
Hyaluronic Acid and Radiofrequency in Patients with Urogenital Atrophy and Vaginal Laxity
 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Hyaluronic Acid
2.2. Radiofrequency (RF)
2.3. Histochemical Analysis
3. Results
3.1. Outcome Measures and Statistic Evaluation
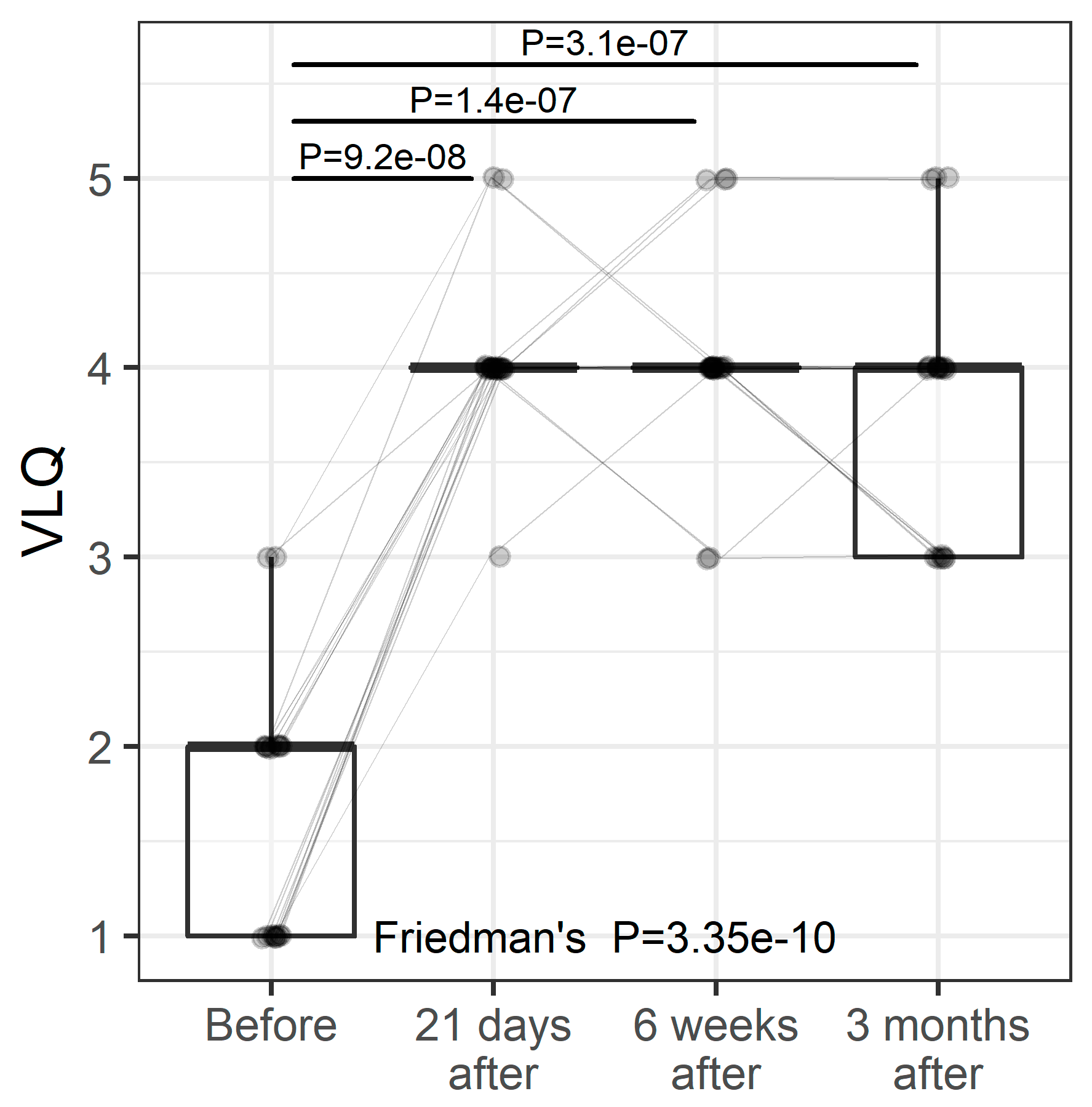
3.2. VL
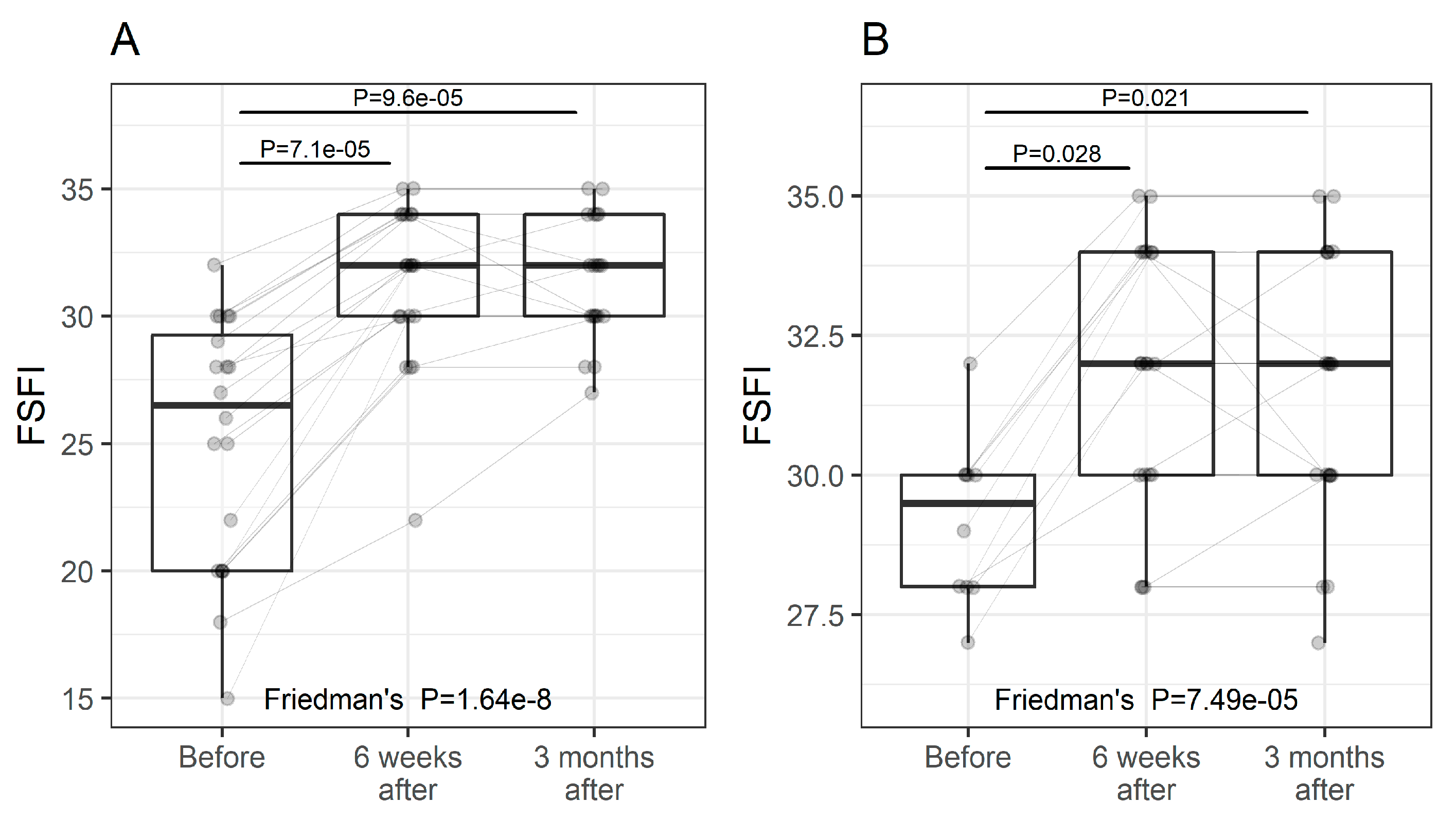
3.3. FSFI
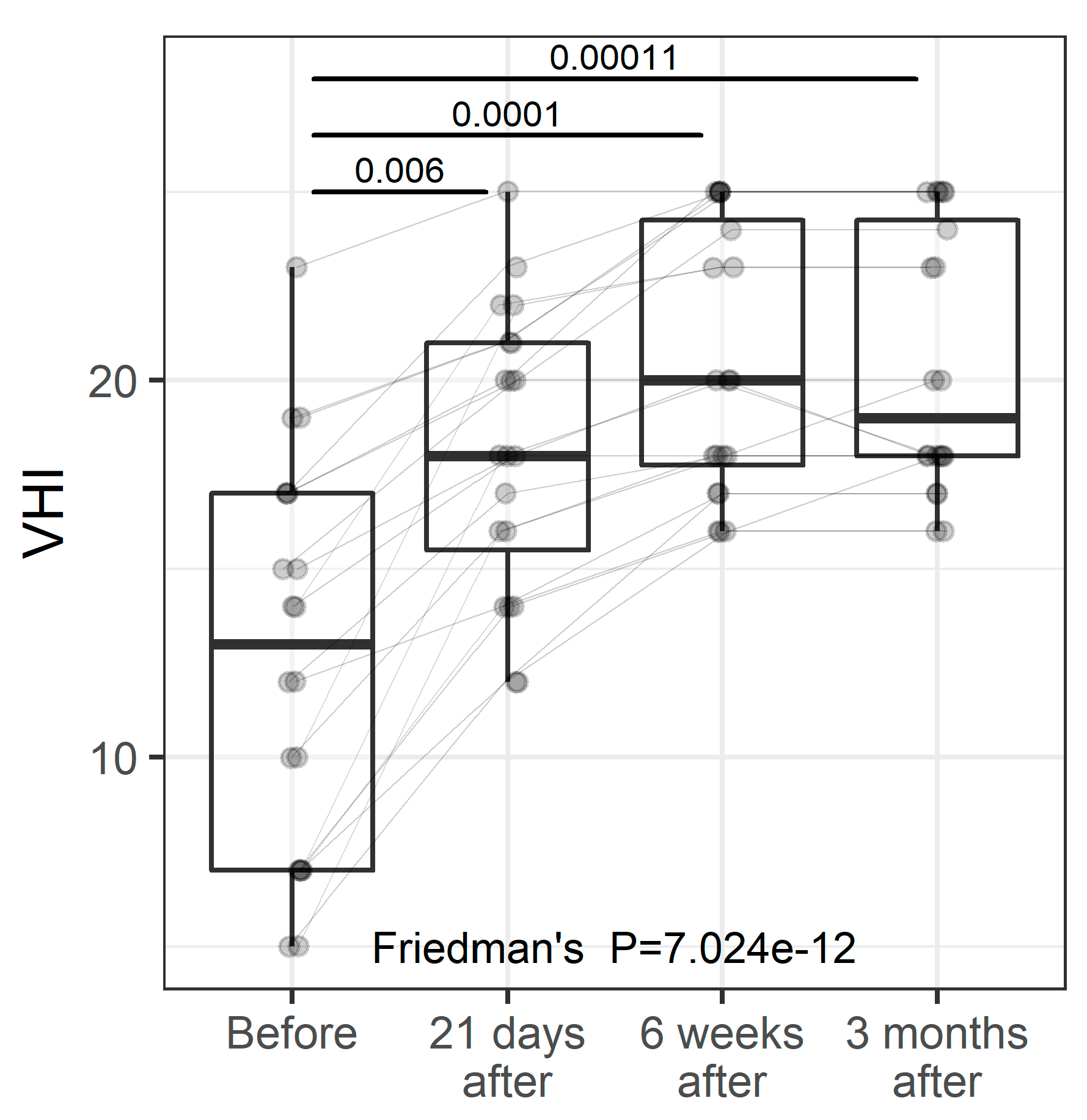
3.4. VHI
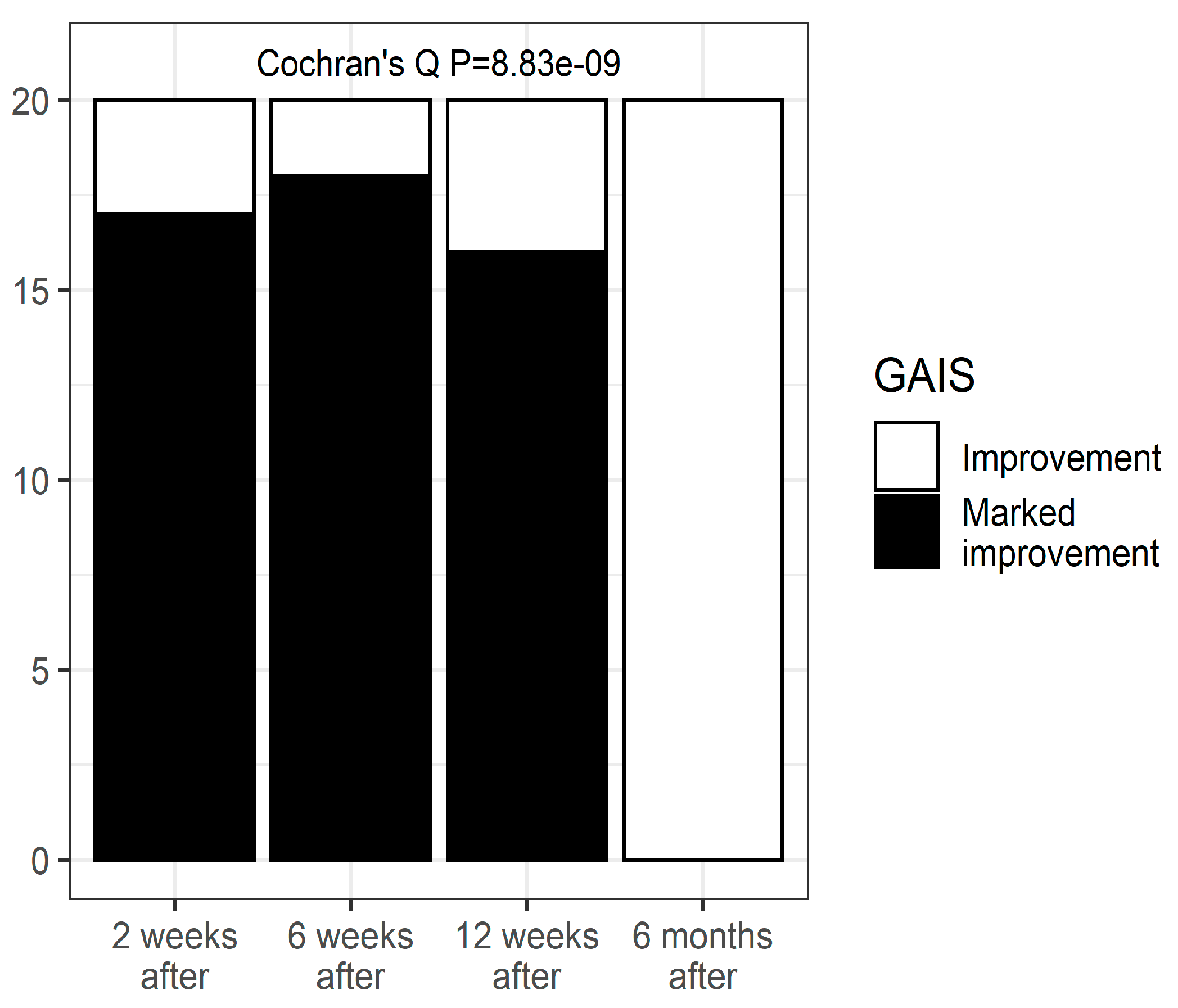
3.5. GAIS
 |  |
| Clinical case 1 before and after the procedure. | |
 |  |
| Clinical case 2, before the and after the procedure. | |
 |  |
| Clinical case 3, before and after the procedure. | |
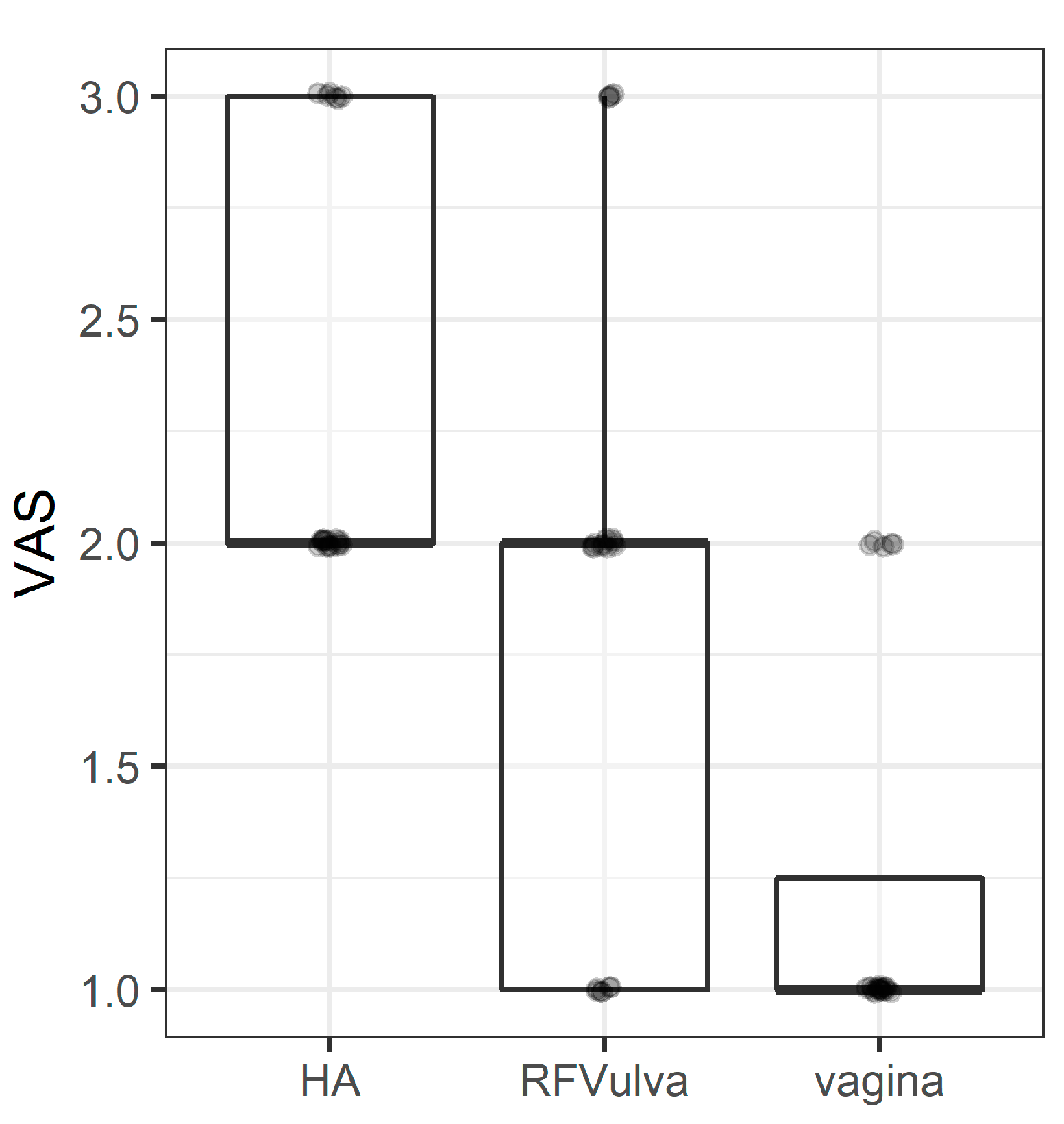
3.6. VAS
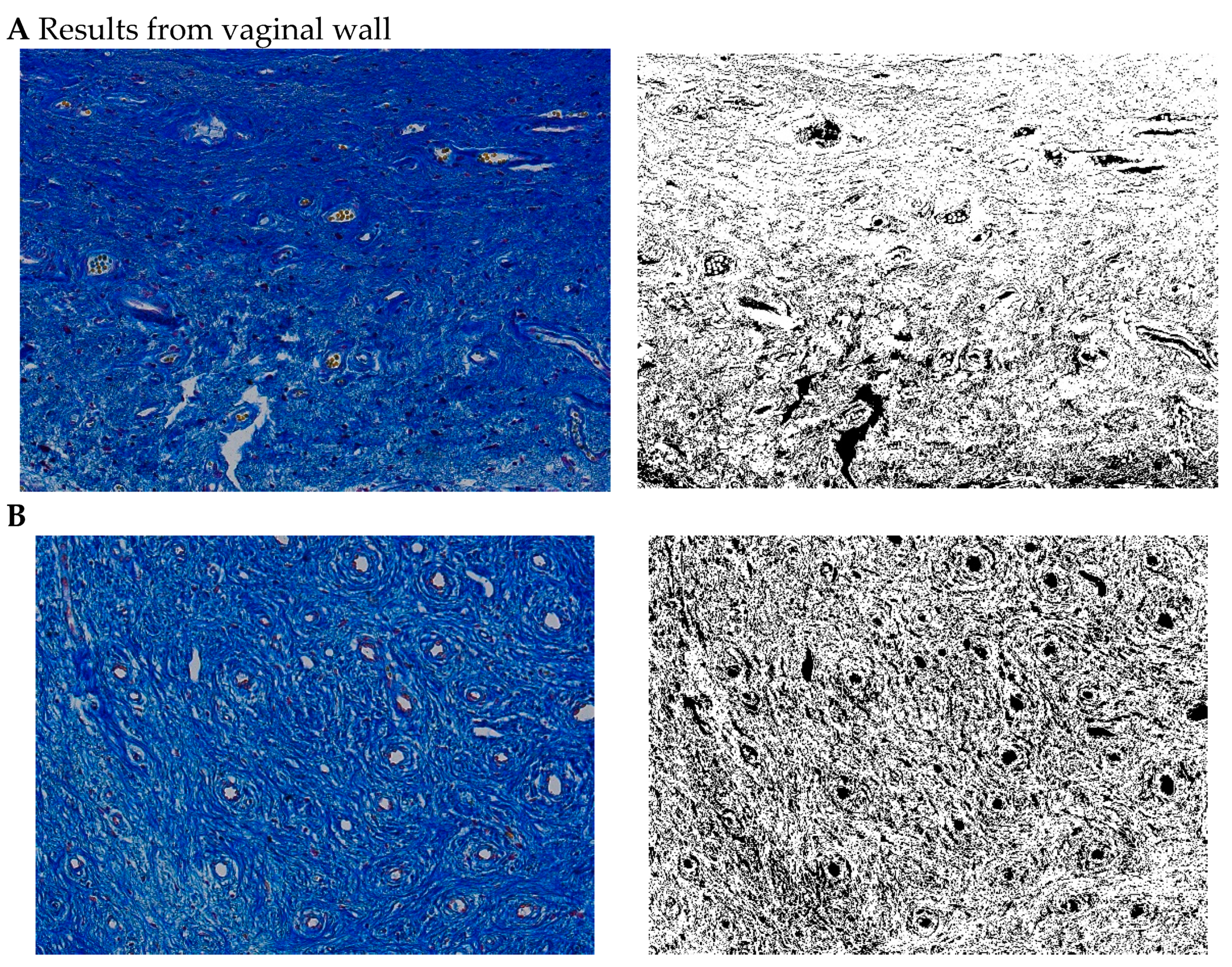
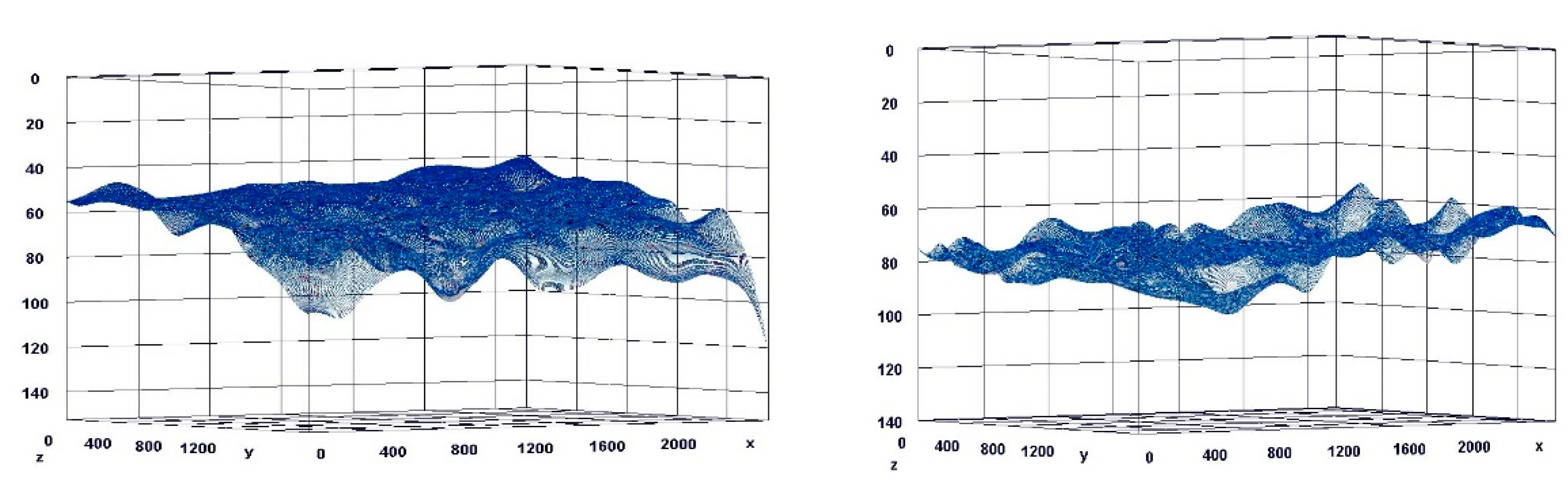
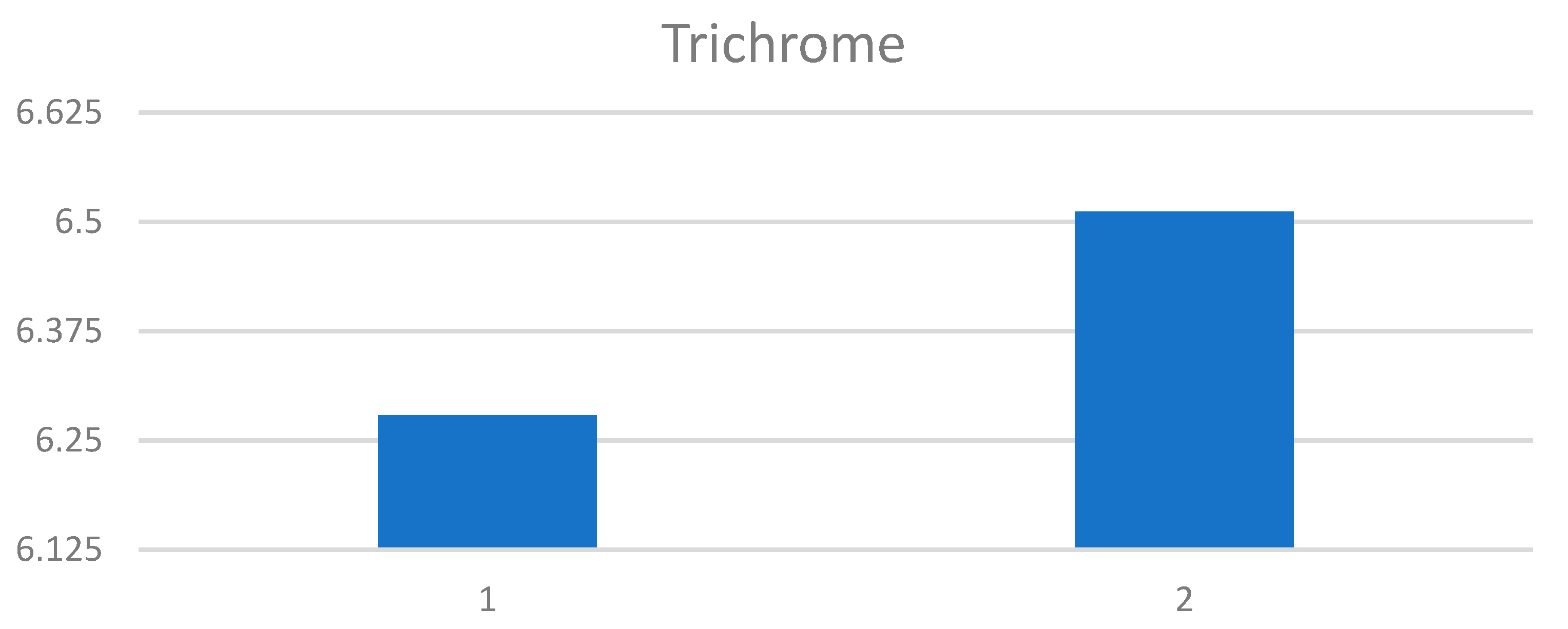
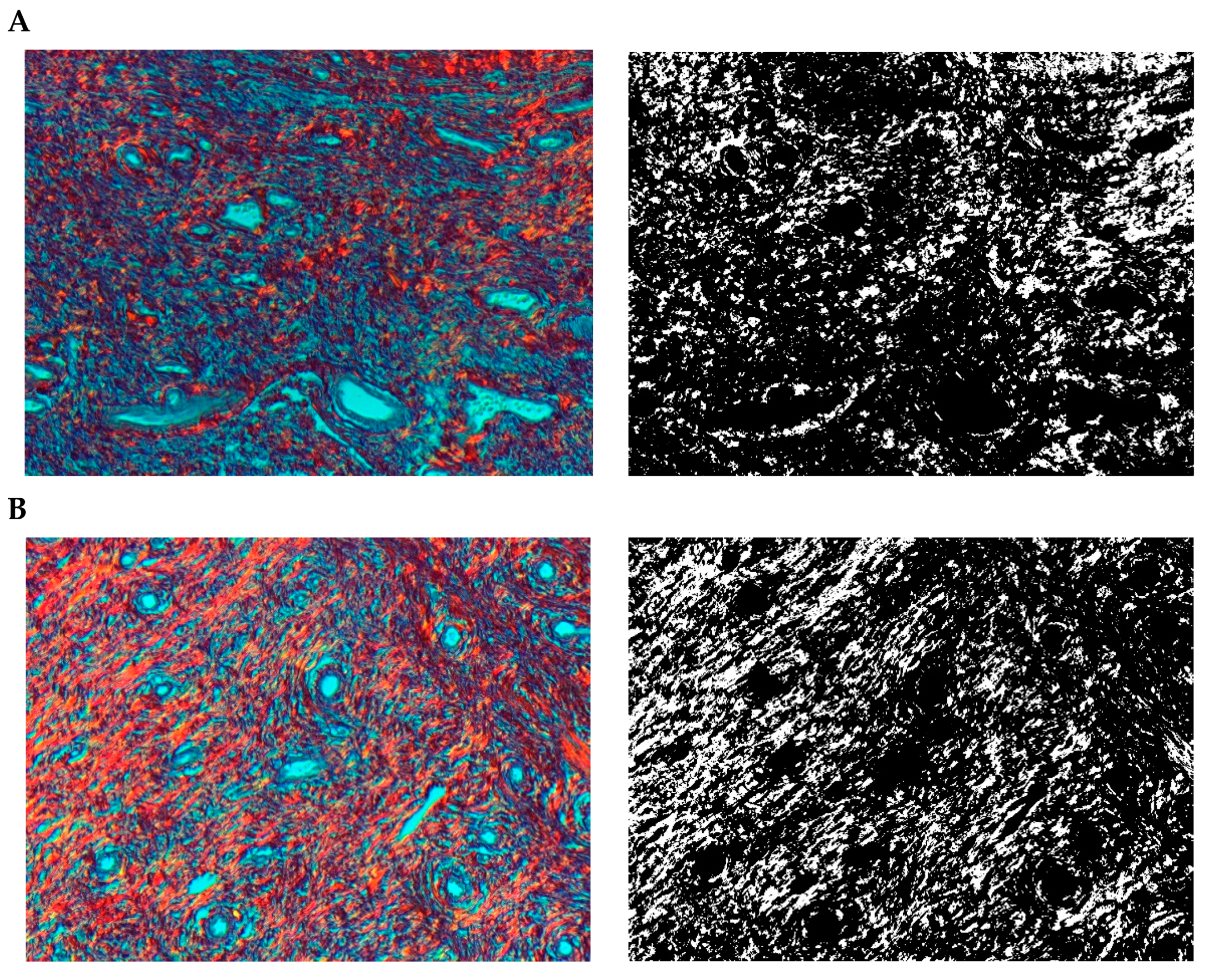
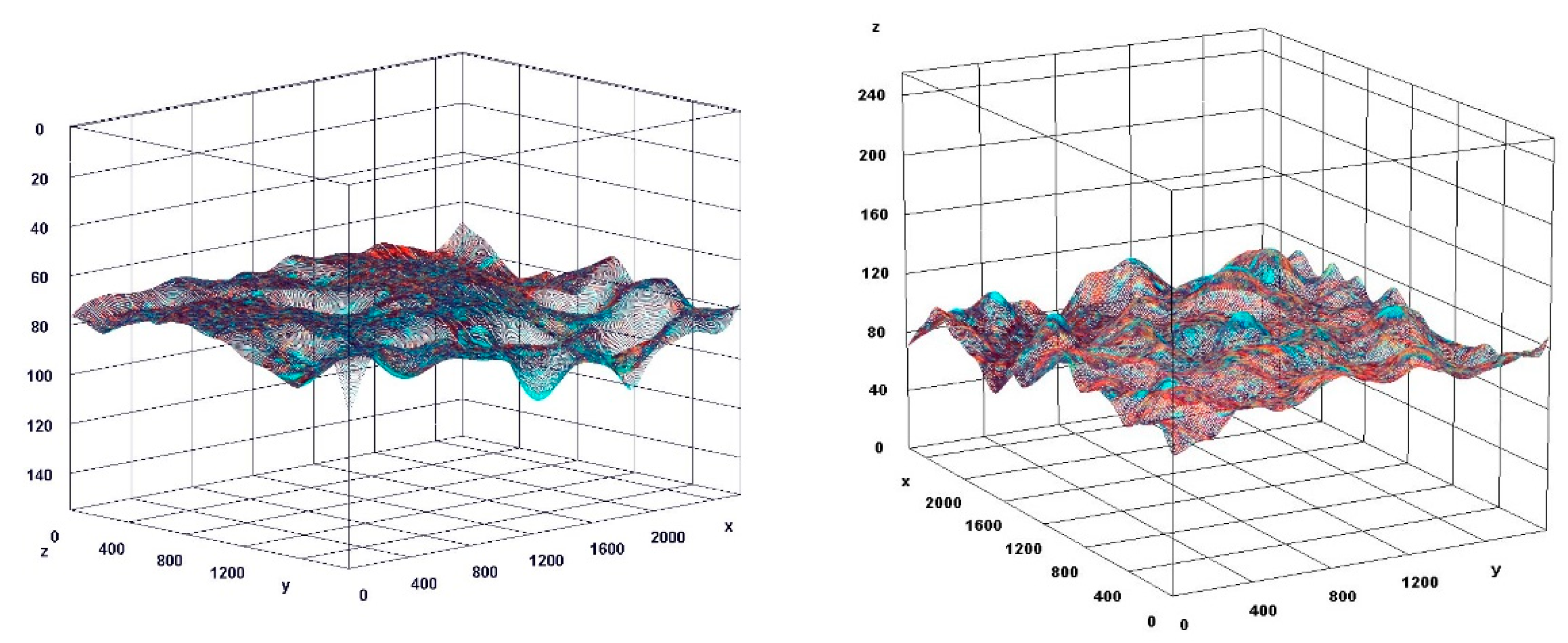
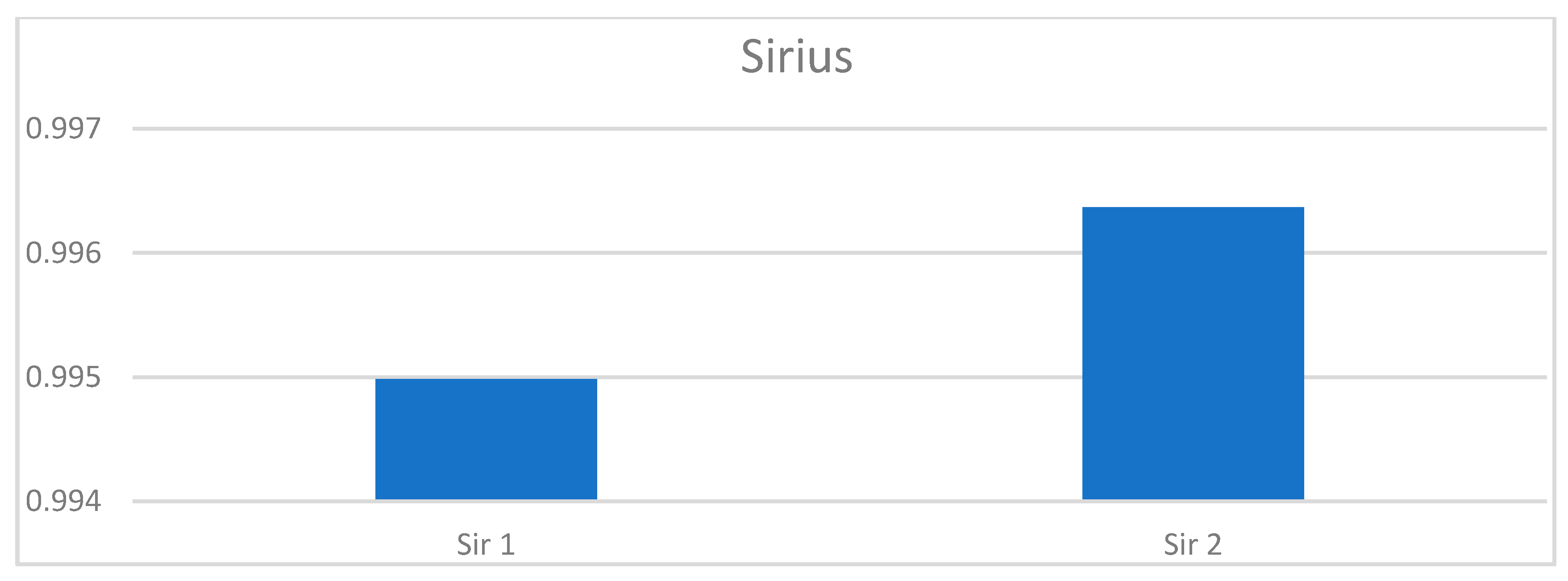
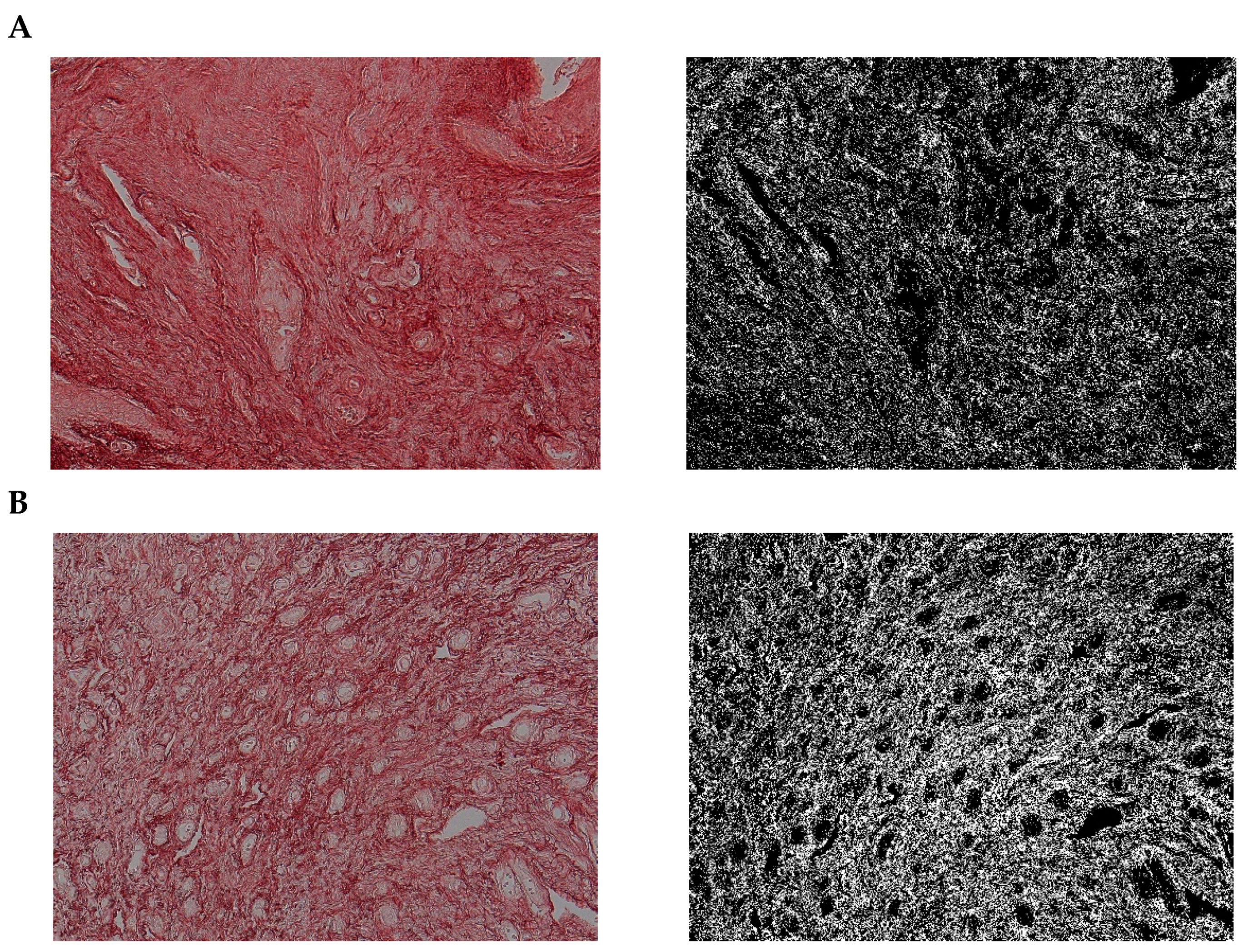
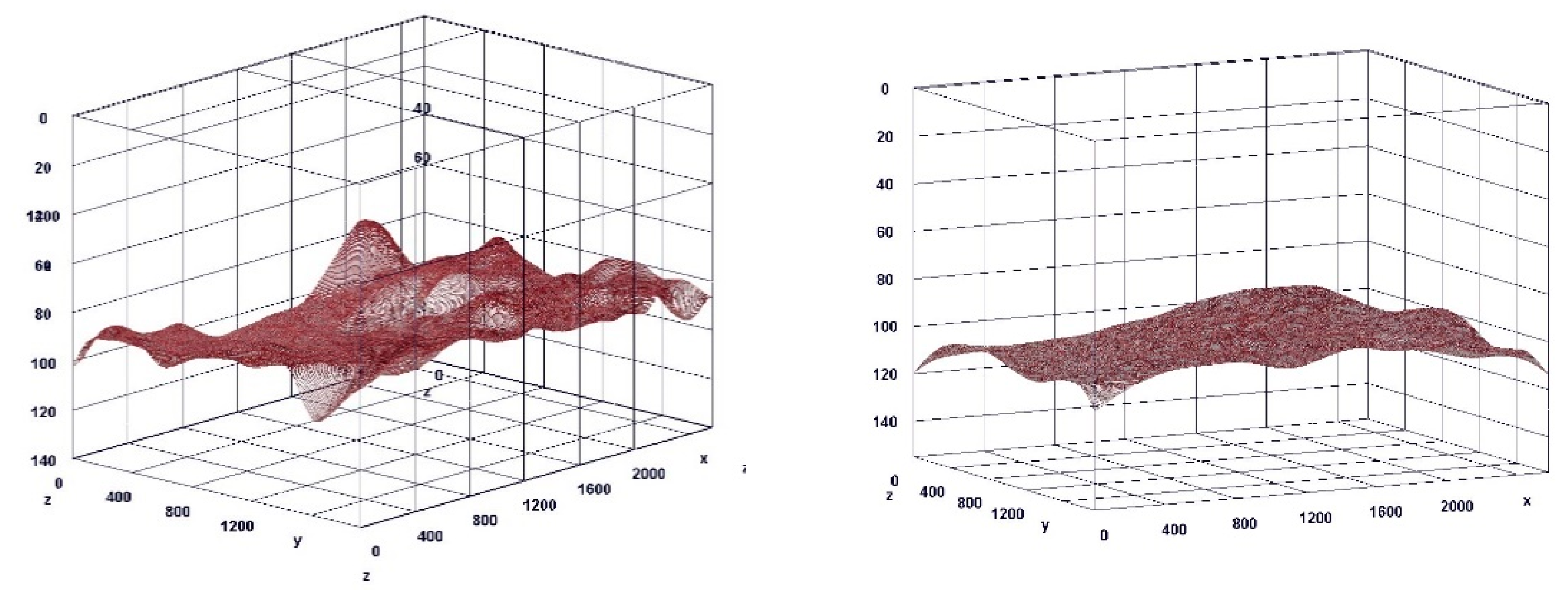
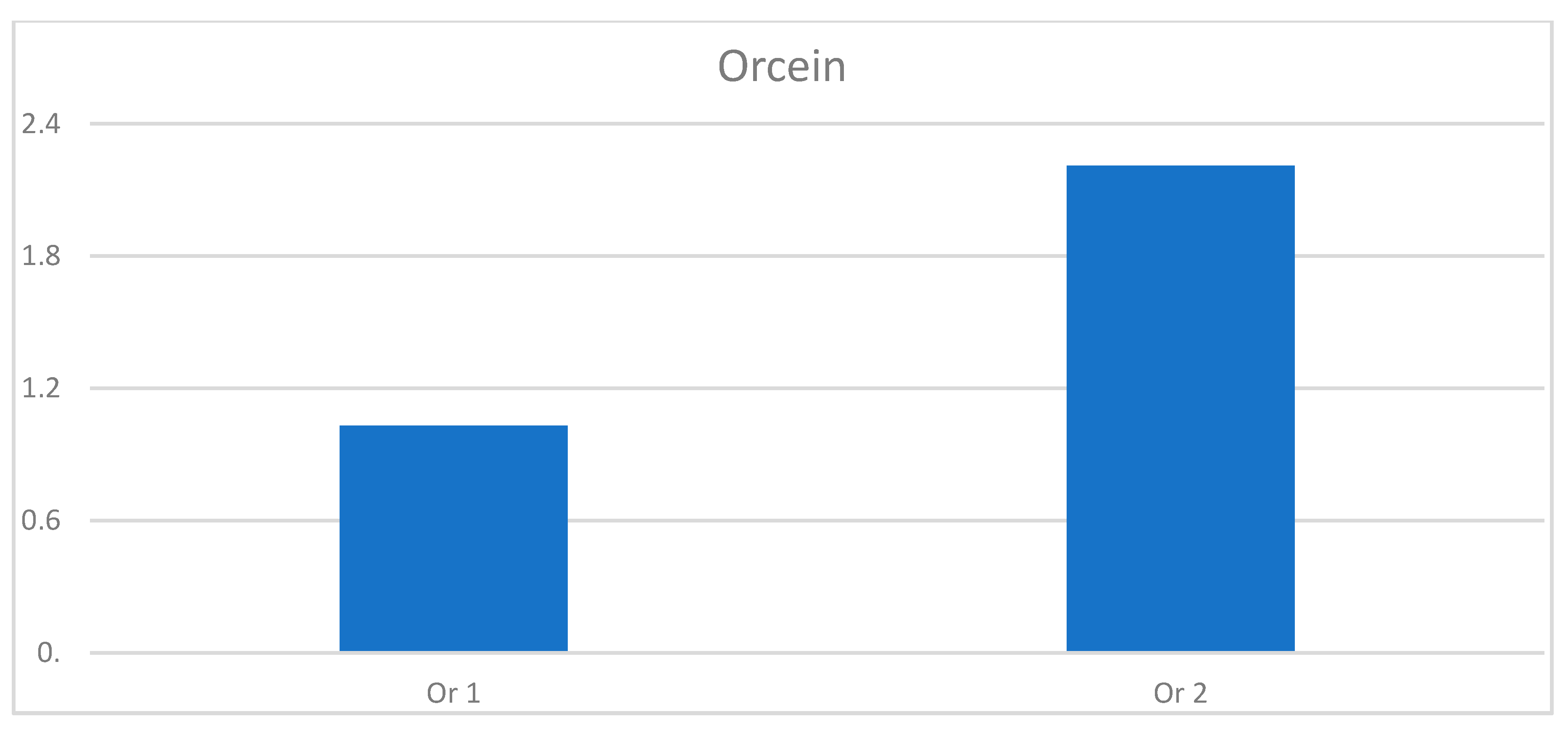
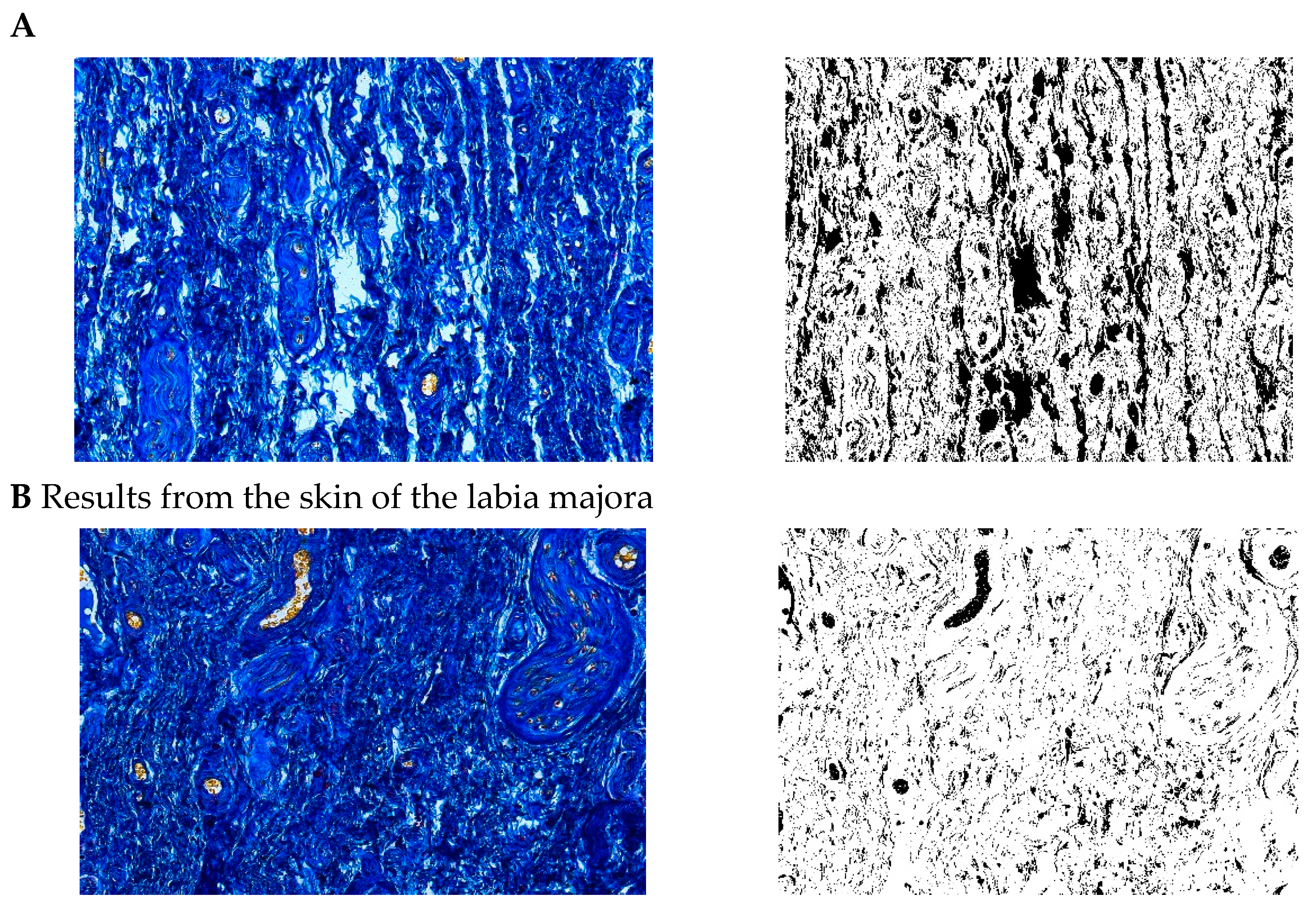
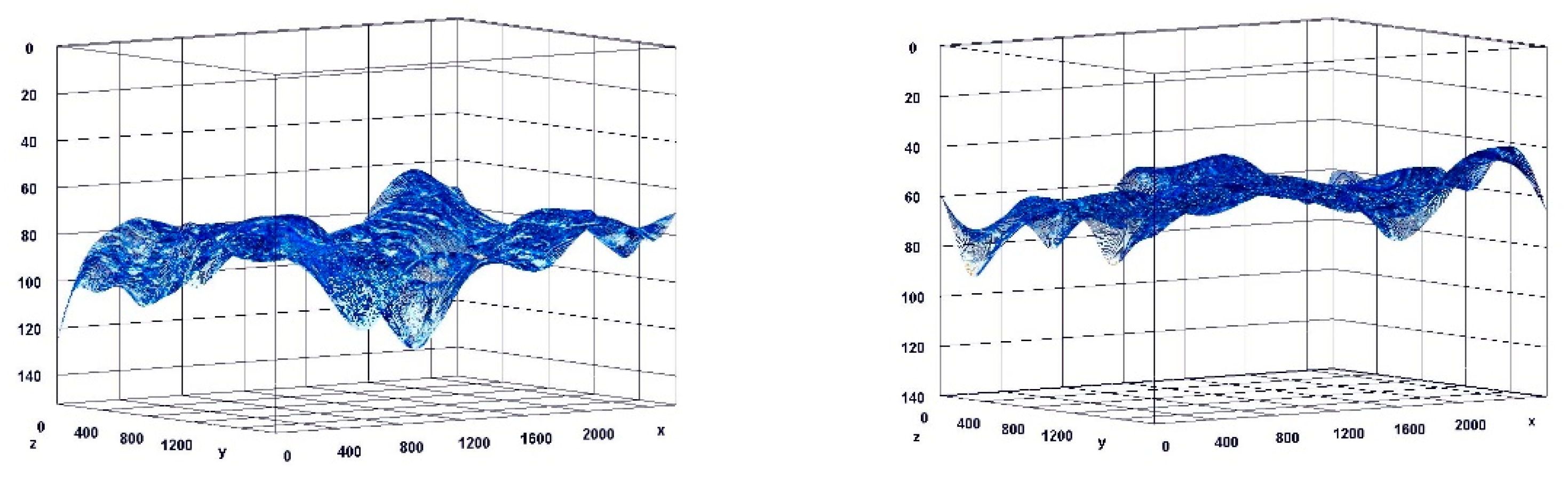
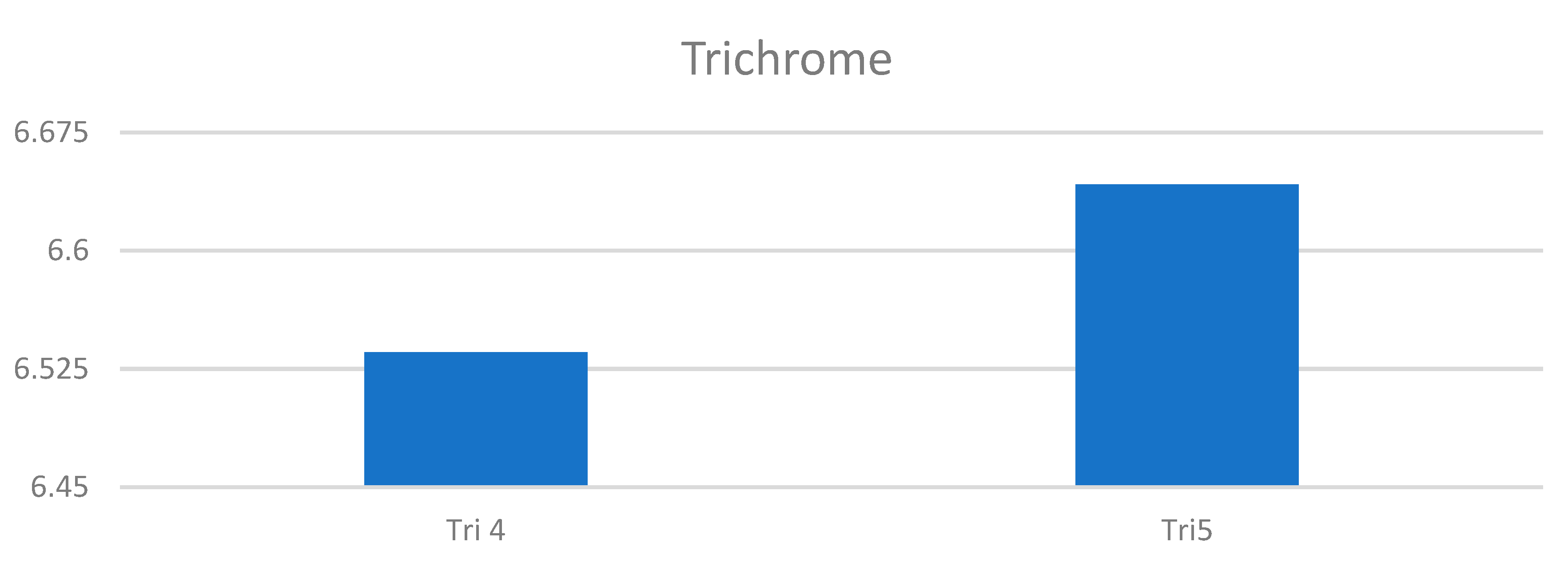
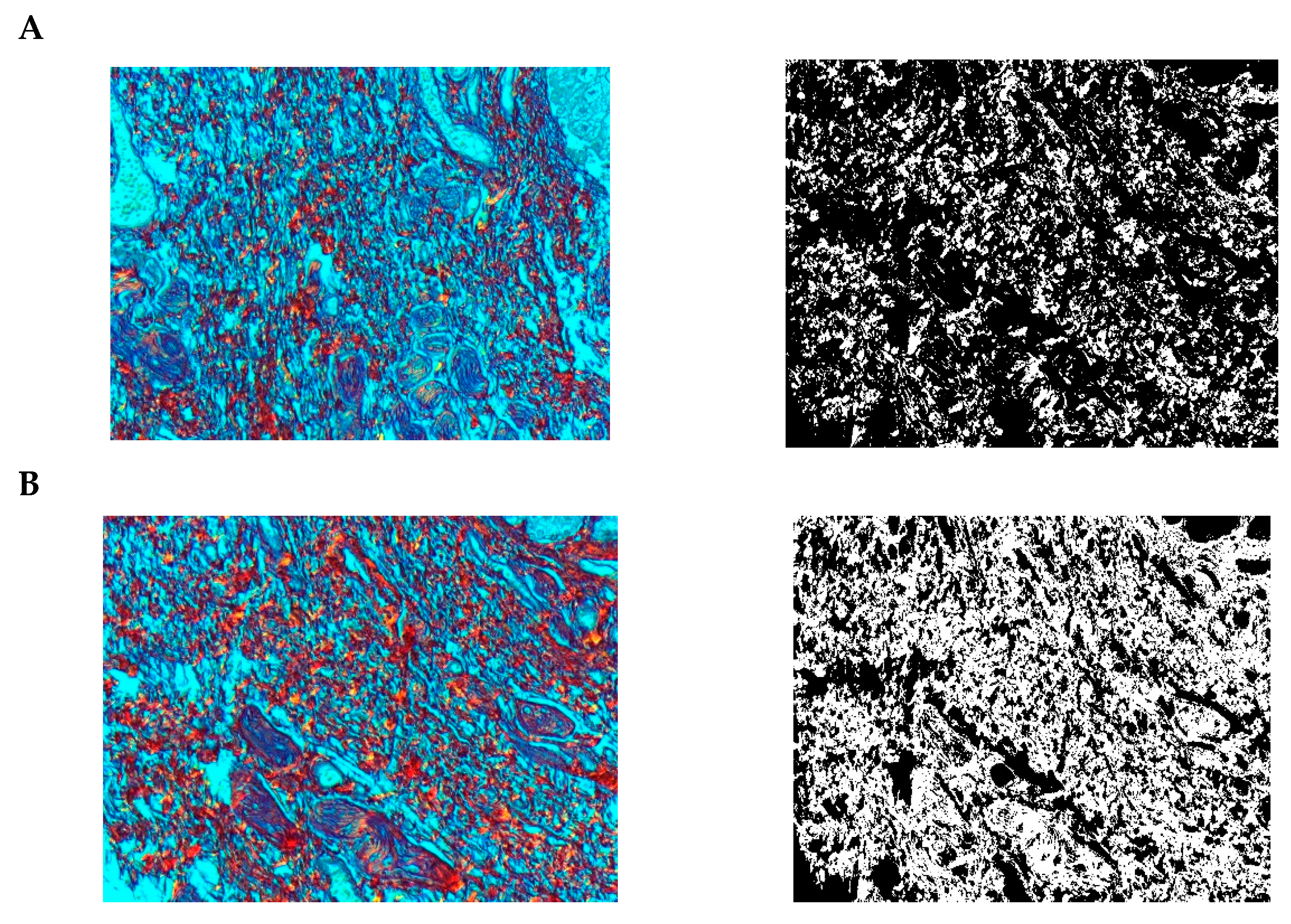
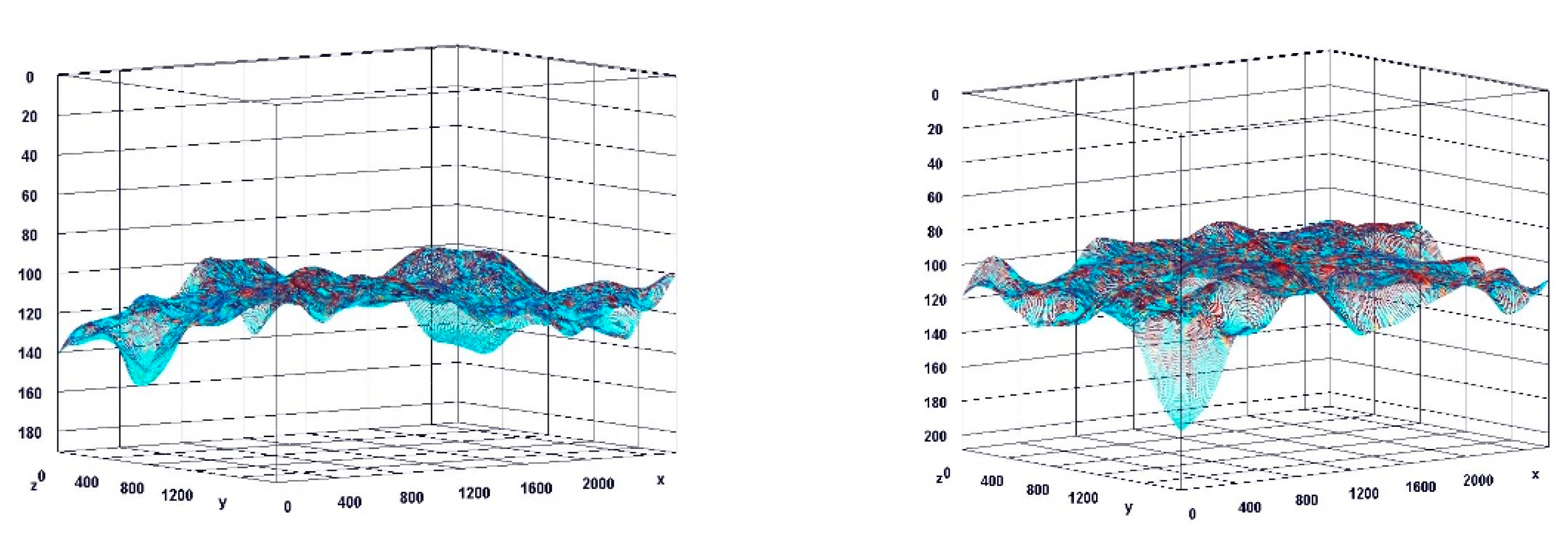
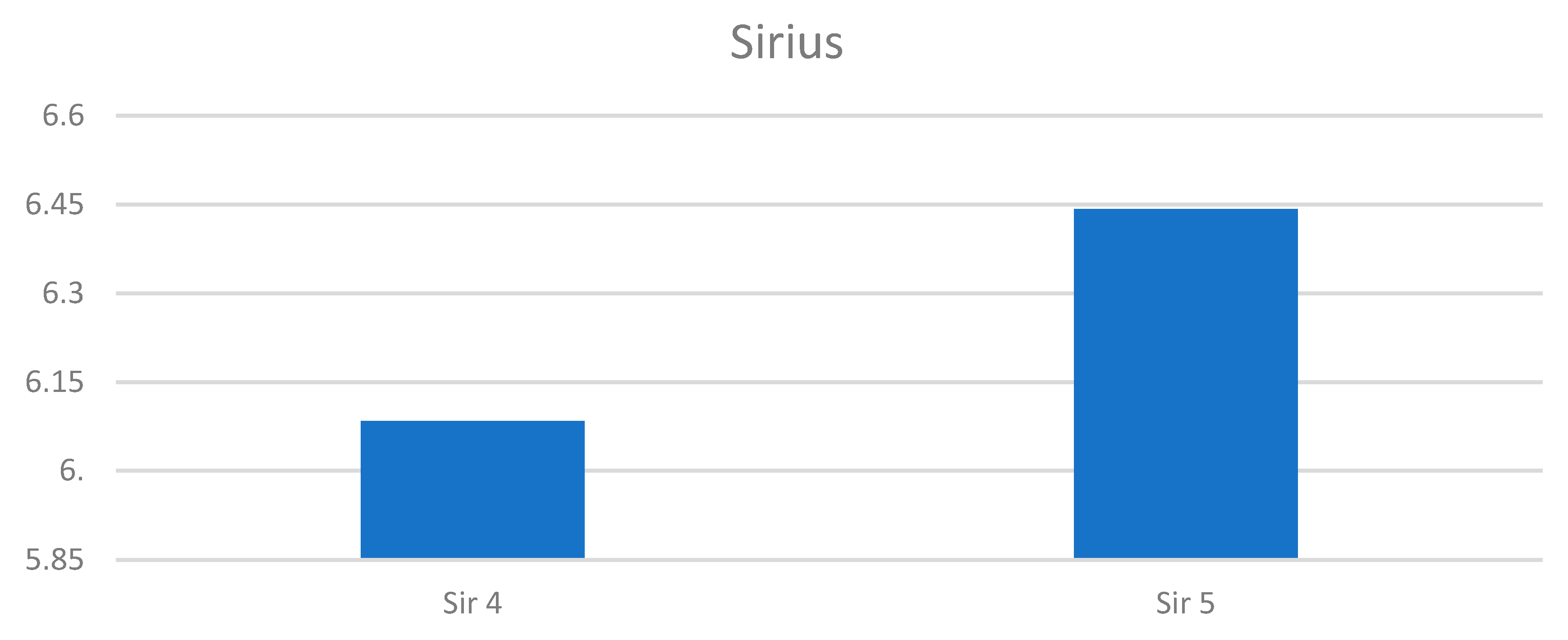
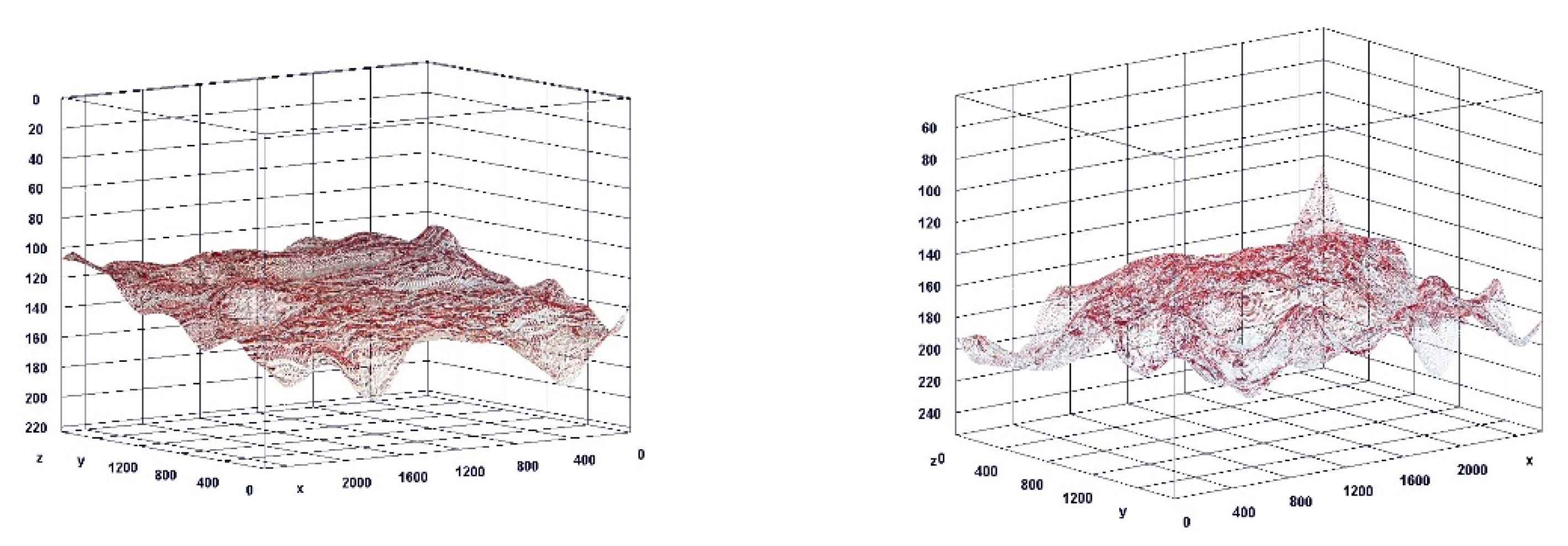
3.7. Histochemical Staining Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Portman, D.J.; Gass, M.L. Vulvovaginal Atrophy Terminology Consensus Conference Panel. Genitourinary syndrome of menopause: New terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and the North American Menopause Society. Climacteric 2014, 17, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, J.; Chen, A.; Dagur, G.; Suh, Y.; Smith, N.; Cali, B.; Khan, S.A. Genitourinary syndrome of menopause: An overview of clinical manifestations, pathophysiology, etiology, evaluation, and management. Am. J. Obstet. Gynecol. 