
Enhanced Thrombin Generation Is Associated with Worse Left Ventricular Scarring after ST-Segment Elevation Myocardial Infarction: A Cohort Study

 , ,
, ,
Abstract
:1. Introduction
2. Results
2.1. Baseline Demographics
2.2. Discharge Medications
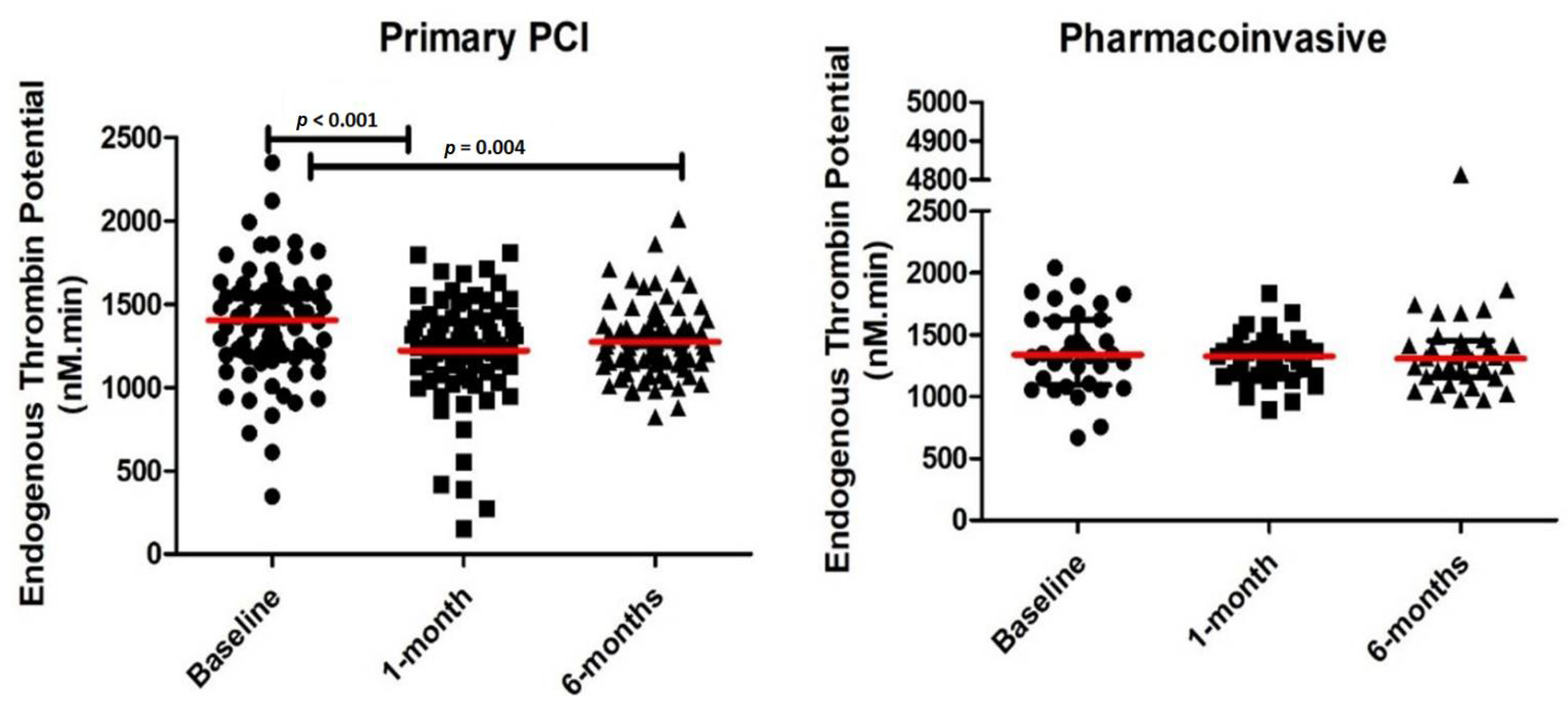
2.3. Thrombin Parameters
2.4. CMR Results
2.5. Relation between ETP and Imaging Endpoints
3. Materials & Methods
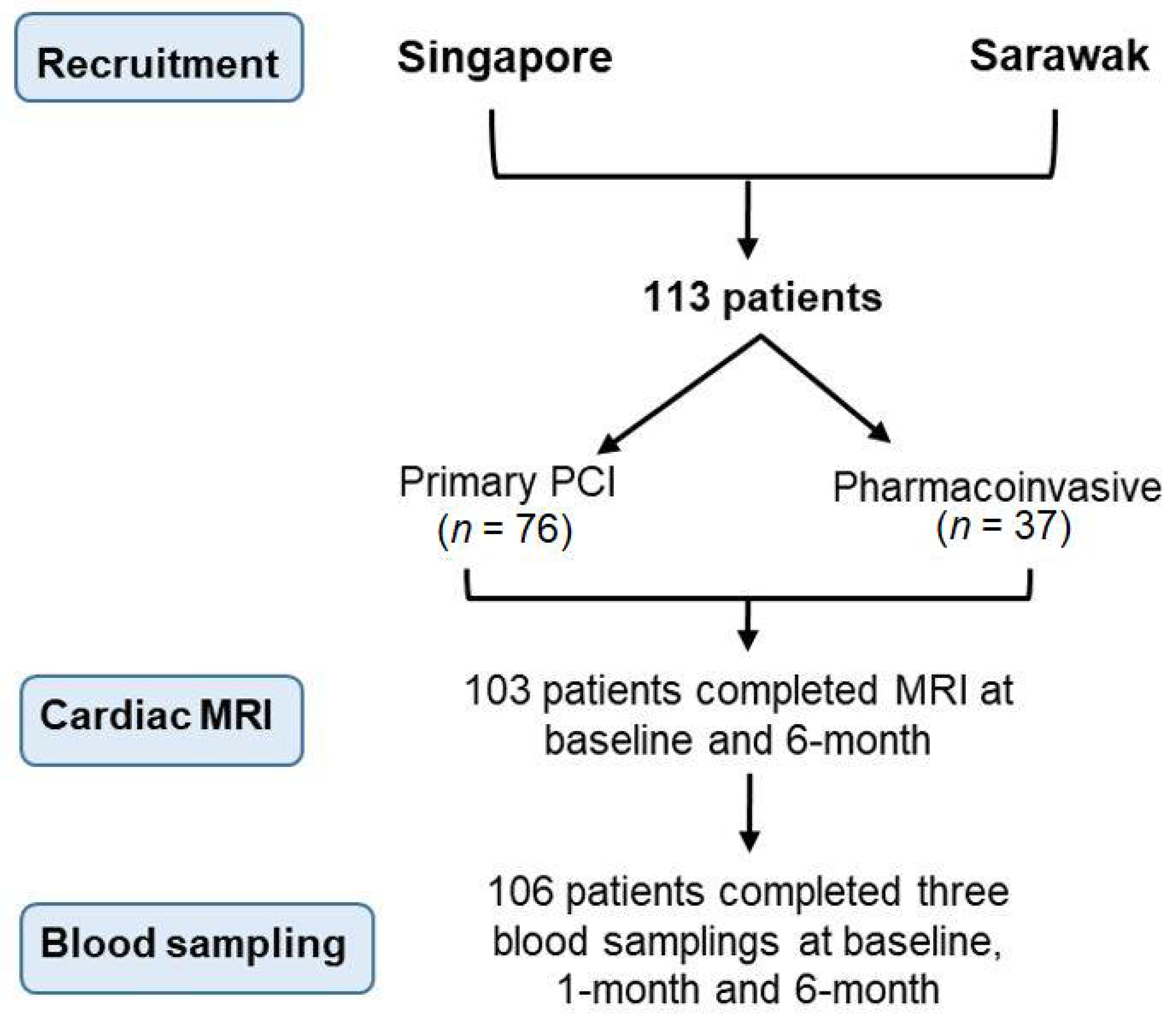
3.1. Study Design and Population
3.2. Study Procedures and Follow-Up
3.3. Laboratory Testing
3.4. Thrombin Generation Measurements
3.5. Cardiac Magnetic Resonance Imaging
3.6. Statistical Analysis
3.7. Ethics Approval
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.M.; Bhutta, Z.A.; Carter, A.; Casey, D.C.; Charlson, F.J.; Chen, A.Z.; Coates, M.M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. [Google Scholar] [CrossRef] [Green Version]
- Frangogiannis, N.G. The inflammatory response in myocardial injury, repair, and remodelling. Nat. Rev. Cardiol. 2014, 11, 255–265. [Google Scholar] [CrossRef] [Green Version]
- Di Bella, G.; Siciliano, V.; Aquaro, G.D.; Molinaro, S.; Lombardi, M.; Carerj, S.; Landi, P.; Rovai, D.; Pingitore, A. Scar extent, left ventricular end-diastolic volume, and wall motion abnormalities identify high-risk patients with previous myocardial infarction: A multiparametric approach for prognostic stratification. Eur. Heart J. 2012, 34, 104–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Palomares, J.F.; Gavara, J.; Ferreira-González, I.; Valente, F.; Rios, C.; Rodríguez-García, J.; Bonanad, C.; García del Blanco, B.; Miñana, G.; Mutuberria, M.; et al. Prognostic Value of Initial Left Ventricular Remodeling in Patients With Reperfused STEMI. JACC Cardiovasc. Imaging 2019, 12, 2445–2456. [Google Scholar] [CrossRef]
- Bahit, M.C.; Kochar, A.; Granger, C.B. Post-Myocardial Infarction Heart Failure. JACC Heart Fail. 2018, 6, 179–186. [Google Scholar] [CrossRef]
- Gu, X.; Zhang, X.; Lu, G.; Li, Y.; Li, X.; Huang, H.; Zeng, J.; Tang, L. Effects of thrombin and thrombin receptor activation on cardiac function after acute myocardial infarction. Am. J. Transl. Res. 2015, 7, 654–669. [Google Scholar]
