
Towards a Miniaturized Photoacoustic Sensor for Transcutaneous CO2 Monitoring

Abstract
:1. Introduction
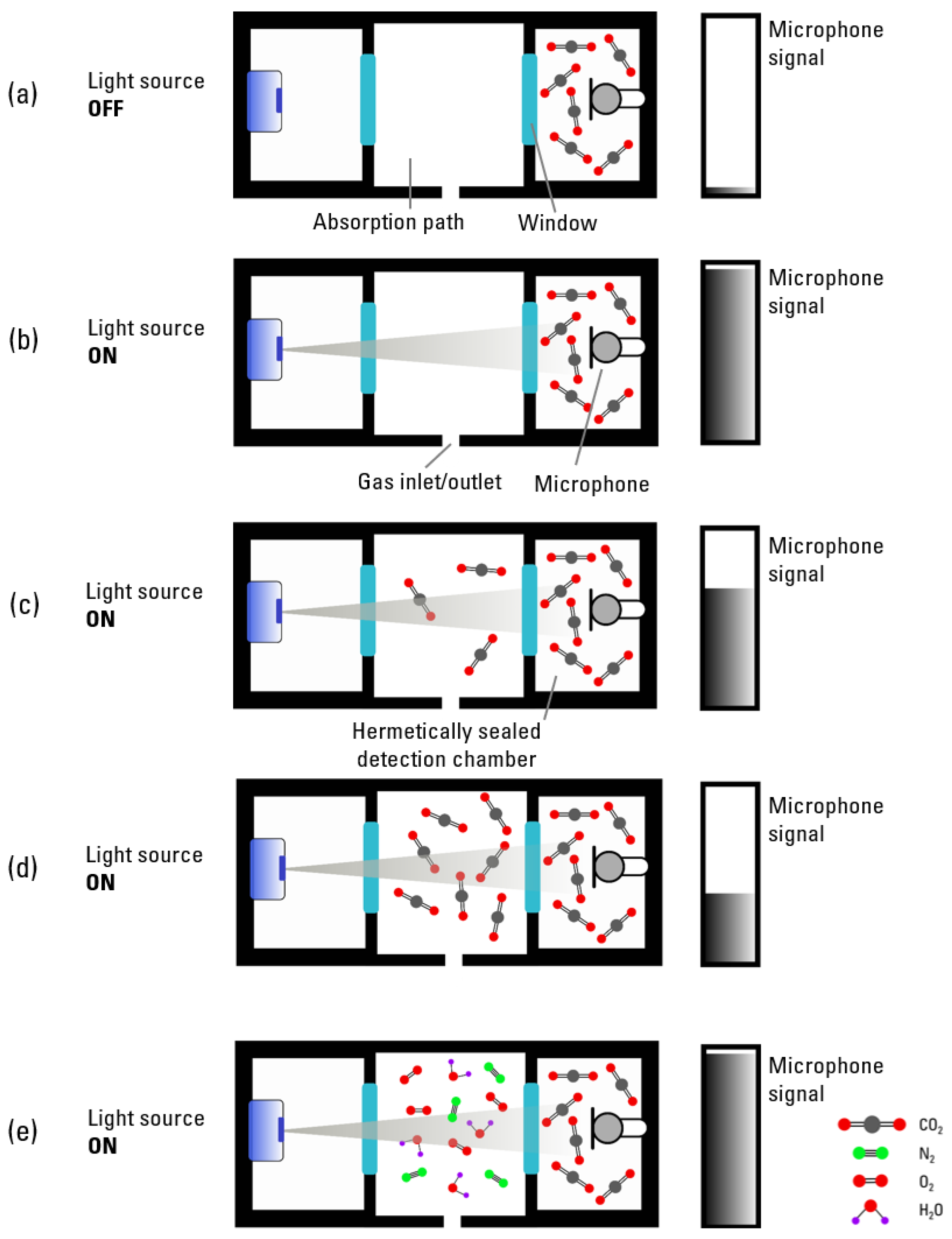
2. Theoretical Background of the Photoacoustic Sensor System
3. Material and Methods
