
Netazepide, an Antagonist of Cholecystokinin Type 2 Receptor, Prevents Vincristine-Induced Sensory Neuropathy in Mice

 ,
,  , , and
, , and 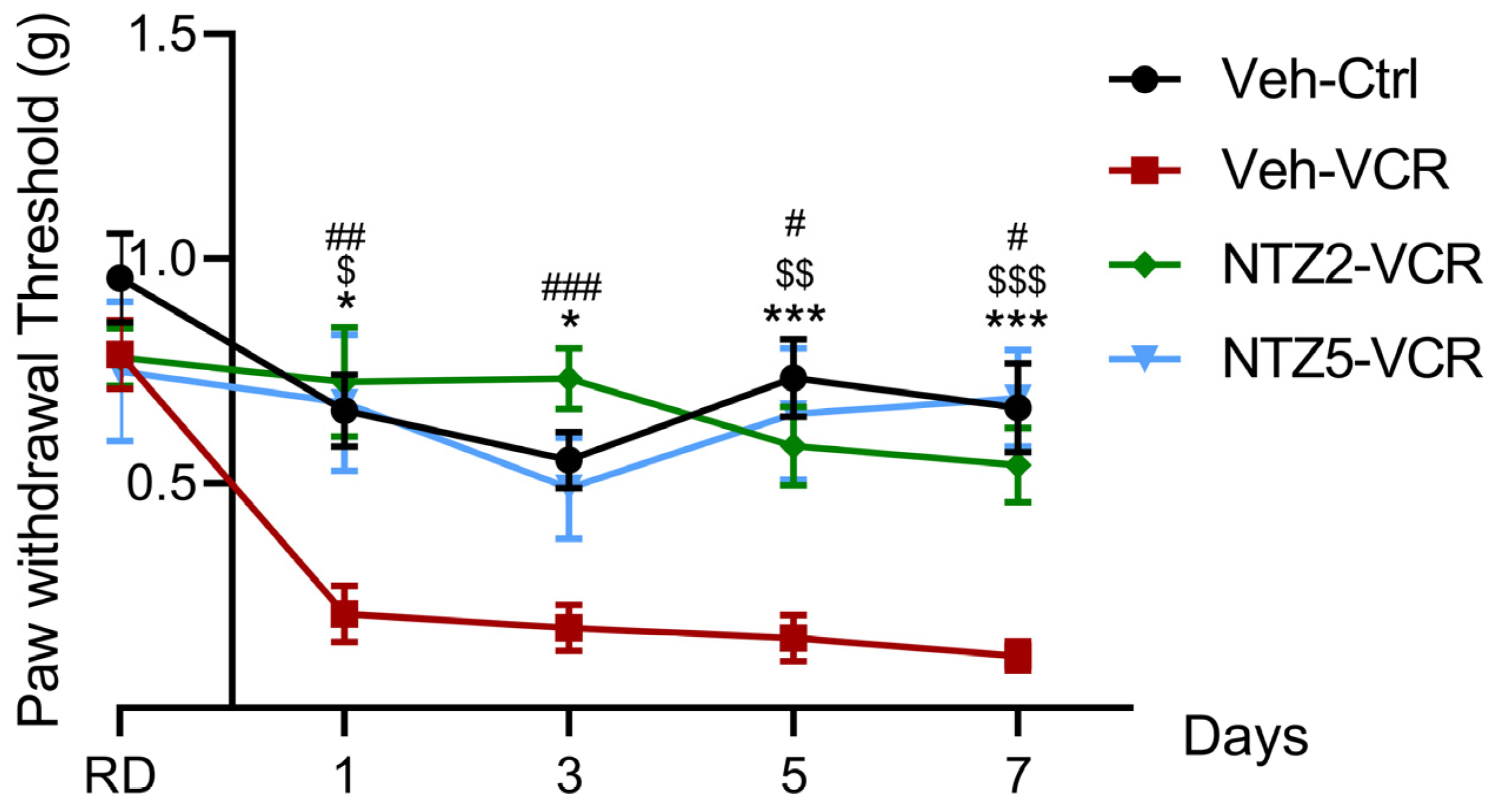{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
2.1. Netazepide at 2 and 5 mg/kg Prevents Vincristine-Induced Allodynia
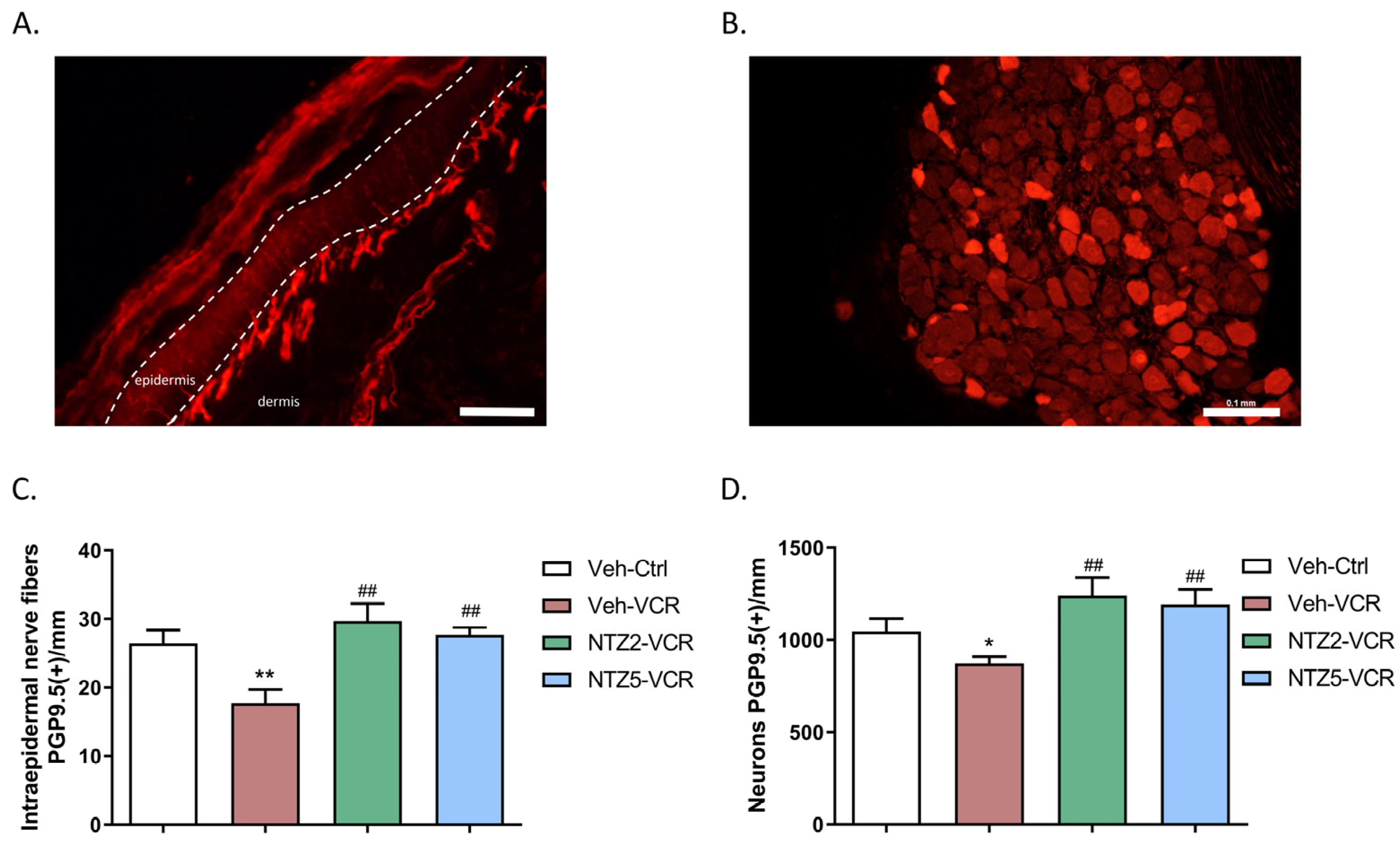
2.2. Netazepide Alleviates the Decrease in IENF and DRG Neuron Densities Induced by Vincristine
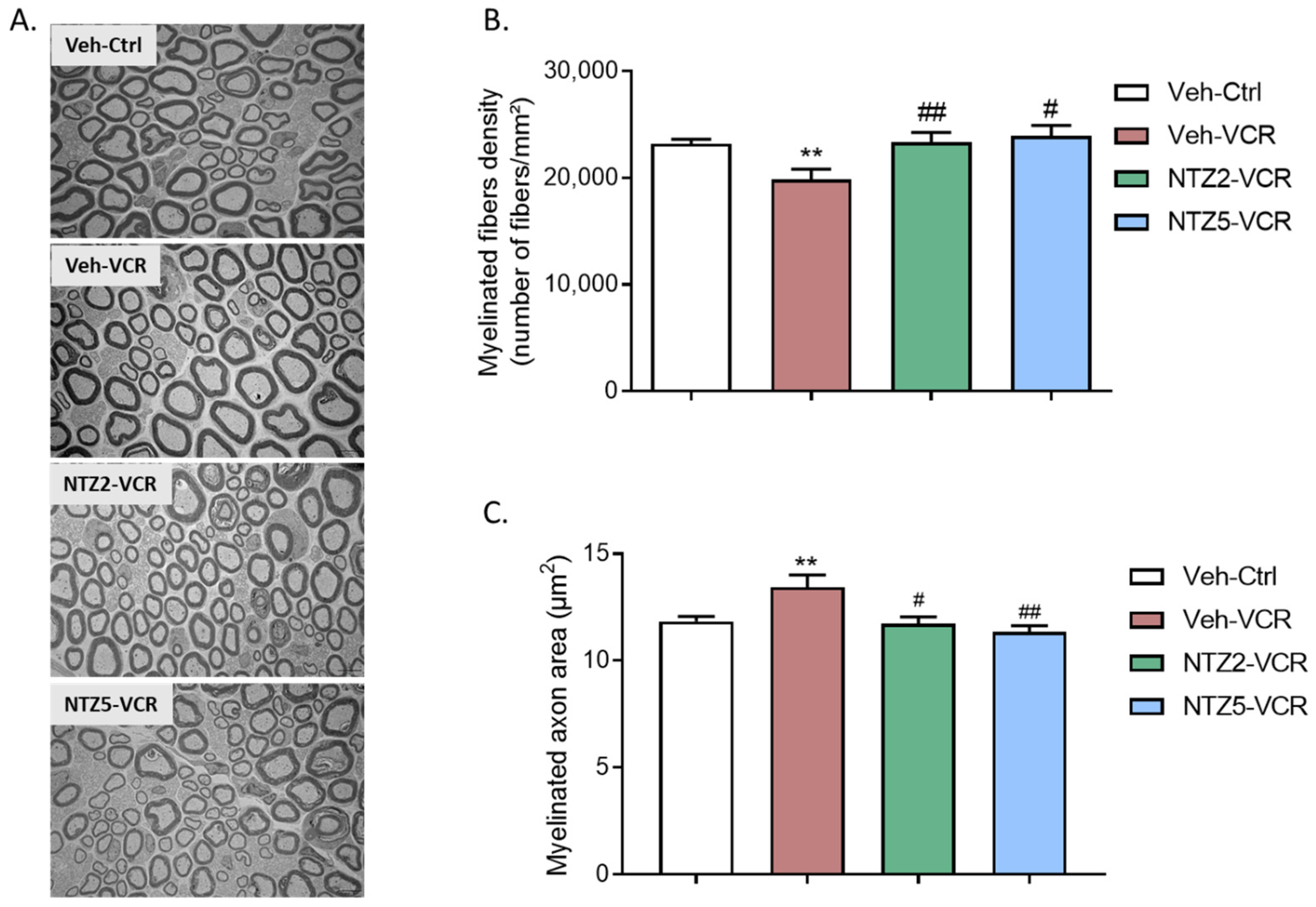
2.3. Effect of Netazepide on Myelinated Nerve Fiber Density and Morphology in Sciatic Nerves on Vincristine-Induced Peripheral Neuropathy Model
3. Discussion
4. Materials and Methods
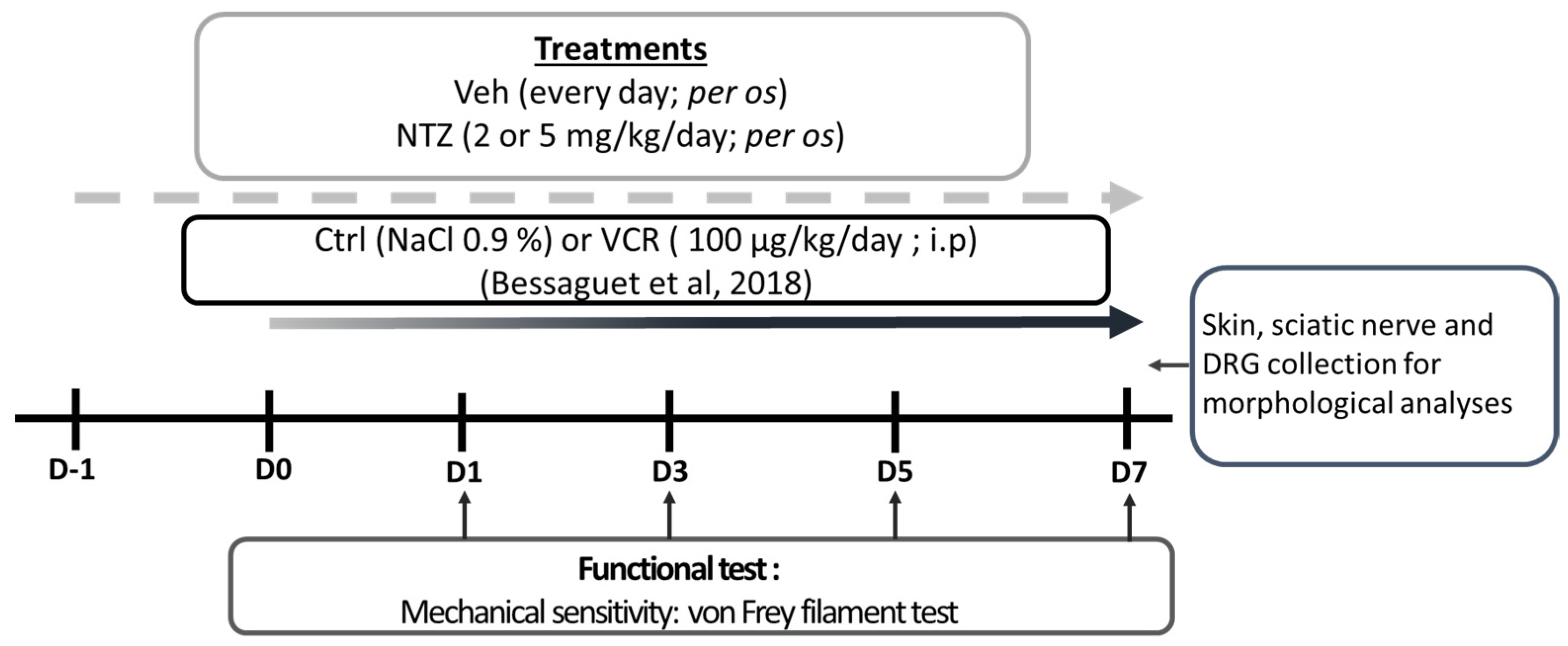
4.1. Treatments
4.2. Behavioral Test
4.3. Immunohistochemistry and Morphological Analyses
4.3.1. Quantification of IENF and DRG Neuron Densities
4.3.2. Sciatic Nerve Ultrastructural Analysis
4.4. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lavoie Smith, E.M.; Li, L.; Chiang, C.; Thomas, K.; Hutchinson, R.J.; Wells, E.M.; Ho, R.H.; Skiles, J.; Chakraborty, A.; Bridges, C.M.; et al. Patterns and Severity of Vincristine-Induced Peripheral Neuropathy in Children with Acute Lymphoblastic Leukemia. J. Peripher. Nerv. Syst. 2015, 20, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Argyriou, A.A.; Bruna, J.; Marmiroli, P.; Cavaletti, G. Chemotherapy-Induced Peripheral Neurotoxicity (CIPN): An Update. Crit. Rev. Oncol. Hematol. 2012, 82, 51–77. [Google Scholar] [CrossRef]
- Awosika, A.O.; Below, J.; Das, J.M. Vincristine. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- Bo, L.; Wang, Y.; Li, Y.; Wurpel, J.N.D.; Huang, Z.; Chen, Z.-S. The Battlefield of Chemotherapy in Pediatric Cancers. Cancers 2023, 15, 1963. [Google Scholar] [CrossRef] [PubMed]
- Bradfield, S.M.; Sandler, E.; Geller, T.; Tamura, R.N.; Krischer, J.P. Glutamic Acid Not Beneficial for the Prevention of Vincristine Neurotoxicity in Children with Cancer: Glutamic Acid for Vincristine Neuroprotection. Pediatr. Blood Cancer 2015, 62, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Mora, E.; Smith, E.M.L.; Donohoe, C.; Hertz, D.L. Vincristine-Induced Peripheral Neuropathy in Pediatric Cancer Patients. Am. J. Cancer Res. 2016, 6, 2416–2430. [Google Scholar] [PubMed]
- Toopchizadeh, V.; Barzegar, M.; Rezamand, A.; Feiz, A.H. Electrophysiological Consequences of Vincristine Contained Chemotherapy in Children: A Cohort Study. J. Pediatr. Neurol. 2009, 7, 351–356. [Google Scholar] [CrossRef]
