
Kreon® (Creon®) vs. Lipancrea®: In Vitro Comparison of Two Encapsulated Pancreatin Preparations
Abstract
:
1. Introduction
2. Results
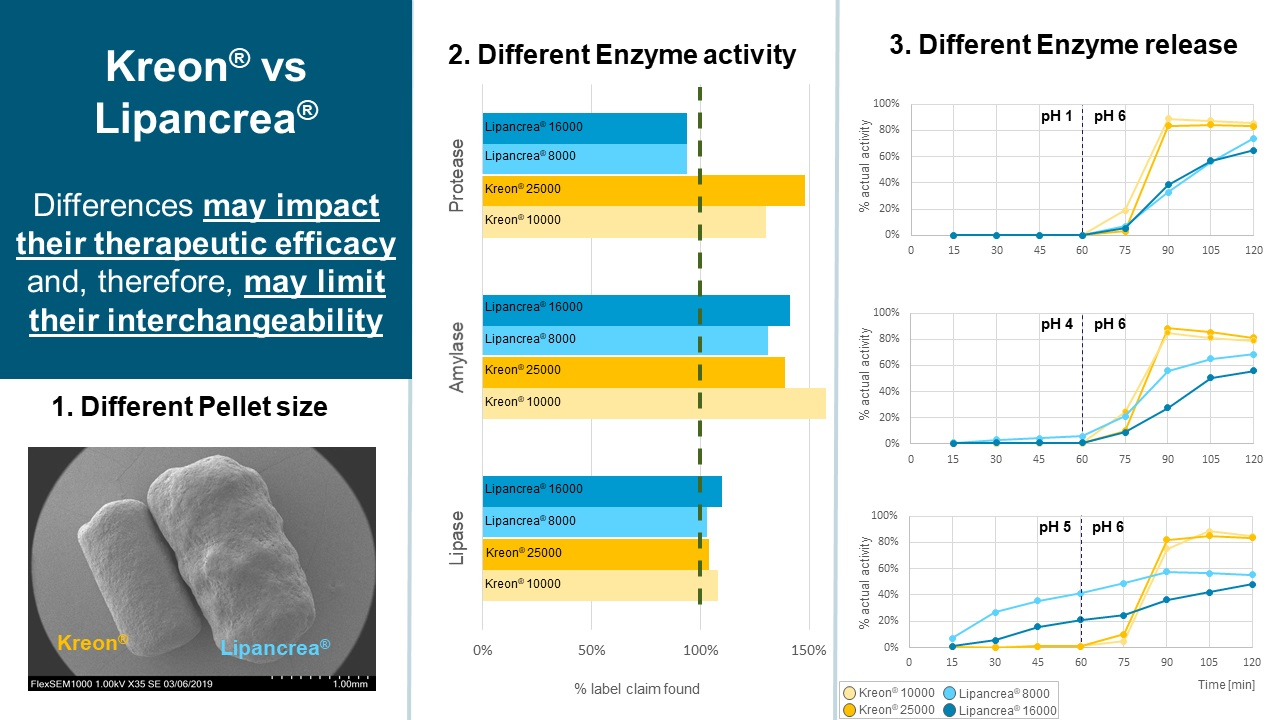
2.1. Physical Properties
2.1.1. Capsule Fill Weight
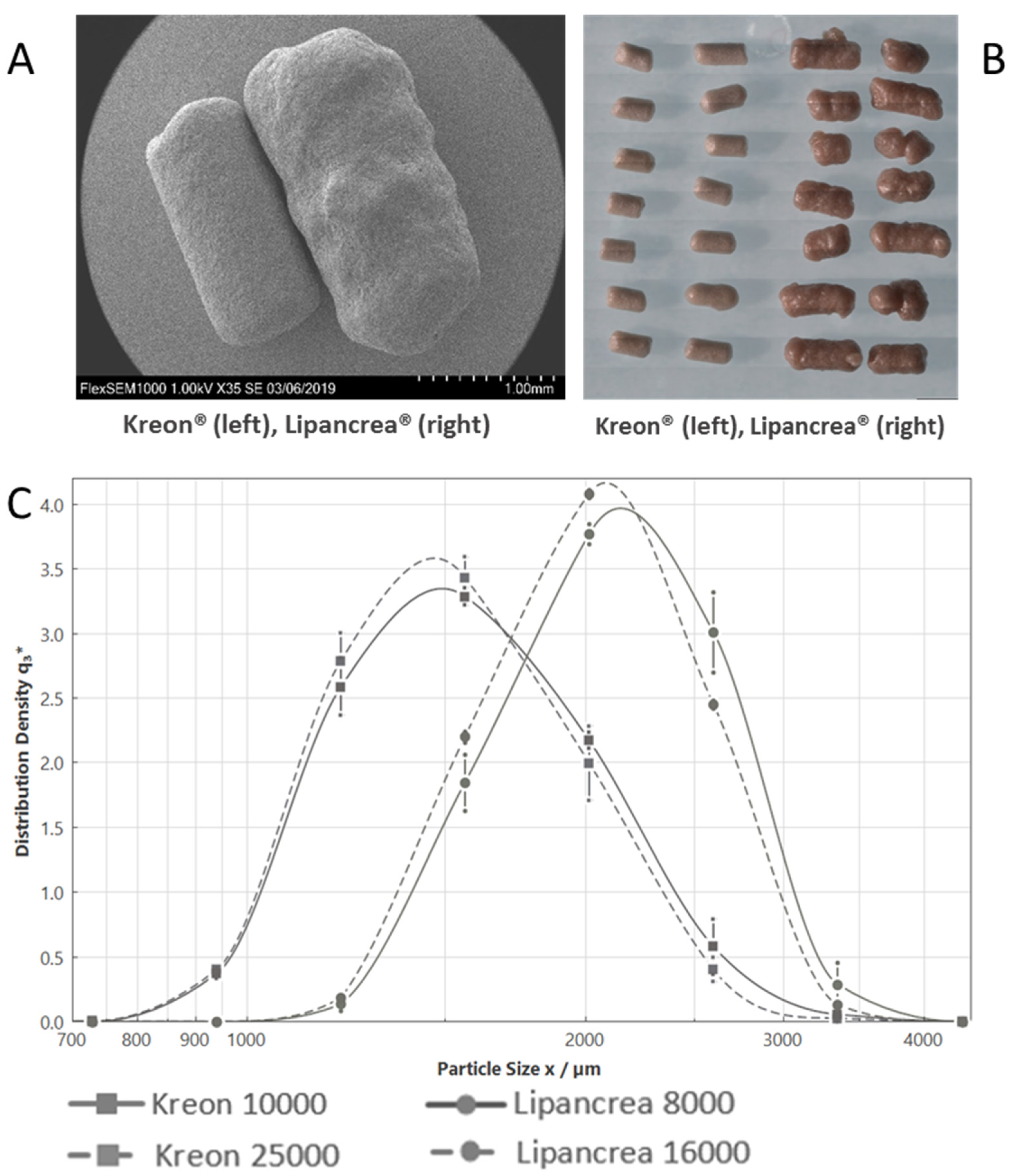
2.1.2. Particle Imaging and Size Determination
2.2. Enzymatic Analysis
2.2.1. Enzyme Activities
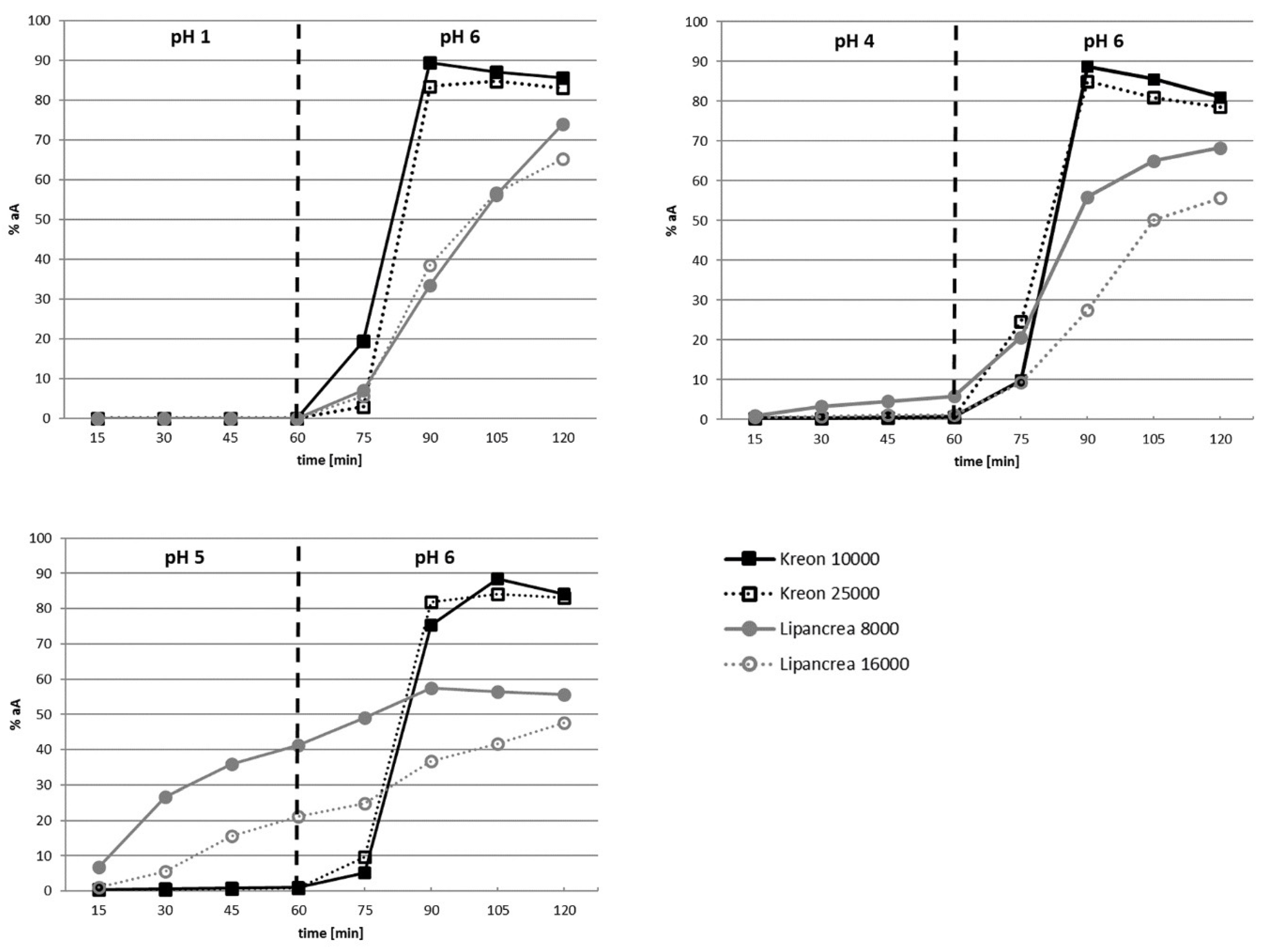
2.2.2. Enzyme Release
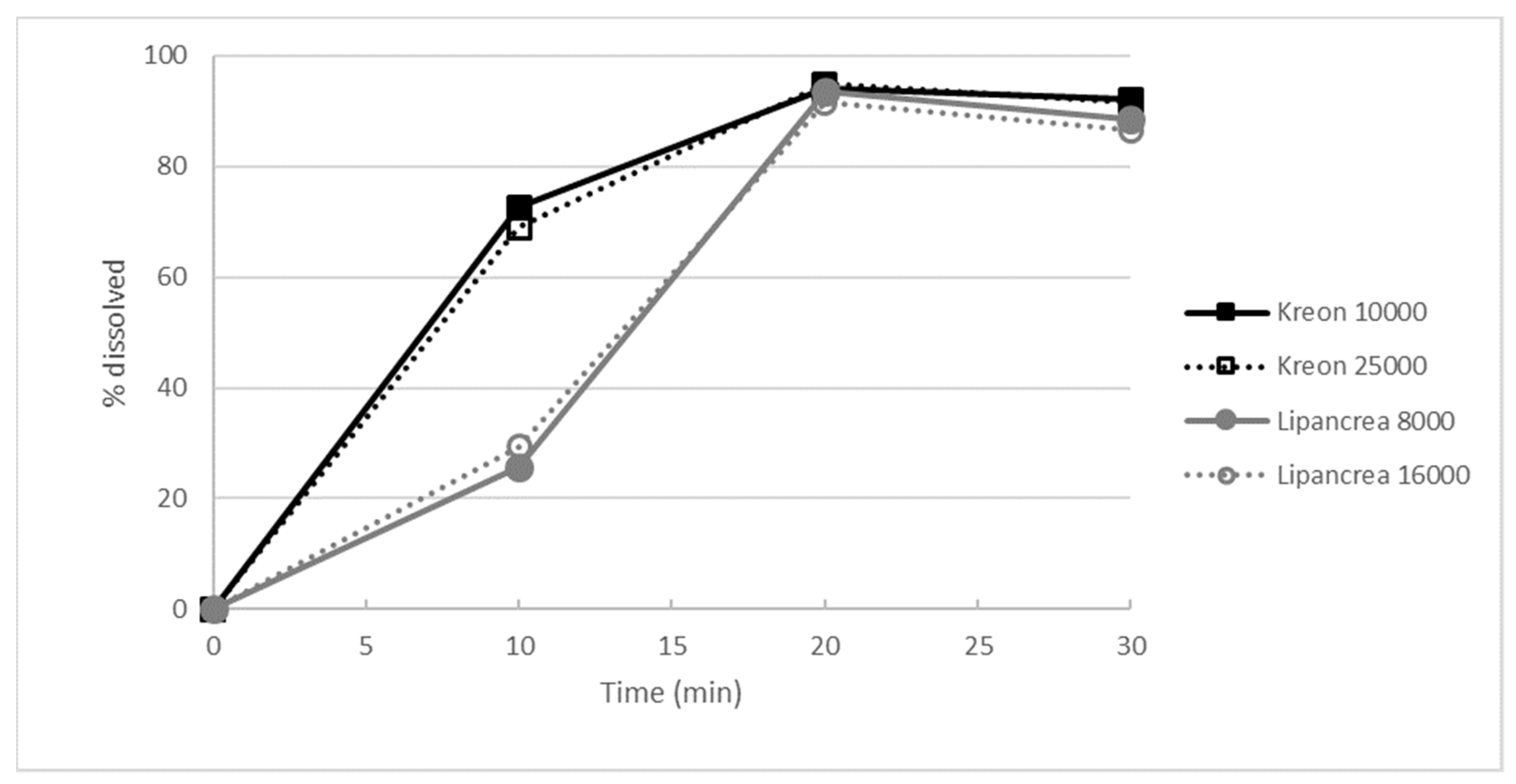
2.2.3. Dissolution Test
3. Discussion
4. Materials and Methods
4.1. Physical Properties
4.1.1. Capsule Fill Weight
4.1.2. Particle Imaging
4.1.3. Particle Size Determination
4.2. Enzymatic Analysis
4.2.1. Enzyme Activities
4.2.2. Enzyme Release
4.2.3. Dissolution Test
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Dominguez-Muñoz, J.E. Diagnosis and treatment of pancreatic exocrine insufficiency. Curr. Opin. Gastroenterol. 2018, 34, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, A.; Domínguez-Muñoz, J.E.; Layer, P.; Lerch, M.M. Pancreatic Exocrine Insufficiency as a Complication of Gastrointestinal Surgery and the Impact of Pancreatic Enzyme Replacement Therapy. Dig. Dis. 2019, 38, 53–68. [Google Scholar] [CrossRef] [PubMed]
