
Association between Genetic Polymorphism of GSTP1 and Toxicities in Patients Receiving Platinum-Based Chemotherapy: A Systematic Review and Meta-Analysis


Abstract
:1. Introduction
2. Methods
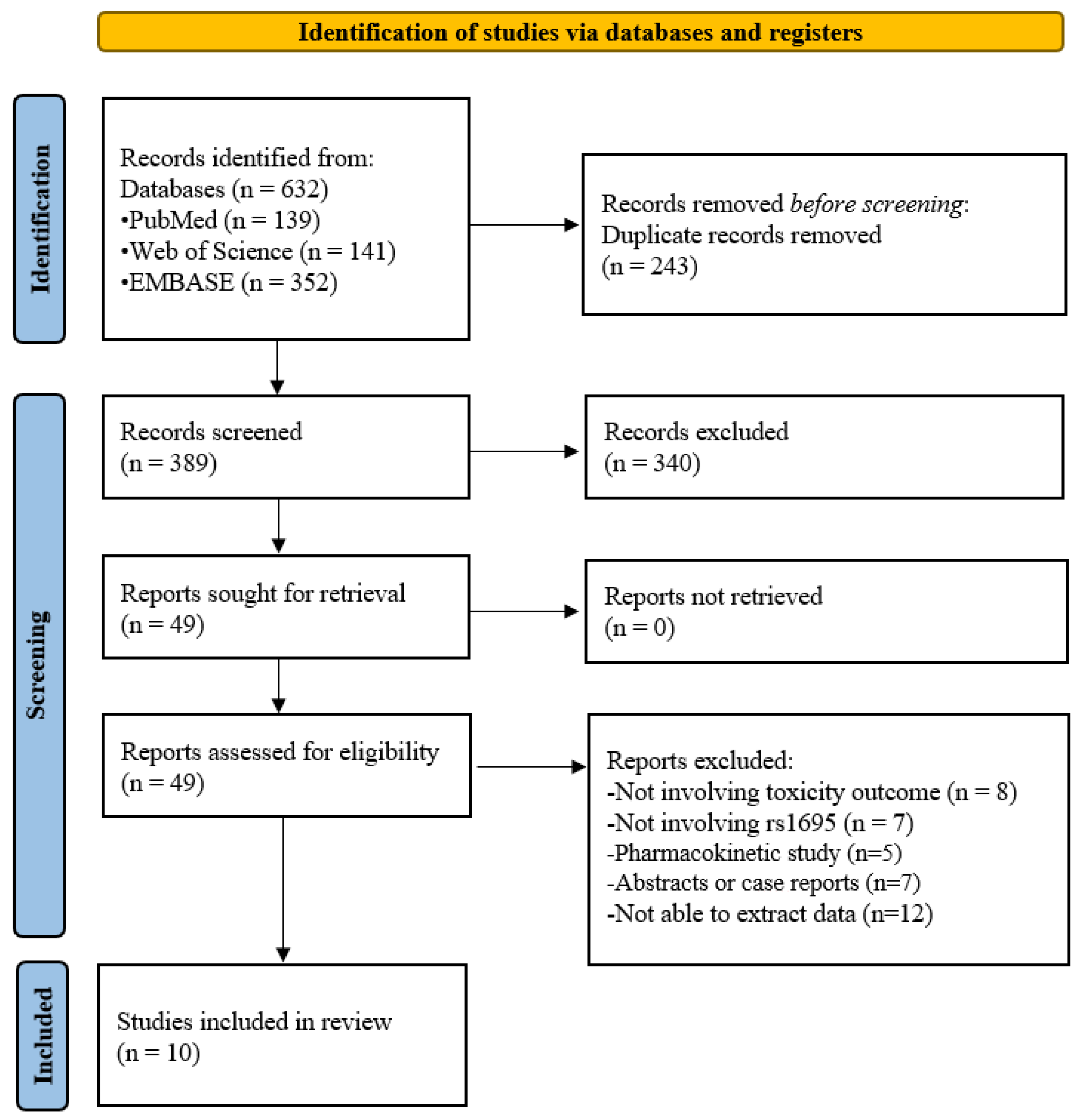
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Quality Assessment
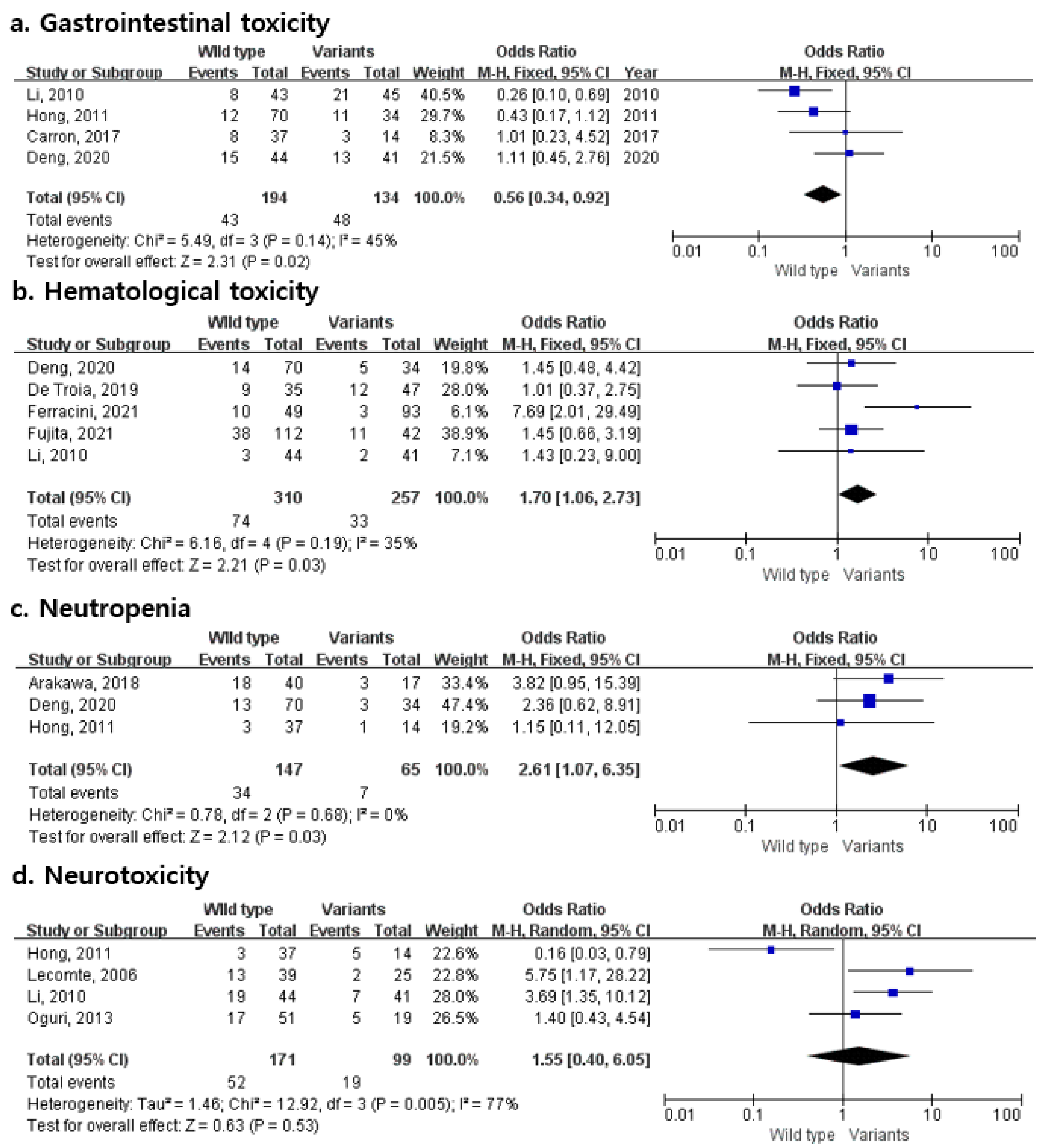
2.4. Statistical Analysis
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Johnstone, T.C.; Park, G.Y.; Lippard, S.J. Understanding and improving platinum anticancer drugs—Phenanthriplatin. Anticancer Res. 2014, 34, 471–476. [Google Scholar] [PubMed]
- Market Study Report. Platinum Based Cancer Drugs Market Size to Reach US$1.8 Billion by 2026. Available online: https://www.globenewswire.com/news-release/2020/03/25/2006050/0/en/Platinum-based-cancer-drugs-market-size-to-reach-US-1-8-billion-by-2026.html (accessed on 18 February 2022).
