
Development of an Oral Isoliquiritigenin Self-Nano-Emulsifying Drug Delivery System (ILQ-SNEDDS) for Effective Treatment of Eosinophilic Esophagitis Induced by Food Allergy
 ,
,
Abstract
:1. Introduction
2. Results and Discussion
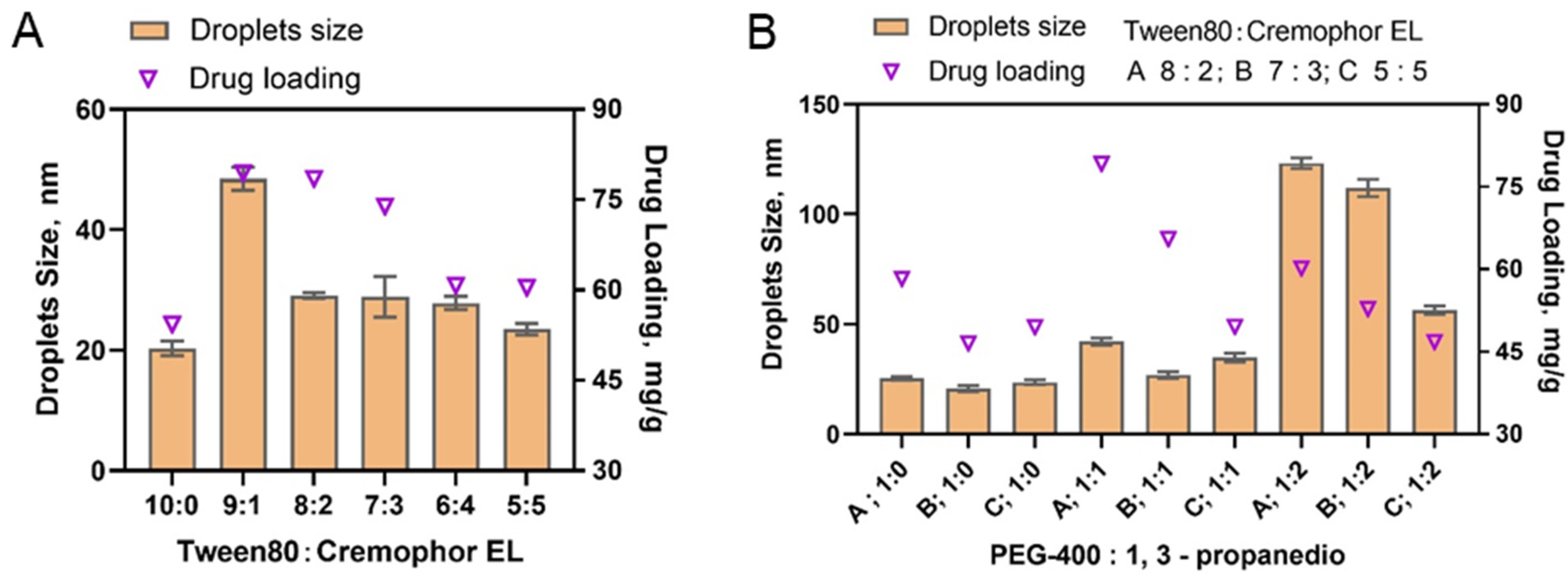
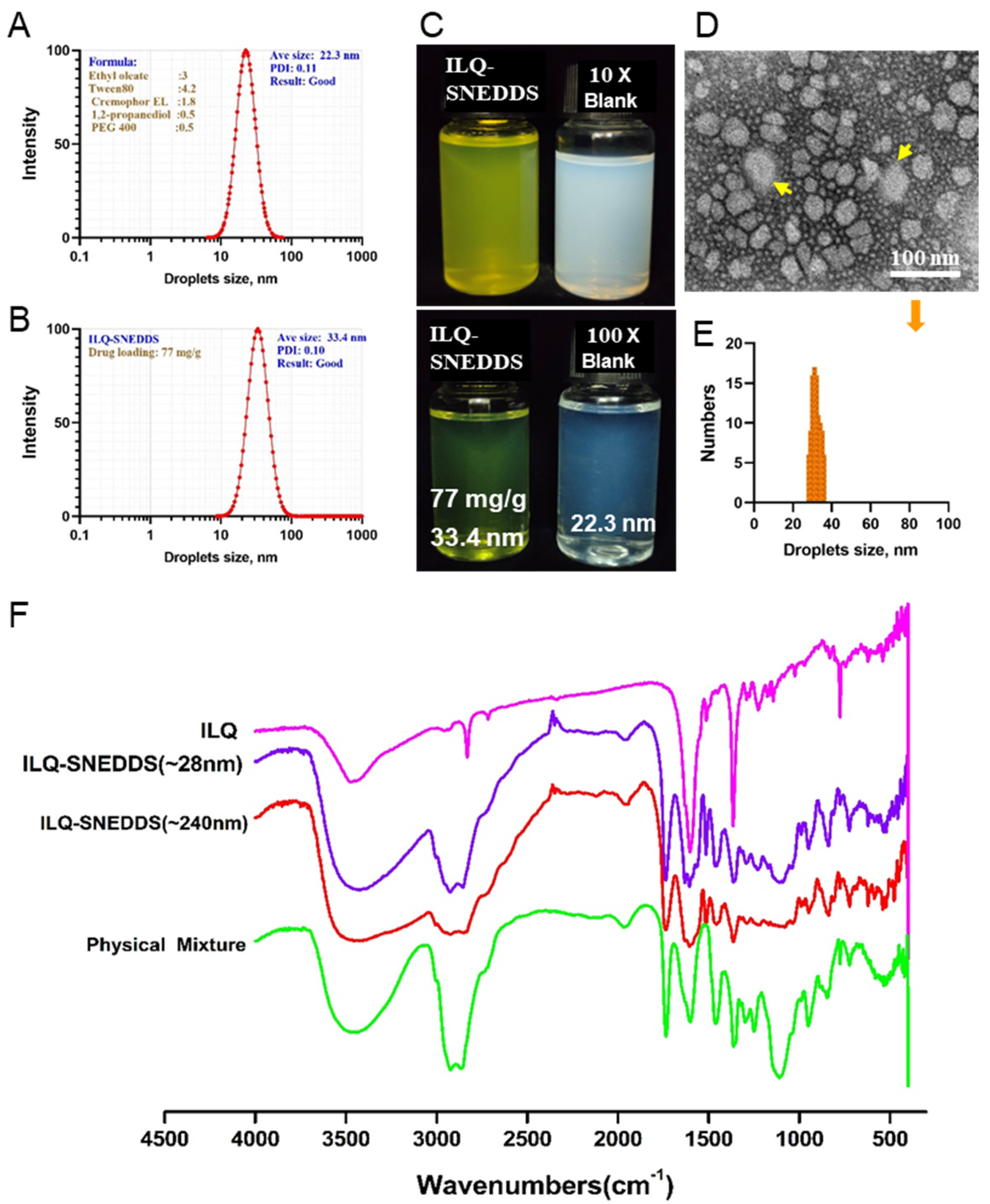
2.1. The Preparation and Characterization of ILQ-SNEDDS
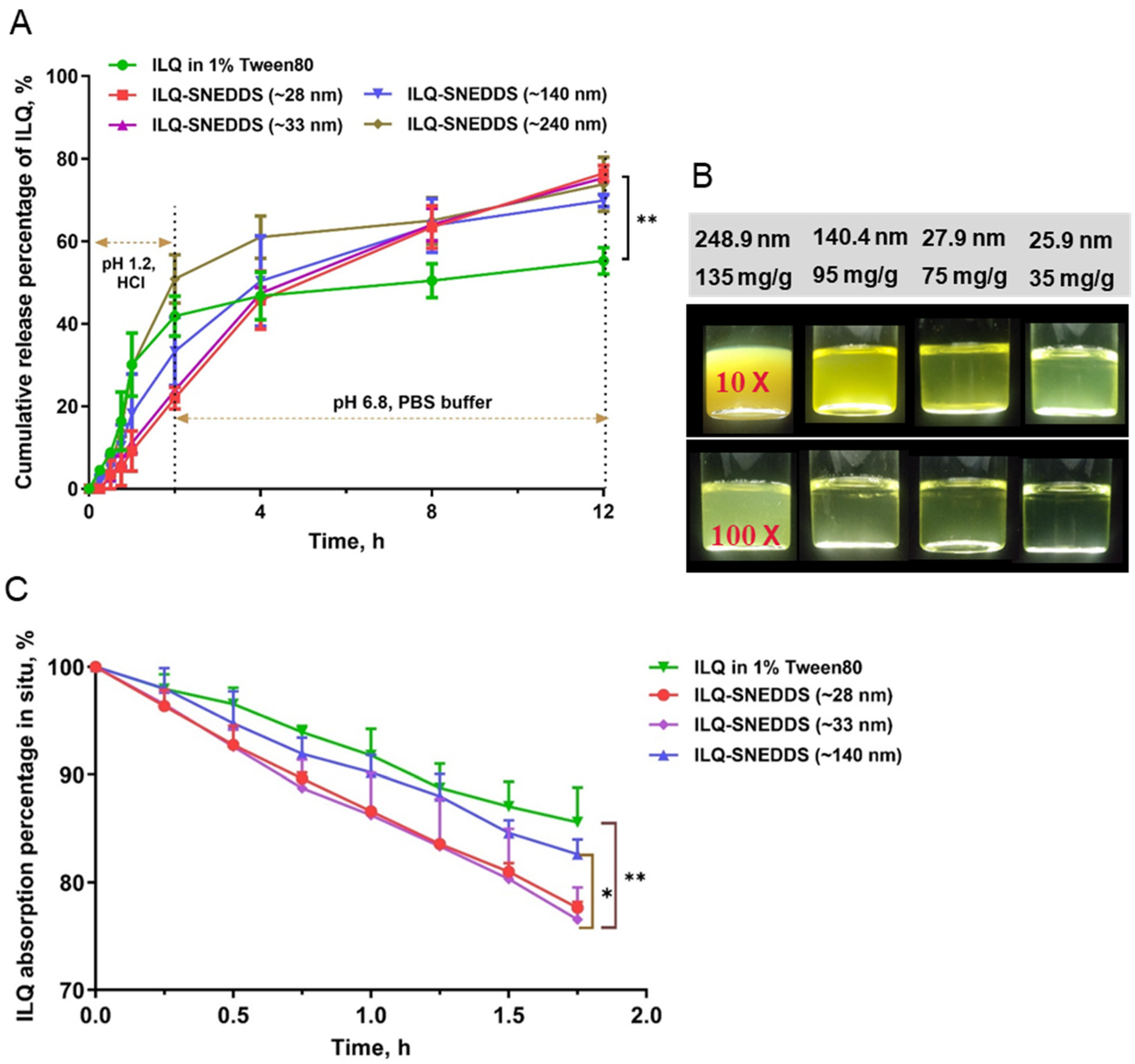
2.2. In Vitro Release Profiles and Stability of ILQ-SNEDDS
2.3. Intestinal Absorption In Situ of ILQ-SNEDDS
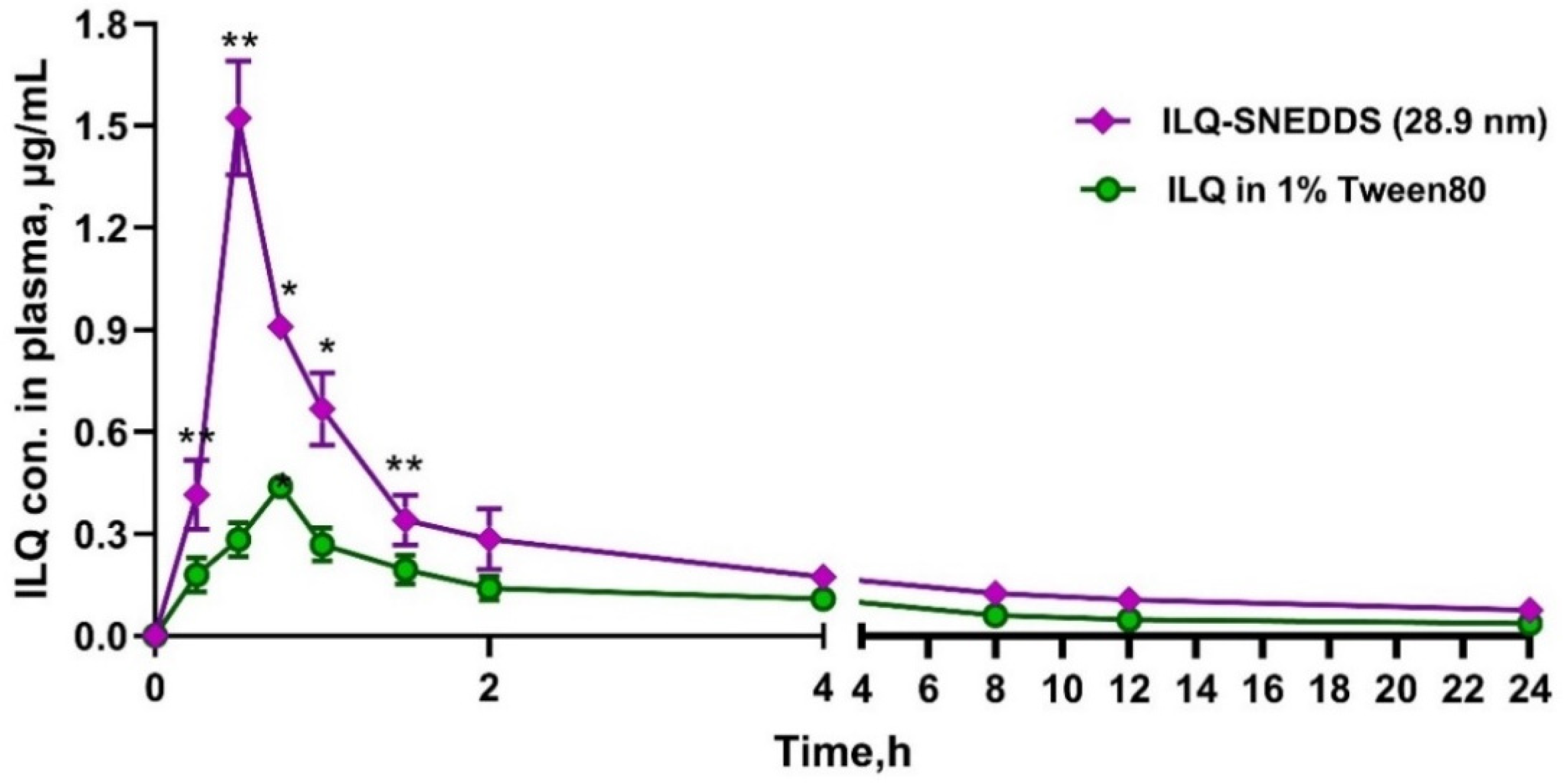
2.4. Pharmacokinetic Study of ILQ-SNEDDS
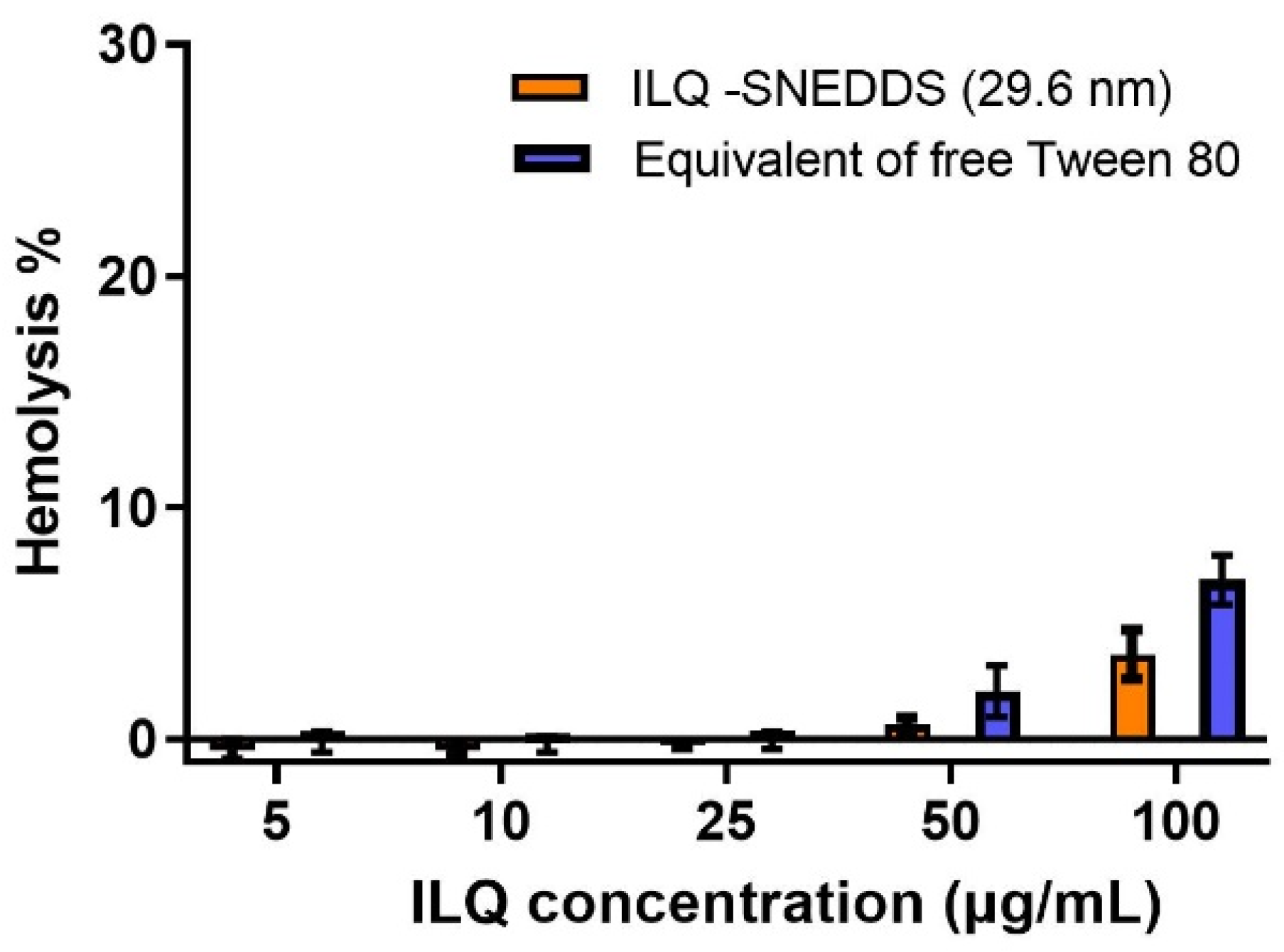
2.5. Hemolytic Toxicity of ILQ-SNEDDS
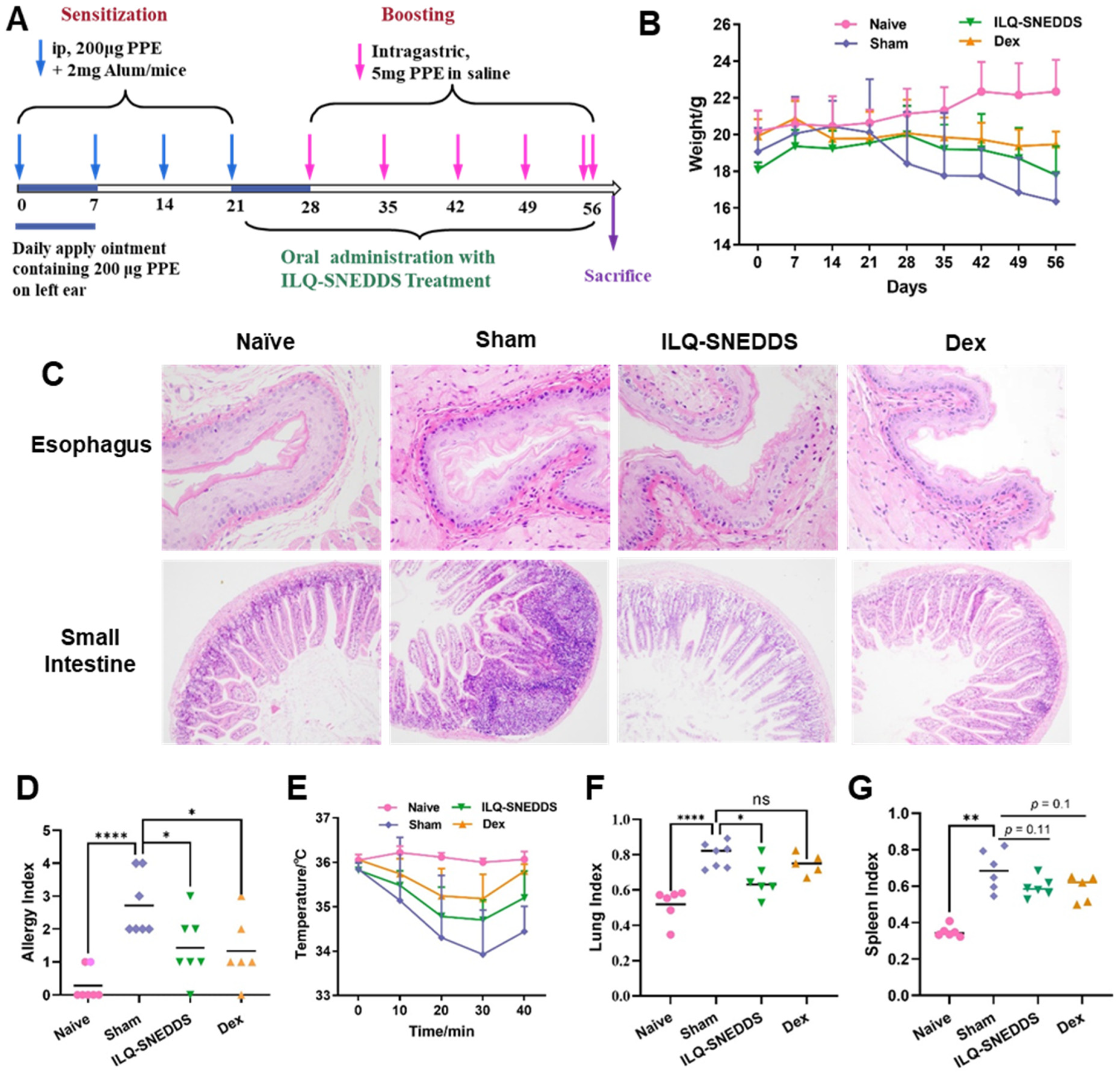
2.6. Pharmacodynamics Effects and Underlying Mechanism of ILQ-SNEDDS on EOE-Like Model Mice
2.6.1. ILQ-SNEDDS Alleviated Weight Loss and Hypothermia in EOE-Like Model Mice
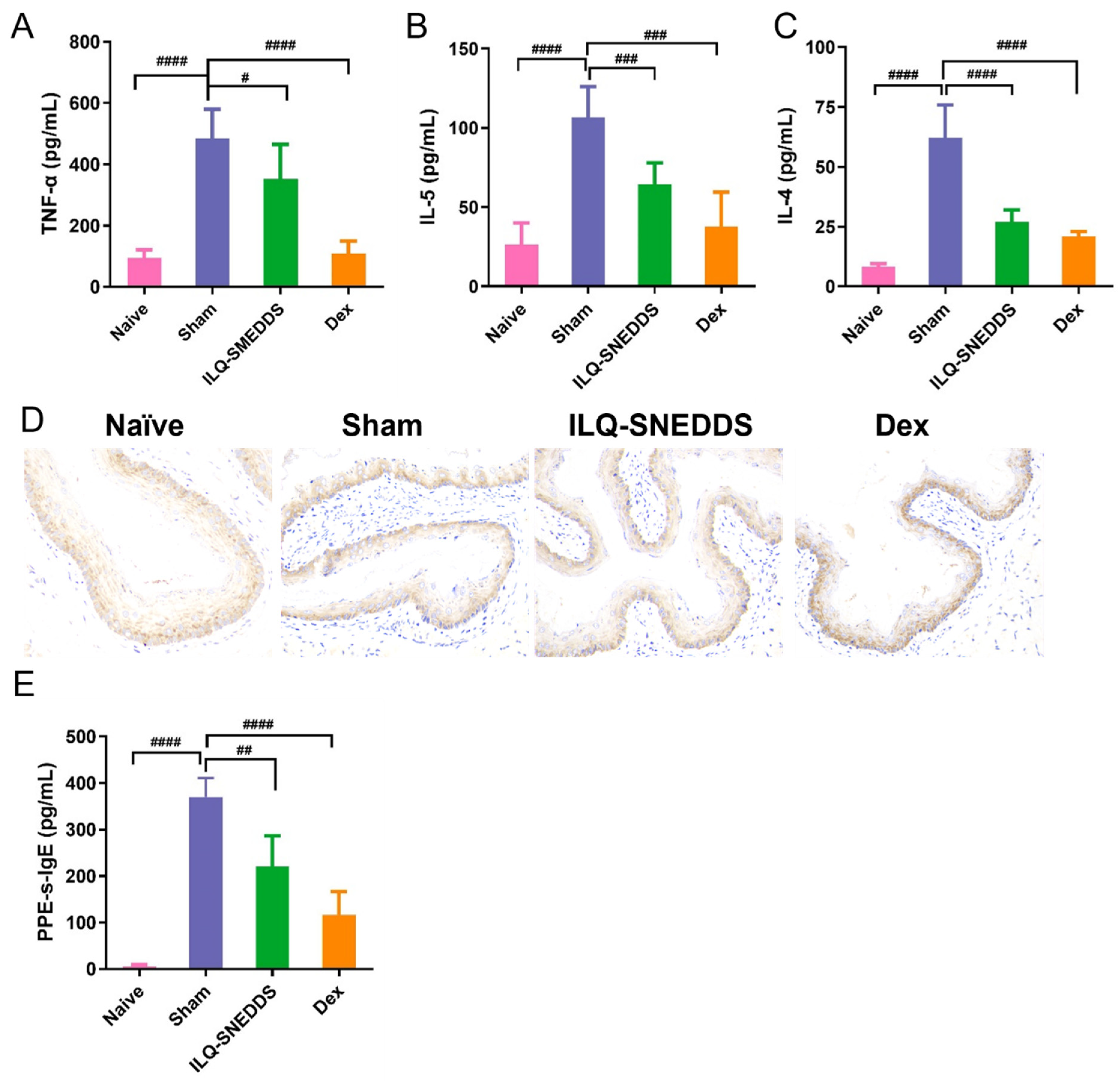
2.6.2. ILQ-SNEDDS Reduced the Levels of IL-4, IL-5 and TNF-α in Peripheral Blood of EoE-Like Model Mice
2.6.3. ILQ-SNEDDS Suppressed the Expression of TGF-β1
2.6.4. ILQ-SNEDDS Reduced PPE-s-IgE Production in Peripheral Blood of EoE-Like Model Mice
3. Materials and Methods
3.1. Animals
3.2. Preparation and Characterization of ILQ-SNEDDS
3.2.1. HPLC Method
3.2.2. Optimization, Preparation, and Characterization of the ILQ-SNEDDS
3.2.3. Stability of ILQ-SNEDDS
3.2.4. In Vitro Release Profile
3.3. Absorption In Situ and Pharmacokinetic In Vivo Studies
Intestinal Absorption In Situ
3.4. Pharmacokinetic Studies
3.5. Hemolytic Toxicity of ILQ-SNEDDS
3.6. Establishment of PPE-Induced EOE Model
3.7. Pharmacodynamic Effect Evaluation
3.8. Statistical Analysis
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lianto, P.; Han, S.; Li, X.; Ogutu, F.O.; Zhang, Y.; Fan, Z.; Che, H. Quail egg homogenate alleviates food allergy induced eosinophilic esophagitis like disease through modulating PAR-2 transduction pathway in peanut sensitized mice. Sci. Rep. 2018, 8, 1049. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dellon, E.S. Epidemiology of eosinophilic esophagitis. Gastroenterol. Clin. N. Am. 2014, 43, 201–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanikowska, A.; Hryhorowicz, S.; Rychter, A.M.; Kucharski, M.A.; Zawada, A.; Iwanik, K.; Eder, P.; Slomski, R.; Dobrowolska, A.; Krela-Kazmierczak, I. Immunogenetic, Molecular and Microbiotic Determinants of Eosinophilic Esophagitis and Clinical Practice-A New Perspective of an Old Disease. Int. J. Mol. Sci. 2021, 22, 10830. [Google Scholar] [CrossRef] [PubMed]