2016, 215, 704–711. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palma, F.; Volpe, A.; Villa, P.; Cagnacci, A. Vaginal atrophy of women in postmenopause. Results from a multicentric observational study: The AGATA study. Maturitas 2016, 83, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Kingsber, S.A.; Krychman, M.; Graham, S.; Bernick, B.; Mirkin, S. The Women’s EMPOWER Survey: Identifying women’s perceptions on vulvar and vaginal atrophy and its treatment. J. Sex. Med. 2017, 14, 413–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nappi, R.E.; Seracchioli, R.; Salvatore, S.; Cagnacci, A.; Di Paolantonio, T.; Busacca, M. Impact of vulvovaginal atrophy of menopause: Prevalence and symptoms in Italian women according to the EVES study. Gynecol. Endocrinol. 2019, 35, 453–459. [Google Scholar] [CrossRef] [PubMed]
- North American Menopause Society. The 2012 hormone therapy position statement of: The North American Menopause Society. Menopause 2012, 19, 257–271. [Google Scholar] [CrossRef] [Green Version]
- Palacios, S. Managing urogenital atrophy. Maturitas 2009, 63, 315–318. [Google Scholar] [CrossRef]
- Archer, D.F. Efficacy and tolerability of local estrogen therapy for urogenital atrophy. Menopause 2010, 17, 194–203. [Google Scholar] [CrossRef]
- Pauls, R.N.; Fellner, A.N.; Davila, G.W. Vaginal laxity: A poorly understood quality of life problem; a survey of physician members of the International Urogynecological Association (IUGA). Int. Urogynecol. J. 2012, 23, 1435–1448. [Google Scholar] [CrossRef]
