
The Occurrence of Hyperactivated Platelets and Fibrinaloid Microclots in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
 and
and
Abstract
:1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Ethical Statement
4.2. Sample Demographics and Blood Collection
4.3. Viscoelastic Analysis
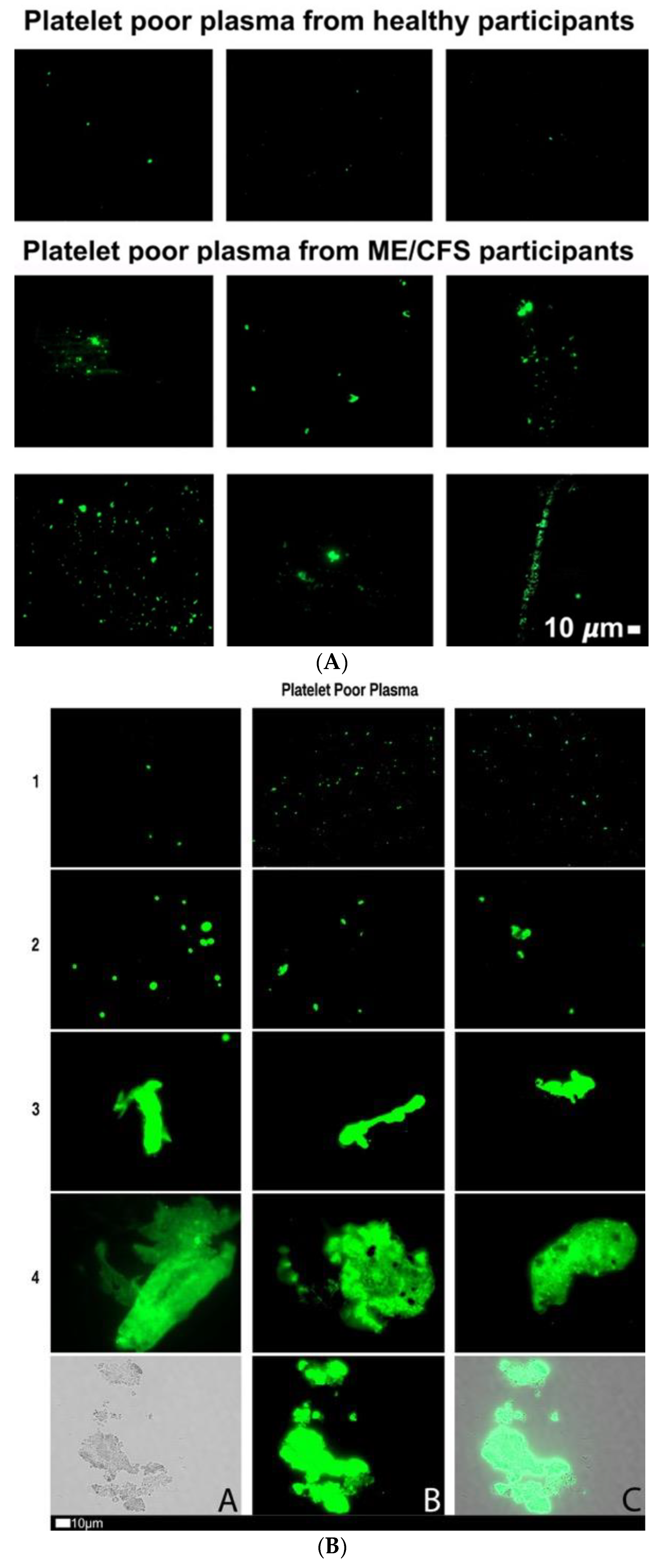
4.4. Fibrinaloid Microclot Analysis of PPP
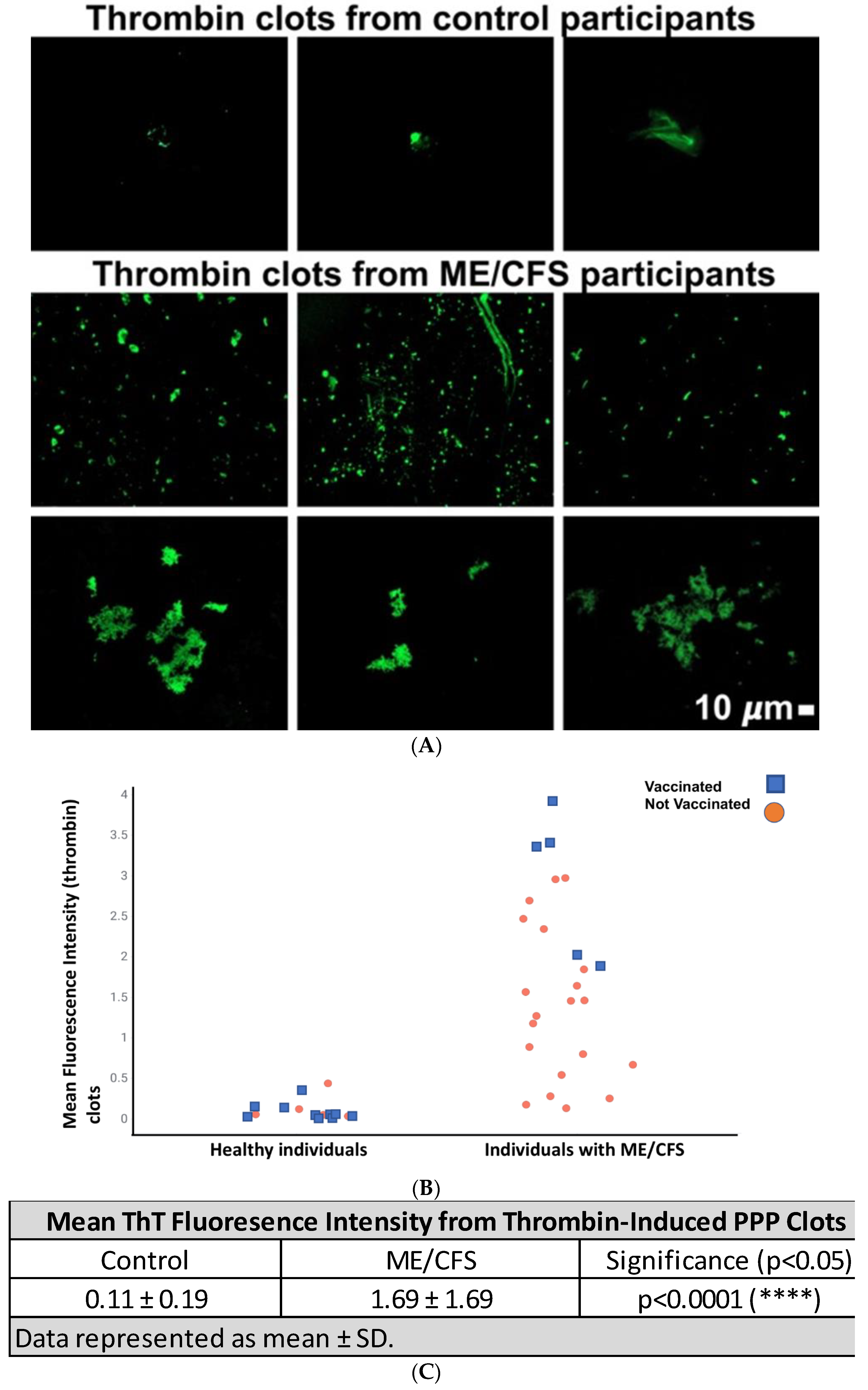
4.5. Amyloid Analysis of PPP Clots after Addition of Thrombin to Create Fibrin Networks
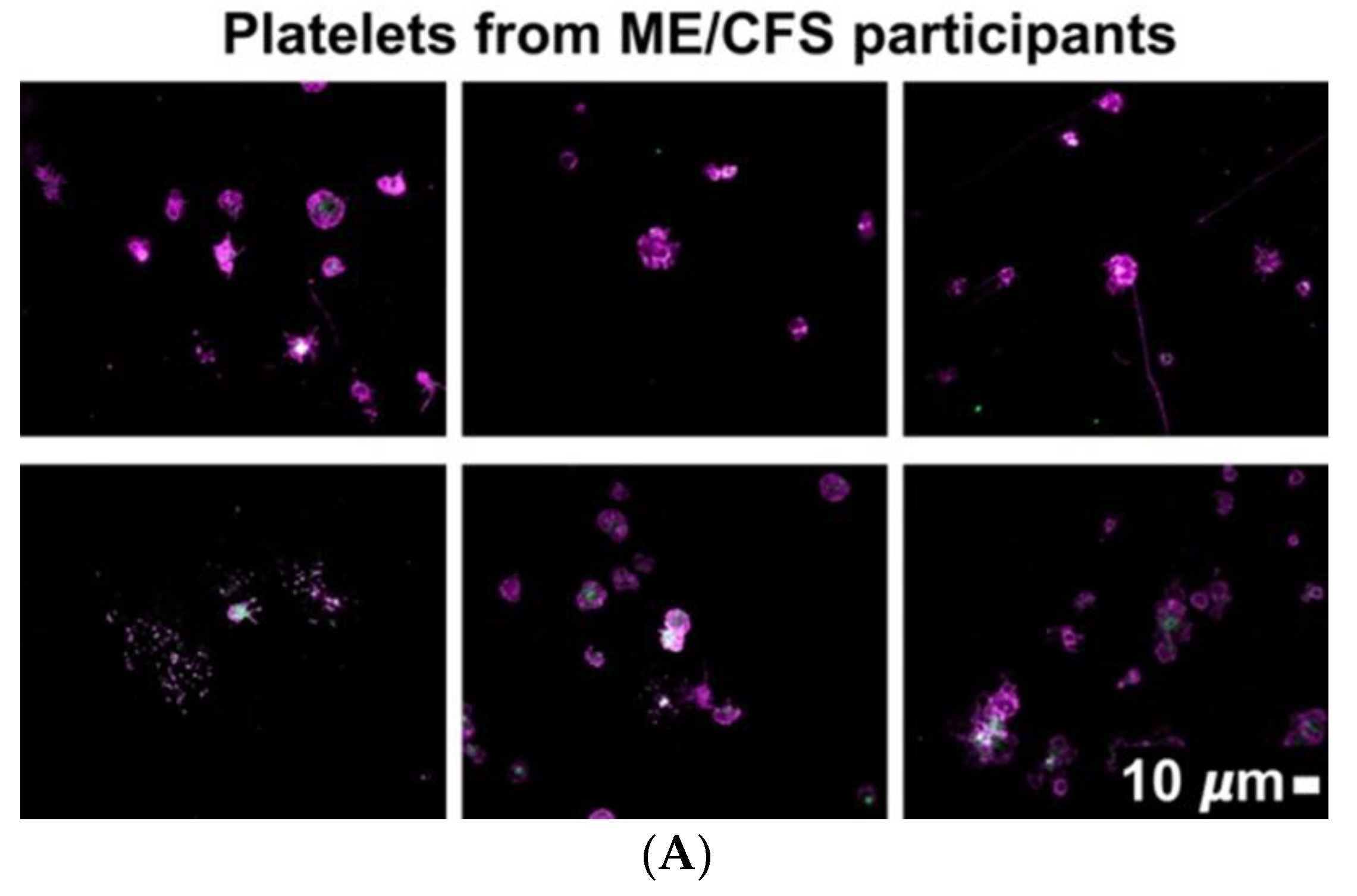
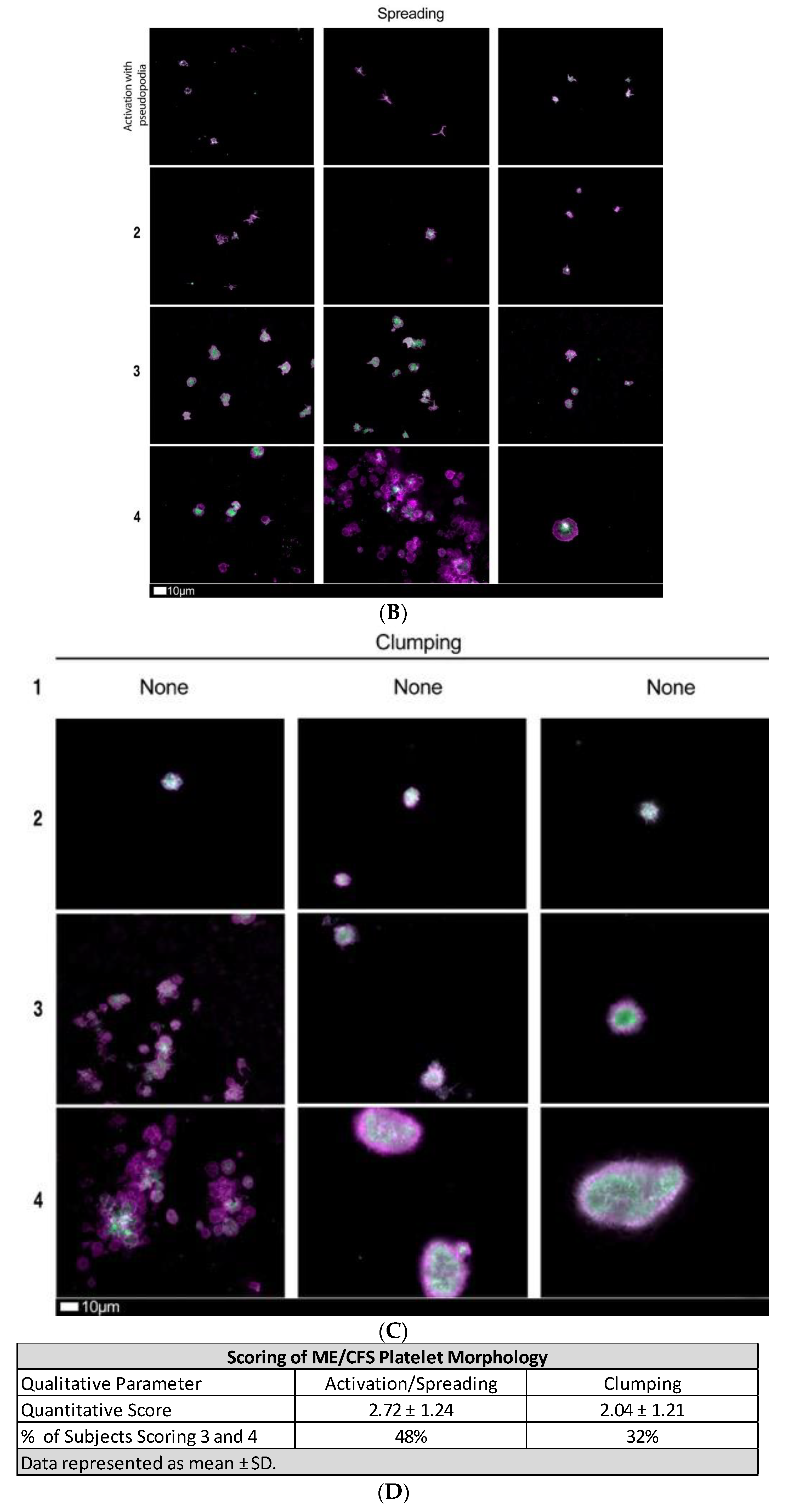
4.6. Assessment of Platelet Phenoptype
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bested, A.C.; Marshall, L.M. Review of Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: An evidence-based approach to diagnosis and management by clinicians. Rev. Environ. Health 2015, 30, 223–249. [Google Scholar] [CrossRef] [PubMed]
- Clayton, E.W. Beyond myalgic encephalomyelitis/chronic fatigue syndrome: An IOM report on redefining an illness. JAMA 2015, 313, 1101–1102. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.; Brenu, E.W.; Staines, D.; Marshall-Gradisnik, S. The prevalence of chronic fatigue syndrome/myalgic encephalomyelitis: A meta-analysis. Clin. Epidemiol. 2013, 5, 105–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, E.J.; Ahn, Y.C.; Jang, E.S.; Lee, S.W.; Lee, S.H.; Son, C.G. Systematic review and meta-analysis of the prevalence of chronic fatigue syndrome/myalgic encephalomyelitis (CFS/ME). J. Transl. Med. 2020, 18, 100. [Google Scholar] [CrossRef] [PubMed]
- Jason, L.A.; Mirin, A.A. Updating the National Academy of Medicine ME/CFS prevalence and economic impact figures to account for population growth and inflation. Fatigue Biomed. Health Behav. 2021, 9, 9–13. [Google Scholar] [CrossRef]
- Mirin, A.A.; Dimmock, M.E.; Jason, L.A. Updated ME/CFS prevalence estimates reflecting post-COVID increases and associated economic costs and funding implications. Fatigue Biomed. Health Behav. 2022, 10, 83–93. [Google Scholar] [CrossRef]
- Chia, J.; Chia, A.; Voeller, M.; Lee, T.; Chang, R. Acute enterovirus infection followed by myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and viral persistence. J. Clin. Pathol. 2010, 63, 165–168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerr, J. Early Growth Response Gene Upregulation in Epstein-Barr Virus (EBV)-Associated Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Biomolecules 2020, 10, 1484. [Google Scholar] [CrossRef]
