
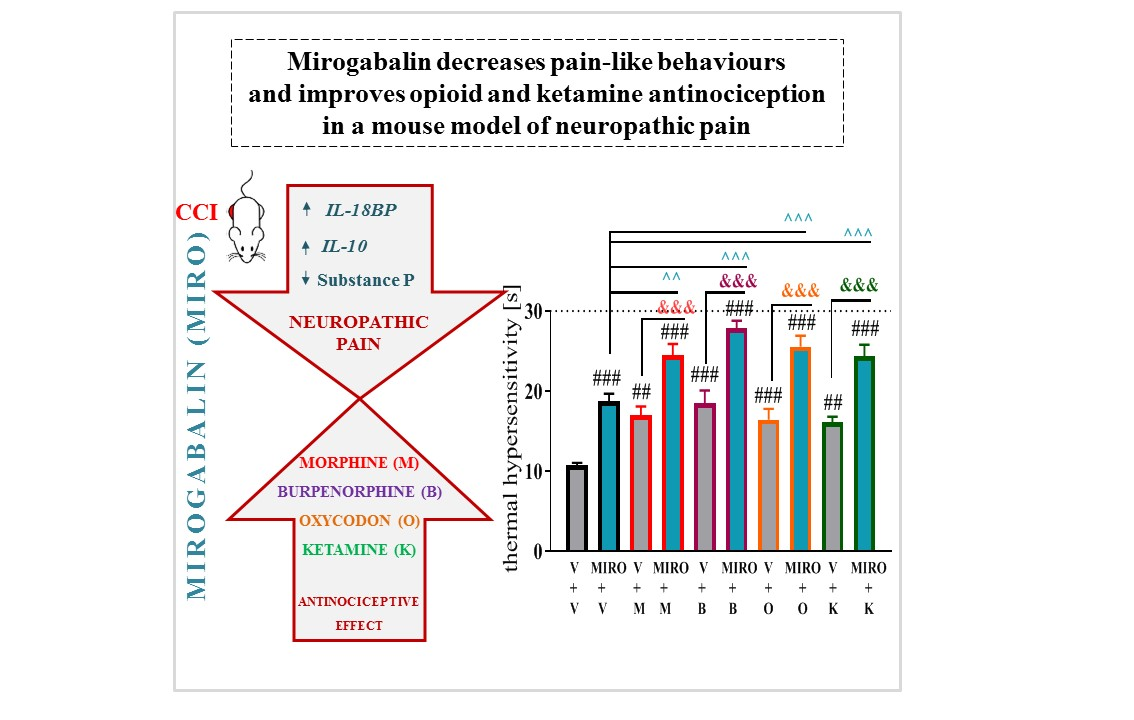
Mirogabalin Decreases Pain-like Behaviours and Improves Opioid and Ketamine Antinociception in a Mouse Model of Neuropathic Pain

 ,
, 
 ,
,
Abstract
:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
1. Introduction
2. Results
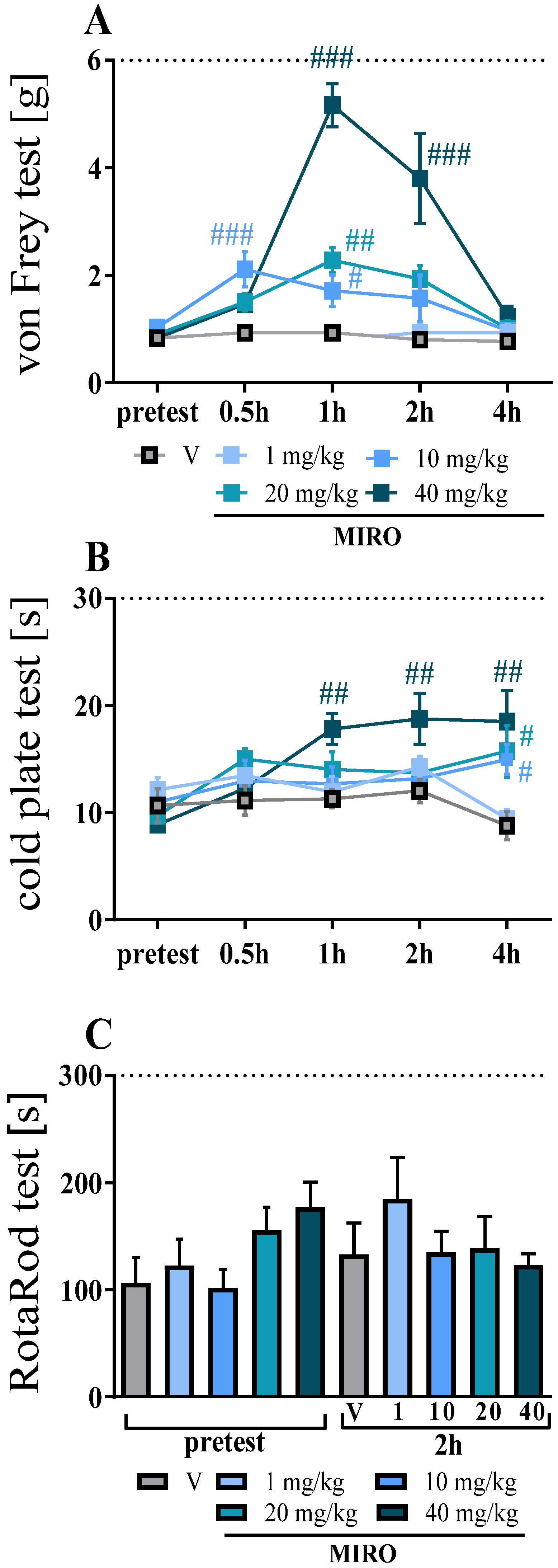
2.1. Effects of a Single i.p. Mirogabalin Administration on Pain-Related Behaviour Measured 11 Days after CCI in Mice
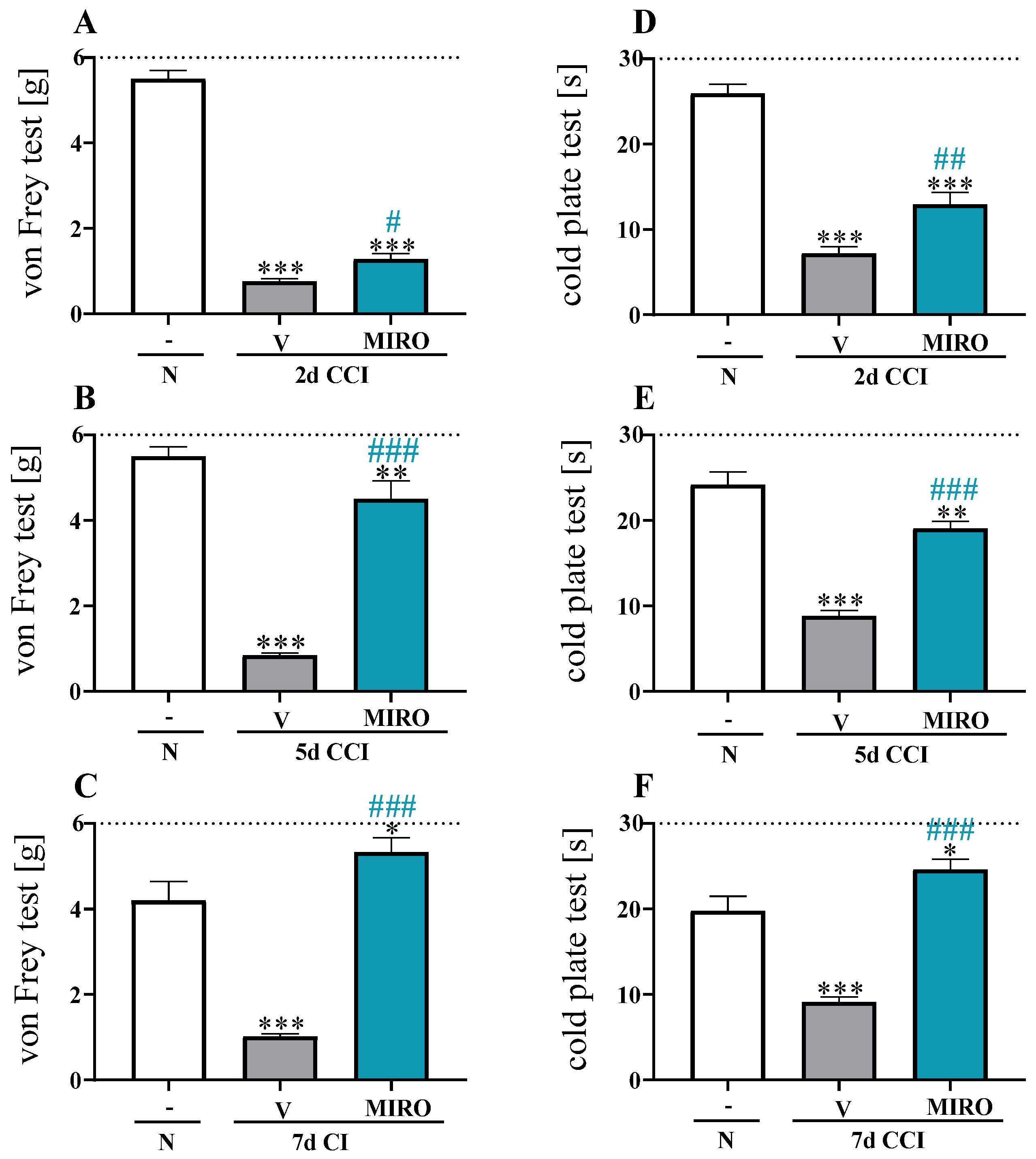
