

External Evaluation of Population Pharmacokinetics Models of Lithium in the Bipolar Population
 ,
, Highlights
- This is the first study to evaluate predictive performances of published population pharmacokinetics models of lithium.
Abstract
:1. Introduction
2. Results
2.1. Published Models
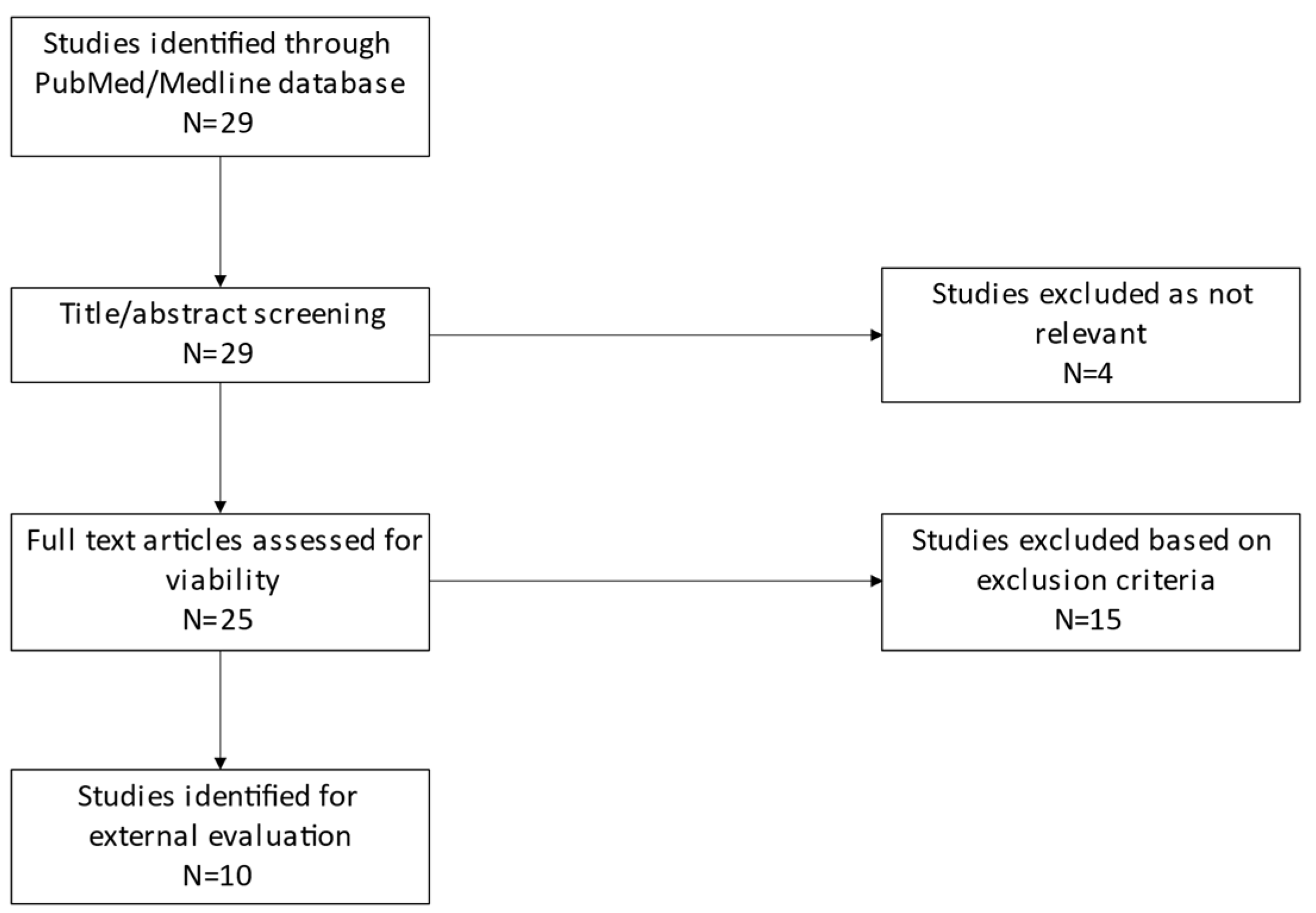
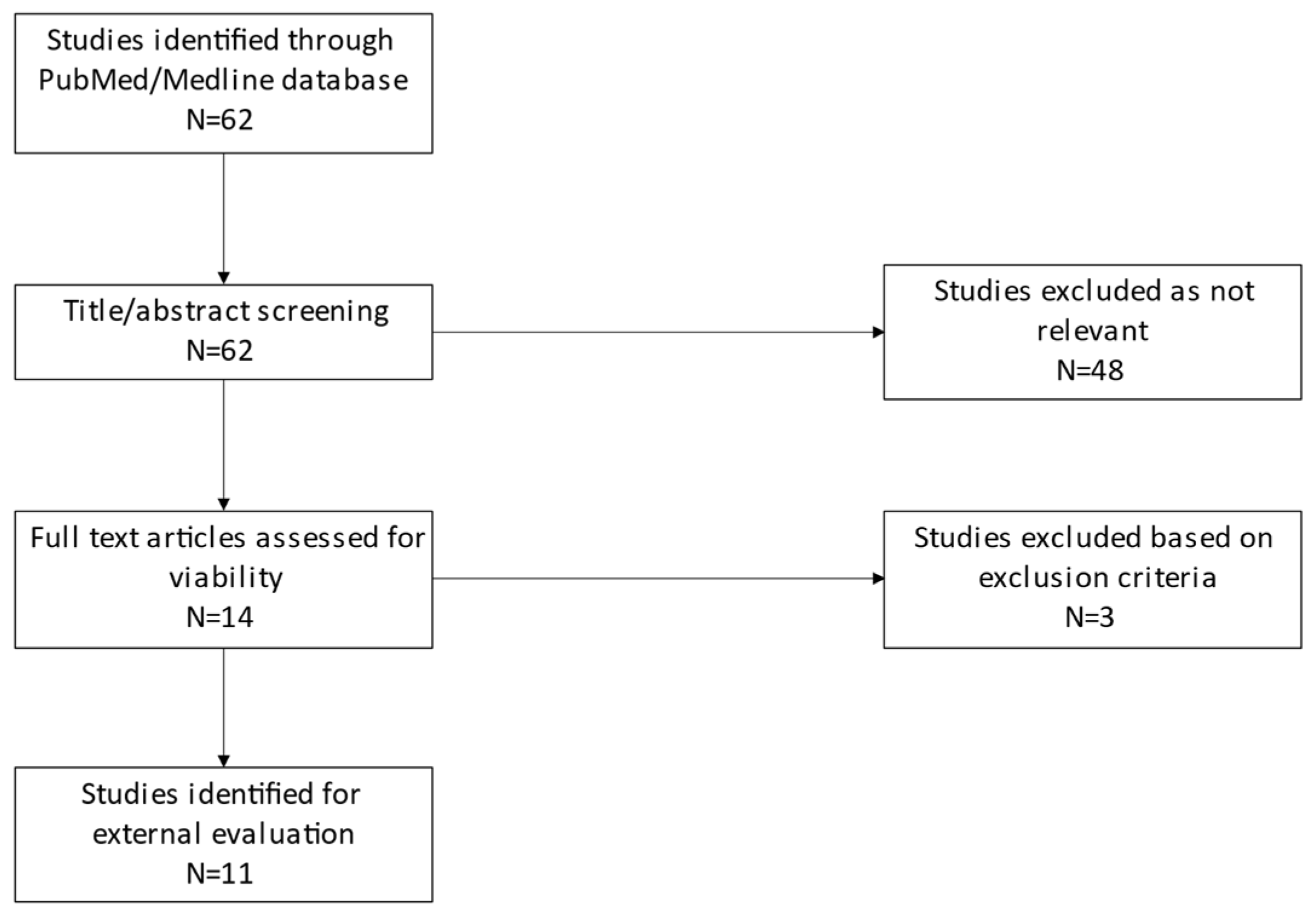
2.2. External Evaluation Data
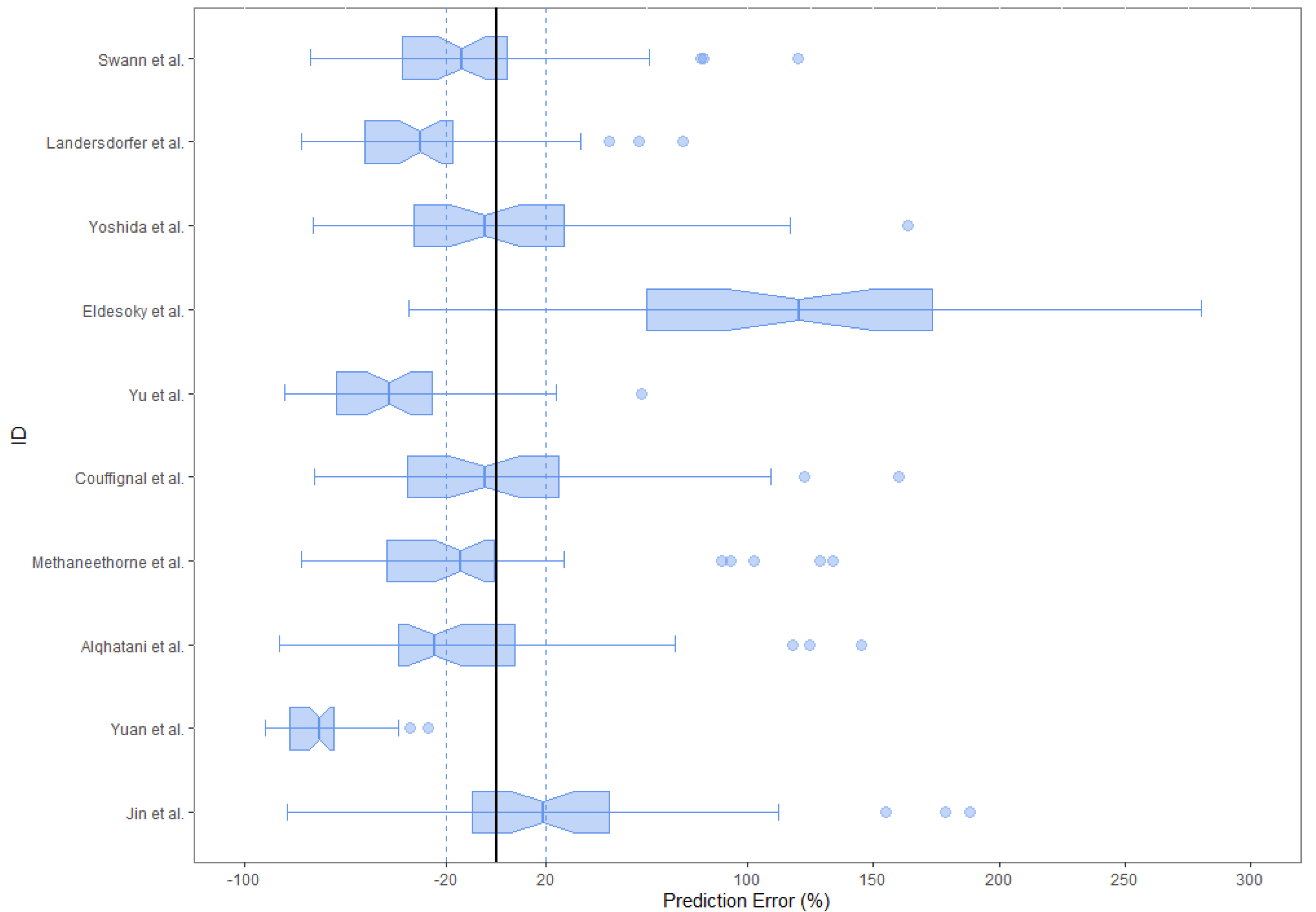
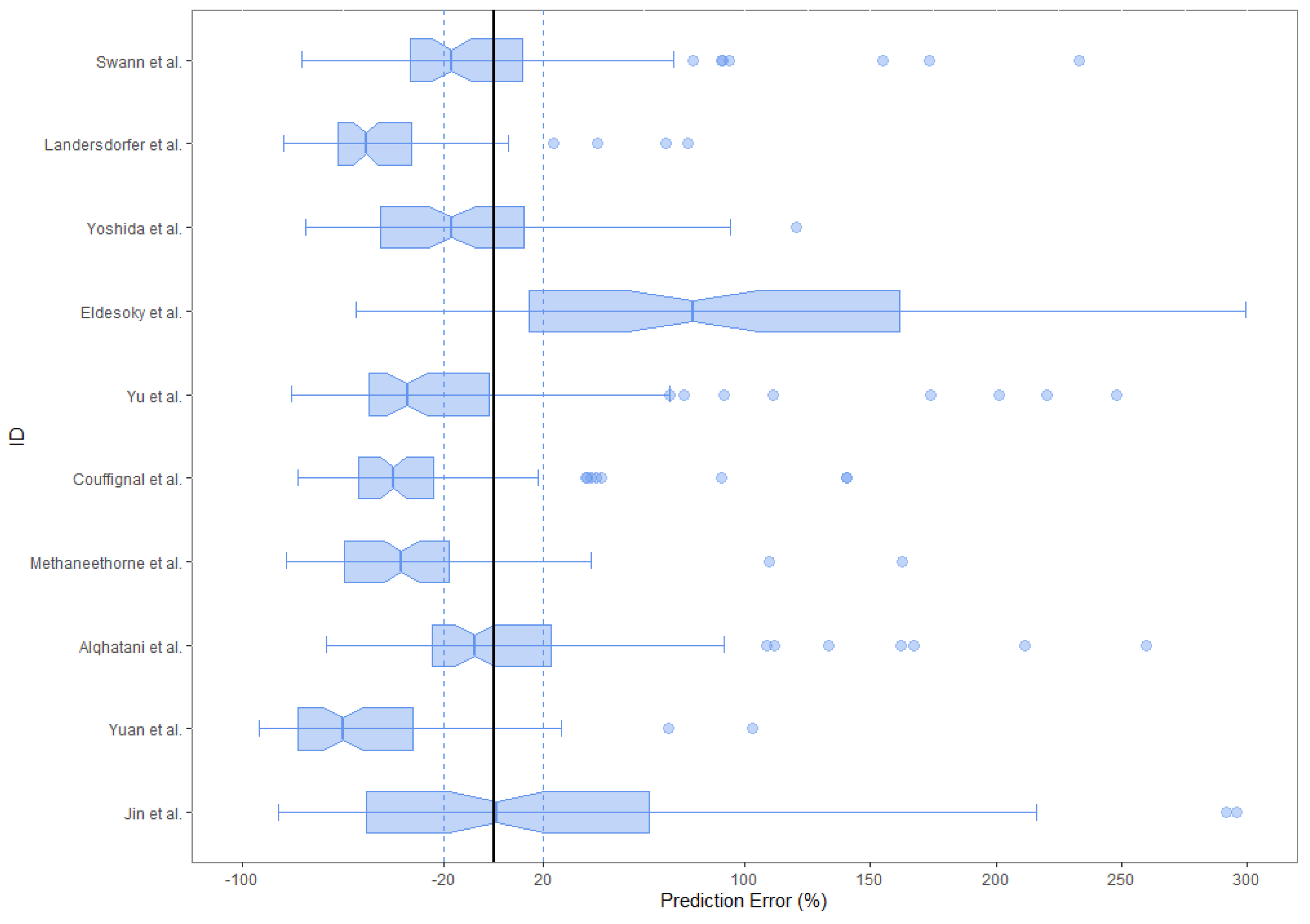
