
Innovative Delivery and Release Systems for Antioxidants and Other Active Substances in the Treatment of Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Reactive Oxygen Species in Cancer
3. Antioxidant-Loaded Delivery Systems as Emerging Therapeutic Strategies against Cancer Diseases
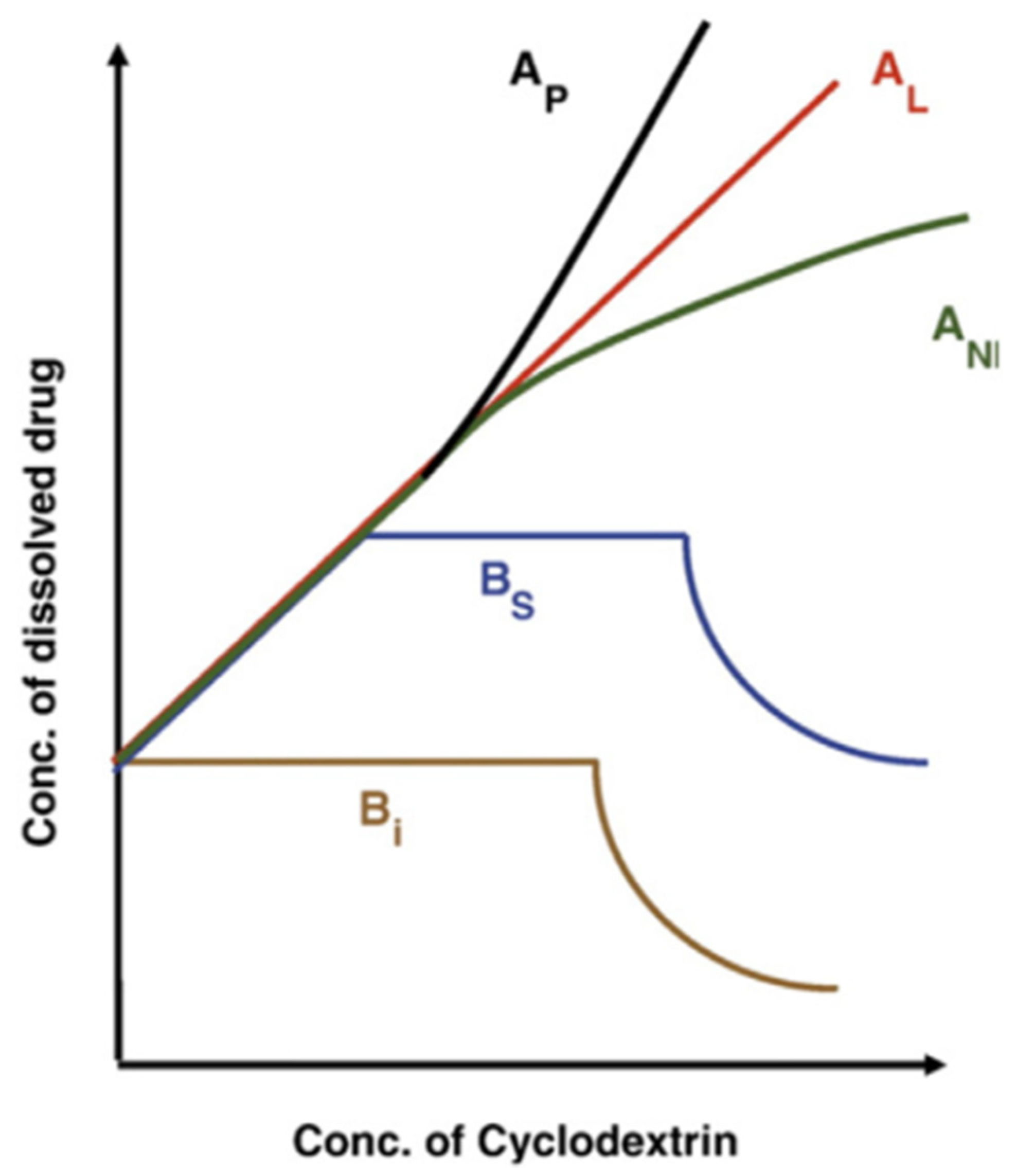
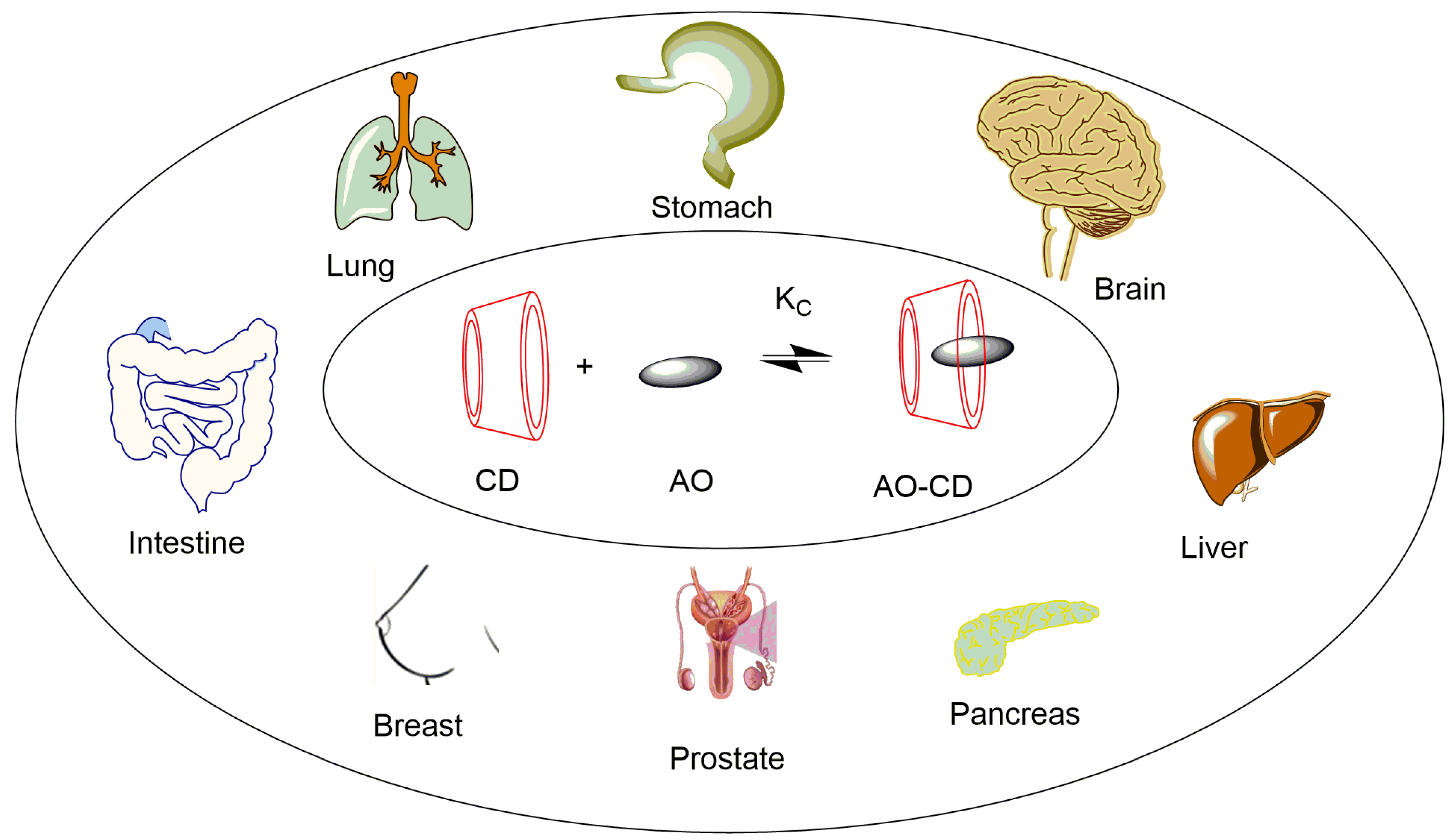
3.1. Cyclodextrins as Delivery Systems of Antioxidants (AOs) with Anticancer Properties
Antioxidants Are Commonly Employed for Effective Cancer Prevention and Therapy
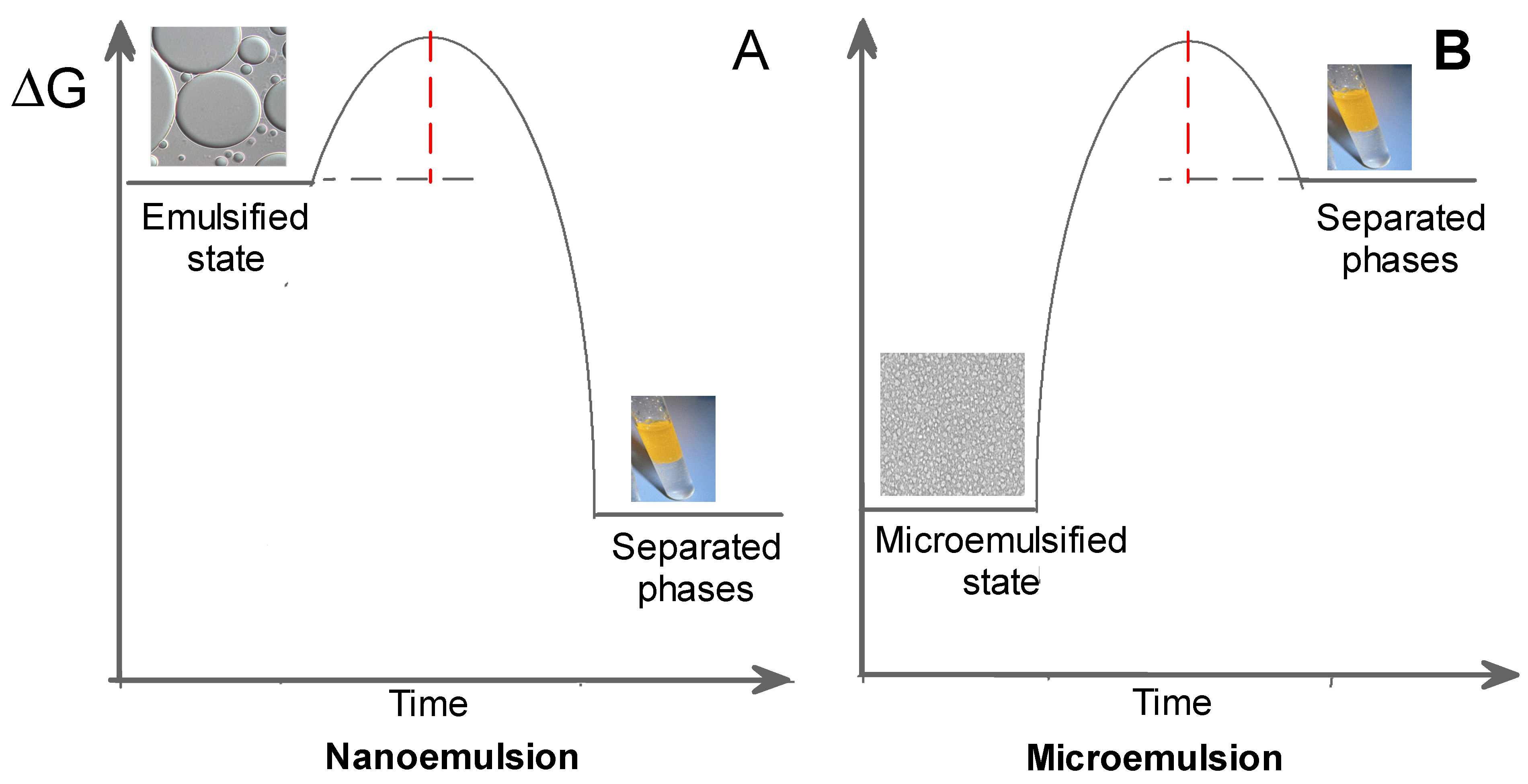
3.2. Microemulsion/Nanoemulsion as Delivery Systems of Antioxidants with Anticancer Properties
- -
- Improvement of the thermodynamic stability of antioxidants;
- -
- Better solubility of lipophilic antioxidants;
- -
- Masking of undesirable tastes;
- -
- Improvement of the bioavailability and biodegradability of antioxidants;
- -
- Reduction in the toxicity of antioxidants;
- -
- Enhancement of the drug release profile.