2.2. Effects of Repeated i.p. Mirogabalin Administration on Pain-Related Behaviour Measured 7 Days after CCI in Mice
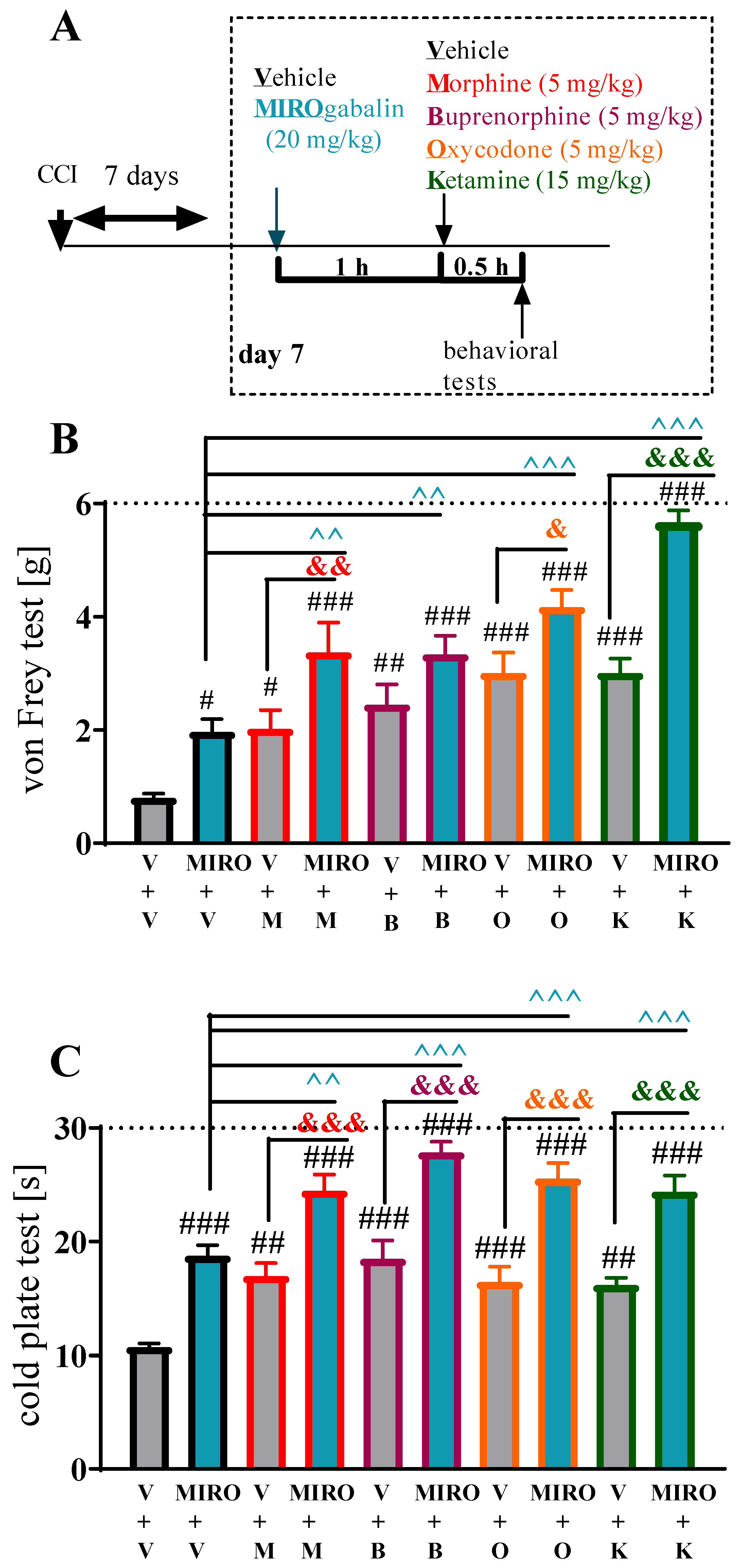
2.3. Effects of a Single i.p. Administration of Mirogabalin on the Efficacy of Morphine, Buprenorphine, Oxycodone and Ketamine Antinociception 7 Days after CCI in Mice
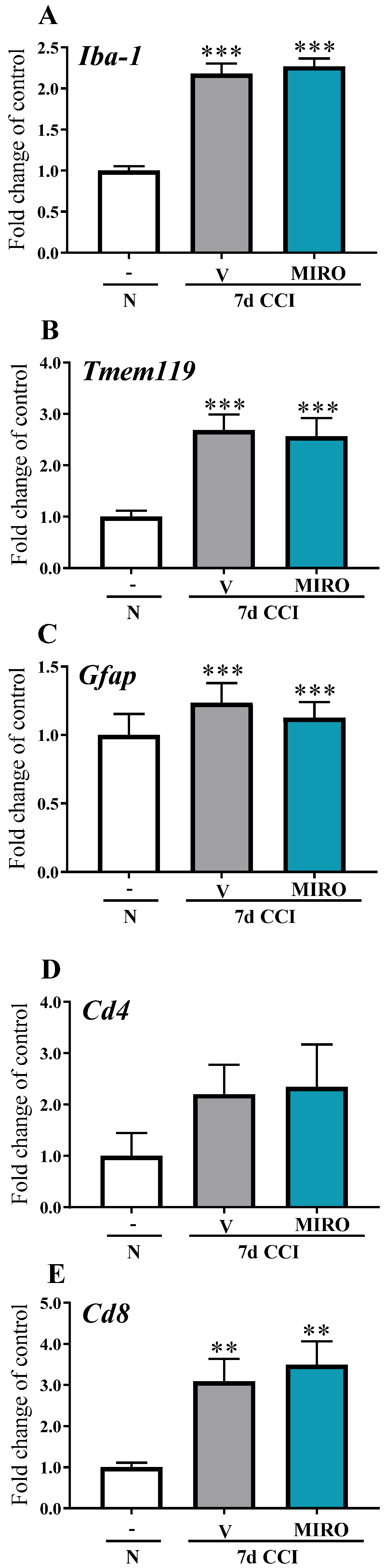
2.4. Effects of Repeated i.p. Administration of Mirogabalin on the mRNA Levels of the Cellular Markers Iba-1, Tmem119, Gfap, Cd4 and Cd8 Measured on Day 7 after CCI in the Spinal Cord of Mice
