
Pharmacokinetic Interaction between Atorvastatin and Omega-3 Fatty Acid in Healthy Volunteers

 , , ,
, , ,
Abstract
:1. Introduction
2. Results
2.1. Subject Demographics
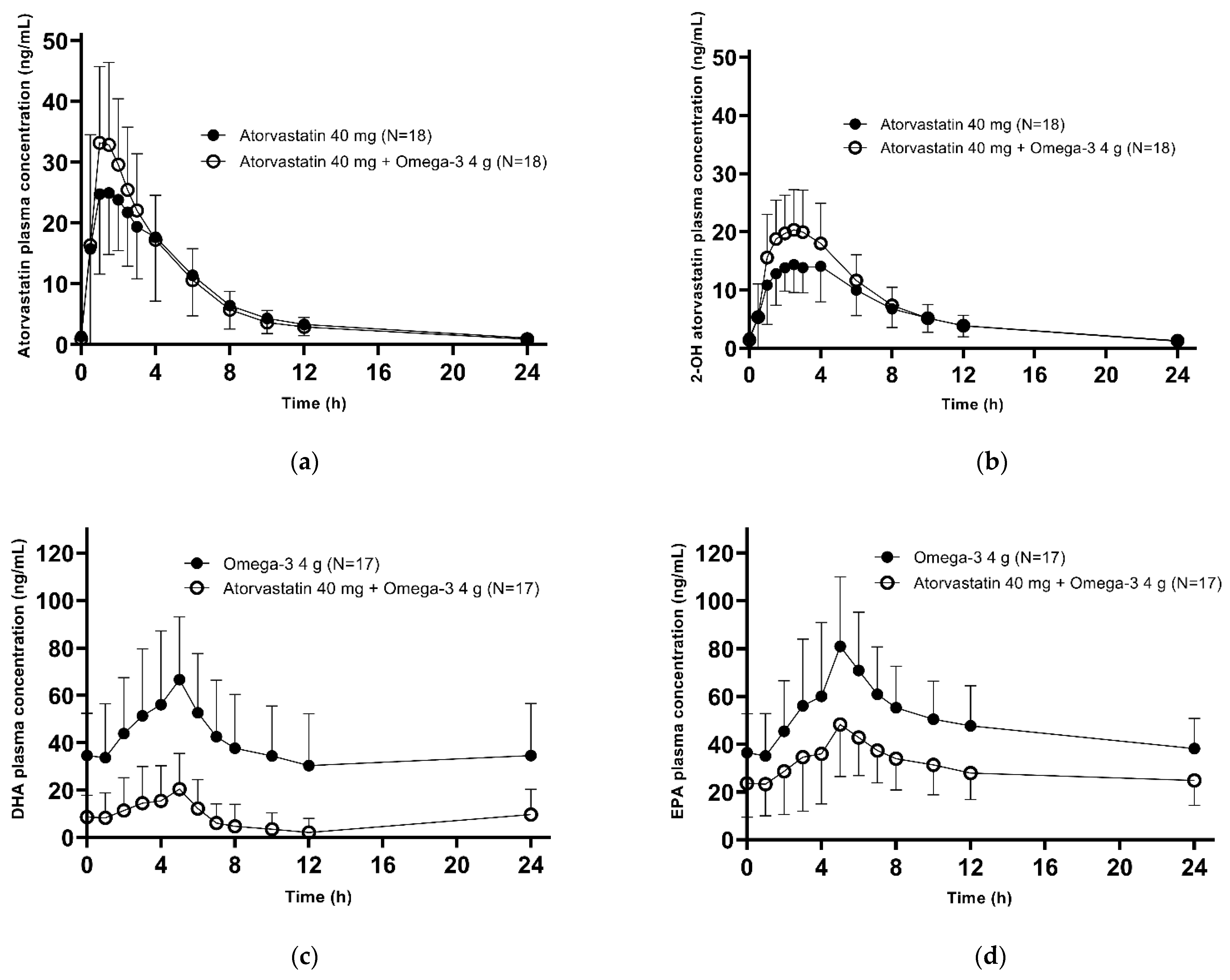
2.2. Pharmacokinetics
2.3. Safety
3. Discussion
4. Materials and Methods
4.1. Subjects
4.2. IPs
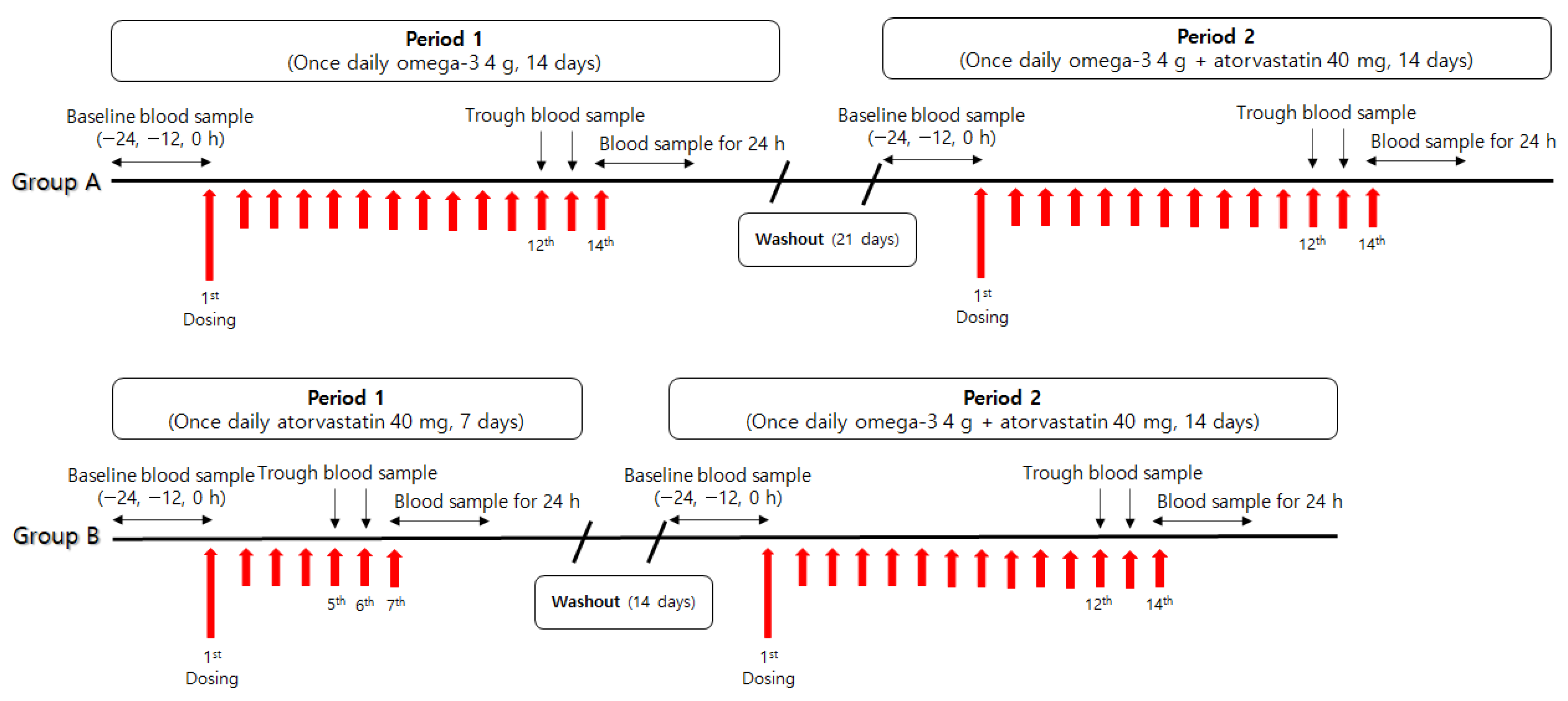
4.3. Study Design
4.4. Determination of Plasma Concentrations
4.4.1. Atorvastatin and 2-OH-Atorvastatin
4.4.2. DHA and EPA
4.5. Pharmacokinetic Analysis
4.6. Statistical Analysis
4.7. Safety and Tolerability
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stancu, C.; Sima, A. Statins: Mechanism of action and effects. J Cell Mol. Med. 2001, 5, 378–387. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Nicholls, S.J.; Sipahi, I.; Libby, P.; Raichlen, J.S.; Ballantyne, C.M.; Davignon, J.; Erbel, R.; Fruchart, J.C.; Tardif, J.C.; et al. Effect Of very high-intensity statin therapy on regression of coronary atherosclerosis—The ASTEROID trial. JAMA-J. Am. Med. Assoc. 2006, 295, 1556–1565. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, T.R.; Kjekshus, J.; Berg, K.; Haghfelt, T.; Faergeman, O.; Thorgeirsson, G.; Pyorala, K.; Miettinen, T.; Wilhelmsen, L.; Olsson, A.G.; et al. Randomized trial of cholesterol-lowering in 4444 patients with coronary-heart-disease—The Scandinavian Simvastatin Survival Study (4s). Lancet 1994, 344, 1383–1389. [Google Scholar]
- Sacks, F.M.; Alaupovic, P.; Moye, L.A.; Cole, T.G.; Sussex, B.; Stampfer, M.J.; Pfeffer, M.A.; Braunwald, E. VLDL, apolipoproteins B, CIII, and E, and risk of recurrent coronary events in the Cholesterol and Recurrent Events (CARE) trial. Circulation 2000, 102, 1886–1892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonkin, A.M.; Glaziou, P.P. The Long-Term Intervention with Pravastatin in Ischaemic Disease (LIPID) study. Int. Congr. Ser. 1998, 1155, 231–237. [Google Scholar]
- Mora, S.; Ridker, P.M. Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin (JUPITER)—Can C-reactive protein be used to target statin therapy in primary prevention? Am. J. Cardiol. 2006, 97, 33a–41a. [Google Scholar] [CrossRef]
