
Dexamethasone Increases the Anesthetic Success in Patients with Symptomatic Irreversible Pulpitis: A Meta-Analysis

 ,
,  , , and
, , and 
Abstract
:1. Introduction
2. Material and Methods
2.1. Registration
2.2. Focused Question
2.3. Population, Interventions, Control, and Outcomes (PICO) Approach
2.3.1. Inclusion Criteria
2.3.2. Exclusion Criteria
2.4. Information Search
2.5. Risk of Bias Assessment
2.6. Information Extraction
2.7. Statistical Analysis
3. Results
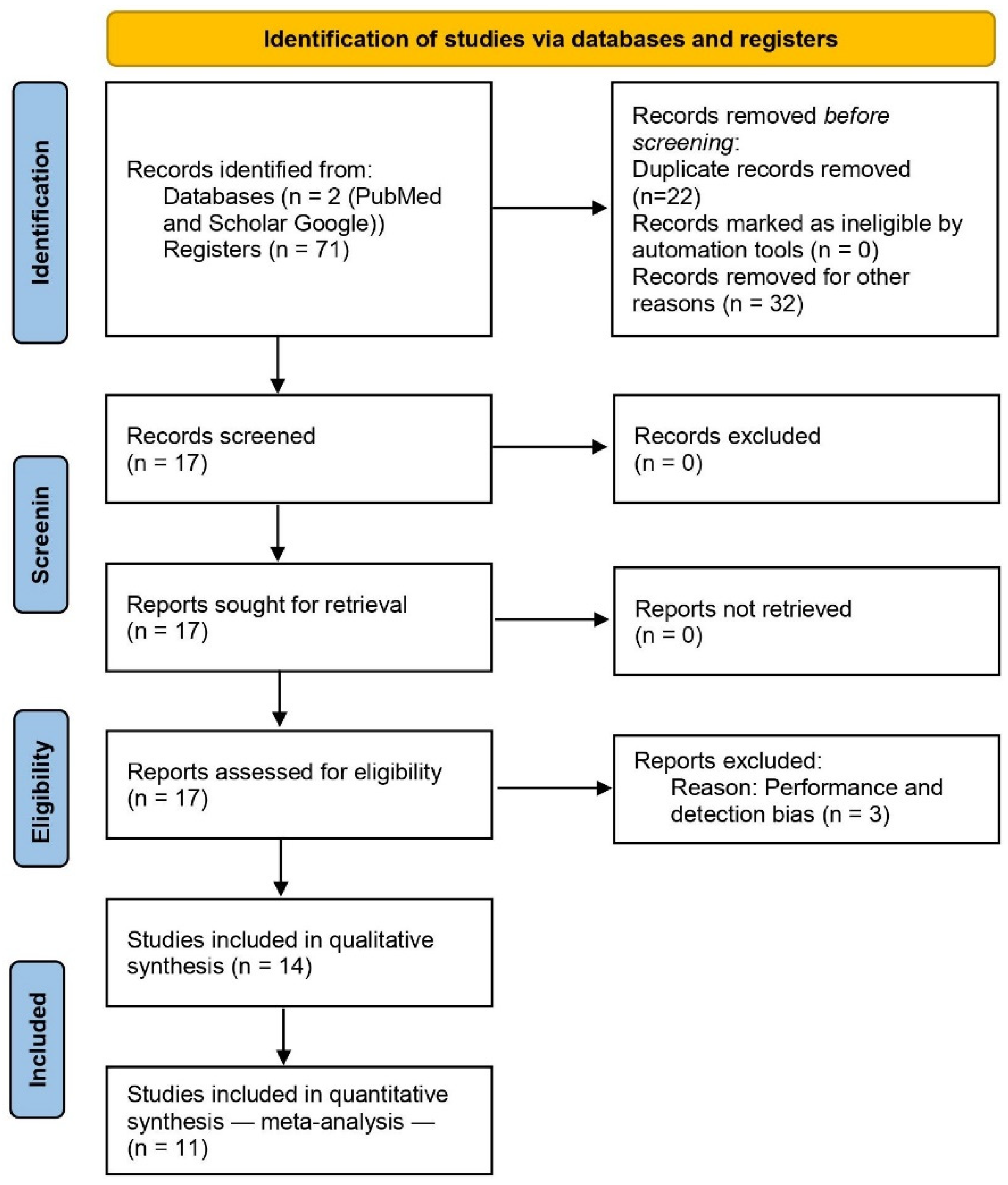
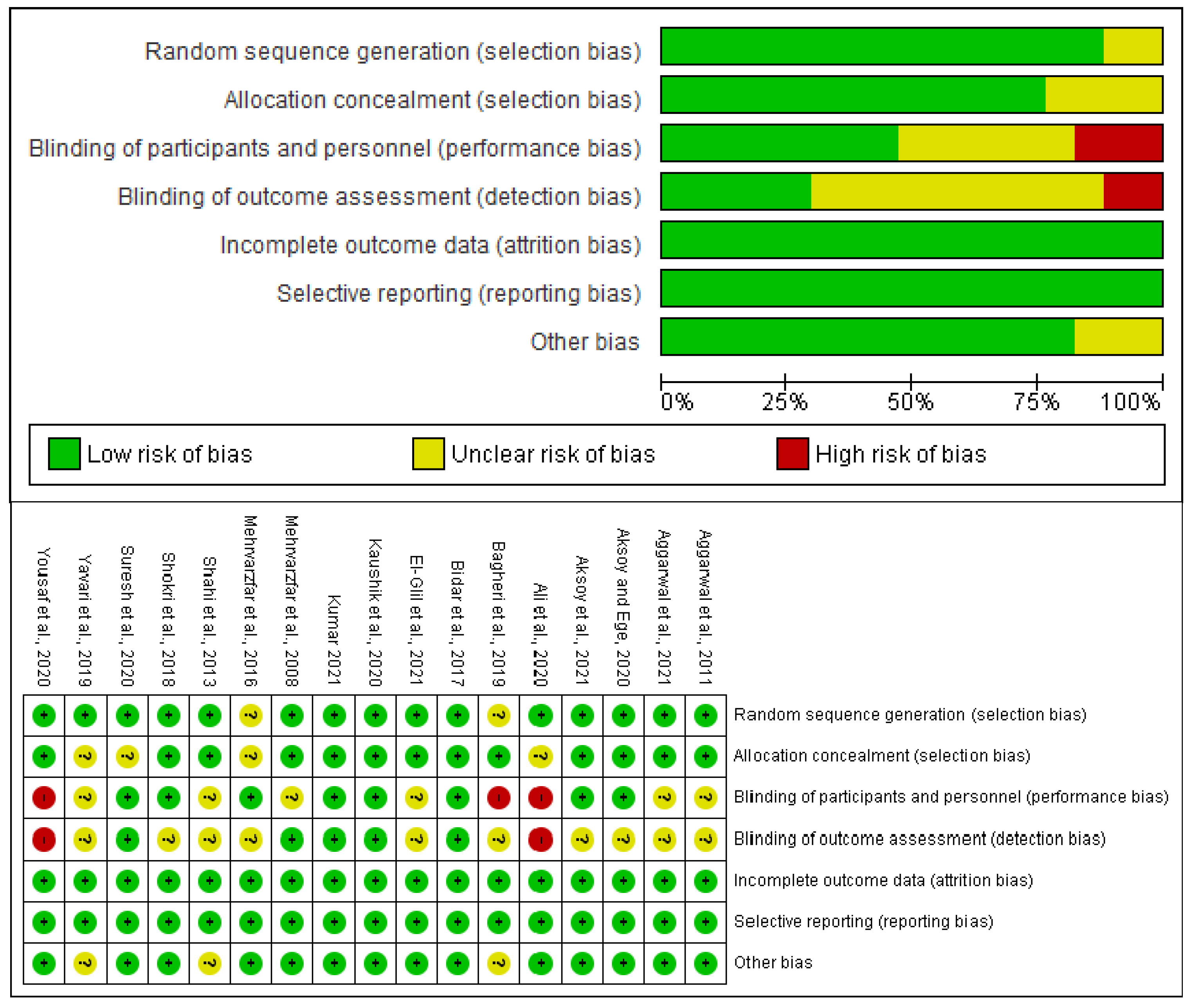
3.1. Search and Evaluation of Bias
3.2. Qualitative Analysis
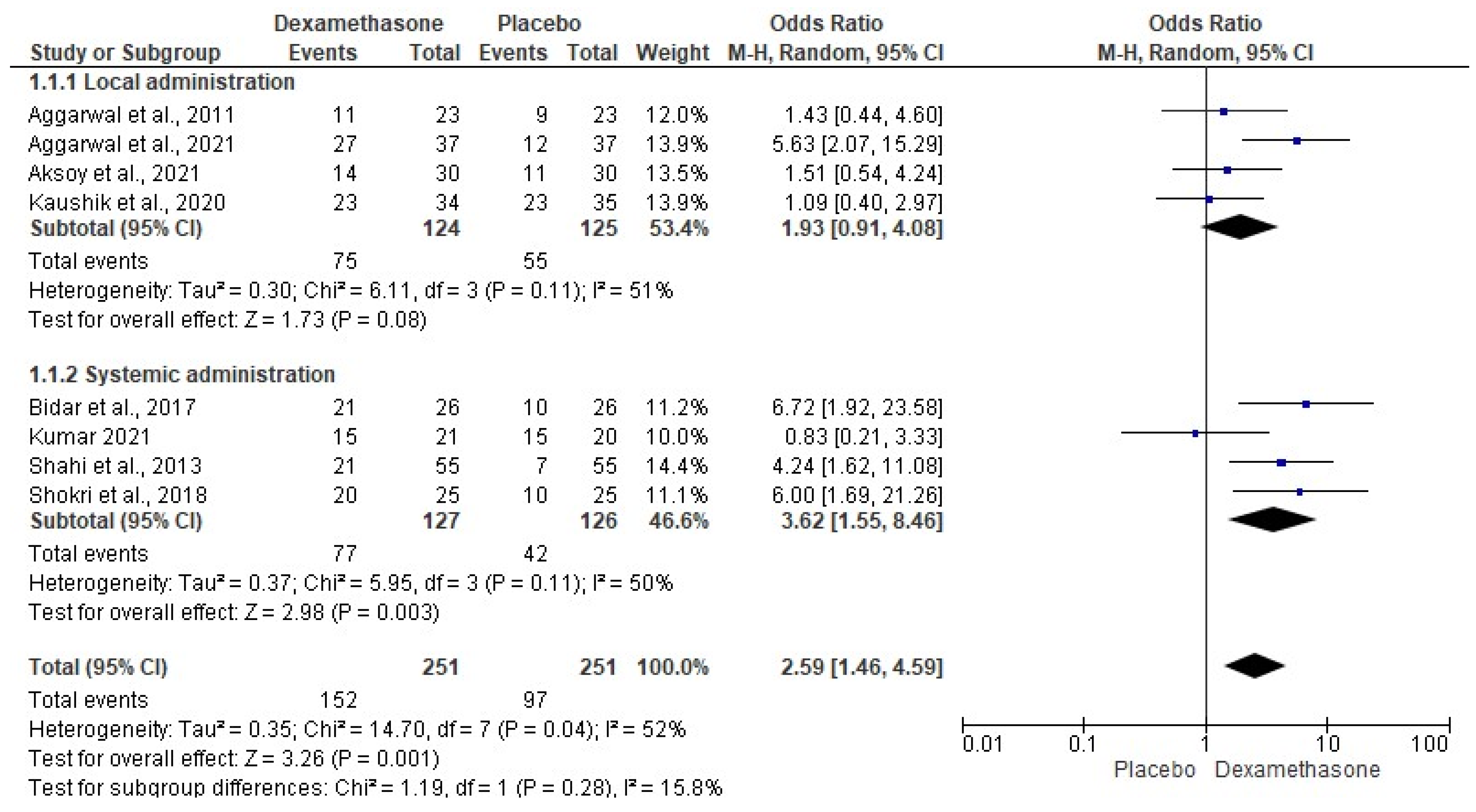
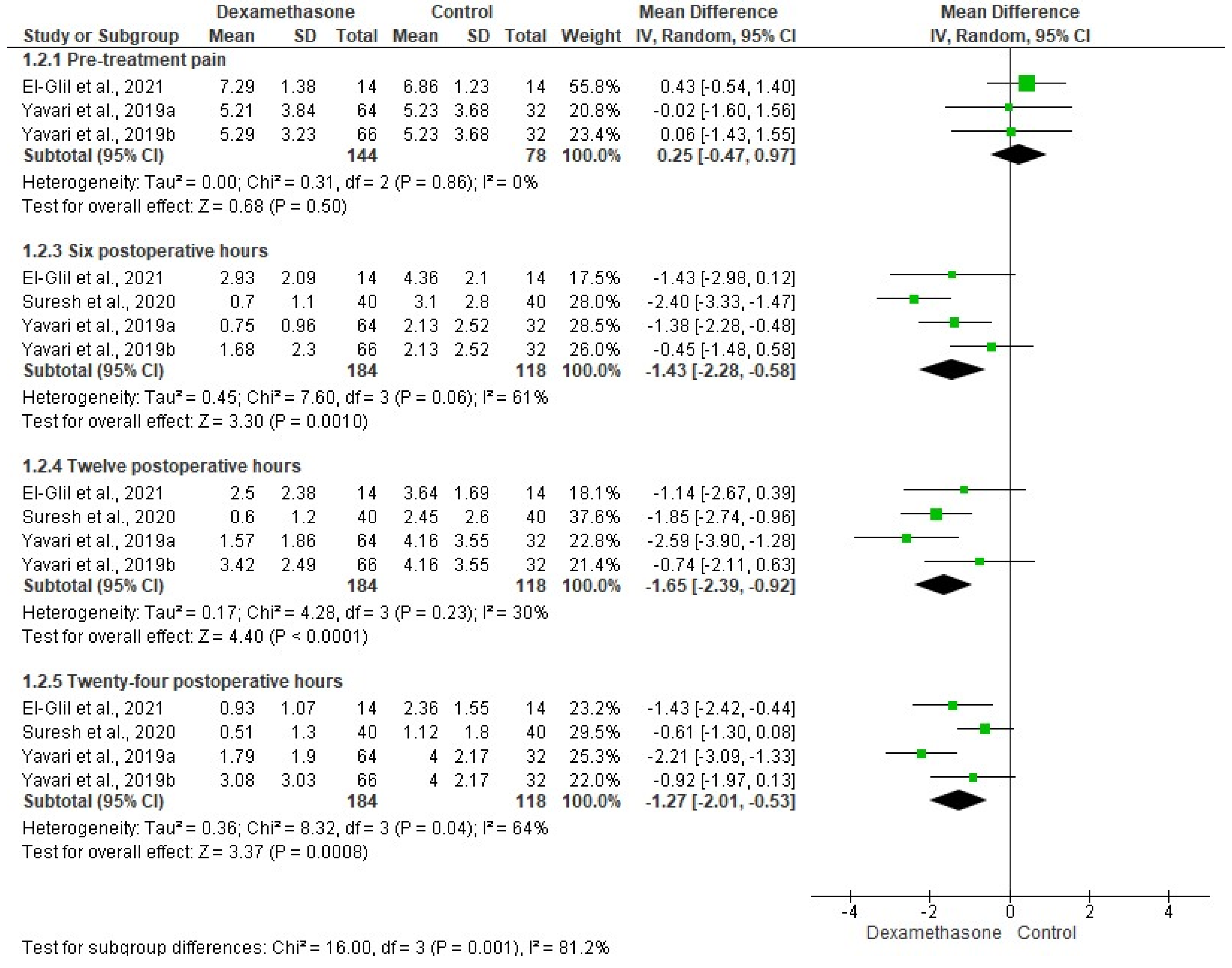
3.3. Quantitative Evaluation
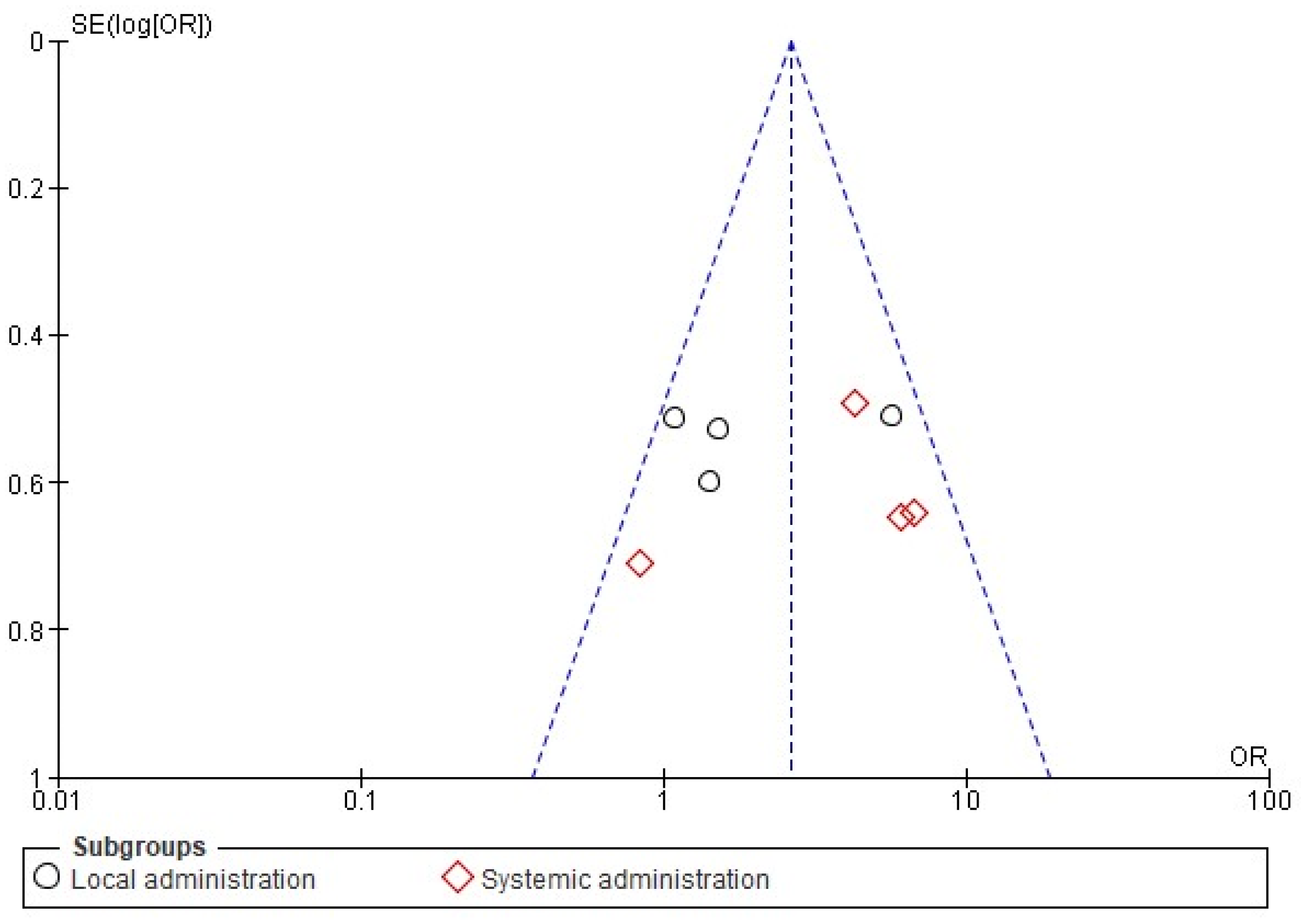
3.4. The Sensitivity Evaluation and Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zanjir, M.; Lighvan, N.L.; Yarascavitch, C.; Beyene, J.; Shah, P.S.; Azarpazhooh, A. Efficacy and safety of pulpal anesthesia strategies during endodontic treatment of permanent mandibular molars with symptomatic irreversible pulpitis: A systematic review and network meta-analysis. J. Endod. 2019, 45, 1435–1464.e10. [Google Scholar] [CrossRef] [PubMed]
- Costa, Y.M.; de Souza, P.R.J.; Marques, V.A.S.; Conti, P.C.R.; Vivan, R.R.; Duarte, M.A.H.; Bonjardim, L.R. Intraoral somatosensory alterations impact pulp sensibility testing in patients with symptomatic irreversible pulpitis. J. Endod. 2020, 46, 786–793. [Google Scholar] [CrossRef] [PubMed]
- Sivaramakrishnan, G.; Alsobaiei, M.; Sridharan, K. Interventions for anesthetic success in symptomatic irreversible pulpitis: A network meta-analysis of randomized controlled trials. J. Dent. Anesth. Pain Med. 2019, 19, 323–341. [Google Scholar] [CrossRef] [PubMed]
- Drum, M.; Reader, A.; Nusstein, J.; Fowler, S. Successful pulpal anesthesia for symptomatic irreversible pulpitis. J. Am. Dent. Assoc. 2017, 148, 267–271. [Google Scholar] [CrossRef] [PubMed]
- Henry, M.A.; Luo, S.; Foley, B.D.; Rzasa, R.S.; Johnson, L.R.; Levinson, S.R. Sodium channel expression and localization at demyelinated sites in painful human dental pulp. J. Pain 2009, 10, 750–758. [Google Scholar] [CrossRef] [Green Version]
- Modaresi, J.; Dianat, O.; Soluti, A. Effect of pulp inflammation on nerve impulse quality with or without anesthesia. J. Endod. 2008, 34, 438–441. [Google Scholar] [CrossRef]
- Nogueira, B.M.L.; Silva, L.G.; Mesquita, C.R.M.; Menezes, S.A.F.; Menezes, T.O.A.; Faria, A.G.M.; Porpino, M.T.M. Is the use of dexamethasone effective in controlling pain associated with symptomatic irreversible pulpitis? A systematic review. J. Endod. 2018, 44, 703–710. [Google Scholar] [CrossRef]
