
Evaluation of Pupillometry for CYP2D6 Phenotyping in Children Treated with Tramadol

 , , and
, , and
Abstract
:1. Introduction
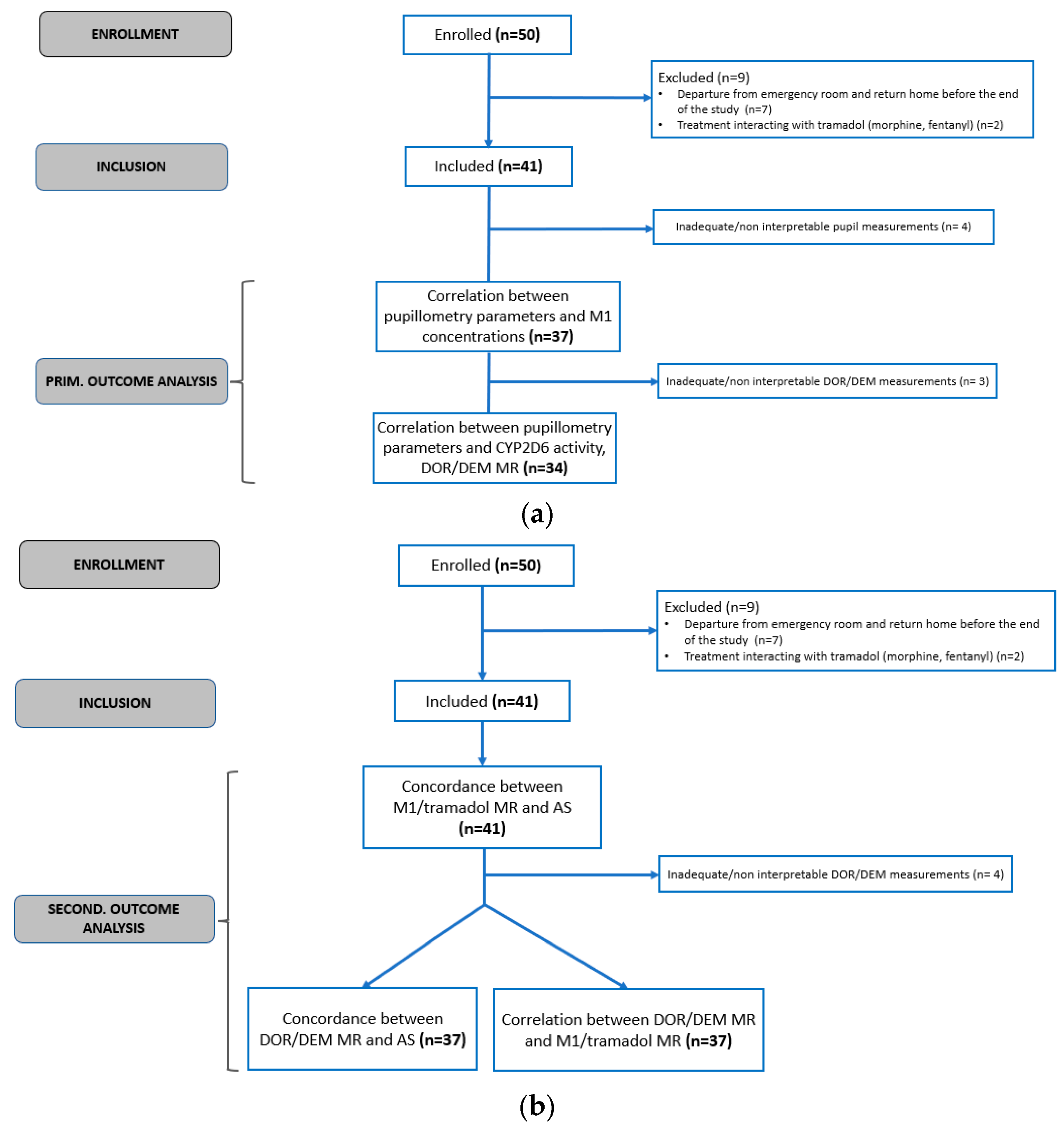
2. Results
2.1. Population Characteristics and Demographics
2.2. Correlation between Pupillometry Parameters and CYP2D6 Activity
Feasibility and Safety
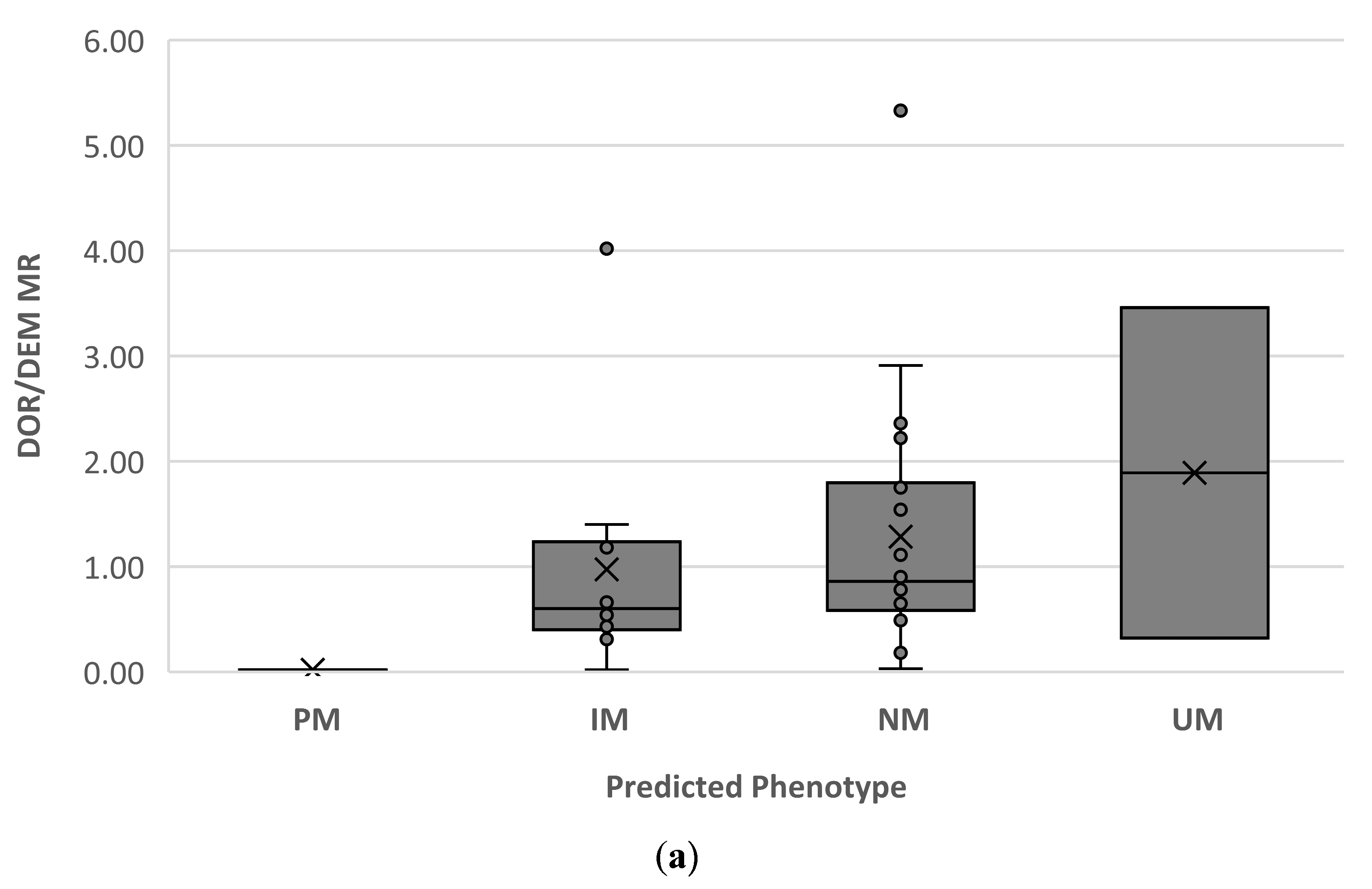
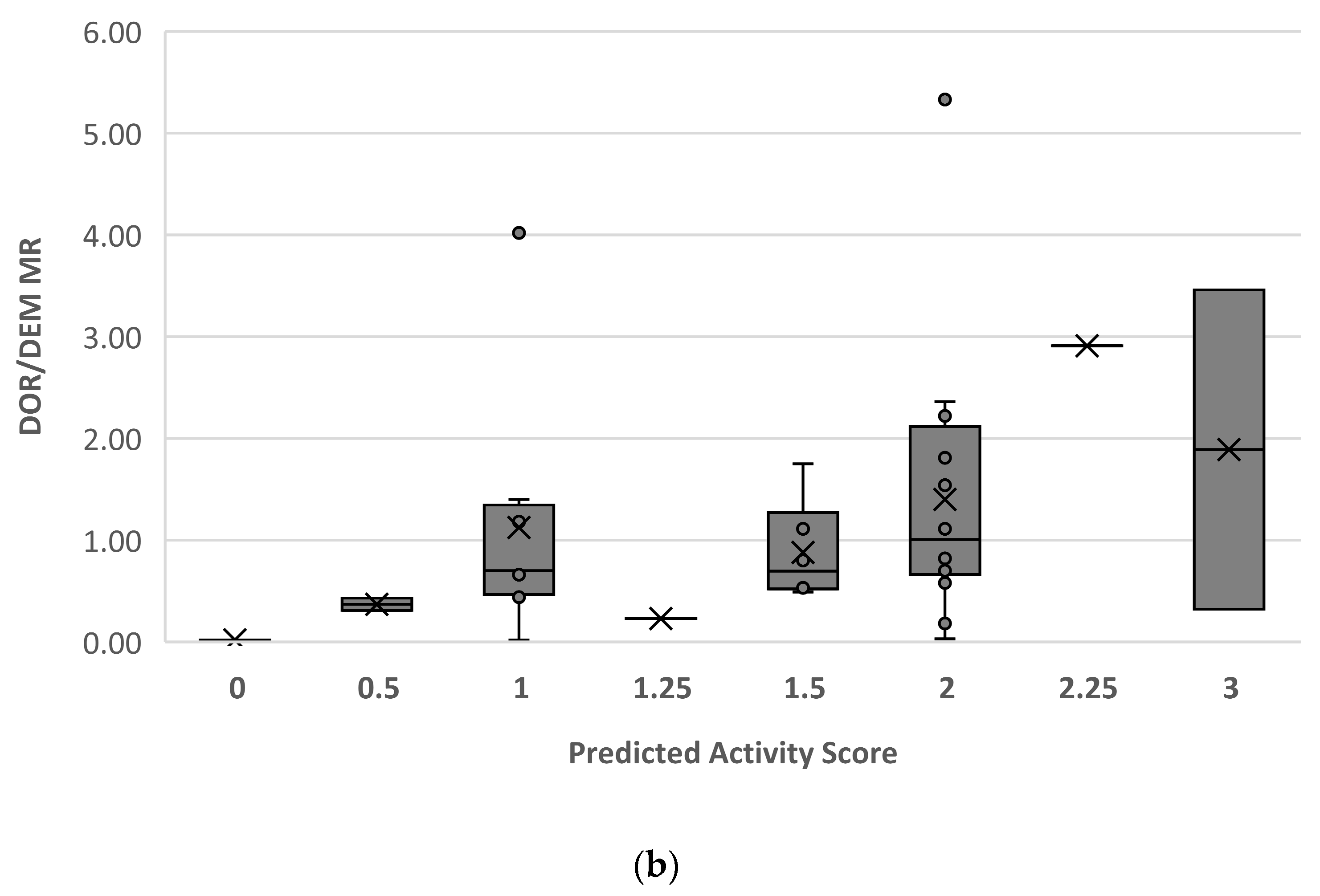
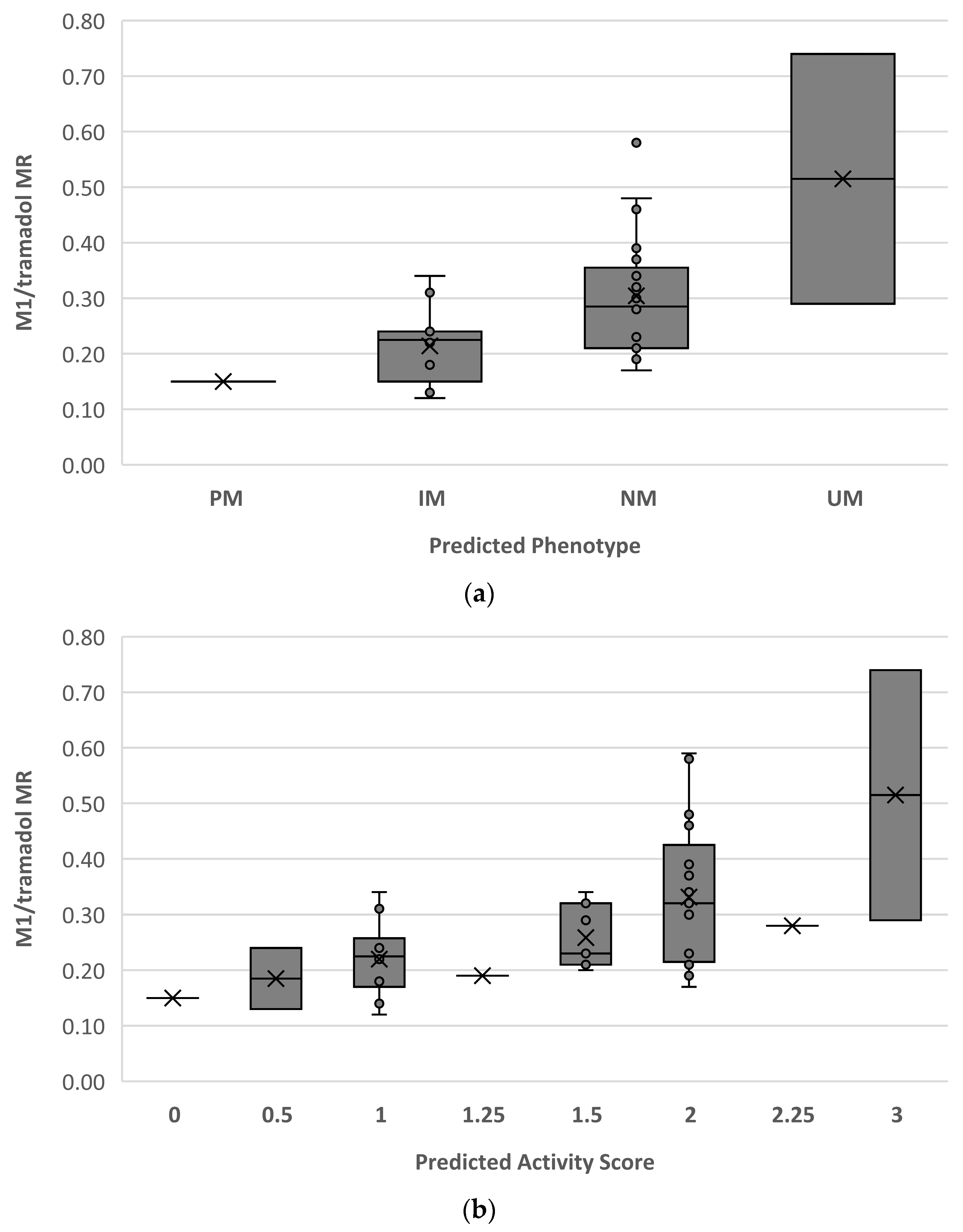
2.3. Correlation between DOR/DEM MR and AS
3. Discussion
4. Material and Methods
4.1. Trial Design
4.2. Intervention
4.3. Phenotyping
4.4. Genotyping
4.5. Pupillometry
4.6. Statistical Analysis
4.7. Assessment of Adverse Events
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CYP | Cytochrome P450 |
| M1 | O-desmethyltramadol |
| MR | Metabolic ratio |
| DEM | Dextromethorphan |
| DOR | Dextrorphan |
| PD | Pupil diameter |
| ER | Emergency room |
| NM | Normal metaboliser |
| PM | Poor metaboliser |
| IM | Intermediate metaboliser |
| UM | Ultrarapid metaboliser |
| CPIC | Clinical Pharmacogenetic Implementation Consortium |
| AS | Activity score |
| restPD | Initial resting PD |
| PLR | Pupillary light reflex |
| minPD | Minimum PD at peak of the constriction |
| CH | % Change |
| LAT | Latency of constriction |
| CV | Average constriction velocity |
| MCV | Maximum constriction velocity |
| DV | Dilation velocity |
| NPi | Neurological Pupil Index™ |
| RA | Reflex amplitude constriction |
| AE | Adverse event |
References
- Paar, W.D.; Poche, S.; Gerloff, J.; Dengler, H.J. Polymorphic CYP2D6 mediates O-demethylation of the opioid analgesic tramadol. Eur. J. Clin. Pharmacol. 1997, 53, 235–239. [Google Scholar] [CrossRef]
- Grond, S.; Sablotzki, A. Clinical pharmacology of tramadol. Clin. Pharmacokinet. 2004, 43, 879–923. [Google Scholar] [CrossRef] [PubMed]
- Gong, L.; Stamer, U.M.; Tzvetkov, M.V.; Altman, R.B.; Klein, T.E. PharmGKB summary: Tramadol pathway. Pharmacogenet. Genom. 2014, 24, 374–380. [Google Scholar] [CrossRef]
- Vandenbossche, J.; Richards, H.; Solanki, B.; Van Peer, A. Single- and multiple-dose pharmacokinetic studies of tramadol immediate-release tablets in children and adolescents. Clin. Pharmacol. Drug Dev. 2015, 4, 184–192. [Google Scholar] [CrossRef]
- Reeves, R.R.; Burke, R.S. Tramadol: Basic pharmacology and emerging concepts. Drugs Today 2008, 44, 827–836. [Google Scholar] [CrossRef]
- Scott, L.J.; Perry, C.M. Tramadol: A review of its use in perioperative pain. Drugs 2000, 60, 139–176. [Google Scholar] [CrossRef]
- Hui-Chen, L.; Yang, Y.; Na, W.; Ming, D.; Jian-Fang, L.; Hong-Yuan, X. Pharmacokinetics of the enantiomers of trans-tramadol and its active metabolite, trans-O-demethyltramadol, in healthy male and female chinese volunteers. Chirality 2004, 16, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Gillen, C.; Haurand, M.; Kobelt, D.J.; Wnendt, S. Affinity, potency and efficacy of tramadol and its metabolites at the cloned human mu-opioid receptor. Naunyn-Schmiedeberg’s Arch. Pharmacol. 2000, 362, 116–121. [Google Scholar] [CrossRef]
