
Efficacy and Safety of Trametinib in Neurofibromatosis Type 1-Associated Plexiform Neurofibroma and Low-Grade Glioma: A Systematic Review and Meta-Analysis

 , and
, and
Abstract
:1. Introduction
2. Results
2.1. Study Characteristics and Quality Assessment
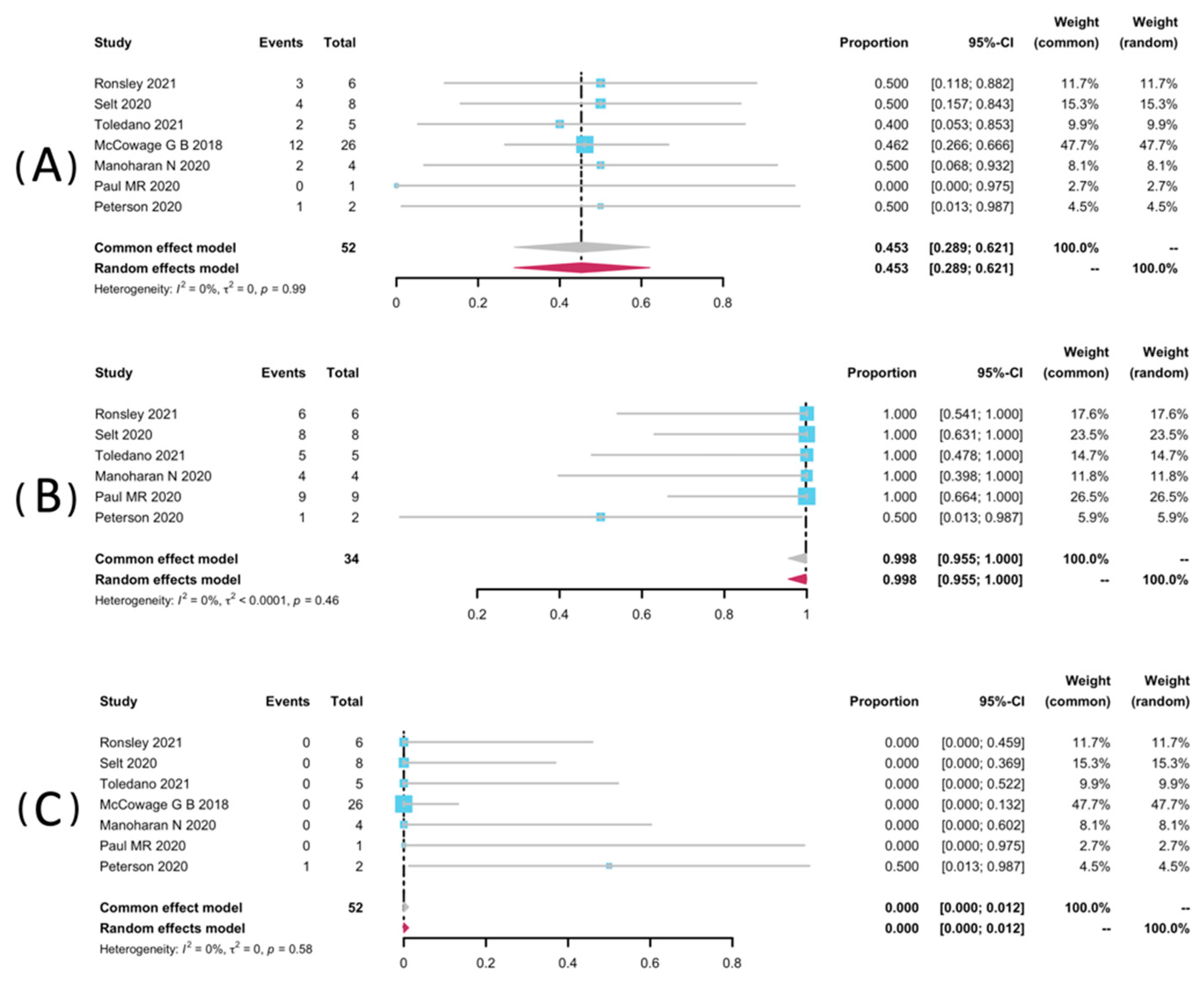
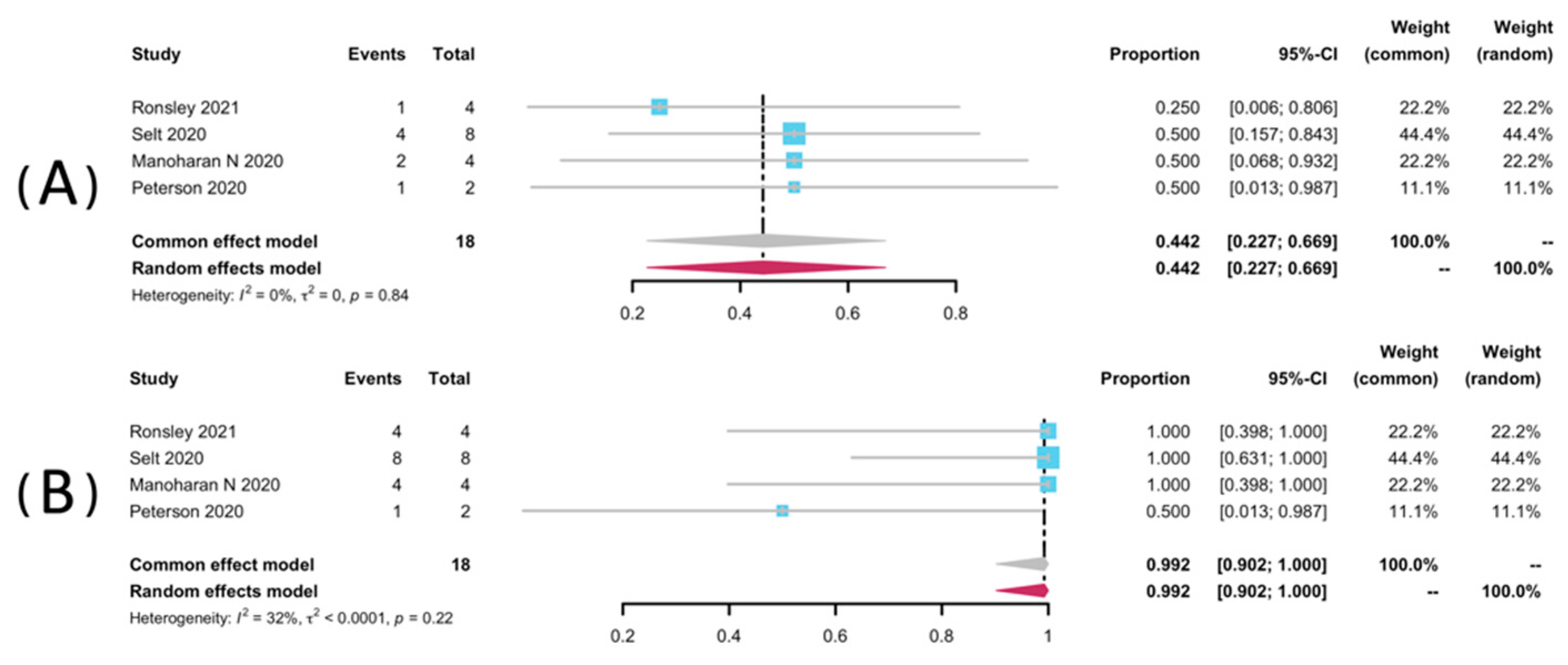
2.2. Efficacy
2.3. Safety
3. Discussion
4. Materials and Methods
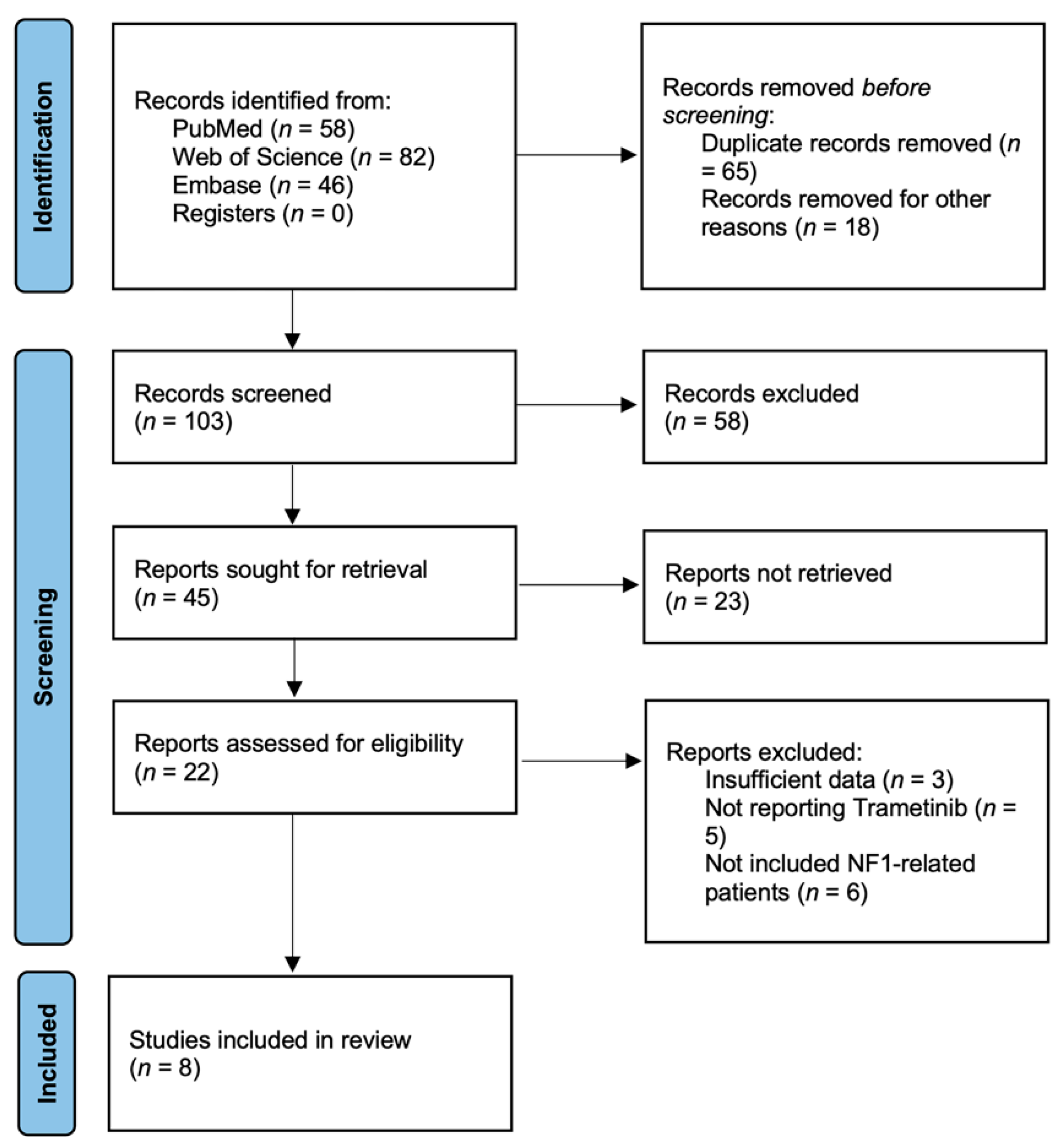
4.1. Systematic Literature Search
4.2. Inclusion Criteria and Exclusion Criteria
4.3. Data Extraction and Quality Assessment
4.4. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Huson, S.M.; Harper, P.S.; Compston, D.A. Von Recklinghausen neurofibromatosis. A clinical and population study in south-east Wales. Brain 1988, 111, 1355–1381. [Google Scholar] [CrossRef] [PubMed]
- Ferner, R.E.; Gutmann, D.H. Neurofibromatosis type 1 (NF1): Diagnosis and management. Handb Clin. Neurol. 2013, 115, 939–955. [Google Scholar] [PubMed]
- Lammert, M.; Friedman, J.M.; Kluwe, L.; Mautner, V.F. Prevalence of neurofibromatosis 1 in German children at elementary school enrollment. Arch. Dermatol. 2005, 141, 71–74. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonsgard, J.H.; Kwak, S.M.; Short, M.P.; Dachman, A.H. CT imaging in adults with neurofibromatosis-1: Frequent asymptomatic plexiform lesions. Neurology 1998, 50, 1755–1760. [Google Scholar] [CrossRef]
- Boulanger, J.M.; Larbrisseau, A. Neurofibromatosis type 1 in a pediatric population: Ste-Justine’s experience. Can. J. Neurol. Sci. 2005, 32, 225–231. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, R.; Kluwe, L.; Fuensterer, C.; Kentsch, M.; Friedrich, R.E.; Mautner, V.-F. Plexiform neurofibromas in children with neurofibromatosis type 1: Frequency and associated clinical deficits. J. Pediatr. 2011, 159, 652–655.e652. [Google Scholar] [CrossRef]
- Katz, D.; Lazar, A.; Lev, D. Malignant peripheral nerve sheath tumour (MPNST): The clinical implications of cellular signalling pathways. Expert Rev. Mol. Med. 2009, 11, e30. [Google Scholar] [CrossRef]
- Needle, M.N.; Cnaan, A.; Dattilo, J.; Chatten, J.; Philips, P.C.; Shochat, S.; Sutton, L.N.; Vaughan, S.N.; Zackai, E.H.; Zhao, H.; et al. Prognostic signs in the surgical management of plexiform neurofibroma: The Children’s Hospital of Philadelphia experience, 1974–1994. J. Pediatr. 1997, 131, 678–682. [Google Scholar] [CrossRef]
- Prada, C.E.; Rangwala, F.A.; Martin, L.J.; Lovell, A.M.; Saal, H.M.; Schorry, E.K.; Hopkin,, R.J. Pediatric plexiform neurofibromas: Impact on morbidity and mortality in neurofibromatosis type 1. J. Pediatr. 2012, 160, 461–467. [Google Scholar] [CrossRef]