- Antoniak, S.; Cardenas, J.C.; Buczek, L.J.; Church, F.C.; Mackman, N.; Pawlinski, R. Protease-Activated Receptor 1 Contributes to Angiotensin II-Induced Cardiovascular Remodeling and Inflammation. Cardiology 2017, 136, 258–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Antoniak, S.; Pawlinski, R.; Mackman, N. Protease-activated receptors and myocardial infarction. IUBMB Life 2011, 63, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Ishiguro, Y.S.; Iida, M.; Yamamoto, M.; Honjo, H.; Kamiya, K. Abstract 12007: Association of Thrombin Generation with Left Ventricular Diastolic Dysfunction in Hypertensive Patients with Heart Failure with Preserved Ejection Fraction. Circulation 2012, 126, A12007. [Google Scholar] [CrossRef]
- Gulba, D.C.; Barthels, M.; Westhoff-Bleck, M.; Jost, S.; Rafflenbeul, W.; Daniel, W.G.; Hecker, H.; Lichtlen, P.R. Increased thrombin levels during thrombolytic therapy in acute myocardial infarction. Relevance for the success of therapy. Circulation 1991, 83, 937–944. [Google Scholar] [CrossRef] [Green Version]
- Zeymer, U.; Rao, S.V.; Montalescot, G. Anticoagulation in coronary intervention. Eur. Heart J. 2016, 37, 3376–3385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smid, M.; Dielis, A.W.; Spronk, H.M.; Rumley, A.; van Oerle, R.; Woodward, M.; ten Cate, H.; Lowe, G. Thrombin generation in the Glasgow Myocardial Infarction Study. PLoS ONE 2013, 8, e66977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beijers, H.J.B.H.; Ferreira, I.; Spronk, H.M.H.; Bravenboer, B.; Dekker, J.M.; Nijpels, G.; Cate, H.T.; Stehouwer, C.D.A. Body Composition as Determinant of Thrombin Generation in Plasma. Arterioscler. Thromb. Vasc. Biol. 2010, 30, 2639–2647. [Google Scholar] [CrossRef] [Green Version]
- Yip, C.; Seneviratna, A.; Tan, S.-H.; Khaing, T.; Chan, S.-P.; Loh, J.; Lee, C.-H.; Low, A.F.; Drum, C.L.; Poh, S.-C.; et al. Patients with acute and chronic coronary syndromes have elevated long-term thrombin generation. J. Thromb. Thrombolysis 2020, 50, 421–429. [Google Scholar] [CrossRef]
- Sutton, M.G.S.J.; Sharpe, N. Left Ventricular Remodeling After Myocardial Infarction. Circulation 2000, 101, 2981–2988. [Google Scholar] [CrossRef] [PubMed]
- Bauters, C.; Dubois, E.; Porouchani, S.; Saloux, E.; Fertin, M.; de Groote, P.; Lamblin, N.; Pinet, F. Long-term prognostic impact of left ventricular remodeling after a first myocardial infarction in modern clinical practice. PLoS ONE 2017, 12, e0188884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerisano, G.; Buonamici, P.; Valenti, R.; Sciagrà, R.; Raspanti, S.; Santini, A.; Carrabba, N.; Dovellini, E.V.; Romito, R.; Pupi, A.; et al. Early short-term doxycycline therapy in patients with acute myocardial infarction and left ventricular dysfunction to prevent the ominous progression to adverse remodelling: The TIPTOP trial. Eur. Heart J. 2013, 35, 184–191. [Google Scholar] [CrossRef] [Green Version]