- Lecomte, T.; Landi, B.; Beaune, P.; Laurent-Puig, P.; Loriot, M.-A. Glutathione S-Transferase P1 Polymorphism (Ile105Val) Predicts Cumulative Neuropathy in Patients Receiving Oxaliplatin-Based Chemotherapy. Clin. Cancer Res. 2006, 12, 3050–3056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stoehlmacher, J.; Park, D.J.; Zhang, W.; Groshen, S.; Tsao-Wei, D.D.; Yu, M.C.; Lenz, H.-J. Association Between Glutathione S-Transferase P1, T1, and M1 Genetic Polymorphism and Survival of Patients With Metastatic Colorectal Cancer. JNCI J. Natl. Cancer Inst. 2002, 94, 936–942. [Google Scholar] [CrossRef] [Green Version]
- Oki, E.; Kakeji, Y.; Ohgaki, K.; Saeki, K.; Morita, M.; Emi, Y.; Maehara, Y. Impact of single nucleotide polymorphisms in glutathione S transferase gene GSTP1 in the treatment with ox-aliplatin based chemotherapy. Gan To Kagaku Ryoho 2008, 35, 1094–1096. [Google Scholar] [PubMed]
- Yadav, P.; Banerjee, A.; Boruah, N.; Singh, C.S.; Chatterjee, P.; Mukherjee, S.; Dakhar, H.; Nongrum, H.B.; Bhattacharjee, A.; Chatterjee, A. Glutathione S-transferasesP1 AA (105Ile) allele increases oral cancer risk, interacts strongly with c-Jun Kinase and weakly detoxifies areca-nut metabolites. Sci. Rep. 2020, 10, 6032. [Google Scholar] [CrossRef] [PubMed]
- Lima, C.; Carron, J.; Lopes-Aguiar, L.; Costa, E.; Nogueira, G.; Lima, T.; Pincinato, E.; Visacri, M.; Quintanilha, J.; Moriel, P.; et al. GSTP1 c.313A>G, XPD c.934G>A, XPF c.2505T>C and CASP9 c.-1339A>G polymorphisms and severity of vomiting in head and neck cancer patients treated with cisplatin chemoradiation. Ann. Oncol. 2017, 28, v388. [Google Scholar] [CrossRef]
- Arakawa, Y.; Shirai, Y.; Hayashi, K.; Tanaka, Y.; Matsumoto, A.; Nishikawa, K.; Yano, S. Effects of gene polymorphisms on the risk of severe hyponatremia during DCF chemotherapy for patients with esophageal squamous cell carcinoma. Oncol. Lett. 2018, 16, 5455–5462. [Google Scholar] [CrossRef] [Green Version]
- Wu, C.; Xu, B.; Yuan, P.; Ott, J.; Guan, Y.; Liu, Y.; Liu, Z.; Shen, Y.; Yu, D.; Lin, D. Genome-wide examination of genetic variants associated with response to platinum-based chemotherapy in patients with small-cell lung cancer. Pharm. Genom. 2010, 20, 389–395. [Google Scholar] [CrossRef]
- Chen, J.; Wang, Z.; Zou, T.; Cui, J.; Yin, J.; Zheng, W.; Jiang, W.; Zhou, H.; Liu, Z. Pharmacogenomics of platinum-based chemotherapy response in NSCLC: A genotyping study and a pooled analysis. Oncotarget 2016, 7, 55741–55756. [Google Scholar] [CrossRef] [Green Version]
- Hong, J.; Han, S.-W.; Ham, H.S.; Kim, T.-Y.; Choi, I.S.; Kim, B.-S.; Oh, D.-Y.; Im, S.-A.; Kang, G.H.; Bang, Y.-J. Phase II study of biweekly S-1 and oxaliplatin combination chemotherapy in metastatic colorectal cancer and pharmacogenetic analysis. Cancer Chemother. Pharmacol. 2011, 67, 1323–1331. [Google Scholar] [CrossRef]
- De Troia, B.; Dalu, D.; Filipazzi, V.; Isabella, L.; Tosca, N.; Ferrario, S.; Gambaro, A.R.; Somma, L.; Fasola, C.; Cheli, S.; et al. ABCB1 c.3435C>T polymorphism is associated with platinum toxicity: A preliminary study. Cancer Chemother. Pharmacol. 2019, 83, 803–808. [Google Scholar] [CrossRef] [PubMed]
