
Theranostic Nanomedicines for the Treatment of Cardiovascular and Related Diseases: Current Strategies and Future Perspectives



 ,
,  , ,
, ,  and
and 
Abstract
:
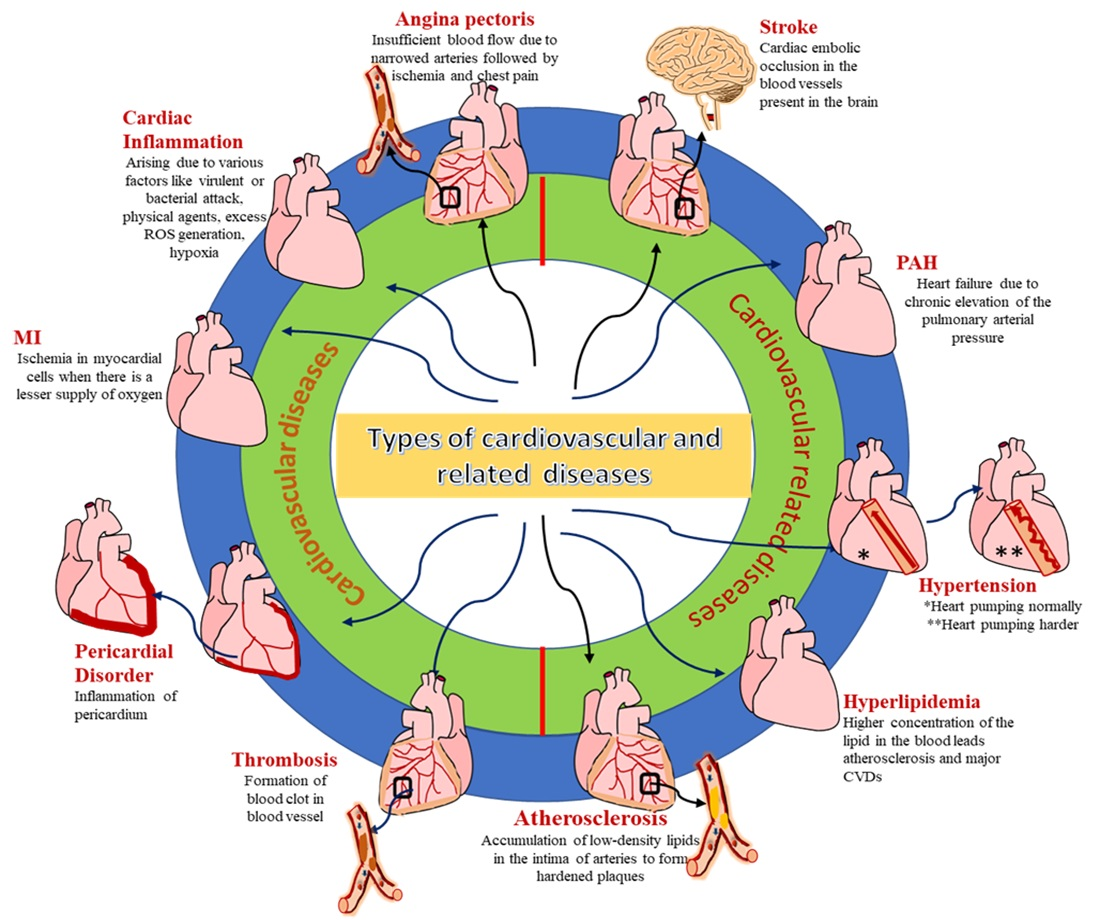
1. Introduction
2. Diagnostic Application of Targeted Nanomedicine in CVRDs
2.1. Quantum Dot-Based Imaging of CVRDs
2.2. Magnetic Nanoparticles-Based Imaging of CVRDs
2.3. Radio-Imaging of CVRDs
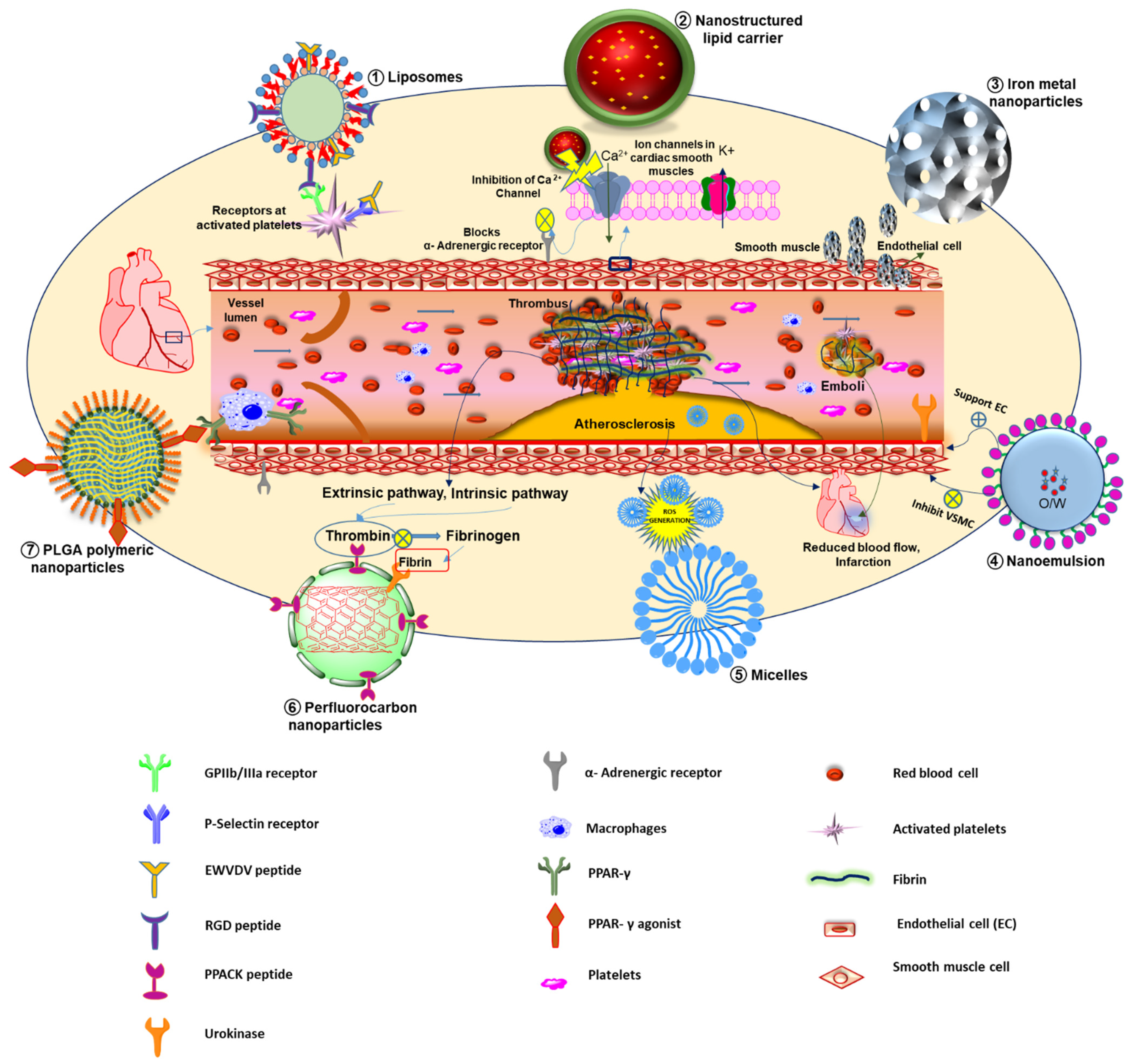
3. Therapeutic and Theranostic Applications of Targeted Nanomedicine in CVRDs
3.1. Nanomedicine as a Drug Delivery System for Cardiovascular Diseases
3.1.1. Nanomedicines for Angina Pectoris
3.1.2. Nanomedicines for Myocarditis
3.1.3. Nanomedicines for Myocardial Infarction
3.1.4. Nanomedicines for Pericardial Disorder
3.1.5. Anti-Thrombotic Nanomedicines
3.2. Nanomedicine Approach in Cardiovascular-Related Diseases
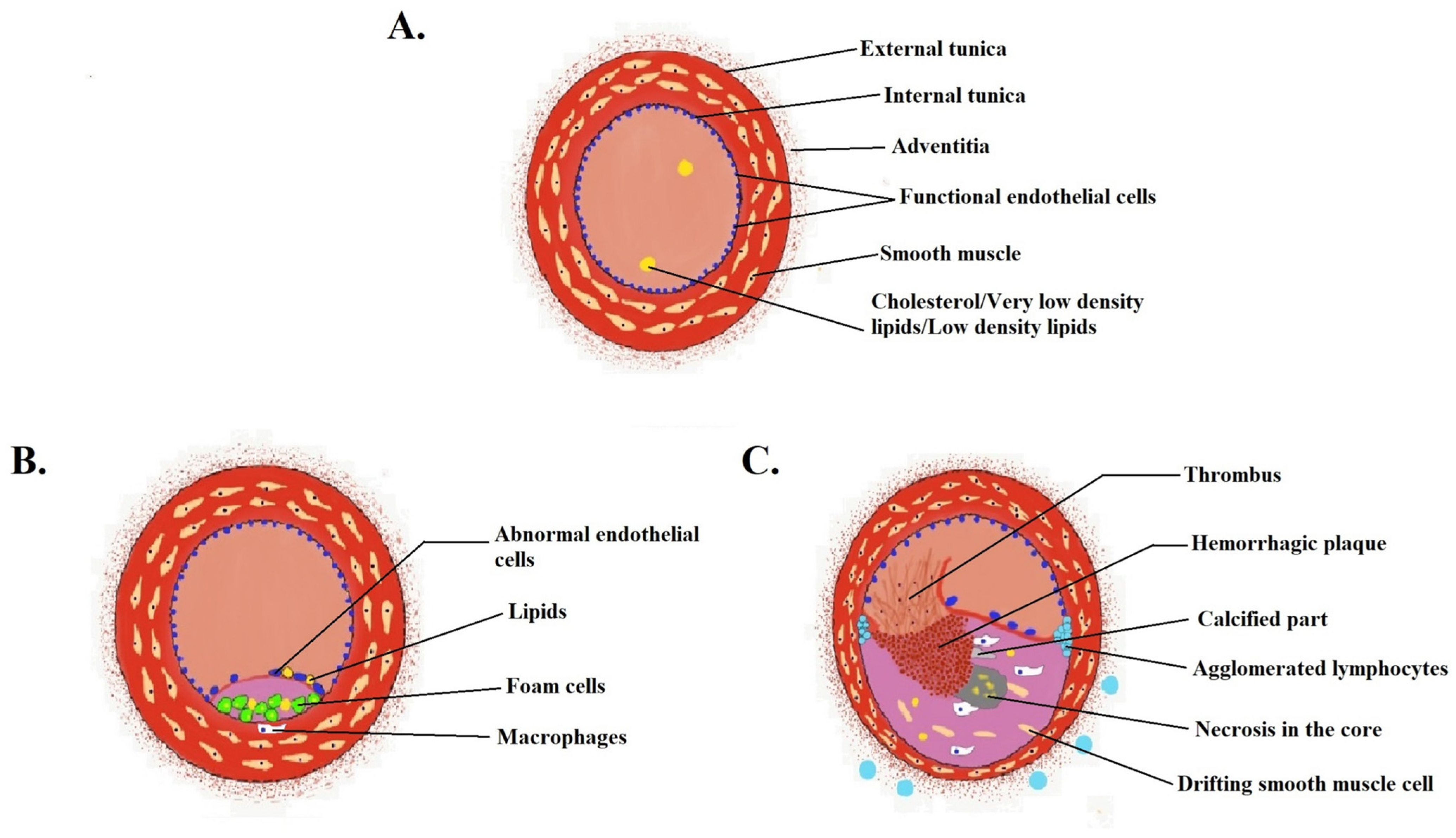
3.2.1. Anti-Atherosclerotic Nanomedicines
3.2.2. Anti-Hyperlipidemic Nanomedicines
3.2.3. Anti-Hypertensive Nanomedicines
3.2.4. Nanomedicines for Pulmonary Arterial Hypertension (PAH)
3.2.5. Nanomedicines for Stroke
4. An Update: Nanomedicine in Clinical Trials for CVRDs
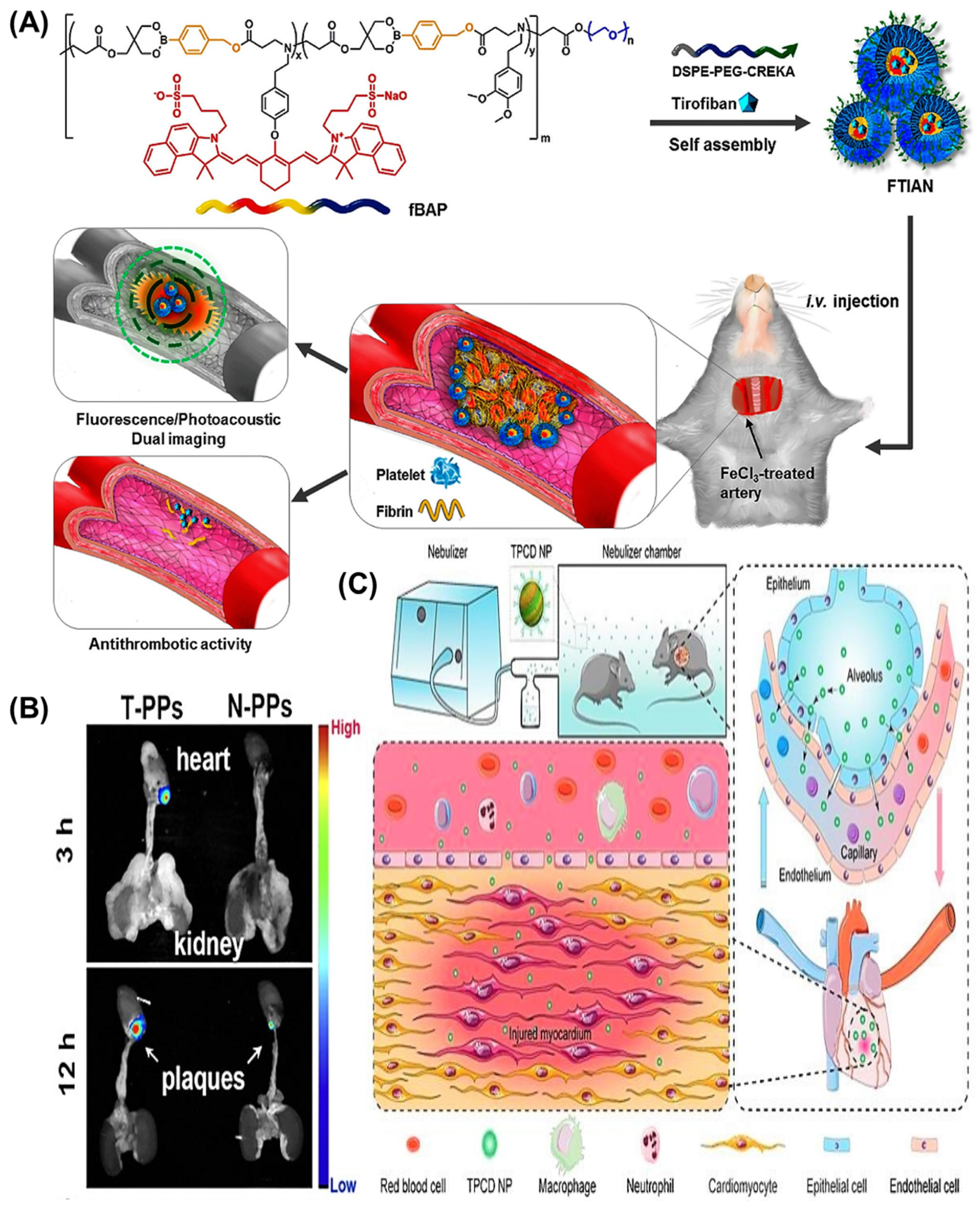
5. Latest Developments in Targeted Nanomedicines for CVRDs
6. Challenges in the Translation of Nanomedicine for CVRDs
7. Future Perspective
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gupta, A.S. Nanomedicine approaches in vascular disease: A review. Nanomedicine 2011, 7, 763–779. [Google Scholar] [CrossRef] [PubMed]
- Passaro, F.; Testa, G.; Ambrosone, L.; Costagliola, C.; Tocchetti, C.G.; di Nezza, F.; Russo, M.; Pirozzi, F.; Abete, P.; Russo, T.; et al. Nanotechnology-based cardiac targeting and direct cardiac reprogramming: The betrothed. Stem. Cells Int. 2017, 2017, 4940397. [Google Scholar] [CrossRef] [Green Version]
- Ambesh, P.; Campia, U.; Obiagwu, C.; Bansal, R.; Shetty, V.; Hollander, G.; Shani, J. Nanomedicine in coronary artery disease. Indian Heart J. 2017, 69, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update From the GBD 2019 Study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- Pala, R.; Anju, V.T.; Dyavaiah, M.; Busi, S.; Nauli, S.M. Nanoparticle-mediated drug delivery for the treatment of cardiovascular diseases. Int. J. Nanomed. 2020, 15, 3741–3769. [Google Scholar] [CrossRef]
- Chen, W.; Schilperoort, M.; Cao, Y.; Shi, J.; Tabas, I.; Tao, W. Macrophage-targeted nanomedicine for the diagnosis and treatment of atherosclerosis. Nat. Rev. Cardiol. 2022, 19, 228–249. [Google Scholar] [CrossRef]
- Godin, B.; Sakamoto, J.H.; Serda, R.E.; Grattoni, A.; Bouamrani, A.; Ferrari, M. Emerging applications of nanomedicine for the diagnosis and treatment of cardiovascular diseases. Trends Pharmacol. Sci. 2010, 31, 199–205. [Google Scholar] [CrossRef] [Green Version]
- Sonali; Viswanadh, M.K.; Singh, R.P.; Agrawal, P.; Mehata, A.K.; Pawde, D.M.; Narendra; Sonkar, R.; Muthu, M.S. Nanotheranostics: Emerging strategies for early diagnosis and therapy of brain cancer. Nanotheranostics 2018, 2, 70–86. [Google Scholar] [CrossRef]
- Rampazzo, E.; Genovese, D.; Palomba, F.; Prodi, L.; Zaccheroni, N. NIR-fluorescent dye doped silica nanoparticles for in vivo imaging, sensing and theranostic. Methods Appl. Fluoresc. 2018, 6, 022002. [Google Scholar] [CrossRef]
- Schroeder, K.L.; Goreham, R.V.; Nann, T. Graphene quantum dots for theranostics and bioimaging. Pharm. Res. 2016, 33, 2337–2357. [Google Scholar] [CrossRef]
- Dadfar, S.M.; Roemhild, K.; Drude, N.I.; von Stillfried, S.; Knüchel, R.; Kiessling, F.; Lammers, T. Iron oxide nanoparticles: Diagnostic, therapeutic and theranostic applications. Adv. Drug Deliv. Rev. 2019, 138, 302–325. [Google Scholar] [CrossRef] [PubMed]
- Choudhury, P.S.; Gupta, M. Differentiated thyroid cancer theranostics: Radioiodine and beyond. Br. J. Radiol. 2018, 91, 20180136. [Google Scholar] [CrossRef] [PubMed]
- Eilsberger, F.; Pfestroff, A. Theranostics in thyroid cancer. PET Clin. 2021, 16, 375–382. [Google Scholar] [CrossRef] [PubMed]
- Mulder, W.J.; Fayad, Z.A. Nanomedicine captures cardiovascular disease. Arterioscler. Thromb. Vasc. Biol. 2008, 28, 801–802. [Google Scholar] [CrossRef] [Green Version]
- Muthu, M.S.; Singh, S. Targeted nanomedicines: Effective treatment modalities for cancer, AIDS and brain disorders. Nanomedicine 2009, 4, 105–118. [Google Scholar] [CrossRef]
- Piras, A.M.; Chiellini, F.; Fiumi, C.; Bartoli, C.; Chiellini, E.; Fiorentino, B.; Farina, C. A new biocompatible nanoparticle delivery system for the release of fibrinolytic drugs. Int. J. Pharm. 2008, 357, 260–271. [Google Scholar] [CrossRef]
- Singh, D.; Dilnawaz, F.; Sahoo, S.K. Challenges of moving theranostic nanomedicine into the clinic. Nanomedicine 2020, 15, 111–114. [Google Scholar] [CrossRef]
- Zhang, F.; Huang, X.; Qian, C.; Zhu, L.; Hida, N.; Niu, G.; Chen, X. Synergistic enhancement of iron oxide nanoparticle and gadolinium for dual-contrast MRI. Biochem. Biophys. Res. Commun. 2012, 425, 886–891. [Google Scholar] [CrossRef] [Green Version]
- Singh, P.; Pandit, S.; Mokkapati, V.; Garg, A.; Ravikumar, V.; Mijakovic, I. Gold nanoparticles in diagnostics and therapeutics for human cancer. Int. J. Mol. Sci. 2018, 19, 1979. [Google Scholar] [CrossRef]
- Pan, D.; Pramanik, M.; Wickline, S.A.; Wang, L.V.; Lanza, G.M. Recent advances in colloidal gold nanobeacons for molecular photoacoustic imaging. Contrast Media Mol. Imaging 2011, 6, 378–388. [Google Scholar] [CrossRef]
- Mehata, A.K.; Dehari, D.; Gupta, A.; Rabin, D.C.; Miya, A. Multifunctional liquid crystal nanoparticles for cancer therapy. Curr. Nanomater. 2021, 6, 4–16. [Google Scholar] [CrossRef]
- Ghann, W.E.; Aras, O.; Fleiter, T.; Daniel, M.C. Syntheses and characterization of lisinopril-coated gold nanoparticles as highly stable targeted CT contrast agents in cardiovascular diseases. Langmuir 2012, 28, 10398–10408. [Google Scholar] [CrossRef] [PubMed]
- Pan, D.; Caruthers, S.D.; Senpan, A.; Yalaz, C.; Stacy, A.J.; Hu, G.; Marsh, J.N.; Gaffney, P.J.; Wickline, S.A.; Lanza, G.M. Synthesis of NanoQ, a copper-based contrast agent for high-resolution magnetic resonance imaging characterization of human thrombus. J. Am. Chem. Soc. 2011, 133, 9168–9171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christodoulides, N.; Pierre, F.N.; Sanchez, X.; Li, L.; Hocquard, K.; Patton, A.; Muldoon, R.; Miller, C.S.; Ebersole, J.L.; Redding, S. Programmable bio-nano-chip technology for the diagnosis of cardiovascular disease at the point-of-care. Methodist Debakey Cardiovasc. J. 2012, 8, 6–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Honikel, M.M.; Lin, C.E.; Probst, D.; La Belle, J.T. Facilitating Earlier Diagnosis of Cardiovascular Disease through Point-of-Care Biosensors: A Review. Crit. Rev. Biomed. Eng. 2018, 46, 53–82. [Google Scholar] [CrossRef] [PubMed]