Some Antioxidant-Loaded Nanoemulsions Employed in Cancer Diseases
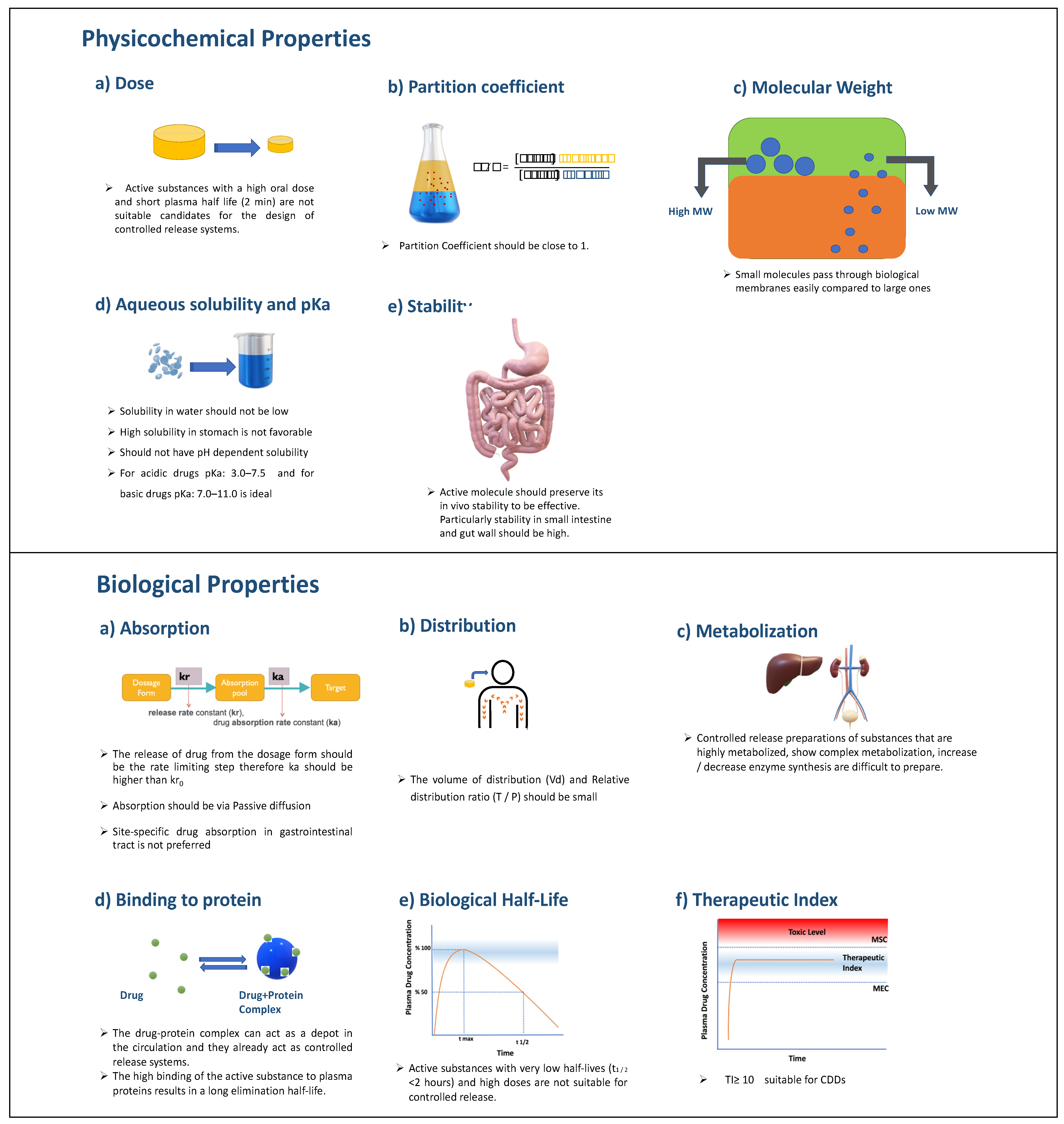
4. Controlled Drug Delivery Systems
4.1. Development of Controlled Drug Delivery Systems
4.2. Polymers for Controlled Drug Delivery
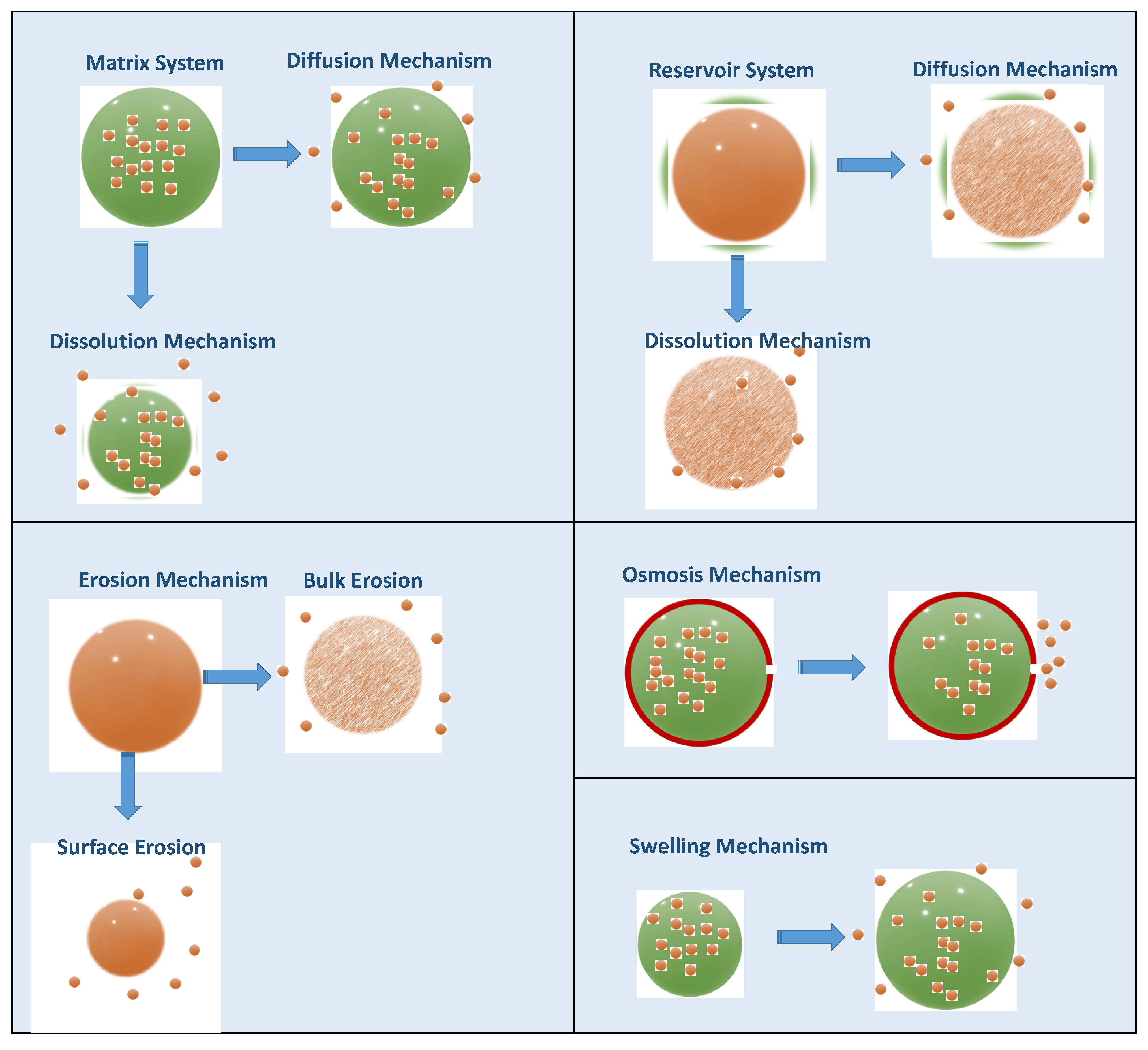
4.3. Mechanisms of Drug Release from CDDS
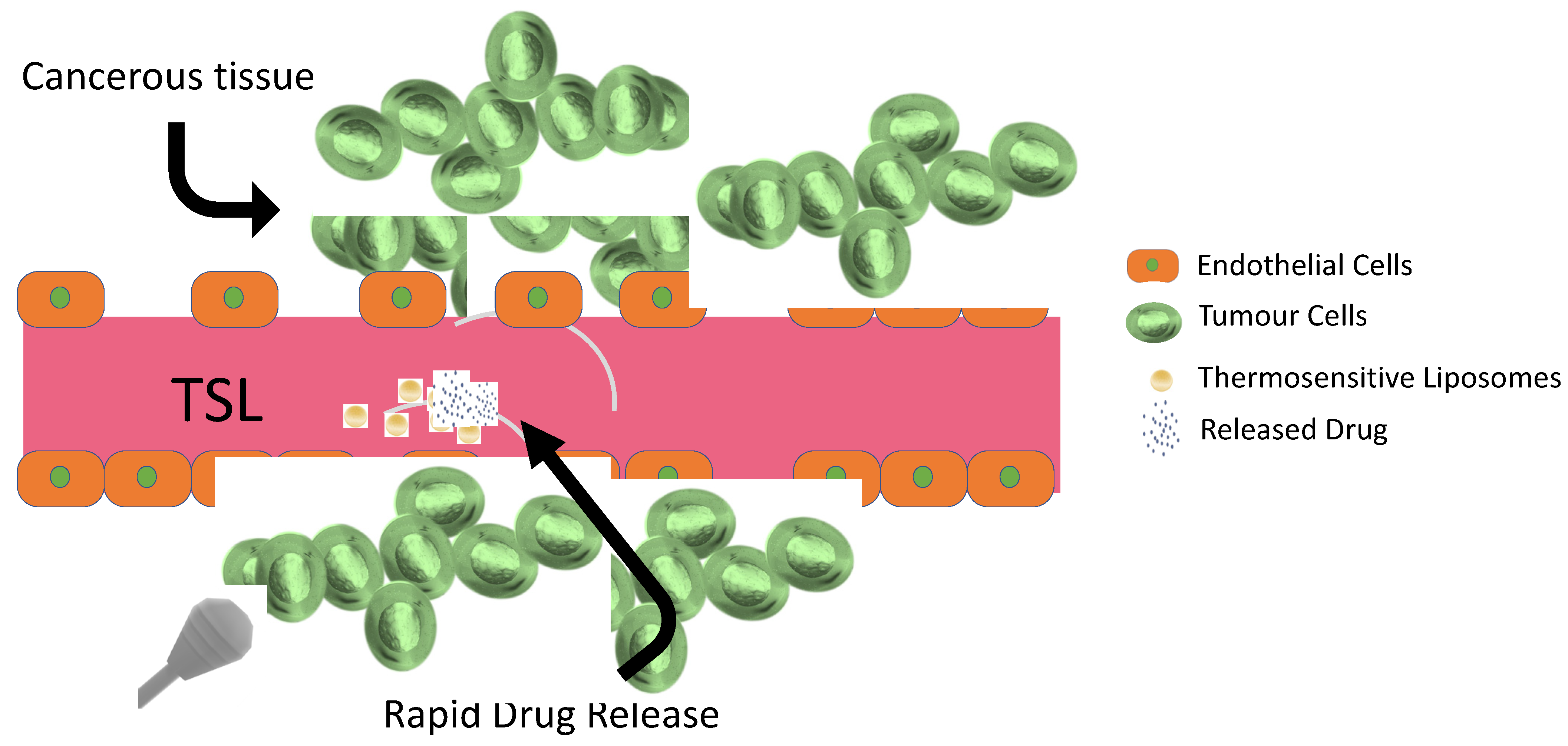
4.4. Thermosensitive Smart Liposomes for Cancer Chemotherapy
4.4.1. Hyperthermia and Cancer
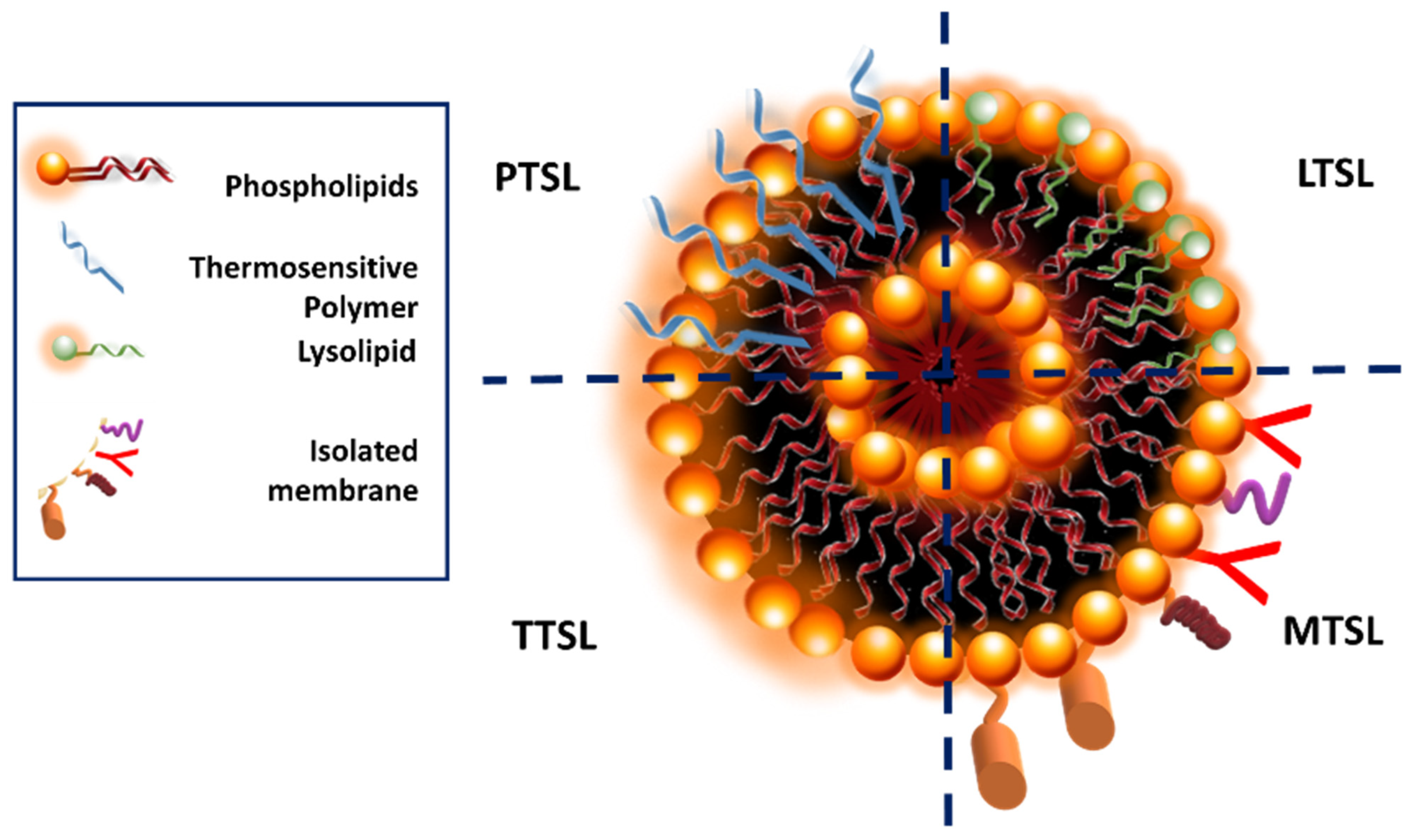
4.4.2. Thermosensitive Smart Liposomes as Drug Carriers
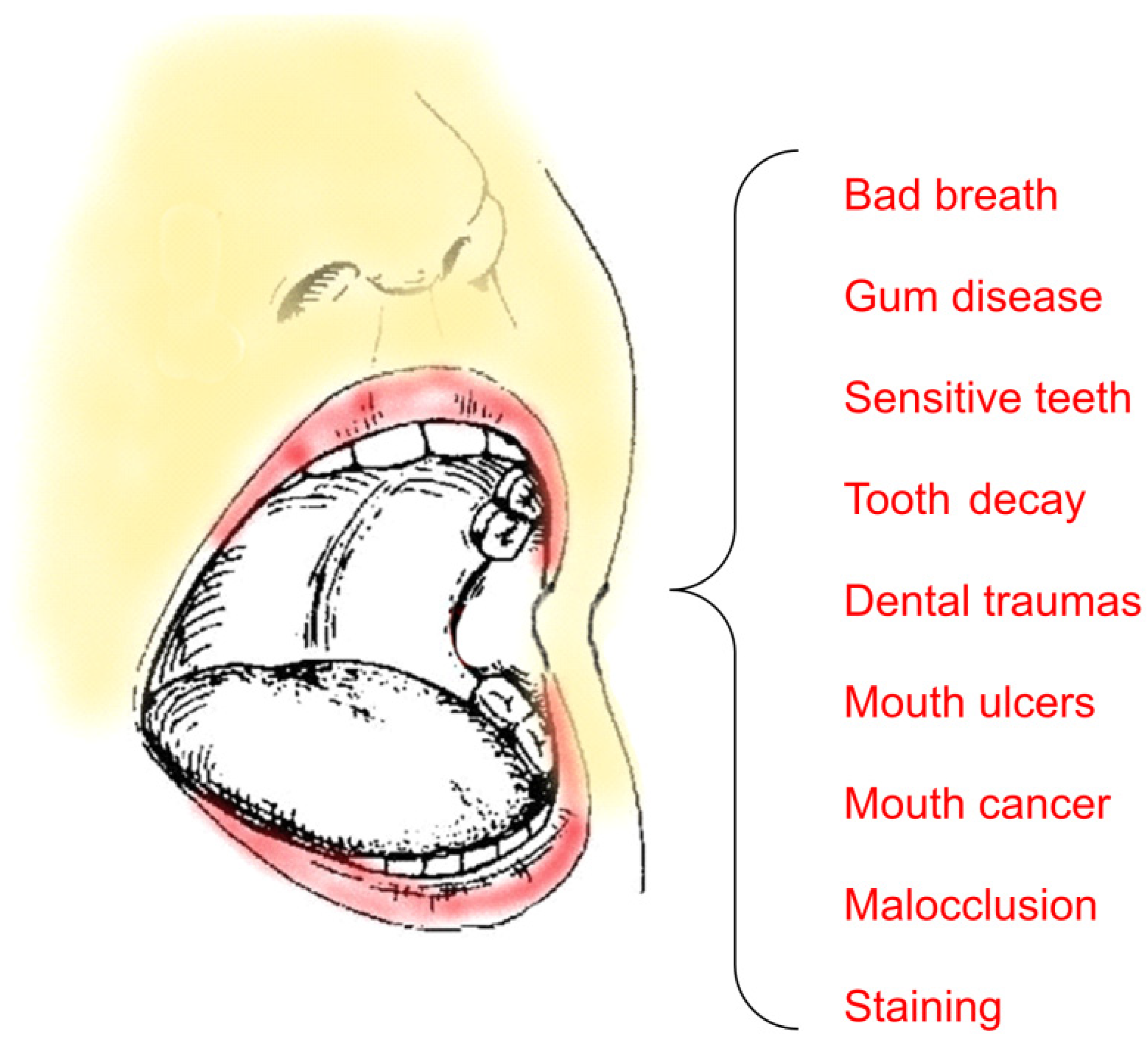
5. Case Study: Delivery Systems for Oral Cancer and Associated Diseases
6. Conclusions and Final Remarks
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Metwaly, A.M.; Ghoneim, M.M.; Eissa, I.H.; Elsehemy, I.A.; Mostafa, A.E.; Hegazy, M.M.; Afifi, W.M.; Dou, D. Traditional ancient Egyptian medicine: A review. Saudi J. Biol. Sci. 2021, 28, 5823–5832. [Google Scholar] [CrossRef] [PubMed]
- Al-Shura, A.N. 1-Traditional Chinese Medicine. In Herbal, Bio-Nutrient and Drug Titration According to Disease Stages in Integrative Cardiovascular Chinese Medicine; Al-Shura, A.N., Ed.; Academic Press: Cambridge, MA, USA, 2020; pp. 1–18. [Google Scholar]
- Dias, D.A.; Urban, S.; Roessner, U. A historical overview of natural products in drug discovery. Metabolites 2012, 2, 303–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bandopadhyay, S.; Manchanda, S.; Chandra, A.; Ali, J.; Deb, P.K. Chapter 5-Overview of different carrier systems for advanced drug delivery. In Drug Delivery Systems; Tekade, R.K., Ed.; Academic Press: Cambridge, MA, USA, 2020; pp. 179–233. [Google Scholar]
- Keservani, R.K.; Bandopadhyay, S.; Bandyopadhyay, N.; Sharma, A.K. Chapter 4-Design and fabrication of transdermal/skin drug-delivery system. In Drug Delivery Systems; Tekade, R.K., Ed.; Academic Press: Cambridge, MA, USA, 2020; pp. 131–178. [Google Scholar]
- Jain, K.K. An Overview of Drug Delivery Systems. In Drug Delivery Systems; Jain, K.K., Ed.; Springer: New York, NY, USA, 2020; pp. 1–54. [Google Scholar]
- Luo, M.; Zhou, L.; Huang, Z.; Li, B.; Nice, E.C.; Xu, J.; Huang, C. Antioxidant Therapy in Cancer: Rationale and Progress. Antioxidants 2022, 11, 1128. [Google Scholar] [CrossRef] [PubMed]
- Virág, L.; Jaén, R.I.; Regdon, Z.; Boscá, L.; Prieto, P. Self-defense of macrophages against oxidative injury: Fighting for their own survival. Redox Biol. 2019, 26, 101261. [Google Scholar] [CrossRef]
- Caserta, S.; Ghezzi, P. Release of redox enzymes and micro-RNAs in extracellular vesicles, during infection and inflammation. Free. Radic. Biol. Med. 2021, 169, 248–257. [Google Scholar] [CrossRef]
- Chaiswing, L.; St Clair, W.H.; St Clair, D.K. Redox Paradox: A Novel Approach to Therapeutics-Resistant Cancer. Antioxid. Redox Signal. 2018, 29, 1237–1272. [Google Scholar] [CrossRef] [PubMed]
- Urso, L.; Cavallari, I.; Sharova, E.; Ciccarese, F.; Pasello, G.; Ciminale, V. Metabolic rewiring and redox alterations in malignant pleural mesothelioma. Br. J. Cancer 2020, 122, 52–61. [Google Scholar] [CrossRef]
- Costa, M.; Sezgin-Bayindir, Z.; Losada-Barreiro, S.; Paiva-Martins, F.; Saso, L.; Bravo-Díaz, C. Polyphenols as Antioxidants for Extending Food Shelf-Life and in the Prevention of Health Diseases: Encapsulation and Interfacial Phenomena. Biomedicines 2021, 9, 1909. [Google Scholar] [CrossRef]
- Sezgin-Bayindir, Z.; Losada-Barreiro, S.; Bravo-Díaz, C.; Sova, M.; Kristl, J.; Saso, L. Nanotechnology-Based Drug Delivery to Improve the Therapeutic Benefits of NRF2 Modulators in Cancer Therapy. Antioxidants 2021, 10, 685. [Google Scholar] [CrossRef]
- Losada-Barreiro, S.; Bravo-Díaz, C. Free radicals and polyphenols: The redox chemistry of neurodegenerative diseases. Eur. J. Med. Chem. 2017, 133, 379–402. [Google Scholar] [CrossRef]
- Losada-Barreiro, S.; Bravo-Díaz, C.; Paiva-Martins, F. Why encapsulate antioxidants in emulsion-based systems, where they are located, and how location affects their efficiency. In Emulsion-Based Encapsulation of Antioxidants; Aboudzadeh, M.A., Ed.; Food Bioactive Ingredients; Springer Nature: Cham, Switzerland, 2021. [Google Scholar]
- Mansour, A.; Romani, M.; Acharya, A.B.; Rahman, B.; Verron, E. Drug Delivery Systems in Regenerative Medicine: An Updated Review. Pharmaceutics 2023, 15, 695. [Google Scholar] [CrossRef]
- Sivadasan, D.; Sultan, M.H.; Alqahtani, S.S.; Javed, S. Cubosomes in Drug Delivery—A Comprehensive Review on Its Structural Components, Preparation Techniques and Therapeutic Applications. Biomedicines 2023, 11, 1114. [Google Scholar]
- Vargason, A.M.; Anselmo, A.C. The evolution of commercial drug delivery technologies. Nat. Biomed. Eng. 2021, 5, 951–967. [Google Scholar] [CrossRef]
- Pingale, P.; Kendre, P.; Pardeshi, K.; Rajput, A. An emerging era in manufacturing of drug delivery systems: Nanofabrication techniques. Heliyon 2023, 9, e14247. [Google Scholar] [CrossRef] [PubMed]
- Chien, Y.W. Rate-control drug delivery systems: Controlled release vs. sustained release. Med. Prog. Through Technol. 1989, 15, 21–46. [Google Scholar]
- Adepu, S.; Ramakrishna, S. Controlled Drug Delivery Systems: Current Status and Future Directions. Molecules 2021, 26, 5905. [Google Scholar] [CrossRef]
- Luo, Y.; De Souza, C.; Ramachandran, M.; Wang, S.; Yi, H.; Ma, Z.; Zhang, L.; Lin, K. Precise oral delivery systems for probiotics: A review. J. Control. Release 2022, 352, 371–384. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, H.; Takada, K. Reactive oxygen species in cancer: Current findings and future directions. Cancer Sci. 2021, 112, 3945–3952. [Google Scholar] [CrossRef]