- Deng, X.; Hou, J.; Deng, Q.; Zhong, Z. Predictive value of clinical toxicities of chemotherapy with fluoropyrimidines and oxaliplatin in colorectal cancer by DPYD and GSTP1 gene polymorphisms. World J. Surg. Oncol. 2020, 18, 321. [Google Scholar] [CrossRef] [PubMed]
- Ferracini, A.C.; Lopes-Aguiar, L.; Lourenço, G.J.; Yoshida, A.; Lima, C.S.P.; Sarian, L.O.; Derchain, S.; Kroetz, D.L.; Mazzola, P.G. GSTP1 and ABCB1 Polymorphisms Predicting Toxicities and Clinical Management on Carboplatin and Paclitaxel-Based Chemotherapy in Ovarian Cancer. Clin. Transl. Sci. 2021, 14, 720–728. [Google Scholar] [CrossRef]
- Fujita, K.; Motoyama, S.; Sato, Y.; Wakita, A.; Nagaki, Y.; Minamiya, Y.; Miura, M. Association between ABCC2 polymorphism and hematological toxicity in patients with esophageal cancer receiving platinum plus 5-fluorouracil therapy. Esophagus 2021, 19, 146–152. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.-F.; Yao, R.-Y.; Liu, K.-W.; Lv, H.-Y.; Jiang, T.; Liang, J. Genetic Polymorphism of GSTP1: Prediction of Clinical Outcome to Oxaliplatin/5-FU-based Chemotherapy in Advanced Gastric Cancer. J. Korean Med. Sci. 2010, 25, 846–852. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oguri, T.; Mitsuma, A.; Inada-Inoue, M.; Morita, S.; Shibata, T.; Shimokata, T.; Sugishita, M.; Nakayama, G.; Uehara, K.; Hasegawa, Y.; et al. Genetic polymorphisms associated with oxaliplatin-induced peripheral neurotoxicity in Japanese patients with colorectal cancer. Int. J. Clin. Pharmacol. Ther. 2013, 51, 475–481. [Google Scholar] [CrossRef]
- Chaney, S.G.; Campbell, S.; Bassett, E.; Wu, Y. Recognition and processing of cisplatin- and oxaliplatin-DNA adducts. Crit. Rev. Oncol. 2005, 53, 3–11. [Google Scholar] [CrossRef]
- Sedletska, Y.; Giraud-Panis, M.J.; Malinge, J.M. Cisplatin is a DNA-damaging antitumour compound triggering multifac-torial biochemical responses in cancer cells: Importance of apoptotic pathways. Curr. Med. Chem. Anticancer Agents 2005, 5, 251–265. [Google Scholar] [CrossRef]
- Dasari, S.; Tchounwou, P.B. Cisplatin in cancer therapy: Molecular mechanisms of action. Eur. J. Pharmacol. 2014, 740, 364–378. [Google Scholar] [CrossRef] [Green Version]
- Apps, M.G.; Choi, E.; Wheate, N.J. The state-of-play and future of platinum drugs. Endocr.-Relat. Cancer 2015, 22, R219–R233. [Google Scholar] [CrossRef] [Green Version]
- Townsend, D.M.; Tew, K.D. The role of glutathione-S-transferase in anti-cancer drug resistance. Oncogene 2003, 22, 7369–7375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watson, M.A.; Stewart, R.K.; Smith, G.B.; Massey, T.E.; Bell, D. Human glutathione S-transferase P1 polymorphisms: Relationship to lung tissue enzyme activity and population frequency distribution. Carcinogenesis 1998, 19, 275–280. [Google Scholar] [CrossRef] [PubMed]
- Santric, V.; Djokic, M.; Suvakov, S.; Pljesa-Ercegovac, M.; Nikitovic, M.; Radic, T.; Acimovic, M.; Stankovic, V.; Bumbasirevic, U.; Milojevic, B.; et al. GSTP1 rs1138272 Polymorphism Affects Prostate Cancer Risk. Medicina 2020, 56, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sophonnithiprasert, T.; Saelee, P.; Pongtheerat, T. Glutathione S-Transferase P1 Polymorphism on Exon 6 and Risk of Hepatocellular Carcinoma in Thai Male Patients. Oncology 2020, 98, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Mir, O.; Alexandre, J.; Tran, A.; Durand, J.-P.; Pons, G.; Treluyer, J.-M.; Goldwasser, F. Relationship between GSTP1 Ile105Val polymorphism and docetaxel-induced peripheral neuropathy: Clinical evidence of a role of oxidative stress in taxane toxicity. Ann. Oncol. 2009, 20, 736–740. [Google Scholar] [CrossRef]
