
Personalised 3D-Printed Mucoadhesive Gastroretentive Hydrophilic Matrices for Managing Overactive Bladder (OAB)
 , and
, and 
Abstract
:1. Introduction
2. Results and Discussion
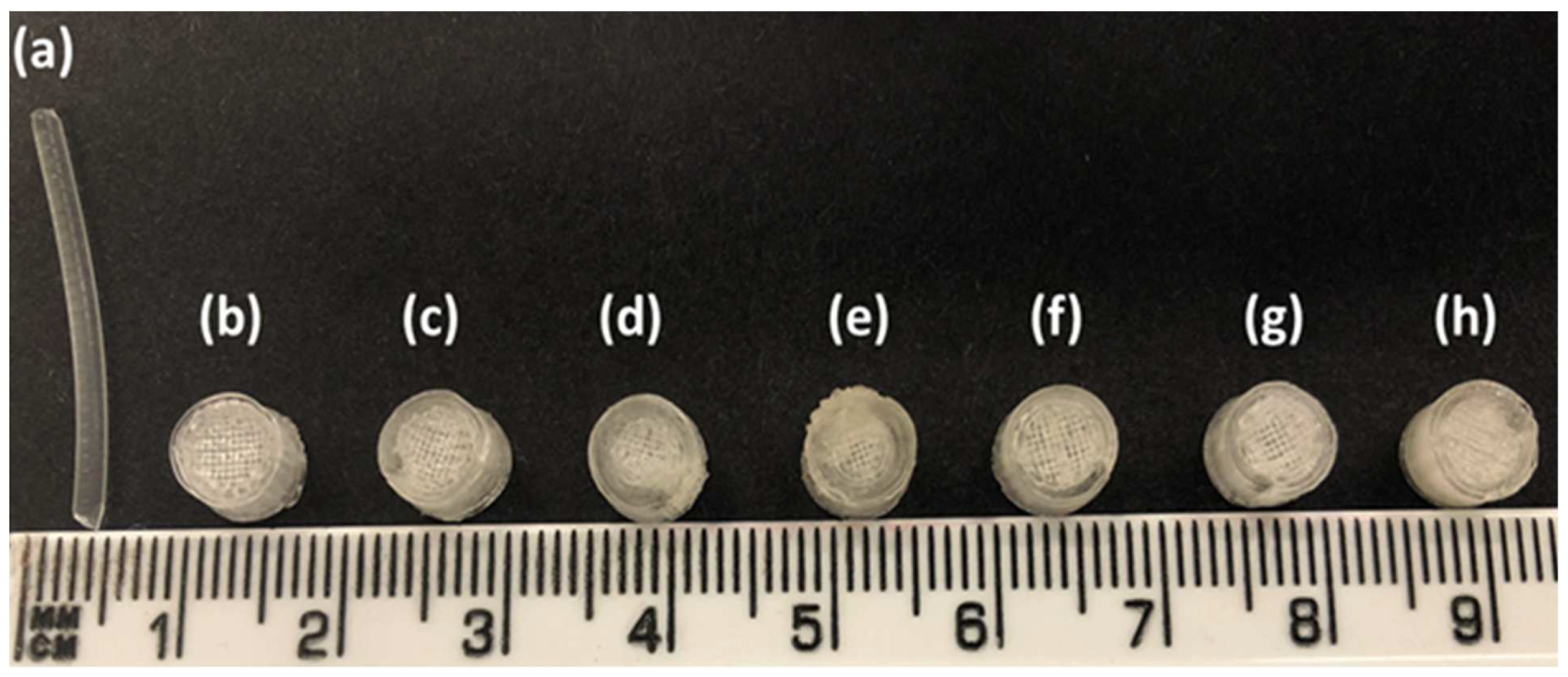
2.1. Development and Characterisation of Filaments
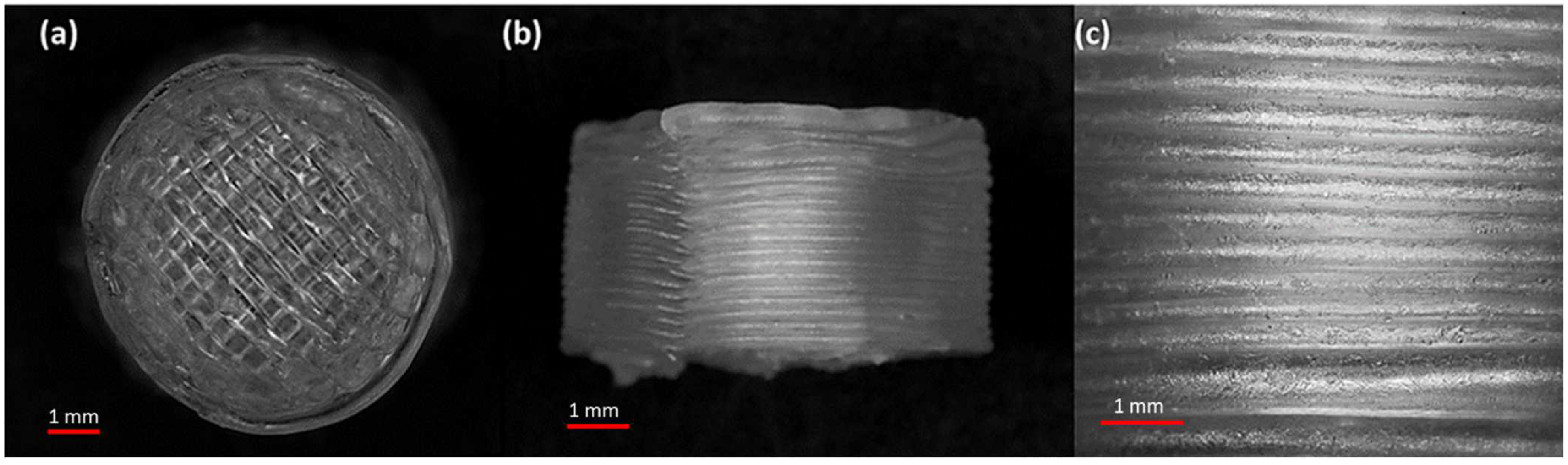
2.2. Development and Characterisation of 3D-Printed Matrix Tablets
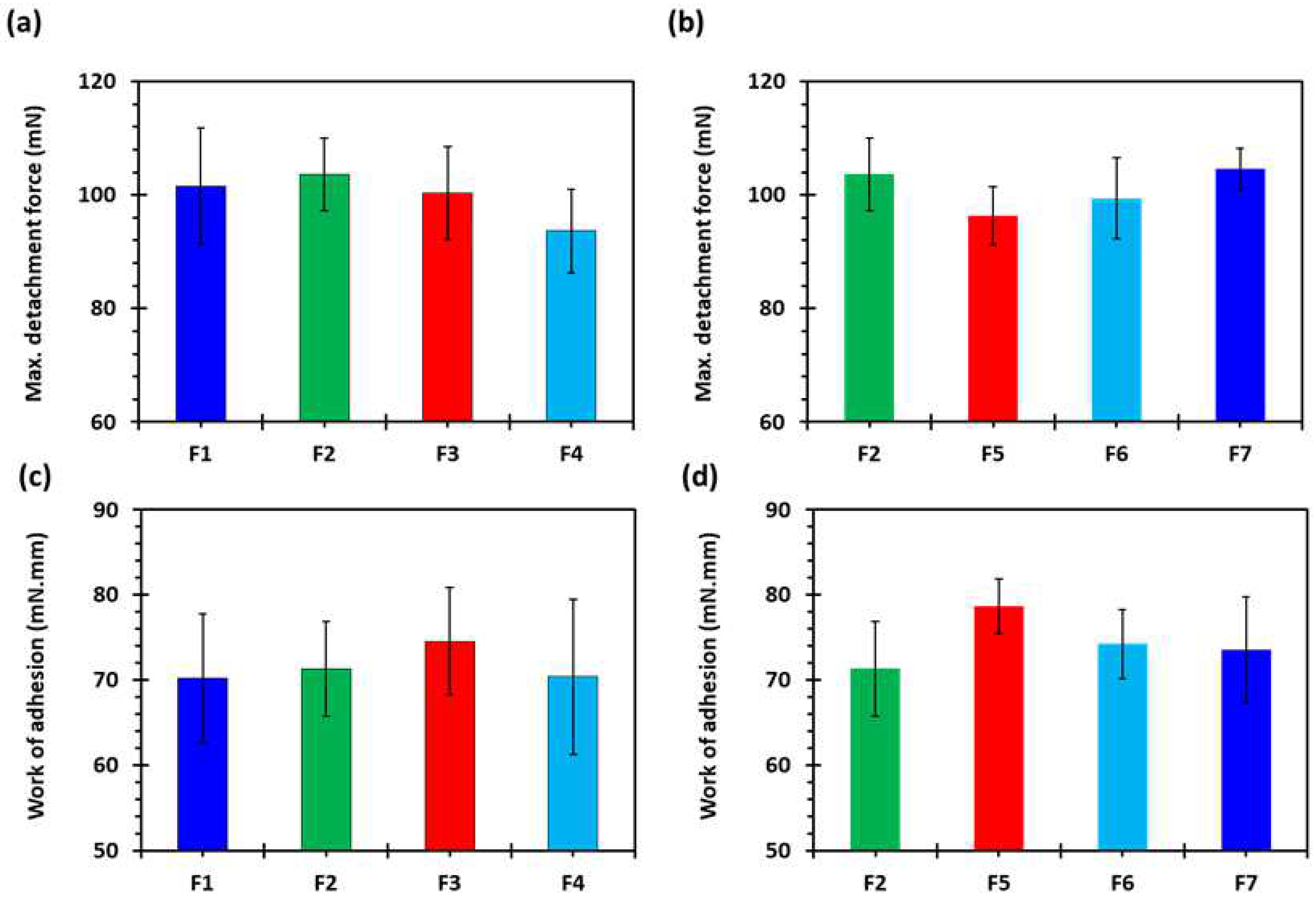
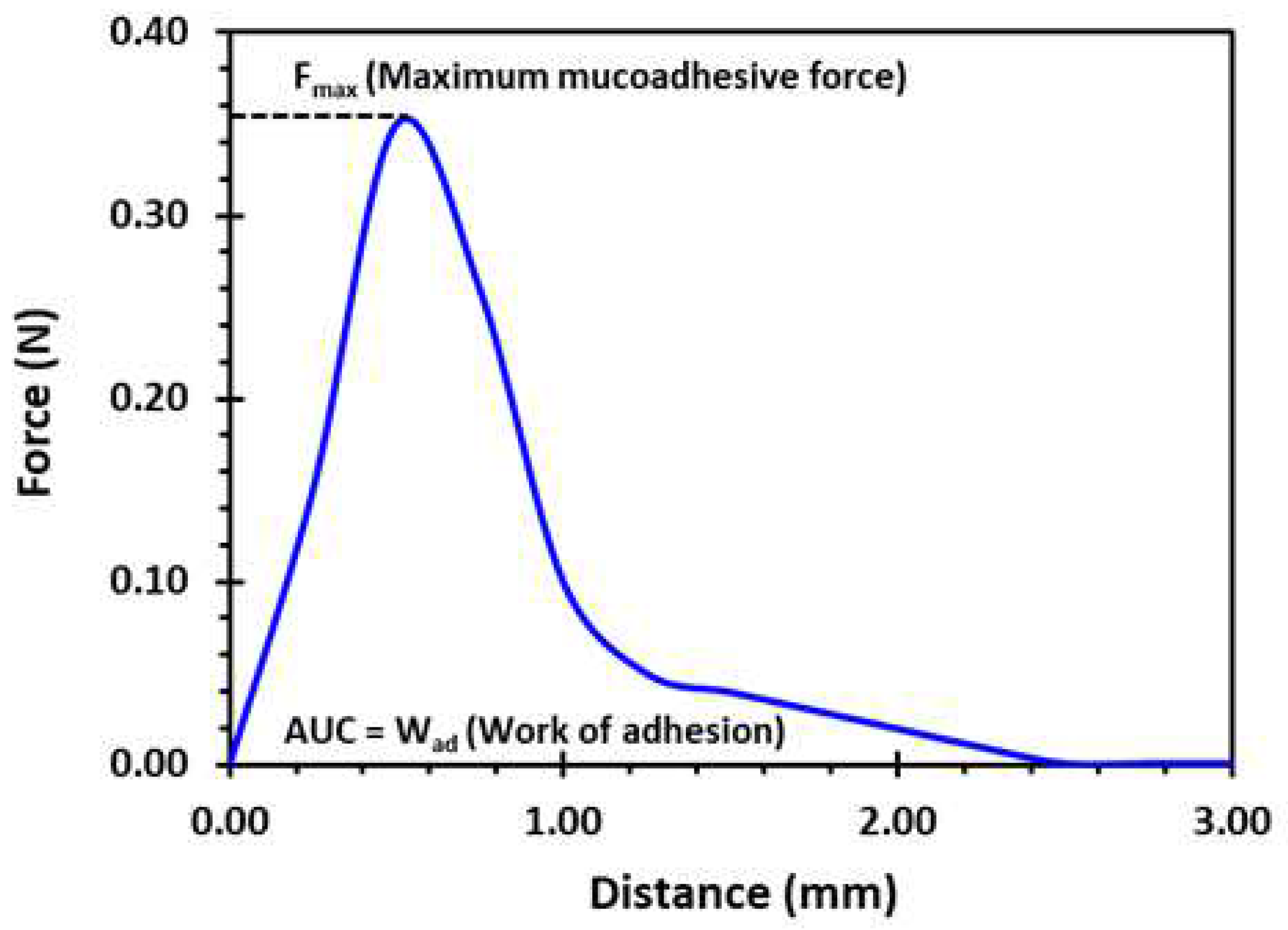
2.3. Ex Vivo Mucoadhesion Studies
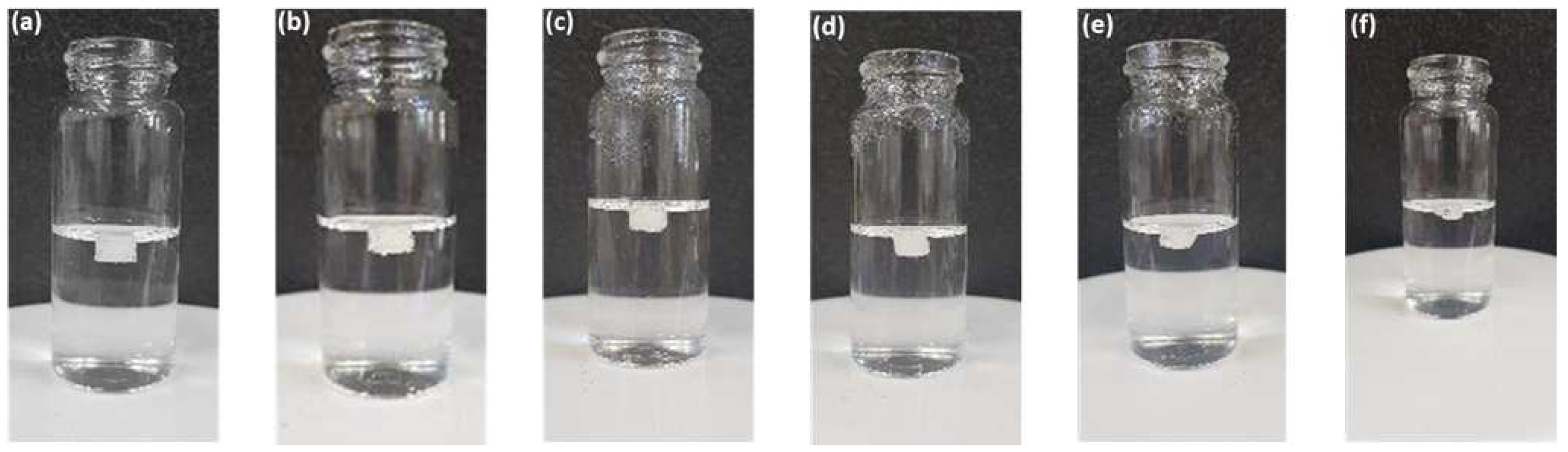
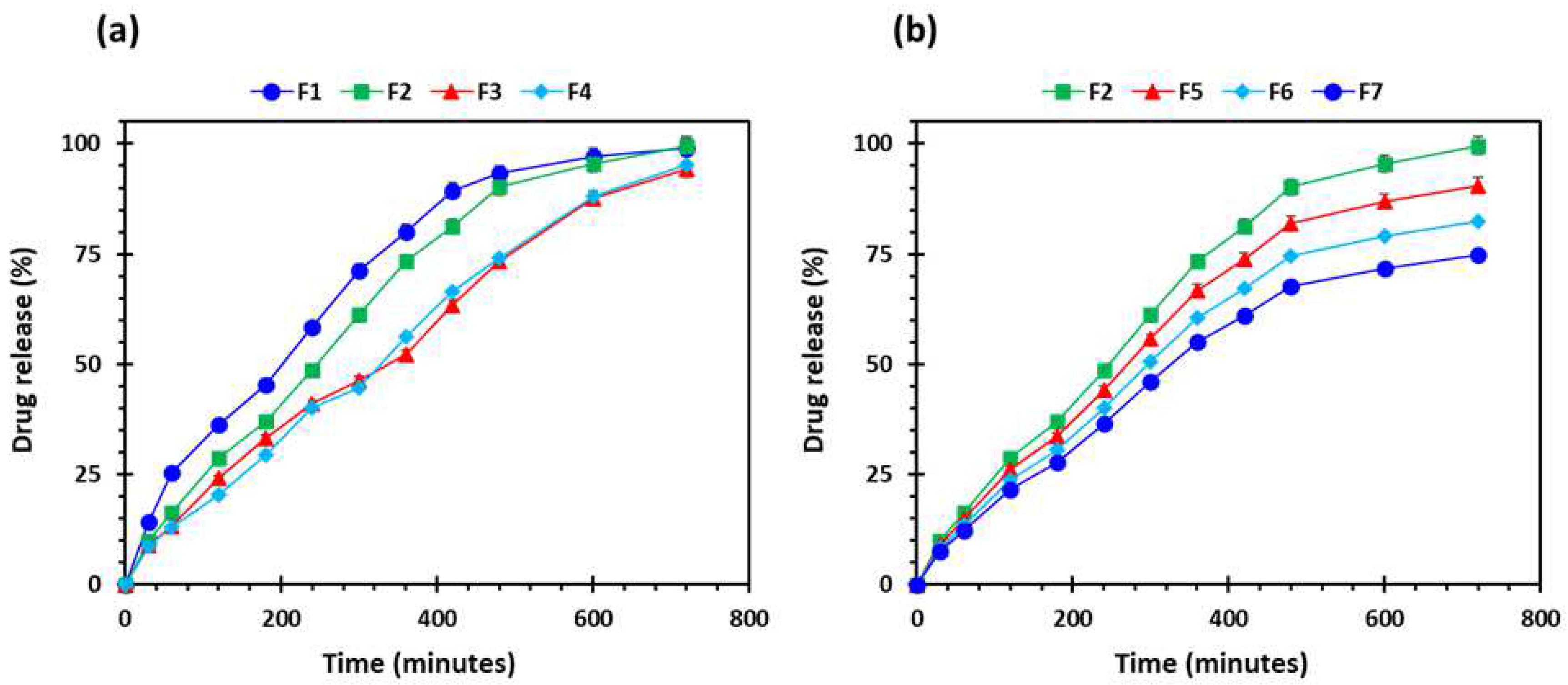
2.4. In Vitro Floating and Drug Release Studies
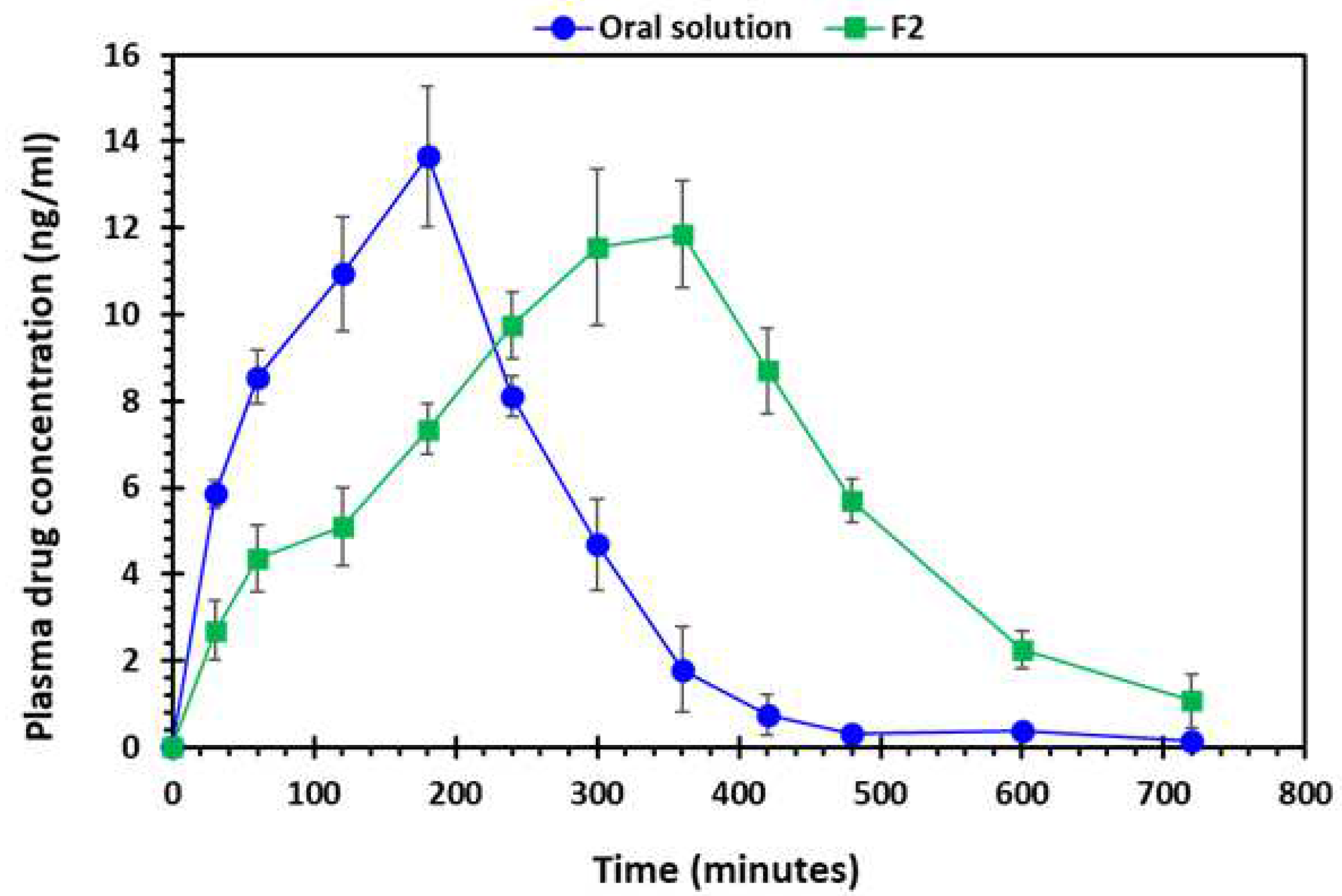
2.5. Pharmacokinetic (In Vivo Drug Absorption) Studies
3. Materials and Methods
3.1. Materials
3.2. Preparation of Filaments
3.3. Physicochemical Characterisation of Filaments
3.3.1. Determination of Drug Loading
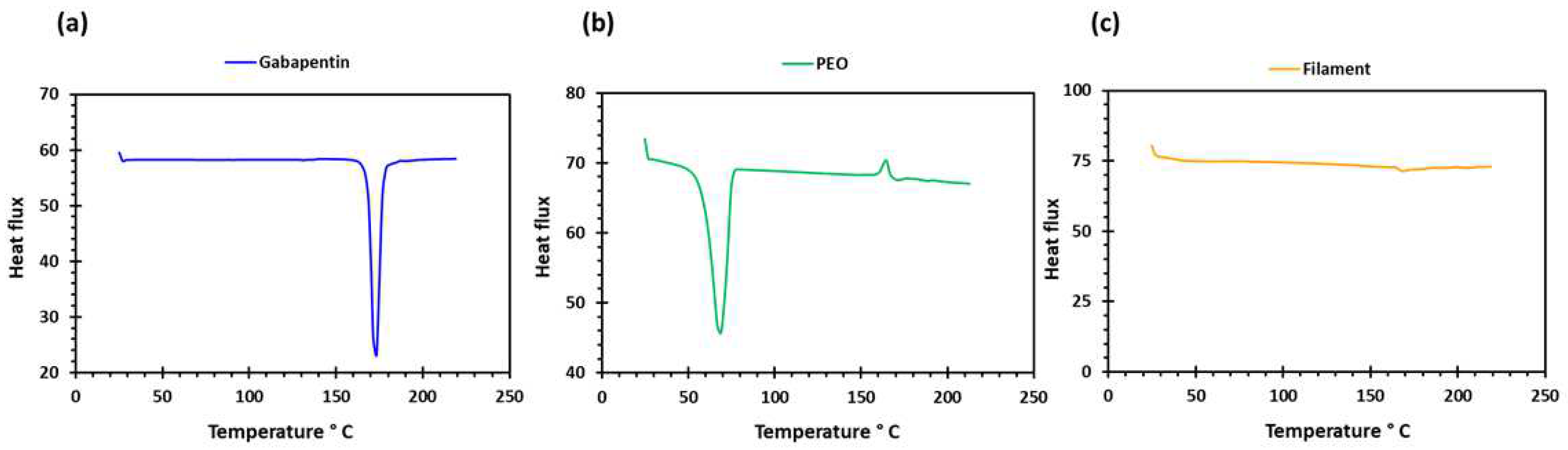
3.3.2. Differential Scanning Calorimetry (DSC)
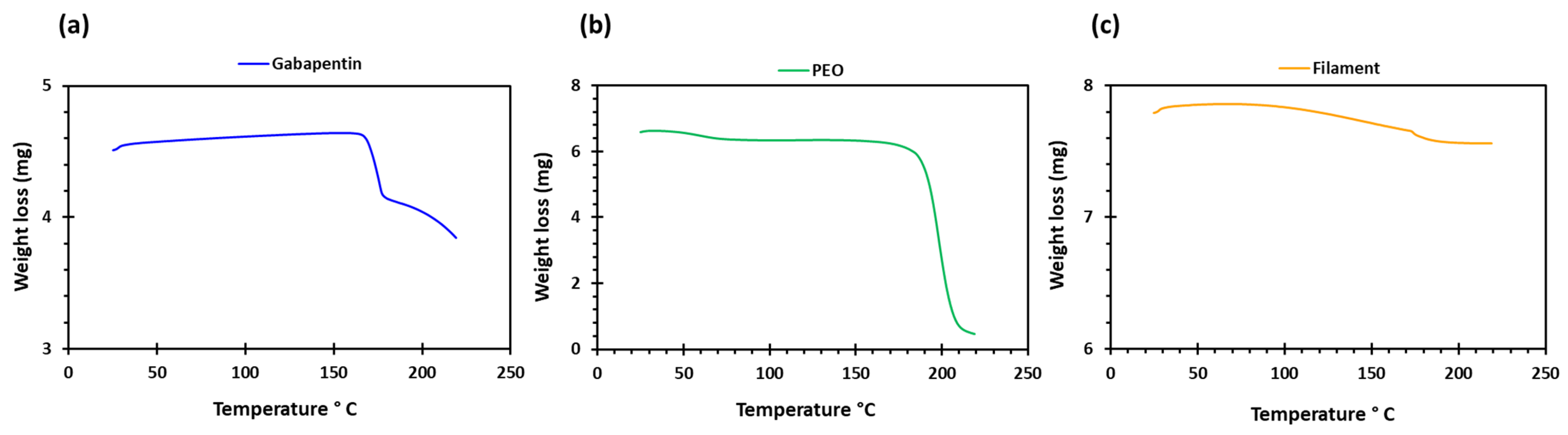
3.3.3. Thermogravimetric Analysis (TGA)
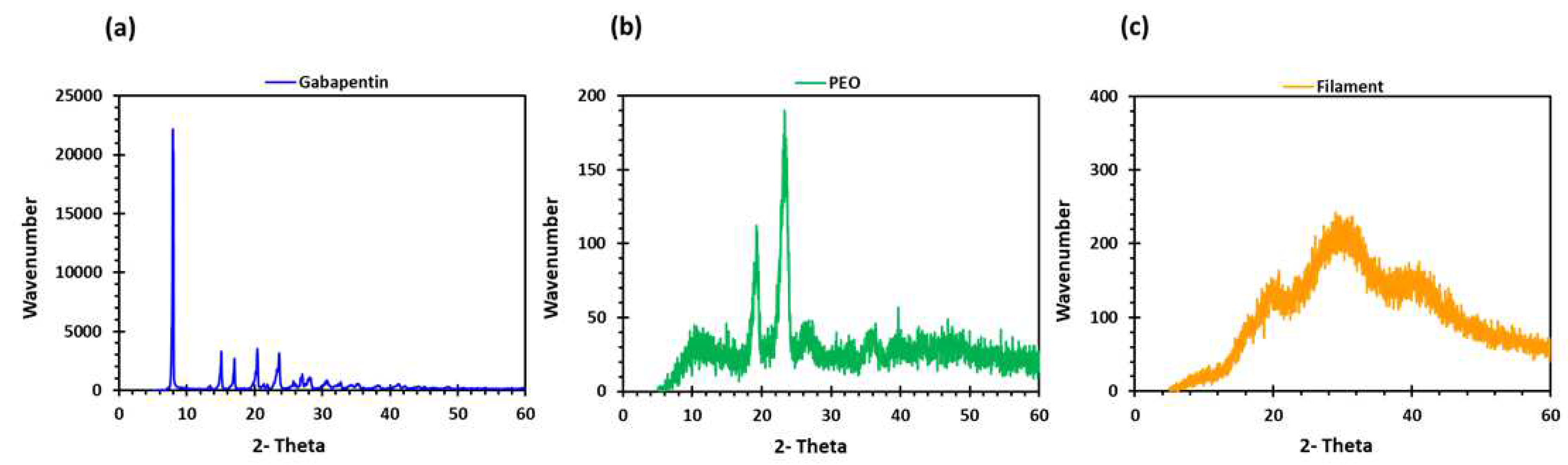
3.3.4. X-ray Diffraction Studies (XRD)
3.3.5. Scanning Electron Microscopy (SEM)
3.3.6. Mechanical Testing of Filaments
3.3.7. Fabrication of 3D Printed Tablets
3.4. Characterisation of 3D Printed Matrix Tablets
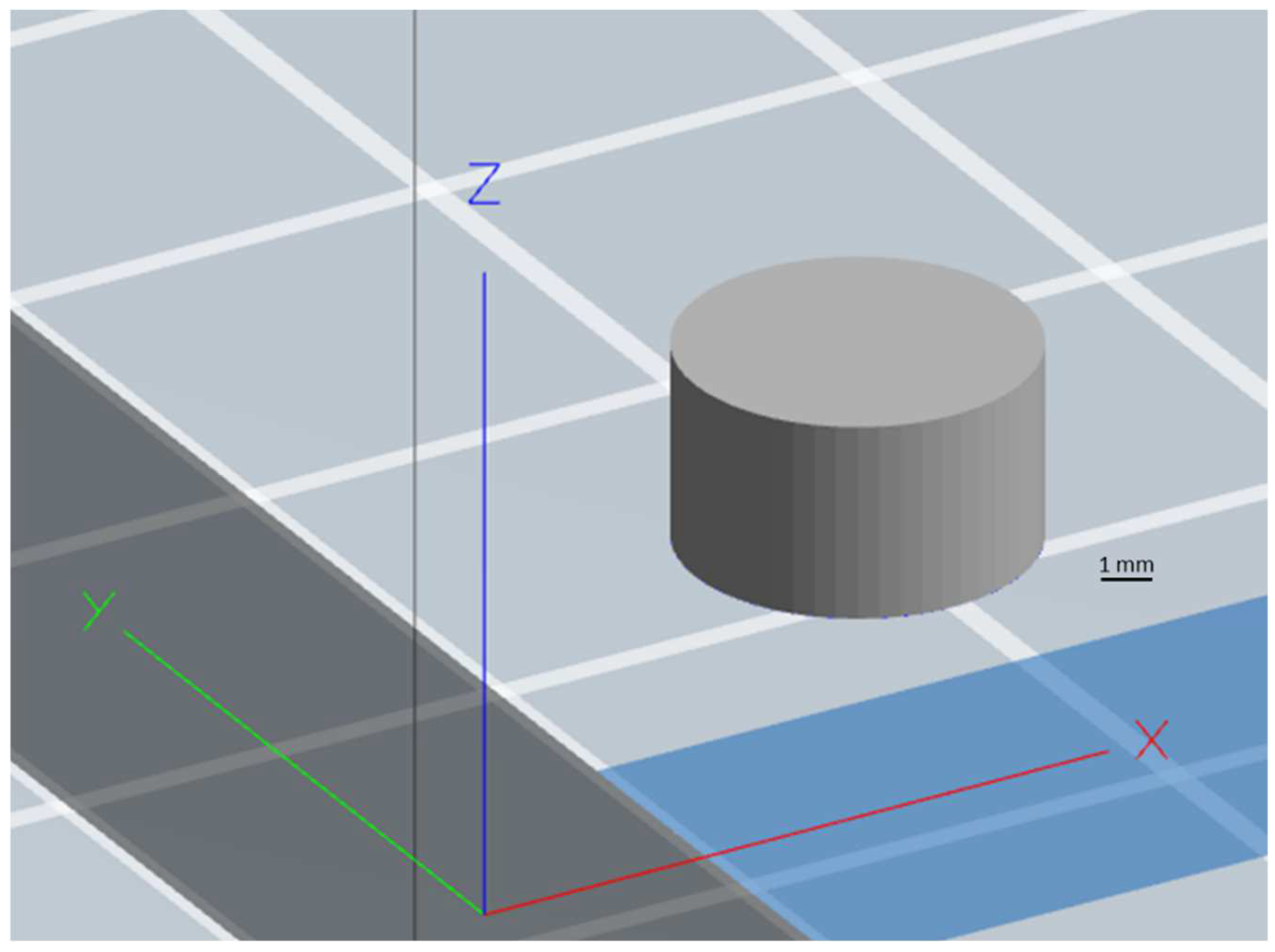
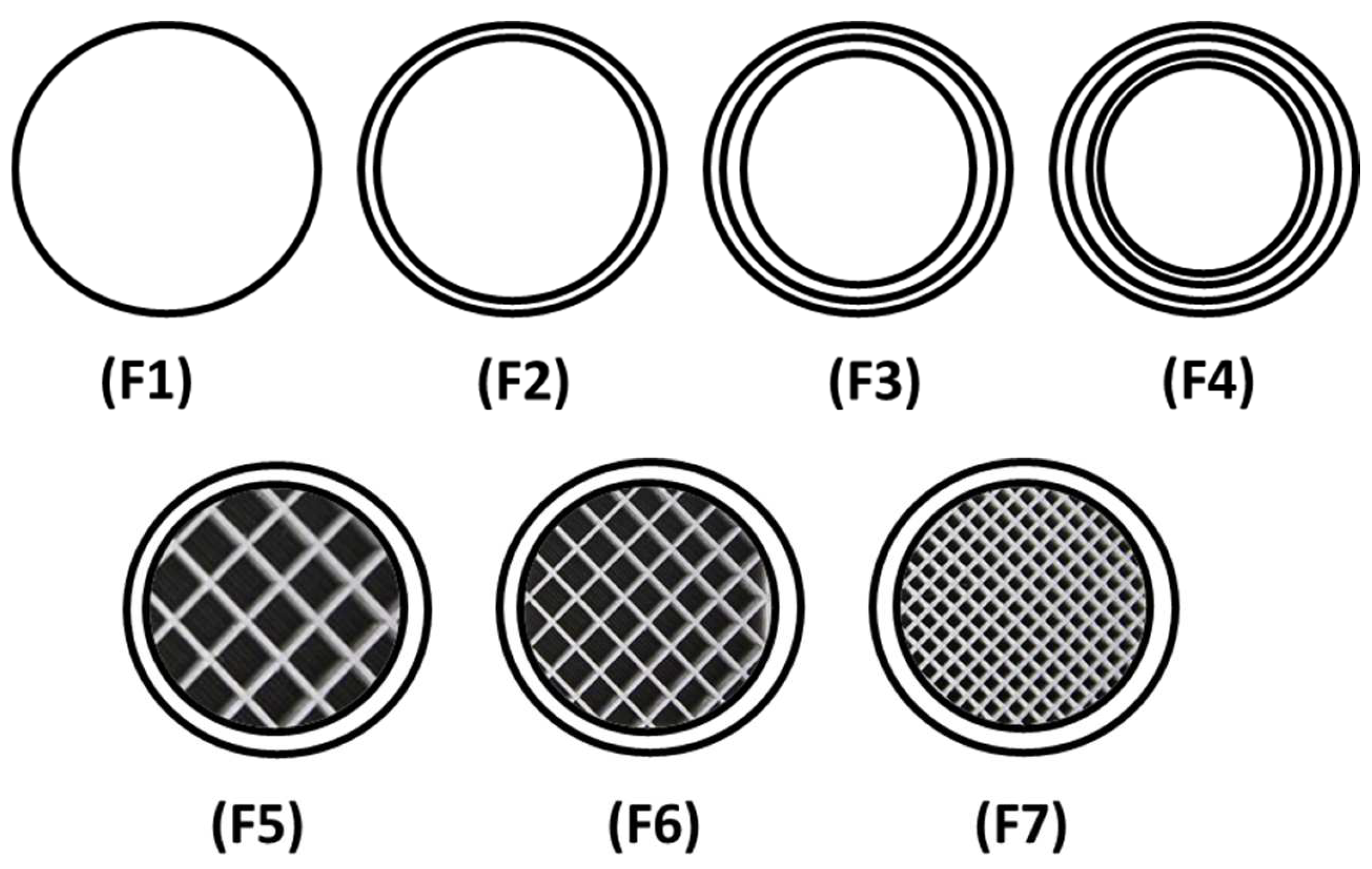
3.4.1. Geometrical and Morphological Assessment of Matrices
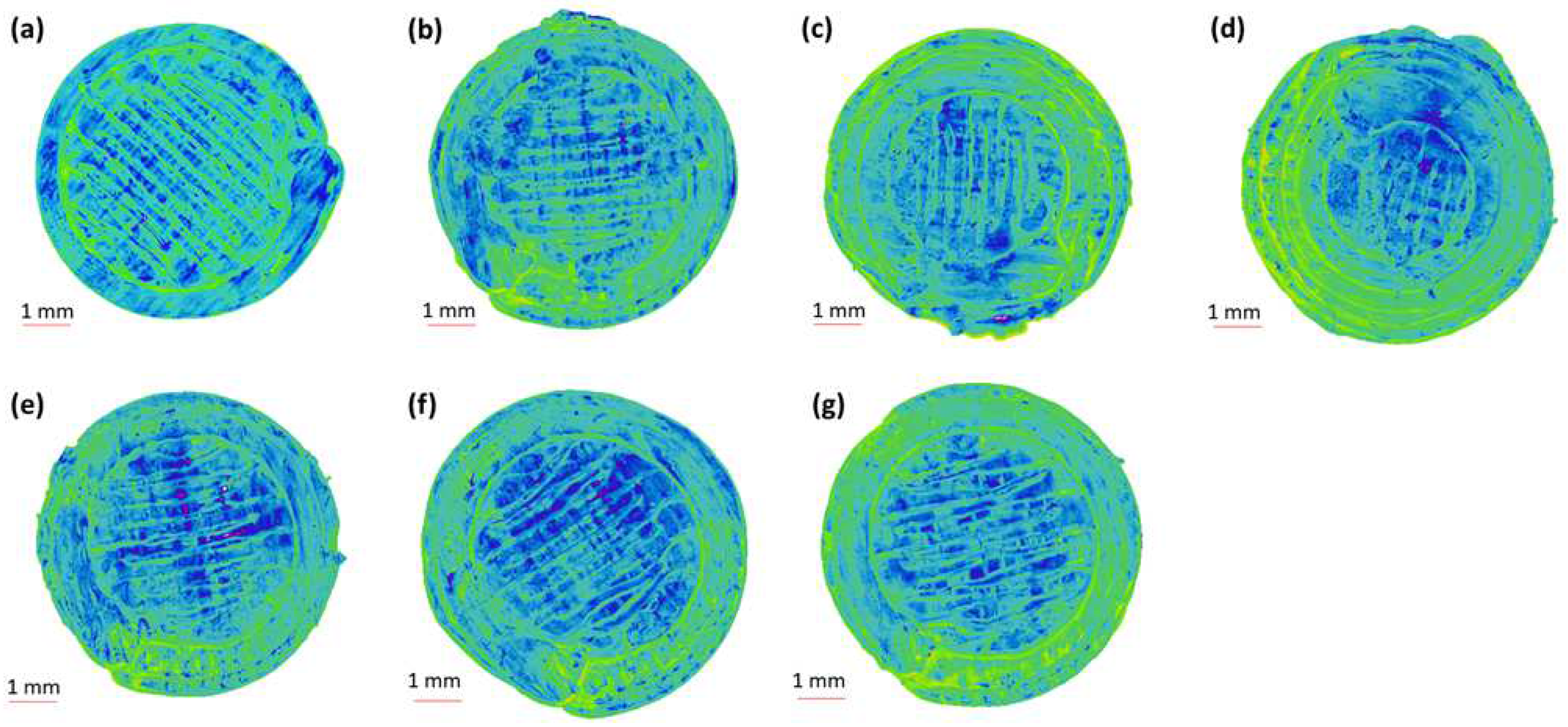
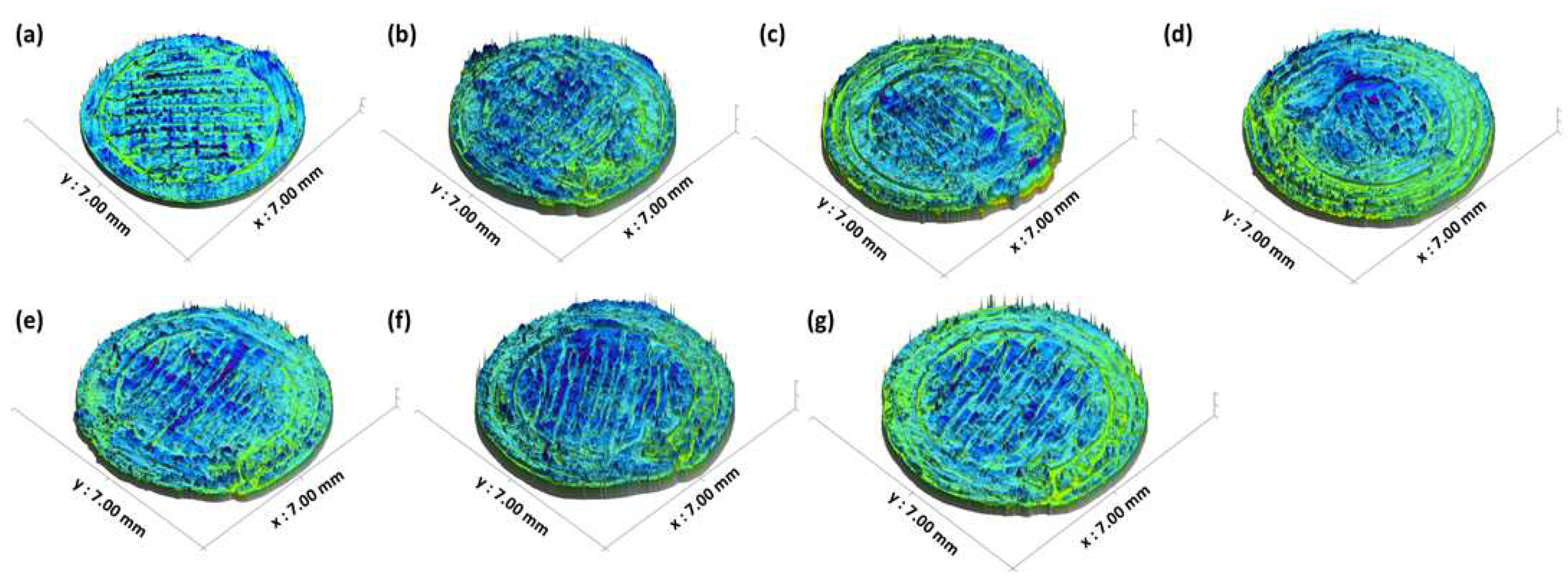
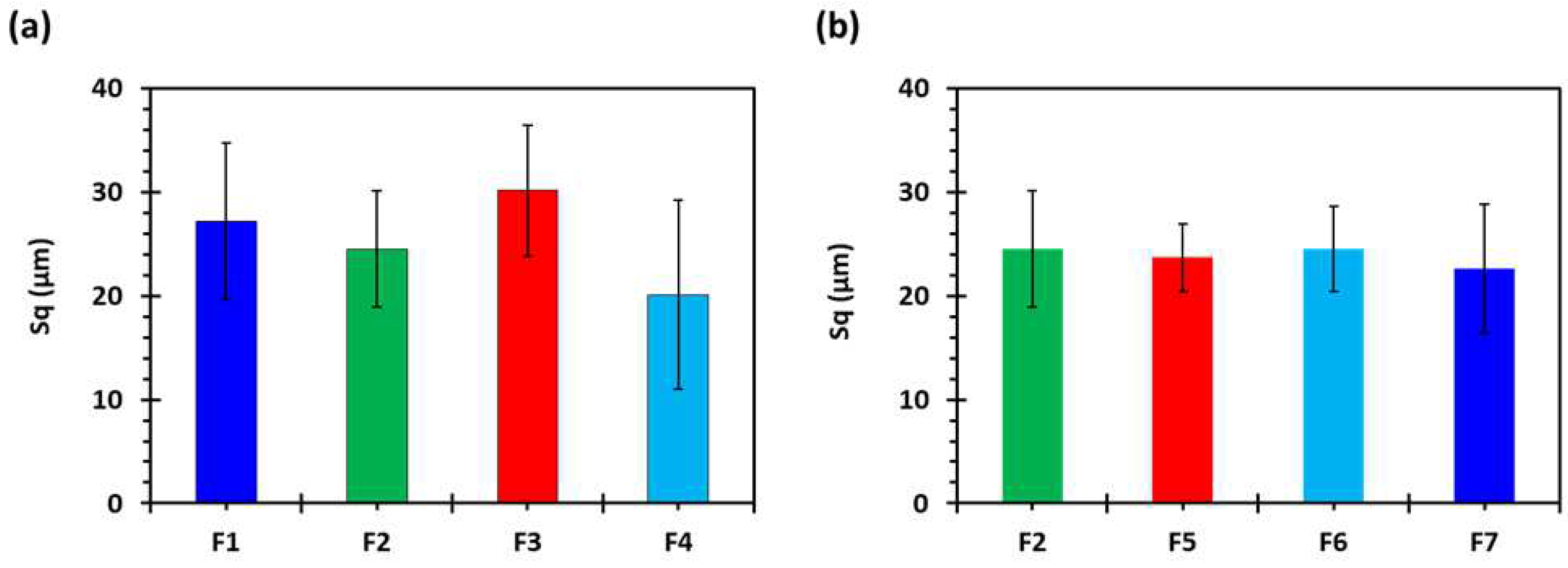
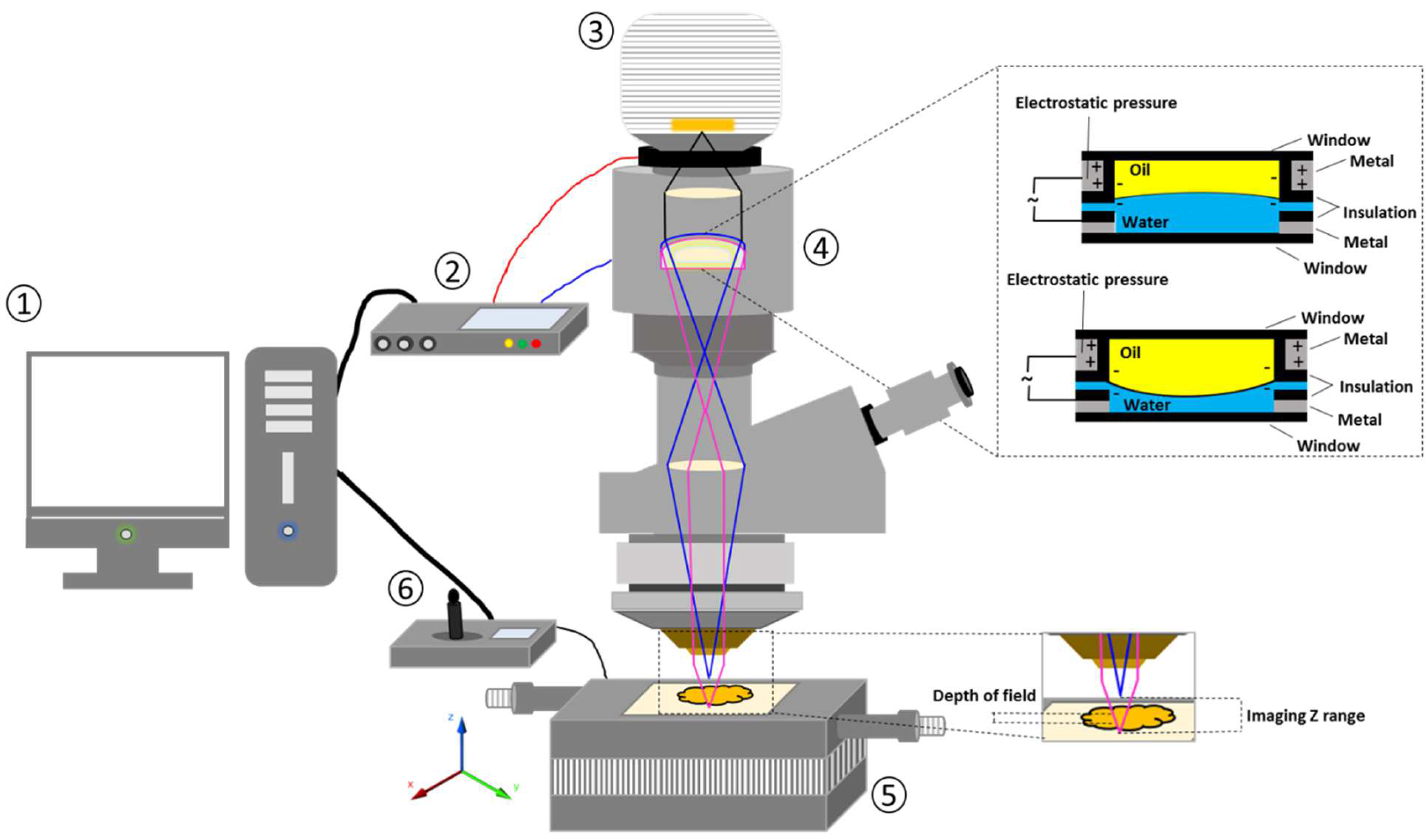
3.4.2. Three-Dimensional Surface Texture Analysis
3.4.3. Determination of Tablet Strength
3.4.4. Determination of Tablet Friability
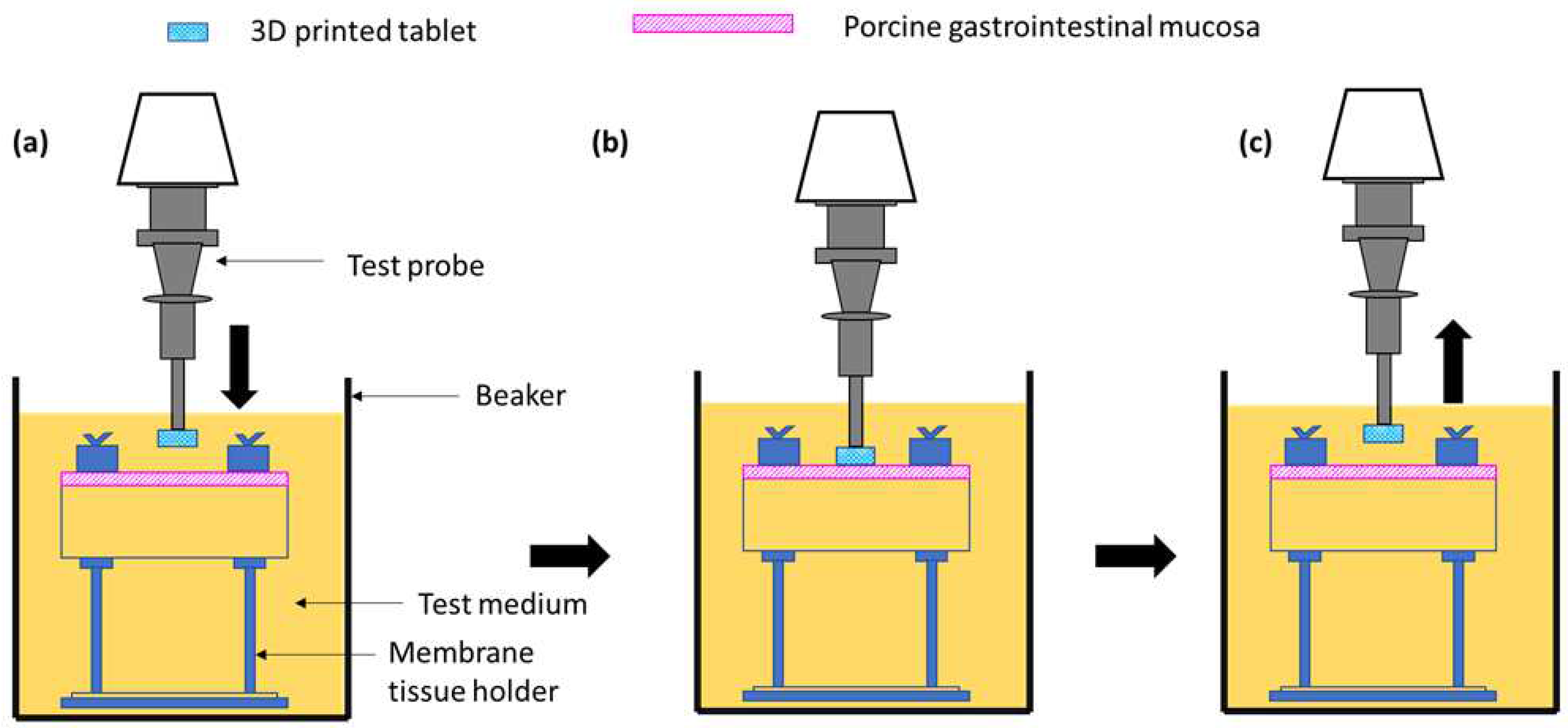
3.4.5. Ex Vivo Mucoadhesive Studies
3.4.6. In Vitro Dissolution Testing
3.4.7. Floating Test
3.4.8. Pharmacokinetic Studies
3.4.9. Statistical Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Haylen, B.T.; De Ridder, D.; Freeman, R.M.; Swift, S.E.; Berghmans, B.; Lee, J.; Monga, A.; Petri, E.; Rizk, D.E.; Sand, P.K. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol. Urodyn. Off. J. Int. Cont. Soc. 2010, 29, 4–20. [Google Scholar] [CrossRef]
- Arnold, J.; McLeod, N.; Thani-Gasalam, R.; Rashid, P. Overactive bladder syndrome: Management and treatment options. Aust. Fam. Physician 2012, 41, 878. [Google Scholar]
- Franco, I. Overactive bladder in children. Part 1: Pathophysiology. J. Urol. 2007, 178, 761–768. [Google Scholar] [CrossRef]