- Muhlestein, J.B. Adverse left ventricular remodelling after acute myocardial infarction: Is there a simple treatment that really works? Eur. Heart J. 2014, 35, 144–146. [Google Scholar] [CrossRef] [Green Version]
- Grabau, R.; Chen, J.; Weinheimer, C.; Kovacs, A.; Pan, H.; Wickline, S.A. Anti-thrombotic and Anti-inflammatory Nanoparticle Limits Early Remodeling in Acute Myocardial Infarction. FASEB J. 2019, 33, 680–687. [Google Scholar] [CrossRef]
- Zannad, F.; Anker, S.D.; Byra, W.M.; Cleland, J.G.F.; Fu, M.; Gheorghiade, M.; Lam, C.S.P.; Mehra, M.R.; Neaton, J.D.; Nessel, C.C.; et al. Rivaroxaban in Patients with Heart Failure, Sinus Rhythm, and Coronary Disease. N. Engl. J. Med. 2018, 379, 1332–1342. [Google Scholar] [CrossRef] [PubMed]
- Mega, J.L.; Braunwald, E.; Wiviott, S.D.; Bassand, J.-P.; Bhatt, D.L.; Bode, C.; Burton, P.; Cohen, M.; Cook-Bruns, N.; Fox, K.A.A.; et al. Rivaroxaban in Patients with a Recent Acute Coronary Syndrome. N. Engl. J. Med. 2011, 366, 9–19. [Google Scholar] [CrossRef] [Green Version]
- Desch, S.; Eitel, I.; de Waha, S.; Fuernau, G.; Lurz, P.; Gutberlet, M.; Schuler, G.; Thiele, H. Cardiac magnetic resonance imaging parameters as surrogate endpoints in clinical trials of acute myocardial infarction. Trials 2011, 12, 204. [Google Scholar] [CrossRef] [Green Version]
- Goldman, S.; Prior, S.M.; Bembenek, J.P.; Niewada, M.; Broniatowska, E.; Członkowska, A.; Butenas, S.; Undas, A. Activation of blood coagulation and thrombin generation in acute ischemic stroke treated with rtPA. J. Thromb. Thrombolysis 2017, 44, 362–370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Simoons, M.L.; Chaitman, B.R.; White, H.D. Third Universal Definition of Myocardial Infarction. Circulation 2012, 126, 2020–2035. [Google Scholar] [CrossRef] [Green Version]
- Iida, M.; Yamamoto, M.; Yamazaki, M.; Sawaguchi, M.; Honjo, H.; Kodama, I.; Kamiya, K. Association of aortic valve sclerosis with thrombin generation in hypertensive patients. J. Hum. Hypertens. 2008, 22, 781–787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruf, W.; Mueller, B.M. Thrombin Generation and the Pathogenesis of Cancer. Semin. Thromb. Hemost. 2006, 32, 061–068. [Google Scholar] [CrossRef] [PubMed]
- Senzolo, M.; Sartori, M.T.; Rodriguez-Castro, K.; Simioni, P.; Rossetto, V. Increased thrombin generation in liver transplant recipients: Does immunosuppressive therapy play a role? Liver Transplant. Off. Publ. Am. Assoc. Study Liver Dis. Int. Liver Transplant. Soc. 2011, 17, 347–348. [Google Scholar] [CrossRef]
