
Withdrawal Symptoms Following Discontinuation of Vortioxetine—Retrospective Chart Review

 ,
,  ,
,
Abstract
:1. Introduction
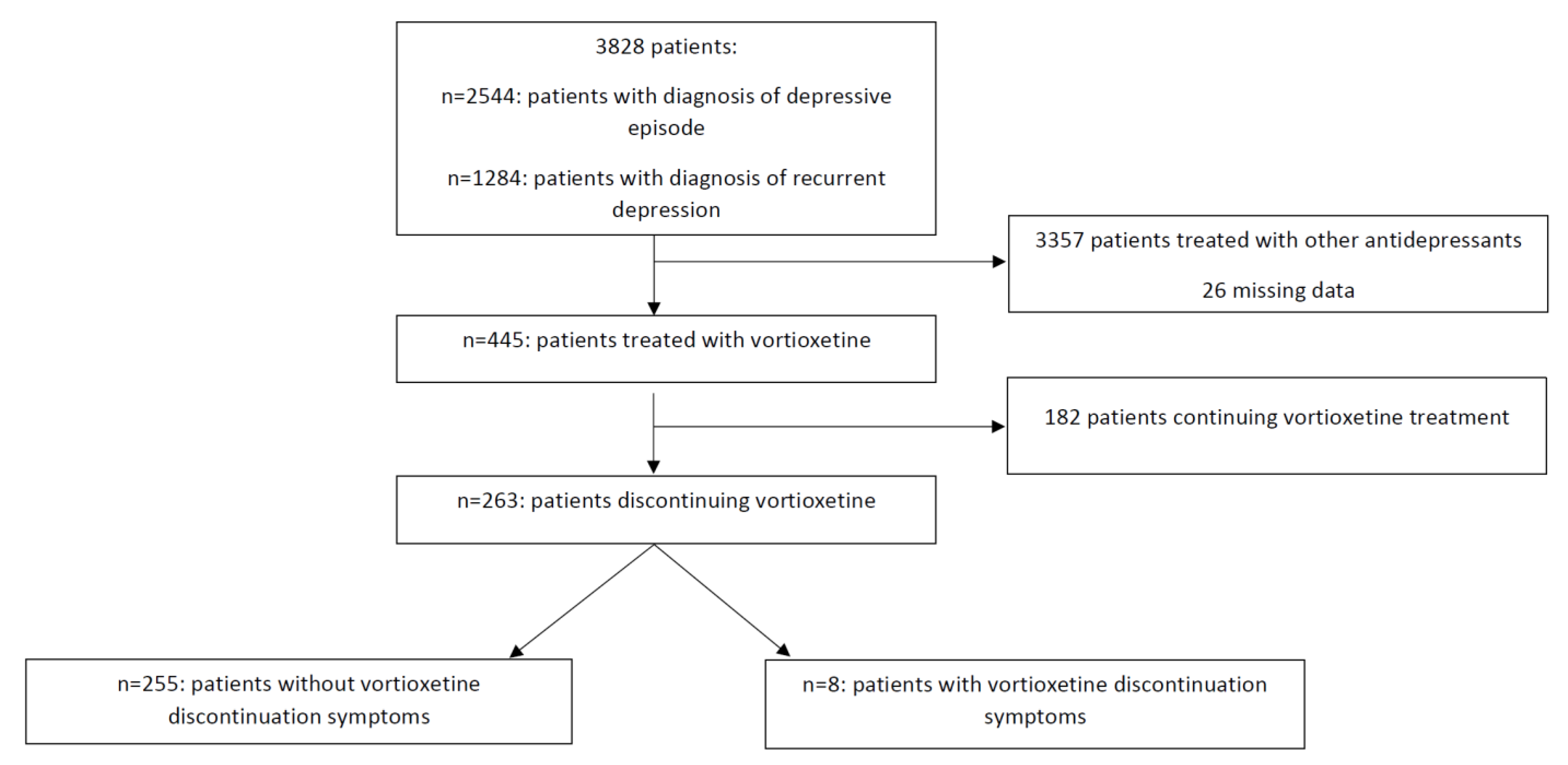
2. Results
3. Discussion
4. Materials and Methods
Data Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Grohol, J. Top 25 Psychiatric Medication Prescriptions for 2013. Available online: https://psychcentral.com/lib/top-25-psychiatric-medication-prescriptions-for-2013/ (accessed on 18 April 2021).