- Aggarwal, V.; Singla, M.; Rizvi, A.; Miglani, S. Comparative evaluation of local infiltration of articaine, articaine plus ketorolac, and dexamethasone on anesthetic efficacy of inferior alveolar nerve block with lidocaine in patients with irreversible pulpitis. J. Endod. 2011, 37, 445–449. [Google Scholar] [CrossRef]
- Aggarwal, V.; Singla, M.; Saatchi, M.; Gupta, A.; Hasija, M.; Meena, B.; Kumar, U. Preoperative intraligamentary injection of dexamethasone can improve the anesthetic success rate of 2% lidocaine during the endodontic management of mandibular molars with symptomatic irreversible pulpitis. J. Endod. 2021, 47, 161–168. [Google Scholar] [CrossRef]
- Aksoy, F.; Ege, B. The effect of pretreatment submucosal injections of tramadol and dexamethasone on post-endodontic pain in mandibular molar teeth with symptomatic irreversible pulpitis: A randomized controlled clinical trial. Int. Endod. J. 2020, 53, 176–185. [Google Scholar] [CrossRef]
- Aksoy, F.; Ege, B.; Tosun, S. The effect of pre-operative submucosal administration of dexamethasone, tramadol, articaine on the success rate of inferior alveolar nerve block on mandibular molars with symptomatic irreversible pulpitis: A randomized, double-blind placebo-controlled clinical trial. Int. Endod. J. 2021, 54, 1982–1992. [Google Scholar] [PubMed]
- Ali, F.; Yousaf, A.; Daud, Z.; Hussain, S.M.; Ullah, M.; Ahmed Rana, M.J. Comparison of two intra-canal medicaments on the incidence of post-operative endodontic pain. J. Ayub Med. Coll. Abbottabad 2020, 32, 299–303. [Google Scholar] [PubMed]
- Bagheri, M.; Khimani, H.; Pishbin, L.; Shahabinejad, H. Effect of pulpotomy procedures with mineral trioxide aggregate and dexamethasone on post-endodontic pain in patients with irreversible pulpitis: A randomized clinical Trial. Eur. Endod. J. 2019, 4, 69–74. [Google Scholar] [PubMed]
- Bidar, M.; Mortazavi, S.; Forghani, M.; Akhlaghi, S. Comparison of effect of oral premedication with ibuprofen or dexamethasone on anesthetic efficacy of inferior alveolar nerve block in patients with irreversible pulpitis: A prospective, randomized, controlled, double-blind study. Bull. Tokyo Dent. Coll. 2017, 58, 231–236. [Google Scholar] [CrossRef] [Green Version]
- El-Glil, S.E.A.; Zakhary, S.Y.; Negm, M.M.; Abu-Naaem, F.M. Comparative evaluation of the effect of intraligamentary injection of dexamethasone and piroxicam on postoperative pain in teeth with symptomatic irreversible pulpitis: A randomized controlled trial. Egypt. Dent. J. 2021, 67, 1619–1627. [Google Scholar] [CrossRef]