- Shikova, E.; Reshkova, V.; Kumanova, A.C.; Raleva, S.; Alexandrova, D.; Capo, N. Cytomegalovirus, Epstein-Barr virus, and human herpesvirus-6 infections in patients with myalgic small ie, Cyrillicncephalomyelitis/chronic fatigue syndrome. J. Med. Virol. 2020, 92, 3682–3688. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ariza, M.E. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: The Human Herpesviruses Are Back! Biomolecules 2021, 11, 185. [Google Scholar] [CrossRef] [PubMed]
- Rasa, S.; Nora-Krukle, Z.; Henning, N.; Eliassen, E.; Shikova, E.; Harrer, T. Chronic viral infections in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J. Transl. Med. 2018, 16, 268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proal, A.; Marshall, T. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome in the Era of the Human Microbiome: Persistent Pathogens Drive Chronic Symptoms by Interfering With Host Metabolism, Gene Expression, and Immunity. Front. Pediatr. 2018, 6, 373. [Google Scholar] [CrossRef] [PubMed]
- Maes, M.; Twisk, F.N.; Kubera, M.; Ringel, K.; Leunis, J.C.; Geffard, M. Increased IgA responses to the LPS of commensal bacteria is associated with inflammation and activation of cell-mediated immunity in chronic fatigue syndrome. J. Affect. Disord. 2012, 136, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Giloteaux, L.; Goodrich, J.K.; Walters, W.A.; Levine, S.M.; Ley, R.E.; Hanson, M.R. Reduced diversity and altered composition of the gut microbiome in individuals with myalgic encephalomyelitis/chronic fatigue syndrome. Microbiome 2016, 4, 30. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hickie, I.; Davenport, T.; Wakefield, D.; Vollmer-Conna, B.; Cameron, B.; Vernon, S.D. Post-infective and chronic fatigue syndromes precipitated by viral and non-viral pathogens: Prospective cohort study. BMJ 2006, 333, 575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raijmakers, R.P.H.; Roerink, M.E.; Jansen, A.F.M.; Keijmel, R.; Gacesa, R.; Li, Y. Multi-omics examination of Q fever fatigue syndrome identifies similarities with chronic fatigue syndrome. J. Transl. Med. 2020, 18, 448. [Google Scholar] [CrossRef]