- Irwin, D.E.; Milsom, I.; Hunskaar, S.; Reilly, K.; Kopp, Z.; Herschorn, S.; Coyne, K.; Kelleher, C.; Hampel, C.; Artibani, W. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: Results of the EPIC study. Eur. Urol. 2006, 50, 1306–1315. [Google Scholar] [CrossRef]
- Botlero, R.; Davis, S.R.; Urquhart, D.M.; Bell, R.J. Incidence and resolution rates of different types of urinary incontinence in women: Findings from a cohort study. J. Urol. 2011, 185, 1331–1337. [Google Scholar] [CrossRef]
- Wolff, G.F.; Kuchel, G.A.; Smith, P.P. Overactive bladder in the vulnerable elderly. Res. Rep. Urol. 2014, 6, 131–138. [Google Scholar] [CrossRef] [Green Version]
- Carbone, A.; Palleschi, G.; Conte, A.; Bova, G.; Iacovelli, E.; Bettolo, R.M.; Pastore, A.; Inghilleri, M. Gabapentin treatment of neurogenic overactive bladder. Clin. Neuropharmacol. 2006, 29, 206–214. [Google Scholar] [CrossRef]
- Ansari, M.S.; Bharti, A.; Kumar, R.; Ranjan, P.; Srivastava, A.; Kapoor, R. Gabapentin: A novel drug as add-on therapy in cases of refractory overactive bladder in children. J. Pediatr. Urol. 2013, 9, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Kurpad, R.; Kennelly, M.J. The Evaluation and Management of Refractory Neurogenic Overactive Bladder. Curr. Urol. Rep. 2014, 15, 444. [Google Scholar] [CrossRef]
- Wein, A.J.; Rackley, R.R. Overactive bladder: A better understanding of pathophysiology, diagnosis and management. J. Urol. 2006, 175, S5–S10. [Google Scholar] [CrossRef]
- Andersson, K.-E. Bladder activation: Afferent mechanisms. Urology 2002, 59, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Tsakiris, P.; Oelke, M.; Michel, M.C. Drug-Induced Urinary Incontinence. Drugs Aging 2008, 25, 541–549. [Google Scholar] [CrossRef] [PubMed]
- Andersson, K.-E. Treatment of the overactive bladder: Possible central nervous system drug targets. Urology 2002, 59, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Zinner, N.; Susset, J.; Gittelman, M.; Arguinzoniz, M.; Rekeda, L.; Haab, F. Efficacy, tolerability and safety of darifenacin, an M3 selective receptor antagonist: An investigation of warning time in patients with OAB. Int. J. Clin. Pract. 2006, 60, 119–126. [Google Scholar] [CrossRef] [PubMed]
- MacDiarmid, S.A. Maximizing anticholinergic therapy for overactive bladder: Has the ceiling been reached? BJU Int. 2007, 99, 8–12. [Google Scholar] [CrossRef]
