
Impact of Duodenal Pathology on Oral Drug Bioavailability and Disease Outcomes in Pediatric Crohn’s Disease
 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Entire Cohort
2.2. Subset of TPMT Normal Metabolizers
3. Discussion
4. Materials and Methods
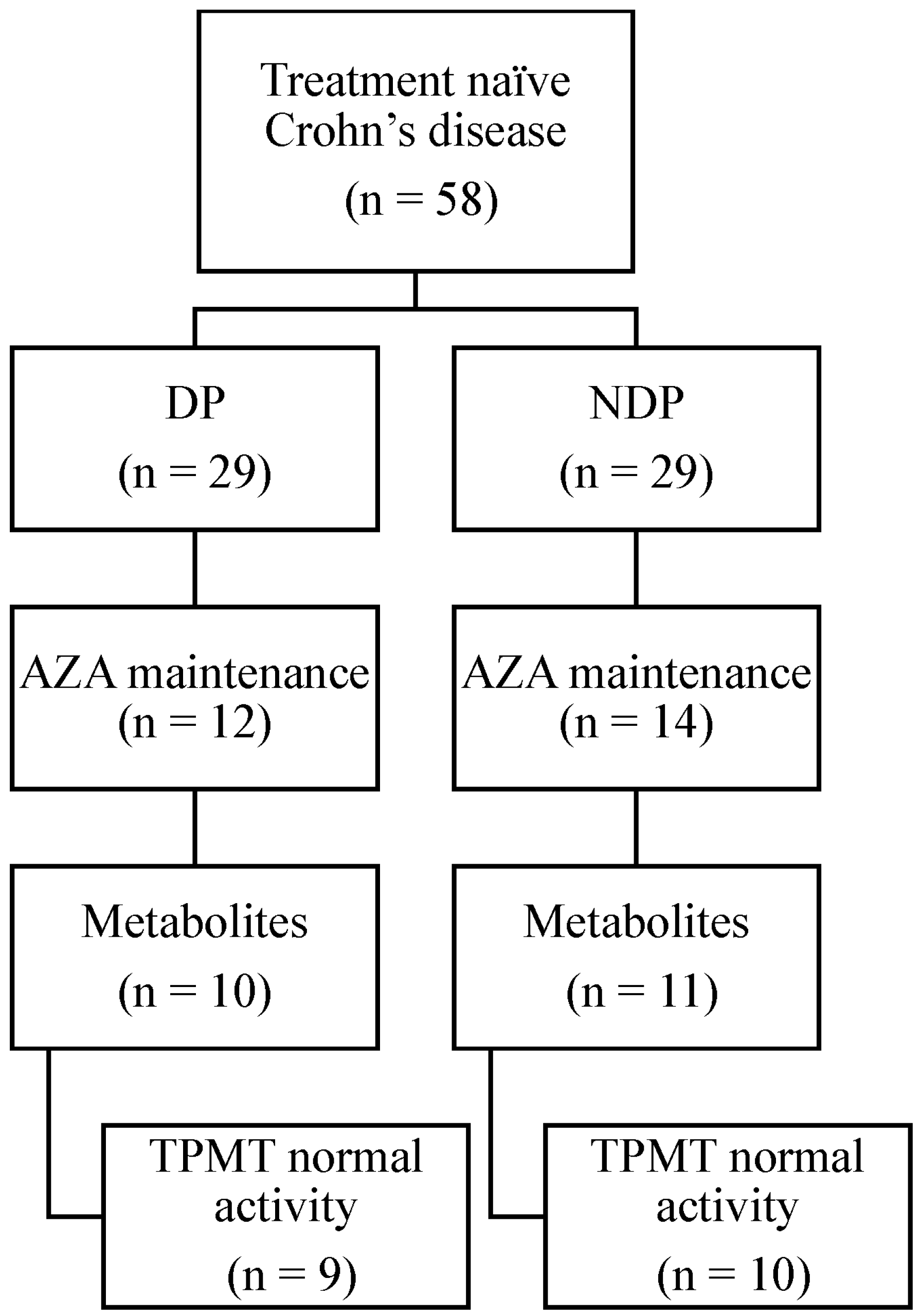
4.1. Study Population
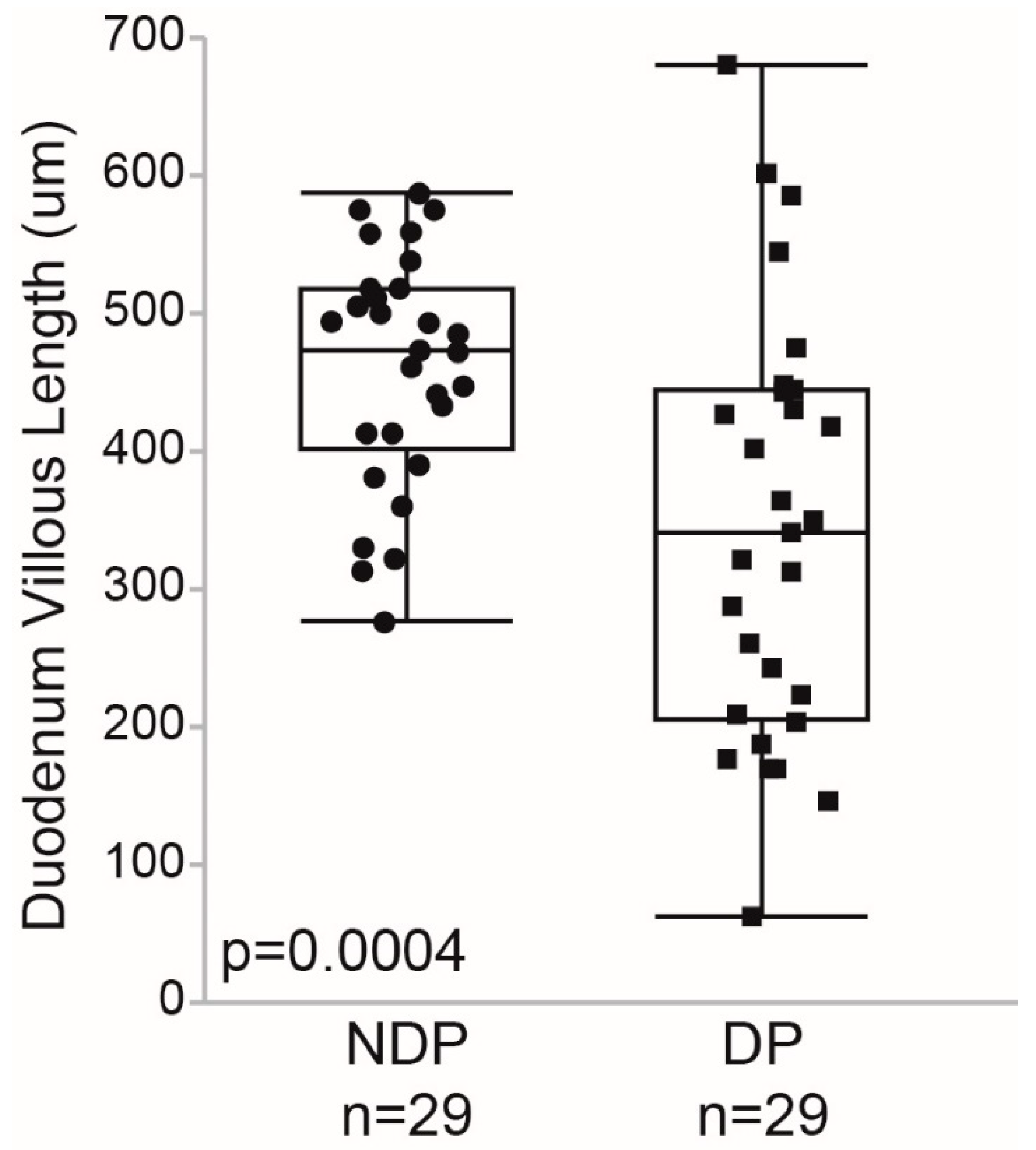
4.2. Duodenal Histopathology Review
4.3. Azathioprine Bioavailability Assessment
4.4. Statistical Analyses
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sonnenberg, A.; Melton, S.D.; Genta, R.M. Frequent occurrence of gastritis and duodenitis in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2011, 17, 39–44. [Google Scholar] [CrossRef] [PubMed]
- Diaz, L.; Hernandez-Oquet, R.E.; Deshpande, A.R.; Moshiree, B. Upper gastrointestinal involvement in Crohn Disease: Histopathologic and endoscopic findings. South Med. J. 2015, 108, 695–700. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.Z.; ten Kate, F.J.; Reitsma, J.B.; Benninga, M.A.; Kindermann, A. Additional value of upper GI tract endoscopy in the diagnostic assessment of childhood IBD. J. Pediatr. Gastroenterol. Nutr. 2012, 54, 753–757. [Google Scholar] [CrossRef] [PubMed]
- Tobin, J.M.; Sinha, B.; Ramani, P.; Saleh, A.R.; Murphy, M.S. Upper gastrointestinal mucosal disease in pediatric Crohn disease and ulcerative colitis: A blinded, controlled study. J. Pediatr. Gastroenterol. Nutr. 2001, 32, 443–448. [Google Scholar] [CrossRef] [PubMed]
- Lenaerts, C.; Roy, C.C.; Vaillancourt, M.; Weber, A.M.; Morin, C.L.; Seidman, E. High incidence of upper gastrointestinal tract involvement in children with Crohn’s disease. Pediatrics 1989, 83, 777–781. [Google Scholar] [CrossRef] [PubMed]