- Keijmel, S.P.; Saxe, J.; van der Meer, J.W.; Nikolaus, S.; Netea, M.G.; Bleijenberg, G. A comparison of patients with Q fever fatigue syndrome and patients with chronic fatigue syndrome with a focus on inflammatory markers and possible fatigue perpetuating cognitions and behaviour. J. Psychosom. Res. 2015, 79, 295–302. [Google Scholar] [CrossRef]
- Al-Aly, Z.; Bowe, B.; Xie, Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat. Med. 2022, 28, 1461–1467. [Google Scholar] [CrossRef]
- Wong, T.L.; Weitzer, D.J. Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)-A Systemic Review and Comparison of Clinical Presentation and Symptomatology. Medicina 2021, 57, 418. [Google Scholar] [CrossRef] [PubMed]
- Hunt, J.; Blease, C.; Geraghty, K.J. Long COVID at the crossroads: Comparisons and lessons from the treatment of patients with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). J. Health Psychol. 2022, 13591053221084494. [Google Scholar] [CrossRef] [PubMed]
- Morrow, A.K.; Malone, L.A.; Kokorelis, C.; Petracek, L.S.; Eastin, E.F.; Lobner, K.L. Long-Term COVID 19 Sequelae in Adolescents: The Overlap with Orthostatic Intolerance and ME/CFS. Curr. Pediatr. Rep. 2022, 10, 31–44. [Google Scholar] [CrossRef] [PubMed]
- Siberry, V.G.R.; Rowe, P.C. Pediatric Long COVID and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Overlaps and Opportunities. Pediatr. Infect. Dis. J. 2022, 41, e139–e141. [Google Scholar] [CrossRef]
- Kedor, C.; Freitag, H.; Meyer-Arndt, L.; Wittke, K.; Zoller, T.; Steinbeis, F. Chronic COVID-19 Syndrome and Chronic Fatigue Syndrome (ME/CFS) following the first pandemic wave in Germany—A first analysis of a prospective observational study. medRxiv 2021. [Google Scholar] [CrossRef]
- Proal, A.D.; VanElzakker, M.B. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front. Microbiol. 2021, 12, 698169. [Google Scholar] [CrossRef]
- Pretorius, E.; Vlok, M.; Venter, C.; Bezuidenhout, J.A.; Laubscher, G.J.; Steenkamp, J. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc. Diabetol. 2021, 20, 172. [Google Scholar] [CrossRef] [PubMed]
- Kell, D.B.; Laubscher, G.J.; Pretorius, E. A central role for amyloid fibrin microclots in long COVID/PASC: Origins and therapeutic implications. Biochem. J. 2022, 479, 537–559. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, G.; Norris, G.; Spence, V.; McLaren, M.; Belch, J.J. Is chronic fatigue syndrome associated with platelet activation? Blood Coagul. Fibrinolysis 2006, 17, 89–92. [Google Scholar] [CrossRef] [PubMed]