- Augusto, O.; Miyamoto, S. Oxygen Radicals and Related Species. In Free Radical Biomedicine; Pantopoulos, K., Schipper, H.M., Eds.; Nova Science Pub. Inc.: New York, NY, USA, 2011; Volume 1. [Google Scholar]
- Krumova, K.; Cosa, G. Overview of Reactive Oxygen Species. In Singlet Oxygen: Applications in Biosciences and Nanosciences; Nonell, S., Flors, C., Eds.; Royal Society of Chemistry: London, UK, 2016. [Google Scholar]
- Wood, P.M. The potential diagram for oxygen at pH 7. Biochem. J. 1988, 253, 287–289. [Google Scholar] [CrossRef]
- Buettner, G.R. The pecking order of free radicals and antioxidants: Lipid peroxidation, alpha-tocopherol, and ascorbate. Arch. Biochem. Biophys. 1993, 300, 535–543. [Google Scholar] [CrossRef] [PubMed]
- Steenken, S.; Neta, P. Transient Phenoxyl Radicals: Formation and Properties in Aqueous Solutions. In PATAI’S Chemistry of Functional Groups; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2009. [Google Scholar]
- Ben Mrid, R.; Bouchmaa, N.; Ouedrhiri, W.; Ennoury, A.; Zouaou, I.Z.; Kabach, I.; Nhiri, M.; El Fatimy, R. Synergistic antioxidant effects of natural compounds on H2O2-induced cytotoxicity of human monocytes. Front. Pharm. 2022, 13, 830323. [Google Scholar] [CrossRef]
- Allen, T.M.; Cullis, P.R. Drug delivery systems: Entering the mainstream. Science 2004, 303, 1818–1822. [Google Scholar] [CrossRef] [Green Version]
- Capecchi, E.; Piccinino, D.; Nascimben, C.; Tomaino, E.; Vlas, N.C.; Gabellone, S.; Saladino, R. Biosynthesis of Novel Ascorbic Acid Esters and Their Encapsulation in Lignin Nanoparticles as Carriers and Stabilizing Systems. Int. J. Mol. Sci. 2023, 24, 9044. [Google Scholar] [CrossRef] [PubMed]
- Lorscheider, M.; Gaudin, A.; Nakhlé, J.; Veiman, K.L.; Richard, J.; Chassaing, C. Challenges and opportunities in the delivery of cancer therapeutics: Update on recent progress. Ther. Deliv. 2021, 12, 55–76. [Google Scholar] [CrossRef] [PubMed]
- Liu, G.; Yang, L.; Chen, G.; Xu, F.; Yang, F.; Yu, H.; Li, L.; Dong, X.; Han, J.; Cao, C.; et al. A Review on Drug Delivery System for Tumor Therapy. Front. Pharm. 2021, 12, 735446. [Google Scholar] [CrossRef] [PubMed]
- Tayeb, H.H.; Sainsbury, F. Nanoemulsions in drug delivery: Formulation to medical application. Nanomedicine 2018, 13, 2507–2525. [Google Scholar] [CrossRef]
- Ohnuma, T.; Matsumoto, T.; Itoi, A.; Kawana, A.; Nishiyama, T.; Ogura, K.; Hiratsuka, A. Enhanced sensitivity of A549 cells to the cytotoxic action of anticancer drugs via suppression of Nrf2 by procyanidins from Cinnamomi Cortex extract. Biochem. Biophys. Res. Commun. 2011, 413, 623–629. [Google Scholar] [CrossRef]
- Chian, S.; Thapa, R.; Chi, Z.; Wang, X.J.; Tang, X. Luteolin inhibits the Nrf2 signaling pathway and tumor growth in vivo. Biochem. Biophys. Res. Commun. 2014, 447, 602–608. [Google Scholar] [CrossRef]
- Foygel, K.; Sekar, T.V.; Paulmurugan, R. Monitoring the Antioxidant Mediated Chemosensitization and ARE-Signaling in Triple Negative Breast Cancer Therapy. PLoS ONE 2015, 10, e0141913. [Google Scholar] [CrossRef] [Green Version]
- Panieri, E.; Buha, A.; Telkoparan-Akillilar, P.; Cevik, D.; Kouretas, D.; Veskoukis, A.; Skaperda, Z.; Tsatsakis, A.; Wallace, D.; Suzen, S.; et al. Potential Applications of NRF2 Modulators in Cancer Therapy. Antioxidants 2020, 9, 193. [Google Scholar] [CrossRef] [Green Version]
- Szejtli, J. Cyclodextrin Technology; Springer: Dordrecht, The Netherlands, 1988. [Google Scholar]
- Higuchi, T.; Connors, K.A. Phase-Solubility Techniques. Adv. Anal. 1965, 4, 117–212. [Google Scholar]
- Martínez-Alonso, A.; Losada-Barreiro, S.; Bravo-Díaz, C. Encapsulation and solubilization of the antioxidants gallic acid and ethyl, propyl and butyl gallate with β-cyclodextrin. J. Mol. Liq. 2015, 210, 143–150. [Google Scholar] [CrossRef]
- Hincal, A.A.; Eroğlu, H.; Bilensoy, E. Regulatory Status of Cyclodextrins in Pharmaceutical Products. In Cyclodextrins in Pharmaceutics, Cosmetics, and Biomedicine; Wiley: New York, NY, USA, 2011; pp. 123–130. [Google Scholar]
- Raut, S.Y.; Manne, A.S.N.; Kalthur, G.; Jain, S.; Mutalik, S. Cyclodextrins as Carriers in Targeted Delivery of Therapeutic Agents: Focused Review on Traditional and Inimitable Applications. Curr. Pharm. Des. 2019, 25, 444–454. [Google Scholar] [CrossRef]
- Mazyed, E.A.; Badria, F.A.; ElNaggar, M.H.; El-Masry, S.M.; Helmy, S.A. Development of Cyclodextrin-Functionalized Transethoniosomes of 6-Gingerol: Statistical Optimization, In Vitro Characterization and Assessment of Cytotoxic and Anti-Inflammatory Effects. Pharmaceutics 2022, 14, 1170. [Google Scholar] [CrossRef]
- Wang, X.; Parvathaneni, V.; Shukla, S.K.; Kulkarni, N.S.; Muth, A.; Kunda, N.K.; Gupta, V. Inhalable resveratrol-cyclodextrin complex loaded biodegradable nanoparticles for enhanced efficacy against non-small cell lung cancer. Int. J. Biol. Macromol. 2020, 164, 638–650. [Google Scholar] [CrossRef]
- Shukla, S.K.; Chan, A.; Parvathaneni, V.; Kanabar, D.D.; Patel, K.; Ayehunie, S.; Muth, A.; Gupta, V. Enhanced solubility, stability, permeation and anti-cancer efficacy of Celastrol-β-cyclodextrin inclusion complex. J. Mol. Liq. 2020, 318, 113936. [Google Scholar] [CrossRef]
- Forma, E.; Bryś, M. Anticancer Activity of Propolis and Its Compounds. Nutrients 2021, 13, 2594. [Google Scholar] [CrossRef] [PubMed]
- Zafar, A.; Alruwaili, N.K.; Imam, S.S.; Alsaidan, O.A.; Alharbi, K.S.; Mostafa, E.M.; Musa, A.; Gilani, S.J.; Ghoneim, M.M.; Alshehri, S.; et al. Formulation of ternary genistein β-cyclodextrin inclusion complex: In vitro characterization and cytotoxicity assessment using breast cancer cell line. J. Drug Deliv. Sci. Technol. 2022, 67, 102932. [Google Scholar] [CrossRef]