- Oderich, G.S.; Sullivan, T.M.; Bower, T.C.; Gloviczki, P.; Miller, D.V.; Babovic-Vuksanovic, D.; Macedo, T.A.; Stanson, A. Vascular abnormalities in patients with neurofibromatosis syndrome type I: Clinical spectrum, management, and results. J. Vasc. Surg. 2007, 46, 475–484. [Google Scholar] [CrossRef] [Green Version]
- Hivelin, M.; Plaud, B.; Hemery, F.; Boulat, C.; Ortonne, N.; Valleyrie-Allanore, L.; Wolkenstein, P.; Lantieri, L. Low Rates of Blood Transfusion in Elective Resections of Neurofibromas in a Cohort Study: Neurofibroma Length as a Predictor of Transfusion Requirement. Plast Reconstr. Surg. 2016, 137, 700e–711e. [Google Scholar] [CrossRef]
- Konno, E.; Kishi, K. Use of the LigaSure™ vessel sealing system in neurofibroma excision to control postoperative bleeding. J. Plast Reconstr. Aesthet. Surg. 2012, 65, 814–817. [Google Scholar] [CrossRef]
- Ratner, N.; Miller, S.J. A RASopathy gene commonly mutated in cancer: The neurofibromatosis type 1 tumour suppressor. Nat. Rev. Cancer 2015, 15, 290–301. [Google Scholar] [CrossRef]
- Wise, J.B.; Cryer, J.E.; Belasco, J.B.; Jacobs, I.; Elden, L. Management of head and neck plexiform neurofibromas in pediatric patients with neurofibromatosis type 1. Arch. Otolaryngol. Head. Neck. Surg. 2005, 131, 712–718. [Google Scholar] [CrossRef] [Green Version]
- Friedrich, R.E.; Diekmeier, C. Peripheral nerve sheath tumors of the upper extremity and hand in patients with neurofibromatosis type 1: Topography of tumors and evaluation of surgical treatment in 62 patients. GMS Interdiscip. Plast. Reconstr. Surg. DGPW 2017, 6, Doc15. [Google Scholar]
- Avery, R.A.; Katowitz, J.A.; Fisher, M.J.; Heidary, G.; Dombi, E.; Packer, R.J.; Widemann, B.C. Orbital/Periorbital Plexiform Neurofibromas in Children with Neurofibromatosis Type 1: Multidisciplinary Recommendations for Care. Ophthalmology 2017, 124, 123–132. [Google Scholar] [CrossRef] [Green Version]
- Louis, D.N.; Perry, A.; Reifenberger, G.; von Deimling, A.; Figarella-Branger, D.; Cavenee, W.K.; Ohgaki, H.; Wiestlrt, O.D.; Kleihues, P.; Ellison, D.W. The 2016 World Health Organization Classification of Tumors of the Central Nervous System: A summary. Acta Neuropathol. 2016, 131, 803–820. [Google Scholar] [CrossRef] [Green Version]
- Gutmann, D.H.; Ferner, R.E.; Listernick, R.H.; Korf, B.R.; Wolters, P.L.; Johnson, K.J. Neurofibromatosis type 1. Nat. Rev. Dis. Primers 2017, 3, 17004. [Google Scholar] [CrossRef]
- Miao, R.; Wang, H.; Jacobson, A.; Lietz, A.P.; Choy, E.; Raskin, K.A.; Schwab, J.H.; Deshpande, V.; Nielse, G.P.; DeLaney, T.F.; et al. Radiation-induced and neurofibromatosis-associated malignant peripheral nerve sheath tumors (MPNST) have worse outcomes than sporadic MPNST. Radiother Oncol. 2019, 137, 61–70. [Google Scholar] [CrossRef]