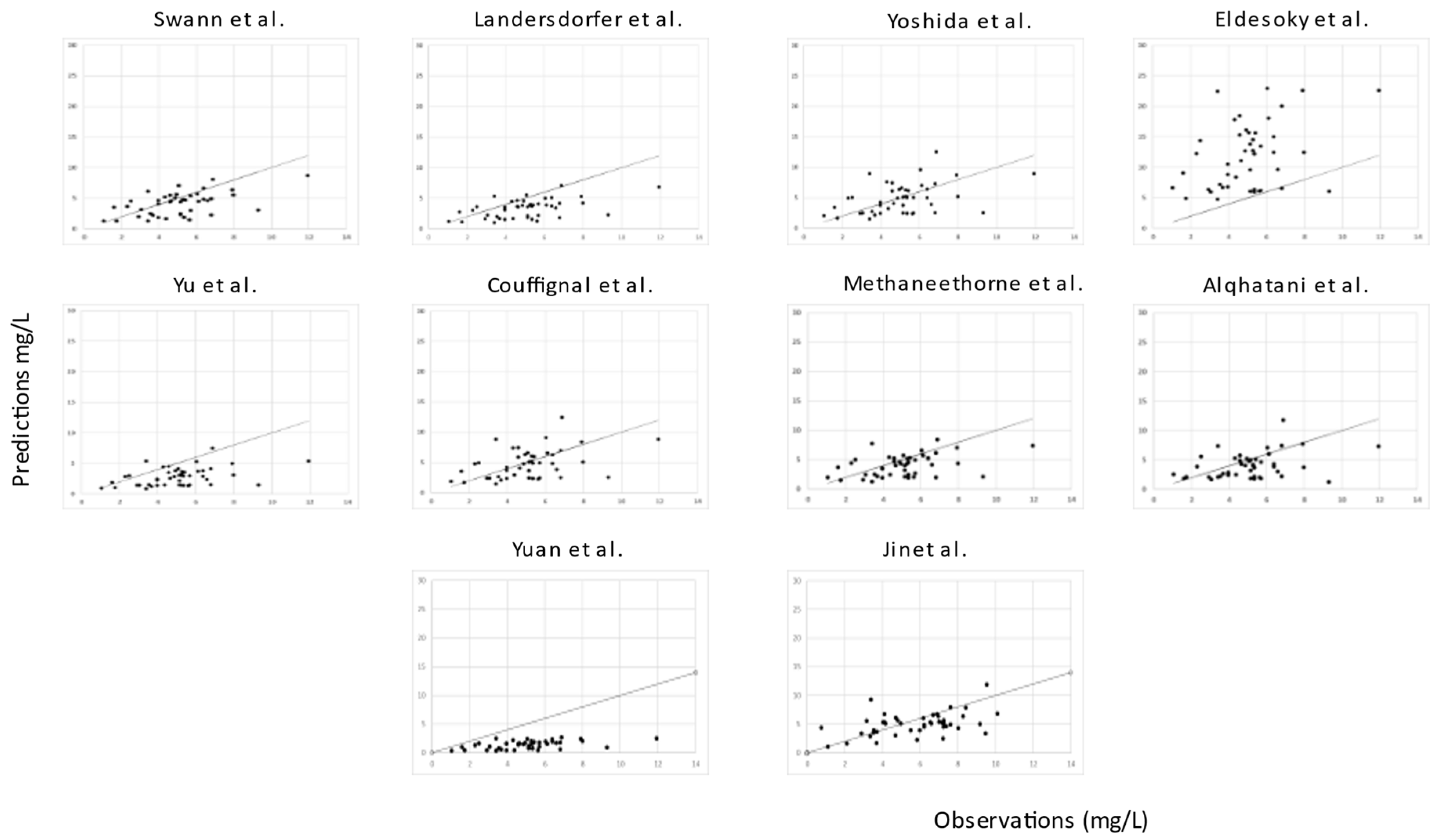
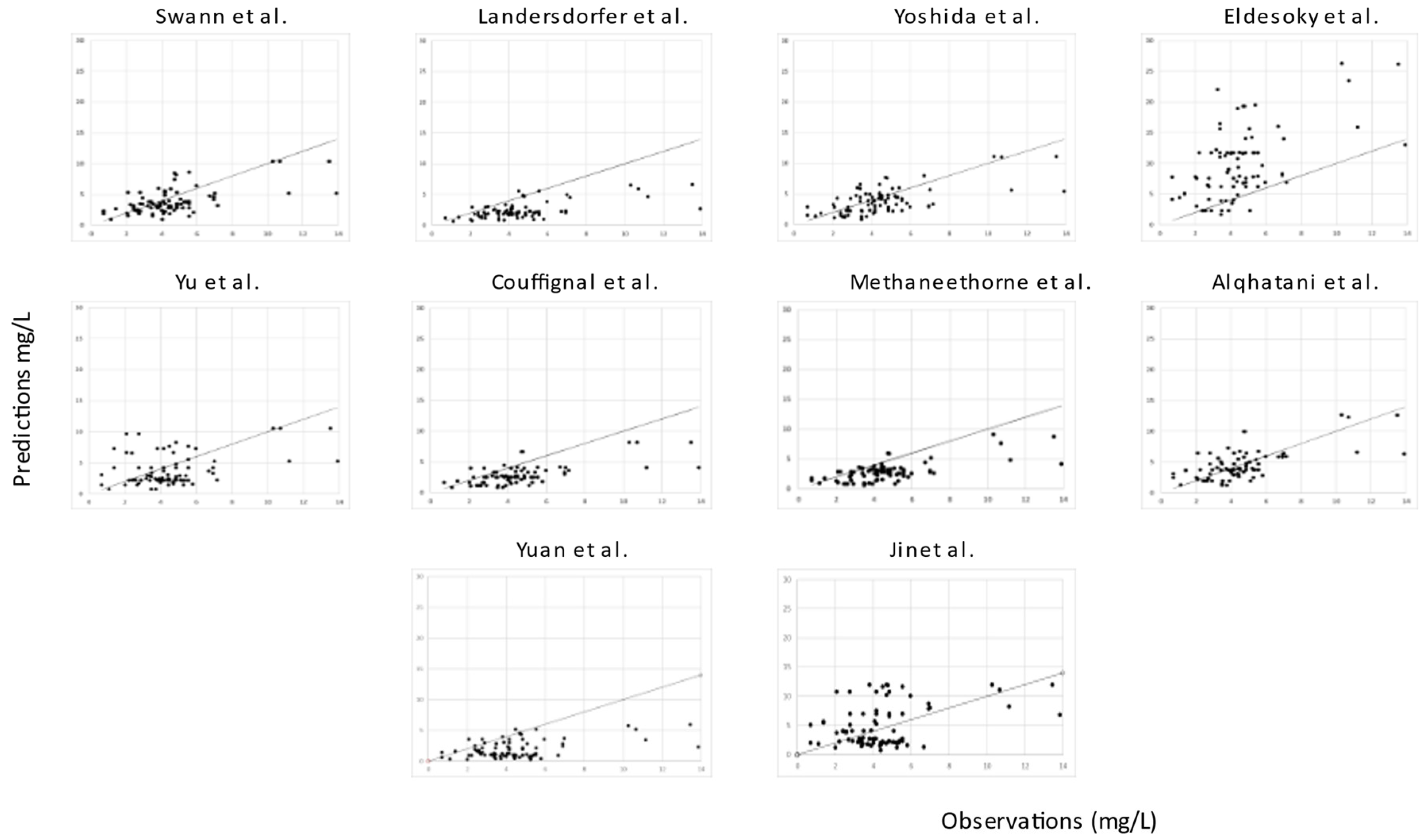
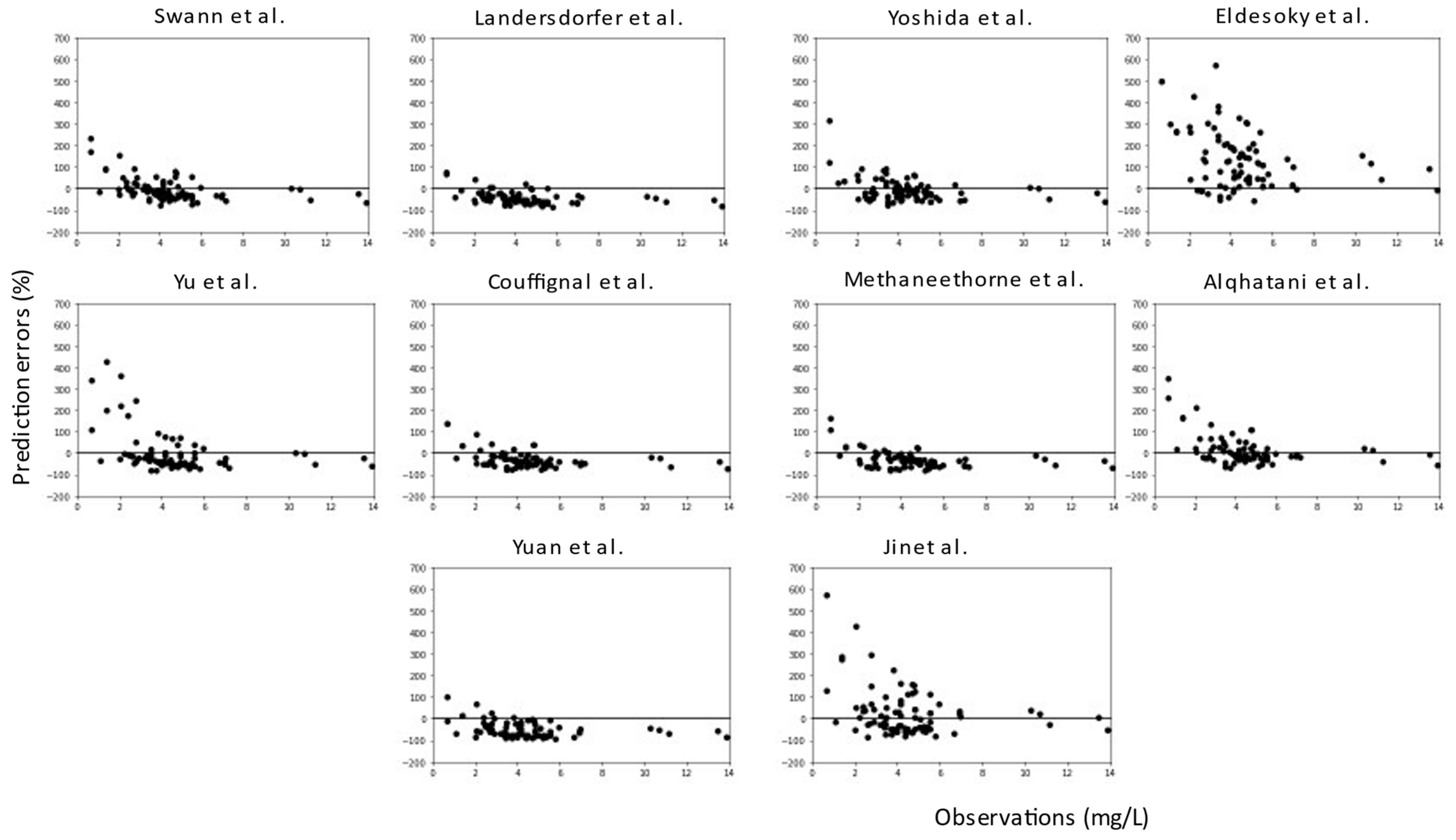
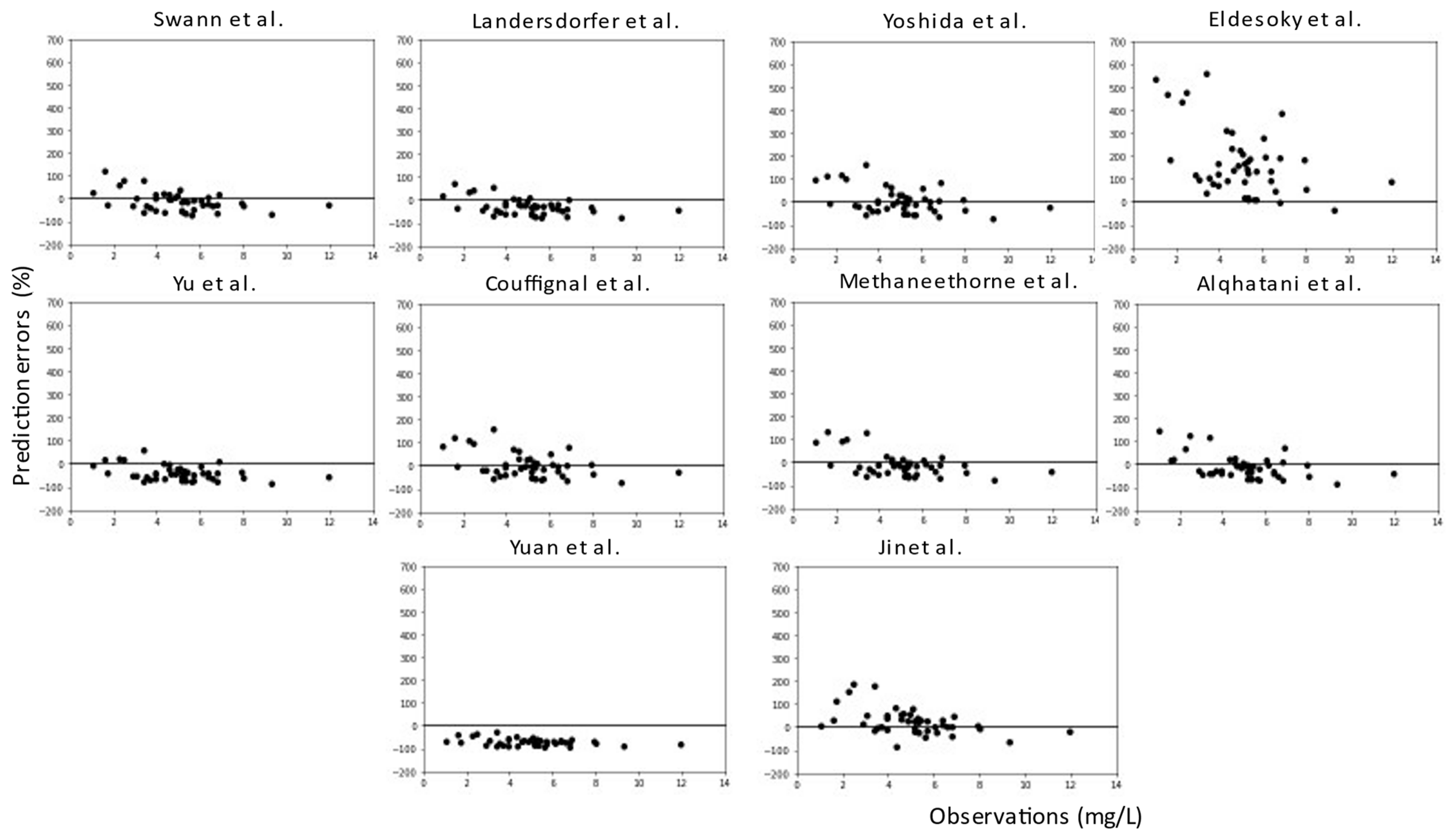
2.3. External Evaluation
3. Discussion
4. Materials and Methods
4.1. Search Methods and Inclusion Criteria
4.2. External Evaluation Data
4.2.1. Literature Cohort
4.2.2. Clinical Cohort
4.3. Model Evaluation
- Bias (i.e., the direction and the size of the deviation from the observed concentration) of model predictions is given for the ith individual and th jth blood sample, by the median prediction error (MDPE):
- Inaccuracy (i.e., the size of the typical error) of model predictions is given for the ith individual and the jth blood sample, by the median absolute performance errors (MADPE).