- Capurso, G.; Traini, M.; Piciucchi, M.; Signoretti, M.; Arcidiacono, P.G. Exocrine pancreatic insufficiency: Prevalence, diagnosis, and management. Clin. Exp. Gastroenterol. 2019, 12, 129–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domínguez-Muñoz, J.E. Pancreatic exocrine insufficiency: Diagnosis and treatment. J. Gastroenterol. Hepatol. 2011, 26, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Dominguez-Muñoz, J.E. Management of pancreatic exocrine insufficiency. Curr. Opin. Gastroenterol. 2019, 35, 455–459. [Google Scholar] [CrossRef]
- Löhr, J.-M.; Hummel, F.M.; Pirilis, K.T.; Steinkamp, G.; Körner, A.; Henniges, F. Properties of different pancreatin preparations used in pancreatic exocrine insufficiency. Eur. J. Gastroenterol. Hepatol. 2009, 21, 1024–1031. [Google Scholar] [CrossRef]
- Pietrzak, J.; Rydzewska, G.; Turecka-Kulesza, E.; Ciok, J.; Szwed, T.; Dzieniszewski, J.; Gil, J.; Gabryelewicz, A.; Butruk, E. An assessment of the efficacy of Lipancrea in replacement therapy of chronic pancreatitis. Ter. I Leki 1997, XXIV/XLVII, 6. [Google Scholar]
