
A 5-Year Study of Lithium and Valproic Acid Drug Monitoring in Patients with Bipolar Disorders in an Italian Clinical Center

 , , and
, , and 
Abstract
:1. Introduction
2. Results
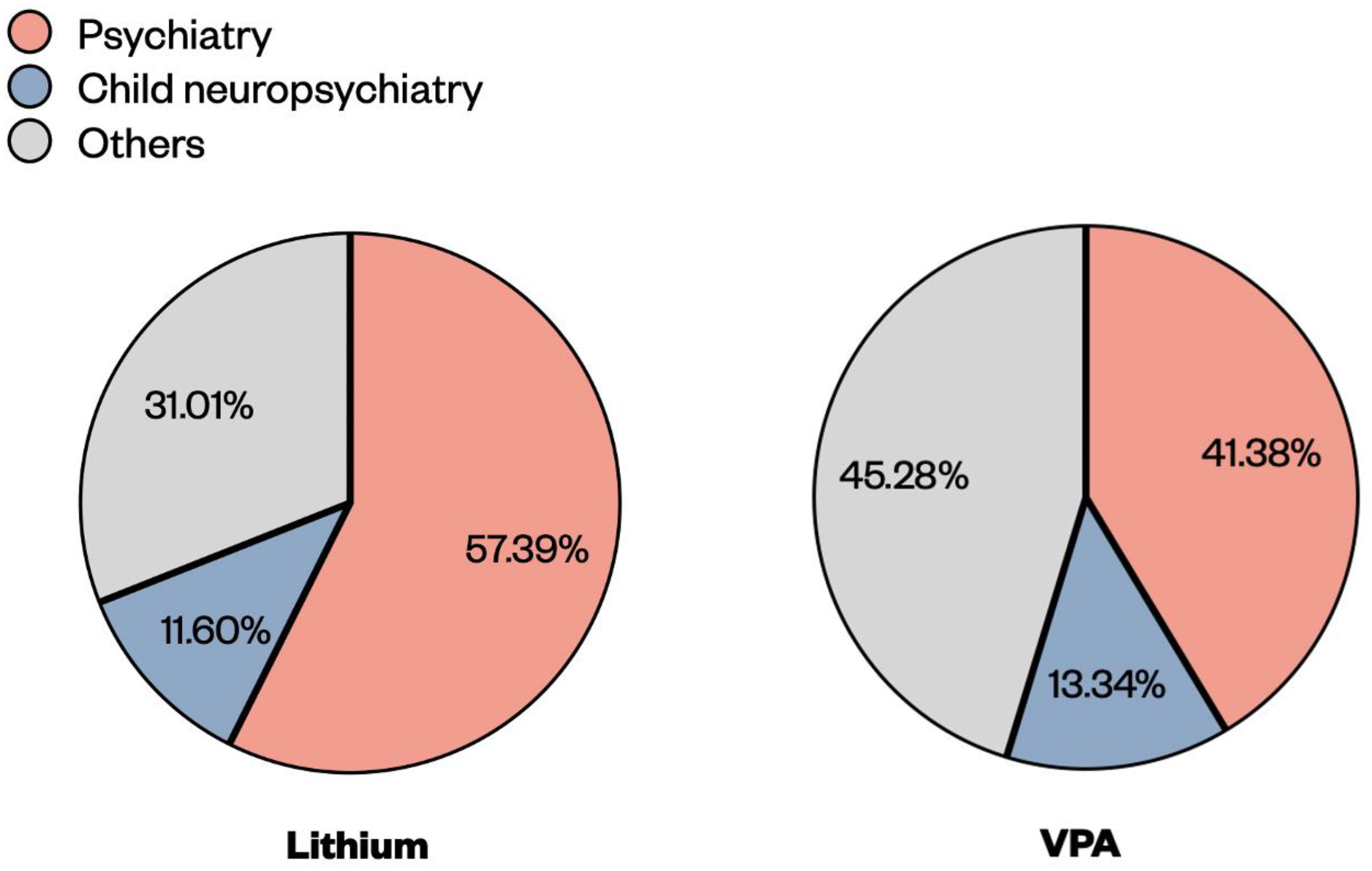
2.1. Description of the Lithium and VPA Blood Samples during the Period 2016–2020
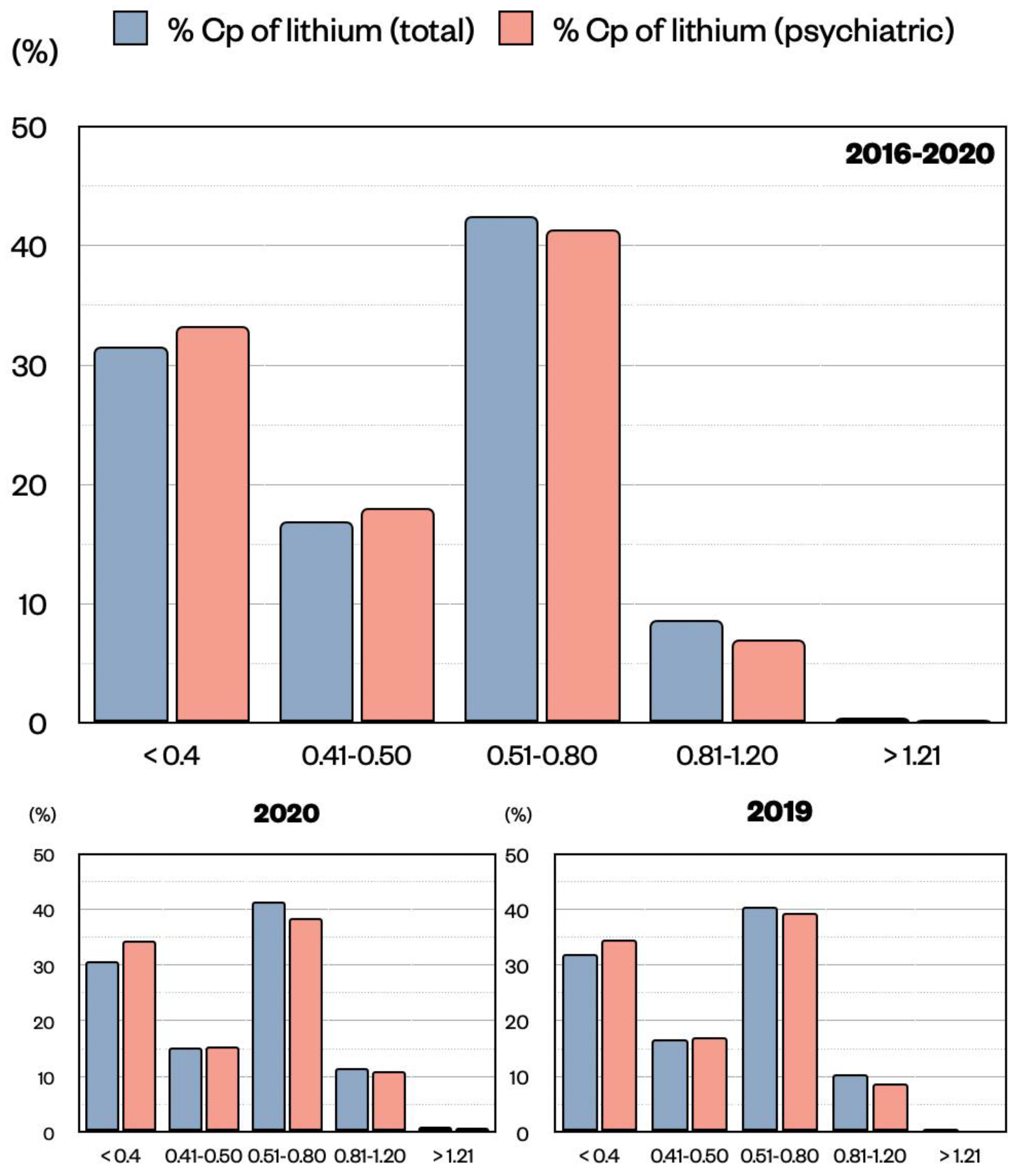
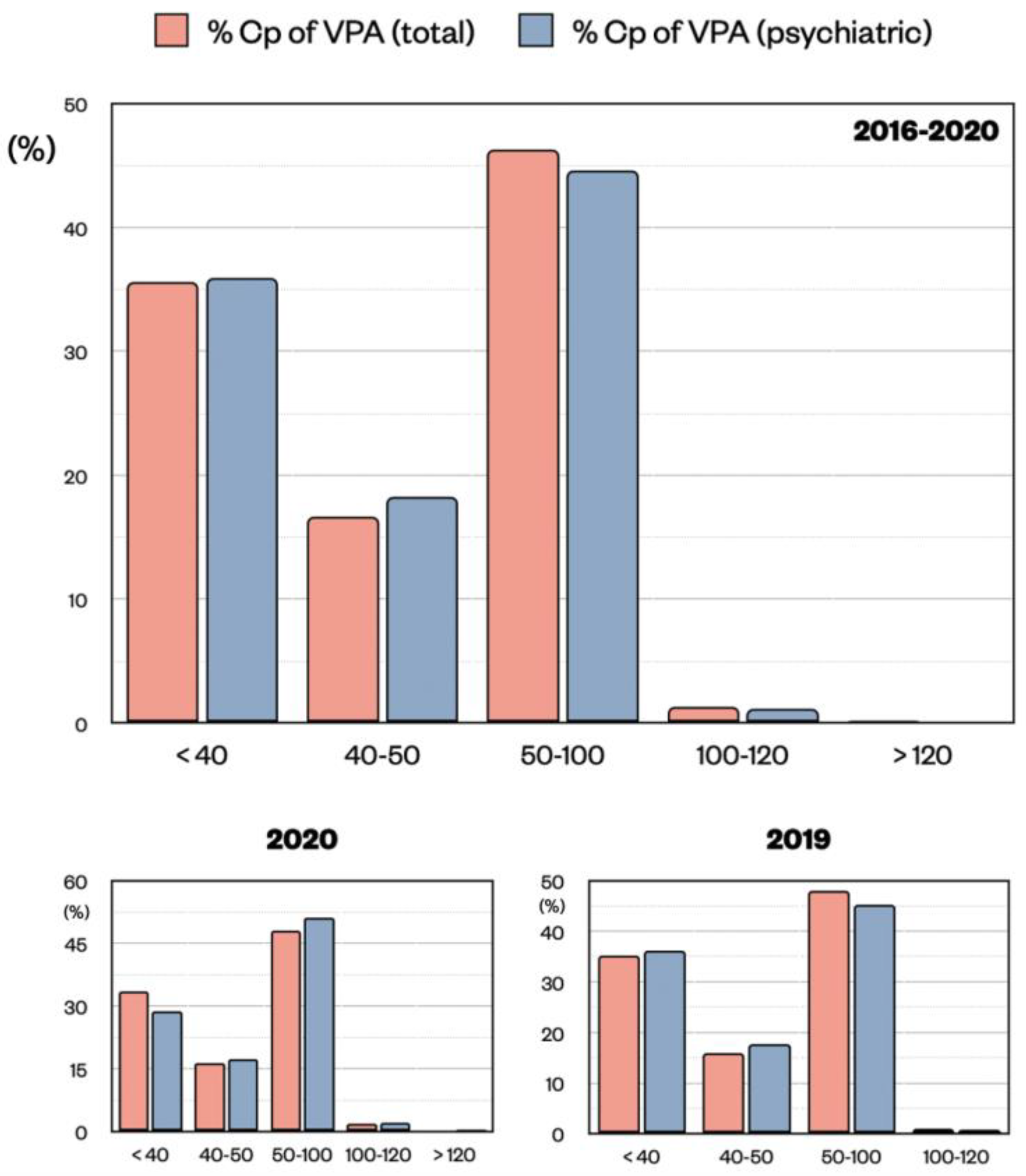
2.2. Distribution of the Lithium and VPA Cp Samples
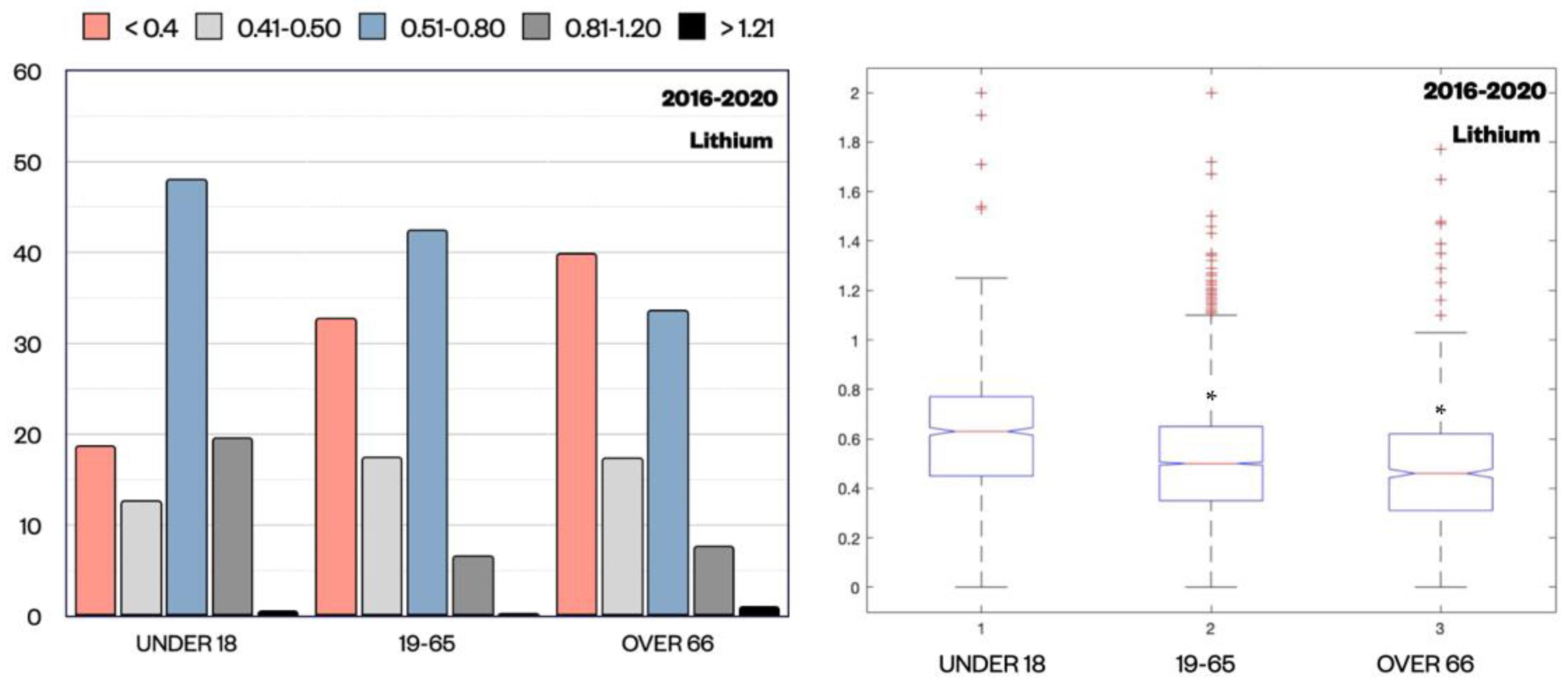
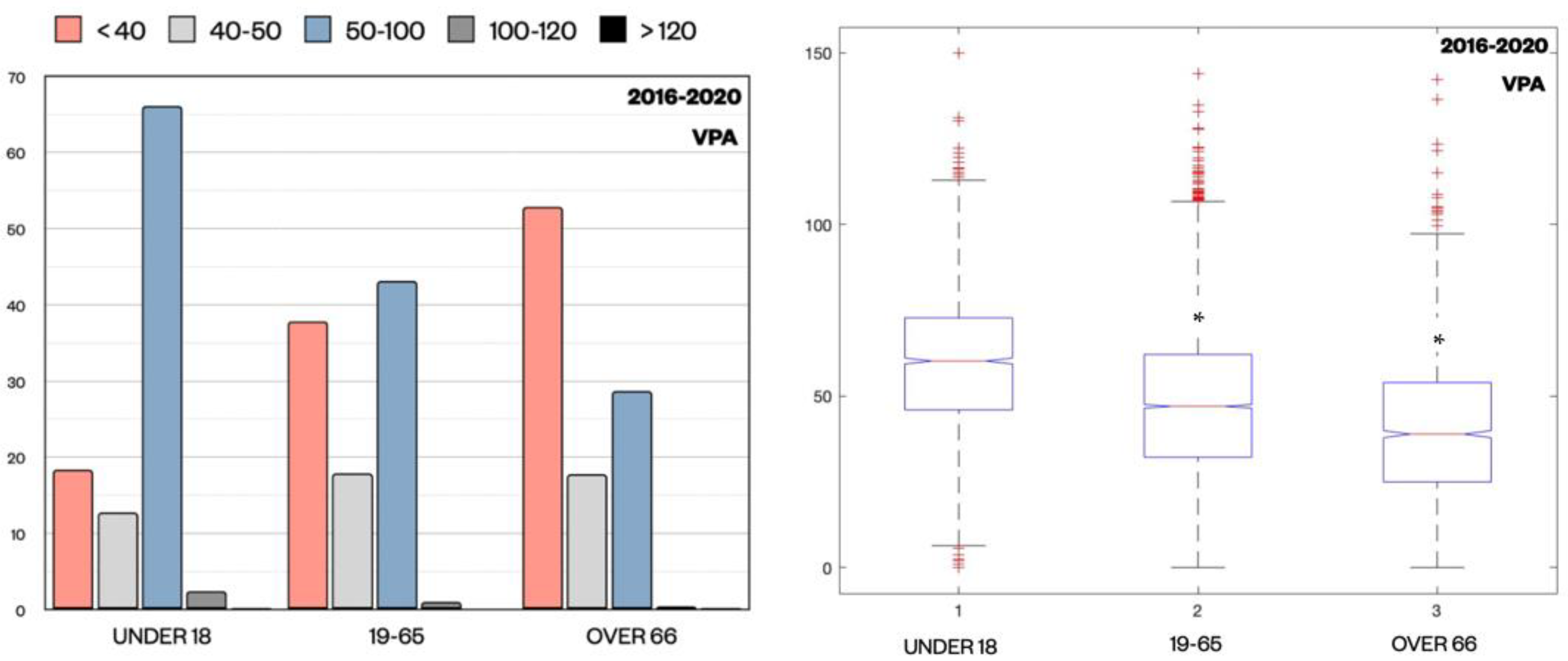
2.3. Distribution of the Lithium and VPA Cp Samples across Different Ages
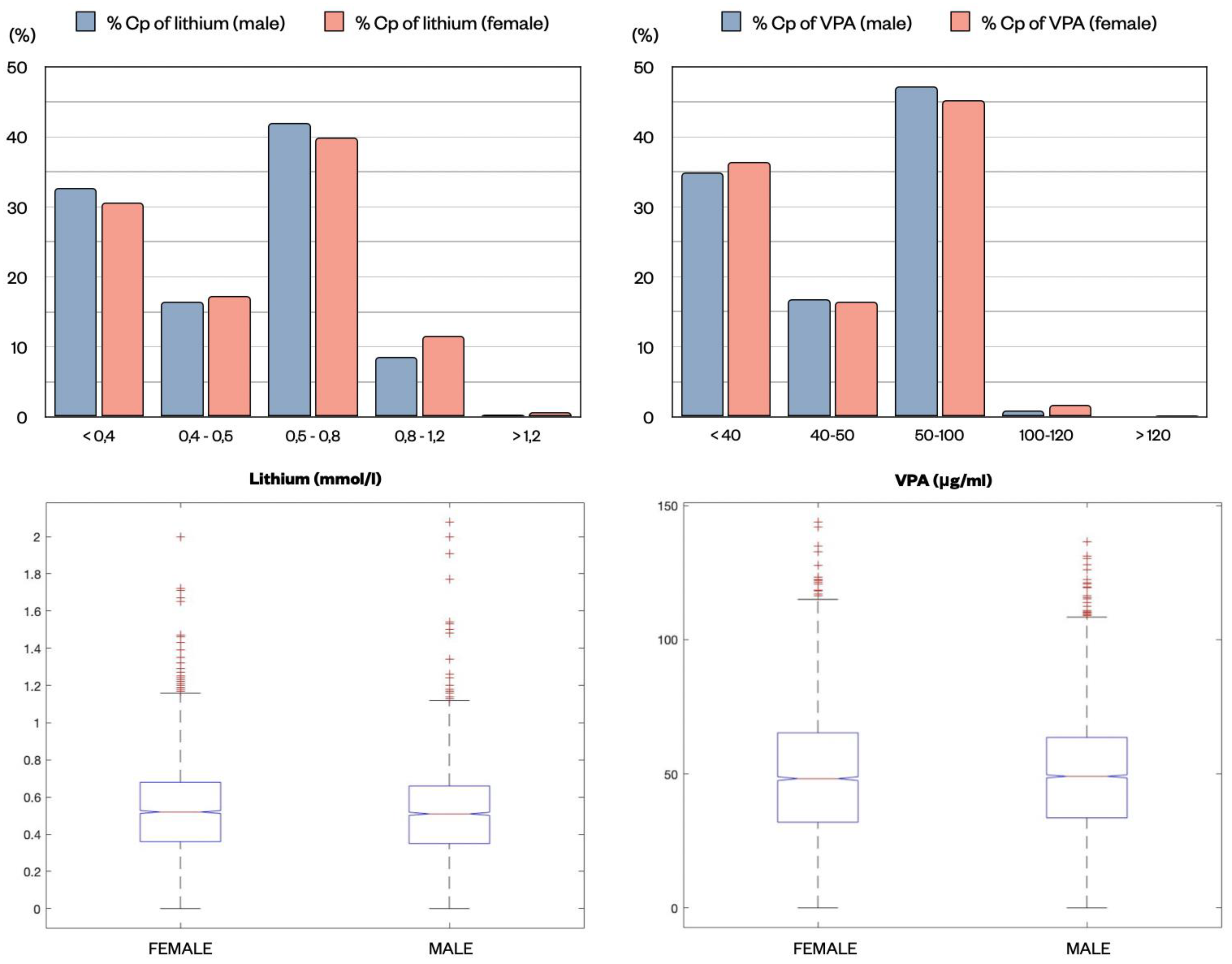
2.4. Distribution of the Lithium and VPA Cp Samples in Relation to Gender
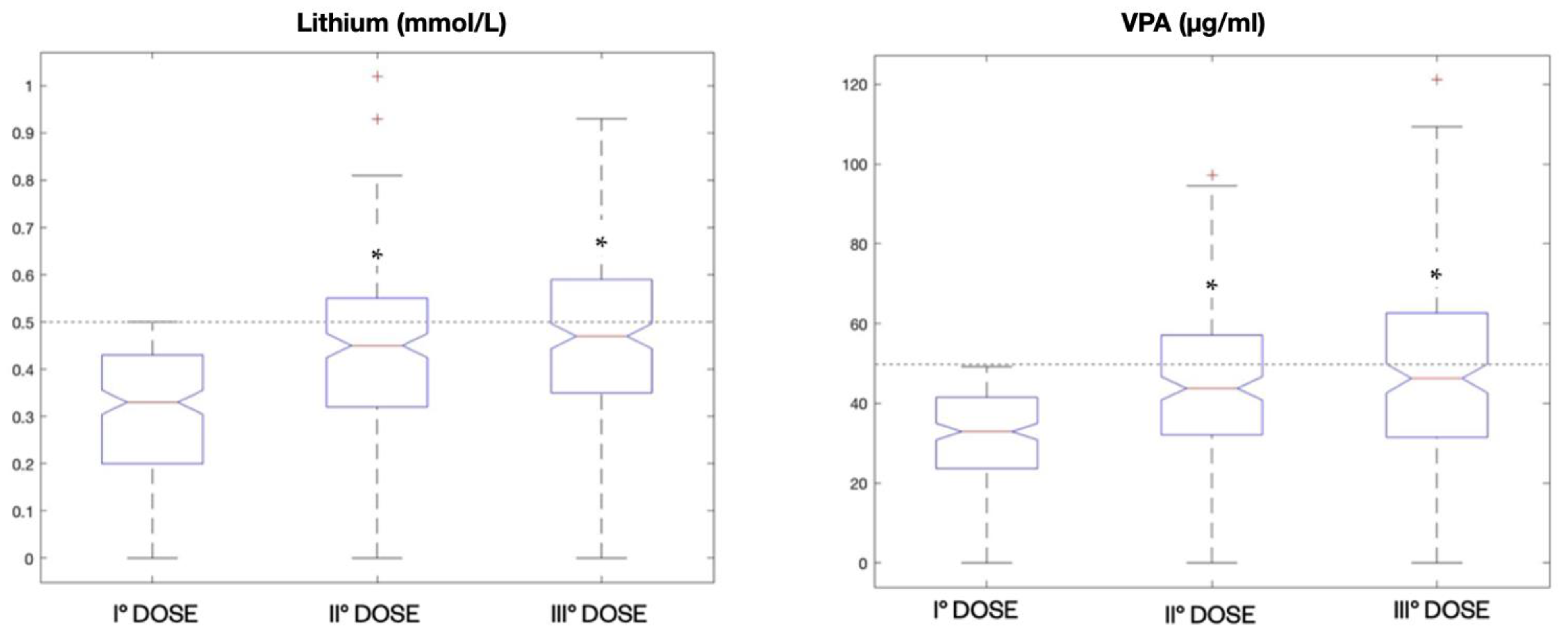
2.5. Analysis of Multiple Dosing for Patients with Lithium and VPA Subtherapeutic Cp
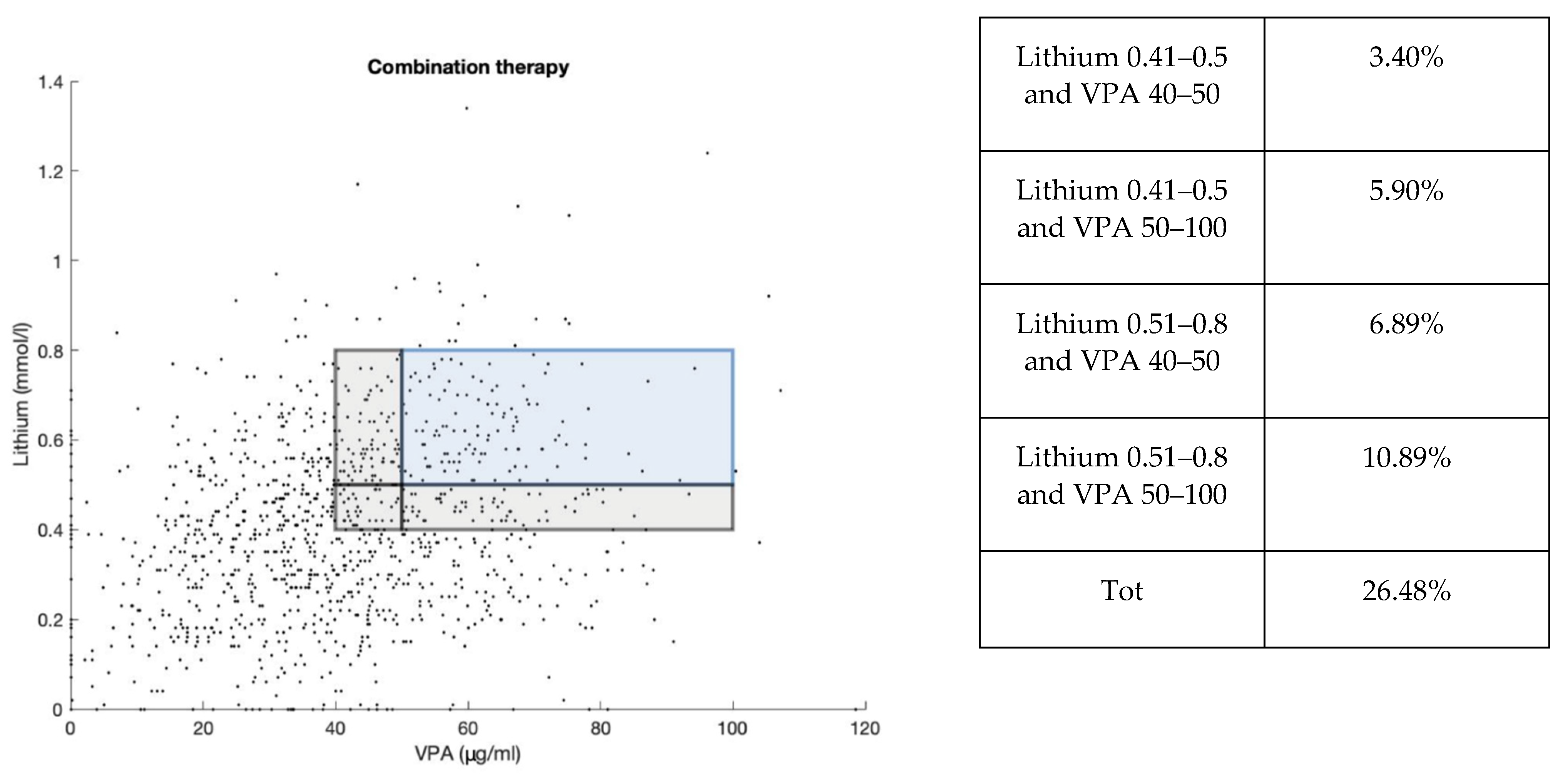
2.6. Distribution of the Lithium and VPA Cp Samples in Combination Therapy
3. Discussion
4. Materials and Methods
4.1. Sample of the Study
4.2. Analytical Determination of Lithium and VPA
4.3. Data Analysis
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Semahegn, A.; Torpey, K.; Manu, A.; Assefa, N.; Tesfaye, G.; Ankomah, A. Psychotropic medication non-adherence and its associated factors among patients with major psychiatric disorders: A systematic review and meta-analysis. Syst. Rev. 2020, 9, 17. [Google Scholar] [CrossRef] [Green Version]
- Carona, A.; Bicker, J.; Silva, R.; Fonseca, C.; Falcão, A.; Fortuna, A. Pharmacology of lacosamide: From its molecular mechanisms and pharmacokinetics to future therapeutic applications. Life Sci. 2021, 275, 119342. [Google Scholar] [CrossRef]