- Madhuvrata, P.; Cody, J.D.; Ellis, G.; Herbison, G.P.; Hay-Smith, E.J.C. Which anticholinergic drug for overactive bladder symptoms in adults. Cochrane Database Syst. Rev. 2012, 1, CD005429. [Google Scholar] [CrossRef]
- Wang, A.C.; Chih, S.-Y.; Chen, M.-C. Comparison of electric stimulation and oxybutynin chloride in management of overactive bladder with special reference to urinary urgency: A randomized placebo-controlled trial. Urology 2006, 68, 999–1004. [Google Scholar] [CrossRef]
- Verpoorten, C.; Buyse, G.M. The neurogenic bladder: Medical treatment. Pediatr. Nephrol. 2008, 23, 717–725. [Google Scholar] [CrossRef] [Green Version]
- Rosa, G.M.; Bauckneht, M.; Scala, C.; Tafi, E.; Leone Roberti Maggiore, U.; Ferrero, S.; Brunelli, C. Cardiovascular effects of antimuscarinic agents in overactive bladder. Expert Opin. Drug Saf. 2013, 12, 815–827. [Google Scholar] [CrossRef]
- Gopal, M.; Haynes, K.; Bellamy, S.L.; Arya, L.A. Discontinuation rates of anticholinergic medications used for the treatment of lower urinary tract symptoms. Obstet. Gynecol. 2008, 112, 1311–1318. [Google Scholar] [CrossRef]
- Basra, R.K.; Wagg, A.; Chapple, C.; Cardozo, L.; Castro-Diaz, D.; Pons, M.E.; Kirby, M.; Milsom, I.; Vierhout, M.; Van Kerrebroeck, P. A review of adherence to drug therapy in patients with overactive bladder. BJU Int. 2008, 102, 774–779. [Google Scholar] [CrossRef]
- Cruz, F.; Silva, C. Refractory neurogenic detrusor overactivity. Int. J. Clin. Pract. 2006, 60, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Andersson, K.-E. Prospective pharmacologic therapies for the overactive bladder. Ther. Adv. Urol. 2009, 1, 71–83. [Google Scholar] [CrossRef]
- Birder, L.A.; De Groat, W.C. Mechanisms of disease: Involvement of the urothelium in bladder dysfunction. Nat. Clin. Pract. Urol. 2007, 4, 46–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wein, A.J. CNS Involvement in Overactive Bladder. Pathophysiology and Opportunities for Pharmacological Intervention. J. Urol. 2004, 172, 2502–2503. [Google Scholar] [CrossRef]
- Striano, P.; Striano, S. Gabapentin: A Ca2+ channel alpha 2-delta ligand far beyond epilepsy therapy. Drugs Today 2008, 44, 353–368. [Google Scholar] [CrossRef] [PubMed]
- Maneuf, Y.; Gonzalez, M.; Sutton, K.; Chung, F.-Z.; Pinnock, R.; Lee, K. Cellular and molecular action of the putative GABA-mimetic, gabapentin. Cell. Mol. Life Sci. CMLS 2003, 60, 742–750. [Google Scholar]