- Kaushik, M.; Mehra, N.; Sharma, R.; Moturi, K.; Podugu, U.K.; George, A. Comparing the efficacy of twin mix and lidocaine for inferior alveolar nerve blocks in patients with symptomatic irreversible pulpitis. Anesth. Prog. 2020, 67, 207–213. [Google Scholar] [CrossRef]
- Kumar, M.; Singla, R.; Gill, G.S.; Kalra, T.; Jain, N. Evaluating combined effect of oral premedication with ibuprofen and dexamethasone on success of inferior alveolar nerve block in mandibular molars with symptomatic irreversible pulpitis: A prospective, double-blind, randomized clinical trial. J. Endod. 2021, 47, 705–710. [Google Scholar] [CrossRef]
- Mehrvarzfar, P.; Esnashari, E.; Salmanzadeh, R.; Fazlyab, M.; Fazlyab, M. Effect of dexamethasone intraligamentary injection on post-endodontic pain in patients with symptomatic irreversible pulpitis: A randomized controlled clinical trial. Iran. Endod. J. 2016, 11, 261–266. [Google Scholar]
- Mehrvarzfar, P.; Shababi, B.; Sayyad, R.; Fallahdoost, A.; Kheradpir, K. Effect of supraperiosteal injection of dexamethasone on postoperative pain. Aust. Endod. J. 2008, 34, 25–29. [Google Scholar] [CrossRef]
- Shahi, S.; Mokhtari, H.; Rahimi, S.; Yavari, H.R.; Narimani, S.; Abdolrahimi, M.; Nezafati, S. Effect of premedication with ibuprofen and dexamethasone on success rate of inferior alveolar nerve block for teeth with asymptomatic irreversible pulpitis: A randomized clinical trial. J. Endod. 2013, 39, 160–162. [Google Scholar] [CrossRef]
- Shokri, M.; Node, S.R.; Mortazavi, S. The Effect of pretreatment with ibuprofen and dexamethasone on the effect of nerve block lower alveolar marked in irreversible pulpitis teeth. Neurosci. J. Shefaye Khatam 2018, 6, 71. [Google Scholar]
- Suresh, N.; Nagendrababu, V.; Koteeswaran, V.; Haritha, J.S.; Swetha, S.D.; Varghese, A.; Natanasabapathy, V. Effect of preoperative oral administration of steroids in comparison to an anti-inflammatory drug on postoperative pain following single-visit root canal treatment-a double-blind, randomized clinical trial. Int. Endod. J. 2021, 54, 198–209. [Google Scholar] [CrossRef] [PubMed]
- Yavari, H.R.; Jafari, F.; Jamloo, H.; Hallaj-Nezhadi, S.; Jafari, S. The effect of submucosal injection of corticosteroids on pain perception and quality of life after root canal treatment of teeth with irreversible pulpitis: A randomized clinical trial. J. Endod. 2019, 45, 477–482. [Google Scholar] [CrossRef] [PubMed]
- Yousaf, A.; Ali, F.; Hussain, S.M.; Bhangar, F.; Yousaf, N.; Bangash, K.A. Effect of supraperiosteal injection of dexamethasone on interappointment pain in teeth with symptomatic irreversible pulpitis: A comparative study. Life Sci. 2020, 1, 145–148. [Google Scholar] [CrossRef]
