
Inflammatory Biomarkers of Traumatic Brain Injury

 , , ,
, , , 
Abstract
:1. Introduction
2. Results
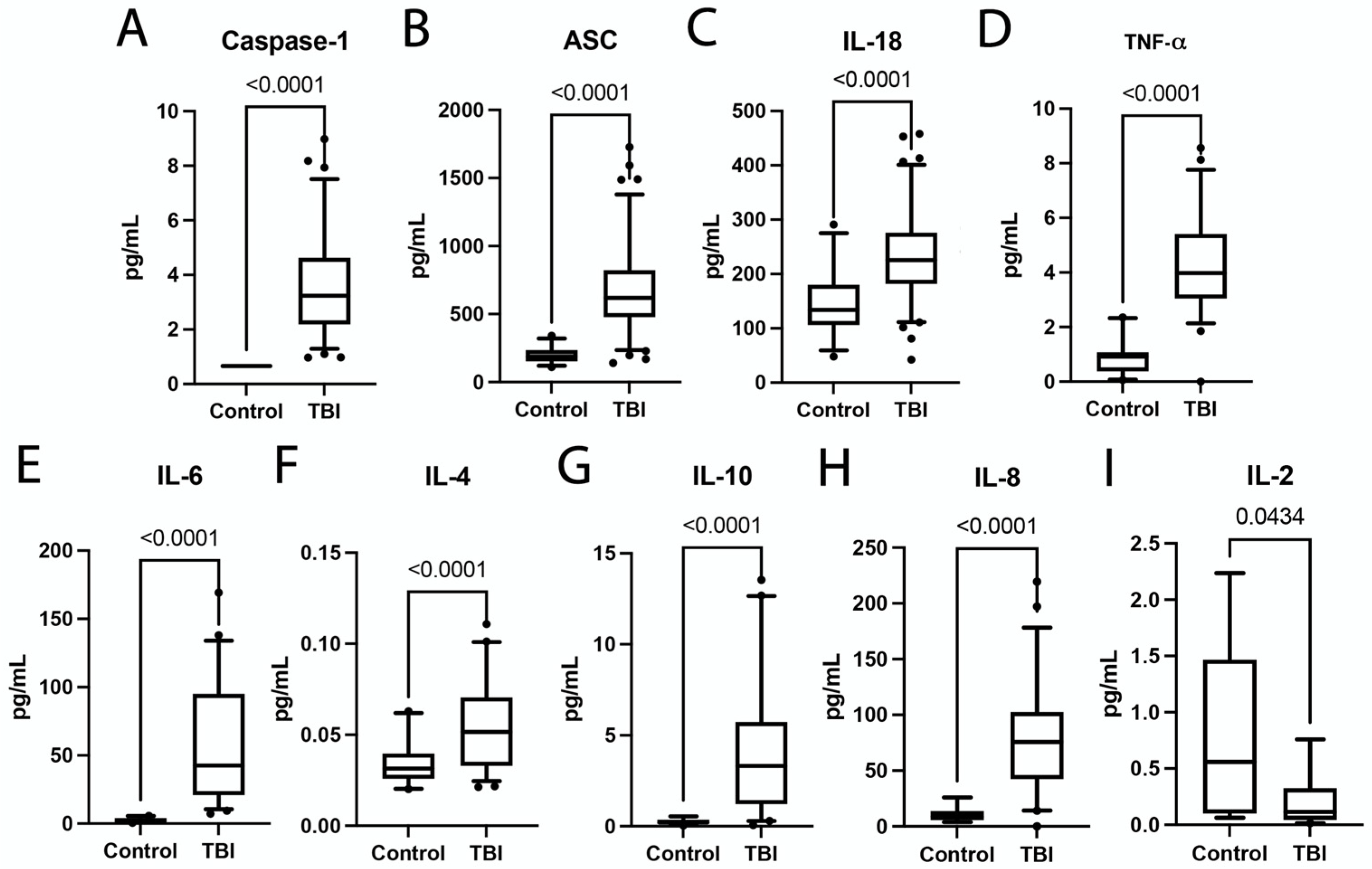
2.1. Inflammasome Proteins and Inflammatory Cytokines Are Elevated in TBI Patients
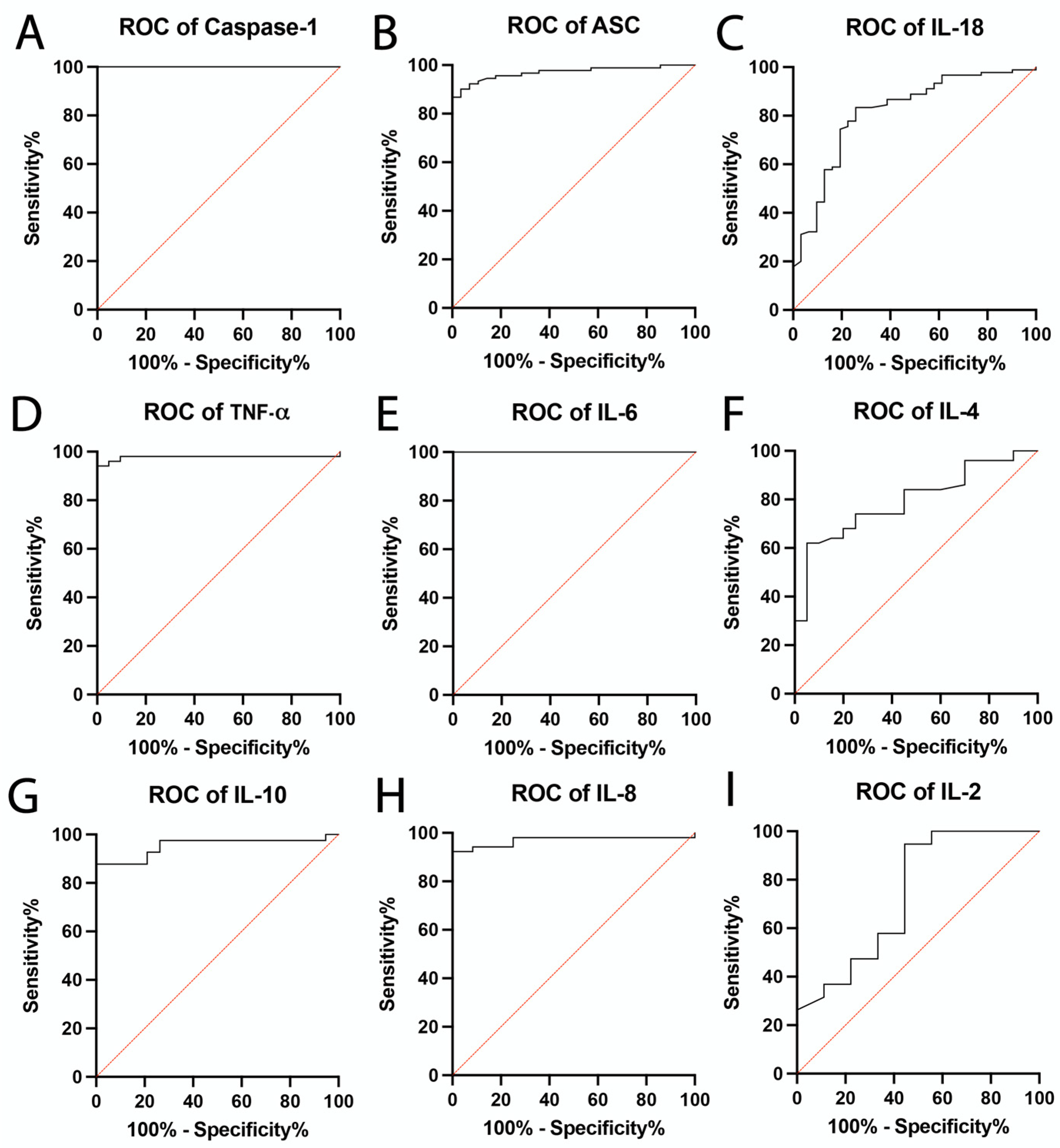
2.2. Inflammatory Biomarkers of TBI
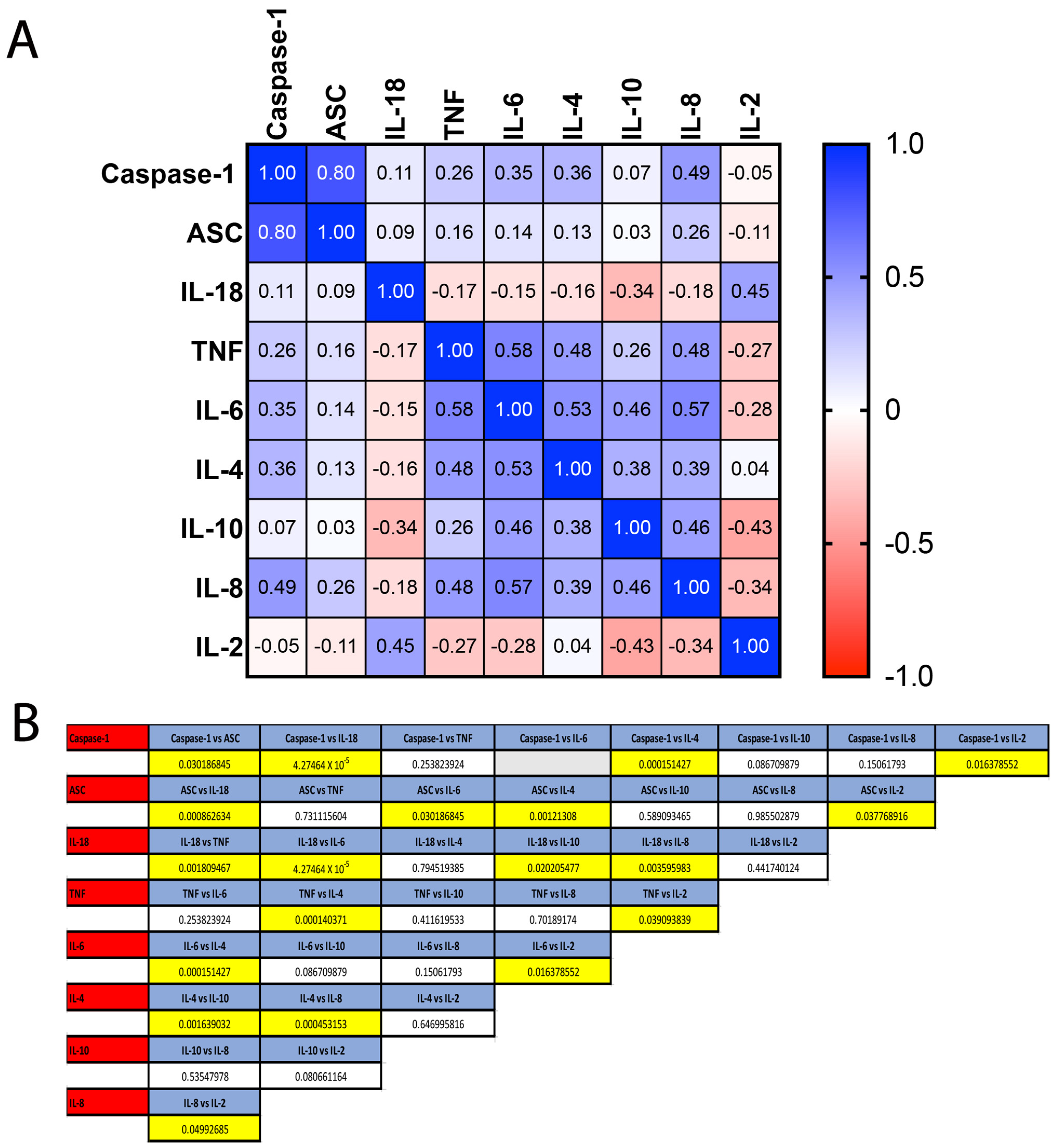
2.3. Comparison between ROC Curves for Identified Inflammatory Biomarkers
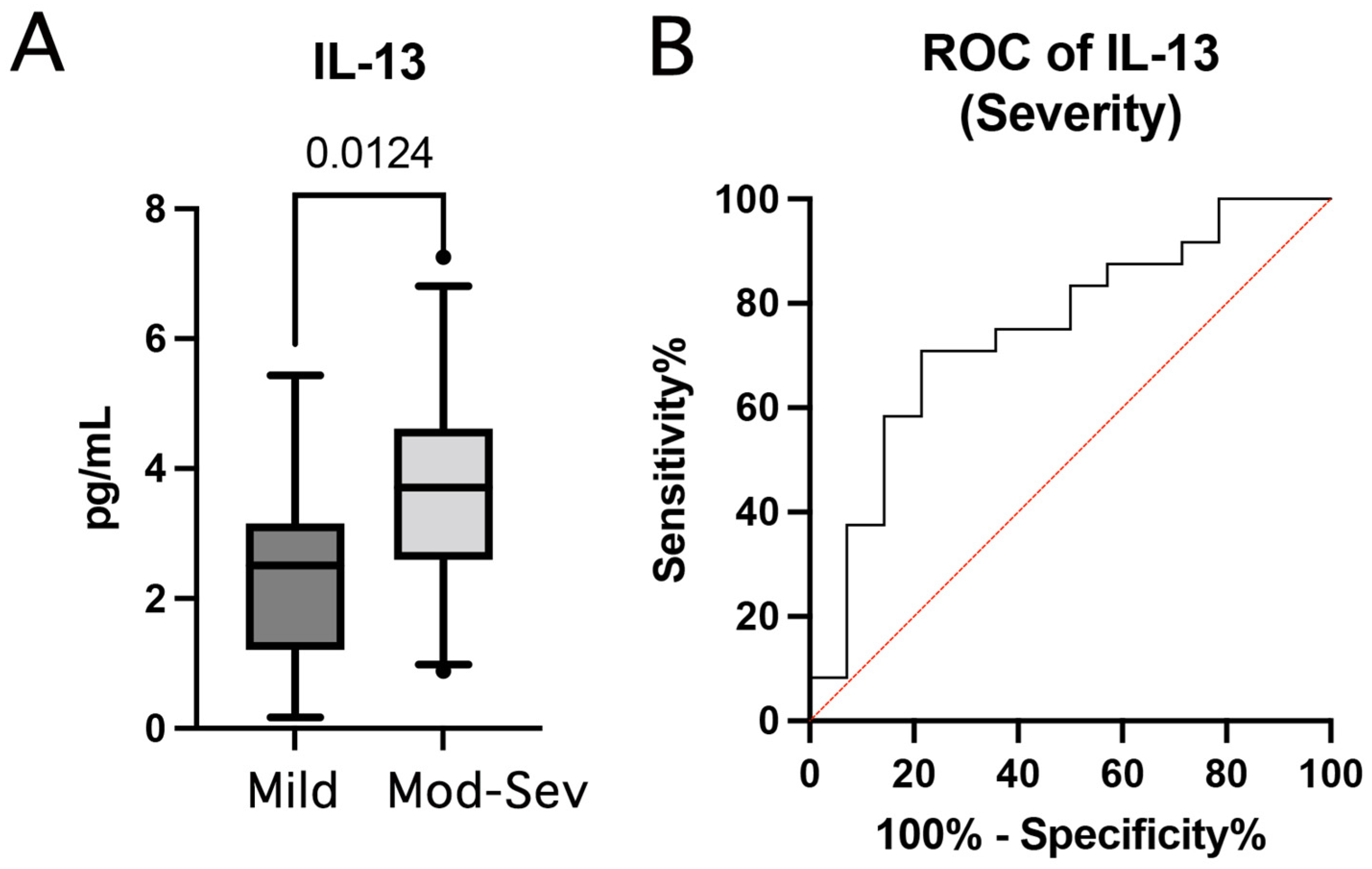
2.4. Inflammatory Biomarkers of Injury Severity
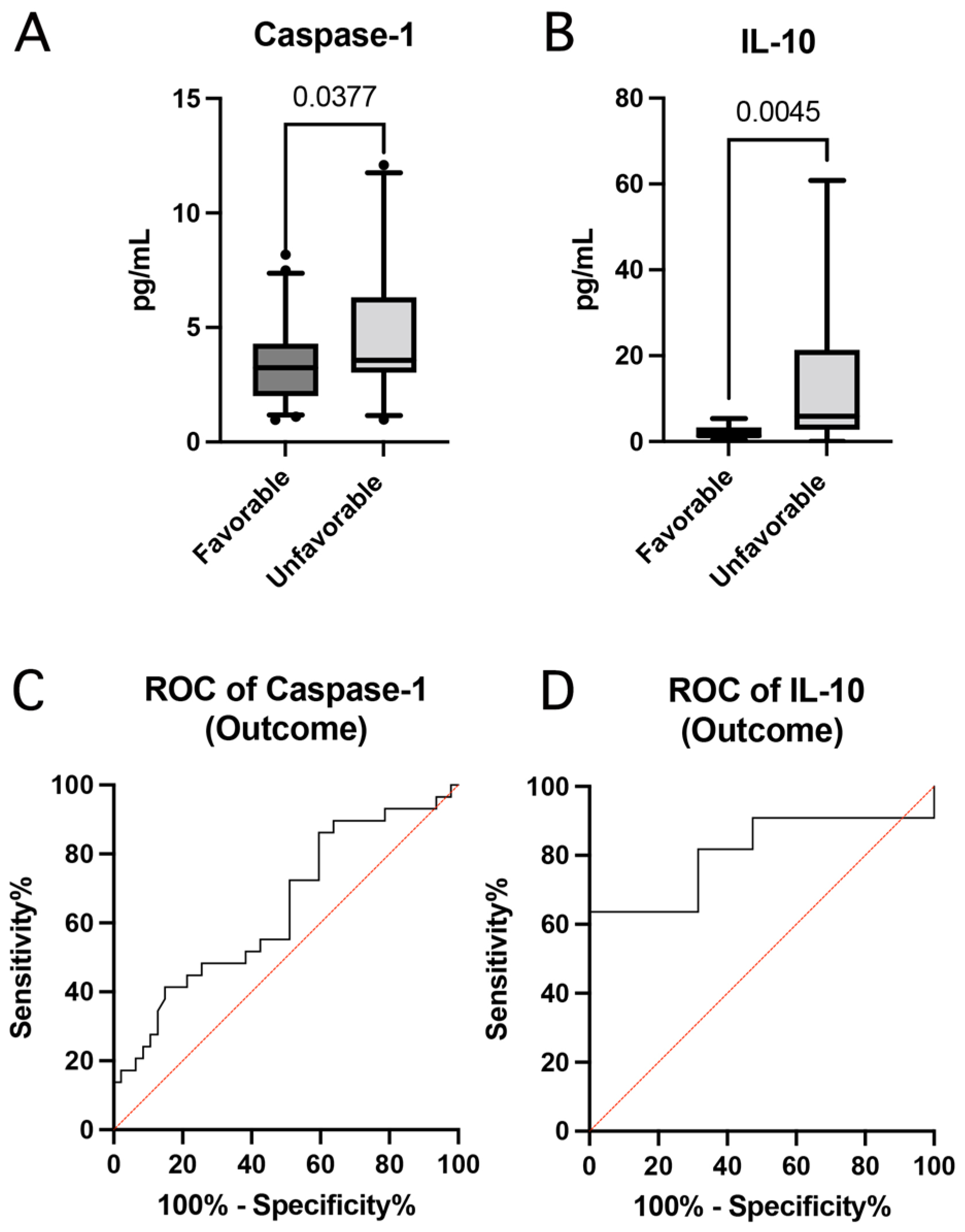
2.5. Inflammatory Biomarkers of Outcome
3. Discussion
4. Materials and Methods
4.1. Participants
4.2. Data Collection
4.3. Simple Plex Assay
4.4. MSD V-PLEX Inflammatory Panel
4.5. Statistical & Biomarker Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bachynski, K.E.; Goldberg, D.S. Youth sports & public health: Framing risks of mild traumatic brain injury in american football and ice hockey. J. Law Med. Ethics 2014, 42, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Dams-O’Connor, K.; Cantor, J.B.; Brown, M.; Dijkers, M.P.; Spielman, L.A.; Gordon, W.A. Screening for traumatic brain injury: Findings and public health implications. J. Head Traum. Rehabil. 2014, 29, 479–489. [Google Scholar] [CrossRef] [PubMed]
- Othman, H.; Ludin, S.M.; Saidi, S.; Awang, M.S. The needs of traumatic brain injury survivors’ caregivers and the implication required during the COVID-19 pandemic: Public health issues. J. Public Health Res. 2021, 10, 2205. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.E. Traumatic brain injury in older adults: Shining light on a growing public health crisis. Int. Rev. Psychiatry 2020, 32, 1–2. [Google Scholar] [CrossRef]
- Waltzman, D.; Haarbauer-Krupa, J.; Womack, L.S. Traumatic Brain Injury in Older Adults-A Public Health Perspective. JAMA Neurol. 2022, 79, 437–438. [Google Scholar] [CrossRef]
- Titus, D.J.; Johnstone, T.; Johnson, N.H.; London, S.H.; Chapalamadugu, M.; Hogenkamp, D.; Gee, K.W.; Atkins, C.M. Positive allosteric modulation of the alpha7 nicotinic acetylcholine receptor as a treatment for cognitive deficits after traumatic brain injury. PLoS ONE 2019, 14, e0223180. [Google Scholar] [CrossRef] [Green Version]
- Lassaren, P.; Lindblad, C.; Frostell, A.; Carpenter, K.L.H.; Guilfoyle, M.R.; Hutchinson, P.J.A.; Helmy, A.; Thelin, E.P. Systemic inflammation alters the neuroinflammatory response: A prospective clinical trial in traumatic brain injury. J. Neuroinflamm. 2021, 18, 221. [Google Scholar] [CrossRef]
- Risbrough, V.B.; Vaughn, M.N.; Friend, S.F. Role of Inflammation in Traumatic Brain Injury-Associated Risk for Neuropsychiatric Disorders: State of the Evidence and Where Do We Go From Here. Biol. Psychiatry 2022, 91, 438–448. [Google Scholar] [CrossRef]
- Visser, K.; Koggel, M.; Blaauw, J.; van der Horn, H.J.; Jacobs, B.; van der Naalt, J. Blood-based biomarkers of inflammation in mild traumatic brain injury: A systematic review. Neurosci. Biobehav. Rev. 2022, 132, 154–168. [Google Scholar] [CrossRef]
- Xu, W.; Yue, S.; Wang, P.; Wen, B.; Zhang, X. Systemic inflammation in traumatic brain injury predicts poor cognitive function. Immun. Inflamm. Dis. 2022, 10, e577. [Google Scholar] [CrossRef]