- Tripodi, A. Thrombin Generation Assay and Its Application in the Clinical Laboratory. Clin. Chem. 2016, 62, 699–707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fadil, H.; Totman, J.J.; Hausenloy, D.J.; Ho, H.-H.; Joseph, P.; Low, A.F.-H.; Richards, A.M.; Chan, M.Y.; Marchesseau, S. A deep learning pipeline for automatic analysis of multi-scan cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2021, 23, 47. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation; Springer: Cham, Switzerland, 2015; pp. 234–241. [Google Scholar]
- Granger, C.B.; Becker, R.; Tracy, R.P.; Califf, R.M.; Topol, E.J.; Pieper, K.S.; Ross, A.M.; Roth, S.; Lambrew, C.; Bovill, E.G. Thrombin generation, inhibition and clinical outcomes in patients with acute myocardial infarction treated with thrombolytic therapy and heparin: Results from the GUSTO-I Trial. GUSTO-I Hemostasis Substudy Group. Global Utilization of Streptokinase and TPA for Occluded Coronary Arteries. J. Am. Coll. Cardiol. 1998, 31, 497–505. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Galli, A.; Lombardi, F. Postinfarct Left Ventricular Remodelling: A Prevailing Cause of Heart Failure. Cardiol. Res. Pract. 2016, 2016, 2579832. [Google Scholar] [CrossRef] [Green Version]
- Durighel, G.; Dawes, T.; Ashwin, C.; Cook, S.A.; O’Regan, D.P. Paradoxical effect of smoking following acute myocardial infarction. J. Cardiovasc. Magn. Reson. 2013, 15, O107. [Google Scholar] [CrossRef] [Green Version]
- Ohman, E.M.; Roe, M.T.; Steg, P.G.; James, S.K.; Povsic, T.J.; White, J.; Rockhold, F.; Plotnikov, A.; Mundl, H.; Strony, J.; et al. Clinically significant bleeding with low-dose rivaroxaban versus aspirin, in addition to P2Y12 inhibition, in acute coronary syndromes (GEMINI-ACS-1): A double-blind, multicentre, randomised trial. Lancet 2017, 389, 1799–1808. [Google Scholar] [CrossRef]
- Pan, H.; Lindon, A.; Grabau, R.; Dominguez, W.; Wickline, S. P3100Anti-thrombin nanoparticles limit ischemia-reperfusion injury and no-reflow in myocardial infarction. Eur. Heart J. 2019, 40, ehz745.0176. [Google Scholar] [CrossRef]
- Jumeau, C.; Rupin, A.; Chieng-Yane, P.; Mougenot, N.; Zahr, N.; David-Dufilho, M.; Hatem, S.N. Direct Thrombin Inhibitors Prevent Left Atrial Remodeling Associated With Heart Failure in Rats. JACC Basic Transl. Sci. 2016, 1, 328–339. [Google Scholar] [CrossRef]
- Dong, A.; Mueller, P.; Yang, F.; Yang, L.; Morris, A.; Smyth, S.S. Direct thrombin inhibition with dabigatran attenuates pressure overload-induced cardiac fibrosis and dysfunction in mice. Thromb. Res. 2017, 159, 58–64. [Google Scholar] [CrossRef]