- Barra, E.; Socha, J.; Oralewska, B.; Stolarczyk, A.; Kowalska, M.; Skoczen, M.; Wawer, Z. A comparative assessment of efficacy and tolerability of Lipancrea and kreon25000 in children with exocrine pancreatic insufficiency secondary to cystic fibrosis. Ter. I Leki 1997, XXIV/XLVII, 8. [Google Scholar]
- Kühnelt, P.; Mundlos, S.; Adler, G. Effect of pellet size of a pancreas enzyme preparation on duodenal lipolytic activity. Z. Fur. Gastroenterol. 1991, 29, 417–421. [Google Scholar]
- Kong, F.; Singh, R.P. Disintegration of Solid Foods in Human Stomach. J. Food Sci. 2008, 73, R67–R80. [Google Scholar] [CrossRef]
- Bruno, M.J.; Borm, J.J.; Hoek, F.J.; Delzenne, B.; Hofmann, A.F.; de Goeij, J.J.; van Royen, E.A.; van Leeuwen, D.J.; Tytgat, G.N. Gastric Transit and Pharmacodynamics of a Two-Millimeter Enteric-Coated Pancreatin Microsphere Preparation in Patients with Chronic Pancreatitis. Dig. Dis. Sci. 1998, 43, 203–213. [Google Scholar] [CrossRef] [PubMed]