- Irrera, N.; Russo, M.; Pallio, G.; Bitto, A.; Mannino, F.; Minutoli, L.; Altavilla, D.; Squadrito, F. The Role of NLRP3 Inflammasome in the Pathogenesis of Traumatic Brain Injury. Int. J. Mol. Sci. 2020, 21, 6204. [Google Scholar] [CrossRef]
- Ismael, S.; Ahmed, H.A.; Adris, T.; Parveen, K.; Thakor, P.; Ishrat, T. The NLRP3 inflammasome: A potential therapeutic target for traumatic brain injury. Neural. Regen. Res. 2021, 16, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Mortezaee, K.; Khanlarkhani, N.; Beyer, C.; Zendedel, A. Inflammasome: Its role in traumatic brain and spinal cord injury. J. Cell Physiol. 2018, 233, 5160–5169. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, W.T.; Pham, L.; Symons, G.F.; Monif, M.; Shultz, S.R.; McDonald, S.J. The NLRP3 inflammasome in traumatic brain injury: Potential as a biomarker and therapeutic target. J. Neuroinflamm. 2020, 17, 104. [Google Scholar] [CrossRef] [PubMed]
- Kumar, R.G.; Boles, J.A.; Wagner, A.K. Chronic Inflammation After Severe Traumatic Brain Injury: Characterization and Associations with Outcome at 6 and 12 Months Postinjury. J. Head Traum. Rehabil. 2015, 30, 369–381. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Niu, X.; Bai, L.; Sun, Y.; Wang, Y.; Bai, G.; Yin, B.; Wang, S.; Gan, S.; Jia, X.; Liu, H. Mild traumatic brain injury is associated with effect of inflammation on structural changes of default mode network in those developing chronic pain. J. Headache Pain 2020, 21, 135. [Google Scholar] [CrossRef] [PubMed]
- Witcher, K.G.; Bray, C.E.; Chunchai, T.; Zhao, F.; O’Neil, S.M.; Gordillo, A.J.; Campbell, W.A.; McKim, D.B.; Liu, X.; Dziabis, J.E.; et al. Traumatic Brain Injury Causes Chronic Cortical Inflammation and Neuronal Dysfunction Mediated by Microglia. J. Neurosci. 2021, 41, 1597–1616. [Google Scholar] [CrossRef]
- Kamajaya, L.J.; Boucher, D. Gasdermin D Cleavage Assay Following Inflammasome Activation. Methods Mol. Biol. 2022, 2459, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Kayagaki, N.; Stowe, I.B.; Lee, B.L.; O’Rourke, K.; Anderson, K.; Warming, S.; Cuellar, T.; Haley, B.; Roose-Girma, M.; Phung, Q.T.; et al. Caspase-11 cleaves gasdermin D for non-canonical inflammasome signalling. Nature 2015, 526, 666–671. [Google Scholar] [CrossRef]
- Liu, X.; Zhang, Z.; Ruan, J.; Pan, Y.; Magupalli, V.G.; Wu, H.; Lieberman, J. Inflammasome-activated gasdermin D causes pyroptosis by forming membrane pores. Nature 2016, 535, 153–158. [Google Scholar] [CrossRef] [Green Version]
- Mascarenhas, D.P.A.; Cerqueira, D.M.; Pereira, M.S.F.; Castanheira, F.V.S.; Fernandes, T.D.; Manin, G.Z.; Cunha, L.D.; Zamboni, D.S. Inhibition of caspase-1 or gasdermin-D enable caspase-8 activation in the Naip5/NLRC4/ASC inflammasome. PLoS Pathog. 2017, 13, e1006502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, K.K.; Yang, Z.; Zhu, T.; Shi, Y.; Rubenstein, R.; Tyndall, J.A.; Manley, G.T. An update on diagnostic and prognostic biomarkers for traumatic brain injury. Expert. Rev. Mol. Diagn. 2018, 18, 165–180. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.; Sun, J.; Meng, X. Pyroptosis by caspase-11 inflammasome-Gasdermin D pathway in autoimmune diseases. Pharmacol. Res. 2021, 165, 105408. [Google Scholar] [CrossRef] [PubMed]