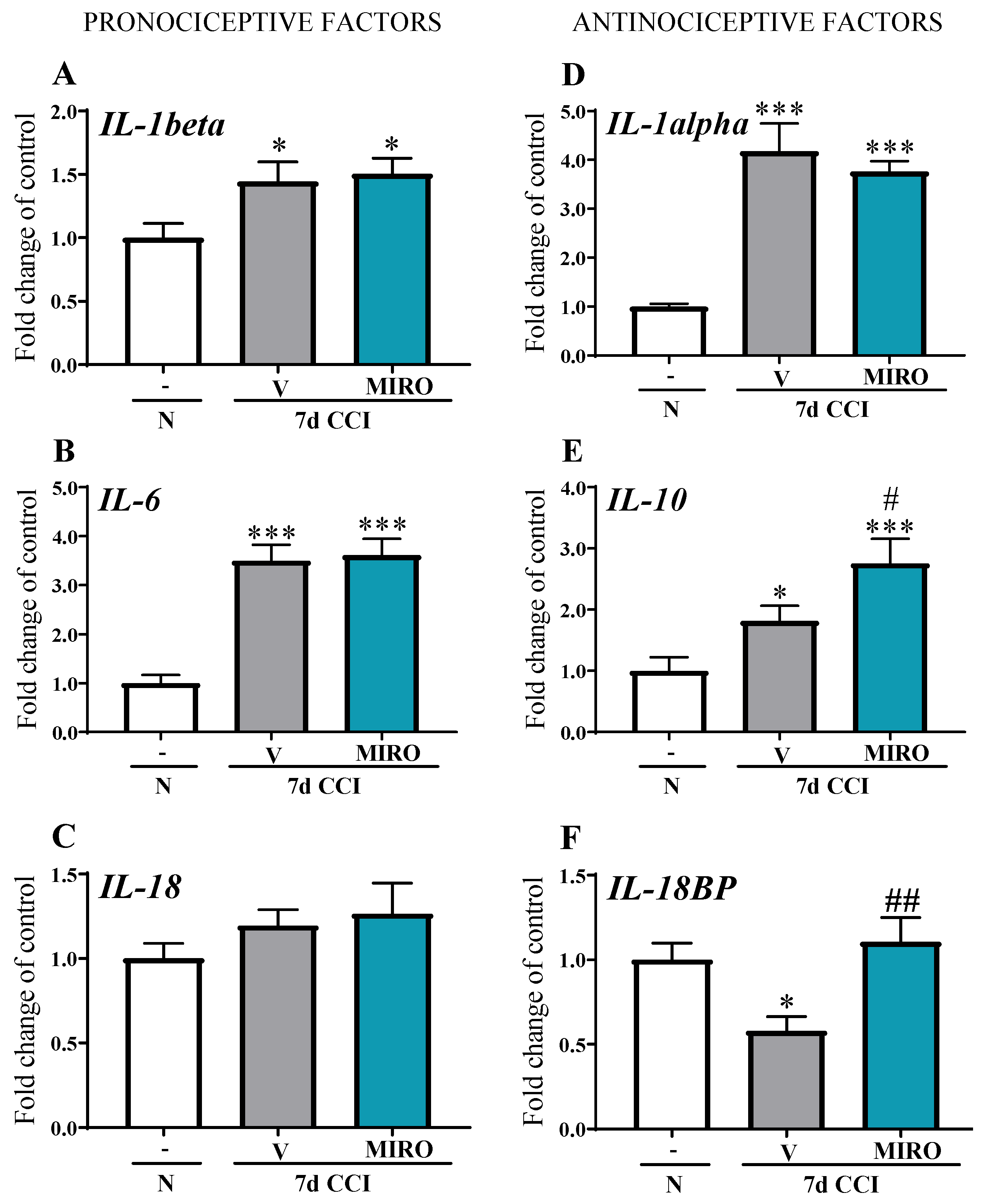
2.5. Effects of Repeated i.p. Administration of Mirogabalin on mRNA Levels of Pro-(IL1-Beta, IL-6, IL-18) and Anti-(IL-1alpha, IL-10, IL-18BP) Nociceptive Factors Measured on Day 7 after CCI in the Spinal Cord in Mice
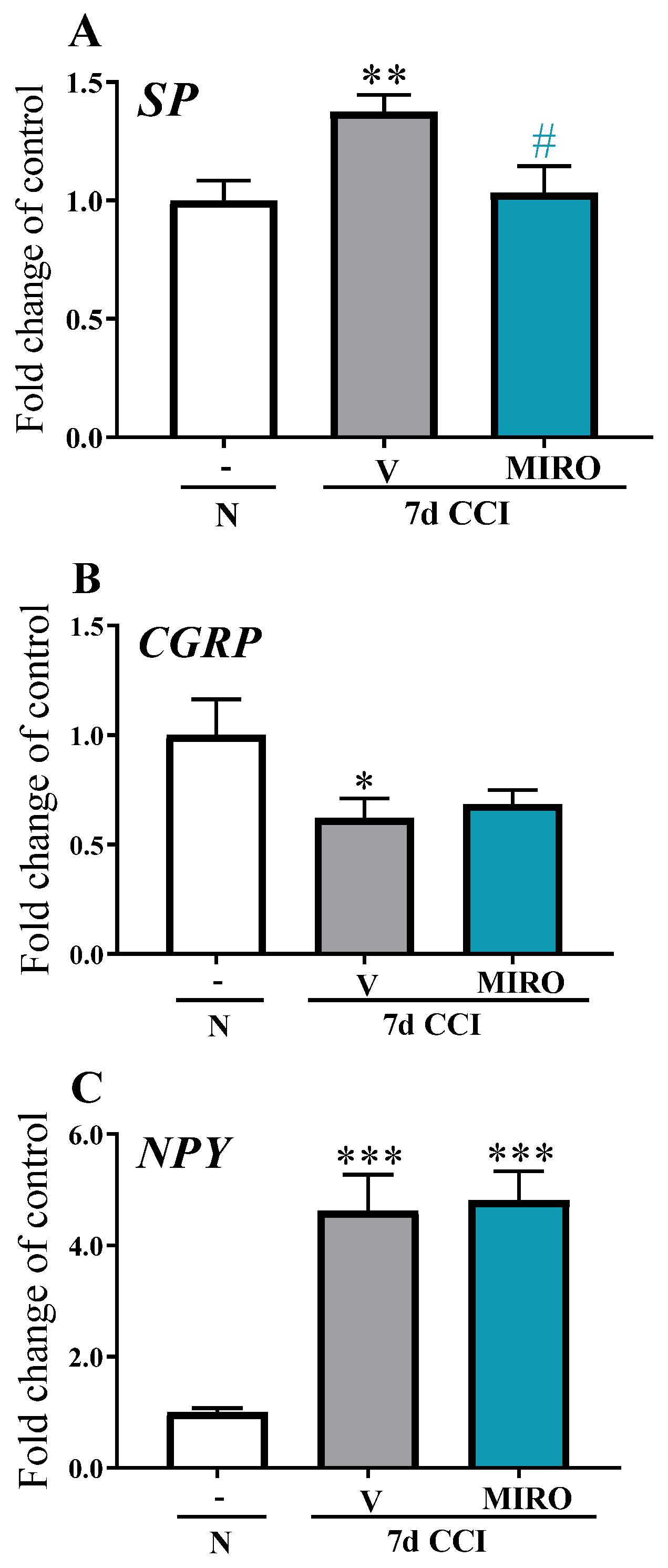
2.6. Effects of Repeated i.p. Administration of Mirogabalin on Pronociceptive Neuropeptide (Substance P, CGRP, Neuropeptide Y) mRNA Levels Measured on Day 7 after CCI in the Spinal Cord in Mice