- Cuadrado, I.; Piedras, M.J.; Herruzo, I.; Turpin Mdel, C.; Castejón, B.; Reventun, P.; Martin, A.; Saura, M.; Zamorano, J.L.; Zaragoza, C. EMMPRIN-targeted magnetic nanoparticles for in vivo visualization and regression of acute myocardial infarction. Theranostics 2016, 6, 545–557. [Google Scholar] [CrossRef]
- Pan, D.; Caruthers, S.D.; Chen, J.; Winter, P.M.; SenPan, A.; Schmieder, A.H.; Wickline, S.A.; Lanza, G.M. Nanomedicine strategies for molecular targets with MRI and optical imaging. Future Med. Chem. 2010, 2, 471–490. [Google Scholar] [CrossRef] [Green Version]
- Sosnovik, D.E.; Schellenberger, E.A.; Nahrendorf, M.; Novikov, M.S.; Matsui, T.; Dai, G.; Reynolds, F.; Grazette, L.; Rosenzweig, A.; Weissleder, R.; et al. Magnetic resonance imaging of cardiomyocyte apoptosis with a novel magneto-optical nanoparticle. Magn. Reson. Med. 2005, 54, 718–724. [Google Scholar] [CrossRef]
- Chen, H.H.; Josephson, L.; Sosnovik, D.E. Imaging of apoptosis in the heart with nanoparticle technology. Wiley Interdiscip Rev. Nanomed. Nanobiotechnol. 2011, 3, 86–99. [Google Scholar] [CrossRef] [Green Version]
- van Tilborg, G.A.; Vucic, E.; Strijkers, G.J.; Cormode, D.P.; Mani, V.; Skajaa, T.; Reutelingsperger, C.P.; Fayad, Z.A.; Mulder, W.J.; Nicolay, K. Annexin A5-functionalized bimodal nanoparticles for MRI and fluorescence imaging of atherosclerotic plaques. Bioconjug. Chem. 2010, 21, 1794–1803. [Google Scholar] [CrossRef] [Green Version]
- Mulder, W.J.; Jaffer, F.A.; Fayad, Z.A.; Nahrendorf, M. Imaging and nanomedicine in inflammatory atherosclerosis. Sci. Transl. Med. 2014, 6, 239sr231. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, W.T.; Shih, T.T.; Chen, R.C.; Tu, S.Y.; Hsieh, W.Y.; Yang, P.C. Integrin αvβ3-targeted dynamic contrast-enhanced magnetic resonance imaging using a gadolinium-loaded polyethylene gycol-dendrimer-cyclic RGD conjugate to evaluate tumor angiogenesis and to assess early antiangiogenic treatment response in a mouse xenograft tumor model. Mol. Imaging 2012, 11, 286–300. [Google Scholar] [PubMed]
- Karagkiozaki, V.C.; Logothetidis, S.D.; Kassavetis, S.N.; Giannoglou, G.D. Nanomedicine for the reduction of the thrombogenicity of stent coatings. Int. J. Nanomed. 2010, 5, 239–248. [Google Scholar] [CrossRef] [Green Version]
- Flacke, S.; Fischer, S.; Scott, M.J.; Fuhrhop, R.J.; Allen, J.S.; McLean, M.; Winter, P.; Sicard, G.A.; Gaffney, P.J.; Wickline, S.A.; et al. Novel MRI contrast agent for molecular imaging of fibrin: Implications for detecting vulnerable plaques. Circulation 2001, 104, 1280–1285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suzuki, M.; Bachelet-Violette, L.; Rouzet, F.; Beilvert, A.; Autret, G.; Maire, M.; Menager, C.; Louedec, L.; Choqueux, C.; Saboural, P.; et al. Ultrasmall superparamagnetic iron oxide nanoparticles coated with fucoidan for molecular MRI of intraluminal thrombus. Nanomedicine 2015, 10, 73–87. [Google Scholar] [CrossRef]
- Morawski, A.M.; Winter, P.M.; Yu, X.; Fuhrhop, R.W.; Scott, M.J.; Hockett, F.; Robertson, J.D.; Gaffney, P.J.; Lanza, G.M.; Wickline, S.A. Quantitative “magnetic resonance immunohistochemistry” with ligand-targeted (19)F nanoparticles. Magn. Reson. Med. 2004, 52, 1255–1262. [Google Scholar] [CrossRef]
- Mehata, A.K.; Viswanadh, M.K.; Priya, V.; Muthu, M.S. Dendritic cell-targeted theranostic nanomedicine: Advanced cancer nanotechnology for diagnosis and therapy. Nanomedicine 2020, 15, 947–949. [Google Scholar] [CrossRef] [Green Version]
- Takahama, H.; Shigematsu, H.; Asai, T.; Matsuzaki, T.; Sanada, S.; Fu, H.Y.; Okuda, K.; Yamato, M.; Asanuma, H.; Asano, Y.; et al. Liposomal amiodarone augments anti-arrhythmic effects and reduces hemodynamic adverse effects in an ischemia/reperfusion rat model. Cardiovasc. Drugs Ther. 2013, 27, 125–132. [Google Scholar] [CrossRef]
- Sercombe, L.; Veerati, T.; Moheimani, F.; Wu, S.Y.; Sood, A.K.; Hua, S. Advances and challenges of liposome assisted drug delivery. Front. Pharmacol. 2015, 6, 286. [Google Scholar] [CrossRef] [Green Version]
- Sharma, V.; Dewangan, H.K.; Maurya, L.; Vats, K.; Verma, H. Rational design and in-vivo estimation of Ivabradine Hydrochloride loaded nanoparticles for management of stable angina. J. Drug Deliv. Sci. Technol. 2019, 54, 101337. [Google Scholar] [CrossRef]
- Khan, A.A.; Abdulbaqi, I.M.; Abou Assi, R.; Murugaiyah, V.; Darwis, Y. Lyophilized hybrid nanostructured lipid carriers to enhance the cellular uptake of verapamil: Statistical optimization and in vitro evaluation. Nanoscale Res. Lett. 2018, 13, 323. [Google Scholar] [CrossRef] [PubMed]
- Al-Ansari, D.E.; Mohamed, N.A.; Marei, I.; Zekri, A.; Kameno, Y.; Davies, R.P.; Lickiss, P.D.; Rahman, M.M.; Abou-Saleh, H. Internalization of metal-organic framework nanoparticles in human vascular cells: Implications for cardiovascular disease therapy. Nanomaterials 2020, 10, 1028. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Zeng, G.; Cheng, J.; Hu, J.; Zhang, M.; Li, Y. Engineered macrophage membrane-enveloped nanomedicine for ameliorating myocardial infarction in a mouse model. Bioeng. Transl. Med. 2021, 6, e10197. [Google Scholar] [CrossRef] [PubMed]
- Tokutome, M.; Matoba, T.; Nakano, Y.; Okahara, A.; Fujiwara, M.; Koga, J.I.; Nakano, K.; Tsutsui, H.; Egashira, K. Peroxisome proliferator-activated receptor-gamma targeting nanomedicine promotes cardiac healing after acute myocardial infarction by skewing monocyte/macrophage polarization in preclinical animal models. Cardiovasc. Res. 2019, 115, 419–431. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Li, W.; Yu, D. Atrial natriuretic peptide modified oleate adenosine prodrug lipid nanocarriers for the treatment of myocardial infarction: In vitro and in vivo evaluation. Drug Des. Devel. Ther. 2018, 12, 1697–1706. [Google Scholar] [CrossRef] [Green Version]
- Qiu, J.; Cai, G.; Liu, X.; Ma, D. α(v)β(3) integrin receptor specific peptide modified, salvianolic acid B and panax notoginsenoside loaded nanomedicine for the combination therapy of acute myocardial ischemia. Biomed. Pharmacother. 2017, 96, 1418–1426. [Google Scholar] [CrossRef]