- Baumert, B.G.; Hegi, M.E.; van den Bent, M.J.; Deimling, A.v.; Gorlia, T.; Hoang-Xuan, K.; Brandes, A.A.; Kantor, G.; Taphoorn, M.J.B.; Hassel, M.B. Temozolomide chemotherapy versus radiotherapy in high-risk low-grade glioma (EORTC 22033-26033): A randomised, open-label, phase 3 intergroup study. Lancet Oncol. 2016, 17, 1521–1532. [Google Scholar] [CrossRef] [Green Version]
- Buckner, J.C.; Shaw, E.G.; Pugh, S.L.; Chakravarti, A.; Gilbert, M.R.; Barger, G.R.; Coons, S.; Ricci, P.; Bullard, D.; Brown, P.D.; et al. Radiation plus Procarbazine, CCNU, and Vincristine in Low-Grade Glioma. N. Engl. J. Med. 2016, 374, 1344–1355. [Google Scholar] [CrossRef] [PubMed]
- Bell, E.; Won, M.; Fleming, J.; Becker, A.; McElroy, J.; Shaw, E.G.; Mehta, M.P.; Brachman, D.G.; Gertler, S.; Murtha, A.D. Comprehensive prognostic and predictive molecular subgroup analysis within the high-risk treatment arms of NRG oncology/RTOG 9802: A phase III trial of RT versus RT+ PCV in high-risk low-grade gliomas. Int. J. Radiat. Oncol. Biol. Phys. 2019, 105, S78–S79. [Google Scholar] [CrossRef]
- Castro, E.; Goh, C.; Olmos, D.; Saunders, E.; Leongamornlert, D.; Tymrakiewicz, M.; Mahmud, N.; Dadaev, T.; Govindasami, K.; Guy, M. Germline BRCA mutations are associated with higher risk of nodal involvement, distant metastasis, and poor survival outcomes in prostate cancer. J. Clin. Oncol. 2013, 31, 1748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van den Bent, M.J.; Brandes, A.A.; Taphoorn, M.J.; Kros, J.M.; Kouwenhoven, M.C.M.; Delattre, J.; Bernsen, H.J.J.A.; Frenay, M.; Tijssen, C.C.; Grisold., W. Adjuvant procarbazine, lomustine, and vincristine chemotherapy in newly diagnosed anaplastic oligodendroglioma: Long-term follow-up of EORTC brain tumor group study 26951. J. Clin. Oncol. 2013, 31, 344–350. [Google Scholar] [CrossRef]
- Peterson, R.K.; McKeown, T.; Tabori, U.; Bartels, U.; Bouffet, E.; Janzen, L. Neuropsychological impact of trametinib in pediatric low-grade glioma: A case series. Pediatr Blood Cancer 2020, 67, e28690. [Google Scholar] [CrossRef]
- Gururangan, S.; Fangusaro, J.; Poussaint, T.Y.; McLendon, R.E.; Onar-Thomas, A.; Wu, S.; Packer, R.J.; Banerjee, A.; Gilbertson, R.J.; Fahey, F. Efficacy of bevacizumab plus irinotecan in children with recurrent low-grade gliomas--a Pediatric Brain Tumor Consortium study. Neuro. Oncol. 2014, 16, 310–317. [Google Scholar] [CrossRef] [Green Version]