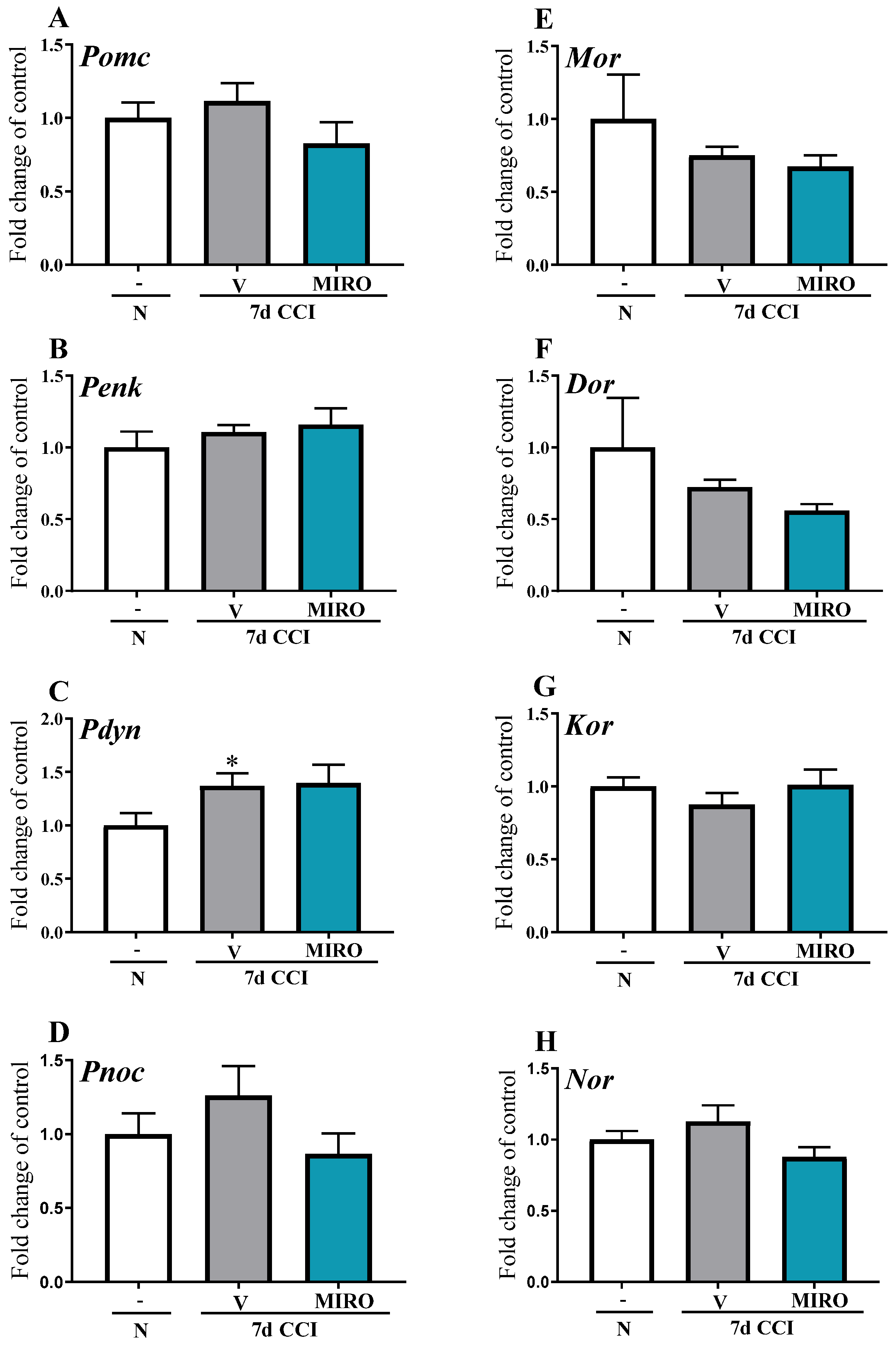
2.7. Effects of Repeated i.p. Mirogabalin Administration on Opioid Prohormone (Pomc, Penk, Pdyn, Pnoc) and Receptor (Mor, Dor, Kor, Nor) mRNA Levels Measured on Day 7 after CCI in the Spinal Cord in Mice
3. Discussion
4. Materials and Methods
4.1. Animals
4.2. Sciatic Nerve Surgery
4.3. Drug Administration
4.4. Behavioural Tests
4.4.1. Von Frey Test
4.4.2. Cold Plate Test
4.5. RT-qPCR
4.6. Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Finnerup, N.B.; Haroutounian, S.; Kamerman, P.; Baron, R.; Bennett, D.L.; Bouhassira, D.; Cruccu, G.; Freeman, R.; Hansson, P.; Nurmikko, T.; et al. Neuropathic pain: An updated grading system for research and clinical practice. Pain 2016, 157, 1599–1606. [Google Scholar] [CrossRef] [Green Version]
- Daiichi Sankyo Company. Tarlige® Tablets: Prescribing Information. 2019. Available online: http://www.info.pmda.go.jp/downf (accessed on 15 April 2019).