- Bahall, M.; Seemungal, T.; Khan, K.; Legall, G. Medical care of acute myocardial infarction patients in a resource limiting country, Trinidad: A cross-sectional retrospective study. BMC Health Serv. Res. 2019, 19, 501. [Google Scholar] [CrossRef] [Green Version]
- Medagama, A.; Bandara, R.; De Silva, C.; Galgomuwa, M.P. Management of acute coronary syndromes in a developing country; time for a paradigm shift? an observational study. BMC Cardiovasc. Disord. 2015, 15, 133. [Google Scholar] [CrossRef] [Green Version]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef] [PubMed]
- Gupta, T.; Kolte, D.; Khera, S.; Harikrishnan, P.; Mujib, M.; Aronow, W.S.; Jain, D.; Ahmed, A.; Cooper, H.A.; Frishman, W.H.; et al. Smoker’s Paradox in Patients With ST-Segment Elevation Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention. J. Am. Heart Assoc. 2016, 5, e003370. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Feistritzer, H.-J.; Eitel, I.; Jobs, A.; de Waha-Thiele, S.; Stiermaier, T.; Abdel-Wahab, M.; Lurz, P.; Reinstadler, S.J.; Reindl, M.; Klug, G.; et al. Impact of smoking on cardiac magnetic resonance infarct characteristics and clinical outcome in patients with non-ST-elevation myocardial infarction. Int. J. Cardiovasc. Imaging 2019, 35, 1079–1087. [Google Scholar] [CrossRef]
- Turkbey, E.B.; Nacif, M.S.; Guo, M.; McClelland, R.L.; Teixeira, P.B.; Bild, D.E.; Barr, R.G.; Shea, S.; Post, W.; Burke, G.; et al. Prevalence and Correlates of Myocardial Scar in a US Cohort. JAMA 2015, 314, 1945–1954. [Google Scholar] [CrossRef] [PubMed]
- Gori, T.; Lisi, M.; Dragoni, S.; Leone, M.C.; Forconi, S.; Munzel, T.; Parker, J.D. Smoking-induced preconditioning: Acute, but not chronic, smoking paradoxically protects the endothelium from ischemia and reperfusion. Eur. Heart J. 2013, 34, eht310.P5546. [Google Scholar] [CrossRef] [Green Version]
- Koerselman, J.; de Jaegere, P.P.; Verhaar, M.C.; Grobbee, D.E.; van der Graaf, Y. Coronary collateral circulation: The effects of smoking and alcohol. Atherosclerosis 2007, 191, 191–198. [Google Scholar] [CrossRef]
- West, R. Tobacco smoking: Health impact, prevalence, correlates and interventions. Psychol. Health 2017, 32, 1018–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonzalez, P.E.; Omar, W.; Patel, K.V.; Lemos, J.A.d.; Bavry, A.A.; Koshy, T.P.; Mullasari, A.S.; Alexander, T.; Banerjee, S.; Kumbhani, D.J. Fibrinolytic Strategy for ST-Segment–Elevation Myocardial Infarction. Circ. Cardiovasc. Interv. 2020, 13, e009622. [Google Scholar] [CrossRef]