- Golomb, B.A.; Evans, M.A. Statin adverse effects a review of the literature and evidence for a mitochondrial mechanism. Am. J. Cardiovasc. Drug 2008, 8, 373–418. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Tatsuno, I. Prevention of cardiovascular events with omega-3 polyunsaturated fatty acids and the mechanism involved. J. Atheroscler. Thromb. 2020, 27, 183–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guallar, E.; Aro, A.; Jimenez, F.J.; Martin-Moreno, J.M.; Salminen, I.; van’t Veer, P.; Kardinaal, A.F.M.; Gomez-Aracena, J.; Martin, B.C.; Kohlmeier, L.; et al. Omega-3 fatty acids in adipose tissue and risk of myocardial infarction—The EURAMIC study. Arterioscl. Throm. Vas. 1999, 19, 1111–1118. [Google Scholar] [CrossRef] [Green Version]
- Chang, C.H.; Tseng, P.T.; Chen, N.Y.; Lin, P.C.; Ling, P.Y.; Chang, J.P.C.; Kuo, F.Y.; Lin, J.; Wu, M.C.; Su, K.P. Safety and tolerability of prescription omega-3 fatty acids: A systematic review and meta-analysis of randomized controlled trials. Prostag. Leukotr. Ess. 2018, 129, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Grundy, S.M.; Stone, N.J.; Bailey, A.L.; Beam, C.; Birtcher, K.K.; Blumenthal, R.S.; Braun, L.T.; de Ferranti, S.; Faiella-Tommasino, J.; Forman, D.E.; et al. 2018 AHA/ACC/AACVPR/AAPA/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the management of blood cholesterol: A report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 139, e1082–e1143. [Google Scholar] [CrossRef] [PubMed]
- Fulcher, J.; O’Connell, R.; Voysey, M.; Emberson, J.; Blackwell, L.; Mihaylova, B.; Simes, J.; Collins, R.; Kirby, A.; Colhoun, H.; et al. Efficacy and safety of LDL-lowering therapy among men and women: Meta-analysis of individual data from 174 000 subjects in 27 randomised trials. Lancet 2015, 385, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.M.J.; Lee, H.; Lee, H.H.; Baek, J.; Heo, J.E.; Joo, H.J.; Hong, S.J.; Kim, H.C.; Korean Society of Lpid and Atherosclerosis Public Relations Committee. Dyslipidemia Fact Sheets in Korea 2020: An analysis of nationwide population-based data. J. Lipid. Atheroscler. 2021, 10, 202–209. [Google Scholar] [CrossRef]
- Barter, P.; Ginsberg, H.N. Effectiveness of combined statin plus omega-3 fatty acid therapy for mixed dyslipidemia. Am. J. Cardiol. 2008, 102, 1040–1045. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nambi, V.; Ballantyne, C.M. Combination therapy with statins and omega-3 fatty acids. Am. J. Cardiol. 2006, 98, 34i–38i. