
ADAM10 and ADAM17 as Biomarkers Linked to Inflammation, Metabolic Disorders and Colorectal Cancer
 , , ,
, , ,
Abstract
:1. Introduction
2. Material and Methods
2.1. Study Population and Data Acquisition
2.2. Preparation of Tissue Homogenates
2.3. Total Protein Concentration Determinations
2.4. Determination of ADAM10 and ADAM17 Protein Concentrations
2.5. Statistical Analysis
3. Results
3.1. ADAM10 Protein Concentration
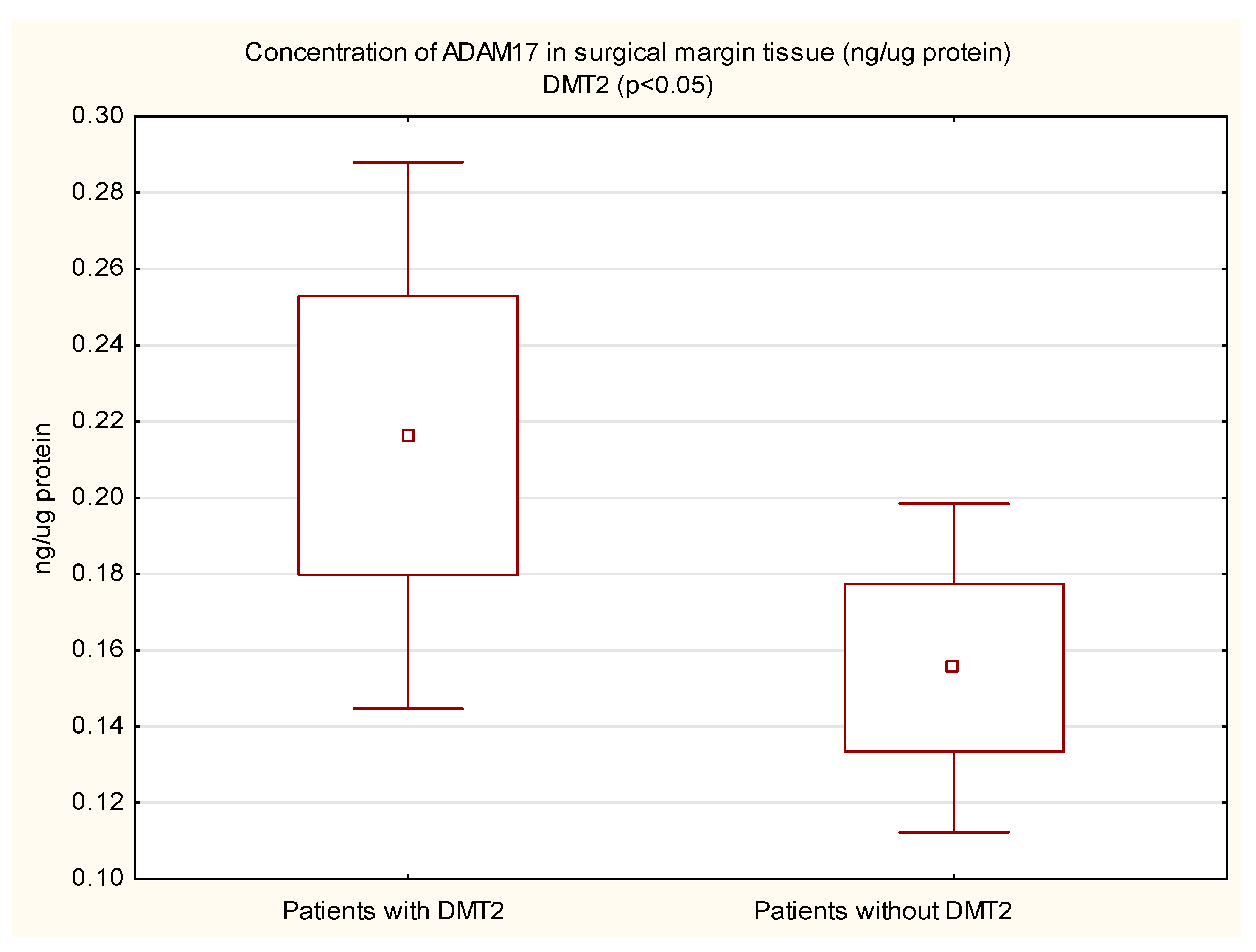
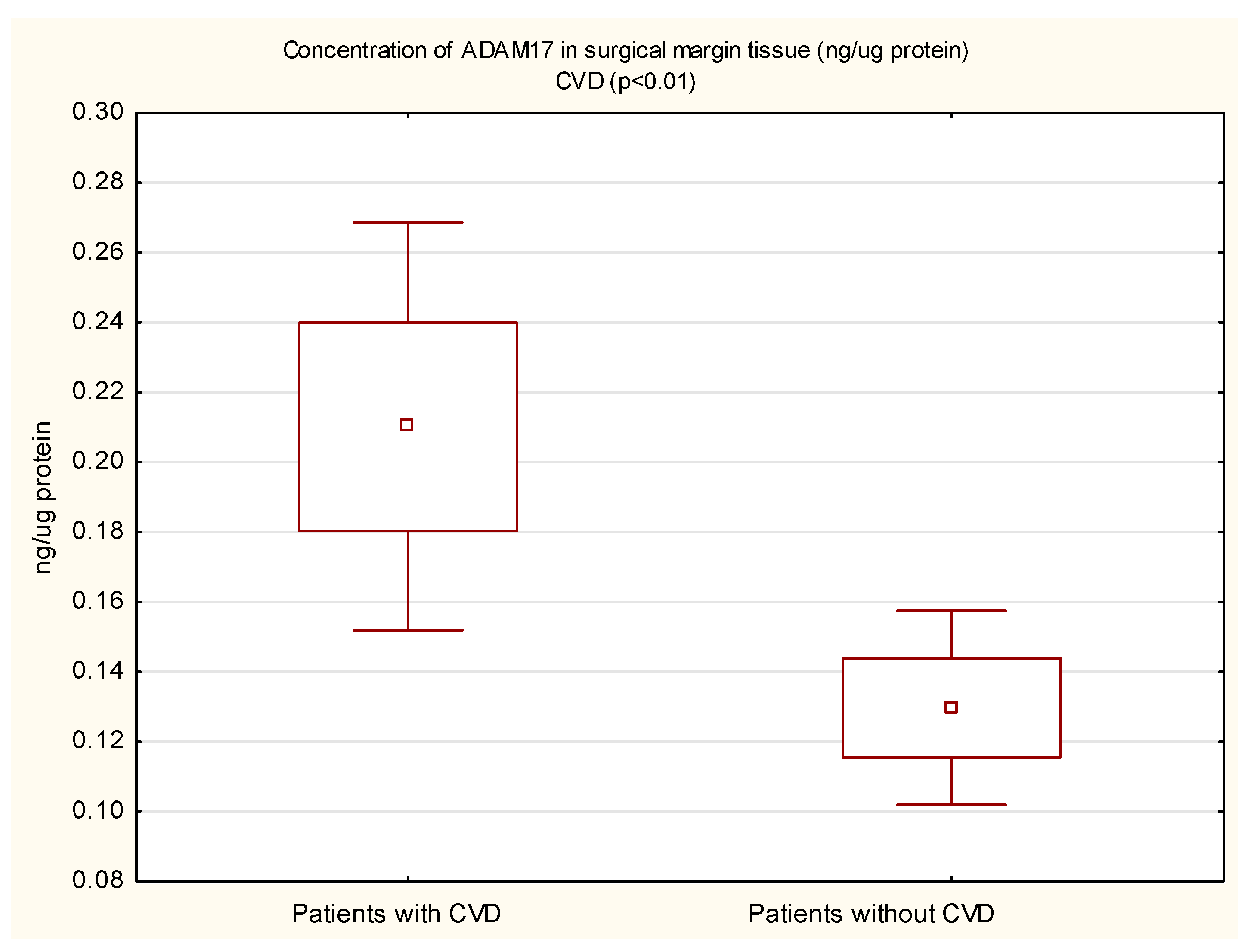
3.2. ADAM17 Protein Concentration
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CVD | Cardiovascular diseases |
| CRC | Colorectal cancer |
| DMT2 | Diabetes mellitus type 2 |
| IBD | Inflammatory bowel diseases |
| CAC | Colitis-associated cancer |
| IGF | Insulin-like growth factor |
| TNFα | Tumor necrosis factor α |
| VEGF | Vascular endothelial growth factor |
| EGF | Epidermal growth factor |
| FGF | Fibroblast growth factor |
| TGFα | Transforming growth factor-alpha |
| IL-6 | Interleukin 6 |
| ADAM | A disintegrin and metalloproteinase |
| ELISA | Enzyme-linked immunosorbent assay |
| BMI | Body mass index |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Axelrad, J.E.; Lichtiger, S.; Yajnik, V. Inflammatory Bowel Disease and Cancer: The Role of Inflammation, Immunosuppression, and Cancer Treatment. World J. Gastroenterol. 2016, 22, 4794. [Google Scholar] [CrossRef] [PubMed]
- Ekbom, A.; Helmick, C.; Zack, M.; Adami, H.O. Ulcerative Colitis and Colorectal Cancer: A Population-Based Study. N. Engl. J. Med. 1990, 323, 7–8. [Google Scholar] [CrossRef]
- Canavan, C.; Abrams, K.R.; Mayberry, J. Meta-Analysis: Colorectal and Small Bowel Cancer Risk in Patients with Crohn’s Disease. Aliment. Pharmacol. Ther. 2006, 23, 1097–1104. [Google Scholar] [CrossRef] [PubMed]
- Walkiewicz, K.; Nowakowska-Zajdel, E.; Kozieł, P.; Muc-Wierzgoń, M. The Role of Some ADAM-Proteins and Activation of the Insulin Growth Factor-Related Pathway in Colorectal Cancer. Cent. Eur. J. Immunol. 2018, 43, 109–113. [Google Scholar] [CrossRef]