- Nagendrababu, V.; Dilokthornsakul, P.; Jinatongthai, P.; Veettil, S.K.; Pulikkotil, S.J.; Duncan, H.F.; Dummer, P.M.H. Glossary for systematic reviews and meta-analyses. Int. Endod. J. 2020, 53, 232–249. [Google Scholar] [CrossRef] [Green Version]
- Nagendrababu, V.; Duncan, H.F.; Tsesis, I.; Sathorn, C.; Pulikkotil, S.J.; Dharmarajan, L.; Dummer, P.M.H. PRISMA for abstracts: Best practice for reporting abstracts of systematic reviews in Endodontology. Int. Endod. J. 2019, 19, 1096–1107. [Google Scholar]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Leonardo, R. PICO: Model for clinical questions. Evid. Based Med. Pract. 2018, 3, 2. [Google Scholar]
- Higgins, J.P.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: Oxford, UK, 2011. [Google Scholar]
- Jones, A.; Steel, D. Evaluating the quality of medical evidence in real-world contexts. J. Eval. Clin. Pract. 2018, 24, 950–956. [Google Scholar] [CrossRef]
- Atkins, D.; Eccles, M.; Flottorp, S.; Guyatt, G.H.; Henry, D.; Hill, S.; Liberati, A.; O’Connell, D.; Oxman, A.D.; Phillips, B.; et al. Systems for grading the quality of evidence and the strength of recommendations I: Critical appraisal of existing approaches The GRADE Working Group. BMC Health Serv. Res. 2004, 4, 38. [Google Scholar] [CrossRef]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Figueroa-Fernández, N.P.; Hernández-Miramontes, Y.A.; Alonso-Castro, Á.J.; Isiordia-Espinoza, M.A. A meta-analysis on the efficacy of the ropivacaine infiltration in comparison with other dental anesthetics. Clin. Oral Investig. 2021, 25, 6779–6790. [Google Scholar] [CrossRef]
- Isiordia-Espinoza, M.A.; Franco-González, M.A.; Alonso-Castro, Á.J.; Franco-de la Torre, L. Analgesic effectiveness and safety of celecoxib versus non-opioid active controls after third molar surgery: A meta-analytical evaluation. J. Stomatol. Oral Maxillofac. Surg. 2021, 123, e1–e9. [Google Scholar] [CrossRef]
- Franco-de la Torre, L.; Figueroa-Fernández, N.P.; Franco-González, D.L.; Alonso-Castro, Á.J.; Rivera-Luna, F.; Isiordia-Espinoza, M.A. A Meta-analysis of the analgesic efficacy of single-doses of ibuprofen compared to traditional non-opioid analgesics following third molar surgery. Pharmaceuticals 2021, 14, 360. [Google Scholar] [CrossRef]
- Pehora, C.; Pearson, A.M.; Kaushal, A.; Crawford, M.W.; Johnston, B. Dexamethasone as an adjuvant to peripheral nerve block. Cochrane Database Syst. Rev. 2017, 11, CD011770. [Google Scholar] [CrossRef] [PubMed]