- Adamczak, S.; Dale, G.; de Rivero Vaccari, J.P.; Bullock, M.R.; Dietrich, W.D.; Keane, R.W. Inflammasome proteins in cerebrospinal fluid of brain-injured patients as biomarkers of functional outcome: Clinical article. J. Neurosurg. 2012, 117, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- de Rivero Vaccari, J.P.; Lotocki, G.; Alonso, O.F.; Bramlett, H.M.; Dietrich, W.D.; Keane, R.W. Therapeutic neutralization of the NLRP1 inflammasome reduces the innate immune response and improves histopathology after traumatic brain injury. J. Cereb. Blood Flow Metab. 2009, 29, 1251–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kerr, N.; Lee, S.W.; Perez-Barcena, J.; Crespi, C.; Ibanez, J.; Bullock, M.R.; Dietrich, W.D.; Keane, R.W.; de Rivero Vaccari, J.P. Inflammasome proteins as biomarkers of traumatic brain injury. PLoS ONE 2018, 13, e0210128. [Google Scholar] [CrossRef] [PubMed]
- de Rivero Vaccari, J.P.; Dietrich, W.D.; Keane, R.W. Therapeutics targeting the inflammasome after central nervous system injury. Transl. Res. 2016, 167, 35–45. [Google Scholar] [CrossRef] [Green Version]
- Diaz-Parga, P.; de Alba, E. Inflammasome regulation by adaptor isoforms, ASC and ASCb, via differential self-assembly. J. Biol. Chem. 2022, 298, 101566. [Google Scholar] [CrossRef]
- Li, S.; Wang, L.; Xu, Z.; Huang, Y.; Xue, R.; Yue, T.; Xu, L.; Gong, F.; Bai, S.; Wu, Q.; et al. ASC deglutathionylation is a checkpoint for NLRP3 inflammasome activation. J. Exp. Med. 2021, 218, e20202637. [Google Scholar] [CrossRef]
- Nagar, A.; Rahman, T.; Harton, J.A. The ASC Speck and NLRP3 Inflammasome Function Are Spatially and Temporally Distinct. Front. Immunol. 2021, 12, 752482. [Google Scholar] [CrossRef]
- Wittmann, N.; Behrendt, A.K.; Mishra, N.; Bossaller, L.; Meyer-Bahlburg, A. Instructions for Flow Cytometric Detection of ASC Specks as a Readout of Inflammasome Activation in Human Blood. Cells 2021, 10, 2880. [Google Scholar] [CrossRef] [PubMed]
- Tsuchiya, K.; Hara, H.; Fang, R.; Hernandez-Cuellar, E.; Sakai, S.; Daim, S.; Chen, X.; Dewamitta, S.R.; Qu, H.; Mitsuyama, M.; et al. The adaptor ASC exacerbates lethal Listeria monocytogenes infection by mediating IL-18 production in an inflammasome-dependent and -independent manner. Eur. J. Immunol. 2014, 44, 3696–3707. [Google Scholar] [CrossRef] [PubMed]
- Clark, A.L.; Sorg, S.F.; Schiehser, D.M.; Bigler, E.D.; Bondi, M.W.; Jacobson, M.W.; Jak, A.J.; Delano-Wood, L. White Matter Associations with Performance Validity Testing in Veterans with Mild Traumatic Brain Injury: The Utility of Biomarkers in Complicated Assessment. J. Head Traum. Rehabil. 2016, 31, 346–359. [Google Scholar] [CrossRef] [PubMed]
- Di Battista, A.P.; Buonora, J.E.; Rhind, S.G.; Hutchison, M.G.; Baker, A.J.; Rizoli, S.B.; Diaz-Arrastia, R.; Mueller, G.P. Blood Biomarkers in Moderate-To-Severe Traumatic Brain Injury: Potential Utility of a Multi-Marker Approach in Characterizing Outcome. Front Neurol. 2015, 6, 110. [Google Scholar] [CrossRef]
- Huibregtse, M.E.; Bazarian, J.J.; Shultz, S.R.; Kawata, K. The biological significance and clinical utility of emerging blood biomarkers for traumatic brain injury. Neurosci. Biobehav. Rev. 2021, 130, 433–447. [Google Scholar] [CrossRef]
