 1, 246–251. [Google Scholar] [CrossRef] [PubMed]
- Golubev, A.M.; Grechko, A.V.; Govorukhina, M.A.; Zakharchenko, V.E.; Kuzovlev, A.N.; Petrova, M.V. Molecular Markers of Hemorrhagic Stroke. Gen. Reanimatol. 2020, 16, 34–45. [Google Scholar] [CrossRef]
- Escudero, C.; Acurio, J.; López, E.; Rodríguez, A.; Benavente, A.; Lara, E.; Korzeniewski, S.J. Vascular endothelial growth factor and poor prognosis after ischaemic stroke. Eur. J. Neurol. 2021, 28, 1759–1764. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, H.; Beppu, H.; Mizutani, K.; Okamoto, S.; Sonoda, S. Changes in serum growth factors in stroke rehabilitation patients and their relation to hemiparesis improvement. J. Stroke Cerebrovasc. Dis. 2014, 23, 1703–1708. [Google Scholar] [CrossRef] [PubMed]
- Alrafiah, A.; Alofi, E.; Almohaya, Y.; Hamami, A.; Qadah, T.; Almaghrabi, S.; Hakami, N.; Al-rawaili, M.S.; Tayeb, H.O. Angiogenesis Biomarkers in Ischemic Stroke Patients. J. Inflamm. Res. 2021, 14, 4893–4900. [Google Scholar] [CrossRef] [PubMed]
- Bhasin, A.; Srivastava, M.; Vivekanandhan, S.; Moganty, R.; Talwar, T.; Sharma, S.; Kuthiala, N.; Kumaran, S.; Bhatia, R. Vascular Endothelial Growth Factor as Predictive Biomarker for Stroke Severity and Outcome: An Evaluation of a New Clinical Module in Acute Ischemic Stroke. Neurol. India 2019, 67, 1280–1285. [Google Scholar] [CrossRef] [PubMed]
- Wong, Y.H.; Wu, C.C.; Lai, H.Y.; Jheng, B.R.; Weng, H.Y.; Chang, T.H.; Chen, B.S. Identification of network-based biomarkers of cardioembolic stroke using a systems biology approach with time series data. BMC Syst. Biol. 2015, 9, S4. [Google Scholar] [CrossRef]
- Liu, J.; Li, J. Astrocytes Protect Human Brain Microvascular Endothelial Cells from Hypoxia Injury by Regulating VEGF Expression. J. Healthc. Eng. 2022, 2022, 1884959. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Lei, L.; Cao, J.; Qiao, Y.; Liang, R.; Duan, J.; Feng, Z.; Ding, Y.; Ma, Y.; Yang, Z.; et al. Network pharmacology-based prediction of the active compounds and mechanism of Buyang Huanwu Decoction for ischemic stroke. Exp. Ther. Med. 2021, 22, 1050. [Google Scholar] [CrossRef] [PubMed]
- Jelkmann, W. Pitfalls in the measurement of circulating vascular endothelial growth factor. Clin. Chem. 2001, 47, 617–623. [Google Scholar] [CrossRef] [Green Version]
- da Silva, T.M.V.; Stein, A.M.; de Melo Coelho, F.G.; Rueda, A.V.; Camarini, R.; Galduróz, R.F. Circulating levels of vascular endothelial growth factor in patients with Alzheimer’s disease: A case-control study. Behav. Brain Res. 2022, 437, 114126. [Google Scholar] [CrossRef]
- Belgore, F.M.; Blann, A.D.; Li-Saw-Hee, F.L.; Beevers, D.G.; Lip, G.Y. Plasma levels of vascular en-dothelial growth factor and its soluble receptor (SFlt-1) in essential hypertension. Am. J. Cardiol. 2001, 87, 805–807. [Google Scholar] [CrossRef]