- McCubrey, J.A.; Steelman, L.S.; Chappell, W.H.; Abrams, S.L.; Wong, E.W.T.; Chang, F.; Lehmann, B.; Terrian, D.M.; Milella, M.; Tafuri, A. Roles of the Raf/MEK/ERK pathway in cell growth, malignant transformation and drug resistance. Biochim. Biophys. Acta 2007, 1773, 1263–1284. [Google Scholar] [CrossRef] [Green Version]
- Yap, Y.S.; McPherson, J.R.; Ong, C.K.; Rozen, S.G.; The, B.; Lee, A.S.G.; Callen, D.F. The NF1 gene revisited—From bench to bedside. Oncotarget 2014, 5, 5873–5892. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.; Giaccone, G. MEK inhibitors under development for treatment of non-small-cell lung cancer. Expert Opin. Investig. Drugs 2018, 27, 17–30. [Google Scholar] [CrossRef]
- Lian, T.; Li, C.; Wang, H. Trametinib in the treatment of multiple malignancies harboring MEK1 mutations. Cancer Treat. Rev. 2019, 81, 101907. [Google Scholar] [CrossRef]
- Perreault, S.; Larouche, V.; Tabori, U.; Hawkin, C.; Lippé, S.; Ellezam, B.; Décarie, J.C.; Théoret, Y.; Métras, M.É.; Sultan, S. A phase 2 study of trametinib for patients with pediatric glioma or plexiform neurofibroma with refractory tumor and activation of the MAPK/ERK pathway: TRAM-01. BMC Cancer 2019, 19, 1250. [Google Scholar] [CrossRef] [Green Version]
- Ronsley, R.; Hounjet, C.D.; Cheng, S.; Rassekh, S.R.; Duncan, W.J.; Dunham, C.; Gardiner, J.; Ghag, A.; Ludemann, J.P.; Wensley, D. Trametinib therapy for children with neurofibromatosis type 1 and life-threatening plexiform neurofibroma or treatment-refractory low-grade glioma. Cancer Med. 2021, 10, 3556–3564. [Google Scholar] [CrossRef]
- Selt, F.; van Tilburg, C.M.; Bison, B.; Sievers, P.; Harting, I.; Ecker, J.; Pajtler, K.W.; Sahm, F.; Bahr, A.; Simon, M. Response to trametinib treatment in progressive pediatric low-grade glioma patients. J. Neurooncol. 2020, 149, 499–510. [Google Scholar] [CrossRef]
- Toledano, H.; Dotan, G.; Friedland, R.; Cohen, R.; Yassur, I.; Toledano-Alhadef, H.; Constantini, S.; Rootman, M.S. Trametinib for orbital plexiform neurofibromas in young children with neurofibromatosis type 1. Childs Nerv. Syst. 2021, 37, 1909–1915. [Google Scholar] [CrossRef]
- McCowage, G.B.; Mueller, S.; Pratilas, C.A.; Hargrave, D.R.; Moertel, C.L.; Whitlock, J.; Fox, E.; Hingorani, P.; Russo, M.W.; Dasgupta, K. Trametinib in pediatric patients with neurofibromatosis type 1 (NF-1)–associated plexiform neurofibroma: A phase I/IIa study. Am. Soc. Clin. Oncol. 2018, 36, 10504. [Google Scholar] [CrossRef]
- Manoharan, N.; Choi, J.; Chordas, C.; Zimmerman, M.A.; Scully, J.; Clymer, J.; Filbin, M.; Ullrich, N.J.; Bandopadhayay, P.; Chi, S.N. Trametinib for the treatment of recurrent/progressive pediatric low-grade glioma. J. Neurooncol. 2020, 149, 253–262. [Google Scholar] [CrossRef]