- Mann, A.M.; Macpherson, A.S. Clinical experience with imipramine (G22355) in the treatment of depression. Can. Psychiatr. Assoc. J. 1959, 4, 38–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Keks, N.; Hope, J.; Keogh, S. Switching and stopping antidepressants. Aust. Prescr. 2016, 39, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Heitzman, J.; Solak, M. Zespół objawów odstawiennych po lekach antydepresyjnych w badaniach naukowych-Implikacje dla lekarzy i pacjentów. Psychiatr. Pol. 2009, 43, 545–555. [Google Scholar] [PubMed]
- Warner, C.H.; Bobo, W.; Warner, C.; Reid, S.; Rachal, J. Antidepressant discontinuation syndrome. Am. Fam. Physician 2006, 74, 449–456. [Google Scholar] [PubMed]
- Schweitzer, I.; Maguire, K. Stopping antidepressants. Aust. Prescr. 2001, 24, 13–15. [Google Scholar]
- Haddad, P.M.; Anderson, I.M. Recognising and managing antidepressant discontinuation symptoms. Adv. Psychiatr. Treat. 2007, 13, 447–457. [Google Scholar] [CrossRef]
- Ivd, W.; Ashby, D.; Brook, R.; Mga, C.; Chick, J.; Drummond, C.; Ebmeier, K.P.; Gunnell, D.; Hawking, H.; Mukaetova-Ladinska, E.; et al. Report of the CSM Expert Working Group on the Safety of Selective Serotonin Reuptake Inhibitor Antidepressants; MHRA: Oxford, UK, 2005. [Google Scholar]
- Carvalho, A.F.; Sharma, M.S.; Brunoni, A.R.; Vieta, E.; Fava, G.A. The Safety, Tolerability and Risks Associated with the Use of Newer Generation Antidepressant Drugs: A Critical Review of the Literature. Psychother. Psychosom. 2016, 85, 270–288. [Google Scholar] [CrossRef]
- Fava, G.A.; Gatti, A.; Belaise, C.; Guidi, J.; Offidani, E. Withdrawal symptoms after selective serotonin reuptake inhibitor discontinuation: A systematic review. Psychother. Psychosom. 2015, 84, 72–81. [Google Scholar]
- Campagne, D.M. Venlafaxine and serious withdrawal symptoms: Warning to drivers. Med. Gen. Med. 2005, 7, 22. [Google Scholar]
- Perahia, D.G.; Kajdasz, D.K.; Desaiah, D.; Haddad, P.M. Symptoms following abrupt discontinuation of duloxetine treatment in patients with major depressive disorder. J. Affect. Disord. 2005, 89, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Curtin, F.; Berney, P.; Kaufmann, C. Moclobemide discontinuation syndrome predominantly presenting with influenza-like symptoms. J. Psychopharmacol. 2002, 16, 271–272. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2016/020415s030lbl.pdf (accessed on 11 April 2021).