- Hansen, C.H.; Ritschel, V.; Andersen, G.; Halvorsen, S.; Eritsland, J.; Arnesen, H.; Seljeflot, I. Markers of Thrombin Generation Are Associated With Long-Term Clinical Outcome in Patients With ST-Segment Elevation Myocardial Infarction. Clin. Appl. Thromb. Hemost. Off. J. Int. Acad. Clin. Appl. Thromb. Hemost. 2018, 24, 1088–1094. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Total (n = 113) | Primary PCI (n = 76) | Pharmacoinvasive (n = 37) | p-Value | |
|---|---|---|---|---|
| Mean age (years) | 55.19 ± 8.25 | 55.97 ± 7.69 | 53.57 ± 9.19 | 0.146 |
| Male (%) | 103 (91.2) | 72 (94.7) | 31 (83.8) | 0.054 |
| Ethnicity (%) Chinese Malay Indian Others | 49 (43.4) 35 (31.0) 11 (9.7) 18 (15.9) | 42 (55.3) 16 (21.1) 11 (14.5) 7 (9.2) | 7 (18.9) 19 (51.4) 0 (0.0) 11 (29.7) | <0.001 |
| Smoking status Current Ex-smoker Never smoker | 66 (58.4) 12 (10.6) 35 (31.0) | 42 (55.3) 7 (9.2) 27 (35.5) | 24 (64.9) 5 (13.5) 8 (21.6) | 0.304 |
| History of diabetes | 26 (23.0) | 17 (22.4) | 9 (24.3) | 0.817 |
| History of hypertension | 54 (47.8) | 41 (53.9) | 13 (35.1) | 0.060 |
| History of hyperlipidaemia | 49 (43.4) | 35 (46.1) | 14 (37.8) | 0.408 |
| Family history of premature CAD | 15 (13.3) | 8 (10.5) | 7 (18.9) | 0.217 |
| Prior MI | 3 (2.7) | 2 (2.6) | 1 (2.7) | 0.982 |
| Prior PCI | 2 (1.8) | 1 (1.3) | 1 (2.7) | 0.600 |
| Prior CABG | 0 (0.0) | 0 (0.0) | 0 (0.0) | N/A |
| Prior stroke | 4 (3.5) | 4 (5.3) | 0 (0.0) | 0.155 |
| Laboratory Parameters | ||||
| Total cholesterol (mmol/dL) | 5.33 (4.61, 5.87) | 5.26 (4.65, 5.68) | 5.40 (4.50, 5.90) | 0.503 |
| Triglyceride (mmol/dL) | 1.59 (1.16, 2.29) | 1.51 (1.16, 2.22) | 1.77 (1.22, 2.50) | 0.230 |
| Low density lipoprotein cholesterol (mmol/dL) | 3.43 (2.70, 4.00) | 3.50 (2.63, 4.00) | 3.40 (2.95, 4.05) | 0.752 |
| High density lipoprotein (mmol/dL) | 1.06 (0.96, 1.20) | 1.08 (0.96, 1.22) | 1.03 (0.93, 1.17) | 0.222 |
| HbA1c (%) | 6.1 (5.7, 7.0) | 5.95 (5.65, 6.95) | 6.75 (6.10, 10.95) | 0.127 |
| Creatinine (umol/L) | 87.0 (77.0, 102.0) | 84.0 (75.0, 98.5) | 94.0 (80.0, 108.0) | 0.017 |
| Troponin I (ng/mL) | 14,492.1 (1787.7, 38,633.0) | 11,311.6 (913.1, 26,518.0) | 30,641 (14,233.2, 46,625.2) | <0.001 |
| Troponin T (ng/mL) | 2086.0 (600.1, 3898.0) | 1581.5 (395.1, 3349.5) | 3054.0 (1816.0, 5478.0) | 0.001 |
| NT-ProBNP | 831.1 (493.6, 1463.0) | 822.2 (530.4, 1469.0) | 899.5 (327.3, 1463.0) | 0.920 |
| GDF15 | 1278.0 (926.0, 1778.0) | 1298.0 (902.0, 1787.0) | 1252.5 (929.4, 1771.0) | 0.882 |