- Yao, C.; Shi, X.; Lin, X.; Shen, L.; Xu, D.; Feng, Y. Increased cardiac distribution of mono-PEGylated Radix Ophiopogonis polysaccharide in both myocardial infarction and ischemia/reperfusion rats. Int. J. Nanomed. 2015, 10, 409–418. [Google Scholar] [CrossRef] [Green Version]
- Liu, C.; Chen, L.; Ma, Y.; Hu, K.; Wu, P.; Pan, L.; Chen, H.; Li, L.; Hu, H.; Zhang, J. Pulmonary circulation-mediated heart targeting for the prevention of heart failure by inhalation of intrinsically bioactive nanoparticles. Theranostics 2021, 11, 8550–8569. [Google Scholar] [CrossRef]
- Leach, J.K.; O’Rear, E.A.; Patterson, E.; Miao, Y.; Johnson, A.E. Accelerated thrombolysis in a rabbit model of carotid artery thrombosis with liposome-encapsulated and microencapsulated streptokinase. Thromb. Haemost. 2003, 90, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Pawlowski, C.L.; Li, W.; Sun, M.; Ravichandran, K.; Hickman, D.; Kos, C.; Kaur, G.; Sen Gupta, A. Platelet microparticle-inspired clot-responsive nanomedicine for targeted fibrinolysis. Biomaterials 2017, 128, 94–108. [Google Scholar] [CrossRef]
- Palekar, R.U.; Jallouk, A.P.; Myerson, J.W.; Pan, H.; Wickline, S.A. Inhibition of thrombin with PPACK-nanoparticles restores disrupted endothelial barriers and attenuates thrombotic risk in experimental atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2016, 36, 446–455. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, J.P.; Yang, P.C.; Ma, Y.H.; Wu, T. Characterization of chitosan magnetic nanoparticles for in situ delivery of tissue plasminogen activator. Carbohydr. Polym. 2011, 84, 364–372. [Google Scholar] [CrossRef]
- McCarthy, J.R.; Sazonova, I.Y.; Erdem, S.S.; Hara, T.; Thompson, B.D.; Patel, P.; Botnaru, I.; Lin, C.P.; Reed, G.L.; Weissleder, R.; et al. Multifunctional nanoagent for thrombus-targeted fibrinolytic therapy. Nanomedicine 2012, 7, 1017–1028. [Google Scholar] [CrossRef] [Green Version]
- Kang, C.; Gwon, S.; Song, C.; Kang, P.M.; Park, S.C.; Jeon, J.; Hwang, D.W.; Lee, D. Fibrin-targeted and H2O2-responsive nanoparticles as a theranostics for thrombosed vessels. ACS Nano 2017, 11, 6194–6203. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.; Chen, X.; Wang, Y.; Xiao, H.; Peng, Y.; Lin, L.; Xia, W.; Long, M.; Tao, J.; Shuai, X. Aortic plaque-targeted andrographolide delivery with oxidation-sensitive micelle effectively treats atherosclerosis via simultaneous ROS capture and anti-inflammation. Nanomedicine 2018, 14, 2215–2226. [Google Scholar] [CrossRef]
- Lobatto, M.E.; Fayad, Z.A.; Silvera, S.; Vucic, E.; Calcagno, C.; Mani, V.; Dickson, S.D.; Nicolay, K.; Banciu, M.; Schiffelers, R.M.; et al. Multimodal clinical imaging to longitudinally assess a nanomedical anti-inflammatory treatment in experimental atherosclerosis. Mol. Pharm. 2010, 7, 2020–2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.; Sahu, A.; Hwang, Y.; Kim, G.B.; Nam, G.H.; Kim, I.S.; Chan Kwon, I.; Tae, G. Targeted delivery of anti-inflammatory cytokine by nanocarrier reduces atherosclerosis in Apo E(-/-) mice. Biomaterials 2020, 226, 119550. [Google Scholar] [CrossRef]
- Winter, P.M.; Neubauer, A.M.; Caruthers, S.D.; Harris, T.D.; Robertson, J.D.; Williams, T.A.; Schmieder, A.H.; Hu, G.; Allen, J.S.; Lacy, E.K.; et al. Endothelial alpha(v)beta3 integrin-targeted fumagillin nanoparticles inhibit angiogenesis in atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 2103–2109. [Google Scholar] [CrossRef] [Green Version]
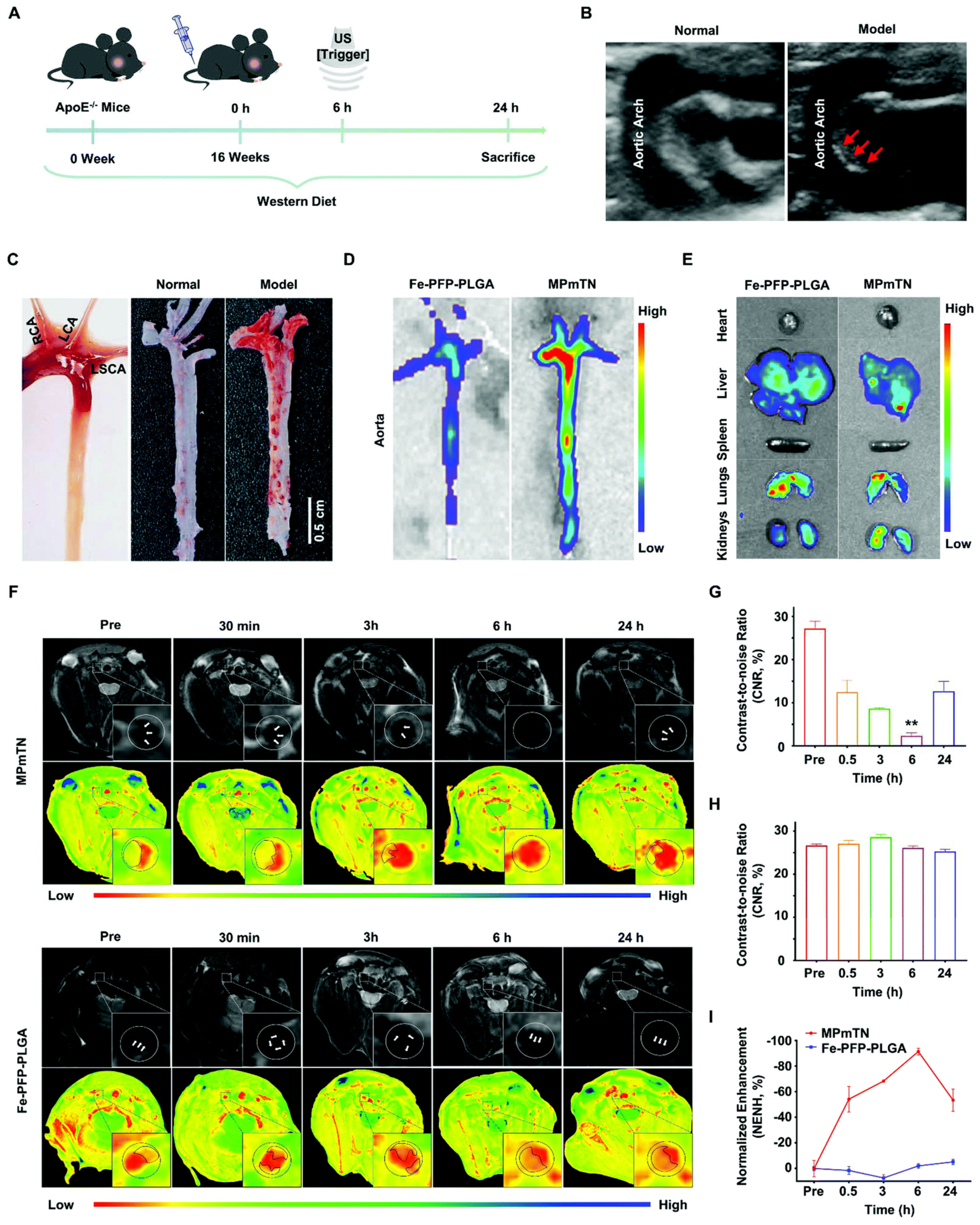
- Gao, B.; Xu, J.; Zhou, J.; Zhang, H.; Yang, R.; Wang, H.; Huang, J.; Yan, F.; Luo, Y. Multifunctional pathology-mapping theranostic nanoplatforms for US/MR imaging and ultrasound therapy of atherosclerosis. Nanoscale 2021, 13, 8623–8638. [Google Scholar] [CrossRef]
- Selvasudha, N.; Koumaravelou, K. The multifunctional synergistic effect of chitosan on simvastatin loaded nanoparticulate drug delivery system. Carbohydr. Polym. 2017, 163, 70–80. [Google Scholar] [CrossRef]
- Liu, L.; He, H.; Zhang, M.; Zhang, S.; Zhang, W.; Liu, J. Hyaluronic acid-decorated reconstituted high density lipoprotein targeting atherosclerotic lesions. Biomaterials 2014, 35, 8002–8014. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, D.; Janero, D.R.; Amiji, M. Engineering of an ω-3 polyunsaturated fatty acid-containing nanoemulsion system for combination C6-ceramide and 17β-estradiol delivery and bioactivity in human vascular endothelial and smooth muscle cells. Nanomedicine 2013, 9, 885–894. [Google Scholar] [CrossRef] [PubMed]
- Savalia, K.; Manickam, D.S.; Rosenbaugh, E.G.; Tian, J.; Ahmad, I.M.; Kabanov, A.V.; Zimmerman, M.C. Neuronal uptake of nanoformulated superoxide dismutase and attenuation of angiotensin II-dependent hypertension after central administration. Free Radic. Biol. Med. 2014, 73, 299–307. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onyüksel, H.; Séjourné, F.; Suzuki, H.; Rubinstein, I. Human VIP-alpha: A long-acting, biocompatible and biodegradable peptide nanomedicine for essential hypertension. Peptides 2006, 27, 2271–2275. [Google Scholar] [CrossRef]
- Qadri, G.R.; Ahad, A.; Aqil, M.; Imam, S.S.; Ali, A. Invasomes of isradipine for enhanced transdermal delivery against hypertension: Formulation, characterization, and in vivo pharmacodynamic study. Artif. Cells Nanomed. Biotechnol. 2017, 45, 139–145. [Google Scholar] [CrossRef] [Green Version]
- Gupta, V.; Gupta, N.; Shaik, I.H.; Mehvar, R.; McMurtry, I.F.; Oka, M.; Nozik-Grayck, E.; Komatsu, M.; Ahsan, F. Liposomal fasudil, a rho-kinase inhibitor, for prolonged pulmonary preferential vasodilation in pulmonary arterial hypertension. J. Control. Release 2013, 167, 189–199. [Google Scholar] [CrossRef] [Green Version]
- Akagi, S.; Nakamura, K.; Miura, D.; Saito, Y.; Matsubara, H.; Ogawa, A.; Matoba, T.; Egashira, K.; Ito, H. Delivery of imatinib-incorporated nanoparticles into lungs suppresses the development of monocrotaline-induced pulmonary arterial hypertension. Int. Heart J. 2015, 56, 354–359. [Google Scholar] [CrossRef] [Green Version]
- Juenet, M.; Aid-Launais, R.; Li, B.; Berger, A.; Aerts, J.; Ollivier, V.; Nicoletti, A.; Letourneur, D.; Chauvierre, C. Thrombolytic therapy based on fucoidan-functionalized polymer nanoparticles targeting P-selectin. Biomaterials 2018, 156, 204–216. [Google Scholar] [CrossRef]