- Thibault-Gagnon, S.; Yusuf, S.; Langer, S.; Wong, V.; Shek, K.; Dietz, H. Do women notice the impact of childbirth-related levator trauma on pelvic floor and sexual function? Int. Urogynecol. J. 2014, 25, 1389–1398. [Google Scholar] [CrossRef]
- Dietz, H.; Wilson, P.; Milsomc, I. Maternal birth trauma: Why should it matter to urogynaecologists? Curr. Opin. Obstet. Gynecol. 2016, 28, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Kamisan Atan, I.; Gerges, B.; Shek, K.; Dietz, H.P. The association between vaginal childbirth and hiatal dimensions: A retrospective observational study in a tertiary urogynaecological centre. Br. J. Obstet. Gynaecol. 2015, 122, 867–872. [Google Scholar] [CrossRef] [PubMed]
- Abdool, Z.; Shek, K.; Dietz, H. The effect of levator avulsion on hiataldimensions and function. Am. J. Obstet. Gynecol. 2009, 201, 89. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.; Miklos, J.; Chinthakanan, O. Evaluation of sexual function outcomes in women undergoing vaginal rejuvenation/vaginoplasty procedures for symptoms of vaginal laxity/decreased vaginal sensation utilizing validated sexual function questionnaire (PISQ-12). Surg. Technol. Int. 2014, 24, 253–260. [Google Scholar] [PubMed]
- Singh, A.; Swift, S.; Khullar, V.; Digesu, A. Laser vaginal rejuvenation: Not ready for prime time. Int. Urogynecol. J. 2015, 26, 163–164. [Google Scholar] [CrossRef] [Green Version]
- Hamori, C. Aesthetic surgery of the female genitalia: Labiaplasty and beyond. Plast Reconstr. Surg. 2014, 134, 661–673. [Google Scholar] [CrossRef]
- Campbell, P.; Krychman, M.; Gray, T.; Vickers, H.; Money-Taylor, J.; Li, W.; Radley, S. Self-Reported Vaginal Laxity-Prevalence, Impact, and Associated Symptoms in Women Attending a Urogynecology Clinic. J. Sex. Med. 2018, 15, 1515–1517. [Google Scholar] [CrossRef]