3.1. Laboratory Setup
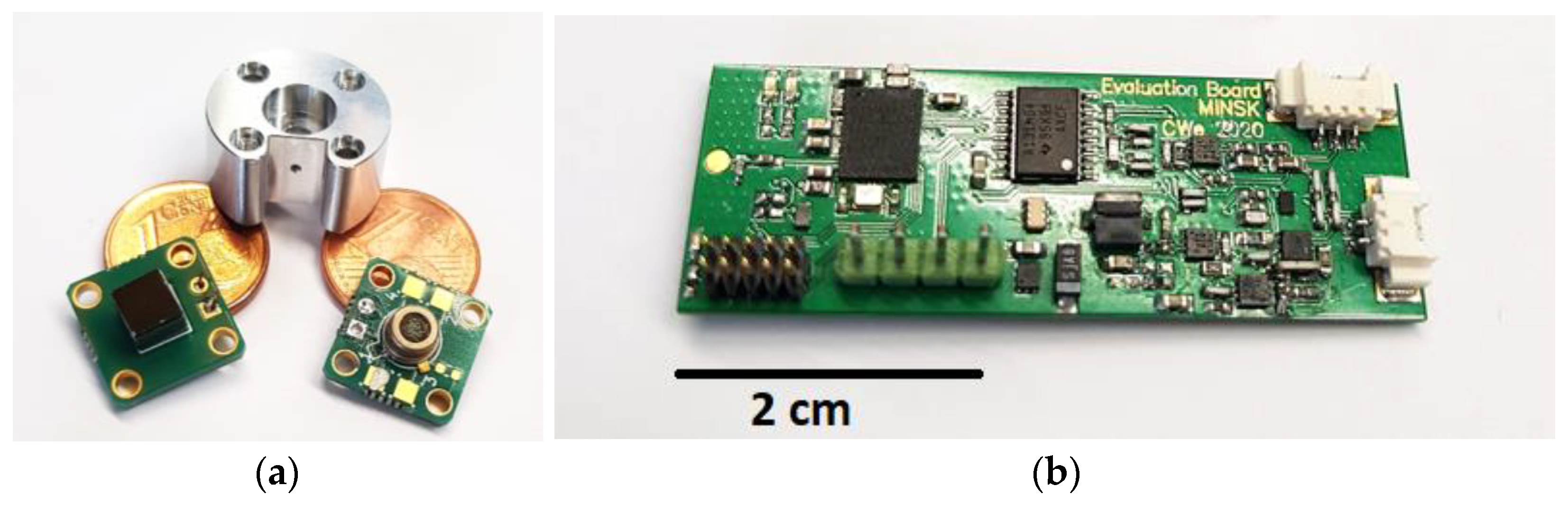
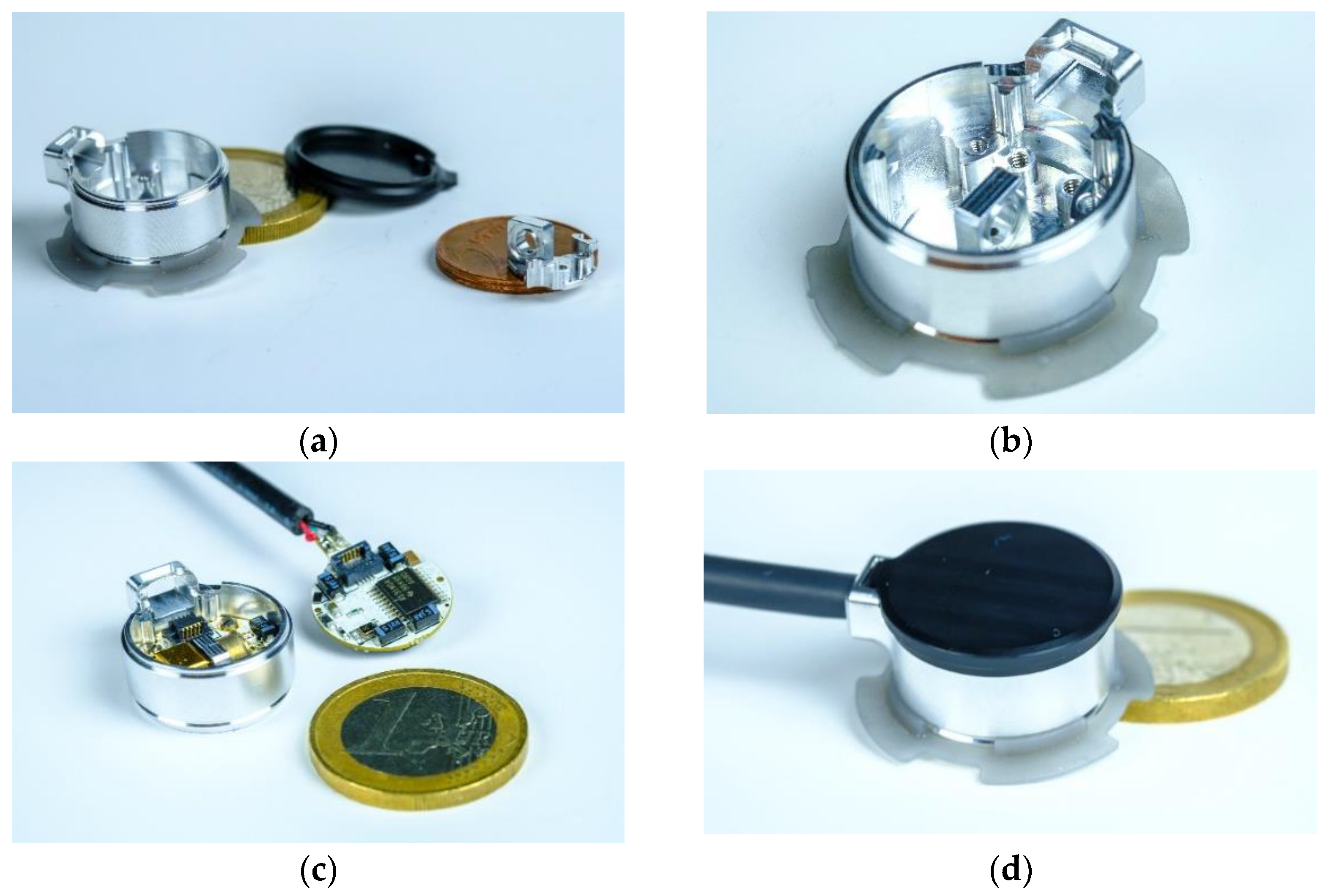