- Isiordia-Espinoza, M.A.; Pozos-Guillén, A.J.; Martínez-Rider, R.; Herrera-Abarca, J.E.; Pérez-Urizar, J. Preemptive analgesic effectiveness of oral ketorolac plus local tramadol after impacted mandibular third molar surgery. Med. Oral Patol. Oral Cir. Bucal. 2011, 16, e776–e780. [Google Scholar] [CrossRef] [Green Version]
- Isiordia-Espinoza, M.A.; Orozco-Solis, M.; Tobías-Azúa, F.J.; Méndez-Gutiérrez, E.P. Submucous tramadol increases the anesthetic efficacy of mepivacaine with epinephrine in inferior alveolar nerve block. Br. J. Oral Maxillofac. Surg. 2012, 50, 157–160. [Google Scholar] [CrossRef]
- Rodríguez-Wong, L.; Pozos-Guillen, A.; Silva-Herzog, D.; Chavarría-Bolaños, D. Efficacy of mepivacaine-tramadol combination on the success of inferior alveolar nerve blocks in patients with symptomatic irreversible pulpitis: A randomized clinical trial. Int. Endod. J. 2016, 49, 325–333. [Google Scholar] [CrossRef]
- Zhang, L.; Russell, D.; Conway, B.R.; Batchelor, H. Strategies and therapeutic opportunities for the delivery of drugs to the esophagus. Crit. Rev. Ther. Drug Carr. Syst. 2008, 25, 259–304. [Google Scholar] [CrossRef]
- Das Neves, J.; Notario-Pérez, F.; Sarmento, B. Women-specific routes of administration for drugs: A critical overview. Adv. Drug Deliv. Rev. 2021, 176, 113865. [Google Scholar] [CrossRef]
- Trombino, S.; Curcio, F.; Poerio, T.; Pellegrino, M.; Russo, R.; Cassano, R. Chitosan Membranes Filled with Cyclosporine A as Possible Devices for Local Administration of Drugs in the Treatment of Breast Cancer. Molecules 2021, 26, 1889. [Google Scholar] [CrossRef]
- Miyazawa, K.; Asano, Y.; Tabuchi, M.; Kako, S.; Kawatani, M.; Osada, H.; Maeda, H.; Goto, S. Local administration of ReveromycinA ointment suppressed alveolar bone loss in mice. J. Pharmacol. Sci. 2021, 147, 40–47. [Google Scholar] [CrossRef]
- Pitorre, M.; Gazaille, C.; Pham, L.T.T.; Frankova, K.; Béjaud, J.; Lautram, N.; Riou, J.; Perrot, R.; Geneviève, F.; Moal, V.; et al. Polymer-free hydrogel made of lipid nanocapsules, as a local drug delivery platform. Mater. Sci. Eng. C Mater. Biol. Appl. 2021, 126, 112188. [Google Scholar] [CrossRef]
- Waldron, N.H.; Jones, C.A.; Gan, T.J.; Allen, T.K.; Habib, A.S. Impact of perioperative dexamethasone on postoperative analgesia and side-effects: Systematic review and meta-analysis. Br. J. Anaesth. 2013, 110, 191–200. [Google Scholar] [CrossRef] [Green Version]
- Knezevic, N.N.; Anantamongkol, U.; Candido, K.D. Perineural dexamethasone added to local anesthesia for brachial plexus block improves pain but delays block onset and motor blockade recovery. Pain Physician 2015, 18, 1–14. [Google Scholar]