- Allegaert, K.; Holford, N.; Anderson, B.J.; Holford, S.; Stuber, F.; Rochette, A.; Troconiz, I.F.; Beier, H.; de Hoon, J.N.; Pedersen, R.S.; et al. Tramadol and o-desmethyl tramadol clearance maturation and disposition in humans: A pooled pharmacokinetic study. Clin. Pharmacokinet. 2015, 54, 167–178. [Google Scholar] [CrossRef]
- Allegaert, K.; Rochette, A.; Veyckemans, F. Developmental pharmacology of tramadol during infancy: Ontogeny, pharmacogenetics and elimination clearance. Paediatr. Anaesth. 2011, 21, 266–273. [Google Scholar] [CrossRef] [PubMed]
- Saudan, S.; Habre, W. Pharmacokinetics of tramadol in children. Ann. Fr. D’anesthesie Reanim. 2007, 26, 560–563. [Google Scholar] [CrossRef]
- Veyckemans, F.; Pendeville, P.E. Tramadol for acute postoperative pain in children. Ann. Fr. D’anesthesie Reanim. 2007, 26, 564–569. [Google Scholar] [CrossRef] [PubMed]
- Ostadhadi, S.; Norouzi-Javidan, A.; Chamanara, M.; Akbarian, R.; Imran-Khan, M.; Ghasemi, M.; Dehpour, A.R. Involvement of NMDA receptors in the antidepressant-like effect of tramadol in the mouse forced swimming test. Brain Res. Bull 2017, 134, 136–141. [Google Scholar] [CrossRef]
- Hara, K.; Minami, K.; Sata, T. The effects of tramadol and its metabolite on glycine, gamma-aminobutyric acidA, and N-methyl-D-aspartate receptors expressed in Xenopus oocytes. Anesth. Analg. 2005, 100, 1400–1405. [Google Scholar] [CrossRef]
- Zahir, M.; Rashidian, A.; Hoseini, M.; Akbarian, R.; Chamanara, M. Pharmacological evidence for the possible involvement of the NMDA receptor pathway in the anticonvulsant effect of tramadol in mice. AIMS Neurosci. 2022, 9, 444–453. [Google Scholar] [CrossRef]
- Enggaard, T.P.; Poulsen, L.; Arendt-Nielsen, L.; Brøsen, K.; Ossig, J.; Sindrup, S.H. The analgesic effect of tramadol after intravenous injection in healthy volunteers in relation to CYP2D6. Anesth. Analg. 2006, 102, 146–150. [Google Scholar] [CrossRef] [PubMed]
- Kirchheiner, J.; Keulen, J.T.; Bauer, S.; Roots, I.; Brockmöller, J. Effects of the CYP2D6 gene duplication on the pharmacokinetics and pharmacodynamics of tramadol. J. Clin. Psychopharmacol. 2008, 28, 78–83. [Google Scholar] [CrossRef]
- Stamer, U.M.; Lehnen, K.; Höthker, F.; Bayerer, B.; Wolf, S.; Hoeft, A.; Stuber, F. Impact of CYP2D6 genotype on postoperative tramadol analgesia. Pain 2003, 105, 231–238. [Google Scholar] [CrossRef]
- Fulton, C.R.; Zang, Y.; Desta, Z.; Rosenman, M.B.; Holmes, A.M.; Decker, B.S.; Zhang, Y.; T Callaghan, J.; Pratt, V.M.; Levy, K.D.; et al. Drug-gene and drug-drug interactions associated with tramadol and codeine therapy in the INGENIOUS trial. Pharmacogenomics 2019, 20, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Bradford, L.D. CYP2D6 allele frequency in European Caucasians, Asians, Africans and their descendants. Pharmacogenomics 2002, 3, 229–243. [Google Scholar] [CrossRef]