- Guo, J.; Huo, Y.; Li, F.; Li, Y.; Guo, Z.; Han, H.; Zhou, Y. Impact of gender, albumin, and CYP2C19 polymorphisms on valproic acid in Chinese patients: A population pharmacokinetic model. J. Int. Med. Res. 2020, 48, 0300060520952281. [Google Scholar] [CrossRef]
- Smith, R.L.; Haslemo, T.; Refsum, H.; Molden, E. Impact of age, gender and CYP2C9/2C19 genotypes on dose-adjusted steady-state serum concentrations of valproic acid—A large-scale study based on naturalistic therapeutic drug monitoring data. Eur. J. Clin. Pharmacol. 2016, 72, 1099–1104. [Google Scholar] [CrossRef] [PubMed]
- Hiemke, C.; Bergemann, N.; Clement, H.W.; Conca, A.; Deckert, J.; Domschke, K.; Eckermann, G.; Egberts, K.; Gerlach, M.; Greiner, C.; et al. Consensus Guidelines for Therapeutic Drug Monitoring in Neuropsychopharmacology: Update 2017. Pharmacopsychiatry 2018, 51, 9–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patsalos, P.N.; Berry, D.J.; Bourgeois, B.F.D.; Cloyd, J.C.; Glauser, T.A.; Johannessen, S.I.; Leppik, I.E.; Tomson, T.; Perucca, E. Antiepileptic drugs—Best practice guidelines for therapeutic drug monitoring: A position paper by the subcommission on therapeutic drug monitoring, ILAE Commission on Therapeutic Strategies. Epilepsia 2008, 49, 1239–1276. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, V.; Al-Sukhni, M.; Lawson, A.; Chandler, G. Lithium Prescribing and Therapeutic Drug Monitoring in Bipolar Disorder: A Survey of Current Practices and Perspectives. J. Psychiatr. Pract. 2020, 26, 360–366. [Google Scholar] [CrossRef]
- Müller, M.J.; Dragicevic, A.; Fric, M.; Gaertner, I.; Grasmäder, K.; Härtter, S.; Hermann, E.; Kuss, H.J.; Laux, G.; Oehl, W.; et al. Therapeutic drug monitoring of tricyclic antidepressants: How does it work under clinical conditions? Pharmacopsychiatry 2003, 36, 98–104. [Google Scholar] [CrossRef]