- Polderman, J.A.; Farhang-Razi, V.; Van Dieren, S.; Kranke, P.; DeVries, J.H.; Hollmann, M.W.; Preckel, B.; Hermanides, J. Adverse side effects of dexamethasone in surgical patients. Cochrane Database Syst. Rev. 2018, 8, CD011940. [Google Scholar]
- Chen, F.; Hao, L.; Zhu, S.; Yang, X.; Shi, W.; Zheng, K.; Wang, T.; Chen, H. Potential adverse effects of dexamethasone therapy on covid-19 patients: Review and recommendations. Infect. Dis. Ther. 2021, 10, 1907–1931. [Google Scholar] [CrossRef]
- La Torre, L.F.; Franco-González, D.L.; Brennan-Bourdon, L.M.; Molina-Frechero, N.; Alonso-Castro, Á.J.; Isiordia-Espinoza, M.A. Analgesic efficacy of etoricoxib following third molar surgery: A meta-analysis. Behav. Neurol. 2021, 2021, 9536054. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ID Study and Study Design | Treatments (n) | Details of Patients, Dental Procedure, and Evaluation | Important Results/Conclusions |
|---|---|---|---|
| Aggarwal et al., 2011 [8]. Randomized, double-blind, parallel, clinical investigation. | Group A: dexamethasone 4 mg/1 mL (n = 23) Group B: 4% articaine and 1:100,000 epinephrine/1.8 mL (n = 24). Group C: 4% articaine plus ketorolac 30 mg / 1 mL (n = 24). Group D: patients received no treatment (n = 23). All treatments were carried out as pre-anesthetic supplemental buccal injection. | ASA I or II patients with pain in a lower molar (moderate-to-severe pain) and diagnosis of SIP with a normal periapical radiograph. Patients without NSAIDs, at least 12 h before the study. All patients were given an IANB using lidocaine 2% and 1:200,000 epinephrine. Success rates were evaluated. | Administration of dexamethasone increased the success rate of local anesthesia. |
| Aggarwal et al., 2021 [9]. Randomized, double-blind, parallel, clinical assay. | Group A: 1.8 mL of dexamethasone 4 mg/1 mL (n = 37). Group B: 1.8 mL of diclofenac from a vial with 75 mg/3 mL (n = 38). Group C: normal saline 0.9%/1.8 mL (n = 37). All treatments were performed as pre-anesthetic intraligamentary administration. | ASA I or II patients with pain in a lower molar (moderate-to-severe pain) and diagnosis of SIP with a normal periapical radiograph. Patients with prolonged positive response to cold tests. For all patients, IANB was performed using lidocaine 2%, and 1:200,000 epinephrine was employed. The anesthetic success index and the heart rates were assessed. | Intraligamentary dexamethasone administration increased the success rate of anesthesia. |
| Aksoy and Ege, 2020 [10]. Randomized, double-blind, parallel, clinical trial. | Group A: dexamethasone 8 mg/2 mL (n = 30).