- Mundlos, S.; Kuhnelt, P.; Adler, G. Monitoring enzyme replacement treatment in exocrine pancreatic insufficiency using the cholesteryl octanoate breath test. Gut 1990, 31, 1324–1328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norregaard, P.; Lysgaard Madsen, J.; Larsen, S.; Worning, H. Gastric emptying of pancreatin granules and dietary lipids in pancreatic insufficiency. Aliment. Pharmacol. Ther. 1996, 10, 427–432. [Google Scholar] [CrossRef]
- Meyer, J.H.; Elashoff, J.; Porter-Fink, V.; Dressman, J.; Amidon, G.L. Human postprandial gastric emptying of 1–3-millimeter spheres. Gastroenterology 1988, 94, 1315–1325. [Google Scholar] [CrossRef] [PubMed]
- Maev, I.V.; Kucheryavyy, Y.A.; Gubergrits, N.B.; Bonnacker, I.; Shelest, E.A.; Janssen-van Solingen, G.P.; Domínguez-Muñoz, J.E. Differences in In Vitro Properties of Pancreatin Preparations for Pancreatic Exocrine Insufficiency as Marketed in Russia and CIS. Drugs R&D 2020, 20, 369–376. [Google Scholar] [CrossRef]
- Case, C.L.; Henniges, F.; Barkin, J.S. Enzyme Content and Acid Stability of Enteric-Coated Pancreatic Enzyme Products In Vitro. Pancreas 2005, 30, 180–183. [Google Scholar] [CrossRef]