- Dellon, E.S.; Jensen, E.T.; Martin, C.F.; Shaheen, N.J.; Kappelman, M.D. Prevalence of eosinophilic esophagitis in the United States. Clin. Gastroenterol. Hepatol. 2014, 12, 589–596.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nhu, Q.M.; Hsieh, L.; Dohil, L.; Dohil, R.; Newbury, R.O.; Kurten, R.; Moawad, F.J.; Aceves, S.S. Antifibrotic Effects of the Thiazolidinediones in Eosinophilic Esophagitis Pathologic Remodeling: A Preclinical Evaluation. Clin. Transl. Gastroenterol. 2020, 11, e00164. [Google Scholar] [CrossRef]
- Iuliano, S.; Minelli, R.; Vincenzi, F.; Gaiani, F.; Ruberto, C.; Leandro, G.; Bizzarri, B.; Nouvenne, A.; Di Mario, F.; De’Angelis, G.L. Eosinophilic esophagitis in pediatric age, state of the art and review of the literature. Acta Biomed. 2018, 89, 20–26. [Google Scholar] [CrossRef]
- Dellon, E.S.; Kim, H.P.; Sperry, S.L.; Rybnicek, D.A.; Woosley, J.T.; Shaheen, N.J. A phenotypic analysis shows that eosinophilic esophagitis is a progressive fibrostenotic disease. Gastrointest. Endosc. 2014, 79, 577–585.e4. [Google Scholar] [CrossRef] [Green Version]
- Noti, M.; Wojno, E.D.; Kim, B.S.; Siracusa, M.C.; Giacomin, P.R.; Nair, M.G.; Benitez, A.J.; Ruymann, K.R.; Muir, A.B.; Hill, D.A.; et al. Thymic stromal lymphopoietin-elicited basophil responses promote eosinophilic esophagitis. Nat. Med. 2013, 19, 1005–1013. [Google Scholar] [CrossRef]
- Ho, S.C.; Kuo, C.T. Hesperidin, nobiletin, and tangeretin are collectively responsible for the anti-neuroinflammatory capacity of tangerine peel (Citri reticulatae pericarpium). Food Chem. Toxicol. Int. J. Publ. Br. Ind. Biol. Res. Assoc. 2014, 71, 176–182. [Google Scholar] [CrossRef]
- Salinas, E.; Reyes-Pavon, D.; Cortes-Perez, N.G.; Torres-Maravilla, E.; Bitzer-Quintero, O.K.; Langella, P.; Bermudez-Humaran, L.G. Bioactive Compounds in Food as a Current Therapeutic Approach to Maintain a Healthy Intestinal Epithelium. Microorganisms 2021, 9, 1634. [Google Scholar] [CrossRef]