- Lewis, L.M.; Schloemann, D.T.; Papa, L.; Fucetola, R.P.; Bazarian, J.; Lindburg, M.; Welch, R.D. Utility of Serum Biomarkers in the Diagnosis and Stratification of Mild Traumatic Brain Injury. Acad Emerg. Med. 2017, 24, 710–720. [Google Scholar] [CrossRef] [Green Version]
- Lifshitz, J.; Rowe, R.K.; Griffiths, D.R.; Evilsizor, M.N.; Thomas, T.C.; Adelson, P.D.; McIntosh, T.K. Clinical relevance of midline fluid percussion brain injury: Acute deficits, chronic morbidities and the utility of biomarkers. Brain Inj. 2016, 30, 1293–1301. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Rodriguez, A.; Egea-Guerrero, J.J. The utility of biomarkers in traumatic brain injury clinical management. Crit. Care 2016, 20, 376. [Google Scholar] [CrossRef] [Green Version]
- Strathmann, F.G.; Schulte, S.; Goerl, K.; Petron, D.J. Blood-based biomarkers for traumatic brain injury: Evaluation of research approaches, available methods and potential utility from the clinician and clinical laboratory perspectives. Clin. Biochem. 2014, 47, 876–888. [Google Scholar] [CrossRef]
- Al-Adli, N.; Akbik, O.S.; Rail, B.; Montgomery, E.; Caldwell, C.; Barrie, U.; Vira, S.; Al Tamimi, M.; Bagley, C.A.; Aoun, S.G. The Clinical Use of Serum Biomarkers in Traumatic Brain Injury: A Systematic Review Stratified by Injury Severity. World Neurosurg. 2021, 155, e418–e438. [Google Scholar] [CrossRef]
- Anada, R.P.; Wong, K.T.; Jayapalan, J.J.; Hashim, O.H.; Ganesan, D. Panel of serum protein biomarkers to grade the severity of traumatic brain injury. Electrophoresis 2018, 39, 2308–2315. [Google Scholar] [CrossRef] [PubMed]
- Carabias, C.S.; Gomez, P.A.; Panero, I.; Eiriz, C.; Castano-Leon, A.M.; Egea, J.; Lagares, A. i+12 Neurotraumatology Group, C. Chitinase-3-Like Protein 1, Serum Amyloid A1, C-Reactive Protein, and Procalcitonin Are Promising Biomarkers for Intracranial Severity Assessment of Traumatic Brain Injury: Relationship with Glasgow Coma Scale and Computed Tomography Volumetry. World Neurosurg. 2020, 134, e120–e143. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.; Cao, H.L.; Chen, S.W.; Guo, Y.; Gao, W.W.; Tian, H.L.; Xue, L.X. Neuroglobin and Nogo-a as biomarkers for the severity and prognosis of traumatic brain injury. Biomarkers 2015, 20, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Czeiter, E.; Amrein, K.; Gravesteijn, B.Y.; Lecky, F.; Menon, D.K.; Mondello, S.; Newcombe, V.F.J.; Richter, S.; Steyerberg, E.W.; Vyvere, T.V.; et al. Blood biomarkers on admission in acute traumatic brain injury: Relations to severity, CT findings and care path in the CENTER-TBI study. EBioMedicine 2020, 56, 102785. [Google Scholar] [CrossRef]
- Sharma, S.; Kumar, A.; Choudhary, A.; Sharma, S.; Khurana, L.; Sharma, N.; Kumar, V.; Bisht, A. Neuroprotective Role of Oral Vitamin D Supplementation on Consciousness and Inflammatory Biomarkers in Determining Severity Outcome in Acute Traumatic Brain Injury Patients: A Double-Blind Randomized Clinical Trial. Clin. Drug Investig. 2020, 40, 327–334. [Google Scholar] [CrossRef]
- Zoltewicz, J.S.; Mondello, S.; Yang, B.; Newsom, K.J.; Kobeissy, F.; Yao, C.; Lu, X.C.; Dave, J.R.; Shear, D.A.; Schmid, K.; et al. Biomarkers track damage after graded injury severity in a rat model of penetrating brain injury. J. Neurotraum. 2013, 30, 1161–1169. [Google Scholar] [CrossRef]