- Verma, J.K.; Mohapatra, S. Mirtazapine withdrawal-induced mania. J. Pharmacol. Pharmacother. 2015, 6, 214–215. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berigan, T.R. Mirtazapine-Associated Withdrawal Symptoms: A Case Report. Prim. Care Companion J. Clin. Psychiatry 2001, 3, 143. [Google Scholar] [CrossRef] [PubMed]
- Kuniyoshi, M.; Arikawa, K.; Miura, C.; Inanaga, K. Panic Anxiety after Abrupt Discontinuation of Mianserin. Psychiatry Clin. Neurosci. 1989, 43, 155–159. [Google Scholar] [CrossRef]
- Plesničar, B.K. Efficacy and tolerability of agomelatine in the treatment of depression. Patient Prefer. Adherence 2014, 8, 603–612. [Google Scholar]
- Stoukides, J.A.; Stoukides, C.A. Extrapyramidal symptoms upon discontinuation of fluoxetine. Am. J. Psychiatry 1991, 148, 1263. [Google Scholar]
- Narayan, V.; Haddad, P.M. Antidepressant discontinuation manic states: A critical review of the literature and suggested diagnostic criteria. J. Psychopharmacol. 2011, 25, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Blum, D.; Maldonado, J.; Meyer, E.; Lansberg, M. Delirium following abrupt discontinuation of fluoxetine. Clin. Neurol. Neurosurg. 2008, 110, 69–70. [Google Scholar] [CrossRef]
- Van Noorden, M.S.; Vergouwen, A.C.M.; Koerselman, G.F. Delirium bij afbouw van venlafaxine. Ned. Tijdschr. Geneeskd. 2002, 146, 1236–1237. [Google Scholar] [PubMed]
- Wang, J.; Greenberg, H. Status cataplecticus precipitated by abrupt withdrawal of venlafaxine. J. Clin. Sleep Med. 2013, 9, 715–716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabljić, V.; Ružić, K.; Rakun, R. Venlafaxine withdrawal syndrome. Psychiatr. Danub. 2011, 23, 117–119. [Google Scholar]
- Haddad, P.; Devarajan, S.; Dursun, S. Antidepressant discontinuation (withdrawal) symptoms presenting as “stroke”. J. Psychopharmacol. 2001, 15, 139–141. [Google Scholar] [CrossRef]
- Jacobsen, P.L.; Mahableshwarkar, A.R.; Serenko, M.; Chan, S.; Trivedi, M.H. A randomized, double-blind, placebo-controlled study of the efficacy and safety of vortioxetine 10 mg and 20 mg in adults with major depressive disorder. J. Clin. Psychiatry 2015, 76, 575–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baldwin, D.S.; Chrones, L.; Florea, I.; Nielsen, R.; Nomikos, G.G.; Palo, W.; Reines, E. The safety and tolerability of vortioxetine: Analysis of data from randomized placebo-controlled trials and open-label extension studies. J. Psychopharmacol. 2016, 30, 242–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cubała, W.; Landowski, J.; Springer, J. Discontinuation-emergent signs and symptoms inventory-Polish translation of the discontinuation signs and symptoms checklist. Psychiatr. Pol. 2013, 47, 715–725. [Google Scholar] [PubMed]
- Rosenthal, R. Meta-Analytic Procedures for Social Research; SAGE Publications, Inc.: Newbury Park, CA, USA; London, UK; New Delhi, India, 2011. [Google Scholar]
- Zhang, J.; Mathis, M.V.; Sellers, J.W.; Kordzakhia, G.; Jackson, A.J.; Dow, A.; Yang, P.; Fossom, L.; Zhu, H.; Patel, H.; et al. The US Food and Drug Administration’s perspective on the new antidepressant vortioxetine. J. Clin. Psychiatry 2015, 76, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Rosenbaum, J.F.; Fava, M.; Hoog, S.L.; Ascroft, R.C.; Krebs, W.B. Selective serotonin reuptake inhibitor discontinuation syndrome: A randomized clinical trial. Biol. Psychiatry 1998, 44, 77–87. [Google Scholar] [CrossRef]