- Marsh, J.N.; Hu, G.; Scott, M.J.; Zhang, H.; Goette, M.J.; Gaffney, P.J.; Caruthers, S.D.; Wickline, S.A.; Abendschein, D.; Lanza, G.M. A fibrin-specific thrombolytic nanomedicine approach to acute ischemic stroke. Nanomedicine 2011, 6, 605–615. [Google Scholar] [CrossRef] [Green Version]
- Singh, B.; Garg, T.; Goyal, A.K.; Rath, G. Development, optimization, and characterization of polymeric electrospun nanofiber: A new attempt in sublingual delivery of nicorandil for the management of angina pectoris. Artif. Cells Nanomed. Biotechnol. 2016, 44, 1498–1507. [Google Scholar] [CrossRef]
- Gorlin, R. Pathophysiology of cardiac pain. Circulation 1965, 32, 138–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prinzmetal, M.; Kennamer, R.; Merliss, R.; Wada, T.; Bor, N. Angina pectoris. I. A variant form of angina pectoris; preliminary report. Am. J. Med. 1959, 27, 375–388. [Google Scholar] [CrossRef]
- Fuchs, R.M.; Becker, L.C. Pathogenesis of angina pectoris. Arch. Intern. Med. 1982, 142, 1685–1692. [Google Scholar] [CrossRef] [PubMed]
- Zhuge, Y.; Zheng, Z.F.; Xie, M.Q.; Li, L.; Wang, F.; Gao, F. Preparation of liposomal amiodarone and investigation of its cardiomyocyte-targeting ability in cardiac radiofrequency ablation rat model. Int. J. Nanomed. 2016, 11, 2359–2367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rupp, H.; Zarain-Herzberg, A.; Maisch, B. The use of partial fatty acid oxidation inhibitors for metabolic therapy of angina pectoris and heart failure. Herz 2002, 27, 621–636. [Google Scholar] [CrossRef] [PubMed]
- Brusini, R.; Varna, M.; Couvreur, P. Advanced nanomedicines for the treatment of inflammatory diseases. Adv. Drug Deliv. Rev. 2020, 157, 161–178. [Google Scholar] [CrossRef]
- Molinaro, R.; Boada, C.; Del Rosal, G.M.; Hartman, K.A.; Corbo, C.; Andrews, E.D.; Toledano-Furman, N.E.; Cooke, J.P.; Tasciotti, E. Vascular inflammation: A novel access route for nanomedicine. Methodist Debakey Cardiovasc. J. 2016, 12, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Noels, H.; Weber, C.; Koenen, R.R. Chemokines as therapeutic targets in cardiovascular disease. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 583–592. [Google Scholar] [CrossRef] [Green Version]
- Detry, J.M. The pathophysiology of myocardial ischaemia. Eur. Heart J. 1996, 17 (Suppl. G), 48–52. [Google Scholar] [CrossRef]
- O’Dwyer, J.; Murphy, R.; Dolan, E.B.; Kovarova, L.; Pravda, M.; Velebny, V.; Heise, A.; Duffy, G.P.; Cryan, S.A. Development of a nanomedicine-loaded hydrogel for sustained delivery of an angiogenic growth factor to the ischaemic myocardium. Drug Deliv. Transl. Res. 2020, 10, 440–454. [Google Scholar] [CrossRef]
- Sosunov, E.A.; Anyukhovsky, E.P.; Sosunov, A.A.; Moshnikova, A.; Wijesinghe, D.; Engelman, D.M.; Reshetnyak, Y.K.; Andreev, O.A. pH (low) insertion peptide (pHLIP) targets ischemic myocardium. Proc. Natl. Acad. Sci. USA 2013, 110, 82–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paul, A.; Hasan, A.; Kindi, H.A.; Gaharwar, A.K.; Rao, V.T.; Nikkhah, M.; Shin, S.R.; Krafft, D.; Dokmeci, M.R.; Shum-Tim, D.; et al. Injectable graphene oxide/hydrogel-based angiogenic gene delivery system for vasculogenesis and cardiac repair. ACS Nano 2014, 8, 8050–8062. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, H.; Lee, J.S.; Chen, E.; Wang, M.; Xing, Y.; Fahmy, T.M.; Dardik, A. Covalent modification of pericardial patches for sustained rapamycin delivery inhibits venous neointimal hyperplasia. Sci. Rep. 2017, 7, 40142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stapleton, L.M.; Steele, A.N.; Wang, H.; Lopez Hernandez, H.; Yu, A.C.; Paulsen, M.J.; Smith, A.A.A.; Roth, G.A.; Thakore, A.D.; Lucian, H.J.; et al. Use of a supramolecular polymeric hydrogel as an effective post-operative pericardial adhesion barrier. Nat. Biomed. Eng. 2019, 3, 611–620. [Google Scholar] [CrossRef] [PubMed]
- Priya, V.; Viswanadh, M.K.; Mehata, A.K.; Jain, D.; Singh, S.K.; Muthu, M.S. Targeted nanotherapeutics in the prophylaxis and treatment of thrombosis. Nanomedicine 2021, 16, 1153–1176. [Google Scholar] [CrossRef]
- Zenych, A.; Fournier, L.; Chauvierre, C. Nanomedicine progress in thrombolytic therapy. Biomaterials 2020, 258, 120297. [Google Scholar] [CrossRef]
- Varna, M.; Juenet, M.; Bayles, R.; Mazighi, M.; Chauvierre, C.; Letourneur, D. Nanomedicine as a strategy to fight thrombotic diseases. Future Sci. OA 2015, 1, Fso46. [Google Scholar] [CrossRef] [Green Version]
- Srinivasan, R.; Marchant, R.E.; Gupta, A.S. In vitro and in vivo platelet targeting by cyclic RGD-modified liposomes. J. Biomed. Mater. Res. A 2010, 93, 1004–1015. [Google Scholar] [CrossRef] [Green Version]
- Gupta, A.S.; Huang, G.; Lestini, B.J.; Sagnella, S.; Kottke-Marchant, K.; Marchant, R.E. RGD-modified liposomes targeted to activated platelets as a potential vascular drug delivery system. Thromb. Haemost. 2005, 93, 106–114. [Google Scholar] [CrossRef]
- Huang, G.; Zhou, Z.; Srinivasan, R.; Penn, M.S.; Kottke-Marchant, K.; Marchant, R.E.; Gupta, A.S. Affinity manipulation of surface-conjugated RGD peptide to modulate binding of liposomes to activated platelets. Biomaterials 2008, 29, 1676–1685. [Google Scholar] [CrossRef] [Green Version]
- Wu, T.; Xiao, H.; Lu, L.; Chen, Y.; Wang, Y.; Xia, W.; Long, M.; Tao, J.; Shen, J.; Shuai, X. Polymeric Vector-Mediated Targeted Delivery of Anti-PAK1 siRNA to Macrophages for Efficient Atherosclerosis Treatment. ACS Biomater. Sci. Eng. 2019, 5, 4455–4462. [Google Scholar] [CrossRef] [PubMed]
- Bergheanu, S.C.; Bodde, M.C.; Jukema, J.W. Pathophysiology and treatment of atherosclerosis: Current view and future perspective on lipoprotein modification treatment. Neth. Heart J. 2017, 25, 231–242. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Valk, F.M.; van Wijk, D.F.; Lobatto, M.E.; Verberne, H.J.; Storm, G.; Willems, M.C.; Legemate, D.A.; Nederveen, A.J.; Calcagno, C.; Mani, V.; et al. Prednisolone-containing liposomes accumulate in human atherosclerotic macrophages upon intravenous administration. Nanomedicine 2015, 11, 1039–1046. [Google Scholar] [CrossRef] [Green Version]