- Yoshimura, N.; Chancellor, M.B. Current and future pharmacological treatment for overactive bladder. J. Urol. 2002, 168, 1897–1913. [Google Scholar] [CrossRef]
- Hansen, H.C. Interstitial cystitis and the potential role of gabapentin. South. Med. J. 2000, 93, 238–242. [Google Scholar] [CrossRef]
- Kim, Y.T.; Kwon, D.D.; Kim, J.; Kim, D.K.; Lee, J.Y.; Chancellor, M.B. Gabapentin for overactive bladder and nocturia after anticholinergic failure. Int. Braz. J. Urol. 2004, 30, 275–278. [Google Scholar] [CrossRef]
- Chang, C.Y.; Challa, C.K.; Shah, J.; Eloy, J.D. Gabapentin in acute postoperative pain management. BioMed Res. Int. 2014, 1–7, 1756. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beydoun, A.; Uthman, B.M.; Sackellares, J.C. Gabapentin: Pharmacokinetics, efficacy, and safety. Clin. Neuropharmacol. 1995, 18, 469–481. [Google Scholar] [CrossRef] [PubMed]
- Clarke’s Analysis of Drugs and Poisons. Available online: https://www.medicinescomplete.com/#/content/clarke/CLK0777 (accessed on 22 February 2023).
- Stewart, B.H.; Kugler, A.R.; Thompson, P.R.; Bockbrader, H.N. A saturable transport mechanism in the intestinal absorption of gabapentin is the underlying cause of the lack of proportionality between increasing dose and drug levels in plasma. Pharm. Res. 1993, 10, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Uchino, H.; Kanai, Y.; Kim, D.K.; Wempe, M.F.; Chairoungdua, A.; Morimoto, E.; Anders, M.; Endou, H. Transport of amino acid-related compounds mediated by L-type amino acid transporter 1 (LAT1): Insights into the mechanisms of substrate recognition. Mol. Pharmacol. 2002, 61, 729–737. [Google Scholar] [CrossRef] [Green Version]
- Kagan, L.; Hoffman, A. Biopharmaceutical aspects of gastro-retentive dosage forms: The gabapentin paradigm. J. Drug Deliv. Sci. Technol. 2009, 19, 233–239. [Google Scholar] [CrossRef]
- Murphy, C.; Pillay, V.; Choonara, Y.E.; du Toit, L.C.; Ndesendo, V.M.; Chirwa, N.; Kumar, P. Optimization of a dual mechanism gastrofloatable and gastroadhesive delivery system for narrow absorption window drugs. AAPS PharmSciTech 2012, 13, 1–15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Claxton, A.J.; Cramer, J.; Pierce, C. A systematic review of the associations between dose regimens and medication compliance. Clin. Ther. 2001, 23, 1296–1310. [Google Scholar] [CrossRef]
- Rice, A.; Maton, S.; Group1UK, P.N.S. Gabapentin in postherpetic neuralgia: A randomised, double blind, placebo controlled study. Pain 2001, 94, 215–224. [Google Scholar] [CrossRef]