- Fushida, S.; Oyama, K.; Kinoshita, J.; Yagi, Y.; Okamoto, K.; Tajima, H.; Ninomiya, I.; Fujimura, T.; Ohta, T. VEGF Is a Target Molecule for Peritoneal Metastasis and Malignant Ascites in Gastric Cancer: Prognostic Significance of VEGF in Ascites and Efficacy of Anti-VEGF Monoclonal Antibody. OncoTargets Ther. 2013, 6, 1445–1451. [Google Scholar] [CrossRef]
- Gao, M.Q.; Kim, B.G.; Kang, S.; Choi, Y.P.; Yoon, J.H.; Cho, N.H. Human Breast Cancer-Associated Fibroblasts Enhance Cancer Cell Proliferation through Increased TGF-α Cleavage by ADAM17. Cancer Lett. 2013, 336, 240–246. [Google Scholar] [CrossRef]
- Moss, M.L.; Minond, D. Recent Advances in ADAM17 Research: A Promising Target for Cancer and Inflammation. Mediat. Inflamm. 2017, 2017, 9673537. [Google Scholar] [CrossRef]
- Jowett, J.B.M.; Okada, Y.; Leedman, P.J.; Curran, J.E.; Johnson, M.P.; Moses, E.K.; Goring, H.H.H.; Mochizuki, S.; Blangero, J.; Stone, L.; et al. ADAM28 Is Elevated in Humans with the Metabolic Syndrome and Is a Novel Sheddase of Human Tumour Necrosis Factor-α. Immunol. Cell Biol. 2012, 90, 966–973. [Google Scholar] [CrossRef]
- Menghini, R.; Fiorentino, L.; Casagrande, V.; Lauro, R.; Federici, M. The Role of ADAM17 in Metabolic Inflammation. Atherosclerosis 2013, 228, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Yuan, S.; Yin, Y.; Wang, K.; Zhou, H.; Qian, C. Tetraspanin-29 Activates Notch Signaling by Interacting with ADAM10 to Enhance Its Activity in Colorectal Cancer. Biochem. Cell Biol. 2022, 100, 292–300. [Google Scholar] [CrossRef] [PubMed]
- Duffy, M.J.; McKiernan, E.; O’Donovan, N.; McGowan, P.M. Role of ADAMs in Cancer Formation and Progression. Clin. Cancer Res. 2009, 15, 1140–1144. [Google Scholar] [CrossRef] [PubMed]
- Matthews, J.; Villescas, S.; Herat, L.; Schlaich, M.; Matthews, V. Implications of ADAM17 Activation for Hyperglycaemia, Obesity and Type 2 Diabetes. Biosci. Rep. 2021, 41, BSR20210029. [Google Scholar] [CrossRef]
- Chemaly, M.; McGilligan, V.; Gibson, M.; Clauss, M.; Watterson, S.; Alexander, H.D.; Bjourson, A.J.; Peace, A. Role of Tumour Necrosis Factor Alpha Converting Enzyme (TACE/ADAM17) and Associated Proteins in Coronary Artery Disease and Cardiac Events. Arch. Cardiovasc. Dis. 2017, 110, 700–711. [Google Scholar] [CrossRef] [PubMed]