- Geoerger, B.; Moertel, C.L.; Whitlock, J.; McCowage, B.; Kieran, M.W.; Broniscer, A.; Hargrave, D.R.; Hingorani, P.; Kilburn, L.B.; Mueller, S. Phase 1 trial of trametinib alone and in combination with dabrafenib in children and adolescents with relapsed solid tumors or neurofibromatosis type 1 (NF1) progressive plexiform neurofibromas (PN). Am. Soc. Clin. Oncol. 2018, 36, 10537. [Google Scholar] [CrossRef]
- Paul, M.R.; Pehlivan, K.C.; Milburn, M.; Yeh-Nayre, L.; Elster, J.; Crawford, J.R. Trametinib-based Treatment of Pediatric CNS Tumors: A Single Institutional Experience. J. Pediatr. Hematol. Oncol. 2020, 42, e730–e737. [Google Scholar] [CrossRef]
- Tiffany, N.; Kathleen, M.M.; Molly, H.; Jean, M.L.; Nicholas, F.; Katheleen, D. LGG-27. Targeted Therapy for Pediatric Low-Grade Gliomas and Plexiform Neurofibromas with Trametinib. Neuro Oncol. 2020, 3, iii371. [Google Scholar]
- Sato, A.; Millard, N.; Perez, F.; Barker, F.G.; Connor, S.; Evans, D.G.; Fisher, M.J. NFB-13. Trametinib for Plexiform Neurofibroma and Recurrent Low-Grade Glioma. Neuro-Oncology 2020, 22, iii420. [Google Scholar] [CrossRef]
- Dombi, E.; Ardern-Holmes, S.L.; Babovic-Vuksanovic, D.; Barker, F.G.; Connor, S.; Evans, D.G.; Fisher, M.J.; Goutagny, S.; Harris, G.J.; Jaramillo, D. Recommendations for imaging tumor response in neurofibromatosis clinical trials. Neurology 2013, 81, S33–S40. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wen, P.Y.; Chang, S.M.; Van den Bent, M.J.; Vogelbaum, M.A.; Macdonald, D.R.; Lee, E.Q. Response Assessment in Neuro-Oncology Clinical Trials. J. Clin. Oncol. 2017, 35, 2439–2449. [Google Scholar] [CrossRef] [PubMed]
- Markham, A.; Keam, S.J. Selumetinib: First Approval. Drugs 2020, 80, 931–937. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.; Yoon, H.M.; Lee, B.H.; Kim, P.H.; Kim, K.W. Efficacy and Safety of Selumetinib in Pediatric Patients With Neurofibromatosis Type 1: A Systematic Review and Meta-analysis. Neurology 2022, 98, e938–e946. [Google Scholar] [CrossRef]
- Goerne, R.; Bogdahn, U.; Hau, P. Procarbazine—A traditional drug in the treatment of malignant gliomas. Curr. Med. Chem. 2008, 15, 1376–1387. [Google Scholar] [CrossRef]
- el Saghir, N.S.; Hawkins, K.A. Hepatotoxicity following vincristine therapy. Cancer 1984, 54, 2006–2008. [Google Scholar] [CrossRef]
- Park, S.B.; Goldstein, D.; Krishnan, A.V.; Lin, C.S.Y.; Friedlander, M.L.; Cassidy, J.; Koltzenburg, M.; Kiernan, M.C. Chemotherapy-induced peripheral neurotoxicity: A critical analysis. CA Cancer J. Clin. 2013, 63, 419–437. [Google Scholar] [CrossRef]