- Lopes, C.M.; Bettencourt, C.; Rossi, A.; Buttini, F.; Barata, P. Overview on gastroretentive drug delivery systems for improving drug bioavailability. Int. J. Pharm. 2016, 510, 144–158. [Google Scholar] [CrossRef]
- Arora, S.; Ali, J.; Ahuja, A.; Khar, R.K.; Baboota, S. Floating drug delivery systems: A review. Aaps PharmSciTech 2005, 6, E372–E390. [Google Scholar] [CrossRef] [Green Version]
- Kotreka, U.; Adeyeye, M.C. Gastroretentive floating drug-delivery systems: A critical review. Crit. Rev. ™ Ther. Drug Carr. Syst. 2011, 28, 287. [Google Scholar] [CrossRef]
- Goyanes, A.; Kobayashi, M.; Martínez-Pacheco, R.; Gaisford, S.; Basit, A.W. Fused-filament 3D printing of drug products: Microstructure analysis and drug release characteristics of PVA-based caplets. Int. J. Pharm. 2016, 514, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Goyanes, A.; Buanz, A.B.; Hatton, G.B.; Gaisford, S.; Basit, A.W. 3D printing of modified-release aminosalicylate (4-ASA and 5-ASA) tablets. Eur. J. Pharm. Biopharm. 2015, 89, 157–162. [Google Scholar] [CrossRef] [PubMed]
- Pietrzak, K.; Isreb, A.; Alhnan, M.A. A flexible-dose dispenser for immediate and extended release 3D printed tablets. Eur. J. Pharm. Biopharm. 2015, 96, 380–387. [Google Scholar] [CrossRef] [PubMed]
- Edgar, J.; Tint, S. Additive manufacturing technologies: 3D printing, rapid prototyping, and direct digital manufacturing. Johns. Matthey Technol. Rev. 2015, 59, 193–198. [Google Scholar] [CrossRef]
- Delgado Rosero, M.I.; Jurado Meneses, N.M.; Uribe Kaffure, R. Thermal properties of composite polymer electrolytes poly (ethylene oxide)/sodium trifluoroacetate/aluminum oxide (PEO) 10CF3COONa+ x wt.% Al2O3. Materials 2019, 12, 1464. [Google Scholar] [CrossRef] [Green Version]
- Diryak, R.; Kontogiorgos, V.; Ghori, M.U.; Bills, P.; Tawfik, A.; Morris, G.A.; Smith, A.M. Behavior of In Situ Cross-Linked Hydrogels with Rapid Gelation Kinetics on Contact with Physiological Fluids. Macromol. Chem. Phys. 2018, 219, 1700584. [Google Scholar] [CrossRef] [Green Version]
- Korte, C.; Quodbach, J. Formulation development and process analysis of drug-loaded filaments manufactured via hot-melt extrusion for 3D-printing of medicines. Pharm. Dev. Technol. 2018, 23, 1117–1127. [Google Scholar] [CrossRef]
- Öblom, H.; Zhang, J.; Pimparade, M.; Speer, I.; Preis, M.; Repka, M.; Sandler, N. 3D-printed isoniazid tablets for the treatment and prevention of tuberculosis—Personalized dosing and drug release. Aaps PharmSciTech 2019, 20, 52. [Google Scholar] [CrossRef] [Green Version]