- Yu, D.; Liu, X.; Zhang, G.; Ming, Z.; Wang, T. Isoliquiritigenin Inhibits Cigarette Smoke-Induced COPD by Attenuating Inflammation and Oxidative Stress via the Regulation of the Nrf2 and NF-kappaB Signaling Pathways. Front. Pharmacol. 2018, 9, 1001. [Google Scholar] [CrossRef]
- Liu, C.; Yang, N.; Chen, X.; Tversky, J.; Zhan, J.; Chehade, M.; Miller, R.L.; Li, X.M. The Flavonoid 7,4′-Dihydroxyflavone Prevents Dexamethasone Paradoxical Adverse Effect on Eotaxin Production by Human Fibroblasts. Phytother. Res. 2017, 31, 449–458. [Google Scholar] [CrossRef]
- Alshangiti, A.M.; Togher, K.L.; Hegarty, S.V.; Sullivan, A.M.; O’Keeffe, G.W. The dietary flavonoid isoliquiritigenin is a potent cytotoxin for human neuroblastoma cells. Neuronal Signal. 2019, 3, NS20180201. [Google Scholar] [CrossRef] [Green Version]
- Liu, B.; Yang, J.; Wen, Q.; Li, Y. Isoliquiritigenin, a flavonoid from licorice, relaxes guinea-pig tracheal smooth muscle in vitro and in vivo: Role of cGMP/PKG pathway. Eur. J. Pharmacol. 2008, 587, 257–266. [Google Scholar] [CrossRef]
- Yu, H.; Li, H.; Li, Y.; Li, M.; Chen, G. Effect of isoliquiritigenin for the treatment of atopic dermatitis-like skin lesions in mice. Arch. Dermatol. Res. 2017, 309, 805–813. [Google Scholar] [CrossRef]
- Jayaprakasam, B.; Doddaga, S.; Wang, R.; Holmes, D.; Goldfarb, J.; Li, X.M. Licorice flavonoids inhibit eotaxin-1 secretion by human fetal lung fibroblasts in vitro. J. Agric. Food Chem. 2009, 57, 820–825. [Google Scholar] [CrossRef] [Green Version]
- Yang, N.; Patil, S.; Zhuge, J.; Wen, M.C.; Bolleddula, J.; Doddaga, S.; Goldfarb, J.; Sampson, H.A.; Li, X.M. Glycyrrhiza uralensis flavonoids present in anti-asthma formula, ASHMI, inhibit memory Th2 responses in vitro and in vivo. Phytother. Res. 2013, 27, 1381–1391. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.K.; Chin, Y.W.; Bae, J.K.; Seo, J.S.; Choi, Y.H. Pharmacokinetics of isoliquiritigenin and its metabolites in rats: Low bioavailability is primarily due to the hepatic and intestinal metabolism. Planta Med. 2013, 79, 1656–1665. [Google Scholar] [CrossRef] [Green Version]