- Ganoci, L.; Božina, T.; Mirošević Skvrce, N.; Lovrić, M.; Mas, P.; Božina, N. Genetic polymorphisms of cytochrome P450 enzymes: CYP2C9, CYP2C19, CYP2D6, CYP3A4, and CYP3A5 in the Croatian population. Drug Metab. Pers. Ther. 2017, 32, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Gaedigk, A.; Sangkuhl, K.; Whirl-Carrillo, M.; Klein, T.; Leeder, J.S. Prediction of CYP2D6 phenotype from genotype across world populations. Genet. Med. 2017, 19, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Dagostino, C.; Allegri, M.; Napolioni, V.; D’Agnelli, S.; Bignami, E.; Mutti, A.; van Schaik, R.H. CYP2D6 genotype can help to predict effectiveness and safety during opioid treatment for chronic low back pain: Results from a retrospective study in an Italian cohort. Pharmacogenom. Pers. Med. 2018, 11, 179–191. [Google Scholar] [CrossRef]
- Orliaguet, G.; Hamza, J.; Couloigner, V.; Denoyelle, F.; Loriot, M.A.; Broly, F.; Garabedian, E.N. A case of respiratory depression in a child with ultrarapid CYP2D6 metabolism after tramadol. Pediatrics 2015, 135, e753–e755. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.M.; Weitzel, K.W.; Cavallari, L.H.; Elsey, A.R.; Schmidt, S.O. Clinical application of pharmacogenetics in pain management. Pers. Med. 2018, 15, 117–126. [Google Scholar] [CrossRef]
- Crews, K.R.; Monte, A.A.; Huddart, R.; Caudle, K.E.; Kharasch, E.D.; Gaedigk, A.; Dunnenberger, H.M.; Leeder, J.S.; Callaghan, J.T.; Samer, C.F.; et al. Clinical Pharmacogenetics Implementation Consortium Guideline for CYP2D6, OPRM1, and COMT Genotypes and Select Opioid Therapy. Clin. Pharmacol. Ther. 2021, 110, 888–896. [Google Scholar] [CrossRef]
- Samer, C.F.; Lorenzini, K.I.; Rollason, V.; Daali, Y.; Desmeules, J.A. Applications of CYP450 testing in the clinical setting. Mol. Diagn. Ther. 2013, 17, 165–184. [Google Scholar] [CrossRef]
- Magliocco, G.; Rodieux, F.; Desmeules, J.; Samer, C.F.; Daali, Y. Toward precision medicine in pediatric population using cytochrome P450 phenotyping approaches and physiologically based pharmacokinetic modeling. Pediatr. Res. 2020, 87, 441–449. [Google Scholar] [CrossRef]
- Allegaert, K.; van den Anker, J. Ontogeny of Phase I Metabolism of Drugs. J. Clin. Pharmacol. 2019, 59 (Suppl. 1), S33–S41. [Google Scholar] [CrossRef]
- van den Anker, J.; Reed, M.D.; Allegaert, K.; Kearns, G.L. Developmental Changes in Pharmacokinetics and Pharmacodynamics. J. Clin. Pharmacol. 2018, 58 Suppl. 10, S10–S25. [Google Scholar] [CrossRef]
- Johnson, T.N.; Tucker, G.T.; Rostami-Hodjegan, A. Development of CYP2D6 and CYP3A4 in the first year of life. Clin. Pharmacol. Ther. 2008, 83, 670–671. [Google Scholar] [CrossRef] [PubMed]