- Dressman, J.B.; Berardi, R.R.; Dermentzoglou, L.C.; Russell, T.L.; Schmaltz, S.P.; Barnett, J.L.; Jarvenpaa, K.M. Upper gastrointestinal (GI) pH in young, healthy men and women. Pharm. Res. 1990, 7, 756–761. [Google Scholar] [CrossRef] [Green Version]
- Russell, T.L.; Berardi, R.R.; Barnett, J.L.; Dermentzoglou, L.C.; Jarvenpaa, K.M.; Schmaltz, S.P.; Dressman, J.B. Upper gastrointestinal pH in seventy-nine healthy, elderly, North American men and women. Pharm. Res. 1993, 10, 187–196. [Google Scholar] [CrossRef] [Green Version]
- Lipancrea 8000 Summary of Products Characteristics. Available online: https://www.polfawarszawa.pl/products/chpl/spc-lipancrea-8000-2016-09pl.pdf (accessed on 4 October 2021).
- Lipancrea 16000 Summary of Products Characteristics. Available online: https://www.polfawarszawa.pl/products/chpl/spc-lipancrea-16000-2016-09pl.pdf (accessed on 4 October 2021).
- Kreon 10000 Summary of Products Characteristics. Available online: https://www.medicines.org.uk/emc/product/1167/smpc#PHARMACEUTICAL_PARTS (accessed on 4 October 2021).
- Kreon 25000 Summary of Product Characteristics. Available online: https://www.medicines.org.uk/emc/product/1168 (accessed on 4 October 2021).