- Casini, R.; Cho, M.; Fioravanti, V.; Sing, V.; Shakhnovich, V. Prevalence of Duodenal Pathology in Pediatric Crohn’s Disease. J. Pediatr. Gastroenterol. Nutr. 2016, 63 (Suppl. 2), S82–S83. [Google Scholar]
- Gasparetto, M.; Guariso, G. Crohn’s disease and growth deficiency in children and adolescents. World J. Gastroenterol. 2014, 20, 13219–13233. [Google Scholar] [CrossRef] [PubMed]
- Johson, T.N.; Tanner, M.S.; Taylor, C.J.; Tucker, G.T. Enterocytic CYP3A4 in a paediatric population: Developmental changes and the effect of coeliac disease and cystic fibrosis. Br. J. Clin. Pharmacol. 2001, 51, 451–460. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boda, M.; Németh, I.; Boda, D. The caffeine metabolic ratio as an index of xanthine oxidase activity in clinically active and silent celiac patients. J. Pediatr. Gastroenterol. Nutr. 1999, 29, 546–550. [Google Scholar] [CrossRef] [PubMed]
- Shakhnovich, V.; Vyhlidal, C.; Friesen, C.; Hildreth, A.; Singh, V.; Daniel, J.; Kearns, G.L.; Leeder, J.S. Decreased pregnane X receptor expression in children with active Crohn’s disease. Drug Metab. Dispos. 2016, 44, 1066–1069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, A.; Tirona, R.G.; Kim, R.B. CYP3A4 Activity is Markedly Lower in Patients with Crohn’s Disease. Inflamm. Bowel Dis. 2017, 23, 804–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vyhlidal, C.A.; Chapron, B.D.; Ahmed, A.; Singh, V.; Casini, R.; Shakhnovich, V. Effect of Crohn’s disease on villous length and CYP3A4 expression