- Van Der Vorst, E.P.C.; Weber, C.; Donners, M.M.P.C. A Disintegrin and Metalloproteases (ADAMs) in Cardiovascular, Metabolic and Inflammatory Diseases: Aspects for Theranostic Approaches. Thromb. Haemost. 2018, 118, 1167–1175. [Google Scholar] [CrossRef]
- Koenen, R.R.; Pruessmeyer, J.; Soehnlein, O.; Fraemohs, L.; Zernecke, A.; Schwarz, N.; Reiss, K.; Sarabi, A.; Lindbom, L.; Hackeng, T.M.; et al. Regulated Release and Functional Modulation of Junctional Adhesion Molecule A by Disintegrin Metalloproteinases. Blood 2009, 113, 4799–4809. [Google Scholar] [CrossRef]
- Donners, M.M.P.C.; Wolfs, I.M.J.; Olieslagers, S.; Mohammadi-Motahhari, Z.; Tchaikovski, V.; Heeneman, S.; Van Buul, J.D.; Caolo, V.; Molin, D.G.M.; Post, M.J.; et al. A Disintegrin and Metalloprotease 10 Is a Novel Mediator of Vascular Endothelial Growth Factor-Induced Endothelial Cell Function in Angiogenesis and Is Associated with Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 2188–2195. [Google Scholar] [CrossRef]
- Yoshimura, T.; Tomita, T.; Dixon, M.F.; Axon, A.T.R.; Robinson, P.A.; Crabtree, J.E. ADAMs (A Disintegrin and Metalloproteinase) Messenger RNA Expression in Helicobacter Pylori–Infected, Normal, and Neoplastic Gastric Mucosa. J. Infect. Dis. 2002, 185, 332–340. [Google Scholar] [CrossRef]
- Wang, Y.Y.; Ye, Z.Y.; Li, L.; Zhao, Z.S.; Shao, Q.S.; Tao, H.Q. ADAM 10 Is Associated with Gastric Cancer Progression and Prognosis of Patients. J. Surg. Oncol. 2011, 103, 116–123. [Google Scholar] [CrossRef]
- Shou, Z.X.; Jin, X.; Zhao, Z.S. Upregulated Expression of ADAM17 Is a Prognostic Marker for Patients with Gastric Cancer. Ann. Surg. 2012, 256, 1014–1022. [Google Scholar] [CrossRef]
- Zhang, T.C.; Zhu, W.G.; De Huang, M.; Fan, R.H.; Chen, X.F. Prognostic Value of ADAM17 in Human Gastric Cancer. Med. Oncol. 2012, 29, 2684–2690. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Wang, D.; Sun, X.; Zhang, Y.; Wang, L.; Suo, J. ADAM17 Promotes Lymph Node Metastasis in Gastric Cancer via Activation of the Notch and Wnt Signaling Pathways. Int. J. Mol. Med. 2019, 43, 914–926. [Google Scholar] [CrossRef] [PubMed]