- Sowa-Kućma, M.; Pańczyszyn-Trzewik, P.; Misztak, P.; Jaeschke, R.R.; Sendek, K.; Styczeń, K.; Datka, W.; Koperny, M. Vortioxetine: A review of the pharmacology and clinical profile of the novel antidepressant. Pharmacol. Rep. 2017, 69, 595–601. [Google Scholar] [CrossRef]


{kind=link}
| KERRYPNX | Patients without Vortioxetine Discontinuation Symptoms (n = 255) | Patients with Vortioxetine Discontinuation Symptoms (n = 8) | p |
|---|---|---|---|
| Age (median number of years, (25th percentile–75th percentile)) | 39 (30–51) | 31 (27–52.8) | pMann–Whitney = 0.326 |
| Sex (women/men) | 143/112 | 5/3 | pFisher’s exact test > 0.999 |
| Therapy (% of patients with monotherapy) | 23.5% | 62.5% | pFisher’s exact test = 0.024 |
| Vortioxetine dose (mean mg, (SD)) | 10.58 (2.38) | 11.25 (2.32) | pMann–Whitney = 0.057 |
| Somatic comorbidities (%) | 20% | 37.5% | pFisher’s exact test = 0.212 |
| Number of psychiatric comorbidities | pFisher’s exact test = 0.947 | ||
| 0 | 36.9% | 50% | |
| 1 | 36.1% | 37.5% | |
| 2 | 19.6% | 12.5% | |
| 3 | 5.9% | 0% | |
| 4 | 1.6% | 0% | |
| Comorbid anxiety disorders (% of patients) | 42% | 50% | PFisher’s exact test = 0.725 |
| Days of pharmacotherapy prior to discontinuation (median number of days, (25th percentile–75th percentile)) | 74 (38.8–170.3) | 272 (71–375) | pMann–Whitney = 0.032 |
| Discontinuing: gradual or sudden (n, (%) of sudden) | 208 (81.6%) | 5 (62.5%) | pFisher’s exact test = 0.179 |
| Discontinuing: with or without prior medical advice (n, (%) of without) | 47 (18.4%) | 5 (62. 5%) | pFisher’s exact test = 0.009 * |
| Reason for discontinuation (n, (%)) | pFFH < 0.001 * | ||
| Side effects | 40 (17.3%) | 1 (14.3%) | |
| Lack of effectiveness | 135 (58.4%) | 0 (0%) | |
| Symptomatic improvement/remission | 32 (13.9%) | 2 (28.5%) | |
| Accidental discontinuation | 2 (0.9%) | 4 (57.1%) | |
| Others | 22 (9.5%) | 0 (0%) | |
| Switch to different antidepressant medication (n, (%)) | pFisher’s exact test = 0.003 * | ||
| SSRI | 134 (52.5%) | 0 (0%) | |
| Other | 37 (14.5%) | 2 (25%) | |
| No switch | 69 (27%) | 6 (75%) | |
| Median DESS score (range) | 4 (4–6) | ||
| Median number of days between vortioxetine withdrawal and emergence of DS (n, (25th percentile–75th percentile)) | - | 3 (1.25–4.75) |
| DS Symptom | No. of Patients (%) |
|---|---|
| DESS symptoms | |
| Lability | 8 (100%) |
| Irritability | 6 (75%) |
| Sudden worsening of mood | 6 (75%) |
| Nervousness | 3 (38%) |
| Agitation | 3 (38%) |
| Tearfulness | 2 (25%) |
| Headache | 2 (25%) |
| Concentration deficits | 1 (13%) |
| Stomach cramps | 1 (13%) |
| Sleep disorders | 1 (13%) |
| Tremor | 1 (13%) |
| Dizziness | 1 (13%) |
| Hypersensitivity to stimuli | 1 (13%) |
| Symptoms not represented in DESS | |
| Anergy | 2 (25%) |
| Apathy | 1 (13%) |
| Amotivation | 1 (13%) |
| Physical weakness | 1 (13%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Siwek, M.; Chrobak, A.A.; Gorostowicz, A.; Krupa, A.J.; Dudek, D. Withdrawal Symptoms Following Discontinuation of Vortioxetine—Retrospective Chart Review. Pharmaceuticals 2021, 14, 451. https://doi.org/10.3390/ph14050451
Siwek M, Chrobak AA, Gorostowicz A, Krupa AJ, Dudek D. Withdrawal Symptoms Following Discontinuation of Vortioxetine—Retrospective Chart Review. Pharmaceuticals. 2021; 14(5):451. https://doi.org/10.3390/ph14050451
Chicago/Turabian StyleSiwek, Marcin, Adrian Andrzej Chrobak, Aleksandra Gorostowicz, Anna Julia Krupa, and Dominika Dudek. 2021. "Withdrawal Symptoms Following Discontinuation of Vortioxetine—Retrospective Chart Review" Pharmaceuticals 14, no. 5: 451. https://doi.org/10.3390/ph14050451