in the pediatric small intestine. Clin. Transl. Sci. 2021, 14, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Ansari, A.; Aslam, Z.; De Sica, A.; Smith, M.; Gilshenan, K.; Fairbanks, L.; Marinaki, A.; Sanderson, J.; Duley, J. Influence of xanthine oxidase on thiopurine metabolism in Crohn’s disease. Ailment. Pharmacol. Ther. 2008, 28, 749–757. [Google Scholar] [CrossRef] [PubMed]
- Thiopurine Methyltransferase (TPMT) Activity Profile, Erythrocytes. Test Catalog. Mayo Clinic, Medical Laboratories, Rochester, MN 55904, USA. Available online: https://www.mayomedicallaboratories.com/test-catalog/ (accessed on 24 May 2018).
- Alrubia, S.; Mao, J.; Chen, Y.; Barber, J.; Rostami-Hodjegan, A. Altered Bioavailability and Pharmacokinetics in Crohn’s Disease: Capturing Systems Parameters for PBPK to Assist with Predicting the Fate of Orally Administered Drugs. Clin. Pharmacokinet. 2022, 61, 1365–1392. [Google Scholar] [CrossRef] [PubMed]
- Cosnes, J.; Cattan, S.; Blain, A.; Beaugerie, L.; Carbonnel, F.; Parc, R.; Gendre, J.-P. Long-term evolution of disease behavior of Crohn’s disease. Inflamm. Bowel Dis. 2002, 8, 244–250. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.S.; Kim, M.J. Upper gastrointestinal tract involvement of Crohn disease: Clinical implications in children and adolescents. Clin. Exp. Pediatr. 2022, 65, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Prometheus TPMT Enzyme. Test Catalog. Prometheus Laboratories, San Diego, CA 92121, USA. Available online: https://www.prometheuslabs.com/Resources/PTM/TPMT_Enzyme_Product_Detail_PTM16005_Feb_1_2016.pdf (accessed on 24 May 2018).