- Brenu, E.W.; Staines, D.R.; Baskurt, O.K.; Ashton, K.J.; Ramos, S.B.; Christy, R.M. Immune and hemorheological changes in chronic fatigue syndrome. J. Transl. Med. 2010, 8, 1. [Google Scholar] [CrossRef] [Green Version]
- Brewer, J.H.; Berg, D. Hypercoaguable State Associated with Active Human Herpesvirus-6 (HHV-6) Viremia in Patients with Chronic Fatigue Syndrome. J. Chronic Fatigue Syndr. 2001, 8, 111–116. [Google Scholar] [CrossRef]
- Berg, D.; Berg, L.H.; Couvaras, J.; Harrison, H. Chronic fatigue syndrome and/or fibromyalgia as a variation of antiphospholipid antibody syndrome: An explanatory model and approach to laboratory diagnosis. Blood Coagul. Fibrinolysis 1999, 10, 435–438. [Google Scholar] [CrossRef] [Green Version]
- Bonilla, H.; Hampton, D.; Marques de Menezes, E.G.; Deng, X.; Montoya, J.G.; Anderson, J. Comparative Analysis of Extracellular Vesicles in Patients with Severe and Mild Myalgic Encephalomyelitis/Chronic Fatigue Syndrome. Front. Immunol. 2022, 13, 841910. [Google Scholar] [CrossRef] [PubMed]
- Newton, D.J.; Kennedy, G.; Chan, K.K.; Lang, C.C.; Belch, J.J.; Khan, F. Large and small artery endothelial dysfunction in chronic fatigue syndrome. Int. J. Cardiol. 2012, 154, 335–336. [Google Scholar] [CrossRef] [PubMed]
- Scherbakov, N.; Szklarski, M.; Hartwig, J.; Sotzny, F.; Lorenz, S.; Meyer, A. Peripheral endothelial dysfunction in myalgic encephalomyelitis/chronic fatigue syndrome. ESC Heart Fail. 2020, 7, 1064–1071. [Google Scholar] [CrossRef] [PubMed]
- Bertinat, R.; Villalobos-Labra, R.; Hofmann, L.; Blauensteiner, J.; Sepulveda, N.; Westermeier, F. Decreased NO production in endothelial cells exposed to plasma from ME/CFS patients. Vasc. Pharm. 2022, 143, 106953. [Google Scholar] [CrossRef]
- Lopes Pires, M.E.; Clarke, S.R.; Marcondes, S.; Gibbins, J.M. Lipopolysaccharide potentiates platelet responses via toll-like receptor 4-stimulated Akt-Erk-PLA2 signalling. PLoS ONE 2017, 12, e0186981. [Google Scholar] [CrossRef]