- Zajączkowska, R.; Mika, J.; Leppert, W.; Kocot-Kępska, M.; Malec-Milewska, M.; Wordliczek, J. Mirogabalin—A Novel Selective Ligand for the α2δ Calcium Channel Subunit. Pharmaceuticals 2021, 14, 112. [Google Scholar] [CrossRef]
- Chaparro, L.E.; Wiffen, P.J.; Moore, R.A.; Gilron, I. Combination pharmacotherapy for the treatment of neuropathic pain in adults. Cochrane Database Syst. Rev. 2012, CD008943. [Google Scholar] [CrossRef]
- Madden, K.; Haider, A.; Rozman De Moraes, A.; Naqvi, S.M.; Enriquez, P.A.; Wu, J.; Williams, J.; Liu, D.; Bruera, E. Frequency of Concomitant Use of Gabapentinoids and Opioids among Patients with Cancer-Related Pain at an Outpatient Palliative Care Clinic. J. Palliat. Med. 2021, 24, 91–96. [Google Scholar] [CrossRef]
- Moisset, X.; Bouhassira, D.; Avez Couturier, J.; Alchaar, H.; Conradi, S.; Delmotte, M.H.; Lanteri-Minet, M.; Lefaucheur, J.P.; Mick, G.; Piano, V.; et al. Pharmacological and non-pharmacological treatments for neuropathic pain: Systematic review and French recommendations. Rev. Neurol. 2020, 176, 325–352. [Google Scholar] [CrossRef]
- Gilron, I.; Bailey, J.M.; Tu, D.; Holden, R.R.; Weaver, D.F.; Houlden, R.L. Morphine, gabapentin, or their combination for neuropathic pain. N. Engl. J. Med. 2005, 352, 1324–1334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanna, M.; O’Brien, C.; Wilson, M.C. Prolonged-release oxycodone enhances the effects of existing gabapentin therapy in painful diabetic neuropathy patients. Eur. J. Pain 2008, 12, 804–813. [Google Scholar] [CrossRef]
- Amr, Y.M. Multi-Day Low Dose Ketamine Infusion as an adjuvant to Oral Gabapentin in Spinal Cord Injury Related Chronic Pain: A Prospective, Randomized, Double Blind Trial. Pain Physician 2010, 13, 245–249. [Google Scholar] [CrossRef] [PubMed]
- Murasawa, H.; Kobayashi, H.; Saeki, K.; Kitano, Y. Anxiolytic effects of the novel α2δ ligand mirogabalin in a rat model of chronic constriction injury, an experimental model of neuropathic pain. Psychopharmacology 2020, 237, 189–197. [Google Scholar] [CrossRef] [PubMed]
- Domon, Y.; Kitano, Y.; Makino, M. Analgesic effects of the novel α2δ ligand mirogabalin in a rat model of spinal cord injury. Pharmazie 2018, 73, 659–661. [Google Scholar] [PubMed]
- Saeki, K.; Yasuda, S.I.; Kato, M.; Kano, M.; Domon, Y.; Arakawa, N.; Kitano, Y. Analgesic effects of mirogabalin, a novel ligand for α2δ subunit of voltage-gated calcium channels, in experimental animal models of fibromyalgia. Naunyn Schmiedebergs Arch. Pharm. 2019, 392, 723–728. [Google Scholar] [CrossRef]
- Austin, P.J.; Moalem-Taylor, G. The neuro-immune balance in neuropathic pain: Involvement of inflammatory immune cells, immune-like glial cells and cytokines. J. Neuroimmunol. 2010, 229, 26–50. [Google Scholar] [CrossRef]
- Mika, J.; Zychowska, M.; Popiolek-Barczyk, K.; Rojewska, E.; Przewlocka, B. Importance of glial activation in neuropathic pain. Eur. J. Pharmacol. 2013, 716, 106–119. [Google Scholar] [CrossRef]
- Mika, J.; Osikowicz, M.; Rojewska, E.; Korostynski, M.; Wawrzczak-Bargiela, A.; Przewlocki, R.; Przewlocka, B. Differential activation of spinal microglial and astroglial cells in a mouse model of peripheral neuropathic pain. Eur. J. Pharmacol. 2009, 623, 65–72. [Google Scholar] [CrossRef]
- Rojewska, E.; Popiolek-Barczyk, K.; Jurga, A.M.; Makuch, W.; Przewlocka, B.; Mika, J. Involvement of pro- and antinociceptive factors in minocycline analgesia in rat neuropathic pain model. J. Neuroimmunol. 2014, 77, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Wodarski, R.; Clark, A.K.; Grist, J.; Marchand, F.; Malcangio, M. Gabapentin reverses microglial activation in the spinal cord of streptozotocin-induced diabetic rats. Eur. J. Pain 2009, 13, 807–811. [Google Scholar] [CrossRef]
- Rosa, A.S.; Freitas, M.F.; Rocha, I.R.C.; Chacur, M. Gabapentin decreases microglial cells and reverses bilateral hyperalgesia and allodynia in rats with chronic myositis. Eur. J. Pharmacol. 2017, 799, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.L.; Xu, B.; Li, S.S.; Zhang, W.S.; Xu, H.; Deng, X.M.; Zhang, Y.O. Gabapentin reduces CX3CL1 signaling and blocks spinal microglial activation in monoarthritic rats. Mol. Brain 2012, 5, 1–12. Available online: http://www.molecularbrain.com/content/5/1/18 (accessed on 15 April 2019). [CrossRef] [PubMed] [Green Version]
- Hundehege, P.; Fernandez-Orth, J.; Römer, P.; Ruck, T.; Müntefering, T.; Eichler, S.; Cerina, M.; Epping, L.; Albrechta, S.; Menke, A.F.; et al. Targeting Voltage-Dependent Calcium Channels with Pregabalin Exerts a Direct Neuroprotective Effect in an Animal Model of Multiple Sclerosis. Neurosignals 2018, 26, 77–93. [Google Scholar] [CrossRef] [PubMed]