- Trindade, G.G.G.; Thrivikraman, G.; Menezes, P.P.; França, C.M.; Lima, B.S.; Carvalho, Y.M.B.G.; Souza, E.P.B.S.S.; Duarte, M.C.; Shanmugam, S.; Quintans-Júnior, L.J.; et al. Carvacrol/β-cyclodextrin inclusion complex inhibits cell proliferation and migration of prostate cancer cells. Food Chem. Toxicol. 2019, 125, 198–209. [Google Scholar] [CrossRef]
- Shahriari, M.; Kesharwani, P.; Johnston, T.P.; Sahebkar, A. Anticancer potential of curcumin-cyclodextrin complexes and their pharmacokinetic properties. Int. J. Pharm. 2023, 631, 122474. [Google Scholar] [CrossRef]
- Tønnesen, H.H.; Másson, M.; Loftsson, T. Studies of curcumin and curcuminoids. XXVII. Cyclodextrin complexation: Solubility, chemical and photochemical stability. Int. J. Pharm. 2002, 244, 127–135. [Google Scholar] [CrossRef] [PubMed]
- Patro, N.M.; Sultana, A.; Terao, K.; Nakata, D.; Jo, A.; Urano, A.; Ishida, Y.; Gorantla, R.N.; Pandit, V.; Devi, K.; et al. Comparison and correlation of in vitro, in vivo and in silico evaluations of alpha, beta and gamma cyclodextrin complexes of curcumin. J. Incl. Phenom. Macrocycl. Chem. 2014, 78, 471–483. [Google Scholar] [CrossRef]
- Ma, Z.; Wang, N.; He, H.; Tang, X. Pharmaceutical strategies of improving oral systemic bioavailability of curcumin for clinical application. J. Control. Release Off. J. Control. Release Soc. 2019, 316, 359–380. [Google Scholar] [CrossRef] [PubMed]
- Purpura, M.; Lowery, R.P.; Wilson, J.M.; Mannan, H.; Münch, G.; Razmovski-Naumovski, V. Analysis of different innovative formulations of curcumin for improved relative oral bioavailability in human subjects. Eur. J. Nutr. 2018, 57, 929–938. [Google Scholar] [CrossRef] [Green Version]
- Yallapu, M.M.; Jaggi, M.; Chauhan, S.C. β-Cyclodextrin-curcumin self-assembly enhances curcumin delivery in prostate cancer cells. Colloids Surf. B Biointerfaces 2010, 79, 113–125. [Google Scholar] [CrossRef]
- Rocks, N.; Bekaert, S.; Coia, I.; Paulissen, G.; Gueders, M.; Evrard, B.; Van Heugen, J.C.; Chiap, P.; Foidart, J.M.; Noel, A.; et al. Curcumin-cyclodextrin complexes potentiate gemcitabine effects in an orthotopic mouse model of lung cancer. Br. J. Cancer 2012, 107, 1083–1092. [Google Scholar] [CrossRef] [Green Version]
- Kazemi-Lomedasht, F.; Rami, A.; Zarghami, N. Comparison of inhibitory effect of curcumin nanoparticles and free curcumin in human telomerase reverse transcriptase gene expression in breast cancer. Adv. Pharm. Bull. 2013, 3, 127–130. [Google Scholar] [CrossRef]
- Low, Z.X.; Teo, M.Y.M.; Nordin, F.J.; Dewi, F.R.P.; Palanirajan, V.K.; In, L.L.A. Biophysical Evaluation of Water-Soluble Curcumin Encapsulated in β-Cyclodextrins on Colorectal Cancer Cells. Int. J. Mol. Sci. 2022, 23, 12866. [Google Scholar] [CrossRef]
- Boztas, A.O.; Karakuzu, O.; Galante, G.; Ugur, Z.; Kocabas, F.; Altuntas, C.Z.; Yazaydin, A.O. Synergistic interaction of paclitaxel and curcumin with cyclodextrin polymer complexation in human cancer cells. Mol. Pharm. 2013, 10, 2676–2683. [Google Scholar] [CrossRef]
- Roozbehi, S.; Dadashzadeh, S.; Sajedi, R.H. An enzyme-mediated controlled release system for curcumin based on cyclodextrin/cyclodextrin degrading enzyme. Enzym. Microb. Technol. 2021, 144, 109727. [Google Scholar] [CrossRef]
- Rauf, A.; Imran, M.; Butt, M.S.; Nadeem, M.; Peters, D.G.; Mubarak, M.S. Resveratrol as an anti-cancer agent: A review. Crit. Rev. Food Sci. Nutr. 2018, 58, 1428–1447. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.; Farkhondeh, T.; Aschner, M.; Samarghandian, S. Resveratrol mediates its anti-cancer effects by Nrf2 signaling pathway activation. Cancer Cell Int. 2021, 21, 579. [Google Scholar] [CrossRef] [PubMed]
- Venuti, V.; Cannavà, C.; Cristiano, M.C.; Fresta, M.; Majolino, D.; Paolino, D.; Stancanelli, R.; Tommasini, S.; Ventura, C.A. A characterization study of resveratrol/sulfobutyl ether-β-cyclodextrin inclusion complex and in vitro anticancer activity. Colloids Surf. B Biointerfaces 2014, 115, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Berta, G.N.; Salamone, P.; Sprio, A.E.; Di Scipio, F.; Marinos, L.M.; Sapino, S.; Carlotti, M.E.; Cavalli, R.; Di Carlo, F. Chemoprevention of 7,12-dimethylbenz[a]anthracene (DMBA)-induced oral carcinogenesis in hamster cheek pouch by topical application of resveratrol complexed with 2-hydroxypropyl-β-cyclodextrin. Oral Oncol. 2010, 46, 42–48. [Google Scholar] [CrossRef]
- Lu, Z.; Chen, R.; Fu, R.; Xiong, J.; Hu, Y. Cytotoxicity and inhibition of lipid peroxidation activity of resveratrol/cyclodextrin inclusion complexes. J. Incl. Phenom. Macrocycl. Chem. 2012, 73, 313–320. [Google Scholar] [CrossRef]
- Zafar, A.; Alruwaili, N.K.; Imam, S.S.; Alsaidan, O.A.; Alkholifi, F.K.; Alharbi, K.S.; Mostafa, E.M.; Alanazi, A.S.; Gilani, S.J.; Musa, A.; et al. Formulation of Genistein-HP β Cyclodextrin-Poloxamer 188 Ternary Inclusion Complex: Solubility to Cytotoxicity Assessment. Encapsulation Nat. Polyphen. Compd. A Rev. 2021, 13, 1997. [Google Scholar] [CrossRef]
- Başaran, E.; Öztürk, A.A.; Şenel, B.; Demirel, M.; Sarica, Ş. Quercetin, Rutin and Quercetin-Rutin Incorporated Hydroxypropyl β-Cyclodextrin Inclusion Complexes. Eur. J. Pharm. Sci. Off. J. Eur. Fed. Pharm. Sci. 2022, 172, 106153. [Google Scholar] [CrossRef]
- Cheng, Z.; Zhang, Z.; Han, Y.; Wang, J.; Wang, Y.; Chen, X.; Shao, Y.; Cheng, Y.; Zhou, W.; Lu, X.; et al. A review on anti-cancer effect of green tea catechins. J. Funct. Foods 2020, 74, 104172. [Google Scholar] [CrossRef]
- McClements, D.J. Food Emulsions, Principles, Practices and Techniques; CRC Press: Boca Raton, FL, USA, 2015. [Google Scholar]