- Li, C.; Li, J.; Ni, H. Crosstalk Between Platelets and Microbial Pathogens. Front. Immunol. 2020, 11, 1962. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Pretorius, E. A Champion of Host Defense: A Generic Large-Scale Cause for Platelet Dysfunction and Depletion in Infection. Semin. Thromb. Hemost. 2020, 46, 302–319. [Google Scholar] [CrossRef] [Green Version]
- Antoniak, S.; Mackman, N. Platelets and viruses. Platelets 2021, 32, 325–330. [Google Scholar] [CrossRef]
- Branchford, B.R.; Carpenter, S.L. The Role of Inflammation in Venous Thromboembolism. Front. Pediatr. 2018, 6, 142. [Google Scholar] [CrossRef]
- Pretorius, L.; Thomson, G.J.A.; Adams, R.C.M.; Nell, T.A.; Laubscher, W.A.; Pretorius, E. Platelet activity and hypercoagulation in type 2 diabetes. Cardiovasc. Diabetol. 2018, 17, 141. [Google Scholar] [CrossRef] [Green Version]
- Aksu, K.; Donmez, A.; Keser, G. Inflammation-induced thrombosis: Mechanisms, disease associations and management. Curr. Pharm. Des. 2012, 18, 1478–1493. [Google Scholar] [CrossRef] [PubMed]
- Kell, D.B.; Pretorius, E. The simultaneous occurrence of both hypercoagulability and hypofibrinolysis in blood and serum during systemic inflammation, and the roles of iron and fibrin(ogen). Integr. Biol. 2015, 7, 24–52. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bester, J.; Soma, P.; Kell, D.B.; Pretorius, E. Viscoelastic and ultrastructural characteristics of whole blood and plasma in Alzheimer-type dementia, and the possible role of bacterial lipopolysaccharides (LPS). Oncotarget 2015, 6, 35284–35303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nunes, J.M.; Fillis, T.; Page, M.J.; Venter, C.; Lancry, O.; Kell, D.B. Gingipain R1 and Lipopolysaccharide From Porphyromonas gingivalis Have Major Effects on Blood Clot Morphology and Mechanics. Front. Immunol. 2020, 11, 1551. [Google Scholar] [CrossRef]
- Abou-Ismail, M.Y.; Diamond, A.; Kapoor, S.; Arafah, Y.; Nayak, L. The hypercoagulable state in COVID-19: Incidence, pathophysiology, and management. Thromb. Res. 2020, 194, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, E.; Swanepoel, A.C.; DeVilliers, S.; Bester, J. Blood clot parameters: Thromboelastography and scanning electron microscopy in research and clinical practice. Thromb. Res. 2017, 154, 59–63. [Google Scholar] [CrossRef] [PubMed]