- Triarico, S.; Romano, A.; Attinà, G.; Capozza, M.A.; Maurizi, P.; Mastrangelo, S.; Ruggiero, A. Vincristine-Induced Peripheral Neuropathy (VIPN) in Pediatric Tumors: Mechanisms, Risk Factors, Strategies of Prevention and Treatment. Int. J. Mol. Sci. 2021, 22, 4112. [Google Scholar] [CrossRef]
- Windebank, A.J.; Grisold, W. Chemotherapy-Induced Neuropathy. J. Peripher. Nerv. Syst. 2008, 13, 27–46. [Google Scholar] [CrossRef]
- Sahenk, Z.; Brady, S.T.; Mendell, J.R. Studies on the Pathogenesis of Vincristine-Induced Neuropathy. Muscle Nerve 1987, 10, 80–84. [Google Scholar] [CrossRef]
- Tanner, K.D.; Levine, J.D.; Topp, K.S. Microtubule Disorientation and Axonal Swelling in Unmyelinated Sensory Axons during Vincristine-Induced Painful Neuropathy in Rat. J. Comp. Neurol. 1998, 395, 481–492. [Google Scholar] [CrossRef]
- D’Souza, R.S.; Alvarez, G.A.M.; Dombovy-Johnson, M.; Eller, J.; Abd-Elsayed, A. Evidence-Based Treatment of Pain in Chemotherapy-Induced Peripheral Neuropathy. Curr. Pain Headache Rep. 2023, 27, 99–116. [Google Scholar] [CrossRef]
- Vecchio, M.; Chiaramonte, R.; Romano, M.; Pavone, P.; Musumeci, G.; Mauro, G.L. A Systematic Review of Pharmacologic and Rehabilitative Treatment of Small Fiber Neuropathies. Diagnostics 2020, 10, 1022. [Google Scholar] [CrossRef]
- Chiaramonte, R.; Pavone, V.; Testa, G.; Pesce, I.; Scaturro, D.; Musumeci, G.; Mauro, G.L.; Vecchio, M. The Role of Physical Exercise and Rehabilitative Implications in the Process of Nerve Repair in Peripheral Neuropathies: A Systematic Review. Diagnostics 2023, 13, 364. [Google Scholar] [CrossRef] [PubMed]
- Colvin, L.A. Chemotherapy-Induced Peripheral Neuropathy (CIPN): Where Are We Now? Pain 2019, 160, S1–S10. [Google Scholar] [CrossRef] [PubMed]
- Anghelescu, D.L.; Tesney, J.M.; Jeha, S.; Wright, B.B.; Trujillo, L.; Sandlund, J.T.; Pauley, J.; Cheng, C.; Pei, D.; Pui, C.-H. Prospective Randomized Trial of Interventions for Vincristine-Related Neuropathic Pain. Pediatr. Blood Cancer 2020, 67, e28539. [Google Scholar] [CrossRef]
- Bernard, A.; Danigo, A.; Bourthoumieu, S.; Mroué, M.; Desmoulière, A.; Sturtz, F.; Rovini, A.; Demiot, C. The Cholecystokinin Type 2 Receptor, a Pharmacological Target for Pain Management. Pharmaceuticals 2021, 14, 1185. [Google Scholar] [CrossRef]
- LaVigne, J.E.; Alles, S.R.A. CCK2 Receptors in Chronic Pain. Neurobiol. Pain 2022, 11, 100092. [Google Scholar] [CrossRef]
- Dockray, G.; Dimaline, R.; Varro, A. Gastrin: Old Hormone, New Functions. Pflug. Arch. 2005, 449, 344–355. [Google Scholar] [CrossRef] [PubMed]