- Qureshi, A.A.; Sharma, K.; Thornton, M.; Myckatyn, T.M.; Tenenbaum, M.M. Vaginal Laxity, Sexual Distress, and Sexual Dysfunction: A Cross-Sectional Study in a Plastic Surgery Practice. Aesthetic Surg. J. 2018, 38, 873–880. [Google Scholar] [CrossRef] [Green Version]
- Davies, M.C.; Creighton, S.M.; Woodhouse, C.R. The pitfalls of vaginal reconstruction. BJU Int. 2005, 95, 1293–1298. [Google Scholar] [CrossRef]
- Committee on Gynecologic Practice, American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 378: Vaginal “rejuvenation” and cosmetic vaginal procedures. Obstet. Gynecol. 2007, 110, 737–738. [Google Scholar] [CrossRef] [PubMed]
- Karcher, C.; Sadick, N. Vaginal rejuvenation using energy-based devices. Int. J. Women’s Dermatol. 2016, 2, 85–88. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tadir, Y.; Gaspar, A.; Lev-Sagie, A.; Alexiades, M.; Alinsod, R.; Bader, A.; Calligaro, A.; Elias, J.A.; Gambaciani, M.; Gaviria, J.E.; et al. Light and energy based therapeutics for genitourinary syndrome of menopause: Consensus and controversies. Lasers Surg. Med. 2017, 49, 137–159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulrich, D.; Edwards, S.L.; Letouzey, V.; Su, K.; White, J.F.; Rosamilia, A.; Gargett, C.E.; Werkmeister, J.A. Regional variation in tissue composition and biomechanical properties of postmenopausal ovine and human vagina. PLoS ONE 2014, 9, e104972. [Google Scholar] [CrossRef] [PubMed]
- Kent, D.E.; Bernardy, J. Safety and mechanism of action of noninvasive radio frequency treatment for vaginal laxity: Histological study in the swine vaginal model. J. Cosmet. Dermatol. 2019, 19, 1361–1366. [Google Scholar] [CrossRef]