- Borgström, B.; Dahlqvist, A.; Lundh, G.; Sjövall, J. Studies of Intestinal Digestion and Absorption in the Human1. J. Clin. Investig. 1957, 36, 1521–1536. [Google Scholar] [CrossRef] [Green Version]
- Keller, J.; Runzi, M.; Goebell, H.; Layer, P. Duodenal and ileal nutrient deliveries regulate human intestinal motor and pancreatic responses to a meal. Am. J. Physiol. Gastrointest. Liver Physiol. 1997, 272, G632–G637. [Google Scholar] [CrossRef]
- Aloulou, A.; Puccinelli, D.; Sarles, J.; Laugier, R.; Leblond, Y.; Carriere, F. In vitro comparative study of three pancreatic enzyme preparations: Dissolution profiles, active enzyme release and acid stability. Aliment. Pharmacol. Ther. 2007, 27, 283–292. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, R.J.; Eyting, S.; Henniges, F.; Potthoff, A. In Vitro Comparison of Physical Parameters, Enzyme Activity, Acid Resistance, and pH Dissolution Characteristics of Enteric-Coated Pancreatic Enzyme Preparations: Implications for Clinical Variability and Pharmacy Substitution. J. Pediatr. Pharmacol. Ther. 2007, 12, 115–128. [Google Scholar] [CrossRef] [PubMed]
- European Pharmacopeia, Monograph 0350, Pancreas Powder. 2019.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product | Capsule Fill Weight (mg) | Relative Standard Deviation (%) |
|---|---|---|
| Kreon® 10000 | 252.1 | 2.7 |
| Kreon® 25000 | 481.7 | 1.6 |
| Lipancrea® 8000 | 139.1 | 3.9 |
| Lipancrea® 16000 | 272.3 | 2.5 |
| Product | D [v, 0.1]/µm | D [v, 0.5]/µm | D [v, 0.9]/µm |
|---|---|---|---|
| Kreon® 10000 | 1131 | 1566 | 2225 |
| Kreon® 25000 | 1122 | 1531 | 2161 |
| Lipancrea® 8000 | 1542 | 2120 | 2814 |
| Lipancrea® 16000 | 1506 | 2043 | 2740 |
| Enzyme | Product | Label Claim (U) | Activity Measured (U); Mean (SD) | % Label Claim Found; Mean (SD) |
|---|---|---|---|---|
| Lipase | Kreon® 10000 | 10,000 | 10,779 (189) | 108 (2) |
| Kreon® 25000 | 25,000 | 26,025 (463) | 104 (2) | |
| Lipancrea® 8000 | 8000 | 8255 (49) | 103 (1) | |
| Lipancrea® 16000 | 16,000 | 17,617 (324) | 110 (2) | |
| Amylase | Kreon® 10000 | 8000 | 12,602 (39) | 158 (0) |
| Kreon® 25000 | 18,000 | 25,063 (194) | 139 (1) | |
| Lipancrea® 8000 | 5750 | 7530 (66) | 131 (1) | |
| Lipancrea® 16000 | 11,500 | 16,417 (147) | 143 (1) | |
| Protease | Kreon® 10000 | 600 | 780 (10) | 130 (2) |
| Kreon® 25000 | 1000 | 1480 (22) | 148 (2) | |
| Lipancrea® 8000 | 450 | 422 (21) | 94 (5) | |
| Lipancrea® 16000 | 900 | 844 (21) | 94 (2) |
| Product | Mean % Actual Activity Released after 60 min (Individual Values Given in Brackets) | ||
|---|---|---|---|
| pH 1.0 | pH 4.0 | pH 5.0 | |
| Kreon® 10000 | 0 (0; 0) | 1 (0.5; 0.9) | 1 (0.8; 1.4) |
| Kreon® 25000 | 0 (0; 0) | 1 (0.3; 0.8) | 1 (0.7; 0.9) |
| Lipancrea® 8000 | 0 (0; 0) | 6 (7.0; 4.8) | 41 (44.6; 37.9) |
| Lipancrea® 16000 | 0 (0; 0) | 1 (1.0; 1.3) | 21 (25.4; 16.8) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hartmann, S.; Rydzewska, G.; Domínguez-Muñoz, J.E. Kreon® (Creon®) vs. Lipancrea®: In Vitro Comparison of Two Encapsulated Pancreatin Preparations. Pharmaceuticals 2022, 15, 1570. https://doi.org/10.3390/ph15121570
Hartmann S, Rydzewska G, Domínguez-Muñoz JE. Kreon® (Creon®) vs. Lipancrea®: In Vitro Comparison of Two Encapsulated Pancreatin Preparations. Pharmaceuticals. 2022; 15(12):1570. https://doi.org/10.3390/ph15121570
Chicago/Turabian StyleHartmann, Sven, Grazyna Rydzewska, and J. Enrique Domínguez-Muñoz. 2022. "Kreon® (Creon®) vs. Lipancrea®: In Vitro Comparison of Two Encapsulated Pancreatin Preparations" Pharmaceuticals 15, no. 12: 1570. https://doi.org/10.3390/ph15121570