- Mucalo, M.R.; Rathbone, M.J. Melt-extruded polyethylene oxide (PEO) rods as drug delivery vehicles: Formulation, performance as controlled release devices and the influence of co-extruded excipients on drug release profiles. Chem. N. Z. 2012, 76, 85–95. [Google Scholar]
- Li, D.; Jiang, Y.; Lv, S.; Liu, X.; Gu, J.; Chen, Q.; Zhang, Y. Preparation of plasticized poly (lactic acid) and its influence on the properties of composite materials. PLoS ONE 2018, 13, e0193520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coppens, K.; Hall, M.; Larsen, P.; Mitchell, S.; Nguyen, P.; Read, M.; Shrestha, U.; Walia, P. Thermal and rheological evaluation of pharmaceutical excipients for hot melt extrusion. In Proceedings of the AAPS Annual Meeting and Exposition, Baltimore, MD, USA; 2004. [Google Scholar]
- Syrlybayev, D.; Zharylkassyn, B.; Seisekulova, A.; Akhmetov, M.; Perveen, A.; Talamona, D. Optimisation of Strength Properties of FDM Printed Parts—A Critical Review. Polymers 2021, 13, 1587. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.; Acosta, N.; Heras, A. Chitosan and inhalers: A bioadhesive polymer for pulmonary drug delivery. In Inhaler Devices; Elsevier: Amsterdam, The Netherlands, 2013; pp. 77–93. [Google Scholar]
- Sandri, G.; Ruggeri, M.; Rossi, S.; Bonferoni, M.C.; Vigani, B.; Ferrari, F. (Trans) buccal drug delivery. Nanotechnol. Oral Drug Deliv. 2020, 2, 225–250. [Google Scholar]
- Madsen, F.; Eberth, K.; Smart, J.D. A rheological examination of the mucoadhesive/mucus interaction: The effect of mucoadhesive type and concentration. J. Control. Release 1998, 50, 167–178. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Deng, L.; Chen, J. Applications of poly (ethylene oxide) in controlled release tablet systems: A review. Drug Dev. Ind. Pharm. 2014, 40, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Ghori, M.U.; Ginting, G.; Smith, A.M.; Conway, B.R. Simultaneous quantification of drug release and erosion from hypromellose hydrophilic matrices. Int. J. Pharm. 2014, 465, 405–412. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pyteraf, J.; Jamróz, W.; Kurek, M.; Szafraniec-Szczęsny, J.; Kramarczyk, D.; Jurkiewicz, K.; Knapik-Kowalczuk, J.; Tarasiuk, J.; Wroński, S.; Paluch, M. How to Obtain the Maximum Properties Flexibility of 3D Printed Ketoprofen Tablets Using Only One Drug-Loaded Filament? Molecules 2021, 26, 3106. [Google Scholar] [CrossRef] [PubMed]