- Lu, H.; Rosenbaum, S. Developmental pharmacokinetics in pediatric populations. J. Pediatr. Pharmacol. Ther. 2014, 19, 262–276. [Google Scholar] [CrossRef] [PubMed]
- Frank, D.; Jaehde, U.; Fuhr, U. Evaluation of probe drugs and pharmacokinetic metrics for CYP2D6 phenotyping. Eur. J. Clin. Pharmacol. 2007, 63, 321–333. [Google Scholar] [CrossRef]
- Bosilkovska, M.; Déglon, J.; Samer, C.; Walder, B.; Desmeules, J.; Staub, C.; Daali, Y. Simultaneous LC-MS/MS quantification of P-glycoprotein and cytochrome P450 probe substrates and their metabolites in DBS and plasma. Bioanalysis 2014, 6, 151–164. [Google Scholar] [CrossRef]
- Bosilkovska, M.; Samer, C.F.; Deglon, J.; Rebsamen, M.; Staub, C.; Dayer, P.; Walder, B.; Desmeules, J.A.; Daali, Y. Geneva cocktail for cytochrome p450 and P-glycoprotein activity assessment using dried blood spots. Clin. Pharmacol. Ther. 2014, 96, 349–359. [Google Scholar] [CrossRef]
- Klomp, S.D.; Manson, M.L.; Guchelaar, H.J.; Swen, J.J. Phenoconversion of Cytochrome P450 Metabolism: A Systematic Review. J. Clin. Med. 2020, 9, 2890. [Google Scholar] [CrossRef] [PubMed]
- Shah, R.R.; Smith, R.L. Addressing phenoconversion: The Achilles’ heel of personalized medicine. Br. J. Clin. Pharmacol. 2015, 79, 222–240. [Google Scholar] [CrossRef]
- Matouskova, O.; Slanar, O.; Chytil, L.; Perlik, F. Pupillometry in healthy volunteers as a biomarker of tramadol efficacy. J. Clin. Pharm. Ther. 2011, 36, 513–517. [Google Scholar] [CrossRef]
- Fliegert, F.; Kurth, B.; Göhler, K. The effects of tramadol on static and dynamic pupillometry in healthy subjects—The relationship between pharmacodynamics, pharmacokinetics and CYP2D6 metaboliser status. Eur. J. Clin. Pharmacol. 2005, 61, 257–266. [Google Scholar] [CrossRef] [PubMed]
- Slanar, O.; Nobilis, M.; Kvetina, J.; Idle, J.R.; Perlík, F. CYP2D6 polymorphism, tramadol pharmacokinetics and pupillary response. Eur. J. Clin. Pharmacol. 2006, 62, 75–76; author reply 77–78. [Google Scholar] [CrossRef]
- Kasthurirangan, S.; Glasser, A. Characteristics of pupil responses during far-to-near and near-to-far accommodation. Ophthalmic Physiol. Opt. J. Br. Coll. Ophthalmic Opt. Optom. 2005, 25, 328–339. [Google Scholar] [CrossRef]
- Larson, M.D.; Behrends, M. Portable infrared pupillometry: A review. Anesth. Analg. 2015, 120, 1242–1253. [Google Scholar] [CrossRef]
- Murray, R.B.; Adler, M.W.; Korczyn, A.D. The pupillary effects of opioids. Life Sci. 1983, 33, 495–509. [Google Scholar] [CrossRef]
- Henderson, R.R.; Bradley, M.M.; Lang, P.J. Emotional imagery and pupil diameter. Psychophysiology 2018, 55, e13050. [Google Scholar] [CrossRef] [PubMed]
- Winn, B.; Whitaker, D.; Elliott, D.B.; Phillips, N.J. Factors affecting light-adapted pupil size in normal human subjects. Investig. Ophthalmol. Vis. Sci. 1994, 35, 1132–1137. [Google Scholar]