- Jutras, G.; Bélanger, K.; Letarte, N.; Adam, J.P.; Roberge, D.; Lemieux, B.; Lemieux-Blanchard, É.; Masucci, L.; Ménard, C.; Bahary, J.P. Procarbazine, lomustine and vincristine toxicity in low-grade gliomas. Curr. Oncol. 2018, 25, e33–e39. [Google Scholar] [CrossRef] [Green Version]
- Kondyli, M.; Larouche, V.; Saint-Martin, C.; Ellezam, B.; Pouliot, L.; Sinnett, D.; Legault, G.; Crevier, L.; Weil, A.; Farmer, J.P. Trametinib for progressive pediatric low-grade gliomas. J. Neurooncol. 2018, 140, 435–444. [Google Scholar] [CrossRef]
- Blumenschein, G.R., Jr.; Smit, E.F.; Planchard, D.; Kim, D.W.; Cadranel, J.; Pas, T.D.; Dunphy, F.; Udud, K.; Ahn, M.J.; Hanna, N.H. A randomized phase II study of the MEK1/MEK2 inhibitor trametinib (GSK1120212) compared with docetaxel in KRAS-mutant advanced non-small-cell lung cancer (NSCLC)†. Ann. Oncol. 2015, 26, 894–901. [Google Scholar] [CrossRef]
- Anforth, R.; Liu, M.; Nguyen, B.; Pablo, U.; Kefford, R.; Clements, A.; Long, G.V.; Fernandez-Peñas, P. Acneiform eruptions: A common cutaneous toxicity of the MEK inhibitor trametinib. Australas J. Derm. 2014, 55, 250–254. [Google Scholar] [CrossRef]
- Weiss, B.; Plotkin, S.; Widemann, B.; Tonsgard, J.H.; Blakeley, J.; Allen, J.C.; Schorry, E.; Korf, B.; Robison, N.J. NFM-06. NF106: Phase 2 trial of the MEK inhibitor PD-0325901 in adolescents and adults with NF1-related plexiform neurofibromas: An NF clinical trials consortium study. Neuro Oncol. 2018, 20, i143. [Google Scholar] [CrossRef]
- Pérez, J.P.M.; Muchart, J.; López, V.S.; Capella, M.S.; Salvador, N.; Jaume, S.P.; Martínez, O.C.; La Madrid, A.M. Targeted therapy for pediatric low-grade glioma. Childs Nerv. Syst. 2021, 37, 2511–2520. [Google Scholar] [CrossRef]
- Klesse, L.J.; Jordan, J.T.; Radtke, H.B.; Rosser, T.; Schorry, E.; Ullrich, N.; Viskochil, D.; Knight, P.; Plotkin, S.R.; Yohay, K. The Use of MEK Inhibitors in Neurofibromatosis Type 1-Associated Tumors and Management of Toxicities. Oncologist 2020, 25, e1109–e1116. [Google Scholar] [CrossRef] [Green Version]
- Dombi, E.; Solomon, J.; Gillespie, A.J.; Fox, E.; Balis, F.M.; Patronas, N.; Korf, B.R.; Babovic-Vuksanovic, D.; Packer, R.J.; Belasco, J. NF1 plexiform neurofibroma growth rate by volumetric MRI: Relationship to age and body weight. Neurology 2007, 68, 643–647. [Google Scholar] [CrossRef]
- Kluwe, L.; Nguyen, R.; Vogt, J.; Bengesser, K.; Mussotter, T.; Friedrich, R.E.; Jett, K.; Kehrer-Sawatzki, H.; Mautner, V.F. Internal tumor burden in neurofibromatosis Type I patients with large NF1 deletions. Genes Chromosomes Cancer 2012, 51, 447–451. [Google Scholar] [CrossRef]