- Ghori, M.; Šupuk, E.; Conway, B. Tribo-electrification and Powder Adhesion Studies in the Development of Polymeric Hydrophilic Drug Matrices. Materials 2015, 8, 1482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahzad, Y.; Saeed, S.; Ghori, M.U.; Mahmood, T.; Yousaf, A.M.; Jamshaid, M.; Sheikh, R.; Rizvi, S.A. Influence of polymer ratio and surfactants on controlled drug release from cellulosic microsponges. Int. J. Biol. Macromol. 2018, 109, 963–970. [Google Scholar] [CrossRef]
- Nirwan, J.S.; Lou, S.; Hussain, S.; Nauman, M.; Hussain, T.; Conway, B.R.; Ghori, M.U. Electrically Tunable Lens (ETL)-Based Variable Focus Imaging System for Parametric Surface Texture Analysis of Materials. Micromachines 2022, 13, 17. [Google Scholar] [CrossRef] [PubMed]
- Khizer, Z.; Akram, M.R.; Sarfraz, R.M.; Nirwan, J.S.; Farhaj, S.; Yousaf, M.; Hussain, T.; Lou, S.; Timmins, P.; Conway, B.R. Plasticiser-free 3D printed hydrophilic matrices: Quantitative 3D surface texture, mechanical, swelling, erosion, drug release and pharmacokinetic studies. Polymers 2019, 11, 1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thirawong, N.; Nunthanid, J.; Puttipipatkhachorn, S.; Sriamornsak, P. Mucoadhesive properties of various pectins on gastrointestinal mucosa: An in vitro evaluation using texture analyzer. Eur. J. Pharm. Biopharm. 2007, 67, 132–140. [Google Scholar] [CrossRef] [PubMed]
- RWF (Rabbit Welfare Association and Fund) Dose Regime for Commonly Used Drugs in Rabbits. Available online: https://rabbitwelfare.co.uk/wp-content/uploads/2019/03/Drugs-regime-poster.pdf (accessed on 13 February 2023).
- Yamamoto, P.A.; de Lima Benzi, J.R.; de Moraes, N.V. Simple and rapid HPLC-UV methods for gabapentin quantification in human plasma and urine: Applicability in pharmacokinetics and drug monitoring. Rev. Ciências Farm. Básica Apl. 2021, 42, 1–11. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Loading (%) | Force (N) | Distance (mm) | Stress (MPa) | Strain | Young Modulus (E) MPa |
|---|---|---|---|---|---|
| 98.5 (1.05) | 2.4 (0.22) | 5.9 (1.15) | 17.22 (1.35) | 0.95 (0.21) | 18.12 (1.19) |
| Formulation Code | Formulation Composition (Weight Ratio %) | Dimensions (D × H mm) | Shell Number | Infill Percentage (%) |
|---|---|---|---|---|
| F1 | PEO:Gabapentin (80:20) | 7 × 4 | 1 | 0 |
| F2 | PEO:Gabapentin (80:20) | 7 × 4 | 2 | 0 |
| F3 | PEO:Gabapentin (80:20) | 7 × 4 | 3 | 0 |