- Ebi, M.; Kataoka, H.; Shimura, T.; Kubota, E.; Hirata, Y.; Mizushima, T.; Mizoshita, T.; Tanaka, M.; Mabuchi, M.; Tsukamoto, H.; et al. TGFβ Induces ProHB-EGF Shedding and EGFR Transactivation through ADAM Activation in Gastric Cancer Cells. Biochem. Biophys. Res. Commun. 2010, 402, 449–454. [Google Scholar] [CrossRef]
- Liu, H.B.; Zhu, Y.; Yang, Q.C.; Shen, Y.; Zhang, X.J.; Chen, H. Expression and Clinical Significance of ADAM17 Protein in Esophageal Squamous Cell Carcinoma. Genet. Mol. Res. 2015, 14, 4391–4398. [Google Scholar] [CrossRef]
- Ringel, J.; Jesnowski, R.; Moniaux, N.; Lüttges, J.; Ringel, J.; Choudhury, A.; Batra, S.K.; Klöppel, G.; Löhr, M. Aberrant Expression of a Disintegrin and Metalloproteinase 17/Tumor Necrosis Factor-α Converting Enzyme Increases the Malignant Potential in Human Pancreatic Ductal Adenocarcinoma. Cancer Res. 2006, 66, 9045–9053. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, P.J. Role of ADAM10 in Intestinal Crypt Homeostasis and Tumorigenesis. Biochim. Biophys. Acta Mol. Cell Res. 2017, 1864, 2228–2239. [Google Scholar] [CrossRef]
- Knösel, T.; Emde, A.; Schlüns, K.; Chen, Y.; Jürchott, K.; Krause, M.; Dietel, M.; Petersen, I. Immunoprofiles of 11 Biomarkers Using Tissue Microarrays Identify Prognostic Subgroups in Colorectal Cancer. Neoplasia 2005, 7, 741–747. [Google Scholar] [CrossRef]
- Terzić, J.; Grivennikov, S.; Karin, E.; Karin, M. Inflammation and Colon Cancer. Gastroenterology 2010, 138, 2101–2114.e5. [Google Scholar] [CrossRef]
- Blanchot-Jossic, F.; Jarry, A.; Masson, D.; Bach-Ngohou, K.; Paineau, J.; Denis, M.G.; Laboisse, C.L.; Mosnier, J.F. Up-Regulated Expression of ADAM17 in Human Colon Carcinoma: Co-Expression with EGFR in Neoplastic and Endothelial Cells. J. Pathol. 2005, 207, 156–163. [Google Scholar] [CrossRef]
- Das, S.; Czarnek, M.; Bzowska, M.; Mężyk-Kopeć, R.; Stalińska, K.; Wyroba, B.; Sroka, J.; Jucha, J.; Deneka, D.; Stokłosa, P.; et al. ADAM17 Silencing in Mouse Colon Carcinoma Cells: The Effect on Tumoricidal Cytokines and Angiogenesis. PLoS ONE 2012, 7, e50791. [Google Scholar] [CrossRef]
- Lichtenstern, C.R.; Ngu, R.K.; Shalapour, S.; Karin, M. Immunotherapy, Inflammation and Colorectal Cancer. Cells 2020, 9, 618. [Google Scholar] [CrossRef] [PubMed]