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.S.; Hong, S.J.; Cha, D.H.; Kim, K.S.; Kim, M.H.; Lee, J.W.; Jeong, M.H.; Jeong, J.O.; Lee, J.H.; Jeon, D.S.; et al. Comparison of the efficacy and safety of atorvastatin 40 mg/omega-3 fatty acids 4 g fixed-dose combination and atorvastatin 40 mg monotherapy in hypertriglyceridemic patients who poorly respond to atorvastatin 40 mg monotherapy: An 8-week, multicenter, randomized, double-blind phase III study. Clin. Ther. 2021, 43, 1419–1430. [Google Scholar] [CrossRef] [PubMed]
- Sudsakorn, S.; Bahadduri, P.; Fretland, J.; Lu, C. 2020 FDA Drug-drug Interaction Guidance: A comparison analysis and action plan by pharmaceutical industrial scientists. Curr. Drug Metab. 2020, 21, 403–426. [Google Scholar] [CrossRef] [PubMed]
- Braeckman, R.A.; Stirtan, W.G.; Soni, P.N. Pharmacokinetics of Eicosapentaenoic Acid in Plasma and Red Blood Cells After Multiple Oral Dosing With Icosapent Ethyl in Healthy Subjects. Clin. Pharm. Drug Dev. 2014, 3, 101–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenney, J.M.; Swearingen, D.; Di Spirito, M.; Doyle, R.; Pantaleon, C.; Kling, D.; Shalwitz, H.A. Study of the pharmacokinetic interaction between simvastatin and prescription omega-3-acid ethyl esters. J. Clin. Pharmacol. 2006, 46, 785–791. [Google Scholar] [CrossRef] [PubMed]
- Ciucanu, C.I.; Olariu, S.; Vlad, D.C.; Dumitrascu, V. Effect of rosuvastatin on the concentration of each fatty acid in the fraction of free fatty acids and total lipids in human plasma: The role of cholesterol homeostasis. Biochem. Biophys. Rep. 2020, 24, 100822. [Google Scholar] [CrossRef] [PubMed]
- Hirunpanich, V.; Sethabouppha, B.; Sato, H. Inhibitory effects of saturated and polyunsaturated fatty acids on the cytochrome p450 3a activity in rat liver microsomes. Biol. Pharm. Bull. 2007, 30, 1586–1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yao, H.T.; Chang, Y.W.; Lan, S.J.; Chen, C.T.; Hsu, J.T.; Yeh, T.K. The inhibitory effect of polyunsaturated fatty acids on human cyp enzymes. Life Sci. 2006, 79, 2432–2440. [Google Scholar] [CrossRef]
- Hu, N.; Hu, M.; Duan, R.; Liu, C.; Guo, H.; Zhang, M.; Yu, Y.; Wang, X.; Liu, L.; Liu, X. Increased levels of fatty acids contributed to induction of hepatic CYP3A4 activity induced by diabetes—In vitro evidence from HepG2 cell and Fa2N-4 cell lines. J. Pharmacol. Sci. 2014, 124, 433–444. [Google Scholar] [CrossRef] [Green Version]