- Wilson, R.J.; Li, Y.; Yang, G.; Zhao, C.-X. Nanoemulsions for drug delivery. Particuology 2022, 64, 85–97. [Google Scholar] [CrossRef]
- Gallegos, C.; Partal, P.; Franco, J.M. Droplet-size distribution and stability of lipid injectable emulsions. Am. J. Health-Syst. Pharm. AJHP: Off. J. Am. Soc. Health-Syst. Pharm. 2009, 66, 162–166. [Google Scholar] [CrossRef]
- Losada-Barreiro, S.; Sezgin-Bayindir, Z.; Paiva-Martins, F.; Bravo-Díaz, C. Biochemistry of Antioxidants: Mechanisms and Pharmaceutical Applications. Biomedicines 2022, 10, 3051. [Google Scholar] [CrossRef]
- Bravo-Díaz, C. Advances in the control of lipid peroxidation in oil-in-water emulsions: Kinetic approaches. Crit. Rev. Food Sci. Nutr. 2022, 1, 1–33. [Google Scholar] [CrossRef] [PubMed]
- Takino, T.; Konishi, K.; Takakura, Y.; Hashida, M. Long circulating emulsion carrier systems for highly lipophilic drugs. Biol. Pharm. Bull. 1994, 17, 121–125. [Google Scholar] [CrossRef] [Green Version]
- Hippalgaonkar, K.; Majumdar, S.; Kansara, V. Injectable lipid emulsions-advancements, opportunities and challenges. AAPS Pharm. Sci. Tech. 2010, 11, 1526–1540. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ragelle, H.; Crauste-Manciet, S.; Seguin, J.; Brossard, D.; Scherman, D.; Arnaud, P.; Chabot, G.G. Nanoemulsion formulation of fisetin improves bioavailability and antitumour activity in mice. Int. J. Pharm. 2012, 427, 452–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Touil, Y.S.; Seguin, J.; Scherman, D.; Chabot, G.G. Improved antiangiogenic and antitumour activity of the combination of the natural flavonoid fisetin and cyclophosphamide in Lewis lung carcinoma-bearing mice. Cancer Chemother. Pharmacol. 2011, 68, 445–455. [Google Scholar] [CrossRef] [Green Version]
- Huang, R.F.; Wei, Y.J.; Inbaraj, B.S.; Chen, B.H. Inhibition of colon cancer cell growth by nanoemulsion carrying gold nanoparticles and lycopene. Int. J. Nanomed. 2015, 10, 2823–2846. [Google Scholar] [CrossRef] [Green Version]
- Ali, H.; Shirode, A.B.; Sylvester, P.W.; Nazzal, S. Preparation, characterization, and anticancer effects of simvastatin-tocotrienol lipid nanoparticles. Int. J. Pharm. 2010, 389, 223–231. [Google Scholar] [CrossRef]
- Steuber, N.; Vo, K.; Wadhwa, R.; Birch, J.; Iacoban, P.; Chavez, P.; Elbayoumi, T.A. Tocotrienol Nanoemulsion Platform of Curcumin Elicit Elevated Apoptosis and Augmentation of Anticancer Efficacy against Breast and Ovarian Carcinomas. Int. J. Mol. Sci. 2016, 17, 1792. [Google Scholar] [CrossRef] [Green Version]
- Bharmoria, P.; Bisht, M.; Gomes, M.C.; Martins, M.; Neves, M.C.; Mano, J.F.; Bdikin, I.; Coutinho, J.A.P.; Ventura, S.P.M. Protein-olive oil-in-water nanoemulsions as encapsulation materials for curcumin acting as anticancer agent towards MDA-MB-231 cells. Sci. Rep. 2021, 11, 9099. [Google Scholar] [CrossRef]
- Machado, F.C.; Adum de Matos, R.P.; Primo, F.L.; Tedesco, A.C.; Rahal, P.; Calmon, M.F. Effect of curcumin-nanoemulsion associated with photodynamic therapy in breast adenocarcinoma cell line. Bioorganic Med. Chem. 2019, 27, 1882–1890. [Google Scholar] [CrossRef]
- Guan, Y.B.; Zhou, S.Y.; Zhang, Y.Q.; Wang, J.L.; Tian, Y.D.; Jia, Y.Y.; Sun, Y.J. Therapeutic effects of curcumin nanoemulsions on prostate cancer. J. Huazhong Univ. Sci. Technol. Med. Sci. 2017, 37, 371–378. [Google Scholar] [CrossRef]
- Kour, P.; Ahmad Dar, A. Effect of interfacially-engineered nanoemulsions of linoleic acid stabilized by mixed surfactant systems and curcumin on their physicochemical properties, induction times and peroxidation stability. J. Mol. Liq. 2023, 384, 122243. [Google Scholar] [CrossRef]
- Fofaria, N.M.; Qhattal, H.S.; Liu, X.; Srivastava, S.K. Nanoemulsion formulations for anti-cancer agent piplartine--Characterization, toxicological, pharmacokinetics and efficacy studies. Int. J. Pharm. 2016, 498, 12–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, B.H.; Hsieh, C.H.; Tsai, S.Y.; Wang, C.Y.; Wang, C.C. Anticancer effects of epigallocatechin-3-gallate nanoemulsion on lung cancer cells through the activation of AMP-activated protein kinase signaling pathway. Sci. Rep. 2020, 10, 5163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ceramella, J.; Groo, A.-C.; Iacopetta, D.; Séguy, L.; Mariconda, A.; Puoci, F.; Saturnino, C.; Leroy, F.; Since, M.; Longo, P.; et al. A winning strategy to improve the anticancer properties of Cisplatin and Quercetin based on the nanoemulsions formulation. J. Drug Deliv. Sci. Technol. 2021, 66, 102907. [Google Scholar] [CrossRef]
- Sharifi-Rad, J.; Quispe, C.; Mukazhanova, Z.; Knut, E.; Turgumbayeva, A.; Kipchakbayeva, A.; Seitimova, G.; Mahomoodally, M.F.; Lobine, D.; Koay, A.; et al. Resveratrol-Based Nanoformulations as an Emerging Therapeutic Strategy for Cancer. Front. Mol. Biosci. 2021, 8, 649395. [Google Scholar] [CrossRef]
- Pund, S.; Thakur, R.; More, U.; Joshi, A. Lipid based nanoemulsifying resveratrol for improved physicochemical characteristics, in vitro cytotoxicity and in vivo antiangiogenic efficacy. Colloids Surf. B Biointerfaces 2014, 120, 110–117. [Google Scholar] [CrossRef]
- EMA. Guideline on Quality of Oral Modified Release Products; European Medicines Agency: London, UK, 2014. [Google Scholar]
- Langer, R.; Wise, D. Medical Applications of Controlled Release, 1st ed.; CRC Press: Boca Raton, FL, USA, 1984. [Google Scholar]
- Wen, H.; Park, K. Introduction and Overview of Oral Controlled Release Formulation Design. In Oral Controlled Release Formulation Design and Drug Delivery; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2010; pp. 1–19. [Google Scholar]