- Takasusuki, T. The Effects of Intrathecal and Systemic Gabapentin on Spinal Substance P Release. Anesth. Analg. 2011, 112, 971–976. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fu, W.; Wessel, C.R.; Taylor, B.K. Neuropeptide Y tonically inhibits an NMDAR → AC1 → TRPA1/TRPV1 mechanism of the affective dimension of chronic neuropathic pain. Neuropeptides 2020, 80, 102024. [Google Scholar] [CrossRef]
- McCarthy, P.W.; Lawson, S.N. Cell type and conduction velocity of rat primary sensory neurons with substance P-like immunoreactivity. Neuroscience 1989, 28, 745–753. [Google Scholar] [CrossRef]
- Dias, J.M.; de Brito, T.V.; de Aguiar Magalhaes, D. Gabapentin, a synthetic analogue of gamma aminobutyric acid, reverses systemic acute inflammation and oxidative stress in mice. Inflammation 2014, 37, 1826–1836. [Google Scholar] [CrossRef]
- Lee, B.S.; Jun, G.; Kim, S. Intrathecal gabapentin increases interleukin-10 expression and inhibits proinflammatory cytokine in a rat model of neuropathic pain. J. Korean Med. Sci. 2013, 28, 308–314. [Google Scholar] [CrossRef] [Green Version]
- Bao, Y.H.; Zhou, Q.H.; Chen, R. Gabapentin enhances the morphine antinociceptive effect in neuropathic pain via the interleukin-10-heme oxygenase-1 signalling pathway in rats. J. Mol. Neurosci. 2014, 54, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Malcangio, M.; Bowery, N.G.; Flower, R.J.; Perretti, M. Effect of interleukin-1 beta on the release of substance P from rat isolated spinal cord. Eur. J. Pharmacol. 1996, 299, 113–118. [Google Scholar] [CrossRef]
- Kawasaki, Y.; Zhang, L.; Cheng, J.K.; Ji, R.R. Cytokine mechanisms of central sensitization: Distinct and overlapping role of interleukin-1beta, interleukin-6, and tumor necrosis factor-alpha in regulating synaptic and neuronal activity in the superficial spinal cord. J. Neurosci. 2008, 28, 5189–5194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mika, J.; Korostynski, M.; Kaminska, D.; Wawrzczak-Bargiela, A.; Osikowicz, M.; Makuch, W.; Przewlocki, R.; Przewlocka, B. Interleukin-1 alpha has antiallodynic and antihyperalgesic activities in a rat neuropathic pain model. Pain 2008, 138, 587–597. [Google Scholar] [CrossRef]
- Dinarello, C.A.; Fantuzzi, G. Interleukin-18 and host defense against infection. J. Infect. Dis. 2003, 187 (Suppl. 2), S370–S384. [Google Scholar] [CrossRef]
- Pilat, D.; Piotrowska, A.; Rojewska, E.; Jurga, A.; Ślusarczyk, J.; Makuch, W.; Basta-Kaim, A.; Przewlocka, B.; Mika, J. Blockade of IL-18 signaling diminished neuropathic pain and enhanced the efficacy of morphine and buprenorphine. Mol. Cell Neurosci. 2016, 71, 114–124. [Google Scholar] [CrossRef] [PubMed]
- Dubový, P.; Brázda, V.; Klusáková, I.; Hradilová-Svíženská, I. Bilateral elevation of interleukin-6 protein and mRNA in both lumbar and cervical dorsal root ganglia following unilateral chronic compression injury of the sciatic nerve. J. Neuroinflamm. 2013, 10, 55. [Google Scholar] [CrossRef] [Green Version]
- Ledeboer, A.; Jekich, B.; Sloane, E.M.; Mahoney, J.F.; Langer, S.J.; Milligan, E.D.; Martin, D.; Maier, S.F.; Johnson, K.W.; Leinwand, L.A.; et al. Intrathecal Interleukin-10 Gene Therapy Attenuates Paclitaxel-Induced Mechanical Allodynia and Proinflammatory Cytokine Expression in Dorsal Root Ganglia in Rats. Brain Behav. Immun. 2007, 21, 686–698. [Google Scholar] [CrossRef] [Green Version]
- Kilic, F.S.; Kaygisiz, B.; Aydin, S.; Yildirim, C.; Karimkhani, H.; Oner, S. Pregabalin attenuates carrageenan-induced acute inflammation in rats by inhibiting proinflammatory cytokine levels. Eurasian J. Med. 2018, 50, 156–159. [Google Scholar] [CrossRef]
- Finnerup, N.B.; Attal, N.; Haroutounian, S.; McNicol, E.; Baron, R.; Dworkin, R.H.; Gilron, I.; Haanpää, M.; Hansson, P.; Jensen, T.S.; et al. Pharmacotherapy for neuropathic pain in adults: A systematic review and meta-analysis. Lancet Neurol. 2015, 14, 162–173. [Google Scholar] [CrossRef] [Green Version]
- Holbech, J.V.; Jung, A.; Jonsson, T.; Wanning, M.; Bredahl, C.; Bach, F.W. Combination treatment of neuropathic pain: Danish expert recommendations based on a Delphi process. J. Pain Res. 2017, 10, 1467–1475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caraceni, A.; Zecca, E.; Bonezzi, C.; Arcuri, E.; Tur, R.Y.; Maltoni, M.; Visentin, M.; Gorni, G.; Martini, C.; Tirelli, W.; et al. Gabapentin for neuropathic cancer pain: A randomized controlled trial from the Gabapentin Cancer Pain Study Group. J. Clin. Oncol. 2004, 22, 2909–2917. [Google Scholar] [CrossRef]
- Stein, C. New concepts in opioid analgesia. Expert Opin. Investig. Drugs 2018, 27, 765–775. [Google Scholar] [CrossRef]