- Nozue, T.; Michishita, I. Statin treatment alters serum n-3 to n-6 polyunsaturated fatty acids ratio in patients with dyslipidemia. Lipids Health Dis. 2015, 14, 67. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, N.; Hamazaki, T.; Ohta, M.; Okuda, K.; Urakaze, M.; Sawazaki, S.; Yamazaki, K.; Satoh, A.; Temaru, R.; Ishikura, Y.; et al. Joint effects of HMG-CoA reductase inhibitors and eicosapentaenoic acids on serum lipid profile and plasma fatty acid concentrations in patients with hyperlipidemia. Int. J. Clin. Lab. Res. 1999, 29, 22–25. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.I.; Hibbeln, J.R.; Mackey, R.H.; Muldoon, M.F. Statin treatment alters serum n-3 and n-6 fatty acids in hypercholesterolemic patients. Prostaglandins Leukot Essent Fat. Acids 2004, 71, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Kurisu, S.; Ishibashi, K.; Kato, Y.; Mitsuba, N.; Dohi, Y.; Nishioka, K.; Kihara, Y. Effects of lipid-lowering therapy with strong statin on serum polyunsaturated fatty acid levels in patients with coronary artery disease. Heart Vessels 2013, 28, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Eussen, S.R.; Geleijnse, J.M.; Giltay, E.J.; Rompelberg, C.J.; Klungel, O.H.; Kromhout, D. Effects of n-3 fatty acids on major cardiovascular events in statin users and non-users with a history of myocardial infarction. Eur. Heart J. 2012, 33, 1582–1588. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Parikh, R.; Bates, J.H.T.; Poynter, M.E.; Suratt, B.T.; Parsons, P.E.; Kien, C.L.; Heyland, D.K.; Crain, K.I.; Martin, J.; Garudathri, J.; et al. Pharmacokinetics of omega-3 fatty acids in patients with severe sepsis compared with healthy volunteers: A prospective cohort study. Clin. Nutr. 2020, 39, 958–965. [Google Scholar] [CrossRef] [PubMed]
- Zuijdgeest-Van Leeuwen, S.D.; Dagnelie, P.C.; Rietveld, T.; van den Berg, J.W.O.; Wilson, J.H.P. Incorporation and washout of orally administered n-3 fatty acid ethyl esters in different plasma lipid fractions. Brit. J. Nutr. 1999, 82, 481–488. [Google Scholar] [CrossRef] [Green Version]