- Perry, P.J. Therapeutic drug monitoring of antipsychotics. Psychopharmacol. Bull. 2001, 35, 19–29. [Google Scholar]
- Connolly, K.R.; Thase, M.E. The clinical management of bipolar disorder: A review of evidence-based guidelines. Prim. Care Companion CNS Disord. 2011, 13. [Google Scholar] [CrossRef] [Green Version]
- Hodges, J.C.; Treadwell, J.; Malphrus, A.D.; Tran, X.G.; Giardino, A.P. Identification and Prevention of Antiepileptic Drug Noncompliance: The Collaborative Use of State-Supplied Pharmaceutical Data. ISRN Pediatr. 2014, 2014, 734689. [Google Scholar] [CrossRef] [PubMed]
- Perugi, G.; De Rossi, P.; Fagiolini, A.; Girardi, P.; Maina, G.; Sani, G.; Serretti, A. Personalized and precision medicine as informants for treatment management of bipolar disorder. Int. Clin. Psychopharmacol. 2019, 34, 189–205. [Google Scholar] [CrossRef]
- Barbuti, M.; Colombini, P.; Ricciardulli, S.; Amadori, S.; Gemmellaro, T.; De Dominicis, F.; Della Rocca, F.; Petrucci, A.; Schiavi, E.; Perugi, G. Treatment adherence and tolerability of immediate- and prolonged-release lithium formulations in a sample of bipolar patients: A prospective naturalistic study. Int. Clin. Psychopharmacol. 2021, 36, 230–237. [Google Scholar] [CrossRef] [PubMed]
- Geddes, J.R.; Goodwin, G.M.; Rendell, J.; Azorin, J.-M.; Cipriani, A.; Ostacher, M.J.; Morriss, R.; Alder, N.; Juszczak, E. Lithium plus valproate combination therapy versus monotherapy for relapse prevention in bipolar I disorder (BALANCE): A randomised open-label trial. Lancet 2010, 375, 385–395. [Google Scholar] [CrossRef]
- Brady, K.T.; Sonne, S.C.; Anton, R.; Ballenger, J.C. Valproate in the treatment of acute bipolar affective episodes complicated by substance abuse: A pilot study. J. Clin. Psychiatry 1995, 56, 118–121. [Google Scholar] [PubMed]