- Laubscher, G.J.; Lourens, P.J.; Venter, C.; Kell, D.B.; Pretorius, E. TEG((R)), Microclot and Platelet Mapping for Guiding Early Management of Severe COVID-19 Coagulopathy. J. Clin. Med. 2021, 10, 5381. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T. Myalgic encephalomyelitis: International Consensus Criteria. J. Intern. Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grobbelaar, L.M.; Venter, C.; Vlok, M.; Ngoepe, M.; Laubscher, G.J.; Lourens, P.J. SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: Implications for microclot formation in COVID-19. Biosci. Rep. 2021, 41, BSR20210611. [Google Scholar] [CrossRef] [PubMed]
- Kell, D.B.; Pretorius, E. Proteins behaving badly. Substoichiometric molecular control and amplification of the initiation and nature of amyloid fibril formation: Lessons from and for blood clotting. Prog. Biophys. Mol. Biol. 2017, 123, 16–41. [Google Scholar] [CrossRef]
- Varin, R.; Mirshahi, S.; Mirshahi, P.; Klein, C.; Jamshedov, J.; Chidiac, J. Whole blood clots are more resistant to lysis than plasma clots--greater efficacy of rivaroxaban. Thromb. Res. 2013, 131, e100–e109. [Google Scholar] [CrossRef]
- Gade Malmos, K.; Blancas-Mejia, L.M.; Weber, B.; Buchner, J.; Ramirez-Alvarado, M.; Naiki, H. ThT 101: A primer on the use of thioflavin T to investigate amyloid formation. Amyloid 2017, 24, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, E.; Page, M.J.; Engelbrecht, L.; Ellis, G.C.; Kell, D.B. Substantial fibrin amyloidogenesis in type 2 diabetes assessed using amyloid-selective fluorescent stains. Cardiovasc. Diabetol. 2017, 16, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pretorius, E.; Mbotwe, S.; Bester, J.; Robinson, C.J.; Kell, D.B. Acute induction of anomalous and amyloidogenic blood clotting by molecular amplification of highly substoichiometric levels of bacterial lipopolysaccharide. J. R. Soc. Interface 2016, 13, 20160539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakashima, M.O.; Rogers, H.J. Hypercoagulable states: An algorithmic approach to laboratory testing and update on monitoring of direct oral anticoagulants. Blood Res. 2014, 49, 85–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics | ||
| p value (parametric analysis) | 0.54 | |
| Age of control population (n = 15; 9 females; 6 males) | 45.7 ± 6.9 | |
| Age of ME/CFS population (n = 25; 20 females; 5 males) | 48.2 ± 14.1 | |
| Comorbidities of ME/CFS Population | ||
| Comorbidity | % Prevalence | |