- Cai, W.; Steinberg, S.M.; Bredella, M.A.; Basinsky, G.; Somarouthu, B.; Plotkin, S.R.; Solomon, J.; Widemann, B.C.; Harris, G.J.; Dombi, E. Volumetric MRI Analysis of Plexiform Neurofibromas in Neurofibromatosis Type 1: Comparison of Two Methods. Acad. Radiol. 2018, 25, 144–152. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 372. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; DeBeer, H. GRADE guidelines: 1. Introduction-GRADE evidence profiles and summary of findings tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services NIoH; National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE); U.S. Department of Health and Human Services NIoH: Washington, DC, USA; National Cancer Institute: Bethesda, MD, USA, 2009. [Google Scholar]
- Alduzzi, S.R.G.; Schwarzer, G. How to perform a meta-analysis with R: A practical tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J. Cochrane Handbook for Systematic Reviews of Interventions; John Wiley & Sons: Hoboken, NJ, USA, 2019. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Trametinib Dosage | NR | 0.025 mg/kg (n = 3), 0.032 mg/kg (n = 2), 0.016 mg/kg (n = 1) Daily | 0.03 mg/kg Daily | 0.032 mg/kg Daily | 0.025 mg/kg (n = 21), 0.032 mg/kg (n = 1), 0.040 mg/kg (n = 4) Daily | 0.025 mg/kg Daily | 0.025 mg/kg 0.04 mg/kg Daily | 0.025 mg/kg Daily |
| Tumor | LGG | pNF and LGG | LGG | pNF | pNF | pNF | pNF | pNF |
| Age, year (Range) | Median 3 (0.5–6.8) | Median 9 (1–14) | Median 2.1 (0.5–9.9) | Median 2.3 (0.5–3.2) | Median 5.5 (1–16) | Median 14.7 (7.3–25.9) | Median 8 (0–18) | Median 10.8 (5.2–17.1) |
| Included Patients number | 2 | 6 | 8 | 5 | 26 | 4 | 40 | 1 |
| Patient Number (Male/Female) | 8 (5/3) | 6 (3/3) | 18 (8/10) | 5 (1/4) | 26 | 10 (6/5) | 40 | 14 (9/5) |
| Enrollment period | 2014–2019 | 2017.12–2020.5 | 2015–2019 | 2016.1–2018.8 | 2014.4–2021.6 | 2016–2018 | 2014.4–2021.6 | 2015.1–2019.9 |
| Country | USA | Canada | Germany | Israel | Australia | USA | France | USA |
| Institution | Multicenter | University of British Columbia | Multicenter | Multicenter | Multicenter | Multicenter | Multicenter | Multicenter |
| Study | Peterson et al. 2020 [25] | Ronsley et al. 2021 [32] | Selt et al. 2020 [33] | Toledano et al. 2021 [34] | McCowage et al. 2018 [35] | Manoharan et al. 2020 [36] | Geoerger et al. 2018 [37] | Paul et al. 2020 [38] |
| Study | Criteria |
|---|---|
| Ronsley et al., 2021 [32] | LGG: Partial response: decrease ≥50% Minor response: decrease 25–49% Progression: increase ≥25% pNF: Partial response: decrease ≥20% Progression: increase ≥20% |