- Fujita, M.; Matsubara, N.; Matsuda, I.; Maejima, K.; Oosawa, A.; Yamano, T.; Fujimoto, A.; Furuta, M.; Nakano, K.; Oku-Sasaki, A.; et al. Genomic Landscape of Colitis-Associated Cancer Indicates the Impact of Chronic Inflammation and Its Stratification by Mutations in the Wnt Signaling. Oncotarget 2017, 9, 969–981. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Yu, Z.; Yue, B.; Ren, J.; Zhang, J.; Mani, S.; Wang, Z.; Dou, W. Obacunone Reduces Inflammatory Signalling and Tumour Occurrence in Mice with Chronic Inflammation-Induced Colorectal Cancer. Pharm. Biol. 2020, 58, 886–897. [Google Scholar] [CrossRef]
- Walkiewicz, K.; Strzelczyk, J.; Waniczek, D.; Biernacki, K.; Muc-Wierzgoń, M.; Copija, A.; Nowakowska-Zajdel, E. Adamalysines as Biomarkers and a Potential Target of Therapy in Colorectal Cancer Patients: Preliminary Results. Dis. Markers 2019, 2019, 5035234. [Google Scholar] [CrossRef]
- Walkiewicz, K.; Kozieł, P.; Bednarczyk, M.; Błazelonis, A.; Mazurek, U.; Muc-Wierzgoń, M. Expression of Migration-Related Genes in Human Colorectal Cancer and Activity of a Disintegrin and Metalloproteinase 17. BioMed Res. Int. 2016, 2016, 8208904. [Google Scholar] [CrossRef]
- Rios-Doria, J.; Sabol, D.; Chesebrough, J.; Stewart, D.; Xu, L.; Tammali, R.; Cheng, L.; Du, Q.; Schifferli, K.; Rothstein, R.; et al. Amonoclonal Antibody to ADAM17 Inhibits Tumor Growth by Inhibiting EGFR and Non-EGFR-Mediated Pathways. Mol. Cancer Ther. 2015, 14, 1637–1649. [Google Scholar] [CrossRef] [PubMed]
- Dosch, J.; Ziemke, E.; Wan, S.; Luker, K.; Welling, T.; Hardiman, K.; Fearon, E.; Thomas, S.; Flynn, M.; Rios-Doria, J.; et al. Targeting ADAM17 Inhibits Human Colorectal Adenocarcinoma Progression and Tumor-Initiating Cell Frequency. Oncotarget 2017, 8, 65090–65099. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All Patients | Male | Female |
|---|---|---|---|
| n | 72 | 36 | 36 |
| Age (years) | 66.29 ± 10.03 | 64.47 ± 9.83 | 68.11 ± 10.04 |
| BMI (kg/m2) | 27.44 ± 4.42 | 28.36 ± 3.79 | 26.53 ± 4.85 |
| I stage (n) | 13 | 6 | 7 |
| II stage (n) | 16 | 9 | 7 |
| III stage (n) | 21 | 7 | 14 |
| IV stage (n) | 22 | 14 | 8 |
| DMT2 (n) | 29 | 16 | 13 |
| CVD (n) | 44 | 24 | 20 |
| ADAM10 (pg/µg Protein) | ADAM17 (ng/µg Protein) | ||||