| Gut Dysbiosis | 40% | |
| POTS | 16% | |
| Fibromyalgia | 16% | |
| Psoriasis | 16% | |
| Gingivitis/Periodontitis | 16% | |
| Hypercholesterolemia | 16% | |
| Hypertension | 16% | |
| Rheumatoid Arthritis | 12% | |
| Cardiovascular Disease | 12% | |
| Orthostatic Hypotension | 4% | |
| Mast Cell Activation Syndrome | 4% | |
| Rosacea | 4% | |
| Dysautonomia | 4% | |
| ICC Questionnaire Results | ||
| Parameter | Average Score (out of 10) | % of Subjects Experiencing Severely (Score of 8–10) |
| 1. Post-Exertional Neuroimmune Exhaustion | 7.8 ± 1.6 | 60% |
| a. Marked, rapid physical and/or cognitive fatigability in response to exertion | 7.9 ± 1.6 | 64% |
| b. Post-exertional symptom exacerbation (worsening of other symptoms) | 7.8 ± 1.4 | 56% |
| c. Post-exertional exhaustion | 8.1 ± 1.3 | 64% |
| d. Recovery period is prolonged | 7.4 ± 2.0 | 48% |
| e. Low threshold of physical and mental fatigability (lack of stamina) | 8.1 ± 1.7 | 68% |
| 2. Neurological Impairments | 6.6 ± 2.6 | 44% |
| a. Difficulty processing information | 6.52 ± 2.00 | 32% |
| b. Short-term memory loss | 6.64 ± 2.04 | 44% |
| c. Headaches | 6.00 ± 3.27 | 40% |
| d. Significant pain (in muscles, tendons, abdomen, or chest) | 6.68 ± 2.84 | 52% |
| e. Disturbed sleep pattern (from the previous night, e.g., insomnia, sleeping most of the day and being awake most of the night) | 6.72 ± 2.82 | 48% |
| f. Unrefreshing sleep (from the previous night) | 7.92 ± 2.08 | 60% |
| g. Neurosensory and perceptual symptoms (e.g., inability to focus vision, sensitivity to light, noise, etc.) | 7.20± 1.87 | 56% |
| h. Motor symptoms (e.g., twitching, poor coordination) | 5.12 ± 2.65 | 16% |
| 3. Immuno, Gastrointestinal, and Genitourinary Impairments | 5.9 ± 2.7 | 35% |
| a. Flu-like symptoms (e.g., sore throat, sinusitis, enlarged or tender lymph nodes) | 5.48 ± 1.94 | 16% |
| b. Gastrointestinal tract symptoms (e.g., nausea, abdominal pain, bloating, irritable bowel) | 6.32 ± 2.66 | 44% |
| c. Genitourinary symptoms (e.g., urinary urgency, urinary frequency, nocturia or having to urinate two or more times a night) | 5.76 ± 2.96 | 32% |
| d. Sensitivities to food, medications, odors, or chemicals | 6.16 ± 3.05 | 48% |
| Energy Production/Transportation Impairments | 6.6 ± 2.6 | 45% |