- Dockray, G.J.; Moore, A.; Varro, A.; Pritchard, D.M. Gastrin Receptor Pharmacology. Curr. Gastroenterol. Rep. 2012, 14, 453–459. [Google Scholar] [CrossRef] [PubMed]
- Brifault, C.; Romero, H.; Van-Enoo, A.; Pizzo, D.; Azmoon, P.; Kwon, H.; Nasamran, C.; Gonias, S.L.; Campana, W.M. Deletion of the Gene Encoding the NMDA Receptor GluN1 Subunit in Schwann Cells Causes Ultrastructural Changes in Remak Bundles and Hypersensitivity in Pain Processing. J. Neurosci. 2020, 40, 9121–9136. [Google Scholar] [CrossRef]
- Xu, X.J.; Puke, M.J.; Verge, V.M.; Wiesenfeld-Hallin, Z.; Hughes, J.; Hökfelt, T. Up-Regulation of Cholecystokinin in Primary Sensory Neurons Is Associated with Morphine Insensitivity in Experimental Neuropathic Pain in the Rat. Neurosci. Lett. 1993, 152, 129–132. [Google Scholar] [CrossRef]
- Yin, K.; Deuis, J.R.; Lewis, R.J.; Vetter, I. Transcriptomic and Behavioural Characterisation of a Mouse Model of Burn Pain Identify the Cholecystokinin 2 Receptor as an Analgesic Target. Mol. Pain 2016, 12, 1744806916665366. [Google Scholar] [CrossRef] [PubMed]
- McCleane, G.J. The Cholecystokinin Antagonist Proglumide Enhances the Analgesic Efficacy of Morphine in Humans with Chronic Benign Pain. Anesth. Analg. 1998, 87, 1117–1120. [Google Scholar] [CrossRef] [PubMed]
- Xiao-Jun, X.; Jing-Xia, H.; Seiger, Å.; Hughes, J.; Hökfelt, T.; Wiesenfeld-Hallin, Z. Chronic Pain-Related Behaviors in Spinally Injured Rats: Evidence for Functional Alterations of the Endogenous Cholecystokinin and Opioid Systems. Pain 1994, 56, 271–277. [Google Scholar] [CrossRef]
- Bernard, A.; Danigo, A.; Mroué, M.; Rovini, A.; Richard, L.; Nizou, A.; Desmoulière, A.; Sturtz, F.; Demiot, C.; Bourthoumieu, S. Blockade of Cholecystokinin Type 2 Receptors Prevents the Onset of Vincristine-Induced Neuropathy in Mice. Pharmaceutics 2022, 14, 2823. [Google Scholar] [CrossRef] [PubMed]
- Semple, G.; Ryder, H.; Rooker, D.P.; Batt, A.R.; Kendrick, D.A.; Szelke, M.; Ohta, M.; Satoh, M.; Nishida, A.; Akuzawa, S.; et al. (3R)-N-(1-(Tert-Butylcarbonylmethyl)-2,3-Dihydro-2-Oxo-5-(2-Pyridyl)-1H- 1,4-Benzodiazepin-3-Yl)-N‘-(3-(Methylamino)Phenyl)Urea (YF476): A Potent and Orally Active Gastrin/CCK-B Antagonist. J. Med. Chem. 1997, 40, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Herranz, R. Cholecystokinin Antagonists: Pharmacological and Therapeutic Potential. Med. Res. Rev. 2003, 23, 559–605. [Google Scholar] [CrossRef] [PubMed]
- Black, J.W.; Kalindjian, S.B. Gastrin Agonists and Antagonists. Pharmacol. Toxicol. 2002, 91, 275–281. [Google Scholar] [CrossRef]