- Millheiser, L.S.; Pauls, R.N.; Herbst, S.J.; Chen, B.H. Radiofrequency treatment of vaginal laxity after vaginal delivery: Nonsurgical vaginal tightening. J. Sex. Med. 2010, 7, 3088–3095. [Google Scholar] [CrossRef] [PubMed]
- Krychman, M.; Rowan, C.G.; Allan, B.B.; DeRogatis, L.; Durbin, S.; Yacoubian, A.; Wilkerson, D. Effect of Single-Treatment, Surface-Cooled Radiofrequency Therapy on Vaginal Laxity and Female Sexual Function: The VIVEVE I Randomized Controlled Trial. J. Sex. Med. 2017, 14, 215–225. [Google Scholar] [CrossRef]
- Krychman, M.; Rowan, C.G.; Allan, B.B.; Durbin, S.; Yacoubian, A.; Wilkerson, D. Effect of Single-Session, Cryogen-Cooled Monopolar Radiofrequency Therapy on Sexual Function in Women with Vaginal Laxity: The VIVEVE I Trial. J. Women’s Health 2018, 27, 297–304. [Google Scholar] [CrossRef] [Green Version]
- Sekiguchi, Y.; Utsugisawa, Y.; Azekosi, Y.; Kinjo, M.; Song, M.; Kubota, Y.; Kingsberg, S.A.; Krychman, M.L. Laxity of the vaginal introitus after childbirth: Nonsurgical outpatient procedure for vaginal tissue restoration and improved sexual satisfaction using low-energy radiofrequency thermal therapy. J. Women’s Health 2013, 22, 775–781. [Google Scholar] [CrossRef]
- Sarmento, A.C.A.; Fernandes, F.S.; Costa, A.P.F.; Medeiros, K.S.; Crispim, J.C.; Gonçalves, A.K. Microablative fractional radio frequency for genitourinary syndrome of menopause: Protocol of randomised controlled trial. BMJ Open 2021, 11, e046372. [Google Scholar] [CrossRef]
- Shim, S.; Park, K.M.; Chung, Y.J.; Kim, M.R. Updates on therapeutic alternatives for genitourinary syndrome of menopause: Hormonal and non-hormonal managements. J. Menopausal Med. 2021, 27, 1–7. [Google Scholar] [CrossRef]