- Sandborn, W.J. Rational dosing of azathioprine and 6-mercaptopurine. Gut 2001, 48, 590–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moller, S.; Ahrenfeldt, L. Estimating Relative Risk When Observing Zero Events—Frequentist Inference and Bayesian Credibility Intervals. Int. J. Environ. Res. Public Health 2021, 18, 5527. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Demographic Information | Duodenal Pathology (n = 29) | No Duodenal Pathology (n = 29) | p-Value |
|---|---|---|---|
| Age (years) | 12.8 ± 3.4 | 13.2 ± 3.2 | 0.700 |
| % Female | 41.3% | 31.0% | 0.412 |
| Ethnicity | 79.3% White | 86.2% White | 0.706 |
| 17.2% Black | 6.9% Black | ||
| 3.4% Asian | 3.4% Asian | ||
| 0% Hispanic | 0% Hispanic | ||
| 0% Multiracial | 3.4% Multiracial | ||
| TPMT Normal Metabolizer Phenotype | Duodenal Pathology (n = 9) | No Duodenal Pathology (n = 10) | p-Value |
| Age (years) | 12.5 ± 2.8 | 13.1 ± 3.6 | 0.690 |
| % Female | 22.2% | 40.0% | 0.629 |
| Ethnicity | 88.9% White 11.1% Black | 100.0% White | 0.474 |
| All | DP (n = 29) | NDP (n = 29) | p-Value at Diagnosis | DP (n = 29) | NDP (n = 29) | p-Value at 9 Months |
|---|---|---|---|---|---|---|
| BMI z-score | −0.4 ± 1.5 | −0.7 ± 1.5 | 0.46 | −0.2 ± 1.2 | 0.4 ± 1.0 | 0.13 |
| White blood cells (mcL) | 9.1 ± 5.0 | 8.9 ± 3.0 | 0.83 | 7.5 ± 3.1 | 6.6 ± 1.6 | 0.29 |
| Hemoglobin (g/dL) | 11.0 ± 1.7 | 11.4 ± 1.9 | 0.38 | 12.5 ± 1.0 | 13.0 ± 1.4 | 0.27 |
| Platelets (mcL) | 425.5 ± 179.8 | 382.3 ± 142.3 | 0.31 | 335.2 ± 102.4 | 287.4 ± 77.7 | 0.14 |
| Albumin (g/dL) | 3.5 ± 0.7 | 3.6 ± 0.6 | 0.35 | 4.3 ± 0.4 | 4.3 ± 0.4 | 0.92 |
| ESR (mm/hr) | 37.0 (18, 59) | 19.5 (13,44.5) | 0.13 | 13.5 (8.0, 17.0) | 10.0 (7.0, 17.5) | 0.61 |
| CRP (mg/dL) | 2.5 (0.8, 4.2) | 3.2 (1.3, 5.5) | 0.41 | 0.6 (0.4, 1.1) | 0.6 (0.5, 0.7) | 1.0 |
| DP (n = 9) | NDP (n = 10) | Relevant Statistics | |
|---|---|---|---|
| AZA dose (mg/kg/day) | 2.5 (2.3, 2.6) | 2.2 (2.0, 2.2) | p = 0.006 |
| 6-MMPN | 0 hepatotoxic 9 normal | 1 hepatotoxic 9 normal | RR = 1.11 (95% CI 0.08, 15.28) |
| 6-TGN | 5 sub-therapeutic 4 therapeutic | 3 sub-therapeutic 7 therapeutic | RR = 1.85 (95% CI 0.61, 5.63) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Casini, R.; Vyhlidal, C.A.; Bracken, J.M.; Sherman, A.K.; Ahmed, A.; Singh, V.; Williams, V.; Shakhnovich, V. Impact of Duodenal Pathology on Oral Drug Bioavailability and Disease Outcomes in Pediatric Crohn’s Disease. Pharmaceuticals 2023, 16, 373. https://doi.org/10.3390/ph16030373
Casini R, Vyhlidal CA, Bracken JM, Sherman AK, Ahmed A, Singh V, Williams V, Shakhnovich V. Impact of Duodenal Pathology on Oral Drug Bioavailability and Disease Outcomes in Pediatric Crohn’s Disease. Pharmaceuticals. 2023; 16(3):373. https://doi.org/10.3390/ph16030373
Chicago/Turabian StyleCasini, Rebecca, Carrie A. Vyhlidal, Julia M. Bracken, Ashley K. Sherman, Atif Ahmed, Vivekanand Singh, Veronica Williams, and Valentina Shakhnovich. 2023. "Impact of Duodenal Pathology on Oral Drug Bioavailability and Disease Outcomes in Pediatric Crohn’s Disease" Pharmaceuticals 16, no. 3: 373. https://doi.org/10.3390/ph16030373