- Boyce, M.; Dowen, S.; Turnbull, G.; van den Berg, F.; Zhao, C.-M.; Chen, D.; Black, J. Effect of Netazepide, a Gastrin/CCK2 Receptor Antagonist, on Gastric Acid Secretion and Rabeprazoleinduced Hypergastrinaemia in Healthy Subjects. Br. J. Clin. Pharmacol. 2015, 79, 744–755. [Google Scholar] [CrossRef]
- Boyce, M.; Warrington, S.; Black, J. Netazepide, a Gastrin/CCK2 Receptor Antagonist, Causes Dose-Dependent, Persistent Inhibition of the Responses to Pentagastrin in Healthy Subjects. Br. J. Clin. Pharmacol. 2013, 76, 689–698. [Google Scholar] [CrossRef]
- Boyce, M.; David, O.; Darwin, K.; Mitchell, T.; Johnston, A.; Warrington, S. Single Oral Doses of Netazepide (YF476), a Gastrin Receptor Antagonist, Cause Dose-Dependent, Sustained Increases in Gastric pH Compared with Placebo and Ranitidine in Healthy Subjects. Aliment. Pharmacol. Ther. 2012, 36, 181–189. [Google Scholar] [CrossRef] [PubMed]
- Boyce, M.; Warrington, S. Effect of Repeated Doses of Netazepide, a Gastrin Receptor Antagonist, Omeprazole and Placebo on 24 h Gastric Acidity and Gastrin in Healthy Subjects. Br. J. Clin. Pharmacol. 2013, 76, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Abrams, J.A.; Del Portillo, A.; Hills, C.; Compres, G.; Friedman, R.A.; Cheng, B.; Poneros, J.; Lightdale, C.J.; De La Rue, R.; di Pietro, M.; et al. Randomized Controlled Trial of the Gastrin/CCK2 Receptor Antagonist Netazepide in Patients with Barrett’s Esophagus. Cancer Prev. Res. 2021, 14, 675–682. [Google Scholar] [CrossRef]
- Boyce, M.; Moore, A.R.; Sagatun, L.; Parsons, B.N.; Varro, A.; Campbell, F.; Fossmark, R.; Waldum, H.L.; Pritchard, D.M. Netazepide, a Gastrin/Cholecystokinin-2 Receptor Antagonist, Can Eradicate Gastric Neuroendocrine Tumours in Patients with Autoimmune Chronic Atrophic Gastritis. Br. J. Clin. Pharmacol. 2017, 83, 466–475. [Google Scholar] [CrossRef]
- Bessaguet, F.; Danigo, A.; Bouchenaki, H.; Duchesne, M.; Magy, L.; Richard, L.; Sturtz, F.; Desmoulière, A.; Demiot, C. Neuroprotective Effect of Angiotensin II Type 2 Receptor Stimulation in Vincristine-Induced Mechanical Allodynia. Pain 2018, 159, 2538–2546. [Google Scholar] [CrossRef] [PubMed]
- Gauchan, P.; Andoh, T.; Ikeda, K.; Fujita, M.; Sasaki, A.; Kato, A.; Kuraishi, Y. Mechanical Allodynia Induced by Paclitaxel, Oxaliplatin and Vincristine: Different Effectiveness of Gabapentin and Different Expression of Voltage-Dependent Calcium Channel Alpha(2)Delta-1 Subunit. Biol. Pharm. Bull. 2009, 32, 732–734. [Google Scholar] [CrossRef] [PubMed]