- Colloca, L.; Ludman, T.; Bouhassira, D.; Baron, R.; Dickenson, A.H.; Yarnitsky, D.; Freeman, R.; Truini, A.; Attal, N.; Finnerup, N.B.; et al. Neuropathic pain. Nat. Rev. Dis. Primers 2017, 3, 17002. [Google Scholar] [CrossRef] [Green Version]
- Kremer, M.; Yalcin, I.; Nexon, L.; Wurtz, X.; Ceredig, R.A.; Daniel, D.; Hawkes, R.A.; Salvat, E.; Barrot, M. The antiallodynic action of pregabalin in neuropathic pain is independent from the opioid system. Mol. Pain 2016, 12, 1744806916633477. [Google Scholar] [CrossRef] [Green Version]
- Eutamene, H.; Coelho, A.M.; Theodorou, V.; Toulouse, M.; Chovet, M.; Doherty, A.; Fioramonti, J.; Bueno, L. Antinociceptive effect of pregabalin in septic shock induced rectal hypersensitivity in rats. J. Pharmacol. Exp. Ther. 2000, 295, 162–167. [Google Scholar]
- Field, M.J.; Oles, R.J.; Lewis, A.S.; McCleary, S.; Hughes, J.; Singhet, L. Gabapentin (neurontin) and S-(ţ)-3-isobutylgaba represent a novel class of selective antihyperalgesic agents. Br. J. Pharmacol. 1997, 121, 1513–1522. [Google Scholar] [CrossRef] [Green Version]
- Manandhar, P.; Murnion, B.P.; Grimsey, N.L.; Connor, M.; Santiago, M. Do gabapentin or pregabalin directly modulate the μ receptor? PeerJ 2021, 9, e11175. [Google Scholar] [CrossRef]
- Chen, J.; Li, L.; Chen, S.; Chen, H.; Xie, J.; Sirrieh, R.E.; MacLean, D.M.; Zhang, Y.; Zhou, M.H.; Jayaraman, V.; et al. The α2δ-1-NMDA Receptor Complex Is Critically Involved in Neuropathic Pain Development and Gabapentin Therapeutic Actions. Cell Rep. 2018, 22, 2307–2321. [Google Scholar] [CrossRef] [Green Version]
- Meymandi, M.-S.; Keyhanfar, F.; Yazdanpanah, O.; Heravi, G. The Role of NMDARs Ligands on Antinociceptive Effects of Pregabalin in the Tail Flick Test. Anesth. Pain Med. 2015, 5, e28968. [Google Scholar] [CrossRef] [Green Version]
- Zimmermann, M. Ethical guidelines for investigations of experimental pain in conscious animals. Pain 1983, 16, 109–110. [Google Scholar] [CrossRef]
- Bennett, G.J.; Xie, Y.K. A peripheral mononeuropathy in rat that produces disorders of pain sensation like those seen in man. Pain 1988, 33, 87–107. [Google Scholar] [CrossRef]
- Mika, J.; Osikowicz, M.; Makuch, W.; Przewlocka, B. Minocycline and pentoxifylline attenuate allodynia and hyperalgesia and potentiate the effects of morphine in rat and mouse models of neuropathic pain. Eur. J. Pharmacol. 2007, 560, 142–149. [Google Scholar] [CrossRef]
- Bogacka, J.; Ciapala, K.; Pawlik, K.; Kwiatkowski, K.; Dobrogowski, J.; Przeklasa-Muszyńska, A.; Mika, J. CCR4 antagonist (C021) administration diminishes hypersensitivity and enhances the analgesic potency of morphine and buprenorphine in mouse model of neuropathic pain. Front. Immunol. 2020, 11, 1241. [Google Scholar] [CrossRef]
- Nozaki, C.; Saitoh, A.; Tamura, N.; Kamei, J. Antinociceptive effect of oxycodone in diabetic mice. Eur. J. Pharmacol. 2005, 524, 75–79. [Google Scholar] [CrossRef]
- Yang, P.P.; Yeh, G.C.; Huang, E.Y.; Law, P.Y.; Loh, H.H.; Tao, P.L. Effects of dextromethorphan and oxycodone on treatment of neuropathic pain in mice. J. Biomed. Sci. 2015, 22, 81. [Google Scholar] [CrossRef] [Green Version]
- Onaolapo, O.J.; Paul, T.B.; Onaolapo, A.Y. Comparative effects of sertraline, haloperidol or olanzapine treatments on ketamine-induced changes in mouse behaviours. Metab. Brain Dis. 2017, 32, 1475–1489. [Google Scholar] [CrossRef]
- Chomczynski, P.; Sacchi, N. Single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction. Anal. Biochem. 1987, 162, 156–159. [Google Scholar] [CrossRef]
- Chomczynski, P.; Sacchi, N. The single-step method of RNA isolation by acid guanidinium thiocyanate-phenol-chloroform extraction: Twenty-something years on. Nat. Protoc. 2006, 1, 581–585. [Google Scholar] [CrossRef]








Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zajączkowska, R.; Rojewska, E.; Ciechanowska, A.; Pawlik, K.; Ciapała, K.; Kocot-Kępska, M.; Makuch, W.; Wordliczek, J.; Mika, J. Mirogabalin Decreases Pain-like Behaviours and Improves Opioid and Ketamine Antinociception in a Mouse Model of Neuropathic Pain. Pharmaceuticals 2022, 15, 88. https://doi.org/10.3390/ph15010088
Zajączkowska R, Rojewska E, Ciechanowska A, Pawlik K, Ciapała K, Kocot-Kępska M, Makuch W, Wordliczek J, Mika J. Mirogabalin Decreases Pain-like Behaviours and Improves Opioid and Ketamine Antinociception in a Mouse Model of Neuropathic Pain. Pharmaceuticals. 2022; 15(1):88. https://doi.org/10.3390/ph15010088
Chicago/Turabian StyleZajączkowska, Renata, Ewelina Rojewska, Agata Ciechanowska, Katarzyna Pawlik, Katarzyna Ciapała, Magdalena Kocot-Kępska, Wioletta Makuch, Jerzy Wordliczek, and Joanna Mika. 2022. "Mirogabalin Decreases Pain-like Behaviours and Improves Opioid and Ketamine Antinociception in a Mouse Model of Neuropathic Pain" Pharmaceuticals 15, no. 1: 88. https://doi.org/10.3390/ph15010088