- Tekin, K.; Sekeroglu, M.A.; Kiziltoprak, H.; Doguizi, S.; Inanc, M.; Yilmazbas, P. Static and dynamic pupillometry data of healthy individuals. Clin. Exp. Optom. 2018, 101, 659–665. [Google Scholar] [CrossRef]
- Connelly, M.A.; Brown, J.T.; Kearns, G.L.; Anderson, R.A.; St Peter, S.D.; Neville, K.A. Pupillometry: A non-invasive technique for pain assessment in paediatric patients. Arch. Dis. Child. 2014, 99, 1125–1131. [Google Scholar] [CrossRef]
- Bertrand, A.L.; Garcia, J.B.; Viera, E.B.; Santos, A.M.; Bertrand, R.H. Pupillometry: The influence of gender and anxiety on the pain response. Pain Physician 2013, 16, E257–E266. [Google Scholar]
- Rosen, E.S.; Gore, C.L.; Taylor, D.; Chitkara, D.; Howes, F.; Kowalewski, E. Use of a digital infrared pupillometer to assess patient suitability for refractive surgery. J. Cataract Refract Surg. 2002, 28, 1433–1438. [Google Scholar] [CrossRef] [PubMed]
- McKay, R.E.; Larson, M.D. Detection of opioid effect with pupillometry. Auton. Neurosci. Basic Clin. 2021, 235, 102869. [Google Scholar] [CrossRef]
- Pickworth, W.B.; Bunker, E.; Welch, P.; Cone, E. Intravenous buprenorphine reduces pupil size and the light reflex in humans. Life Sci. 1991, 49, 129–138. [Google Scholar] [CrossRef]
- Kongsgaard, U.E.; Høiseth, G. Dynamic assessment of the pupillary reflex in patients on high-dose opioids. Scand. J. Pain 2019, 19, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Larson, M.D.; Tayefeh, F.; Sessler, D.I.; Daniel, M.; Noorani, M. Sympathetic nervous system does not mediate reflex pupillary dilation during desflurane anesthesia. Anesthesiology 1996, 85, 748–754. [Google Scholar] [CrossRef]
- Knaggs, R.D.; Crighton, I.M.; Cobby, T.F.; Fletcher, A.J.; Hobbs, G.J. The pupillary effects of intravenous morphine, codeine, and tramadol in volunteers. Anesth. Analg. 2004, 99, 108–112. [Google Scholar]
- Pickworth, W.B.; Welch, P.; Henningfield, J.E.; Cone, E.J. Opiate-induced pupillary effects in humans. Methods Find. Exp. Clin. Pharmacol. 1989, 11, 759–763. [Google Scholar]
- Peacock, J.E.; Henderson, P.D.; Nimmo, W.S. Changes in pupil diameter after oral administration of codeine. Br. J. Anaesth. 1988, 61, 598–600. [Google Scholar] [CrossRef] [PubMed]
- Yanarates, O.; Dogrul, A.; Yildirim, V.; Sahin, A.; Sizlan, A.; Seyrek, M.; Akgül, O.; Kozak, O.; Kurt, E.; Aypar, U. Spinal 5-HT7 receptors play an important role in the antinociceptive and antihyperalgesic effects of tramadol and its metabolite, O-Desmethyltramadol, via activation of descending serotonergic pathways. Anesthesiology 2010, 112, 696–710. [Google Scholar] [CrossRef]
- Barvais, L.; Engelman, E.; Eba, J.M.; Coussaert, E.; Cantraine, F.; Kenny, G.N. Effect site concentrations of remifentanil and pupil response to noxious stimulation. Br. J. Anaesth. 2003, 91, 347–352. [Google Scholar] [CrossRef]
- Pickworth, W.B.; Lee, H.; Fudala, P.J. Buprenorphine-induced pupillary effects in human volunteers. Life Sci. 1990, 47, 1269–1277. [Google Scholar] [CrossRef] [PubMed]