- Harting, M.T.; Jimenez, F.; Adams, S.D.; Mercer, D.W.; Cox, C.S., Jr. Acute, regional inflammatory response after traumatic brain injury: Implications for cellular therapy. Surgery 2008, 144, 803–813. [Google Scholar] [CrossRef] [Green Version]
- Mautes, A.E.; Fukuda, K.; Noble, L.J. Cellular response in the cerebellum after midline traumatic brain injury in the rat. Neurosci. Lett. 1996, 214, 95–98. [Google Scholar] [CrossRef]
- Anderson, T.N.; Hinson, H.E. Damaged: Elevated GFAP and UCH-L1 as the Black Flag of Brain Injury. Resuscitation 2020, 154, 110–111. [Google Scholar] [CrossRef]
- Middleton, J. UCH-L1 and GFAP Testing (i-STAT TBI Plasma) for the Detection of Intracranial Injury Following Mild Traumatic Brain Injury. Am. Fam. Physician 2022, 105, 313–314. [Google Scholar]
- Papa, L.; Brophy, G.M.; Welch, R.D.; Lewis, L.M.; Braga, C.F.; Tan, C.N.; Ameli, N.J.; Lopez, M.A.; Haeussler, C.A.; Mendez Giordano, D.I.; et al. Time Course and Diagnostic Accuracy of Glial and Neuronal Blood Biomarkers GFAP and UCH-L1 in a Large Cohort of Trauma Patients with and without Mild Traumatic Brain Injury. JAMA Neurol. 2016, 73, 551–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papa, L.; Zonfrillo, M.R.; Welch, R.D.; Lewis, L.M.; Braga, C.F.; Tan, C.N.; Ameli, N.J.; Lopez, M.A.; Haeussler, C.A.; Mendez Giordano, D.; et al. Evaluating glial and neuronal blood biomarkers GFAP and UCH-L1 as gradients of brain injury in concussive, subconcussive and non-concussive trauma: A prospective cohort study. BMJ Paediatr. Open 2019, 3, e000473. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhine, T.; Babcock, L.; Zhang, N.; Leach, J.; Wade, S.L. Are UCH-L1 and GFAP promising biomarkers for children with mild traumatic brain injury? Brain Inj. 2016, 30, 1231–1238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shahim, P.; Politis, A.; van der Merwe, A.; Moore, B.; Ekanayake, V.; Lippa, S.M.; Chou, Y.Y.; Pham, D.L.; Butman, J.A.; Diaz-Arrastia, R.; et al. Time course and diagnostic utility of NfL, tau, GFAP, and UCH-L1 in subacute and chronic TBI. Neurology 2020, 95, e623–e636. [Google Scholar] [CrossRef]
- Yang, Z.; Xu, H.; Sura, L.; Arja, R.D.; Patterson, R.L.; Rossignol, C.; Albayram, M.; Rajderkar, D.; Ghosh, S.; Wang, K.; et al. Combined GFAP, NFL, Tau, and UCH-L1 panel increases prediction of outcomes in neonatal encephalopathy. Pediatr. Res. 2022. Online ahead of print. [Google Scholar] [CrossRef]
- Diaz-Arrastia, R.; Wang, K.K.; Papa, L.; Sorani, M.D.; Yue, J.K.; Puccio, A.M.; McMahon, P.J.; Inoue, T.; Yuh, E.L.; Lingsma, H.F.; et al. Acute biomarkers of traumatic brain injury: Relationship between plasma levels of ubiquitin C-terminal hydrolase-L1 and glial fibrillary acidic protein. J. Neurotraum. 2014, 31, 19–25. [Google Scholar] [CrossRef]
- Perez-Barcena, J.; Crespi, C.; Frontera, G.; Llompart-Pou, J.A.; Salazar, O.; Goliney, V.; Ibanez, J.; Bullock, M.R.; de Rivero Vaccari, J.P. Levels of caspase-1 in cerebrospinal fluid of patients with traumatic brain injury: Correlation with intracranial pressure and outcome. J. Neurosurg. 2020, 134, 1644–1649. [Google Scholar] [CrossRef]
- Csuka, E.; Morganti-Kossmann, M.C.; Lenzlinger, P.M.; Joller, H.; Trentz, O.; Kossmann, T. IL-10 levels in cerebrospinal fluid and serum of patients with severe traumatic brain injury: Relationship to IL-6, TNF-alpha, TGF-beta1 and blood-brain barrier function. J. Neuroimmunol. 1999, 101, 211–221. [Google Scholar] [CrossRef]