| White cell count (109/L) | 11.3 (9.6, 13.9) | 11.2 (9.3, 12.9) | 12.1 (9.9, 14.0) | 0.127 |
| Platelet count (109/L) | 249.0 (214.0, 293.0) | 250.5 (215.0, 296.5) | 244.0 (200.0, 280.0) | 0.305 |
| Haemoglobin (109/L) | 15.1 (13.9, 15.7) | 15.1 (14.0, 15.7) | 14.7 (13.9, 15.7) | 0.825 |
| Endogenous Thrombin Potential (n = 104) (nM.min) | 1355.7 (1170.1, 1570.3) | 1400.3 (1190.6, 1565.2) | 1334.1 (1079.5, 1605.4) | 0.473 |
| Discharge Medications | ||||
| Aspirin | 112 (99.1) | 75 (98.7) | 37 (100.0) | 0.483 |
| P2Y12 Inhibitor Clopidogrel Ticagrelor | 57 (50.4) 56 (49.6) | 21 (27.6) 55 (72.4) | 36 (97.3) 1 (2.7) | <0.001 |
| Statin | 113 (100.0) | 76 (100.0) | 37 (100.0) | N/A |
| Beta-blocker | 88 (77.9) | 64 (84.2) | 24 (64.9) | 0.020 |
| ACE-I/ARB | 72 (63.7) | 52 (68.4) | 20 (54.1) | 0.136 |
| Variable | Primary PCI | Pharmacoinvasive | ||||
|---|---|---|---|---|---|---|
| Baseline | 1 Month | 6 Months | Baseline | 1 Month | 6 Months | |
| Endogenous Thrombin Potential (nM.min) | 1400.29 (1190.57, 1565.19) | 1261.15 (1110.84, 1419.88) * | 1248.01 (1139.72, 1368.45) ** | 1334.14 (1079.45, 1605.42) | 1326.52 (1173.72, 1413.01) | 1307.73 (1161.83, 1448.04) |
| Variable | Primary PCI | Pharmacoinvasive | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Baseline | 6 Months | Change | p Value Comparing Baseline and 6 Months | Baseline | 6 Months | Change | p Value Comparing Baseline and 6 Months | p Value Comparing Change in Value of PPCI and Pharmacoinvasive Groups | |
| Infarct Size (LGE) (%) | 21.68 (14.41, 26.59) | 19.96 (14.48, 24.62) | −0.76 (−7.21, 3.31) | 0.251 | 16.60 (12.88, 21.68) | 15.34 (9.45, 22.92) | −2.88 (−5.46, 2.17) | 0.106 | 0.680 |
| Adverse ventricular remodeling * | - | 7 (10.9) | - | - | 4 (13.8) | - | |||
| LVESV (mL) | 48.74 (38.07, 69.39) | 39.41 (28.98, 56.77) | −7.07 (−16.05, 0.58) | <0.001 | 55.48 (40.57, 71.48) | 48.18 (34.96, 72.27) | −3.87 (−9.83, 6.89) | 0.388 | 0.081 |
| LVEDV (mL) | 117.18 (103.75, 137.94) | 114.22 (97.27, 137.23) | 0.56 (−13.58, 13.02) | 0.863 | 129.20 (111.99, 148.14) | 123.06 (111.17, 149.21) | −1.69 (−9.38, 13.14) | 0.992 | 0.885 |
| LVEF (%) | 57.07 (47.48, 65.17) | 63.42 (56.84, 72.36) | 5.66 (1.68, 11.29) | <0.001 | 55.20 (49.33, 65.59) | 59.33 (48.82, 67.34) | 2.37 (−3.06, 5.56) | 0.337 | 0.005 |
| Variable | Adjusted Odds Ratio | 95% CI | p Value |
|---|---|---|---|
| ETP Base (10 units) | 1.019 | 1.002–1.036 | 0.027 |
| Age | 0.953 | 0.892–1.018 | 0.154 |
| Hypertension | 0.504 | 0.177–1.436 | 0.200 |