- Kiguchi, N.; Maeda, T.; Kobayashi, Y.; Kishioka, S. Up-Regulation of Tumor Necrosis Factor-Alpha in Spinal Cord Contributes to Vincristine-Induced Mechanical Allodynia in Mice. Neurosci. Lett. 2008, 445, 140–143. [Google Scholar] [CrossRef]
- Saika, F.; Kiguchi, N.; Kobayashi, Y.; Fukazawa, Y.; Maeda, T.; Ozaki, M.; Kishioka, S. Suppressive Effect of Imipramine on Vincristine-Induced Mechanical Allodynia in Mice. Biol. Pharm. Bull. 2009, 32, 1231–1234. [Google Scholar] [CrossRef]
- Jensen, T.S.; Finnerup, N.B. Allodynia and Hyperalgesia in Neuropathic Pain: Clinical Manifestations and Mechanisms. Lancet Neurol. 2014, 13, 924–935. [Google Scholar] [CrossRef]
- Mercadante, S.; Arcuri, E.; Santoni, A. Opioid-Induced Tolerance and Hyperalgesia. CNS Drugs 2019, 33, 943–955. [Google Scholar] [CrossRef]
- Yang, Y.; Li, Q.; He, Q.-H.; Han, J.-S.; Su, L.; Wan, Y. Heteromerization of μ-Opioid Receptor and Cholecystokinin B Receptor through the Third Transmembrane Domain of the μ-Opioid Receptor Contributes to the Anti-Opioid Effects of Cholecystokinin Octapeptide. Exp. Mol. Med. 2018, 50, 1–16. [Google Scholar] [CrossRef] [PubMed]
- McCleane, G.J. A Randomised, Double Blind, Placebo Controlled Crossover Study of the Cholecystokinin 2 Antagonist L-365,260 as an Adjunct to Strong Opioids in Chronic Human Neuropathic Pain. Neurosci. Lett. 2003, 338, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Tortorici, V.; Nogueira, L.; Salas, R.; Vanegas, H. Involvement of Local Cholecystokinin in the Tolerance Induced by Morphine Microinjections into the Periaqueductal Gray of Rats. Pain 2003, 102, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Vanderah, T.W.; Bernstein, R.N.; Yamamura, H.I.; Hruby, V.J.; Porreca, F. Enhancement of Morphine Antinociception by a CCKB Antagonist in Mice Is Mediated via Opioid Delta Receptors. J. Pharmacol. Exp. Ther. 1996, 278, 212–219. [Google Scholar] [PubMed]
- Wilson, A.A.; Jin, L.; Garcia, A.; DaSilva, J.N.; Houle, S. Carbon-11 Labelled cholecystokinin B Antagonists: Radiosynthesis and Evaluation in Rats. Life Sci. 2001, 68, 1223–1230. [Google Scholar] [CrossRef] [PubMed]
- Haradahira, T.; Inoue, O.; Kobayashi, K.; Suzuki, K. Synthesis and Evaluation of 11C-Labeled Nonpeptide Antagonists for Cholecystokinin Receptors: [11C]L-365,260 and [11C]L-365,346. Nucl. Med. Biol. 1998, 25, 203–208. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.; Chapman, K.L.; Heald, A.; Smith, A.J.; Freedman, S.B. Measurement of Central Nervous System Activity of Systemically Administered CCKB Receptor Antagonists by Ex Vivo Binding. Eur. J. Pharmacol. 1994, 253, 237–244. [Google Scholar] [CrossRef]