- Zeb, A.; Gul, M.; Nguyen, T.-T.-L.; Maeng, H.-J. Controlled release and targeted drug delivery with poly(lactic-co-glycolic acid) nanoparticles: Reviewing two decades of research. J. Pharm. Investig. 2022, 52, 683–724. [Google Scholar] [CrossRef]
- Yun, Y.H.; Lee, B.K.; Park, K. Controlled Drug Delivery: Historical perspective for the next generation. J. Control. Release 2015, 219, 2–7. [Google Scholar] [CrossRef] [Green Version]
- Park, K. Controlled drug delivery systems: Past forward and future back. J. Control. Release 2014, 190, 3–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, G.; Grewal, J.; Jyoti, K.; Jain, U.K.; Chandra, R.; Madan, J. Chapter 15-Oral controlled and sustained drug delivery systems: Concepts, advances, preclinical, and clinical status. In Drug Targeting and Stimuli Sensitive Drug Delivery Systems; Grumezescu, A.M., Ed.; William Andrew Publishing: Norwich, NY, USA, 2018; pp. 567–626. [Google Scholar]
- Sowjanya, M.; Debnath, S.; Lavanya, P.; Thejovathi, R.; Babu, M. Polymers used in the Designing of Controlled Drug Delivery System. Res. J. Pharm. Technol. 2017, 10, 903. [Google Scholar] [CrossRef]
- Aravamudhan, A.; Ramos, D.M.; Nada, A.A.; Kumbar, S.G. Chapter 4-Natural Polymers: Polysaccharides and Their Derivatives for Biomedical Applications. In Natural and Synthetic Biomedical Polymers; Kumbar, S.G., Laurencin, C.T., Deng, M., Eds.; Elsevier: Oxford, UK, 2014; pp. 67–89. [Google Scholar]
- Zhang, Z.; Ortiz, O.; Goyal, R.; Kohn, J. 13-Biodegradable Polymers. In Handbook of Polymer Applications in Medicine and Medical Devices; Modjarrad, K., Ebnesajjad, S., Eds.; William Andrew Publishing: Oxford, UK, 2014; pp. 303–335. [Google Scholar]
- Pandey, S.P.; Shukla, T.; Dhote, V.K.; Mishra, D.; Maheshwari, R.; Tekade, R.K. Chapter 4-Use of Polymers in Controlled Release of Active Agents. In Basic Fundamentals of Drug Delivery; Tekade, R.K., Ed.; Academic Press: Cambridge, MA, USA, 2019; pp. 113–172. [Google Scholar]
- Doğan Ergin, A.; Bayindir, Z.S.; Ozçelikay, A.T.; Yuksel, N. A novel delivery system for enhancing bioavailability of S-adenosyl-l-methionine: Pectin nanoparticles-in-microparticles and their in vitro-in vivo evaluation’. J. Drug Deliv. Sci. Technol. 2020, 61, 102096. [Google Scholar] [CrossRef]
- Doğan Ergin, N.A.; Sezgin-Bayindir, Z.; Yüskel, N. Characterization and optimization of colon targeted S-adenosyl-L-methionine loaded chitosan nanoparticles. J. Res. Pharm. 2019, 23, 914–926. [Google Scholar] [CrossRef] [Green Version]
- Sanopoulou, M.; Papadokostaki, K.G. Controlled Drug Release Systems: Mechanisms and Kinetics. In Biomedical Membranes and (Bio)Artificial Organs; World Scientific: Singapore, 2017; pp. 1–33. [Google Scholar]
- Sobczak, M.; Kędra, K. Biomedical Polyurethanes for Anti-Cancer Drug Delivery Systems: A Brief, Comprehensive Review. Int. J. Mol. Sci. 2022, 23, 8181. [Google Scholar] [CrossRef]
- Siegel, R.A.; Rathbone, M.J. Overview of Controlled Release Mechanisms. In Fundamentals and Applications of Controlled Release Drug Delivery; Siepmann, J., Siegel, R.A., Rathbone, M.J., Eds.; Springer: Boston, MA, USA, 2012; pp. 19–43. [Google Scholar]
- Heidarli, E.; Dadashzadeh, S.; Haeri, A. State of the Art of Stimuli-Responsive Liposomes for Cancer Therapy. Iran. J. Pharm. Res. 2017, 16, 1273–1304. [Google Scholar] [PubMed]
- Maruyama, K. Intracellular targeting delivery of liposomal drugs to solid tumors based on EPR effects. Adv. Drug Deliv. Rev. 2011, 63, 161–169. [Google Scholar] [CrossRef]
- van Valenberg, F.J.P.; Brummelhuis, I.S.G. DPPG(2)-Based Thermosensitive Liposomes with Encapsulated Doxorubicin Combined with Hyperthermia Lead to Higher Doxorubicin Concentrations in the Bladder Compared to Conventional Application in Pigs: A Rationale for the Treatment of Muscle-Invasive Bladder Cancer. Int. J. Nanomed. 2021, 16, 75–88. [Google Scholar] [CrossRef]
- Nichols, J.W.; Bae, Y.H. EPR: Evidence and fallacy. J. Control. Release 2014, 190, 451–464. [Google Scholar] [CrossRef]
- Yadav, H.K.S.; Dibi, M.; Mohammed, A.; Emad, A. Chapter 13-Thermoresponsive Drug Delivery Systems, Characterization, and Applications. In Characterization and Biology of Nanomaterials for Drug Delivery; Mohapatra, S.S., Ranjan, S., Dasgupta, N., Mishra, R.K., Thomas, S., Eds.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 351–373. [Google Scholar]
- Yang, S.J.; Huang, C.H.; Wang, C.H.; Shieh, M.J.; Chen, K.C. The Synergistic Effect of Hyperthermia and Chemotherapy in Magnetite Nanomedicine-Based Lung Cancer Treatment. Int. J. Nanomed. 2020, 15, 10331–10347. [Google Scholar] [CrossRef]
- An, X.; Gui, R. Chapter 28-Stimuli-responsive liposome and control release drug. In Nanostructures for Drug Delivery; Andronescu, E., Grumezescu, A.M., Eds.; Elsevier: Amsterdam, The Netherlands, 2017; pp. 887–917. [Google Scholar]
- Papaioannou, L.; Avgoustakis, K. Responsive nanomedicines enhanced by or enhancing physical modalities to treat solid cancer tumors: Preclinical and clinical evidence of safety and efficacy. Adv. Drug Deliv. Rev. 2022, 181, 114075. [Google Scholar] [CrossRef]
- Jain, S.; Raza, K.; Agrawal, A.K.; Vaidya, A. Chapter 4-Temperature-sensitive carrier and temperature-directed tumor cell eradication. In Nanotechnology Applications for Cancer Chemotherapy; Jain, S., Raza, K., Agrawal, A.K., Vaidya, A., Eds.; Elsevier: Amsterdam, The Netherlands, 2021; pp. 49–57. [Google Scholar]
- Kono, K. Thermosensitive polymer-modified liposomes. Adv. Drug Deliv. Rev. 2001, 53, 307–319. [Google Scholar] [CrossRef]