- Spernath, A.; Aserin, A. Microemulsions as carriers for drugs and nutraceuticals. Adv. Colloid Interface Sci. 2006, 128–130, 47–64. [Google Scholar] [CrossRef]
- Korolev, D.; Shumilo, M.; Shulmeyster, G.; Krutikov, A.; Golovkin, A.; Mishanin, A.; Gorshkov, A.; Spiridonova, A.; Domorad, A.; Krasichkov, A.; et al. Hemolytic Activity, Cytotoxicity, and Antimicrobial Effects of Human Albumin- and Polysorbate-80-Coated Silver Nanoparticles. Nanomaterials 2021, 11, 1484. [Google Scholar] [CrossRef]
- Liu, W.; Liu, J.; Salt, L.J.; Ridout, M.J.; Han, J.; Wilde, P.J. Structural stability of liposome-stabilized oil-in-water pickering emulsions and their fate during in vitro digestion. Food Funct. 2019, 10, 7262–7274. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.; Singh, S.K.; Verma, P.R. Fabrication of lipidic nanocarriers of loratadine for facilitated intestinal permeation using multivariate design approach. Drug Dev. Ind. Pharm. 2016, 42, 288–306. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, N.; Parikh, A.; Dewangan, R.P.; Biswas, L.; Verma, A.K.; Mittal, S.; Ali, J.; Garg, S.; Baboota, S. Solid Self-Nano Emulsifying Nanoplatform Loaded with Tamoxifen and Resveratrol for Treatment of Breast Cancer. Pharmaceutics 2022, 14, 1486. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Liu, C.S.; Chen, Q.Z.; Wang, S.; Xiong, Y.A.; Jing, J.; Lv, J.J. Characterization, pharmacokinetics and tissue distribution of chlorogenic acid-loaded self-microemulsifying drug delivery system. Eur. J. Pharm. Sci. 2017, 100, 102–108. [Google Scholar] [CrossRef] [PubMed]
- Sawatdee, S.; Atipairin, A.; Sae Yoon, A.; Srichana, T.; Changsan, N.; Suwandecha, T. Formulation Development of Albendazole-Loaded Self-Microemulsifying Chewable Tablets to Enhance Dissolution and Bioavailability. Pharmaceutics 2019, 11, 134. [Google Scholar] [CrossRef]
- Zhang, X.; Qiao, H.; Zhang, T.; Shi, Y.; Ni, J. Enhancement of gastrointestinal absorption of isoliquiritigenin by nanostructured lipid carrier. Adv. Powder Technol. 2014, 25, 1060–1068. [Google Scholar] [CrossRef]
- Han, W.; Xie, B.; Li, Y.; Shi, L.; Wan, J.; Chen, X.; Wang, H. Orally Deliverable Nanotherapeutics for the Synergistic Treatment of Colitis-Associated Colorectal Cancer. Theranostics 2019, 9, 7458–7473. [Google Scholar] [CrossRef]