- Kemp, D.E.; Gao, K.; Ganocy, S.J.; Elhaj, O.; Bilali, S.R.; Conroy, C.; Findling, R.L.; Calabrese, J.R. A 6-month, double-blind, maintenance trial of lithium monotherapy versus the combination of lithium and divalproex for rapid-cycling bipolar disorder and Co-occurring substance abuse or dependence. J. Clin. Psychiatry 2009, 70, 113–121. [Google Scholar] [CrossRef] [Green Version]
- Lin, D.; Mok, H.; Yatham, L.N. Polytherapy in bipolar disorder. CNS Drugs 2006, 20, 29–42. [Google Scholar] [CrossRef]
- Wingård, L.; Brandt, L.; Bodén, R.; Kieler, H.; Andersen, M.; Reutfors, J. Monotherapy vs. combination therapy for post mania maintenance treatment: A population based cohort study. Eur. Neuropsychopharmacol. J. Eur. Coll. Neuropsychopharmacol. 2019, 29, 691–700. [Google Scholar] [CrossRef]
- Aringhieri, S.; Carli, M.; Kolachalam, S.; Verdesca, V.; Cini, E.; Rossi, M.; McCormick, P.J.; Corsini, G.U.; Maggio, R.; Scarselli, M. Molecular targets of atypical antipsychotics: From mechanism of action to clinical differences. Pharmacol. Ther. 2018, 192, 20–41. [Google Scholar] [CrossRef]
- Aringhieri, S.; Kolachalam, S.; Gerace, C.; Carli, M.; Verdesca, V.; Brunacci, M.G.; Rossi, C.; Ippolito, C.; Solini, A.; Corsini, G.U.; et al. Clozapine as the most efficacious antipsychotic for activating ERK 1/2 kinases: Role of 5-HT2A receptor agonism. Eur. Neuropsychopharmacol. 2017, 27, 383–398. [Google Scholar] [CrossRef] [PubMed]
- Carli, M.; Kolachalam, S.; Longoni, B.; Pintaudi, A.; Baldini, M.; Aringhieri, S.; Fasciani, I.; Annibale, P.; Maggio, R.; Scarselli, M. Atypical antipsychotics and metabolic syndrome: From molecular mechanisms to clinical differences. Pharmaceuticals 2021, 14, 238. [Google Scholar] [CrossRef] [PubMed]