Group B: tramadol 100 mg/2 mL (n = 30). Group C: normal saline 0.9%/2 mL (n = 30). All treatments were given (2 mL volume) across the mucobuccal fold of the mandibular molar after anesthesia. | Healthy patients aged 18 to 65 years with a diagnosis of SIP (moderate-to-severe pain) in a mandibular molar, radiographically normal periapical area, and no pain on percussion were included.
Patients without analgesic medication, at least 12 h before the study. Patients with prolonged positive response to cold tests. All patients were administered an IANB using 4% articaine with 1:200,000 epinephrine. Postoperative pain intensity, rescue analgesic medication, and adverse effects were evaluated. | Dexamethasone was more effective for pain control when compared with saline. |
| Aksoy et al., 2021 [11]. Randomized, double-blind, parallel, clinical assay. | Group A: dexamethasone 8 mg/2 mL (n = 30).
Group B: tramadol 100 mg/2 mL (n = 30). Group C: articaine 4%/1.8 mL (n = 30). Group D: normal saline 0.9%/2 mL (n = 30). All treatments were given (2 mL volume) across the mucobuccal fold of the mandibular molar after anesthesia. | Healthy patients aged 18 to 65 years with a diagnosis of SIP (moderate-to-severe pain) in a mandibular molar, radiographically normal periapical area, and no pain on percussion were included.
Patients without analgesic medication, at least 24 h before the study. Patients with prolonged positive response to cold tests. All patients were given an IANB using 4% articaine with 1:200,000 epinephrine. Anesthesia was successful when the pain level of patients included no pain or mild pain. Sensory blockade, duration of anesthesia, success index, and adverse effects were assessed. | Dexamethasone increased the duration of anesthetic activity when compared with saline. |
| Bidar et al., 2017 [14]. Randomized, double-blind, parallel, clinical investigation. | Group A: dexamethasone 4 mg (n = 26). Group B: ibuprofen 400 mg (n = 26) Group C: placebo (n = 26). All treatments were administered via the oral route. | Patients in good health, over 18 years old, with a lower first or second molar with a diagnosis of SIP (moderate-to-severe pain) were included.
Patients with prolonged positive response to cold tests. Patients without analgesic medication, at least 8 h before the study. Standard IANB using 2% lidocaine and 1:80,000 epinephrine was used. Anesthesia was successful when the pain level of patients was no pain or mild pain. The anesthetic success and side effects were evaluated. | Dexamethasone increased the anesthetic success versus placebo. |
| El-Glil et al., 2021 [15]. Randomized, double-blind, parallel, clinical assay. | Group A: 0.4 mL dexamethasone 8 mg/2 mL (n = 14). Group B: 0.4 mL piroxicam 20 mg/mL (n = 14). Group C: 0.4 mL mepivacaine 2% and 1:20,000 levonordefrin (n = 14). An intraligamentary injection was used for the administration of the drugs. | ASA I or II patients (20 to 60 years old) with pain in a lower molar (moderate-to-severe pain) and diagnosis of SIP with a normal periapical radiograph. Patients without analgesic medication or corticosteroids, at least 24 h before the study. IANB with mepivacaine 2% and 1:20,000 levonordefrin was employed. Post-endodontic pain was evaluated. | Dexamethasone was more effective than mepivacaine/levonordefrin for pain control at 4, 6, 12, 24, and 48 postoperative hours. |
| Kaushik et al., 2020 [16]. Randomized, double-blind, parallel, clinical trial. | Group A: dexamethasone 4 mg/1 mL (n = 34). Group B: distilled water/1 mL (n = 35). Treatments were given via the submucosal route. | Patients diagnosed with SIP (moderate-to-severe pain) involving the mandibular molars, without associated pathology. Patients with prolonged positive response to cold tests. IANB 2% lidocaine with 1:200,000 epinephrine was used. Anesthesia success was evaluated. | A similar anesthetic success rate between dexamethasone and distilled water was observed. |
| Kumar et al., 2021 [17]. Randomized, double-blind, parallel, clinical investigation. | Group A: dexamethasone 0.5 mg (n = 21). Group B: ibuprofen 800 mg (n = 21). Group C: dexamethasone–ibuprofen combination (n = 23). Group D: placebo (n = 20). Oral premedication. | ASA I or II patients with pain in a lower molar (moderate-to-severe pain) and diagnosis of SIP with a normal periapical radiograph.