| Diabetes mellitus | 1.398 | 0.435–4.496 | 0.574 |
| Smoking Status Current Ex-smoker | 0.311 0.203 | 0.105–0.919 0.028–1.482 | 0.035 0.116 |
| Previous stroke | 2.185 | 0.170–28.062 | 0.548 |
| Primary PCI Pharmacoinvasive | Reference 1.064 | 0.227–4.992 | 0.938 |
| Clopidogrel Ticagrelor | Reference 1.481 | 0.383–5.731 | 0.569 |
| Variable | Adjusted Odds Ratio | 95% CI | p Value |
|---|---|---|---|
| ETP base (10 units) | 0.986 | 0.962–1.010 | 0.248 |
| Age | 1.012 | 0.917–1.117 | 0.806 |
| Hypertension | 2.432 | 0.483–12.247 | 0.281 |
| Diabetes mellitus | 1.885 | 0.419–8.493 | 0.409 |
| Smoking Status Current Ex-smoker | 0.750 2.984 | 0.173–3.249 0.260–34.170 | 0.700 0.380 |
| Previous stroke | 2.626 | 0.212–32.553 | 0.452 |
| Primary PCI Pharmacoinvasive | Reference 0.581 | 0.033–10.320 | 0.712 |
| Clopidogrel Ticagrelor | Reference 2.265 | 0.266–19.307 | 0.455 |
| Variable | Adjusted Odds Ratio | 95% CI | p Value |
|---|---|---|---|
| ETP base (10 units) | 0.993 | 0.977–1.009 | 0.378 |
| Age | 1.005 | 0.939–1.075 | 0.890 |
| Hypertension | 1.691 | 0.533–5.364 | 0.372 |
| Diabetes mellitus | 0.445 | 0.131–1.512 | 0.195 |
| Smoking Status Current Ex-smoker | 0.766 2.392 | 0.226–2.592 0.181–31.601 | 0.668 0.508 |
| Primary PCI Pharmacoinvasive | Reference 1.194 | 0.263–5.426 | 0.819 |
| Clopidogrel Ticagrelor | Reference 3.378 | 0.806–14.150 | 0.096 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sia, C.-H.; Tan, S.-H.; Chan, S.-P.; Marchesseau, S.; Sim, H.-W.; Carvalho, L.; Chen, R.; Amin, N.H.M.; Fong, A.Y.-Y.; Richards, A.M.; et al. Enhanced Thrombin Generation Is Associated with Worse Left Ventricular Scarring after ST-Segment Elevation Myocardial Infarction: A Cohort Study. Pharmaceuticals 2022, 15, 718. https://doi.org/10.3390/ph15060718
Sia C-H, Tan S-H, Chan S-P, Marchesseau S, Sim H-W, Carvalho L, Chen R, Amin NHM, Fong AY-Y, Richards AM, et al. Enhanced Thrombin Generation Is Associated with Worse Left Ventricular Scarring after ST-Segment Elevation Myocardial Infarction: A Cohort Study. Pharmaceuticals. 2022; 15(6):718. https://doi.org/10.3390/ph15060718
Chicago/Turabian StyleSia, Ching-Hui, Sock-Hwee Tan, Siew-Pang Chan, Stephanie Marchesseau, Hui-Wen Sim, Leonardo Carvalho, Ruth Chen, Nor Hanim Mohd Amin, Alan Yean-Yip Fong, Arthur Mark Richards, and et al. 2022. "Enhanced Thrombin Generation Is Associated with Worse Left Ventricular Scarring after ST-Segment Elevation Myocardial Infarction: A Cohort Study" Pharmaceuticals 15, no. 6: 718. https://doi.org/10.3390/ph15060718