- Severus, W.E.; Kleindienst, N.; Seemüller, F.; Frangou, S.; Möller, H.J.; Greil, W. What is the optimal serum lithium level in the long-term treatment of bipolar disorder--a review? Bipolar Disord. 2008, 10, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Del Grande, C.; Muti, M.; Musetti, L.; Pergentini, I.; Corsi, M.; Turri, M.; Soldani, I.; Corsini, G.U.; Dell’Osso, L. Long-term treatment of bipolar disorder: How should we use lithium salts? Riv. Psichiatr. 2012, 47, 515–526. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, M. Lithium side effects and toxicity: Prevalence and management strategies. Int. J. Bipolar Disord. 2016, 4, 27. [Google Scholar] [CrossRef] [Green Version]
- Bocchetta, A.; Ardau, R.; Fanni, T.; Sardu, C.; Piras, D.; Pani, A.; Del Zompo, M. Renal function during long-term lithium treatment: A cross-sectional and longitudinal study. BMC Med. 2015, 13, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Muti, M.; Del Grande, C.; Musetti, L.; Marazziti, D.; Pergentini, I.; Corsi, M.; Turri, M.; Umberto Corsini, G.; Dell’Osso, L. Prescribing patterns of lithium or lithium+valproate in manic or mixed episodes: A naturalistic study. Int. Clin. Psychopharmacol. 2013, 28, 305–311. [Google Scholar] [CrossRef]
- Ghodke-Puranik, Y.; Thorn, C.F.; Lamba, J.K.; Leeder, J.S.; Song, W.; Birnbaum, A.K.; Altman, R.B.; Klein, T.E. Valproic acid pathway. Pharmacogenet. Genom. 2013, 23, 236–241. [Google Scholar] [CrossRef] [Green Version]
- Cucchiara, F.; Pasqualetti, F.; Giorgi, F.S.; Danesi, R.; Bocci, G. Epileptogenesis and oncogenesis: An antineoplastic role for antiepileptic drugs in brain tumours? Pharmacol. Res. 2020, 156, 104786. [Google Scholar] [CrossRef]