- Ross, S.A.; Halliday, M.I.; Campbell, G.C.; Byrnes, D.P.; Rowlands, B.J. The presence of tumour necrosis factor in CSF and plasma after severe head injury. Br. J. Neurosurg. 1994, 8, 419–425. [Google Scholar] [CrossRef]
- Tobinick, E.; Kim, N.M.; Reyzin, G.; Rodriguez-Romanacce, H.; DePuy, V. Selective TNF inhibition for chronic stroke and traumatic brain injury: An observational study involving 629 consecutive patients treated with perispinal etanercept. CNS Drugs 2012, 26, 1051–1070. [Google Scholar] [CrossRef]
- Aisiku, I.P.; Yamal, J.M.; Doshi, P.; Benoit, J.S.; Gopinath, S.; Goodman, J.C.; Robertson, C.S. Plasma cytokines IL-6, IL-8, and IL-10 are associated with the development of acute respiratory distress syndrome in patients with severe traumatic brain injury. Crit. Care 2016, 20, 288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kossmann, T.; Stahel, P.F.; Lenzlinger, P.M.; Redl, H.; Dubs, R.W.; Trentz, O.; Schlag, G.; Morganti-Kossmann, M.C. Interleukin-8 released into the cerebrospinal fluid after brain injury is associated with blood-brain barrier dysfunction and nerve growth factor production. J. Cereb. Blood Flow Metab. 1997, 17, 280–289. [Google Scholar] [CrossRef] [PubMed]
- Rhodes, J.; Sharkey, J.; Andrews, P. Serum IL-8 and MCP-1 concentration do not identify patients with enlarging contusions after traumatic brain injury. J. Traum. 2009, 66, 1591–1597. [Google Scholar] [CrossRef] [PubMed]
- Timmerman, K.L.; Amonette, W.E.; Markofski, M.M.; Ansinelli, H.A.; Gleason, E.A.; Rasmussen, B.B.; Mossberg, K.A. Blunted IL-6 and IL-10 response to maximal aerobic exercise in patients with traumatic brain injury. Eur. J. Appl. Physiol. 2015, 115, 111–118. [Google Scholar] [CrossRef]
- Dalla Libera, A.L.; Regner, A.; de Paoli, J.; Centenaro, L.; Martins, T.T.; Simon, D. IL-6 polymorphism associated with fatal outcome in patients with severe traumatic brain injury. Brain Inj. 2011, 25, 365–369. [Google Scholar] [CrossRef] [PubMed]
- Kerr, N.; Garcia-Contreras, M.; Abbassi, S.; Mejias, N.H.; Desousa, B.R.; Ricordi, C.; Dietrich, W.D.; Keane, R.W.; de Rivero Vaccari, J.P. Inflammasome Proteins in Serum and Serum-Derived Extracellular Vesicles as Biomarkers of Stroke. Front Mol. Neurosci. 2018, 11, 309. [Google Scholar] [CrossRef] [Green Version]
- Scott, X.O.; Stephens, M.E.; Desir, M.C.; Dietrich, W.D.; Keane, R.W.; de Rivero Vaccari, J.P. The Inflammasome Adaptor Protein ASC in Mild Cognitive Impairment and Alzheimer’s Disease. Int. J. Mol. Sci. 2020, 21, 4674. [Google Scholar] [CrossRef]
- Keane, R.W.; Dietrich, W.D.; de Rivero Vaccari, J.P. Inflammasome Proteins As Biomarkers of Multiple Sclerosis. Front Neurol. 2018, 9, 135. [Google Scholar] [CrossRef]
- Weaver, C.; Cyr, B.; de Rivero Vaccari, J.C.; de Rivero Vaccari, J.P. Inflammasome Proteins as Inflammatory Biomarkers of Age-Related Macular Degeneration. Transl. Vis. Sci. Technol. 2020, 9, 27. [Google Scholar] [CrossRef]
- Forouzandeh, M.; Besen, J.; Keane, R.W.; de Rivero Vaccari, J.P. The Inflammasome Signaling Proteins ASC and IL-18 as Biomarkers of Psoriasis. Front Pharmacol. 2020, 11, 1238. [Google Scholar] [CrossRef]