3.2. Miniaturized Transcutaneous CO2 Sensor System Realization
3.3. Methods
3.3.1. Laboratory Setup
3.3.2. Miniaturized Sensor System
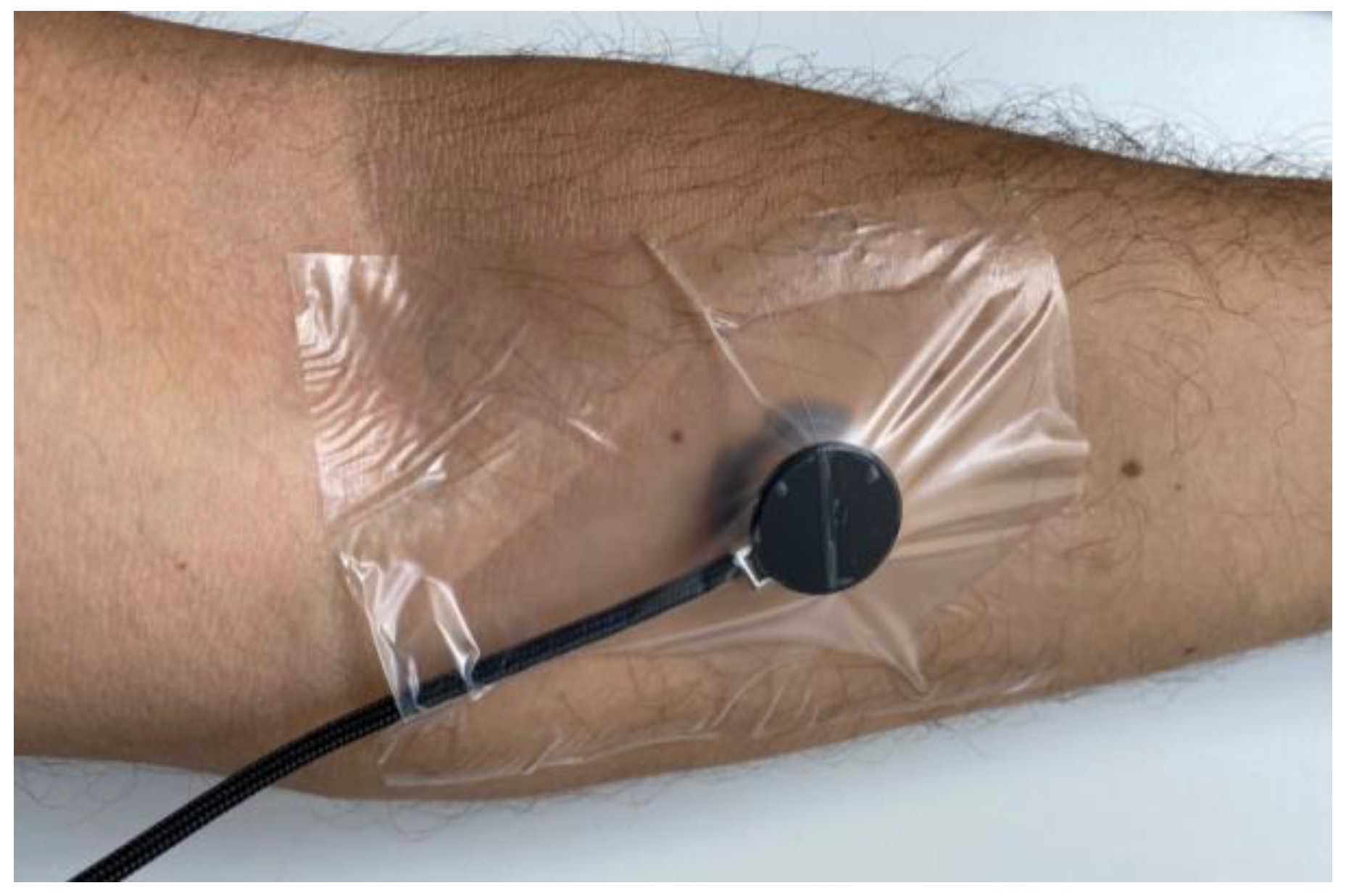
3.3.3. Transcutaneous Measurements on a Test Person
4. Results