- Panth, N.; Paudel, K.R.; Parajuli, K. Reactive oxygen species: A key hallmark of cardiovascular disease. Adv. Med. 2016, 2016, 9152732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gadde, S.; Rayner, K.J. Nanomedicine meets microRNA: Current advances in RNA-based nanotherapies for atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2016, 36, e73–e79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuo, C.H.; Leon, L.; Chung, E.J.; Huang, R.T.; Sontag, T.J.; Reardon, C.A.; Getz, G.S.; Tirrell, M.; Fang, Y. Inhibition of atherosclerosis-promoting microRNAs via targeted polyelectrolyte complex micelles. J. Mater. Chem. B 2014, 2, 8142–8153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mlinar, L.B.; Chung, E.J.; Wonder, E.A.; Tirrell, M. Active targeting of early and mid-stage atherosclerotic plaques using self-assembled peptide amphiphile micelles. Biomaterials 2014, 35, 8678–8686. [Google Scholar] [CrossRef] [PubMed]
- Lanza, G.M.; Winter, P.M.; Caruthers, S.D.; Hughes, M.S.; Cyrus, T.; Marsh, J.N.; Neubauer, A.M.; Partlow, K.C.; Wickline, S.A. Nanomedicine opportunities for cardiovascular disease with perfluorocarbon nanoparticles. Nanomedicine 2006, 1, 321–329. [Google Scholar] [CrossRef]
- Xu, W.; Jambhulkar, S.; Ravichandran, D.; Zhu, Y.; Kakarla, M.; Nian, Q.; Azeredo, B.; Chen, X.; Jin, K.; Vernon, B.; et al. 3D Printing-enabled nanoparticle alignment: A review of mechanisms and applications. Small 2021, 17, e2100817. [Google Scholar] [CrossRef]
- Zang, X.; Cheng, M.; Zhang, X.; Chen, X. Targeting macrophages using nanoparticles: A potential therapeutic strategy for atherosclerosis. J. Mater. Chem. B 2021, 9, 3284–3294. [Google Scholar] [CrossRef]
- Nahrendorf, M.; Zhang, H.; Hembrador, S.; Panizzi, P.; Sosnovik, D.E.; Aikawa, E.; Libby, P.; Swirski, F.K.; Weissleder, R. Nanoparticle PET-CT imaging of macrophages in inflammatory atherosclerosis. Circulation 2008, 117, 379–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, K.S.; Kathiravan, M.K.; Somani, R.S.; Shishoo, C.J. The biology and chemistry of hyperlipidemia. Bioorg. Med. Chem. 2007, 15, 4674–4699. [Google Scholar] [CrossRef] [PubMed]
- Sreedhar, R.; Kumar, V.S.; Bhaskaran Pillai, A.K.; Mangalathillam, S. Omega-3 Fatty Acid Based Nanolipid Formulation of Atorvastatin for Treating Hyperlipidemia. Adv. Pharm. Bull. 2019, 9, 271–280. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.L.; Tao, Y.; Guo, J.; Hu, Y.M.; Su, Z.Q. Hypolipidemic effects of chitosan nanoparticles in hyperlipidemia rats induced by high fat diet. Int. Immunopharmacol. 2011, 11, 457–461. [Google Scholar] [CrossRef]
- Patel, S.; Drew, B.G.; Nakhla, S.; Duffy, S.J.; Murphy, A.J.; Barter, P.J.; Rye, K.A.; Chin-Dusting, J.; Hoang, A.; Sviridov, D.; et al. Reconstituted high-density lipoprotein increases plasma high-density lipoprotein anti-inflammatory properties and cholesterol efflux capacity in patients with type 2 diabetes. J. Am. Coll. Cardiol. 2009, 53, 962–971. [Google Scholar] [CrossRef] [Green Version]
- Serini, S.; Cassano, R.; Trombino, S.; Calviello, G. Nanomedicine-based formulations containing ω-3 polyunsaturated fatty acids: Potential application in cardiovascular and neoplastic diseases. Int. J. Nanomed. 2019, 14, 2809–2828. [Google Scholar] [CrossRef] [Green Version]
- Abdel-Rahman, M.A.; Hamad, H.; Eltamany, E.H.; Al-Sherbini, A.-S. The synthesis and characterization of gold nanoparticles with polyunsaturated oils contribute to hypolipidemic and anti-obesity activities in vivo. Egypt. J. Chem. 2020, 63, 4205–4216. [Google Scholar] [CrossRef]
- Chmielowski, R.A.; Abdelhamid, D.S.; Faig, J.J.; Petersen, L.K.; Gardner, C.R.; Uhrich, K.E.; Joseph, L.B.; Moghe, P.V. Athero-inflammatory nanotherapeutics: Ferulic acid-based poly(anhydride-ester) nanoparticles attenuate foam cell formation by regulating macrophage lipogenesis and reactive oxygen species generation. Acta Biomater. 2017, 57, 85–94. [Google Scholar] [CrossRef]
- Taylor, D.A. Hypertensive Crisis: A Review of Pathophysiology and Treatment. Crit. Care Nurs. Clin. N. Am. 2015, 27, 439–447. [Google Scholar] [CrossRef]
- Rolim, T.; Cancino, J.; Zucolotto, V. A nanostructured genosensor for the early diagnosis of systemic arterial hypertension. Biomed. Microdevices 2015, 17, 3. [Google Scholar] [CrossRef]
- de Azevedo Mde, B.; Tasic, L.; Fattori, J.; Rodrigues, F.H.; Cantos, F.C.; Ribeiro, L.P.; de Paula, V.; Ianzer, D.; Santos, R.A. New formulation of an old drug in hypertension treatment: The sustained release of captopril from cyclodextrin nanoparticles. Int. J. Nanomed. 2011, 6, 1005–1016. [Google Scholar] [CrossRef] [Green Version]
- Venishetty, V.K.; Chede, R.; Komuravelli, R.; Adepu, L.; Sistla, R.; Diwan, P.V. Design and evaluation of polymer coated carvedilol loaded solid lipid nanoparticles to improve the oral bioavailability: A novel strategy to avoid intraduodenal administration. Colloids Surf. B Biointerfaces 2012, 95, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Fancher, I.S.; Rubinstein, I.; Levitan, I. Potential strategies to reduce blood pressure in treatment-resistant hypertension using food and drug administration-approved nanodrug delivery platforms. Hypertension 2019, 73, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Mosgoeller, W.; Prassl, R.; Zimmer, A. Nanoparticle-mediated treatment of pulmonary arterial hypertension. Methods Enzymol. 2012, 508, 325–354. [Google Scholar] [CrossRef]
- Vachiéry, J.L.; Tedford, R.J.; Rosenkranz, S.; Palazzini, M.; Lang, I.; Guazzi, M.; Coghlan, G.; Chazova, I.; De Marco, T. Pulmonary hypertension due to left heart disease. Eur. Respir. J. 2019, 53, 1801897. [Google Scholar] [CrossRef] [Green Version]
- Segura-Ibarra, V.; Wu, S.; Hassan, N.; Moran-Guerrero, J.A.; Ferrari, M.; Guha, A.; Karmouty-Quintana, H.; Blanco, E. Nanotherapeutics for treatment of pulmonary arterial hypertension. Front. Physiol. 2018, 9, 890. [Google Scholar] [CrossRef]
- Beck-Broichsitter, M.; Hecker, A.; Kosanovic, D.; Schmehl, T.; Gessler, T.; Weissmann, N.; Ghofrani, H.A.; Kissel, T.; Seeger, W.; Schermuly, R.T. Prolonged vasodilatory response to nanoencapsulated sildenafil in pulmonary hypertension. Nanomedicine 2016, 12, 63–68. [Google Scholar] [CrossRef]
- Nafee, N.; Makled, S.; Boraie, N. Nanostructured lipid carriers versus solid lipid nanoparticles for the potential treatment of pulmonary hypertension via nebulization. Eur. J. Pharm. Sci. 2018, 125, 151–162. [Google Scholar] [CrossRef]
- Mohamed, N.A.; Abou-Saleh, H.; Kameno, Y.; Marei, I.; de Nucci, G.; Ahmetaj-Shala, B.; Shala, F.; Kirkby, N.S.; Jennings, L.; Al-Ansari, D.E.; et al. Studies on metal-organic framework (MOF) nanomedicine preparations of sildenafil for the future treatment of pulmonary arterial hypertension. Sci. Rep. 2021, 11, 4336. [Google Scholar] [CrossRef]