- Park, J.; Kim, C.O.; Jin, B.H.; Yang, S.; Park, M.S.; Hong, T. Pharmacokinetic drug interaction between atorvastatin and ezetimibe in healthy Korean volunteers. Transl. Clin. Pharmacol. 2017, 25, 202–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Spirito, M.; Morelli, G.; Doyle, R.T.; Johnson, J.; McKenney, J. Effect of omega-3-acid ethyl esters on steady-state plasma pharmacokinetics of atorvastatin in healthy adults. Expert Opin. Pharmacother. 2008, 9, 2939–2945. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Li, J.; He, X.M.; Jia, M.M.; Liu, M.Z.; Li, H.Q.; Xiong, Z.J.; Fan, Y.; Li, W.Y. Development and validation of a liquid chromatography-tandem mass spectrometry method for simultaneous determination of amlodipine, atorvastatin and its metabolites ortho-hydroxy atorvastatin and para-hydroxy atorvastatin in human plasma and its application in a bioequivalence study. J. Pharmaceut. Biomed. 2013, 83, 101–107. [Google Scholar] [CrossRef]
- Fer, M.; Goulitquer, S.; Dreano, Y.; Berthou, F.; Corcos, L.; Amet, Y. Determination of polyunsatured fatty acid monoepoxides by high performance liquid chromatography-mass spectrometry. J. Chromatogr. A 2006, 1115, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Salm, P.; Taylor, P.J.; Kostner, K. Simultaneous quantification of total eicosapentaenoic acid, docosahexaenoic acid and arachidonic acid in plasma by high-performance liquid chromatography-tandem mass spectrometry. Biomed. Chromatogr. 2011, 25, 652–659. [Google Scholar] [CrossRef] [PubMed]
- de Lorgeril, M.; Salen, P.; Defaye, P.; Rabaeus, M. Recent findings on the health effects of omega-3 fatty acids and statins, and their interactions: Do statins inhibit omega-3? BMC Med. 2013, 11, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Group A (n = 17) | Group B (n = 18) | |
|---|---|---|
| Age (year) | 22.9 ± 4.3 | 24.6 ± 3.5 |
| Height (cm) | 175.9 ± 4.7 | 175.3 ± 3.5 |
| Weight (kg) | 69.4 ± 7.5 | 68.4 ± 6.6 |
| Parameter | Atorvastatin (n = 18) | 2-OH-Atorvastatin (n = 18) | DHA (n = 17) | EPA (n = 17) | ||||
|---|---|---|---|---|---|---|---|---|
| Alone | Combination | Alone | Combination | Alone | Combination | Alone | Combination | |
| AUCτ,ss (ng·h/mL) | 170.6 ± 70.2 | 175.3 ± 65.0 | 139.1 ± 48.7 | 164.9 ± 56.1 | 910.5 ± 520.8 | 204.0 ± 211.0 | 1175.2 ± 399.6 | 721.3 ± 298.5 |
| Cmax,ss (ng/mL) | 34.7 ± 10.7 | 40.0 ± 13.5 | 17.9 ± 6.0 | 23.1 ± 6.8 | 69.7 ± 27.6 | 22.4 ± 16.7 | 83.0 ± 27.9 | 51.4 ± 22.3 |