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Xu, Y.-Y.; Xia, Q.-H.; Liang, J.; Cao, Y.; Shan, F.; Liu, Y.; Yan, C.-Y.; Xia, Q.-R. Factors related to lithium blood concentrations in Chinese Han patients with bipolar disorder. NDT 2019, 15, 1929–1937. [Google Scholar]
- Smith, D.J.; Whitham, E.A.; Ghaemi, S.N. Bipolar disorder. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2012; Volume 106, pp. 251–263. ISBN 978-0-444-52002-9. [Google Scholar]
- McCormick, U.; Murray, B.; McNew, B. Diagnosis and treatment of patients with bipolar disorder: A review for advanced practice nurses. J. Am. Assoc. Nurse Pract. 2015, 27, 530–542. [Google Scholar] [PubMed]
- Won, E.; Kim, Y.-K. An Oldie but Goodie: Lithium in the Treatment of Bipolar Disorder through Neuroprotective and Neurotrophic Mechanisms. Int. J. Mol. Sci. 2017, 18, 2679. [Google Scholar] [PubMed]
- Nunes, A.; Ardau, R.; Berghöfer, A.; Bocchetta, A.; Chillotti, C.; Deiana, V.; Garnham, J.; Grof, E.; Hajek, T.; Manchia, M.; et al. Prediction of lithium response using clinical data. Acta Psychiatr. Scand. 2020, 141, 131–141. [Google Scholar]
- Pérez De Mendiola, X.; Hidalgo-Mazzei, D.; Vieta, E.; González-Pinto, A. Overview of lithium’s use: A nationwide survey. Int. J. Bipolar Disord. 2021, 9, 10. [Google Scholar] [PubMed]
- Sköld, M.; Rolstad, S.; Joas, E.; Kardell, M.; Pålsson, E.; Goodwin, G.M.; Landén, M. Regional lithium prescription rates and recurrence in bipolar disorder. Int. J. Bipolar Disord. 2021, 9, 18. [Google Scholar]
- Grandjean, E.M.; Aubry, J.-M. Lithium: Updated Human Knowledge Using an Evidence-Based Approach. CNS Drugs 2009, 23, 225–240. [Google Scholar] [PubMed]
- Yamaguchi, D.; Tsuji, Y.; Sonoda, M.; Shin, K.; Kito, H.; Ogami, C.; Kasai, H.; To, H.; Kamimura, H. Population Pharmacokinetics and Exposure–Response of Lithium Carbonate in Patients Based on Tubular Reabsorption Mechanisms. Eur. J. Drug Metab. Pharmacokinet. 2019, 44, 329–338. [Google Scholar]
- Methaneethorn, J. Population Pharmacokinetic Analyses of Lithium: A Systematic Review. Eur. J. Drug Metab. Pharmacokinet. 2018, 43, 25–34. [Google Scholar]
- Hiemke, C.; Bergemann, N.; Clement, H.; Conca, A.; Deckert, J.; Domschke, K.; Eckermann, G.; Egberts, K.; Gerlach, M.; Greiner, C.; et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017. Pharmacopsychiatry 2018, 51, 9–62. [Google Scholar]
- Malhi, G.S.; Bell, E.; Bassett, D.; Boyce, P.; Bryant, R.; Hazell, P.; Hopwood, M.; Lyndon, B.; Mulder, R.; Porter, R.; et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders. Aust. N. Z. J. Psychiatry 2021, 55, 7–117. [Google Scholar] [PubMed]
- Baird-Gunning, J.; Lea-Henry, T.; Hoegberg, L.C.G.; Gosselin, S.; Roberts, D.M. Lithium Poisoning. J. Intensive Care Med. 2017, 32, 249–263. [Google Scholar] [PubMed]
- Ooba, N.; Tsutsumi, D.; Kobayashi, N.; Hidaka, S.; Hayashi, H.; Obara, T.; Satoh, M.; Kubota, K.; Fukuoka, N. Prevalence of Therapeutic Drug Monitoring for Lithium and the Impact of Regulatory Warnings: Analysis Using Japanese Claims Database. Ther. Drug Monit. 2018, 40, 252–256. [Google Scholar] [CrossRef] [PubMed]
- Hsu, C.-W.; Tsai, S.-Y.; Wang, L.-J.; Liang, C.-S.; Carvalho, A.F.; Solmi, M.; Vieta, E.; Lin, P.-Y.; Hu, C.-A.; Kao, H.-Y. Predicting Serum Levels of Lithium-Treated Patients: A Supervised Machine Learning Approach. Biomedicines 2021, 9, 1558. [Google Scholar] [CrossRef]
- Broeker, A.; Nardecchia, M.; Klinker, K.P.; Derendorf, H.; Day, R.O.; Marriott, D.J.; Carland, J.E.; Stocker, S.L.; Wicha, S.G. Towards precision dosing of vancomycin: A systematic evaluation of pharmacometric models for Bayesian forecasting. Clin. Microbiol. Infect. 2019, 25, 1286.e1–1286.e7. [Google Scholar]
- Wicha, S.G.; Märtson, A.; Nielsen, E.I.; Koch, B.C.P.; Friberg, L.E.; Alffenaar, J.; Minichmayr, I.K.; the International Society of Anti-Infective Pharmacology (ISAP); the PK/PD study group of the European Society of Clinical Microbiology, Infectious Diseases (EPASG). From Therapeutic Drug Monitoring to Model-Informed Precision Dosing for Antibiotics. Clin. Pharmacol. Ther. 2021, 109, 928–941. [Google Scholar] [CrossRef]
- Zhao, W.; Kaguelidou, F.; Biran, V.; Zhang, D.; Allegaert, K.; Capparelli, E.V.; Holford, N.; Kimura, T.; Lo, Y.-L.; Peris, J.-E.; et al. External evaluation of population pharmacokinetic models of vancomycin in neonates: The transferability of published models to different clinical settings: Transferability of published vancomycin population pharmacokinetic models in neonates. Br. J. Clin. Pharmacol. 2013, 75, 1068–1080. [Google Scholar] [CrossRef]
- Swann, A.C.; Berman, N.; Frazer, A.; Koslow, S.H.; Maas, J.W.; Pandey, G.N.; Secunda, S. Lithium distribution in mania: Single-dose pharmacokinetics and sympathoadrenal function. Psychiatry Res. 1990, 32, 71–84. [Google Scholar]