- Blann, A.D.; Belgore, F.M.; McCollum, C.N.; Silverman, S.; Lip, P.L.; Lip, G.Y. Vascular endothelial growth factor and its receptor, Flt-1, in the plasma of patients with coronary or peripheral atherosclerosis, or Type II diabetes. Clin. Sci. 2002, 102, 187–194. [Google Scholar] [CrossRef]
- Hojo, Y.; Ikeda, U.; Zhu, Y.; Okada, M.; Ueno, S.; Arakawa, H.; Fujikawa, H.; Katsuki, T.; Shimada, K. Expression of vascular endothelial growth factor in patients with acute myocardial infarction. J. Am. Coll. Cardiol. 2000, 35, 968–973. [Google Scholar] [CrossRef] [Green Version]
- Chin, B.S.; Chung, N.A.; Gibbs, C.R.; Blann, A.D.; Lip, G.Y. Vascular endothelial growth factor and soluble P-selectin in acute and chronic congestive heart failure. Am. J. Cardiol. 2002, 90, 1258–1260. [Google Scholar] [CrossRef]
- Neufeld, G.; Cohen, T.; Gengrinovitch, S.; Poltorak, Z. Vascular endothelial growth factor (VEGF) and its receptors. FASEB J. 1999, 13, 9–22. [Google Scholar] [CrossRef] [Green Version]
- Peach, C.J.; Mignone, V.W.; Arruda, M.A.; Alcobia, D.C.; Hill, S.J.; Kilpatrick, L.E.; Woolard, J. Molecular Pharmacology of VEGF-A Isoforms: Binding and Signalling at VEGFR2. Int. J. Mol. Sci. 2018, 19, 1264. [Google Scholar] [CrossRef]
- Marks, E.C.A.; Wilkinson, T.M.; Frampton, C.M.; Skelton, L.; Pilbrow, A.P.; Yandle, T.G.; Pemberton, C.J.; Doughty, R.N.; Whalley, G.A.; Ellis, C.J.; et al. Plasma levels of soluble VEGF receptor isoforms, circulating pterins and VEGF system SNPs as prognostic biomarkers in patients with acute coronary syndromes. BMC Cardiovasc. Disord. 2018, 18, 169. [Google Scholar] [CrossRef] [Green Version]
- Cárdenas-Rivera, A.; Campero-Romero, A.N.; Heras-Romero, Y.; Penagos-Puig, A.; Rincón-Heredia, R.; Tovar-Y-Romo, L.B. Early Post-stroke Activation of Vascular Endothelial Growth Factor Receptor 2 Hinders the Receptor 1-Dependent Neuroprotection Afforded by the Endogenous Ligand. Front. Cell. Neurosci. 2019, 13, 270. [Google Scholar] [CrossRef] [PubMed]
- Rosen, L.S. Clinical experience with angiogenesis signaling inhibitors: Focus on vascular endothelial growth factor (VEGF) blockers. Cancer Control 2002, 9, 36–44. [Google Scholar] [CrossRef] [PubMed]
- Yamazaki, Y.; Morita, T. Molecular and functional diversity of vascular endothelial growth factors. Mol. Divers. 2006, 10, 515–527. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Shibuya, M. The vascular endothelial growth factor (VEGF)/VEGF receptor system and its role under physiological and pathological conditions. Clin. Sci. 2005, 109, 227–241. [Google Scholar] [CrossRef] [Green Version]
- Duffy, A.M.; Bouchier-Hayes, D.J.; Harmey, J.H. Vascular Endothelial Growth Factor (VEGF) and Its Role in Non-Endothelial Cells: Autocrine Signalling by VEGF. In Madame Curie Bioscience Database. Austin, TX: Landes Bioscience, 2000–2013. Available online: https://www.ncbi.nlm.nih.gov/books/NBK6482/ (accessed on 21 December 2020).