- Salgado, C.J.; Tang, J.C.; Desrosiers, A.E., 3rd. Use of dermal fat graft for augmentation of the labia majora. J. Plast Reconstr. Aesthetic Surg. 2012, 65, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Monheit, G.D.; Coleman, K.L. Hyaluronic acid fillers. Dermatol. Ther. 2006, 19, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Fasola, E.; Gazzola, R. Labia majora augmentation with hyaluronic acid filler: Technique and results. Aesthetic Surg. J. 2016, 36, 1155–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zerbinati, N.; Haddad, R.G.; Bader, A.; Rauso, R.; D’Este, E.; Cipolla, G.; Calligaro, A.; Gonzalez, P.; Salvatore, S.; Serafin, D. A new hialuronic acid polymer in the augmentation and restoration of labia majora. J. Biol. Regul. Homeost. Agents 2017, 31 (Suppl. S2), 153–161. [Google Scholar]
- El-Domyati, M.; el-Ammawi, T.S.; Medhat, W.; Moawad, O.; Brennan, D.; Mahoney, M.G.; Uitto, J. Radiofrequency facial rejuvenation: Evidence-based effect. J. Am. Acad. Dermatol. 2011, 64, 524–535. [Google Scholar] [CrossRef]
- Alam, M.; Levy, R.; Pajvani, U.; Ramierez, J.A.; Guitart, J.; Veen, H.; Gladstone, H.B. Safety of radiofrequency treatment over human skin previously injected with medium-term injectable soft-tissue augmentation materials: A controlled pilot trial. Lasers Surg. Med. 2006, 38, 205–210. [Google Scholar] [CrossRef]
- England, L.J.; Tan, M.H.; Shumaker, P.R.; Egbert, B.M.; Pittelko, K.; Orentreich, D.; Pope, K. Effects of monopolar radiofrequency treatment over soft-tissue fillers in an animal model. Lasers Surg. Med. 2005, 37, 356–365. [Google Scholar] [CrossRef]
- Goldman, M.P.; Alster, T.S.; Weiss, R. A randomized trial to determine the influence of laser therapy, monopolar radiofrequency treatment, and intense pulsed light therapy administered immediately after hyaluronic acid gel implantation. Dermatol. Surg. 2007, 33, 535–542. [Google Scholar]