- Peng, Z.; Wang, Q.; Gao, J.; Ji, Z.; Yuan, J.; Tian, Y.; Shen, L. Association between GSTP1 Ile105Val polymorphism and oxaliplatin-induced neuropathy: A systematic review and meta-analysis. Cancer Chemother. Pharmacol. 2013, 72, 305–314. [Google Scholar] [CrossRef]
- Lv, F.; Ma, Y.; Zhang, Y.; Li, Z. Relationship between GSTP1 rs1695 gene polymorphism and myelosuppression induced by platinum-based drugs: A meta-analysis. Int. J. Biol. Markers 2018, 33, 364–371. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Authors | Number of Patients | Country | Age (Range, Years) | Female | Cancer Type | Treatment Regimen | Definition of Outcome | Total NOS |
|---|---|---|---|---|---|---|---|---|
| Arakawa, 2018 [8] | 57 | Japan | 66 (45–77) | 11% | Esophageal squamous cell carcinoma | Cisplatin-based chemotherapy | CTCAE v4.0 | 7 |
| Carron, 2017 [7] | 88 | Brazil | 54 (27–66) | 8% | Head and Neck Cancer | Cisplatin-based chemotherapy | NCI criteria v4.0 | 6 |
| De Troia, 2019 [12] | 82 | Italy | Not indicated | 37% | Lung cancer | Platinum-based chemotherapy | CTCAE v4.03 | 6 |
| Deng, 2020 [13] | 104 | China | 56 (25–78) | 47% | Colorectal cancer | Oxaliplatin-based chemotherapy | NCI CTCAE v3.0 | 8 |
| Ferracini, 2021 [14] | 112 | Brazil | 58 (22–87) | 100% | Ovarian Cancer | Carboplatin-based chemotherapy | CTCAE v5.0 | 8 |
| Fujita, 2021 [15] | 239 | Japan | 64.0 (41–83) | 13% | Esophageal cancer | Platinum-based chemotherapy | CTCAE v5.0 | 7 |
| Hong, 2011 [11] | 52 | Korea | 63.0 (37–74) | 29% | Metastatic colorectal cancer | Oxaliplatin-based chemotherapy | NCI CTC v3.0 | 8 |
| Lecomte, 2006 [3] | 64 | France | 64 (24–84) | 45% | Gastrointestinal solid tumors | Oxaliplatin-based chemotherapy | Not indicated | 6 |
| Li, 2010 [16] | 89 | China | 55 (32–77) | 28% | Advanced Gastric Cancer | Oxaliplatin-based chemotherapy | NCI CTC v2.0 | 7 |
| Oguri, 2013 [17] | 70 | Japan | 65 (37–81) | 30% | Colorectal cancer | Oxaliplatin-based chemotherapy | NCI CTCAE v3.0 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, W.; Cho, Y.-A.; Kim, D.-C.; Lee, K.-E. Association between Genetic Polymorphism of GSTP1 and Toxicities in Patients Receiving Platinum-Based Chemotherapy: A Systematic Review and Meta-Analysis. Pharmaceuticals 2022, 15, 439. https://doi.org/10.3390/ph15040439
Kim W, Cho Y-A, Kim D-C, Lee K-E. Association between Genetic Polymorphism of GSTP1 and Toxicities in Patients Receiving Platinum-Based Chemotherapy: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2022; 15(4):439. https://doi.org/10.3390/ph15040439
Chicago/Turabian StyleKim, Woorim, Young-Ah Cho, Dong-Chul Kim, and Kyung-Eun Lee. 2022. "Association between Genetic Polymorphism of GSTP1 and Toxicities in Patients Receiving Platinum-Based Chemotherapy: A Systematic Review and Meta-Analysis" Pharmaceuticals 15, no. 4: 439. https://doi.org/10.3390/ph15040439