- Mitchell, J.A.; Ahmetaj-Shala, B.; Kirkby, N.S.; Wright, W.R.; Mackenzie, L.S.; Reed, D.M.; Mohamed, N. Role of prostacyclin in pulmonary hypertension. Glob. Cardiol. Sci. Pract. 2014, 2014, 382–393. [Google Scholar] [CrossRef] [Green Version]
- Kleemann, E.; Schmehl, T.; Gessler, T.; Bakowsky, U.; Kissel, T.; Seeger, W. Iloprost-containing liposomes for aerosol application in pulmonary arterial hypertension: Formulation aspects and stability. Pharm. Res. 2007, 24, 277–287. [Google Scholar] [CrossRef] [PubMed]
- Gessler, T.; Seeger, W.; Schmehl, T. Inhaled prostanoids in the therapy of pulmonary hypertension. J. Aerosol Med. Pulm. Drug Deliv. 2008, 21, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Mohamed, N.A.; Ahmetaj-Shala, B.; Duluc, L.; Mackenzie, L.S.; Kirkby, N.S.; Reed, D.M.; Lickiss, P.D.; Davies, R.P.; Freeman, G.R.; Wojciak-Stothard, B.; et al. A New NO-Releasing nanoformulation for the treatment of pulmonary arterial hypertension. J. Cardiovasc. Transl. Res. 2016, 9, 162–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arboix, A.; Alió, J. Cardioembolic stroke: Clinical features, specific cardiac disorders and prognosis. Curr. Cardiol. Rev. 2010, 6, 150–161. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Zhang, Y.; Xia, J.; Cai, T.; Du, J.; Chen, J.; Li, P.; Shen, Y.; Zhang, A.; Fu, B.; et al. Neuronal PirB upregulated in cerebral ischemia acts as an attractive theranostic target for ischemic stroke. J. Am. Heart Assoc. 2018, 7, e007197. [Google Scholar] [CrossRef] [Green Version]
- Lanza, G.M.; Marsh, J.N.; Hu, G.; Scott, M.J.; Schmieder, A.H.; Caruthers, S.D.; Pan, D.; Wickline, S.A. Rationale for a nanomedicine approach to thrombolytic therapy. Stroke 2010, 41, S42–S44. [Google Scholar] [CrossRef] [Green Version]
- Bonnard, T.; Gauberti, M.; Martinez de Lizarrondo, S.; Campos, F.; Vivien, D. Recent advances in nanomedicine for ischemic and hemorrhagic stroke. Stroke 2019, 50, 1318–1324. [Google Scholar] [CrossRef]
- Nagasaki, Y. Nitroxide radicals and nanoparticles: A partnership for nanomedicine radical delivery. Ther. Deliv. 2012, 3, 165–179. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.K.; Kim, T.; Choi, I.Y.; Soh, M.; Kim, D.; Kim, Y.J.; Jang, H.; Yang, H.S.; Kim, J.Y.; Park, H.K.; et al. Ceria nanoparticles that can protect against ischemic stroke. Angew. Chem. Int. Ed. Engl. 2012, 51, 11039–11043. [Google Scholar] [CrossRef]
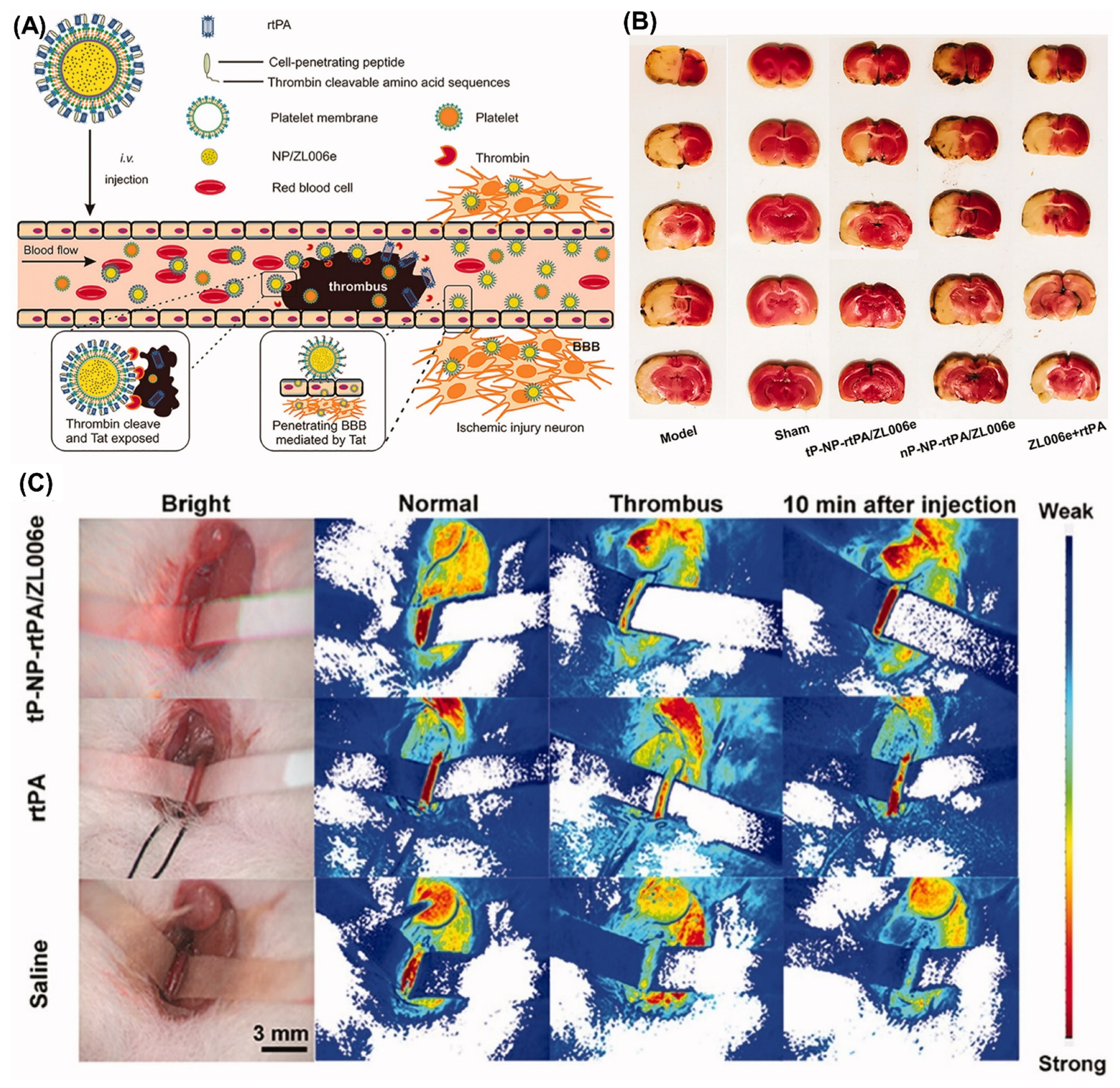
- Xu, J.; Wang, X.; Yin, H.; Cao, X.; Hu, Q.; Lv, W.; Xu, Q.; Gu, Z.; Xin, H. Sequentially site-specific delivery of thrombolytics and neuroprotectant for enhanced treatment of ischemic stroke. ACS Nano 2019, 13, 8577–8588. [Google Scholar] [CrossRef]
- Cicha, I.; Chauvierre, C.; Texier, I.; Cabella, C.; Metselaar, J.M.; Szebeni, J.; Dézsi, L.; Alexiou, C.; Rouzet, F.; Storm, G.; et al. From design to the clinic: Practical guidelines for translating cardiovascular nanomedicine. Cardiovasc. Res. 2018, 114, 1714–1727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trivedi, R.A.; Mallawarachi, C.; JM, U.K.-I.; Graves, M.J.; Horsley, J.; Goddard, M.J.; Brown, A.; Wang, L.; Kirkpatrick, P.J.; Brown, J.; et al. Identifying inflamed carotid plaques using in vivo USPIO-enhanced MR imaging to label plaque macrophages. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 1601–1606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sadat, U.; Howarth, S.P.; Usman, A.; Tang, T.Y.; Graves, M.J.; Gillard, J.H. Sequential imaging of asymptomatic carotid atheroma using ultrasmall superparamagnetic iron oxide-enhanced magnetic resonance imaging: A feasibility study. J. Stroke Cerebrovasc. Dis. 2013, 22, e271–e276. [Google Scholar] [CrossRef] [PubMed]
- Howarth, S.P.; Tang, T.Y.; Trivedi, R.; Weerakkody, R.; U-King-Im, J.; Gaunt, M.E.; Boyle, J.R.; Li, Z.Y.; Miller, S.R.; Graves, M.J.; et al. Utility of USPIO-enhanced MR imaging to identify inflammation and the fibrous cap: A comparison of symptomatic and asymptomatic individuals. Eur. J. Radiol. 2009, 70, 555–560. [Google Scholar] [CrossRef]
- Alam, S.R.; Shah, A.S.; Richards, J.; Lang, N.N.; Barnes, G.; Joshi, N.; MacGillivray, T.; McKillop, G.; Mirsadraee, S.; Payne, J.; et al. Ultrasmall superparamagnetic particles of iron oxide in patients with acute myocardial infarction: Early clinical experience. Circ. Cardiovasc. Imaging 2012, 5, 559–565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lobatto, M.E.; Calcagno, C.; Otten, M.J.; Millon, A.; Ramachandran, S.; Paridaans, M.P.; van der Valk, F.M.; Storm, G.; Stroes, E.S.; Fayad, Z.A.; et al. Pharmaceutical development and preclinical evaluation of a GMP-grade anti-inflammatory nanotherapy. Nanomedicine 2015, 11, 1133–1140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kharlamov, A.N.; Tyurnina, A.E.; Veselova, V.S.; Kovtun, O.P.; Shur, V.Y.; Gabinsky, J.L. Silica-gold nanoparticles for atheroprotective management of plaques: Results of the NANOM-FIM trial. Nanoscale 2015, 7, 8003–8015. [Google Scholar] [CrossRef]
- Banai, S.; Finkelstein, A.; Almagor, Y.; Assali, A.; Hasin, Y.; Rosenschein, U.; Apruzzese, P.; Lansky, A.J.; Kume, T.; Edelman, E.R. Targeted anti-inflammatory systemic therapy for restenosis: The Biorest Liposomal Alendronate with Stenting sTudy (BLAST)—A double blind, randomized clinical trial. Am. Heart J. 2013, 165, 234–240.e231. [Google Scholar] [CrossRef] [Green Version]
- Wilson, B.; Km, G. Artificial intelligence and related technologies enabled nanomedicine for advanced cancer treatment. Nanomedicine 2020, 15, 433–435. [Google Scholar] [CrossRef] [Green Version]
- Yan, C.; Quan, X.J.; Feng, Y.M. Nanomedicine for Gene Delivery for the Treatment of Cardiovascular Diseases. Curr. Gene Ther. 2019, 19, 20–30. [Google Scholar] [CrossRef]