- Tjwa, M.; Luttun, A.; Autiero, M.; Carmeliet, P. VEGF and PlGF: Two pleiotropic growth factors with distinct roles in development and homeostasis. Cell Tissue Res. 2003, 314, 5–14. [Google Scholar] [CrossRef]
- Dragoni, S.; Turowski, P. Polarised VEGFA Signalling at Vascular Blood–Neural Barriers. Int. J. Mol. Sci. 2018, 19, 1378. [Google Scholar] [CrossRef] [Green Version]
- Melincovici, C.S.; Boşca, A.B.; Şuşman, S.; Mărginean, M.; Mihu, C.; Istrate, M.; Moldovan, I.M.; Roman, A.L.; Mihu, C.M. Vascular endothelial growth factor (VEGF)—Key factor in normal and pathological angiogenesis. Rom. J. Morphol. Embryol. 2018, 59, 455–467. [Google Scholar]
- Jean LeBlanc, N.; Guruswamy, R.; ElAli, A. Vascular Endothelial Growth Factor Isoform-B Stimulates Neurovascular Repair After Ischemic Stroke by Promoting the Function of Pericytes via Vascular Endothelial Growth Factor Receptor-1. Mol. Neurobiol. 2018, 55, 3611–3626. [Google Scholar] [CrossRef]
- Hao, T.; Rockwell, P. Signaling through the vascular endothelial growth factor receptor VEGFR-2 protects hippocampal neurons from mitochondrial dysfunction and oxidative stress. Free Radic. Biol. Med. 2013, 63, 421–431. [Google Scholar] [CrossRef] [Green Version]
- Li, T.; Zhu, Y.; Han, L.; Ren, W.; Liu, H.; Qin, C. VEGFR-1 activation induced MMP-9-dependent invasion in hepatocellular carcinoma. Future Oncol. 2015, 11, 3143–3157. [Google Scholar] [CrossRef] [PubMed]
- Wittko-Schneider, I.M.; Schneider, F.T.; Plate, K.H. Brain homeostasis: VEGF receptor 1 and 2—Two unequal brothers in mind. Cell Mol. Life Sci. 2013, 70, 1705–1725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geiseler, S.J.; Morland, C. The Janus Face of VEGF in Stroke. Int. J. Mol. Sci. 2018, 19, 1362. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, D.A.; Jin, K. Vascular endothelial growth factors (VEGFs) and stroke. Cell Mol. Life Sci. 2013, 70, 1753–1761. [Google Scholar] [CrossRef] [Green Version]
- Carmeliet, P.; Ruiz de Almodovar, C. VEGF ligands and receptors: Implications in neurodevelopment and neurodegeneration. Cell. Mol. Life Sci. 2013, 70, 1763–1778. [Google Scholar] [CrossRef] [PubMed]
- Schoch, H.J.; Fischer, S.; Marti, H.H. Hypoxia-induced vascular endothelial growth factor expression causes vascular leakage in the brain. Brain 2002, 125 Pt 11, 2549–2557. [Google Scholar] [CrossRef]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gotzsche, P.C.; Vandenbroucke, J.P. TROBE Initiative: The strengthening the reporting of observational studies in epidemiology (STROBE) statement: Guidelines for reporting observational studies. BMJ 2007, 335, 806–808. [Google Scholar] [CrossRef] [Green Version]