- Park, D.; Tirelli, N.; Hubbell, J.A. Photopolymerized Ha based hydrogels and interpenetrating networks. Biomaterials 2003, 24, 893–900. [Google Scholar] [CrossRef]
- Leach, J.B.; Schmidt, C.E. Characterization of protein release from photocrosslinkable hyaluronic acid polyethylene glycol hydrogel tissue engineering scaffolds. Biomaterials 2005, 26, 125–135. [Google Scholar] [CrossRef]
- Jin, R.; Moreira Teixeira, L.S.; Krouwels, A.; Dijkstra, P.J.; van Bitterswijk, C.A.; Karperien, M.; Feijen, J. Synthesis and characterization of HA poly (ethylene glycol) hydrogels via Michael addition: An injectable biomaterial for cartilage repair. Acta Biomater. 2010, 6, 1968–1977. [Google Scholar] [CrossRef] [PubMed]
- Hassan, W.; Dong, Y.; Wang, W. Encapsulation and 3D culture of human adipose derived stem cells in an in situ crosslinked hybrid hydrogel composed of PEG based hyperbranched copolymer and HA. Stem Cell Res. Ther. 2013, 4, 32. [Google Scholar] [CrossRef] [PubMed]
- Aurand, E.R. The Characterization of HA and Polyethylene Glycol Hydrogels for Neural Tissue Engineering; University of Colorado Denver, Anshutz Medical Campus: Aurora, CO, USA, 2014; p. 3622545. [Google Scholar]
- Rosen, R.; Brown, C.; Heiman, J.; Leiblum, S.; Meston, C.; Shabsigh, R.; Ferguson, D.; D’Agostino, R. The Female Sexual Function Index (FSFI): A multidimensional self-report instrument for the assessment of female sexual function. J. Sex Marital Ther. 2000, 26, 191–208. [Google Scholar] [CrossRef] [PubMed]
- Bradford, A.; Meston, C.M. Behavior and symptom change among women treated with placebo for sexual dysfunction. J. Sex. Med. 2011, 8, 191–201. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobson, N.S.; Truax, P. Clinical significance: A statistical approach to determining meaningful change in psychotherapy research. J. Consult. Clin. Psychol. 1991, 59, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Bachman, G. Urogenital ageing: An old problem newly recognised. Maturitas 1995, 22, S1–S5. [Google Scholar] [CrossRef]