- Zhang, W.; Gardell, S.; Zhang, D.; Xie, J.Y.; Agnes, R.S.; Badghisi, H.; Hruby, V.J.; Rance, N.; Ossipov, M.H.; Vanderah, T.W.; et al. Neuropathic Pain Is Maintained by Brainstem Neurons Co-Expressing Opioid and Cholecystokinin Receptors. Brain 2009, 132, 778–787. [Google Scholar] [CrossRef]
- Zhang, X.; Asim, M.; Fang, W.; Md Monir, H.; Wang, H.; Kim, K.; Feng, H.; Wang, S.; Gao, Q.; Lai, Y.; et al. Cholecystokinin B Receptor Antagonists for the Treatment of Depression via Blocking Long-Term Potentiation in the Basolateral Amygdala. Mol. Psychiatry 2023, 28, 3459–3474. [Google Scholar] [CrossRef]
- Yu, S.; Zhang, Y.; Zhao, X.; Chang, Z.; Wei, Y.; Sun, Y.; Jiang, D.; Jiang, X.; Tao, J. Cholecystokinin Type B Receptor-Mediated Inhibition of a-Type K+ Channels Enhances Sensory Neuronal Excitability Through the Phosphatidylinositol 3-Kinase and C-Src-Dependent Jnk Pathway. Cell. Commun. Signal. 2019, 17, 68. [Google Scholar] [CrossRef]
- Vydyanathan, A.; Wu, Z.-Z.; Chen, S.-R.; Pan, H.-L. A-Type Voltage-Gated K+ Currents Influence Firing Properties of Isolectin B4-Positive but Not Isolectin B4-Negative Primary Sensory Neurons. J. Neurophysiol. 2005, 93, 3401–3409. [Google Scholar] [CrossRef] [PubMed]
- Liljencrantz, J.; Björnsdotter, M.; Morrison, I.; Bergstrand, S.; Ceko, M.; Seminowicz, D.A.; Cole, J.; Bushnell, C.M.; Olausson, H. Altered C-Tactile Processing in Human Dynamic Tactile Allodynia. Pain 2013, 154, 227–234. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, A.; Inomata, Y.; Serizawa, K.; Andoh, T.; Kuraishi, Y. Contribution of Sensory C-Fiber Neuron Injury to Mechanical Dynamic Allodynia in a Murine Model of Postherpetic Neuralgia. NeuroReport 2013, 24, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Smith, A.K.; O’Hara, C.L.; Stucky, C.L. Mechanical Sensitization of Cutaneous Sensory Fibers in the Spared Nerve Injury Mouse Model. Mol. Pain 2013, 9. [Google Scholar] [CrossRef] [PubMed]
- Chiaramonte, R.; Romano, M.; Vecchio, M. A Systematic Review of the Diagnostic Methods of Small Fiber Neuropathies in Rehabilitation. Diagnostics 2020, 10, 613. [Google Scholar] [CrossRef]
- Siau, C.; Xiao, W.; Bennett, G.J. Paclitaxel- and Vincristine-Evoked Painful Peripheral Neuropathies: Loss of Epidermal Innervation and Activation of Langerhans Cells. Exp. Neurol. 2006, 201, 507–514. [Google Scholar] [CrossRef]