- Landersdorfer, C.B.; Findling, R.L.; Frazier, J.A.; Kafantaris, V.; Kirkpatrick, C.M.J. Lithium in Paediatric Patients with Bipolar Disorder: Implications for Selection of Dosage Regimens via Population Pharmacokinetics/Pharmacodynamics. Clin. Pharmacokinet. 2017, 56, 77–90. [Google Scholar] [CrossRef]
- Yoshida, K.; Uchida, H.; Suzuki, T.; Watanabe, M.; Yoshino, N.; Houchi, H.; Mimura, M.; Fukuoka, N. Prediction Model of Serum Lithium Concentrations. Pharmacopsychiatry 2018, 51, 82–88. [Google Scholar] [CrossRef]
- ELDesoky, E.S.; Kumar, V.; Alorainy, M.S.; Hamdi, M.M.; Derendorf, H. Estimation of lithium clearance from routine clinical data in Egyptian bipolar patients. A population pharmacokinetic approach. Int. J. Clin. Pharmacol. Ther. 2008, 46, 617–626. [Google Scholar] [CrossRef]
- Yu, W.; Sun, X.; Li, Y.; Li, M.; Wang, K.; Li, H. Population Pharmacokinetics of Lithium Carbonate in Young Male Healthy Chinese Volunteers. Pharmacopsychiatry 2016, 49, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Couffignal, C.; Bertrand, J.; Sportiche, S.; Jarroir, M.; El Balkhi, S.; Djebrani-Oussedik, N.; Poupon, J.; Declèves, X.; Mentré, F.; Bellivier, F. Population pharmacokinetic modeling of sustained release lithium in the serum, erythrocytes and urine of patients with bipolar disorder. Eur. J. Clin. Pharmacol. 2019, 75, 519–528. [Google Scholar] [CrossRef] [PubMed]
- Alqahtani, S.A.; Alsultan, A.S.; Alqattan, H.M.; Eldemerdash, A.; Albacker, T.B. Population Pharmacokinetic Model for Vancomycin Used in Open Heart Surgery: Model-Based Evaluation of Standard Dosing Regimens. Antimicrob. Agents Chemother. 2018, 62, e00088-18. [Google Scholar] [CrossRef] [PubMed]
- Jin, Z.; Wu, Z.; Cui, Y.; Liu, X.; Liang, H.; You, J.; Wang, C. Population Pharmacokinetics and Dosing Regimen of Lithium in Chinese Patients With Bipolar Disorder. Front. Pharmacol. 2022, 13, 913935. [Google Scholar] [CrossRef] [PubMed]
- Yuan, J.; Zhang, B.; Xu, Y.; Zhang, X.; Song, J.; Zhou, W.; Hu, K.; Zhu, D.; Zhang, L.; Shao, F.; et al. Population Pharmacokinetics of Lithium in Young Pediatric Patients With Intellectual Disability. Front. Pharmacol. 2021, 12, 650298. [Google Scholar] [CrossRef]
- Methaneethorn, J.; Sringam, S. Factors influencing lithium pharmacokinetics in patients with acute mania: A population pharmacokinetic analysis. Hum. Psychopharmacol. Clin. Exp. 2019, 34, e2697. [Google Scholar] [CrossRef]
- Lew, K.H.; Chang, E.Y.; Rajagopalan, K.; Knoth, R.L. The effect of medication adherence on health care utilization in bipolar disorder. Manag. Care Interface 2006, 19, 41–46. [Google Scholar] [PubMed]
- Alqahtani, S.; Aljuma’ah, N.; Aydan, N.B.; Alsultan, A.; Alsarhani, E.; Asiri, Y. Estimation of lithium clearance in patients with bipolar disorder. Int. Clin. Psychopharmacol. 2020, 35, 157–162. [Google Scholar] [CrossRef]
- Aliasgharpour, M.; Hagani, H. Evaluation of lithium determination in three analyzers: Flame emission, flame atomic absorption spectroscopy and ion selective electrode. N. Am. J. Med. Sci. 2009, 1, 244. [Google Scholar] [PubMed]
- Findling, R.L.; Landersdorfer, C.B.; Kafantaris, V.; Pavuluri, M.; McNamara, N.K.; McClellan, J.; Frazier, J.A.; Sikich, L.; Kowatch, R.; Lingler, J.; et al. First-Dose Pharmacokinetics of Lithium Carbonate in Children and Adolescents. J. Clin. Psychopharmacol. 2010, 30, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Johansson, Å.M.; Karlsson, M.O. Comparison of Methods for Handling Missing Covariate Data. AAPS J. 2013, 15, 1232–1241. [Google Scholar] [CrossRef] [PubMed]
- Irby, D.J.; Ibrahim, M.E.; Dauki, A.M.; Badawi, M.A.; Illamola, S.M.; Chen, M.; Wang, Y.; Liu, X.; Phelps, M.A.; Mould, D.R. Approaches to handling missing or “problematic” pharmacology data: Pharmacokinetics. CPT Pharmacomet. Syst. Pharmacol. 2021, 10, 291–308. [Google Scholar] [CrossRef] [PubMed]
- Moons, K.G.M.; Kengne, A.P.; Grobbee, D.E.; Royston, P.; Vergouwe, Y.; Altman, D.G.; Woodward, M. Risk prediction models: II. External validation, model updating, and impact assessment. Heart 2012, 98, 691–698. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.; Wang, C.; Li, Z.; Pan, Y.; Liu, M.; Jiao, Z. Can Population Pharmacokinetics of Antibiotics be Extrapolated? Implications of External Evaluations. Clin. Pharmacokinet. 2021, 60, 53–68. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study (Publication Year) | Country (Single/Multiple Sites) | Number of Patients (Male/Female) | Number of Samples (Sample Type) | Analytical Method | Pathology | Software | Number of Compartments of the Model | Covariates Tested | PK Parameters and Formula (Lithium) | IIV (%) | Residual Error | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Swann et al. (1990) | USA (single) | 14 (10/4) | NA (pk study) | Atomic absorption spectrometry | Manic episode | None | Two | FFM | CL (L/h) V1 (L) V2 (L) K12 (h−1) K21 (h−1) Ka * (h−1) | 0.09 × V1 0.3 × FFM (0.4 × FFM)−0.3 0.56 0.41 1.03 | ||