Patients having taken no analgesics for at least 12 h before the study. Patients with prolonged positive response to cold tests. For all subjects, IANB was performed using lidocaine 2% and 1:200,000 epinephrine. Overall anesthesia success rate was assessed. | A similar anesthesia rate for dexamethasone and placebo was reported. |
| Mehrvarzfar et al., 2008 [19]. Randomized, double-blind, parallel, clinical study. | Group A: dexamethasone 8 mg/2 mL (n = 50). Group B: placebo (lidocaine 2%/1.8 mL) (n = 50). All treatments were given via a supraperiosteal injection (periapical region) after anesthesia. | ASA I or II patients aged 21 to 58 years with a diagnosis of SIP (moderate-to-severe pain) in an incisor or premolar. Patients with positive thermal and electrical tests. The local anesthetic used in all patients was not indicated. Post-endodontic pain was evaluated using VAS. | Dexamethasone was more effective for post-endodontic pain control during the first 24 h than placebo. |
| Mehrvarzfar et al., 2016 [18]. Randomized, double-blind, parallel, clinical trial. | Group A: 0.2 mL dexamethasone 8 mg/2 mL (n = 20). Group B: 0.2 mL lidocaine 2% and 1:80,000 epinephrine mL (n = 20). Group C: 0.2 mL saline (n = 20). All treatments were administered using a periodontal intraligamentary injection after anesthesia. | ASA I or II patients aged 18 to 65 years with clinical manifestation of SIP (moderate-to-severe pain), without radiographic periapical lesions. Patients with prolonged positive response to cold tests. Intake of opioid analgesics, NSAIDs, corticosteroids, and three-cyclic antidepressants 12 h before treatment. Administration of 1.8 mL of 2% lidocaine with 1:80,000 epinephrine was used to obtain the block the maxillary molars or achieve IANB for the mandibular molars. Post-endodontic pain intensity, the rescue analgesic intake, and adverse effects were recorded. | Dexamethasone reduced the postoperative pain when compared with placebo. |
| Shahi et al., 2013 [20]. Randomized, double-blind, parallel, clinical assay. | Group A: dexamethasone 0.5 mg (n = 55). Group B: ibuprofen 400 mg (n = 55). Group C: placebo (n = 55). All patients received the experimental the treatments orally. | Good health in patients (aged ≥ 18) with SIP on mandibular first or second molar and a normal periapical radiograph. Patients not taking any analgesics for at least 12 h before the study. Patients with prolonged positive response to cold tests. IANB with 2% lidocaine and 1:80,000 epinephrine was used. The anesthesia success and side effects were assessed. | Dexamethasone increased the anesthetic success in comparison with placebo. |
| Shokri et al., 2018 [21]. Randomized, double-blind, parallel, clinical investigation. | Group A: dexamethasone 4 mg (n = 25). Group B: ibuprofen 400 mg (n = 25). Group C: placebo (n = 25). All treatments were administered using the oral route. | Emergency patients diagnosed with SIP of a mandibular posterior tooth. IANB was performed. However, the anesthetic agent used was not disclosed. The anesthesia success was analyzed. | Dexamethasone increased the anesthetic success when compared with placebo. |
| Suresh et al., 2020 [22]. Randomized, double-blind, parallel, clinical study. | Group A: dexamethasone 4 mg (n = 40). Group B: piroxicam 20 mg (n = 40). Group C: prednisolone 20 mg (n = 40). Group D: placebo (n = 40). All patients took oral treatments. | Systemic healthy patients aged 18 to 60 years with diagnosed with SIP at a maxillary or mandibular tooth and a normal periapical radiograph. Patients with prolonged positive response to cold tests. Patients having taken no analgesics, steroids, or antibiotics for at least 24 h before the study. Lidocaine 2% and epinephrine 1:100,000 were used to perform the IANB. Post-endodontic pain was assessed at 6, 12, 24, 48, and 72 h. | Dexamethasone reduced the postoperative pain when compared with placebo. |
| Yavari et al., 2019 [23]. Randomized, double-blind, parallel, clinical trial. | Group A: 0.7 mL dexamethasone 4 mg/mL (n = 64) Group B: 0.7 mL long-acting dexamethasone 4 mg/mL (n = 66). Group C: 0.7 mL saline 0.9% (n = 64). All treatments were administered via the submucosal route after anesthesia. | Healthy individuals aged 20 to 50 years and presenting a diagnosis of symptomatic and asymptomatic irreversible pulpitis with a normal periapical condition. Ibuprofen 1.6 g was used during the two previous days. Patients with prolonged positive response to cold tests. For all subjects, the IANB was performed using lidocaine and 1:100,000 epinephrine. Post-treatment pain was evaluated with the VAS. | Both dexamethasone groups had better postoperative pain relief than saline. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Franco-de la Torre, L.; Gómez-Sánchez, E.; Serafín-Higuera, N.A.; Alonso-Castro, Á.J.; López-Verdín, S.; Molina-Frechero, N.; Granados-Soto, V.; Isiordia-Espinoza, M.A. Dexamethasone Increases the Anesthetic Success in Patients with Symptomatic Irreversible Pulpitis: A Meta-Analysis. Pharmaceuticals 2022, 15, 878. https://doi.org/10.3390/ph15070878
Franco-de la Torre L, Gómez-Sánchez E, Serafín-Higuera NA, Alonso-Castro ÁJ, López-Verdín S, Molina-Frechero N, Granados-Soto V, Isiordia-Espinoza MA. Dexamethasone Increases the Anesthetic Success in Patients with Symptomatic Irreversible Pulpitis: A Meta-Analysis. Pharmaceuticals. 2022; 15(7):878. https://doi.org/10.3390/ph15070878
Chicago/Turabian StyleFranco-de la Torre, Lorenzo, Eduardo Gómez-Sánchez, Nicolás Addiel Serafín-Higuera, Ángel Josabad Alonso-Castro, Sandra López-Verdín, Nelly Molina-Frechero, Vinicio Granados-Soto, and Mario Alberto Isiordia-Espinoza. 2022. "Dexamethasone Increases the Anesthetic Success in Patients with Symptomatic Irreversible Pulpitis: A Meta-Analysis" Pharmaceuticals 15, no. 7: 878. https://doi.org/10.3390/ph15070878