| Selt et al., 2020 [33] | Complete response: no evidence of residual or recurrent tumor or dissemination Partial response: decrease ≥50% Minor response: decrease 25–50% without new lesions Stable disease: change in volume between +25–−25% without new lesions Progression: increase ≥25% or appearance of new lesions |
| Toledano et al., 2021 [34] | NA |
| McCowage et al., 2018 [35] | Dombi criteria [41] |
| Manoharan et al., 2020 [36] | RANO criteria [42] Minor response: decrease 25–50% |
| Peterson et al., 2020 [25] | Radiological response, radiologically stable, and progression without clear definition |
| Geoerger et al., 2018 [37] | Dombi criteria [41] |
| Paul et al., 2020 [38] | Complete response, partial response, stable disease, progressive disease without clear definition. |
| Quality of Evidence | Low | Moderate | Moderate | Low | Low | Moderate | Low | Very Low |
|---|---|---|---|---|---|---|---|---|
| Dose effect | NA | NA | NA | NA | NA | NA | NA | NA |
| Effect size | Moderate | Moderate | Moderate | Small | Small | Moderate | NA | Small |
| Publication bias | √ | √ | √ | √ | √ | √ | √ | √ |
| Imprecision | √ | √ | √ | √ | √ | √ | √ | √ |
| Indirectness | √ | √ | √ | √ | √ | √ | √ | √ |
| Inconsistency | √ | √ | √ | √ | √ | √ | √ | √ |
| Risk of bias | × | √ | √ | √ | √ | √ | √ | × |
| Study design | Cases | Retrospective | Retrospective | Retrospective | Non-randomized clinical trial | Non-randomized clinical trial | Non-randomized clinical trial | Retrospective |
| Study | Peterson et al. 2020 [25] | Ronsley et al. 2021 [32] | Selt et al. 2020 [33] | Toledano et al. 2021 [34] | McCowage et al. 2018 [35] | Manoharan et al. 2020 [36] | Geoerger et al. 2018 [37] | Paul et al. 2020 [38] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, D.; Ge, L.; Guo, Z.; Li, Y.; Zhu, B.; Wang, W.; Wei, C.; Li, Q.; Wang, Z. Efficacy and Safety of Trametinib in Neurofibromatosis Type 1-Associated Plexiform Neurofibroma and Low-Grade Glioma: A Systematic Review and Meta-Analysis. Pharmaceuticals 2022, 15, 956. https://doi.org/10.3390/ph15080956
Wang D, Ge L, Guo Z, Li Y, Zhu B, Wang W, Wei C, Li Q, Wang Z. Efficacy and Safety of Trametinib in Neurofibromatosis Type 1-Associated Plexiform Neurofibroma and Low-Grade Glioma: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2022; 15(8):956. https://doi.org/10.3390/ph15080956
Chicago/Turabian StyleWang, Dun, Lingling Ge, Zizhen Guo, Yuehua Li, Beiyao Zhu, Wei Wang, Chengjiang Wei, Qingfeng Li, and Zhichao Wang. 2022. "Efficacy and Safety of Trametinib in Neurofibromatosis Type 1-Associated Plexiform Neurofibroma and Low-Grade Glioma: A Systematic Review and Meta-Analysis" Pharmaceuticals 15, no. 8: 956. https://doi.org/10.3390/ph15080956