- Bachmann, G.A.; Nevadunsky, N.S. Diagnosis and treatment of atrophic vaginitis. Am. Fam. Physician 2000, 61, 3090–3096. [Google Scholar]
- Younger, J.; McCue, R.; Mackey, S. Pain outcomes: A brief review of instruments and techniques. Curr. Pain Headache Rep. 2009, 13, 39–43. [Google Scholar] [CrossRef]
- Collins Sally, L.; Moore Andrew, R.; McQuay Henry, J. The visual analogue pain intensity scale: What is moderate pain in millimetres? Pain 1997, 72, 95–97. [Google Scholar] [CrossRef]























Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kolczewski, P.; Parafiniuk, M.; Zawodny, P.; Haddad, R.; Nalewczyńska, A.; Kolasa, A.K.; Wiszniewska, B.; Menkes, S.; Bader, A.; Stabile, G.; et al. Hyaluronic Acid and Radiofrequency in Patients with Urogenital Atrophy and Vaginal Laxity. Pharmaceuticals 2022, 15, 1571. https://doi.org/10.3390/ph15121571
Kolczewski P, Parafiniuk M, Zawodny P, Haddad R, Nalewczyńska A, Kolasa AK, Wiszniewska B, Menkes S, Bader A, Stabile G, et al. Hyaluronic Acid and Radiofrequency in Patients with Urogenital Atrophy and Vaginal Laxity. Pharmaceuticals. 2022; 15(12):1571. https://doi.org/10.3390/ph15121571
Chicago/Turabian StyleKolczewski, Piotr, Mirosław Parafiniuk, Piotr Zawodny, Rashad Haddad, Agnieszka Nalewczyńska, Agnieszka Kinga Kolasa, Barbara Wiszniewska, Sophie Menkes, Alexander Bader, Giorgio Stabile, and et al. 2022. "Hyaluronic Acid and Radiofrequency in Patients with Urogenital Atrophy and Vaginal Laxity" Pharmaceuticals 15, no. 12: 1571. https://doi.org/10.3390/ph15121571