- Cyr, B.; Keane, R.W.; de Rivero Vaccari, J.P. ASC, IL-18 and Galectin-3 as Biomarkers of Non-Alcoholic Steatohepatitis: A Proof of Concept Study. Int. J. Mol. Sci. 2020, 21, 8580. [Google Scholar] [CrossRef] [PubMed]
- de Rivero Vaccari, J.C.; Brand, F.J., 3rd; Berti, A.F.; Alonso, O.F.; Bullock, M.R.; de Rivero Vaccari, J.P. Mincle signaling in the innate immune response after traumatic brain injury. J. Neurotraum. 2015, 32, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Woodcock, T.; Morganti-Kossmann, M.C. The role of markers of inflammation in traumatic brain injury. Front Neurol. 2013, 4, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xia, J.; Broadhurst, D.I.; Wilson, M.; Wishart, D.S. Translational biomarker discovery in clinical metabolomics: An introductory tutorial. Metabolomics 2013, 9, 280–299. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia, J.M.; Stillings, S.A.; Leclerc, J.L.; Phillips, H.; Edwards, N.J.; Robicsek, S.A.; Hoh, B.L.; Blackburn, S.; Dore, S. Role of Interleukin-10 in Acute Brain Injuries. Front. Neurol. 2017, 8, 244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhu, H.; Hu, S.; Li, Y.; Sun, Y.; Xiong, X.; Hu, X.; Chen, J.; Qiu, S. Interleukins and Ischemic Stroke. Front. Immunol. 2022, 13, 828447. [Google Scholar] [CrossRef] [PubMed]
- Alam, A.; Thelin, E.P.; Tajsic, T.; Khan, D.Z.; Khellaf, A.; Patani, R.; Helmy, A. Cellular infiltration in traumatic brain injury. J. Neuroinflamm. 2020, 17, 328. [Google Scholar] [CrossRef]
- Rodney, T.; Osier, N.; Gill, J. Pro- and anti-inflammatory biomarkers and traumatic brain injury outcomes: A review. Cytokine 2018, 110, 248–256. [Google Scholar] [CrossRef]
- Miao, W.; Zhao, Y.; Huang, Y.; Chen, D.; Luo, C.; Su, W.; Gao, Y. IL-13 Ameliorates Neuroinflammation and Promotes Functional Recovery after Traumatic Brain Injury. J. Immunol. 2020, 204, 1486–1498. [Google Scholar] [CrossRef]
- Abraham, E.; Regan, R.F. The effects of hemorrhage and trauma on interleukin 2 production. Arch. Surg. 1985, 120, 1341–1344. [Google Scholar] [CrossRef]
- Fierz, W.; Bossuyt, X. Likelihood Ratio Approach and Clinical Interpretation of Laboratory Tests. Front. Immunol. 2021, 12, 655262. [Google Scholar] [CrossRef] [PubMed]
- Hanley, J.A.; McNeil, B.J. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983, 148, 839–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Biomarker | Area | Std. Error | 95% C.I. | p-Value |
|---|---|---|---|---|
| Caspase-1 | 1.0 | 0 | 1.0 to 1.0 | <0.0001 |
| ASC | 0.97 | 0.01384 | 0.9428 to 0.9971 | <0.0001 |
| IL-18 | 0.8143 | 0.04538 | 0.7254 to 0.9033 | <0.0001 |
| TNF-α | 0.9776 | 0.01963 | 0.9391 to 1.000 | <0.0001 |
| IL-6 | 1.0 | 0 | 1.0 to 1.0 | <0.0001 |
| IL-4 | 0.7945 | 0.05424 | 0.6882 to 0.9008 | 0.0001 |
| IL-10 | 0.9538 | 0.02697 | 0.9009 to 1.0 | <0.0001 |
| IL-8 | 0.9696 | 0.2115 | 0.9281 to 1.0 | <0.0001 |
| IL-2 | 0.7398 | 0.1084 | 0.5274 to 0.9522 | 0.0437 |
| IL-12 | 0.5333 | 0.07812 | 0.3802 to 0.6864 | 0.6645 |
| IL-13 | 0.5126 | 0.1093 | 0.2985 to 0.7267 | 0.8858 |
| Biomarker | Cut-Off Point (pg/mL) | Sensitivity (%) | Specificity (%) | LR | PPV (%) | NPV (%) | Accuracy (%) |
|---|---|---|---|---|---|---|---|
| Caspase-1 | >0.8150 | 100 | 100 | 100 | 100 | 100 | |
| ASC | >284 | 92 | 93 | 12.92 | 98 | 79 | 92 |