| F4 | PEO:Gabapentin (80:20) | 7 × 4 | 4 | 0 |
| F5 | PEO:Gabapentin (80:20) | 7 × 4 | 2 | 10 |
| F6 | PEO:Gabapentin (80:20) | 7 × 4 | 2 | 20 |
| F7 | PEO:Gabapentin (80:20) | 7 × 4 | 2 | 30 |
| Formulation Code | Drug Loading (%) | Breaking Strength of Tablets (N) | Friability (%) |
|---|---|---|---|
| F1 | 97.51 (0.75) | 411.65 (5.59) | 0 |
| F2 | 98.33 (1.10) | 404.32 (6.20) | 0 |
| F3 | 100.05 (2.53) | 399.21 (11.39) | 0 |
| F4 | 99.1 (2.65) | 421.55 (10.35) | 0 |
| F5 | 97.33 (0.61) | 398.66 (12.35) | 0 |
| F6 | 98.21 (1.10) | 414.99 (15.36) | 0 |
| F7 | 98.87 (0.56) | 410.36 (6.55) | 0 |
| Formulation Code | Measured Volume (mm3) | Measured Mass (mg) | Tablet Density (mg/mm3) | Floating Time (h) |
|---|---|---|---|---|
| F1 | 150.69 (0.98) | 110.15 (1.21) | 0.73 (0.01) | >8 |
| F2 | 154.32 (1.10) | 120.15 (2.42) | 0.77 (0.02) | >10 |
| F3 | 157.16 (3.15) | 130.82 (3.73) | 0.83 (0.03) | >6 |
| F4 | 154.12 (3.11) | 144.28 (2.25) | 0.93 (0.01) | <2 |
| F5 | 149.49 (2.82) | 124.3 (3.36) | 0.83 (0.02) | >6 |
| F6 | 160.50 (4.28) | 135.62 (4.11) | 0.84 (0.02) | >6 |
| F7 | 158.63 (3.92) | 141.21 (3.51) | 0.89 (0.04) | <2 |
| Parameters | Oral Solution | F2 | p-Value |
|---|---|---|---|
| T1/2 (min) | 79.99 (6.22) | 97.96 (8.64) | 0.04 |
| T max (min) | 180 (0.00) | 360 (0.00) | n.c. |
| C max (ng/mL) | 13.65 (3.21) | 11.85 (2.29) | 0.32 |
| AUC 0–t (ng/mL/h) | 3037.05 (174.81) | 4381.65 (251.37) | 0.007 |
| Formulation (Weight Ratio) | Extrusion Temperature (°C) | Screw Speed (rpm) | Torque (N/cm) |
|---|---|---|---|
| PEO:Gabapentin (80:20) | 105 | 30 | 18 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khizer, Z.; Akram, M.R.; Tahir, M.A.; Liu, W.; Lou, S.; Conway, B.R.; Ghori, M.U. Personalised 3D-Printed Mucoadhesive Gastroretentive Hydrophilic Matrices for Managing Overactive Bladder (OAB). Pharmaceuticals 2023, 16, 372. https://doi.org/10.3390/ph16030372
Khizer Z, Akram MR, Tahir MA, Liu W, Lou S, Conway BR, Ghori MU. Personalised 3D-Printed Mucoadhesive Gastroretentive Hydrophilic Matrices for Managing Overactive Bladder (OAB). Pharmaceuticals. 2023; 16(3):372. https://doi.org/10.3390/ph16030372
Chicago/Turabian StyleKhizer, Zara, Muhammad R. Akram, Muhammad Azam Tahir, Weidong Liu, Shan Lou, Barbara R. Conway, and Muhammad Usman Ghori. 2023. "Personalised 3D-Printed Mucoadhesive Gastroretentive Hydrophilic Matrices for Managing Overactive Bladder (OAB)" Pharmaceuticals 16, no. 3: 372. https://doi.org/10.3390/ph16030372