- Allen, M.H.; Hirschfeld, R.M.; Wozniak, P.J.; Baker, J.D.; Bowden, C.L. Linear relationship of valproate serum concentration to response and optimal serum levels for acute mania. Am. J. Psychiatry 2006, 163, 272–275. [Google Scholar] [CrossRef]
- Haddad, P.M.; Das, A.; Ashfaq, M.; Wieck, A. A review of valproate in psychiatric practice. Expert Opin. Drug Metab. Toxicol. 2009, 5, 539–551. [Google Scholar] [CrossRef]
- Chateauvieux, S.; Morceau, F.; Dicato, M.; Diederich, M. Molecular and therapeutic potential and toxicity of valproic acid. J. Biomed. Biotechnol. 2010, 2010. [Google Scholar] [CrossRef] [Green Version]
- Touw, D.J.; Neef, C.; Thomson, A.H.; Vinks, A.A. Cost-effectiveness of therapeutic drug monitoring: A systematic review. Ther. Drug Monit. 2005, 27, 10–17. [Google Scholar] [CrossRef]
- Marcus, S.C.; Olfson, M.; Pincus, H.A.; Zarin, D.A.; Kupfer, D.J. Therapeutic drug monitoring of mood stabilizers in medicaid patients with bipolar disorder. Am. J. Psychiatry 1999, 156, 1014–1018. [Google Scholar] [CrossRef]
- Chiu, C.-T.; Wang, Z.; Hunsberger, J.G.; Chuang, D.-M. Therapeutic potential of mood stabilizers lithium and valproic acid: Beyond bipolar disorder. Pharmacol. Rev. 2013, 65, 105–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, S.; Joshi, S.; Chadda, R.K. Therapeutic Drug Monitoring of Lithium in Patients With Bipolar Affective Disorder: Experiences From a Tertiary Care Hospital in India. Am. J. Ther. 2009, 16, 393–397. [Google Scholar] [CrossRef]
- Keller, M.B.; Lavori, P.W.; Kane, J.M.; Gelenberg, A.J.; Rosenbaum, J.F.; Walzer, E.A.; Baker, L.A. Subsyndromal symptoms in bipolar disorder. A comparison of standard and low serum levels of lithium. Arch. Gen. Psychiatry 1992, 49, 371–376. [Google Scholar] [CrossRef] [PubMed]