- Bernhardt, J.; Hayward, K.; Kwakkel, G.; Ward, N.; Wolf, S.L.; Borschmann, K.; Krakauer, J.W.; Boyd, L.A.; Carmichael, S.T.; Corbett, D.; et al. Agreed definitions and a shared vision for new standards in stroke recovery research: The Stroke Recovery and Rehabilitation Roundtable taskforce. Int. J. Stroke 2017, 12, 444–450. [Google Scholar] [CrossRef]
- Xue, L.; Chen, H.; Zhang, T.; Chen, J.; Geng, Z.; Zhao, Y. Changes in serum vascular endothelial growth factor and endostatin concentrations associated with circulating endothelial progenitor cells after acute ischemic stroke. Metab. Brain Dis. 2017, 32, 641–648. [Google Scholar] [CrossRef]
- Prodjohardjono, A.; Vidyanti, A.N.; Susianti, N.A.; Sudarmanta; Sutarni, S.; Setyopranoto, I. Higher level of acute serum VEGF and larger infarct volume are more frequently associated with post-stroke cognitive impairment. PLoS ONE 2020, 15, e0239370. [Google Scholar] [CrossRef]
- Matsuo, R.; Ago, T.; Kamouchi, M.; Kuroda, J.; Kuwashiro, T.; Hata, J.; Sugimori, H.; Fukuda, K.; Gotoh, S.; Makihara, N.; et al. Clinical significance of plasma VEGF value in ischemic stroke—Research for biomarkers in ischemic stroke (REBIOS) study. BMC Neurol. 2013, 13, 32. [Google Scholar] [CrossRef] [PubMed]
- Seidkhani-Nahal, A.; Khosravi, A.; Mirzaei, A.; Basati, G.; Abbasi, M.; Noori-Zadeh, A. Serum vascular endothelial growth factor (VEGF) levels in ischemic stroke patients: A systematic review and meta-analysis of case–control studies. Neurol. Sci. 2021, 42, 1811–1820. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Fujimoto, M.; Kawakita, F.; Ichikawa, N.; Suzuki, H. Vascular Endothelial Growth Factor in Brain Edema Formation After Subarachnoid Hemorrhage. Acta Neurochir Suppl. 2016, 121, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Åberg, N.D.; Wall, A.; Anger, O.; Jood, K.; Andreasson, U.; Blennow, K.; Zetterberg, H.; Isgaard, J.; Jern, C.; Svensson, J. Circulating levels of vascular endothelial growth factor and post-stroke long-term functional outcome. Acta Neurol. Scand. 2020, 141, 405–414. [Google Scholar] [CrossRef] [Green Version]
- Shibuya, M. Differential roles of vascular endothelial growth factor receptor-1 and receptor-2 in angiogenesis. J. Biochem. Mol. Biol. 2006, 39, 469–478. [Google Scholar] [CrossRef]
- Rud’ko, A.S.; Efendieva, M.K.; Budzinskaia, M.V.; Karpilova, M.A. Influence of vascular endothelial growth factor on angiogenesis and neurogenesis. Vestn. Oftalmol. 2017, 133, 75–81. (In Russian) [Google Scholar] [CrossRef]