- Vandergriff, A.C.; Hensley, T.M.; Henry, E.T.; Shen, D.; Anthony, S.; Zhang, J.; Cheng, K. Magnetic targeting of cardiosphere-derived stem cells with ferumoxytol nanoparticles for treating rats with myocardial infarction. Biomaterials 2014, 35, 8528–8539. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Shen, Y.; Sun, A.; Huang, G.; Zhu, H.; Huang, B.; Xu, J.; Song, Y.; Pei, N.; Ma, J.; et al. Magnetic targeting enhances retrograde cell retention in a rat model of myocardial infarction. Stem Cell. Res. Ther. 2013, 4, 149. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davis, M.E.; Hsieh, P.C.; Takahashi, T.; Song, Q.; Zhang, S.; Kamm, R.D.; Grodzinsky, A.J.; Anversa, P.; Lee, R.T. Local myocardial insulin-like growth factor 1 (IGF-1) delivery with biotinylated peptide nanofibers improves cell therapy for myocardial infarction. Proc. Natl. Acad. Sci. USA 2006, 103, 8155–8160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mittal, R.; Jhaveri, V.M.; McMurry, H.S.; Kay, S.S.; Sutherland, K.J.; Nicole, L.; Mittal, J.; Jayant, R.D. Recent treatment modalities for cardiovascular diseases with a focus on stem cells, aptamers, exosomes and nanomedicine. Artif. Cells Nanomed. Biotechnol. 2018, 46, 831–840. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muniyandi, P.; Palaninathan, V.; Mizuki, T.; Maekawa, T.; Hanajiri, T.; Mohamed, M.S. Poly(lactic-co-glycolic acid)/polyethylenimine nanocarriers for direct genetic reprogramming of microRNA targeting cardiac fibroblasts. ACS Appl. Nano Mater. 2020, 3, 2491–2505. [Google Scholar] [CrossRef]
- Mohammadi Nasr, S.; Rabiee, N.; Hajebi, S.; Ahmadi, S.; Fatahi, Y.; Hosseini, M.; Bagherzadeh, M.; Ghadiri, A.M.; Rabiee, M.; Jajarmi, V.; et al. Biodegradable nanopolymers in cardiac tissue engineering: From concept towards nanomedicine. Int. J. Nanomed. 2020, 15, 4205–4224. [Google Scholar] [CrossRef]
- Witkowski, M.; Weeks, T.L.; Hazen, S.L. Gut microbiota and cardiovascular disease. Circ. Res. 2020, 127, 553–570. [Google Scholar] [CrossRef]
- Salehi, B.; Del Prado-Audelo, M.L.; Cortés, H.; Leyva-Gómez, G.; Stojanović-Radić, Z.; Singh, Y.D.; Patra, J.K.; Das, G.; Martins, N.; Martorell, M.; et al. Therapeutic applications of curcumin nanomedicine formulations in cardiovascular diseases. J. Clin. Med. 2020, 9, 746. [Google Scholar] [CrossRef] [Green Version]
- Masuda, S.; Nakano, K.; Funakoshi, K.; Zhao, G.; Meng, W.; Kimura, S.; Matoba, T.; Miyagawa, M.; Iwata, E.; Sunagawa, K.; et al. Imatinib mesylate-incorporated nanoparticle-eluting stent attenuates in-stent neointimal formation in porcine coronary arteries. J. Atheroscler. Thromb. 2011, 18, 1043–1053. [Google Scholar] [CrossRef] [Green Version]
- McDowell, G.; Slevin, M.; Krupinski, J. Nanotechnology for the treatment of coronary in stent restenosis: A clinical perspective. Vasc. Cell 2011, 3, 8. [Google Scholar] [CrossRef] [Green Version]
- Tsukie, N.; Nakano, K.; Matoba, T.; Masuda, S.; Iwata, E.; Miyagawa, M.; Zhao, G.; Meng, W.; Kishimoto, J.; Sunagawa, K.; et al. Pitavastatin-incorporated nanoparticle-eluting stents attenuate in-stent stenosis without delayed endothelial healing effects in a porcine coronary artery model. J. Atheroscler. Thromb. 2013, 20, 32–45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leopold, J.A.; Loscalzo, J. Emerging role of precision medicine in cardiovascular disease. Circ. Res. 2018, 122, 1302–1315. [Google Scholar] [CrossRef] [PubMed]
- Suk, J.S.; Xu, Q.; Kim, N.; Hanes, J.; Ensign, L.M. PEGylation as a strategy for improving nanoparticle-based drug and gene delivery. Adv. Drug Deliv. Rev. 2016, 99, 28–51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Q.; Lai, S.K. Anti-PEG immunity: Emergence, characteristics, and unaddressed questions. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnol. 2015, 7, 655–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, H.L.; Zhang, Y.S.; Khademhosseini, A. Boosting clinical translation of nanomedicine. Nanomedicine 2016, 11, 1495–1497. [Google Scholar] [CrossRef] [Green Version]
- Ventola, C.L. The nanomedicine revolution: Part 3: Regulatory and safety challenges. Pharm. Ther. 2012, 37, 631–639. [Google Scholar]
- Devasahayam, S. Nanotechnology and nanomedicine in market: A global perspective on regulatory issues. In Characterization and Biology of Nanomaterials for Drug Delivery; Elsevier: Amsterdam, The Netherlands, 2019; pp. 477–522. [Google Scholar]
- Wolfram, J.; Zhu, M.; Yang, Y.; Shen, J.; Gentile, E.; Paolino, D.; Fresta, M.; Nie, G.; Chen, C.; Shen, H.; et al. Safety of nanoparticles in medicine. Curr. Drug Targets 2015, 16, 1671–1681. [Google Scholar] [CrossRef] [Green Version]
- Ventola, C.L. Progress in nanomedicine: Approved and investigational nanodrugs. Pharm. Ther. 2017, 42, 742–755. [Google Scholar]
- Wu, L.P.; Wang, D.; Li, Z. Grand challenges in nanomedicine. Mater. Sci. Eng. C Mater. Biol. Appl. 2020, 106, 110302. [Google Scholar] [CrossRef]
- Bobo, D.; Robinson, K.J.; Islam, J.; Thurecht, K.J.; Corrie, S.R. Nanoparticle-based medicines: A review of fda-approved materials and clinical trials to date. Pharm. Res. 2016, 33, 2373–2387. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diseases/CVRDs | Drug/Nanocarrier | Targeted Areas | Treatment Time | Tested Doses and Route of Administration | Inferences | Ref. |
|---|---|---|---|---|---|---|
| Angina pectoris | Ivabradine/Polymeric nanoparticles | Funny channels of SA-node | 3 days | 1.54 mg/kg, 2 mL; oral | Increased permeability; anti-anginal effects lasted for 3 consecutive days. | [40] |
| Angina pectoris | Verapamil/NLCs | α-adrenergic receptors of myocardial cells | 24 h | - | Prolonged drug release; higher cellular uptake. | [41] |
| Myocarditis | Iron metal/nanoparticle, Materials InstituteLavoisier-89 | Artery endothelial and smooth muscle cells | 24 h | - | Shown anti-inflammatory effect and reduced chemokine CXCL8. | [42] |
| Myocardial infarction | Magnetic nanoparticles | Extracellular matrix—Metalloproteinase inducer | - | 50 mg/Kg i.v. | In vivo visualization and regression of acute myocardial infarction. | [26] |
| Myocardial infarction | miR199a-3p/macrophage membrane coated nanoparticles | IL-1β, -6, and tumor necrosis factor alpha (TNF-α) | 2 weeks | 2.0 mg/kg; i.v. | Reduction in inflammatory cells and increased cell proliferation abilities. | [43] |
| Myocardial infarction | Pioglitazone/Poly (lactic acid/glycolic acid) nanoparticles | Peroxisome proliferator-activated receptor-gamma (PPARγ) | 3 days | 1.0 mg/kg; i.v. | Suppression of Ly6Chigh inflammatory monocyte and inflammatory gene expression. | [44] |
| Myocardial infarction | Oleate adenosine prodrug-atrial natriuretic peptide/Lipid nanocarriers | Natriuretic peptide receptors of ischemic heart | 48 h | 1 mL per rat; i.v. | Reduction in infract size. | [45] |
| Myocardial infarction | Salvianolic acid B-ginsenoside Rg 1/Lipid-polymer hybrid nanoparticles | αvβ3 integrin receptor | 3 days | Sal B: 10 mg/kg, PNS: 10 mg/kg; i.v. | Reduction in infract size. | [46] |
| Myocardial infarction | Radix Ophiopogonis polysaccharide/Mono polyethylene glycol | Hypoxic tissues of the heart | 4 days | 4 μmol/kg; i.v. | Increased drug accumulation in the infarcted myocardium. | [47] |