- Boehmerle, W.; Huehnchen, P.; Peruzzaro, S.; Balkaya, M.; Endres, M. Electrophysiological, Behavioral and Histological Characterization of Paclitaxel, Cisplatin, Vincristine and Bortezomib-Induced Neuropathy in C57Bl/6 Mice. Sci. Rep. 2014, 4, 6370. [Google Scholar] [CrossRef]
- Topp, K.S.; Tanner, K.D.; Levine, J.D. Damage to the Cytoskeleton of Large Diameter Sensory Neurons and Myelinated Axons in Vincristine-Induced Painful Peripheral Neuropathy in the Rat. J. Comp. Neurol. 2000, 424, 563–576. [Google Scholar] [CrossRef]
- Li, G.; Hu, Y.; Li, D.; Zhang, Y.; Guo, H.; Li, Y.; Chen, F.; Xu, J. Vincristine-Induced Peripheral Neuropathy: A Mini-Review. NeuroToxicology 2020, 81, 161–171. [Google Scholar] [CrossRef]
- Morfini, G.A.; Burns, M.; Binder, L.I.; Kanaan, N.M.; LaPointe, N.; Bosco, D.A.; Brown, R.H.; Brown, H.; Tiwari, A.; Hayward, L.; et al. Axonal Transport Defects in Neurodegenerative Diseases. J. Neurosci. 2009, 29, 12776–12786. [Google Scholar] [CrossRef]
- Tari, C.; Fournier, N.; Briand, C.; Ducet, G.; Crevat, A. Action of Vinca Alkaloides on Calcium Movements through Mitochondrial Membrane. Pharmacol. Res. Commun. 1986, 18, 519–528. [Google Scholar] [PubMed]
- Park, J.Y.; Jang, S.Y.; Shin, Y.K.; Koh, H.; Suh, D.J.; Shinji, T.; Araki, T.; Park, H.T. Mitochondrial Swelling and Microtubule Depolymerization Are Associated with Energy Depletion in Axon Degeneration. Neuroscience 2013, 238, 258–269. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.; Pizzo, P.; Filadi, R. Calcium, Mitochondria and Cell Metabolism: A Functional Triangle in Bioenergetics. Biochim. Biophys. Acta (BBA) Mol. Cell Res. 2019, 1866, 1068–1078. [Google Scholar] [CrossRef] [PubMed]
- Kaufmann, R.; Lindschau, C.; Schöneberg, T.; Haller, H.; Henklein, P.; Boomgaarden, M.; Ott, T. Type B Cholecystokinin Receptors on Rat Glioma C6 Cells. Binding Studies and Measurement of Intracellular Calcium Mobilization. Brain Res. 1994, 639, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Kaelberer, M.M.; Caceres, A.I.; Jordt, S.-E. Activation of a Nerve Injury Transcriptional Signature in Airway-Innervating Sensory Neurons after Lipopolysaccharide-Induced Lung Inflammation. Am. J. Physiol. Lung Cell Mol. Physiol. 2020, 318, L953–L964. [Google Scholar] [CrossRef] [PubMed]
- Nadella, S.; Ciofoaia, V.; Cao, H.; Kallakury, B.; Tucker, R.D.; Smith, J.P. Cholecystokinin Receptor Antagonist Therapy Decreases Inflammation and Fibrosis in Chronic Pancreatitis. Dig. Dis. Sci. 2020, 65, 1376–1384. [Google Scholar] [CrossRef]