- Singh, A.; Thakur, S.; Singh, H.; Singh, H.; Kaur, S.; Kaur, S.; Dudi, R.; Mondhe, D.M.; Jain, S.K. Novel Vitamin E TPGS based docetaxel nanovesicle formulation for its safe and effective parenteral delivery: Toxicological, pharmacokinetic and pharmacodynamic evaluation. J. Liposome Res. 2021, 31, 365–380. [Google Scholar] [CrossRef]
- Cao, M.; Zhan, M.; Wang, Z.; Wang, Z.; Li, X.M.; Miao, M. Development of an Orally Bioavailable Isoliquiritigenin Self-Nanoemulsifying Drug Delivery System to Effectively Treat Ovalbumin-Induced Asthma. Int. J. Nanomed. 2020, 15, 8945–8961. [Google Scholar] [CrossRef]
- Hill, D.A.; Grundmeier, R.W.; Ramos, M.; Spergel, J.M. Eosinophilic Esophagitis Is a Late Manifestation of the Allergic March. J. Allergy Clin. Immunology. Pract. 2018, 6, 1528–1533. [Google Scholar] [CrossRef]
- Spergel, J.; Aceves, S.S. Allergic components of eosinophilic esophagitis. J. Allergy Clin. Immunol. 2018, 142, 1–8. [Google Scholar] [CrossRef]
- Blanchard, C.; Simon, D.; Schoepfer, A.; Straumann, A.; Simon, H.U. Eosinophilic esophagitis: Unclear roles of IgE and eosinophils. J. Intern. Med. 2017, 281, 448–457. [Google Scholar] [CrossRef]
- Liu, C.; Yang, N.; Song, Y.; Wang, L.; Zi, J.; Zhang, S.; Dunkin, D.; Busse, P.; Weir, D.; Tversky, J.; et al. Ganoderic acid C1 isolated from the anti-asthma formula, ASHMI suppresses TNF-alpha production by mouse macrophages and peripheral blood mononuclear cells from asthma patients. Int. Immunopharmacol. 2015, 27, 224–231. [Google Scholar] [CrossRef] [Green Version]
- Cho, J.Y.; Doshi, A.; Rosenthal, P.; Beppu, A.; Miller, M.; Aceves, S.; Broide, D. Smad3-deficient mice have reduced esophageal fibrosis and angiogenesis in a model of egg-induced eosinophilic esophagitis. J. Pediatr. Gastroenterol. Nutr. 2014, 59, 10–16. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, N.; Fernando, S.D.; Biette, K.A.; Hammer, J.A.; Capocelli, K.E.; Kitzenberg, D.A.; Glover, L.E.; Colgan, S.P.; Furuta, G.T.; Masterson, J.C. TGF-β1 alters esophageal epithelial barrier function by attenuation of claudin-7 in eosinophilic esophagitis. Mucosal Immunol. 2018, 11, 415–426. [Google Scholar] [CrossRef] [Green Version]