| Heart failure | ATTPCD bioactive nanoparticles | Pulmonary circulation-mediated heart targeting | 12 to 48 h | 50 mg/kg | Prevention of heart failure and imaging of heart and vital organ. | [48] |
| Thrombosis | Streptokinase/Liposome-encapsulated & microencapsulated | Plasminogen | 2 h | 6000 IU/kg; i.v. | Lesser cases of occlusions were observed. | [49] |
| Thrombosis | Streptokinase/platelet-derived Microparticles—inspired nanovesicles | Plasminogen | Overnight | 30 mg/kg; i.v. | Relieving thrombolytic payload. | [50] |
| Thrombosis | D-phenylalanyl-L-prolyl-L-arginyl chloromethyl ketone/Semipermeant perfluorocarbon core nanoparticles | Thrombin | 1 month | - | Inactivates thrombin. | [51] |
| Thrombosis | tPA/Chitosan magnetic nanoparticles | Fibrin clot | 2 h | 150 μL; i.v. | Increased efficacy of drug. | [52] |
| Thrombosis | Recombinant tissue plasminogen activator/magnetofluorescent nanoparticle | Thrombus clot | 1 h | 14 mg/kg; i.v. | Exhibits theranostic capabilities and high affinity towards clot. | [53] |
| Thrombosis | Fibrin targeted H2O2-responsive nanoparticles | Fibrin | 3 min | 24 μg/kg i.v. | Image obstructed vessels and inhibit thrombus formation. | [54] |
| Diseases/CVRDs | Drug/Nanocarrier | Targeted Areas | Treatment Time | Tested Doses and Route of Administration | Inferences | Ref. |
|---|---|---|---|---|---|---|
| Atherosclerosis | Andrographolide/PEG-poly(propylene sulphide) micelles | NF-κB signaling pathway | 30 days | 45 μg/g micelle, 2 μg/g; andro i.v. | Increased delivery efficiency. | [55] |
| Atherosclerosis | Prednisolone/Liposomes | Atherosclerotic macrophages | 10 days | 1.5 mg/kg; i.v. | No anti-inflammatory effect seen. | [56] |
| Atherosclerosis | IL-10/Arginylglycyl aspartic acid conjugated pluronic-based nanocarriers | Atherosclerotic plaques | 1–3 weeks | 1.05 mg of NC with 5 μg IL10; i.v. | Could inhibit the progression of atherosclerotic plaques. | [57] |
| Atherosclerosis | Fumagillin/Paramagnetic nanoparticles | Endothelial αvβ3 integrin | 2–4 h | 1.0 mL/kg; i.v. | Quantification and inhibition of angiogenesis. | [58] |
| Atherosclerosis | PLGA nanoparticles | plaque-targeted peptides PP1 and cRGD | 6 h | - | Diagnosis and therapy of advanced atherosclerotic plaques. | [59] |
| Hyperlipidemia | Simvastatin/chitosan NPs | HMG-CoA reductase enzyme | 16 weeks | 10 mg/kg; Oral | Increased hypolipidemic effect. | [60] |
| Hyperlipidemia | Lovastatin/Hyaluronic acid-reconstituted high-density lipoprotein | Atherosclerotic lesions | 8 weeks | 2 mg/kg; i.v | Greater atheroprotective efficacy. | [61] |
| Hyperlipidemia | N-hexanoylsphingosine or 17-β-estradiol/Nanoemulsions | MAPK enzyme | 24 h | - | Greater anti-proliferative activity. | [62] |
| Hyperlipidemia | Copper/Zinc superoxide dismutase/Poly-L-lysine (PLL50)-polyethylene glycol block co-polymer | Central nerves | 9 days | 130–150 U CuZnSOD activity; ICV injection | Stabilized angiotensin-II-dependent hypertension. | [63] |
| Hyperlipidemia | Human vasoactive intestinal peptide (VIP-α)/Liposomes | Cognate receptors of vascular smooth cells | 6 h | 0.5 mL; i.v | Potent vasodilation and lowers systemic arterial pressure. | [64] |
| Hyperlipidemia | Isradipine/Invasomes | L-type calcium channels of vascular smooth muscle and myocardium | 24 h | Transdermal flux | Improved the antihypertensive activity. | [65] |
| Pulmonary arterial hypertension | Fasudil/Liposomes | Rho-kinase receptors | 4 weeks | 3 mg/kg; intratracheal | Prolonged vasodilatory effect for three hours. | [66] |
| Pulmonary arterial hypertension | Imatinib/Polylactide-glycolide nanoparticles-fluorescein isothiocyanate | Platelet–derived growth factor receptors | 3 weeks | 1 mg/kg; intratracheal instillation | Sustained antiproliferative effects. | [67] |
| Stroke | rtPA/Polysaccharide-poly(isobutylcyanoacrylate)-fucoidan nanoparticles | P-selectin | 30 min | 2.5 mg/kg; i.v. | Thrombus density reduced to one-third of its original sizes. | [68] |
| Stroke | Urokinase anti-fibrin monoclonal antibodies/ Perfluorocarbon nanoparticles | Fibrin clot | 2 h | 2 mL/kg; i.v. | Alternative to reconstituted-Tissue plasminogen activator. | [69] |
| Drug/Nanocarrier | Clinical Trial Types | Purpose | Indications | Benefits | Ref. |
|---|---|---|---|---|---|
| USPIONPs | N/A | Diagnostic | Atherosclerotic plaque | Noninvasive method of imaging carotid atheroma. | [132,133,134] |
| USPIONPs | N/A | Diagnostic | Acute myocardial infarction | Noninvasive method of imaging inflammatory myocytes. | [135] |
| Prednisolone phosphate/liposomes | Randomized, placebo-controlled study | Therapeutic | Inflammatory atherosclerosis | Benefiting image assisted technology | [136] |
| Silica-AuNPs | Multi-center, observational, open-label, three arms study | Therapeutic | Atherosclerosis | Application of novel invasive Plasmonic photothermal therapy using near-infrared laser irradiation. | [137] |
| LABR-312/Liposomes | Prospective, randomized, multicenter, double-blind, placebo-controlled trial | Therapeutic | Atherosclerosis | Much more effective in subjects with proinflammatory state, such as diabetes mellitus and high baseline monocyte count. | [138] |
| TriCor/Nanocrystals | FDA approved | Therapeutic | Hyperlipidemia | Tablets for oral use is available. | [161] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manners, N.; Priya, V.; Mehata, A.K.; Rawat, M.; Mohan, S.; Makeen, H.A.; Albratty, M.; Albarrati, A.; Meraya, A.M.; Muthu, M.S. Theranostic Nanomedicines for the Treatment of Cardiovascular and Related Diseases: Current Strategies and Future Perspectives. Pharmaceuticals 2022, 15, 441. https://doi.org/10.3390/ph15040441
Manners N, Priya V, Mehata AK, Rawat M, Mohan S, Makeen HA, Albratty M, Albarrati A, Meraya AM, Muthu MS. Theranostic Nanomedicines for the Treatment of Cardiovascular and Related Diseases: Current Strategies and Future Perspectives. Pharmaceuticals. 2022; 15(4):441. https://doi.org/10.3390/ph15040441
Chicago/Turabian StyleManners, Natasha, Vishnu Priya, Abhishesh Kumar Mehata, Manoj Rawat, Syam Mohan, Hafiz A. Makeen, Mohammed Albratty, Ali Albarrati, Abdulkarim M. Meraya, and Madaswamy S. Muthu. 2022. "Theranostic Nanomedicines for the Treatment of Cardiovascular and Related Diseases: Current Strategies and Future Perspectives" Pharmaceuticals 15, no. 4: 441. https://doi.org/10.3390/ph15040441