| Cmin,ss (ng/mL) | 1.0 ± 0.7 | 0.7 ± 0.4 | 1.2 ± 0.6 | 1.1 ± 0.6 | 25.0 ± 20.9 | 2.4 ± 6.4 | 32.4 ± 15.8 | 21.1 ± 12.1 |
| Tmax,ss (h) | 1.5 [0.5–4.0] | 1.0 [0.5–2.0] | 2.0 [0.5–4.0] | 1.75 [0.5–3.0] | 5.0 [3.0–7.0] | 5.0 [3.0–6.0] | 5.0 [3.0–7.0] | 5.0 [0.0–7.0] |
| Parameter | Reference | GMR | 90% CI for GMR | |
|---|---|---|---|---|
| Lower Limit (%) | Upper Limit (%) | |||
| Atorvastatin | ||||
| AUCτ,ss | Atorvastatin | 104.2 | 97.1 | 111.8 |
| Cmax,ss | Atorvastatin | 115.0 | 99.0 | 133.5 |
| 2-OH-atorvastatin | ||||
| AUCτ,ss | Atorvastatin | 118.5 | 111.3 | 126.2 |
| Cmax,ss | Atorvastatin | 130.1 | 120.7 | 140.1 |
| DHA | ||||
| AUCτ,ss | Omega-3 | 15.7 | 9.1 | 27.1 |
| Cmax,ss | Omega-3 | 32.0 | 24.3 | 42.2 |
| EPA | ||||
| AUCτ,ss | Omega-3 | 55.7 | 39.6 | 78.4 |
| Cmax,ss | Omega-3 | 58.9 | 48.7 | 71.2 |
| Omega-3 4 g | Omega-3 4 g + Atorvastatin 40 mg | |
| Group A | 20 (100.0) | 19 (100.0) |
| Epigastric discomfort | 3 (15.0) | |
| Alanine aminotransferase level increased | 1 (5.3) | |
| Blood creatine phosphokinase level increased | 1 (5.0) | 2 (10.5) |
| Levels of transaminases increased | 1 (5.3) | |
| Dysuria | 1 (5.0) | |
| Nasopharyngitis | 2 (10.0) | 2 (10.5) |
| Scratch | 1 (5.0) | |
| Atorvastatin 40 mg | Omega-3 4 g + Atorvastatin 40 mg | |
| Group B | 20 (100.0) | 18 (100.0) |
| Hordeolum | 3 (15.0) | |
| Diarrhea | 1 (5.3) | |
| Epigastric discomfort | 1 (5.0) | 2 (10.5) |
| Nasopharyngitis | 1 (5.3) | |
| Cellulitis | 1 (5.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.H.; Sunwoo, J.; Song, J.H.; Seo, Y.-B.; Jung, W.T.; Nam, K.-Y.; Kim, Y.; Lee, H.J.; Moon, J.; Jung, J.-G.; et al. Pharmacokinetic Interaction between Atorvastatin and Omega-3 Fatty Acid in Healthy Volunteers. Pharmaceuticals 2022, 15, 962. https://doi.org/10.3390/ph15080962
Kim JH, Sunwoo J, Song JH, Seo Y-B, Jung WT, Nam K-Y, Kim Y, Lee HJ, Moon J, Jung J-G, et al. Pharmacokinetic Interaction between Atorvastatin and Omega-3 Fatty Acid in Healthy Volunteers. Pharmaceuticals. 2022; 15(8):962. https://doi.org/10.3390/ph15080962
Chicago/Turabian StyleKim, Jae Hoon, Jung Sunwoo, Ji Hye Song, Yu-Bin Seo, Won Tae Jung, Kyu-Yeol Nam, YeSeul Kim, Hye Jung Lee, JungHa Moon, Jin-Gyu Jung, and et al. 2022. "Pharmacokinetic Interaction between Atorvastatin and Omega-3 Fatty Acid in Healthy Volunteers" Pharmaceuticals 15, no. 8: 962. https://doi.org/10.3390/ph15080962