- Percie du Sert, N.; Ahluwalia, A.; Alam, S.; Avey, M.T.; Baker, M.; Browne, W.J.; Clark, A.; Cuthill, I.C.; Dirnagl, U.; Emerson, M.; et al. Reporting Animal Research: Explanation and Elaboration for the ARRIVE Guidelines 2.0. PLoS Biol. 2020, 18, e3000411. [Google Scholar] [CrossRef] [PubMed]
- Boyce, M. Clinical Pharmacology of Netazepide, a Gastrin/CCK2 Receptor Antagonist. Ph.D. Thesis, Institute of Translational Medicine, Department of Cellular and Molecular Physiology, University of Liverpool, Liverpool, UK, 16 May 2016. [Google Scholar]
- Nair, A.B.; Jacob, S. A Simple Practice Guide for Dose Conversion between Animals and Human. J. Basic Clin. Pharm. 2016, 7, 27–31. [Google Scholar] [CrossRef]
- Bouchenaki, H.; Danigo, A.; Bernard, A.; Bessaguet, F.; Richard, L.; Sturtz, F.; Balayssac, D.; Magy, L.; Demiot, C. Ramipril Alleviates Oxaliplatin-Induced Acute Pain Syndrome in Mice. Front. Pharmacol. 2021, 12, 712442. [Google Scholar] [CrossRef]
- Bonin, R.P.; Bories, C.; De Koninck, Y. A Simplified Up-Down Method (SUDO) for Measuring Mechanical Nociception in Rodents Using von Frey Filaments. Mol. Pain 2014, 10, 1–10. [Google Scholar] [CrossRef]
- Boyce, M.; Lloyd, K.A.; Pritchard, D.M. Potential Clinical Indications for a CCK2 Receptor Antagonist. Curr. Opin. Pharmacol. 2016, 31, 68–75. [Google Scholar] [CrossRef] [PubMed]
- Roy, J.; Putt, K.S.; Coppola, D.; Leon, M.E.; Khalil, F.K.; Centeno, B.A.; Clark, N.; Stark, V.E.; Morse, D.L.; Low, P.S. Assessment of Cholecystokinin 2 Receptor (CCK2R) in Neoplastic Tissue. Oncotarget 2016, 7, 14605–14615. [Google Scholar] [CrossRef] [PubMed]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bernard, A.; Mroué, M.; Bourthoumieu, S.; Boyce, M.; Richard, L.; Sturtz, F.; Demiot, C.; Danigo, A. Netazepide, an Antagonist of Cholecystokinin Type 2 Receptor, Prevents Vincristine-Induced Sensory Neuropathy in Mice. Pharmaceuticals 2024, 17, 144. https://doi.org/10.3390/ph17020144
Bernard A, Mroué M, Bourthoumieu S, Boyce M, Richard L, Sturtz F, Demiot C, Danigo A. Netazepide, an Antagonist of Cholecystokinin Type 2 Receptor, Prevents Vincristine-Induced Sensory Neuropathy in Mice. Pharmaceuticals. 2024; 17(2):144. https://doi.org/10.3390/ph17020144
Chicago/Turabian StyleBernard, Amandine, Mohamad Mroué, Sylvie Bourthoumieu, Malcolm Boyce, Laurence Richard, Franck Sturtz, Claire Demiot, and Aurore Danigo. 2024. "Netazepide, an Antagonist of Cholecystokinin Type 2 Receptor, Prevents Vincristine-Induced Sensory Neuropathy in Mice" Pharmaceuticals 17, no. 2: 144. https://doi.org/10.3390/ph17020144