- Halfpenny, D.M.; Callado, L.F.; Hopwood, S.E.; Bamigbade, T.A.; Langford, R.M.; Stamford, J.A. Effects of tramadol stereoisomers on norepinephrine efflux and uptake in the rat locus coeruleus measured by real time voltammetry. Br. J. Anaesth. 1999, 83, 909–915. [Google Scholar] [CrossRef]
- Gloor, Y.; Lloret-Linares, C.; Bosilkovska, M.; Perroud, N.; Richard-Lepouriel, H.; Aubry, J.M.; Daali, Y.; Desmeules, J.A.; Besson, M. Drug metabolic enzyme genotype-phenotype discrepancy: High phenoconversion rate in patients treated with antidepressants. Biomed. Pharmacother. 2022, 152, 113202. [Google Scholar] [CrossRef] [PubMed]
- Caudle, K.E.; Sangkuhl, K.; Whirl-Carrillo, M.; Swen, J.J.; Haidar, C.E.; Klein, T.E.; Gammal, R.S.; Relling, M.V.; Scott, S.A.; Hertz, D.L.; et al. Standardizing CYP2D6 Genotype to Phenotype Translation: Consensus Recommendations from the Clinical Pharmacogenetics Implementation Consortium and Dutch Pharmacogenetics Working Group. Clin. Transl. Sci. 2020, 13, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Jasinski, D.R. Abuse potential of morphine/dextromethorphan combinations. J. Pain Symptom Manag. 2000, 19, S26–S30. [Google Scholar] [CrossRef]
- Martin, E.; Narjoz, C.; Decleves, X.; Labat, L.; Lambert, C.; Loriot, M.A.; Ducheix, G.; Dualé, C.; Pereira, B.; Pickering, G. Dextromethorphan Analgesia in a Human Experimental Model of Hyperalgesia. Anesthesiology 2019, 131, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Rodieux, F.; Daali, Y.; Rollason, V.; Samer, C.F.; Ing Lorenzini, K. Practice of CYP450 genotyping and phenotyping in children in a real-life setting. Front. Pharmacol. 2023, 14, 1130100. [Google Scholar] [CrossRef]
- Rebsamen, M.C.; Desmeules, J.; Daali, Y.; Chiappe, A.; Diemand, A.; Rey, C.; Chabert, J.; Dayer, P.; Hochstrasser, D.; Rossier, M.F. The AmpliChip CYP450 test: Cytochrome P450 2D6 genotype assessment and phenotype prediction. Pharmacogenom. J. 2009, 9, 34–41. [Google Scholar] [CrossRef]
- Kaur, G.; Smyth, R.L.; Powell, C.V.; Williamson, P. A survey of facilitators and barriers to recruitment to the MAGNETIC trial. Trials 2016, 17, 607. [Google Scholar] [CrossRef]
- Patterson, C.A.; Chavez, V.; Mondestin, V.; Deatrick, J.; Li, Y.; Barakat, L.P. Clinical Trial Decision Making in Pediatric Sickle Cell Disease: A Qualitative Study of Perceived Benefits and Barriers to Participation. J. Pediatr. Hematol. Oncol. 2015, 37, 415–422. [Google Scholar] [CrossRef]
- Watson, S.E.; Smith, P.; Snowden, J.; Vaughn, V.; Cottrell, L.; Madden, C.A.; Kong, A.S.; McCulloh, R.; Stack Lim, C.; Bledsoe, M.; et al. Facilitators and barriers to pediatric clinical trial recruitment and retention in rural and community settings: A scoping review of the literature. Clin. Transl. Sci. 2022, 15, 838–853. [Google Scholar] [CrossRef]