- Abri Aghdam, M.; Bagheri, R.; Mosafer, J.; Baradaran, B.; Hashemzaei, M.; Baghbanzadeh, A.; de la Guardia, M.; Mokhtarzadeh, A. Recent advances on thermosensitive and pH-sensitive liposomes employed in controlled release. J. Control. Release Off. J. Control. Release Soc. 2019, 315, 1–22. [Google Scholar] [CrossRef]
- Yatvin, M.B.; Weinstein, J.N.; Dennis, W.H.; Blumenthal, R. Design of liposomes for enhanced local release of drugs by hyperthermia. Science 1978, 202, 1290–1293. [Google Scholar] [CrossRef]
- Haemmerich, D.; Motamarry, A. Chapter Five-Thermosensitive Liposomes for Image-Guided Drug Delivery. In Advances in Cancer Research; Broome, A.-M., Ed.; Academic Press: Cambridge, MA, USA, 2018; Volume 139, pp. 121–146. [Google Scholar]
- Ward, M.A.; Georgiou, T.K. Thermoresponsive Polymers for Biomedical Applications. Polymers 2011, 3, 1215–1242. [Google Scholar] [CrossRef] [Green Version]
- Teotia, A.K.; Sami, H.; Kumar, A. 1-Thermo-responsive polymers: Structure and design of smart materials. In Switchable and Responsive Surfaces and Materials for Biomedical Applications; Zhang, Z., Ed.; Woodhead Publishing: Oxford, UK, 2015; pp. 3–43. [Google Scholar]
- Ta, T.; Porter, T.M. Thermosensitive liposomes for localized delivery and triggered release of chemotherapy. J. Control. Release 2013, 169, 112–125. [Google Scholar] [CrossRef] [Green Version]
- de Matos, M.B.C.; Beztsinna, N.; Heyder, C.; Fens, M.; Mastrobattista, E.; Schiffelers, R.M.; Leneweit, G.; Kok, R.J. Thermosensitive liposomes for triggered release of cytotoxic proteins. Eur. J. Pharm. Biopharm. 2018, 132, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Maia, A.L.C.; e Silva, A.T.M.; César, A.L.A.; Giuberti, C.S.; Evangelista, F.C.G.; Lemos, J.d.A.; Sabino, A.P.; Malachias, Â.; Fernandes, C.; de Barros, A.L.B.; et al. Preparation and characterization of gadolinium-based thermosensitive liposomes: A potential nanosystem for selective drug delivery to cancer cells. J. Drug Deliv. Sci. Technol. 2021, 65, 102686. [Google Scholar] [CrossRef]
- Abu Dayyih, A.; Alawak, M.; Ayoub, A.M.; Amin, M.U.; Abu Dayyih, W.; Engelhardt, K.; Duse, L.; Preis, E.; Brüßler, J.; Bakowsky, U. Thermosensitive liposomes encapsulating hypericin: Characterization and photodynamic efficiency. Int. J. Pharm. 2021, 609, 121195. [Google Scholar] [CrossRef] [PubMed]
- Nai, J.; Zhang, J.; Li, J.; Li, H.; Yang, Y.; Yang, M.; Wang, Y.; Gong, W.; Li, Z.; Li, L.; et al. Macrophage membrane- and cRGD-functionalized thermosensitive liposomes combined with CPP to realize precise siRNA delivery into tumor cells. Mol. Ther. Nucleic Acids 2022, 27, 349–362. [Google Scholar] [CrossRef]
- Ahmadi-Motamayel, F.; Goodarzi, M.T.; Hendi, S.S.; Kasraei, S.; Moghimbeigi, A. Total antioxidant capacity of saliva and dental caries. Med. Oral Patol. Oral Y Cir. Bucal 2013, 18, e553–e556. [Google Scholar] [CrossRef] [PubMed]
- Hujoel, P.P.; Lingström, P. Nutrition, dental caries and periodontal disease: A narrative review. J. Clin. Periodontol. 2017, 44 (Suppl. S18), S79–S84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Armitage, G.C. The complete periodontal examination. Periodontol. 2000 2004, 34, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, S.; Hiorth, M. Advanced drug delivery systems for local treatment of the oral cavity. Ther. Deliv. 2015, 6, 595–608. [Google Scholar] [CrossRef] [Green Version]
- Hakim, L.K.; Yazdanian, M.; Alam, M.; Abbasi, K.; Tebyaniyan, H.; Tahmasebi, E.; Khayatan, D.; Seifalian, A.; Ranjbar, R.; Yazdanian, A. Biocompatible and Biomaterials Application in Drug Delivery System in Oral Cavity. Evid.-Based Complement. Altern. Med. 2021, 2021, 9011226. [Google Scholar] [CrossRef]
- Parmar, A.; Macluskey, M.; Mc Goldrick, N.; Conway, D.I.; Glenny, A.M.; Clarkson, J.E.; Worthington, H.V.; Chan, K.K.W. Interventions for the treatment of oral cavity and oropharyngeal cancer: Chemotherapy. Cochrane Database Syst. Rev. 2021, 4, CD006386. [Google Scholar] [CrossRef]
- Şenel, S.; Özdoğan, A.I.; Akca, G. Current status and future of delivery systems for prevention and treatment of infections in the oral cavity. Drug Deliv. Transl. Res. 2021, 11, 1703–1734. [Google Scholar] [CrossRef]
- Bonilla-Represa, V.; Abalos-Labruzzi, C.; Herrera-Martinez, M.; Guerrero-Pérez, M.O. Nanomaterials in Dentistry: State of the Art and Future Challenges. Nanomaterials 2020, 10, 1770. [Google Scholar] [CrossRef]
- Mehta, S.; Kuriakose, M.A. Principles of Surgical Management of Oral Cancer. In Oral and Maxillofacial Surgery for the Clinician; Bonanthaya, K., Panneerselvam, E., Manuel, S., Kumar, V.V., Rai, A., Eds.; Springer Nature: Singapore, 2021; pp. 1869–1891. [Google Scholar]
- Levine, R.S. Pyrophosphates in toothpaste: A retrospective and reappraisal. Br. Dent. J. 2020, 229, 687–689. [Google Scholar] [CrossRef]
- Faheem, A.M.; Abdelkader, D.H. 1-Novel drug delivery systems. In Engineering Drug Delivery Systems; Seyfoddin, A., Dezfooli, S.M., Greene, C.A., Eds.; Woodhead Publishing: Sawston, UK, 2020; pp. 1–16. [Google Scholar]
- Khan, S.A.; Ali, H. Novel Drug Delivery Systems. In Essentials of Industrial Pharmacy; Khan, S.A., Ed.; Pharmaceutical Science Series; Springer Nature: Basel, Switzerland, 2022; Volume 46. [Google Scholar]






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Radical Couple | Ep0 (mV) |
|---|---|
| ∙OH, H+/H2O | 2330 |
| O3∙−, 2H+/H2O + O2 | 1800 |
| RO∙, H+/ROH | 1600 |
| HOO∙, H+/H2O2 | 1060 |
| ROO∙, H+/ROOH | 1000 |
| O2∙−, H+/H2O2 | 940 |
| RS∙/RS- | 920 |
| GSH/GS∙ | 920 |
| O3/O3∙− | 890 |
| 1O2/1O2∙− | 650 |
| PUFA∙, H+/PUFA | 600 |
| Catechol-O∙/catechol-OH | 530 |
| α-Tocopheroxyl∙, H+/ α-Tocopherol | 500 |
| Trolox∙, H+/Trolox-OH | 480 |
| H2O2, H+/H2O, HO∙ | 380 |
| Ascorbate−∙, H+/Ascorbate | 282 |
| O2/O2∙− | −160 |