- Stevens, M.; Oltean, S. Modulation of Receptor Tyrosine Kinase Activity through Alternative Splicing of Ligands and Receptors in the VEGF-A/VEGFR Axis. Cells 2019, 8, 288. [Google Scholar] [CrossRef] [Green Version]
- Chalela, J.A.; Kidwell, C.S.; Nentwich, L.M.; Luby, M.; Butman, J.A.; Demchuk, A.M.; Hill, M.D.; Patronas, N.; Latour, L.; Warach, S. Magnetic resonance imaging and computed tomography in emergency assessment of patients with suspected acute stroke: A prospective comparison. Lancet 2007, 369, 293–298. [Google Scholar] [CrossRef] [Green Version]
- Kim, I.D.; Cave, J.W.; Cho, S. Aflibercept, a VEGF (Vascular Endothelial Growth Factor)-Trap, Reduces Vascular Permeability and Stroke-Induced Brain Swelling in Obese Mice. Stroke 2021, 52, 2637–2648. [Google Scholar] [CrossRef]
- Esposito, E.; Hayakawa, K.; Ahn, B.J.; Chan, S.J.; Xing, C.; Liang, A.C.; Kim, K.-W.; Arai, K.; Lo, E.H. Effects of ischemic post-conditioning on neuronal VEGF regulation and microglial polarization in a rat model of focal cerebral ischemia. J. Neurochem. 2018, 146, 160–172. [Google Scholar] [CrossRef] [Green Version]
- Mao, Y.; Liu, X.; Song, Y.; Zhai, C.; Zhang, L. VEGF-A/VEGFR-2 and FGF-2/FGFR-1 but not PDGF-BB/PDGFR-β play important roles in promoting immature and inflammatory intraplaque angiogenesis. PLoS ONE 2018, 13, e0201395. [Google Scholar] [CrossRef] [PubMed]
- de Vries, M.R.; Parma, L.; Peters, H.A.B.; Schepers, A.; Hamming, J.F.; Jukema, J.W.; Goumans, M.J.T.H.; Guo, L.; Finn, A.V.; Virmani, R.; et al. Blockade of vascular endothelial growth factor receptor 2 inhibits intraplaque haemorrhage by normalization of plaque neovessels. J. Intern. Med. 2019, 285, 59–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mackenzie, F.; Ruhrberg, C. Diverse roles for VEGF-A in the nervous system. Development 2012, 139, 1371–1380. [Google Scholar] [CrossRef] [Green Version]
- Qiu, S.; Wu, T.; Wang, P.; Li, J.; Li, Q.; Du, J. The Association between VEGFR Gene Polymorphisms and Stroke: A Meta-Analysis. PLoS ONE 2016, 11, e0151371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Góra-Kupilas, K.; Jośko, J. The neuroprotective function of vascular endothelial growth factor (VEGF). Folia Neuropathol. 2005, 43, 31–39. [Google Scholar]