- Barakat, L.P.; Patterson, C.A.; Mondestin, V.; Chavez, V.; Austin, T.; Robinson, M.R.; Li, Y.; Smith-Whitley, K.; Cohen, R. Initial development of a questionnaire evaluating perceived benefits and barriers to pediatric clinical trials participation. Contemp. Clin. Trials 2013, 34, 218–226. [Google Scholar] [CrossRef]
- Denhoff, E.R.; Milliren, C.E.; de Ferranti, S.D.; Steltz, S.K.; Osganian, S.K. Factors Associated with Clinical Research Recruitment in a Pediatric Academic Medical Center—A Web-Based Survey. PLoS ONE 2015, 10, e0140768. [Google Scholar] [CrossRef]
- Jerdi, M.C.; Daali, Y.; Oestreicher, M.K.; Cherkaoui, S.; Dayer, P. A simplified analytical method for a phenotyping cocktail of major CYP450 biotransformation routes. J. Pharm. Biomed. Anal. 2004, 35, 1203–1212. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.T.; Connelly, M.; Nickols, C.; Neville, K.A. Developmental Changes of Normal Pupil Size and Reactivity in Children. J. Pediatr. Ophthalmol. Strabismus 2015, 52, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Taylor, W.R.; Chen, J.W.; Meltzer, H.; Gennarelli, T.A.; Kelbch, C.; Knowlton, S.; Richardson, J.; Lutch, M.J.; Farin, A.; Hults, K.N.; et al. Quantitative pupillometry, a new technology: Normative data and preliminary observations in patients with acute head injury. Technical note. J. Neurosurg. 2003, 98, 205–213. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of individuals (n total = 41) | |
| - Female | 15 |
| - Male | 26 |
| Age (years) | 11 (3–15) |
| Weight (kg) | 48.1 (17–103) |
| Source of pain | |
| - Traumatic | 26 |
| - Non-traumatic | 15 |
| Predicted Metabolic Phenotype Numbers of Individual (%) | PM 1 (2.4) | IM 12 (29.3) | NM 26 (63.4) | UM 2 (4.9) | ||||
|---|---|---|---|---|---|---|---|---|
| Assigned AS Numbers of individual (%) | 0 1 (2.4) | 0.5 2 (4.9) | 1.0 10 (24.4) | 1.25 1 (2.4) | 1.5 7 (17.1) | 2.0 17 (41.5) | 2.25 1 (2.4) | 3 2 (4.9) |
| Genotype; CYP2D6 diplotype | *4/*4 | *4/*41; *10/*10; | *1/*4; *2/*6; *1/*6; *1/*4 × N; *2/*5; *4j/*35 | *1/*10 | *1/*41 *1/*17 *2/*41 *2/*9 *1/*9 | *1/*1 *1/*35 *1/*41 × N *1/*2 *2/*2 | *1 × 2/*10 | *2/*35 × N *2/*2 × N |
| Dependent Variable: Delta RestPD between T0 and T150 (mm) | |||||
|---|---|---|---|---|---|
| a. | Independent Variables | B | 95% CI | p | |
| DOR/DEM MR | 0.127 | [−0.123, 0.378] | 0.308 | (n = 34) (R2 = 0.252, p = 0.011 *). | |
| Mean lux | 0.003 | [0.001, 0.005] | 0.003 ** | ||
| b. | Independent variables | B | 95% CI | p | |
| M1/tramadol MR | −0.033 | [−2.223, 2.160] | 0.976 | (n = 37) (R2 = 0.232, p = 0.011 *). | |
| Mean lux | 0.003 | [0.001, 0.004] | 0.003 ** | ||
| c. | Independent variables | B | 95% CI | p | |
| M1 concentration (LN) | −0.243 | [−0.659, 0.172] | 0.243 | (n = 37) (R2 = 0.263, p = 0.006 **). | |
| Mean lux | 0.003 | [0.001, 0.004] | 0.003 ** | ||
| Dependent Variable Delta RA between T0 and T150 (mm). | ||||
|---|---|---|---|---|