- Rieder, F.; Nonevski, I.; Ma, J.; Ouyang, Z.; West, G.; Protheroe, C.; DePetris, G.; Schirbel, A.; Lapinski, J.; Goldblum, J.; et al. T-helper 2 cytokines, transforming growth factor beta1, and eosinophil products induce fibrogenesis and alter muscle motility in patients with eosinophilic esophagitis. Gastroenterology 2014, 146, 1266–1277.e9. [Google Scholar] [CrossRef] [Green Version]
- Javed, R.; Ghonaim, R.; Shathili, A.; Khalifa, S.A.; El-Seedi, H.R. Phytonanotechnology: A greener approach for biomedical applications. In Biogenic Nanoparticles for Cancer Theranostics; Elsevier: Amsterdam, The Netherlands, 2021; pp. 43–86. [Google Scholar] [CrossRef]
- Moawad, F.J.; Dellon, E.S.; Achem, S.R.; Ljuldjuraj, T.; Green, D.J.; Maydonovitch, C.L.; Brizuela, D.R.; Gupta, S.K.; Chehade, M. Effects of Race and Sex on Features of Eosinophilic Esophagitis. Clin. Gastroenterol. Hepatol. 2016, 14, 23–30. [Google Scholar] [CrossRef]
- Takeda, M.; Tanabe, M.; Ito, W.; Ueki, S.; Konnno, Y.; Chihara, M.; Itoga, M.; Kobayashi, Y.; Moritoki, Y.; Kayaba, H.; et al. Gender difference in allergic airway remodelling and immunoglobulin production in mouse model of asthma. Respirology 2013, 18, 797–806. [Google Scholar] [CrossRef]
- Rossi, A.; Roviezzo, F.; Sorrentino, R.; Riemma, M.A.; Cerqua, I.; Bilancia, R.; Spaziano, G.; Troisi, F.; Pace, S.; Pinto, A.; et al. Leukotriene-mediated sex dimorphism in murine asthma-like features during allergen sensitization. Pharmacol. Res. 2019, 139, 182–190. [Google Scholar] [CrossRef]
- Kralovicova, J.; Bartunek, A.; Hofmann, J.; Krizek, T.; Kozlik, P.; Rousarova, J.; Rysanek, P.; Sima, M.; Slanar, O. Pharmacokinetic Variability in Pre-Clinical Studies: Sample Study with Abiraterone in Rats and Implications for Short-Term Comparative Pharmacokinetic Study Designs. Pharmaceutics 2022, 14, 643. [Google Scholar] [CrossRef]
- Zhang, K.; Wang, Q.; Yang, Q.; Wei, Q.; Man, N.; Adu-Frimpong, M.; Toreniyazov, E.; Ji, H.; Yu, J.; Xu, X. Enhancement of Oral Bioavailability and Anti-hyperuricemic Activity of Isoliquiritigenin via Self-Microemulsifying Drug Delivery System. AAPS PharmSciTech 2019, 20, 218. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zhao, X.; Ma, Y.; Zhai, G.; Li, L.; Lou, H. Enhancement of gastrointestinal absorption of quercetin by solid lipid nanoparticles. J. Control. Release 2009, 133, 238–244. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.; Zou, Y.; Chen, L.; Xu, Y.; Wang, S. Development and In Vivo Evaluation of Ziyuglycoside I-Loaded Self-Microemulsifying Formulation for Activity of Increasing Leukocyte. AAPS PharmSciTech 2019, 20, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greco, I.; Molchanova, N.; Holmedal, E.; Jenssen, H.; Hummel, B.D.; Watts, J.L.; Hakansson, J.; Hansen, P.R.; Svenson, J. Correlation between hemolytic activity, cytotoxicity and systemic in vivo toxicity of synthetic antimicrobial peptides. Sci. Rep. 2020, 10, 13206. [Google Scholar] [CrossRef]
- Harris, M.B.; Chang, C.C.; Berton, M.T.; Danial, N.N.; Zhang, J.; Kuehner, D.; Ye, B.H.; Kvatyuk, M.; Pandolfi, P.P.; Cattoretti, G.; et al. Transcriptional Repression of Stat6-Dependent Interleukin-4-Induced Genes by BCL-6: Specific Regulation of Iɛ Transcription and Immunoglobulin E Switching. Mol. Cell. Biol. 1999, 19, 7264–7275. [Google Scholar] [CrossRef] [Green Version]
- Cao, M.; Liu, C.; Srivastava, K.D.; Lin, A.; Lazarski, C.; Wang, L.; Maskey, A.; Song, Y.; Chen, X.; Yang, N.; et al. Anti-IgE effect of small-molecule-compound arctigenin on food allergy in association with a distinct transcriptome profile. Clin. Exp. Allergy 2022, 52, 250–264. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Num | Factor A | Factor B | Factor C | Drug Loading mg/g | Ave Size (nm) | Ave PDI | ζ Potential (mV) |
|---|---|---|---|---|---|---|---|
| 1 | 25% | 9:1 | 6 | 52.59 | 19.14 | 0.160 | −6.74 |
| 2 | 25% | 8:2 | 2.5 | 76.06 | 237.3 | 0.231 | −5.28 |
| 3 | 25% | 7:3 | 3.7 | 31.92 | 16.89 | 0.152 | −9.27 |
| 4 | 30% | 9:1 | 2.5 | 51.41 | 11.99 | 0.159 | −8.34 |
| 5 | 30% | 8:2 | 3.7 | 44.4 | 15.21 | 0.115 | −8.61 |
| 6 | 30% | 7:3 | 6 | 73.06 | 28.39 | 0.178 | −10.11 |
| 7 | 35% | 9:1 | 3.7 | 46.3 | 29.63 | 0.200 | −9.79 |
| 8 | 35% | 8:2 | 6 | 37.53 | 13.25 | 0.158 | −3.47 |
| 9 | 35% | 7:3 | 2.5 | 54.88 | 190.06 | 0.204 | −4.39 |
| Levels | A | B | C | ||||
| 1 | 53.52 | 50.10 | 56.03 | ||||
| 2 | 57.93 | 52.66 | 40.87 | ||||
| 3 | 46.24 | 54.93 | 60.78 | ||||
| R | 11.69 | 4.83 | 19.91 | ||||
| Ranking | 2 | 3 | 1 |