- Shim, J.W.; Madsen, J.R. VEGF Signaling in Neurological Disorders. Int. J. Mol. Sci. 2018, 19, 275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.T.; Zhang, P.; Gao, Y.; Li, C.L.; Wang, H.J.; Chen, L.C.; Feng, Y.; Li, R.Y.; Li, Y.L.; Jiang, C.L. Early VEGF inhibition attenuates blood-brain barrier disruption in ischemic rat brains by regulating the expression of MMPs. Mol. Med. Rep. 2017, 15, 57–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, S.J.; Esposito, E.; Hayakawa, K.; Mandaville, E.; Smith, R.; Guo, S.; Niu, W.; Wong, P.T.; Cool, S.M.; Lo, E.H.; et al. Vascular endothelial growth factor 165-binding heparan sulfate promotes functional recovery from cerebral ischemia. Stroke 2020, 51, 2844–2853. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Wang, X.; Yu, Z. Ischemia-reperfusion injury in the brain: Mechanisms and potential therapeutic strategies. Biochem. Pharmacol. Open Access 2016, 5, 213. [Google Scholar] [CrossRef] [Green Version]
- Pillai, D.R.; Dittmar, M.; Baldaranov, D.; Heidemann, R.; Henning, E.C.; Schuierer, G.; Bogdahn, U.; Schlachetzki, F. Cerebral ischemia-reperfusion injury in rats—A 3 T MRI study on biphasic blood-brain barrier opening and the dynamics of edema formation. J. Cereb. Blood Flow. Metab. 2009, 29, 1846–1855. [Google Scholar] [CrossRef]
- Durukan, A.; Marinkovic, I.; Strbian, D.; Pitkonen, M.; Pedrono, E.; Soinne, L.; Abo-Ramadan, U.; Tatlisumak, T. Post-ischemic blood-brain barrier leakage in rats: One-week follow-up by MRI. Brain Res. 2009, 1280, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Sargento-Freitas, J.; Aday, S.; Nunes, C.; Cordeiro, M.; Gouveia, A.; Silva, F.; Machado, C.; Rodrigues, B.; Santo, G.C.; Ferreira, C.; et al. Endothelial progenitor cells enhance blood-brain barrier permeability in subacute stroke. Neurology 2018, 90, e127–e134. [Google Scholar] [CrossRef]
- Abo-Ramadan, U.; Durukan, A.; Pitkonen, M.; Marinkovic, I.; Tatlisumak, E.; Pedrono, E.; Soinne, L.; Strbian, D.; Tatlisumak, T. Post-ischemic leakiness of the blood-brain barrier: A quantitative and systematic assessment by Patlak plots. Exp. Neurol. 2009, 219, 328–333. [Google Scholar] [CrossRef]
- Müller, S.; Kufner, A.; Dell’Orco, A.; Rackoll, T.; Mekle, R.; Piper, S.K.; Fiebach, J.B.; Villringer, K.; Flöel, A.; Endres, M.; et al. Evolution of Blood-Brain Barrier Permeability in Subacute Ischemic Stroke and Associations With Serum Biomarkers and Functional Outcome. Front. Neurol. 2021, 20, 730923. [Google Scholar] [CrossRef] [PubMed]
- Bernardo-Castro, S.; Sousa, J.A.; Brás, A.; Cecília, C.; Rodrigues, B.; Almendra, L.; Sargento-Freitas, J. Pathophysiology of blood–brain barrier permeability throughout the different stages of ischemic stroke and its implication on hemorrhagic transformation and recovery. Front. Neurol. 2020, 11, 1605. [Google Scholar] [CrossRef] [PubMed]