|---|---|---|---|---|---|
| Tumor | Surgical Margin | Tumor | Surgical Margin | ||
| Study group (n = 72) | 228.82 ± 112.33 | 249.34 ± 83.44 | 0.23 ± 0.19 | 0.18 ± 0.16 | |
| Stage of colorectal cancer | CSI (n = 13) | 203.5 ± 118.09 | 282.78 ± 69.42 | 0.22 ± 0.19 | 0.12 ± 0.05 |
| CSII (n = 16) | 206.48 ± 113.73 | 266.63 ± 78.65 | 0.23 ± 0.17 | 0.22 ± 0.21 | |
| CSIII (n = 21) | 245.7 ± 120.84 | 248.03 ± 104.37 | 0.25 ± 0.22 | 0.18 ± 0.14 | |
| CSIV (n = 22) | 244.64 ± 100.57 | 219.04 ± 63.92 | 0.23 ± 0.16 | 0.18 ± 0.2 | |
| Sex | Female (n = 36) | 215.40 ± 109.86 | 237.93 ± 82.97 | 0.21 ± 0.15 | 0.14 ± 0.13 a |
| Male (n = 36) | 241.88 ± 114.7 | 260.43 ± 83.55 | 0.25 ± 0.22 | 0.22 ± 0.19 a | |
| BMI | ≥30 kg/m2 (n = 21) | 229.79 ± 96.58 | 253.49 ± 96.57 | 0.26 ± 0.23 | 0.18 ± 0.14 |
| <30 kg/m2 (n = 51) | 228.44 ± 118.83 | 247.71 ± 78.7 | 0.22 ± 0.17 | 0.18 ± 0.17 | |
| DMT2 | Yes (n = 29) | 241.78 ± 124.54 | 250.12 ± 77.68 | 0.28 ± 0.23 b | 0.22 ± 0.2 a |
| No (n = 43) | 226.83 ± 101.75 | 254.43 ± 86.49 | 0.2 ± 0.15 b | 0.16 ± 0.14 a | |
| CVD | Yes (n = 44) | 243.76 ± 115.59 | 258.19 ± 77.91 | 0.25 ± 0.21 | 0.21 ± 0.19 c |
| No (n = 28) | 214.93 ± 102.37 | 242.82 ± 77.91 | 0.19 ± 0.15 | 0.13 ± 0.07 c | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sikora-Skrabaka, M.; Walkiewicz, K.W.; Nowakowska-Zajdel, E.; Waniczek, D.; Strzelczyk, J.K. ADAM10 and ADAM17 as Biomarkers Linked to Inflammation, Metabolic Disorders and Colorectal Cancer. Curr. Issues Mol. Biol. 2022, 44, 4517-4527. https://doi.org/10.3390/cimb44100309
Sikora-Skrabaka M, Walkiewicz KW, Nowakowska-Zajdel E, Waniczek D, Strzelczyk JK. ADAM10 and ADAM17 as Biomarkers Linked to Inflammation, Metabolic Disorders and Colorectal Cancer. Current Issues in Molecular Biology. 2022; 44(10):4517-4527. https://doi.org/10.3390/cimb44100309
Chicago/Turabian StyleSikora-Skrabaka, Magdalena, Katarzyna Weronika Walkiewicz, Ewa Nowakowska-Zajdel, Dariusz Waniczek, and Joanna Katarzyna Strzelczyk. 2022. "ADAM10 and ADAM17 as Biomarkers Linked to Inflammation, Metabolic Disorders and Colorectal Cancer" Current Issues in Molecular Biology 44, no. 10: 4517-4527. https://doi.org/10.3390/cimb44100309