| Items | Droplet Size (nm) | PDI | ζ-Potential (mV) | |
|---|---|---|---|---|
| Freshly prepared (0 day) | 27.93 | 0.151 | −9.84 | |
| Dilution with pH 6.8 PBS | 28.85 | 0.191 | / | |
| Dilution with 0.01 M HCl | 28.33 | 0.204 | / | |
| 1 month | at 4 °C | 28.89 | 0.206 | −8.34 |
| at 37 °C | 29.30 | 0.211 | −8.35 | |
| 2 months | at 4 °C | 140.41 | 0.224 | −8.12 |
| at 37 °C | 241.48 | 0.237 | −4.41 | |
| Items | Globule Size and Drug Loading | Ap/% | Ka/h−1 | Papp·10−4/h−1·cm2 | Enhancement Ratio |
|---|---|---|---|---|---|
| ILQ-SNEDDS | 28.9 nm (35 mg/g) | 22.02 ± 0.39 | 0.144 ± 0.0043 | 29.58 ± 2.03 | 1.61 |
| 33.6 nm (75 mg/g) | 23.45 ± 2.96 | 0.149 ± 0.0060 | 30.97 ± 4.49 | 1.69 | |
| 140.4 nm (95 mg/g) | 17.39 ± 1.34 | 0.104 ± 0.0107 | 20.14 ± 2.46 | 1.10 | |
| ILQ suspension | - | 14.43 ± 3.27 | 0.086 ± 0.0080 | 18.34 ± 2.86 | 1.00 |
| Items | Free ILQ Suspension | ILQ-SNEDDS |
|---|---|---|
| Ke, h−1 | 0.4 ± 0.01 | 0.36 ± 0.01 |
| t1/2, h | 1.79 ± 4.12 | 2.12 ± 6.87 |
| Tmax, h | 0.75 ± 0.00 | 0.5 ± 0.00 * |
| Cmax, μg/mL | 0.43 ± 0.02 | 1.52 ± 0.13 * |
| AUC0–24, μg/mL·h | 1.86 ± 0.12 | 3.76 ± 0.38 * |
| Vz/F, L | 320.32 ± 56.30 | 170.11 ± 13.11 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cao, M.; Wang, Y.; Jing, H.; Wang, Z.; Meng, Y.; Geng, Y.; Miao, M.; Li, X.-M. Development of an Oral Isoliquiritigenin Self-Nano-Emulsifying Drug Delivery System (ILQ-SNEDDS) for Effective Treatment of Eosinophilic Esophagitis Induced by Food Allergy. Pharmaceuticals 2022, 15, 1587. https://doi.org/10.3390/ph15121587
Cao M, Wang Y, Jing H, Wang Z, Meng Y, Geng Y, Miao M, Li X-M. Development of an Oral Isoliquiritigenin Self-Nano-Emulsifying Drug Delivery System (ILQ-SNEDDS) for Effective Treatment of Eosinophilic Esophagitis Induced by Food Allergy. Pharmaceuticals. 2022; 15(12):1587. https://doi.org/10.3390/ph15121587
Chicago/Turabian StyleCao, Mingzhuo, Yuan Wang, Heyun Jing, Zeqian Wang, Yijia Meng, Yu Geng, Mingsan Miao, and Xiu-Min Li. 2022. "Development of an Oral Isoliquiritigenin Self-Nano-Emulsifying Drug Delivery System (ILQ-SNEDDS) for Effective Treatment of Eosinophilic Esophagitis Induced by Food Allergy" Pharmaceuticals 15, no. 12: 1587. https://doi.org/10.3390/ph15121587