| a. Cardiovascular symptoms (e.g., orthostatic intolerance, postural orthostatic tachycardia syndrome or POTS, palpitations, light-headedness/dizziness) | 7.00 ± 2.38 | 52% |
| b. Respiratory symptoms (e.g., air hunger, labored breathing, fatigue of chest wall muscles) | 5.64 ± 2.98 | 32% |
| c. Loss of thermostatic stability (e.g., subnormal body temperature, sweating episodes, recurrent feelings of feverishness, cold extremities) | 7.28 ± 1.54 | 52% |
| d. Intolerance of extremes of temperature | 6.44 ± 2.89 | 44% |
| Data are represented as mean ± standard deviation. | ||
| TEG® of WB | |||
| Parameter | Standard WB Range | ME/CFS WB (n = 25) | Out of Standard Range |
| R | 9–27 | 7.73 ± 2.31 | 16/64% (below) |
| K | 2–9 | 2.39 ± 0.82 | 9/36% (below) |
| α-Angle | 22–58 | 56.99 ± 10.25 | 13/52% (above) |
| Maximum Amplitude | 44–64 | 65.64 ± 7.02 | 14/56% (above) |
| MRTG | 0–10 | 10.05 [7.18–12.12] | 13/52% (above) |
| TMRTG | 5–23 | 9.74 ± 2.73 | 0 |
| TTG | 251–1041 | 787.50 ± 84.07 | 0 |
| TEG® of PPP | |||
| Parameter | Control PPP (n = 15) | ME/CFS PPP (n = 25) | p value |
| R | 10.25 ± 1.97 | 8.54 ± 3.51 | 0.09 |
| K | 3.10 [2.80–3.80] | 1.90 [1.40–4.75] | 0.05 |
| α-Angle | 51.70 [45.00–57.10] | 61.80 [54.00–66.25] | 0.002 (**) |
| Maximum Amplitude | 25.90 [23.00–27.10] | 29.30 [22.05–32.55] | 0.20 |
| MRTG | 8.05 [6.80–8.93] | 12.17 [9.13–15.77] | 0.0009 (***) |
| TMRTG | 11.30 ± 2.20 | 9.68 ± 3.71 | 0.13 |
| TTG | 306.40 [283.30–324.10] | 350.90 [261.30–391.00] | 0.22 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nunes, J.M.; Kruger, A.; Proal, A.; Kell, D.B.; Pretorius, E. The Occurrence of Hyperactivated Platelets and Fibrinaloid Microclots in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Pharmaceuticals 2022, 15, 931. https://doi.org/10.3390/ph15080931
Nunes JM, Kruger A, Proal A, Kell DB, Pretorius E. The Occurrence of Hyperactivated Platelets and Fibrinaloid Microclots in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS). Pharmaceuticals. 2022; 15(8):931. https://doi.org/10.3390/ph15080931
Chicago/Turabian StyleNunes, Jean M., Arneaux Kruger, Amy Proal, Douglas B. Kell, and Etheresia Pretorius. 2022. "The Occurrence of Hyperactivated Platelets and Fibrinaloid Microclots in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)" Pharmaceuticals 15, no. 8: 931. https://doi.org/10.3390/ph15080931