| H2O/e− (aq) | −2870 |
| External Diameter (Å) | Internal Diameter (Å) | Solubility (mg/mL), T = 25 °C | log (PWOCT) | Surface Tension (mM/m) | |
|---|---|---|---|---|---|
| α-CD | 14.6 | 4.7–5.3 | 145 | −13 | 71 |
| β-CD | 15.4 | 6.0–6.5 | 18.5 | −14 | 71 |
| Randomly methylated β-CD | --- | --- | >500 | --- | 62 |
| Dimethyl-β-CD | --- | --- | 570 | −6 | 57.5–54.1 |
| 2-Hydroxypropyl-β-CD (HP--β-CD) | 15.4 | 6.0–6.5 | >1200 | −11 | 54.8–57.5 |
| Sulfobutylether-β-CD sodium salt (SBE--β-CD) | --- | --- | >1200 | −10 | 71 |
| δ-CD | 17.5 | 7.5–8.3 | 232 | −17 | 71 |
| 2-Hydroxypropyl-δ-CD | --- | --- | 800 | −13 | 71 |
| CD-based Nanocarrier | AO with Reported Anticancer Properties | Type(s) of Cancer | Reference |
|---|---|---|---|
| Sulfobutylether-β-CD | Resveratrol | Lung | [45] |
| Sulfobutylether-β-CD | Celastrol | Lung | [46] |
| α-, β-, and γ-CD | New Zealand propolis | Esophageal squamous cell, colon, gastric, and colorectal adenocarcinomas | [47] |
| D-α-tocopherol polyethylene glycol 1000 succinate-modified β-CD | Genistein | Breast | [48] |
| β-CD | Carvacrol | Prostate | [49] |
| α-, β-, and γ-CD | Curcumin | Lung, prostate, breast, and colorectal | [50] |
| Advantages | Limitations |
|---|---|
| Provides a uniform therapeutic response by stabilizing the blood drug concentration and reducing the fluctuations in plasma concentration; Improves patient compliance. The patient care period in hospitals can be reduced; As the drug intake frequency per day/month decreases, the number of missed doses also decreases; Reduces local and systemic toxicity by providing localized drug release and reducing the total drug intake, thus providing maximum bioavailability with the minimum dose; The physicochemical stability of the active molecules can be provided (e.g., protection against enzymatic inactivation or bacterial decomposition via encapsulation); Drugs with a short plasma half-life can be administered at longer dosage intervals; Advantageous for the manufacturer in terms of increased commercial value. | Immediate termination of the therapy just after drug administration is not always possible; The dosage is adjusted by considering the average pharmacokinetic behavior in the normal population; therefore, the dose regimen cannot be freely modified; The sterility necessity of the implants and their application/removal by surgical operation are disadvantages in terms of manufacturing and ease of use; It is not possible to design a controlled-release dosage form for each active molecule; its physicochemical and biological properties must be considered; Research and development costs are higher in terms of manufacturing and equipment. |
| Biodegradable Polymers |
|
| Non- Biodegradable Polymers |
|
| Product Name | Active Ingredient | Indication |
|---|---|---|
| Lupron Depot | Leuprolide | Treatment of prostate cancer and endometriosis |
| Sandostatin LAR | Octreotide | Treatment of acromegaly and endocrine tumors |
| Trelstar Depot | Triptorelin pamoate | Palliative treatment of advanced prostate cancer |
| Zoladex | Goserelin acetate | Advanced prostate cancer and advanced |
| Gliadel | Carmustine | Brain tumors |
| Decapeptyl | Triptorelin acetate | Prostate cancer |
| Profact Depot | Buserelin acetate | Prostate cancer |
| TSL Type | Cargo | Preparation Method | TSL Composition * | Study Outcome | Ref. |
|---|---|---|---|---|---|
| LTSL | Mistletoe lectin-1 (ML1) | Film hydration and extrusion. | DPPC:MSPC:DSPE-PEG2000 (86:10:4%mol). | The bioactivity of TSL against murine CT26 colon carcinoma cells in terms of cytotoxicity and inhibition of tumor cell viability was shown. | [122] |
| TTSL LTSL | Gadolinium-DTPA-BMA) | Film hydration. | DPPC:MSPC:DSPE-PEG2000 (85:10:5). | Gd-DTPA-BMA-loaded TSL exhibited improved cytotoxicity against breast cancer cell lines compared to free Gd-DTPA-BMA, and the low cytotoxicity of TSL on normal cell lines (WI-26 VA 4) revealed the selectivity of the carrier. | [123] |
| LTSL | Hypericin | Film hydration. | DPPC:DSPC:DSPE-mPEG-2000: Hypericin (79:15:5:1). | Safety of hypericin-loaded TSL was shown by hemocompatibility studies; the combination of heat and TSL led to increased ROS levels, enhanced intracellular uptake, and phototoxicity in breast cancer originated from MDA-MB-231 cells. | [124] |
| MTSL | siRNA | Film hydration and extrusion. | DPPC:MSPC:DSPE-PEG2000 (165:5.5:5) macrophage membrane DSPE-PEG2000-cRGD CPP. | Macrophage membrane- and cRGD-functionalized thermosensitive liposomes combined with CPP provided tumor-targeted delivery of siRNA in tumor-bearing mice and tumor inhibition efficacy was shown both in vitro and in vivo. | [125] |
| Advantages | Disadvantages | |
|---|---|---|
| Local drug delivery system |
|
|
| Systemic drug delivery system |
|
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sezgin-Bayindir, Z.; Losada-Barreiro, S.; Fernández-Bravo, S.; Bravo-Díaz, C. Innovative Delivery and Release Systems for Antioxidants and Other Active Substances in the Treatment of Cancer. Pharmaceuticals 2023, 16, 1038. https://doi.org/10.3390/ph16071038
Sezgin-Bayindir Z, Losada-Barreiro S, Fernández-Bravo S, Bravo-Díaz C. Innovative Delivery and Release Systems for Antioxidants and Other Active Substances in the Treatment of Cancer. Pharmaceuticals. 2023; 16(7):1038. https://doi.org/10.3390/ph16071038
Chicago/Turabian StyleSezgin-Bayindir, Zerrin, Sonia Losada-Barreiro, Sofía Fernández-Bravo, and Carlos Bravo-Díaz. 2023. "Innovative Delivery and Release Systems for Antioxidants and Other Active Substances in the Treatment of Cancer" Pharmaceuticals 16, no. 7: 1038. https://doi.org/10.3390/ph16071038