| Landersdorfer et al. (2016) | USA (multiple) | 61 (32/29) | 2730 (pk study) | Atomic absorption spectrometry, ICP-OES, automated assays | Bipolar disorder | S-ADAPT/ NONMEM | Two | TBW, age, LBW, gender, CrCL, Scr | CL (L/h) V1 (L) V2 (L) Q (L/h) Klag (h−1) Ka (h−1) | 1.63 ×(LBW/53)0.75 24.5 × (LBW/53) 33.5 × (LBW/53) 3.19 × (LBW/53)0.75 3.64 1.21 | 20.7 11.6 40.3 31.1 88.2 21.0 | 0.0422 mEq/L |
| Yoshida et al. (2017) | Japan (multiple) | 82 (44/38) | 131 (TDM) | Atomic absorption spectrometry | Bipolar disorder, depression, schizophrenia | SPSS/PRISM | One | CL (L/h) Ka * (h−1) V1 * (L) | 1.236 1.5 0.79 × WT | 0.13 mEq/L | ||
| Eldesoky et al. (2008) | Egypt (single) | 50 (21/29) | 50 (TDM) | Ion sensitive electrode | Bipolar disorder | NONMEM | Two | WT, GFR, gender, age | CL (L/h) V1 * (L) V2 * (L) Q * (L/h) Ka * (h−1) | 0.51 × (GFR/105.3)0.438 15.2 7.44 6.7 0.62 | 12.77 | 15% |
| Yu et al. (2016) | China (single) | 20 (20/0) | 560 (pk study) | Flame photometry | Healthy | NONMEM | Two | Demographic factors and laboratory indicators | CL (L/h) V1 (L) V2 (L) Q (L/h) Tlag (h) Ka * (h−1) | 9.39 10.4 216 22.1 0.186 0.293 | 13.2 84.2 19.7 127 19.4 | 5.19% |
| Couffignal et al. (2018) | France (single) | 17 (6/11) | 68 (pk study) | ICP-OES | Bipolar disorder | MONOLIX | Two | None | CL (L/h) V1 (L) V2 * (L) K12 * (h−1) K21 (h−1) Tlag * (h) Ka * (h−1) F | 1.21 23 64.7 3.63 9.46 0.92 2.22 0.62 | 20 30 27 72 0.98 | 10% |
| Methaneethorne et al. (2019) | Thailand (single) | 222 (114/108) | NA | Ion-sensitive electrode | Bipolar disorder | NONMEM | One | Weight, age, gender, Scr, CrCl, BMI, co administration. | CL (L/h) Ka * (h−1) V1/F * (L) | 1.43 × (WT/65)0.425 × (age/38)−0.242 0.462 54 | 3.11 | 19 mg/L |
| Alqahtani et al. (2019) | Saudi Arabia (single) | 31 (7/24) | 170 (TDM) | Spectrophotometric methods | Bipolar disorder | MONOLIX | Two | CrCl | CL (L/h) V1 * (L) V2 * (L) Q * (L/h) Ka * (h−1) | 1.15 × (ClCr/119.2)0.117 22.1 3.35 0.44 0.62 | 14 | 0.223 mmol/L |
| Yuan et al. (2021) | China (single) | 52 (38/14) | 160 (pk study) | Ion sensitive electrode methos | Intellectual disability, pediatric | NONMEM | Two | Weight, age, gender | Cl/F (L/h) MTT(h) V1/F (L) V2/F (L) Q/F (L/h) | 0.98 × (WT/20) 0.52 13.1 × (WT/20) 8.2 × (WT/20) 0.84 | 4.6 9.9 7.2 17.7 9.5 | 0.091 mmol/L |
| Jin et al. (2022) | China (single) | 268 (NA) | 476 | Phosphatase assay (Siemens® ADVIA 1800) | Bipolar disorder | NONMEM | One | Weight, CrCl, total daily dose, sex | Cl/F (L/h) V1 (L) Ka * (h−1) | 0.909 × (TDD/600)0.354 × (WT/62)0.33 × (CrCl/116)0.186 10.9 0.293 | 20.8 40.4 | 0.0236 mmol/L |
| Characteristics | Number or Mean ± SD Clinical | Median (Range) Clinical | Number or Mean ± SD Literature | Median (Range) Literature |
|---|---|---|---|---|
| No. of patients (male/female) | 46 (20/26) | NA | 89 (62/27) | NA |
| No. of samples | 46 | NA | 89 | NA |
| No. of samples per patient | 1 | NA | 1 | NA |
| Age (years) | 41.15 (±14.78) | 42 (16–68) | 24.76 (±14.68) | 19 (8–87) |
| Weight (kg) | 74.99 (±18.40) | 71.50 (61–127) | 66.30 (±22.94) | 65 (27–125) |
| Height (cm) | 170.39 (±−10.32) | 170 (147–189) | 168 (NA) | 168 (NA) |
| Concentration (mg/L) | 5.04 (±1.99) | 5.14 (1.04–11.94) | 4.50 (±2.31) | 4.16 (0.69–13.9) |
| GFR (mL/min) | 99.80 (±16.05) | 102 (61–127) | 120.61 (±88.54) | 105.50 (66–218) |
| Lithium dose (mg) | 13.23 (±7.57) | 16.22 (3.38–54.05) | 15.84 (±8.24) | 12.16 (4.05–32.43) |
| Bipolar patients | 46 | NA | 65 | NA |
| MDPE (Literature) | MADPE (Literature) | MDPE (Hospital) | MADPE (Hospital) | |
|---|---|---|---|---|
| Swann et al. | −16.7 | 29.5 | −13.5 | 26.7 |
| Landersdorfer et al. | −50.9 | 52.4 | −30.2 | 35.8 |
| Yoshida et al. | 17.4 | 37.4 | −4.5 | 30.5 |
| Eldesoky et al. | 99.8 | 99.8 | 137.6 | 137.6 |
| Yu et al. | −85.7 | 85.7 | −42.7 | 44.2 |
| Couffignal et al. | −8.7 | 31.5 | −4.5 | 29.9 |
| Methaneethorne et al. | −36.5 | 40.4 | −14.4 | 24.9 |
| Alqahtani et al. | −5.5 | 24.4 | 7.8 | 32.4 |
| Yuan et al. | −58.4 | 59.7 | −70.0 | 70.0 |
| Jin et al. | 12.7 | 47.9 | 18.6 | 28.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lereclus, A.; Boniffay, A.; Kallée, G.; Blin, O.; Belzeaux, R.; Frédéric, D.; Benito, S.; Guilhaumou, R. External Evaluation of Population Pharmacokinetics Models of Lithium in the Bipolar Population. Pharmaceuticals 2023, 16, 1627. https://doi.org/10.3390/ph16111627
Lereclus A, Boniffay A, Kallée G, Blin O, Belzeaux R, Frédéric D, Benito S, Guilhaumou R. External Evaluation of Population Pharmacokinetics Models of Lithium in the Bipolar Population. Pharmaceuticals. 2023; 16(11):1627. https://doi.org/10.3390/ph16111627
Chicago/Turabian StyleLereclus, Aurélie, Andréa Boniffay, Gauvind Kallée, Olivier Blin, Raoul Belzeaux, Dayan Frédéric, Sylvain Benito, and Romain Guilhaumou. 2023. "External Evaluation of Population Pharmacokinetics Models of Lithium in the Bipolar Population" Pharmaceuticals 16, no. 11: 1627. https://doi.org/10.3390/ph16111627