| Variable | B | 95% CI | p | |
| M1 concentration (LN) | −0.140 | [−0.407, 0.127] | 0.293 | |
| Mean lux | 0.001 | [0.000, 0.003] | 0.007 ** | (n = 37) (R2 = 0.229, p = 0.012 *). |
| Predicted Phenotype Based on Genotype | Measured Phenotype (DOR/DEM MR) | ||||
|---|---|---|---|---|---|
| PM (%) a | IM (%) a | NM (%) a | UM (%) a | ||
| PM | 1 | 1 (100%) | 0 | 0 | 0 |
| IM | 10 | 1 | 6 (60%) | 3 | 0 |
| NM | 24 | 1 | 8 | 14 (58%) | 1 |
| UM | 2 | 0 | 1 | 1 | 0 (0%) |
| Predicted Phenotype | Activity Score Range | Activity Score/Genotypes | Considered Diplotypes |
|---|---|---|---|
| CYP2D6 ultrarapid metaboliser (UM) | >2.25 | >2.25 | *1/*2 × N, *2/*35 × N |
| CYP2D6 normal metaboliser (NM) | 1.25 ≤ × ≤ 2.25 | 1.25 1.5 1.75 2.0 2.25 | *1/*10 *1/*41, *1/*17, *2/*41, *2/*9 - *1/*1, *1/*35, *1/*41 × N, *1/*2, *2/*2 *1 × 2/*10 |
| CYP2D6 intermediate metaboliser (IM) | 0 < × < 1.25 | 0.25 0.5 0.75 1 | - *4/*41, *10/*10 - *1/*4, *2/*6, *1/*6, *1/*4 × N, *2/*5, *4j/*35 |
| CYP2D6 poor metaboliser (PM) | 0 | 0 | *4/*4 |
| Static | Initial Resting Pupil Diameter = RestPD | Maximum Pupil Size before Constriction |
|---|---|---|
| Dynamic | CH = % Change | % of change = minPD/restPD as a % |
| minPD = minimum pupil diameter | PD at peak of the constriction | |
| LAT = latency of constriction | Time of onset of constriction following initiation of the light stimulus | |
| CV = average constriction velocity | Average of how fast the PD is constricting, measured in millimetres per second | |
| MCV = maximum constriction velocity | Maximum velocity of pupil constriction of the PD responding to the flash of light, measured in millimetres per second | |
| DV = dilation velocity | The average pupillary velocity when, after having reached the peak of constriction, the pupil tends to recover and to dilate back to the initial size, measured in millimetres per second | |
| NPi® = Neurological Pupil Index™ | Numerical expression of pupil reactivity |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodieux, F.; Storelli, F.; Curtin, F.; Manzano, S.; Gervaix, A.; Posfay-Barbe, K.M.; Desmeules, J.; Daali, Y.; Samer, C.F. Evaluation of Pupillometry for CYP2D6 Phenotyping in Children Treated with Tramadol. Pharmaceuticals 2023, 16, 1227. https://doi.org/10.3390/ph16091227
Rodieux F, Storelli F, Curtin F, Manzano S, Gervaix A, Posfay-Barbe KM, Desmeules J, Daali Y, Samer CF. Evaluation of Pupillometry for CYP2D6 Phenotyping in Children Treated with Tramadol. Pharmaceuticals. 2023; 16(9):1227. https://doi.org/10.3390/ph16091227
Chicago/Turabian StyleRodieux, Frédérique, Flavia Storelli, François Curtin, Sergio Manzano, Alain Gervaix, Klara M. Posfay-Barbe, Jules Desmeules, Youssef Daali, and Caroline F. Samer. 2023. "Evaluation of Pupillometry for CYP2D6 Phenotyping in Children Treated with Tramadol" Pharmaceuticals 16, no. 9: 1227. https://doi.org/10.3390/ph16091227