- Amdisen, A. Monitoring of lithium treatment through determination of lithium concentration. Dan. Med. Bull. 1975, 22, 277–291. [Google Scholar]
- Nonaka, S.; Hough, C.J.; Chuang, D.M. Chronic lithium treatment robustly protects neurons in the central nervous system against excitotoxicity by inhibiting N-methyl-D-aspartate receptor-mediated calcium influx. Proc. Natl. Acad. Sci. USA 1998, 95, 2642–2647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adams, J.M.; Cory, S. The Bcl-2 protein family: Arbiters of cell survival. Science 1998, 281, 1322–1326. [Google Scholar] [CrossRef]
- Berger, G.E.; Wood, S.J.; Ross, M.; Hamer, C.A.; Wellard, R.M.; Pell, G.; Phillips, L.; Nelson, B.; Amminger, G.P.; Yung, A.R.; et al. Neuroprotective effects of low-dose lithium in individuals at ultra-high risk for psychosis. A longitudinal MRI/MRS study. Curr. Pharm. Des. 2012, 18, 570–575. [Google Scholar] [CrossRef]
- Jacobsen, F.M. Low-dose valproate: A new treatment for cyclothymia, mild rapid cycling disorders, and premenstrual syndrome. J. Clin. Psychiatry 1993, 54, 229–234. [Google Scholar] [PubMed]
- Dolder, C.; Mckinsey, J. Low-Dose Divalproex in Agitated Patients with Alzheimer’s Disease. J. Psychiatr. Pract. 2010, 16, 63–67. [Google Scholar] [CrossRef] [PubMed]
- Rapoport, S.I.; Basselin, M.; Kim, H.-W.; Rao, J.S. Bipolar disorder and mechanisms of action of mood stabilizers. Brain Res. Rev. 2009, 61, 185–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, V.; Persad, E.; Mazmanian, D.; Karunaratne, K. Treatment of rapid cycling bipolar disorder with combination therapy of valproate and lithium. Can. J. Psychiatry 1993, 38, 137–139. [Google Scholar] [CrossRef]
- Freeman, M.P.; Stoll, A.L. Mood stabilizer combinations: A review of safety and efficacy. Am. J. Psychiatry 1998, 155, 12–21. [Google Scholar] [CrossRef]