| IL-18 | >156 | 83 | 74 | 3.229 | 90 | 61 | 81 |
| TNF-α | >2.202 | 96 | 95 | 20.18 | 98 | 91 | 96 |
| IL-6 | >6.443 | 100 | 100 | 100 | 100 | 100 | |
| IL-4 | >0.03868 | 74 | 75 | 2.96 | 88 | 54 | 74 |
| IL-10 | >0.6527 | 88 | 100 | 100 | 79 | 92 | |
| IL-8 | >29.18 | 92 | 100 | 100 | 75 | 94 | |
| IL-2 | <0.5145 | 95 | 56 | 2.132 | 82 | 83 | 82 |
| IL-12 | <158.1 | 60 | 57 | 1.40 | 75 | 40 | 59 |
| IL-13 | >2.271 | 76 | 57 | 1.784 | 87 | 40 | 72 |
| GCS | Estimate | Std. Error | p-Value | Confidence Interval |
|---|---|---|---|---|
| Intercept | 21.245347 | 2.221427 | 0.000668 | 15.07767794 to 27.413016974 |
| IL-13 | −1.519195 | 0.332622 | 0.010282 | −2.44270084 to −0.595688402 |
| IL-12 | −0.016000 | 0.004802 | 0.029063 | −0.02933364 to −0.002666043 |
| LOG(IL-2) | 2.095605 | 0.670269 | 0.035304 | 0.23463864 to 3.956571427 |
| Adjusted R2 | 0.7798 | |||
| BIC | 35.51754 | |||
| RMSE | 1.644861 | |||
| Mean of Residuals | −6.25 × 10−17 | |||
| DW Statistic | ||||
| rho ! = 0 | p-value = 0.812 | |||
| rho < 0 | p-value = 0.443 | |||
| rho > 0 | p-value = 0.561 | |||
| GCS | Estimate | Std. Error | p-Value | Confidence Interval |
|---|---|---|---|---|
| Intercept | 9.1238 | 0.7938 | 8.74 × 10−05 | 7.0832670 to 11.1643303 |
| IL-10 | 0.2483 | 0.1416 | 0.1398 | −0.1156099 to 0.6122821 |
| LOG(Caspase-1) | −2.5997 | 0.6700 | 0.0116 | −4.3220676 to −0.8772845 |
| Adjusted R2 | 0.6524 | |||
| BIC | 24.35273 | |||
| RMSE | 0.8338086 | |||
| Mean of Residuals | 1.39 × 10−17 | |||
| DW Statistic | ||||
| rho ! = 0 | p-value = 0.574 | |||
| rho < 0 | p-value = 0.716 | |||
| rho > 0 | p-value = 0.316 | |||
| TBI (N = 93) | |
|---|---|
| Gender (n, %) | |
| Male | 74 (80%) |
| Female | 19 (20%) |
| Age (years) median (Range) | 47 (15–83) |
| Injury Mechanism (n; %) | |
| Fall | 52 (56%) |
| Assault | 5 (5%) |
| MVA | 36 (39%) |
| Glasgow Coma Scale (n; %) | |
| 3–8 | 37 (40%) |
| 9–12 | 20 (21%) |
| 13–15 | 34 (37) |
| Undetermined | 2 (2%) |
| Motor score (n; %) | |
| M6 | 38 (41%) |
| M5 | 29 (32%) |
| M4 | 4 (4%) |
| M3 | 2 (2%) |
| M2 | 1 (1%) |
| M1 | 14 (15%) |
| Undetermined | 5 (5%) |
| Pupillary Reactivity (n; %) | |
| Both reactive | 78 (84%) |
| 1 reactive | 8 (9%) |
| None reactive | 7 (7%) |
| Hospital length of stay (days) median (Range) | 13 (1–149) |
| ICU length of stay (days) median (Range) | 5 (1–90) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Johnson, N.H.; Hadad, R.; Taylor, R.R.; Rodríguez Pilar, J.; Salazar, O.; Llompart-Pou, J.A.; Dietrich, W.D.; Keane, R.W.; Pérez-Bárcena, J.; de Rivero Vaccari, J.P. Inflammatory Biomarkers of Traumatic Brain Injury. Pharmaceuticals 2022, 15, 660. https://doi.org/10.3390/ph15060660
Johnson NH, Hadad R, Taylor RR, Rodríguez Pilar J, Salazar O, Llompart-Pou JA, Dietrich WD, Keane RW, Pérez-Bárcena J, de Rivero Vaccari JP. Inflammatory Biomarkers of Traumatic Brain Injury. Pharmaceuticals. 2022; 15(6):660. https://doi.org/10.3390/ph15060660
Chicago/Turabian StyleJohnson, Nathan H., Roey Hadad, Ruby Rose Taylor, Javier Rodríguez Pilar, Osman Salazar, Juan Antonio Llompart-Pou, W. Dalton Dietrich, Robert W. Keane, Jon Pérez-Bárcena, and Juan Pablo de Rivero Vaccari. 2022. "Inflammatory Biomarkers of Traumatic Brain Injury" Pharmaceuticals 15, no. 6: 660. https://doi.org/10.3390/ph15060660