- Sweeney, M.D.; Zhao, Z.; Montagne, A.; Nelson, A.R.; Zlokovic, B.V. Blood-Brain Barrier: From Physiology to Disease and Back. Physiol. Rev. 2019, 99, 21–78. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, L.; Cho, H.J.; Toborek, M. Blood–brain barrier pericytes as a target for HIV-1 infection. Brain 2019, 142, 502–511. [Google Scholar] [CrossRef] [PubMed]
- Kadry, H.; Noorani, B.; Cucullo, L. A blood–brain barrier overview on structure, function, impairment, and biomarkers of integrity. Fluids Barriers CNS 2020, 17, 69. [Google Scholar] [CrossRef] [PubMed]
- Kadry, H.; Noorani, B.; Cucullo, L. Blood-Brain Barrier Dysfunction in CNS Disorders and Putative Therapeutic Targets: An Overview. Pharmaceutics 2021, 13, 1779. [Google Scholar] [CrossRef] [PubMed]
- Solár, P.; Zamani, A.; Lakatosová, K.; Joukal, M. The blood–brain barrier and the neurovascular unit in subarachnoid hemorrhage: Molecular events and potential treatments. Fluids Barriers CNS 2022, 19, 29. [Google Scholar] [CrossRef] [PubMed]
- Topkoru, B.; Egemen, E.; Solaroglu, I.; Zhang, J.H. Early brain injury or vasospasm? An overview of common mechanisms. Expert Rev. Cardiovasc. Ther. 2017, 18, 1424–1429. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Gao, S.; Wang, X.; Cao, Y.; Lu, J.; Chen, S.; Lenahan, C.; Zhang, J.H.; Shao, A.; Zhang, J. Programmed Cell Deaths and Potential Crosstalk With Blood-Brain Barrier Dysfunction After Hemorrhagic Stroke. Front. Cell. Neurosci. 2020, 14, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jiang, X.; Andjelkovic, A.V.; Zhu, L.; Yang, T.; Bennett, M.V.L.; Chen, J.; Keep, R.F.; Shi, Y. Blood-brain barrier dysfunction and recovery after ischemic stroke. Prog. Neurobiol. 2018, 163–164, 144–171. [Google Scholar] [CrossRef] [PubMed]
- Rudilosso, S.; Rodríguez-Vázquez, A.; Urra, X.; Arboix, A. The Potential Impact of Neuroimaging and Translational Research on the Clinical Management of Lacunar Stroke. Int. J. Mol. Sci. 2022, 23, 1497. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Main Group | Control Group | p-Value |
|---|---|---|---|
| N | 108 | 40 | - |
| Sex (M) | 58 (53.7%) | 19 (47.5%) | 0.6 |
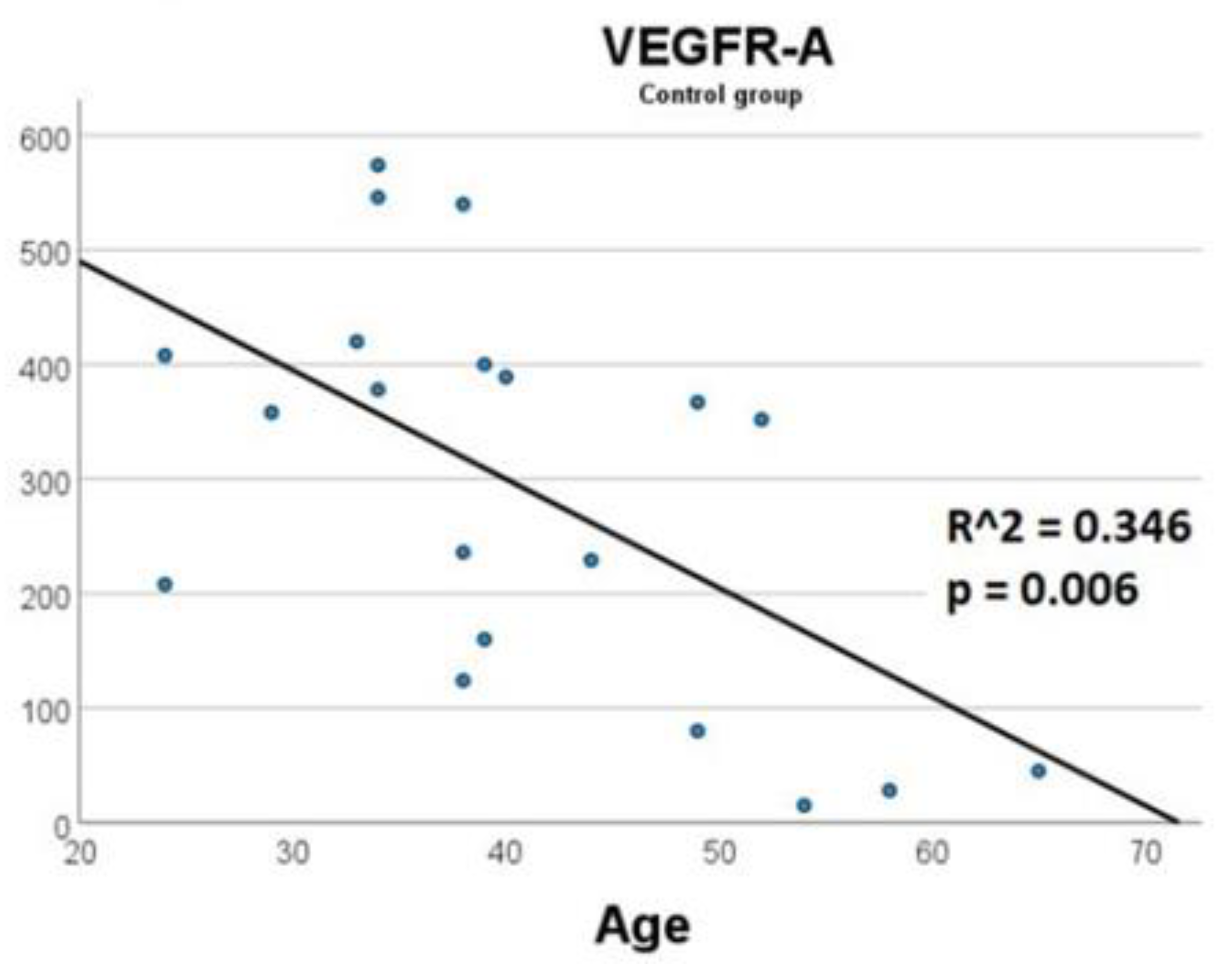
| Age (years) | 68.0 (57.0–79.0), range: 25–89 | 52.5 (38.3–60.0), range: 24–68 | <0.001 * |
| Types and phases of strokes | |||
| Ischemic stroke N = 70 (64.8%) | Hemorrhagic stroke N = 38 (35.2%) | ||
| Age (years): | 75.0 (62.8–80.0) | 58.5 (45.0–62.0) | <0.001 * |
| Sex (M): | 35 (50.0%) | 23 (60.5%) | 0.4 |