- Cipriani, A.; Reid, K.; Young, A.H.; Macritchie, K.; Geddes, J. Valproic acid, valproate and divalproex in the maintenance treatment of bipolar disorder. Cochrane Database Syst. Rev. 2013, 2013, CD003196. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lithium | VPA | |||
|---|---|---|---|---|
| Samples (n) | [Median] mmol/L (IQR) | Samples (n) | [Median] µg/mL (IQR) | |
| 2016 | 205 | 0.46 (0.26) | 1829 | 47.40 (30.80) |
| 2017 | 1529 | 0.50 (0.30) | 2660 | 47.20 (31.25) |
| 2018 | 2188 | 0.52 (0.31) | 2908 | 49.50 (31.25) |
| 2019 | 1989 | 0.52 (0.31) | 2642 | 49.25 (32.20) |
| 2020 | 1538 | 0.53 (0.33) | 2255 | 50.20 (31.70) |
| Total | 7449 | 0.52 (0.31) | 12294 | 48.70 (31.60) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Carli, M.; Risaliti, E.; Francomano, M.; Kolachalam, S.; Longoni, B.; Bocci, G.; Maggio, R.; Scarselli, M. A 5-Year Study of Lithium and Valproic Acid Drug Monitoring in Patients with Bipolar Disorders in an Italian Clinical Center. Pharmaceuticals 2022, 15, 105. https://doi.org/10.3390/ph15010105
Carli M, Risaliti E, Francomano M, Kolachalam S, Longoni B, Bocci G, Maggio R, Scarselli M. A 5-Year Study of Lithium and Valproic Acid Drug Monitoring in Patients with Bipolar Disorders in an Italian Clinical Center. Pharmaceuticals. 2022; 15(1):105. https://doi.org/10.3390/ph15010105
Chicago/Turabian StyleCarli, Marco, Eleonora Risaliti, Mena Francomano, Shivakumar Kolachalam, Biancamaria Longoni, Guido Bocci, Roberto Maggio, and Marco Scarselli. 2022. "A 5-Year Study of Lithium and Valproic Acid Drug Monitoring in Patients with Bipolar Disorders in an Italian Clinical Center" Pharmaceuticals 15, no. 1: 105. https://doi.org/10.3390/ph15010105