| Measurements, N Hyper-acute (N = 35) Acute (N = 42) Early subacute (N = 37) | Measurements, N Hyper-acute (N = 15) Acute (N = 15) Early subacute (N = 13) | ||
| Stroke Phase | Stroke Type | Value | VEGFR-1 (pg/mL) | VEGFR-2 (ng/mL) | VEGF-A (pg/mL) |
|---|---|---|---|---|---|
| Hyper-acute | Hemorrhagic | N | 8 | 8 | 7 |
| Median (IQR) | 1190 (769–1350) | 15.8 (13.6–33.6) | 554 (241–869) | ||
| Min | 461 | 12,7 | 218 | ||
| Max | 2410 | 42,0 | 959 | ||
| Ischemic | N | 18 | 18 | 13 | |
| Median (IQR) | 1412 (957–2055) | 14,2 (11.9–15.6) | 261 (220–410) | ||
| Min | 577 | 10.0 | 65 | ||
| Max | 2840 | 19.1 | 1101 | ||
| Acute | Hemorrhagic | N | 7 | 7 | 8 |
| Median (IQR) | 851 (409–1310) | 19.5 (17.4–21.9) | 1051 (989–1146) | ||
| Min | 105 | 13.0 | 909 | ||
| Max | 1650 | 35.4 | 2221 | ||
| Ischemic | N | 33 | 33 | 9 | |
| Median (IQR) | 793 (535–1055) | 13.3 (11.7–16.6) | 489 (260–742) | ||
| Min | 149 | 9.5 | 45 | ||
| Max | 3910 | 26.5 | 1026 | ||
| Early subacute | Hemorrhagic | N | 9 | 9 | 4 |
| Median (IQR) | 700 (118–1240) | 16.3 (15.1–23.1) | 1034 (1016–1657) | ||
| Min | 99 | 9.7 | 1010 | ||
| Max | 1720 | 29.8 | 1864 | ||
| Ischemic | N | 27 | 27 | 10 | |
| Median (IQR) | 505 (345–753) | 12.8 (10.4–14.8) | 669 (328–779) | ||
| Min | 145 | 6.7 | 196 | ||
| Max | 2770 | 36.5 | 844 | ||
| Control | N/A | N | 20 | 20 | 20 |
| Median (IQR) | 904 (625–1118) | 8.6 (5.9–15.2) | 355 (133–406) | ||
| Min | 260 | 3.7 | 15 | ||
| Max | 1650 | 19.6 | 574 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Babkina, A.S.; Yadgarov, M.Y.; Ostrova, I.V.; Zakharchenko, V.E.; Kuzovlev, A.N.; Grechko, A.V.; Lyubomudrov, M.A.; Golubev, A.M. Serum Levels of VEGF-A and Its Receptors in Patients in Different Phases of Hemorrhagic and Ischemic Strokes. Curr. Issues Mol. Biol. 2022, 44, 4888-4901. https://doi.org/10.3390/cimb44100332
Babkina AS, Yadgarov MY, Ostrova IV, Zakharchenko VE, Kuzovlev AN, Grechko AV, Lyubomudrov MA, Golubev AM. Serum Levels of VEGF-A and Its Receptors in Patients in Different Phases of Hemorrhagic and Ischemic Strokes. Current Issues in Molecular Biology. 2022; 44(10):4888-4901. https://doi.org/10.3390/cimb44100332
Chicago/Turabian StyleBabkina, Anastasiya S., Mikhail Ya. Yadgarov, Irina V. Ostrova, Vladislav E. Zakharchenko, Artem N. Kuzovlev, Andrey V. Grechko, Maxim A. Lyubomudrov, and Arkady M. Golubev. 2022. "Serum Levels of VEGF-A and Its Receptors in Patients in Different Phases of Hemorrhagic and Ischemic Strokes" Current Issues in Molecular Biology 44, no. 10: 4888-4901. https://doi.org/10.3390/cimb44100332