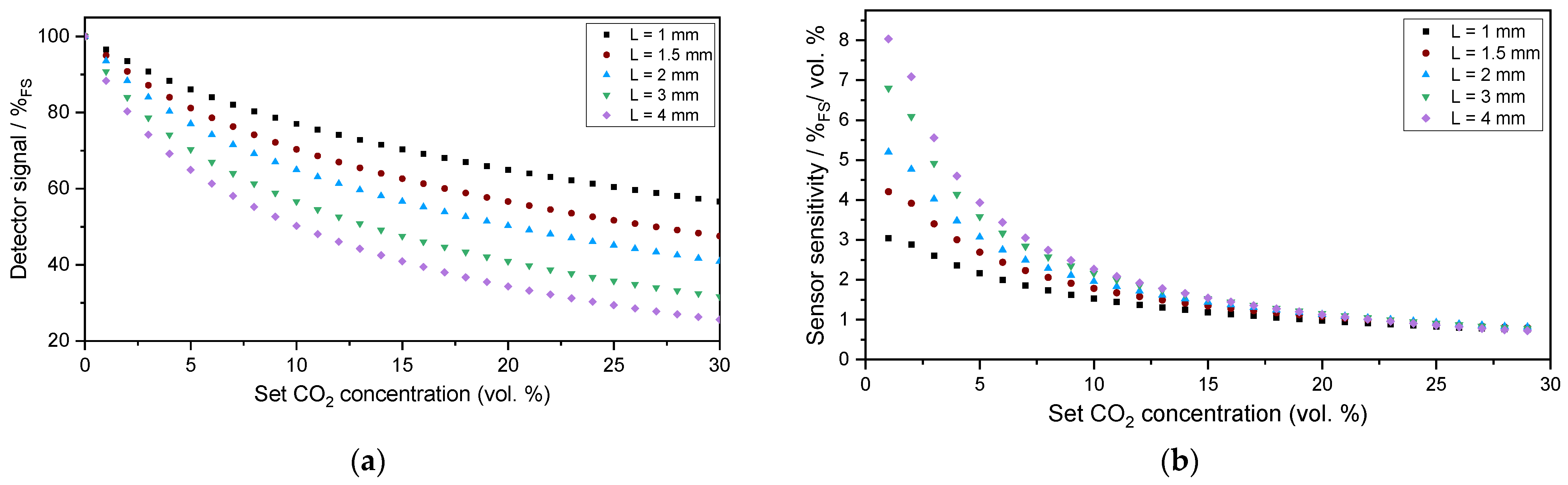
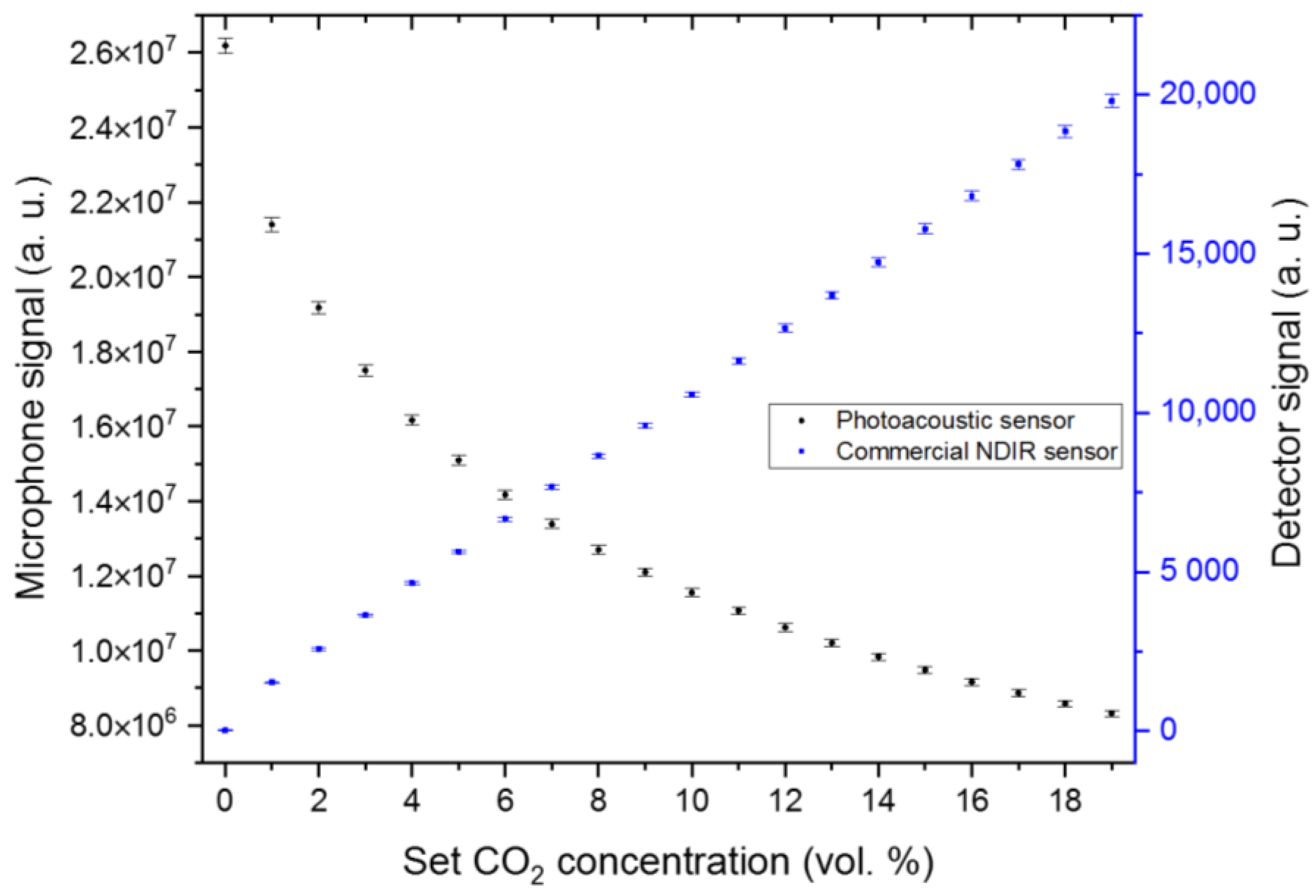
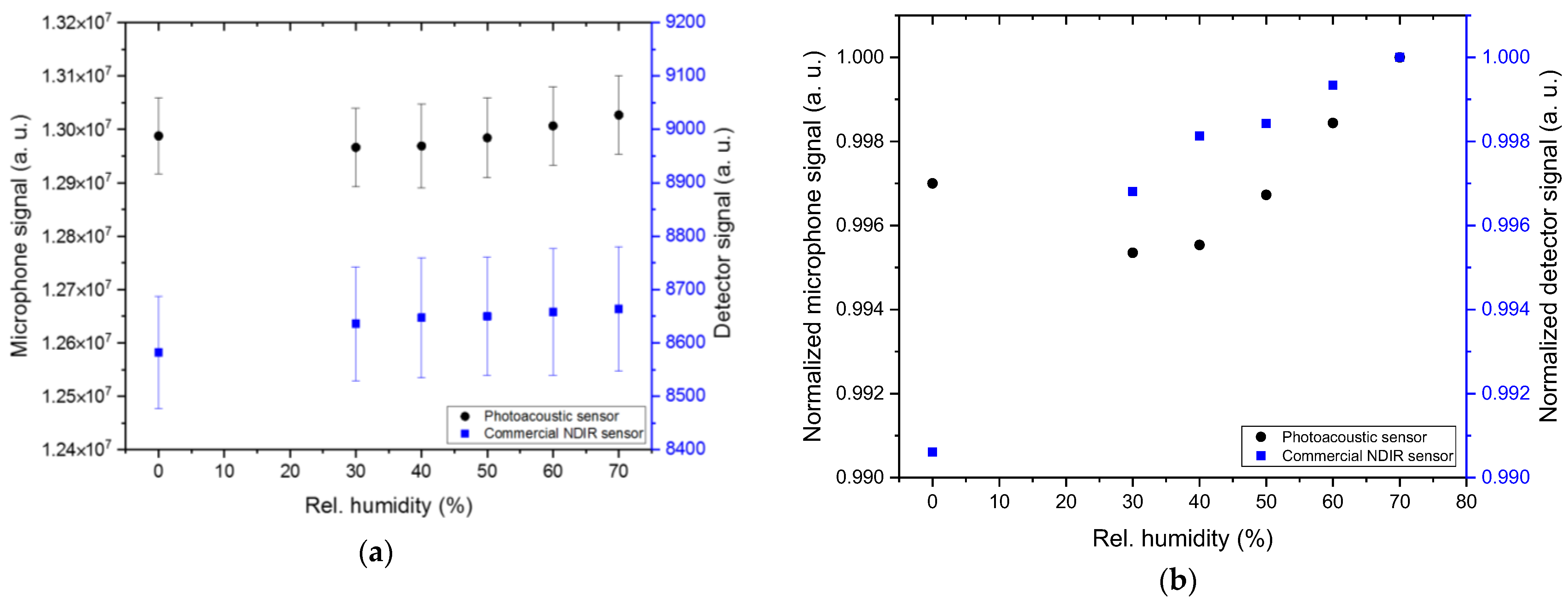
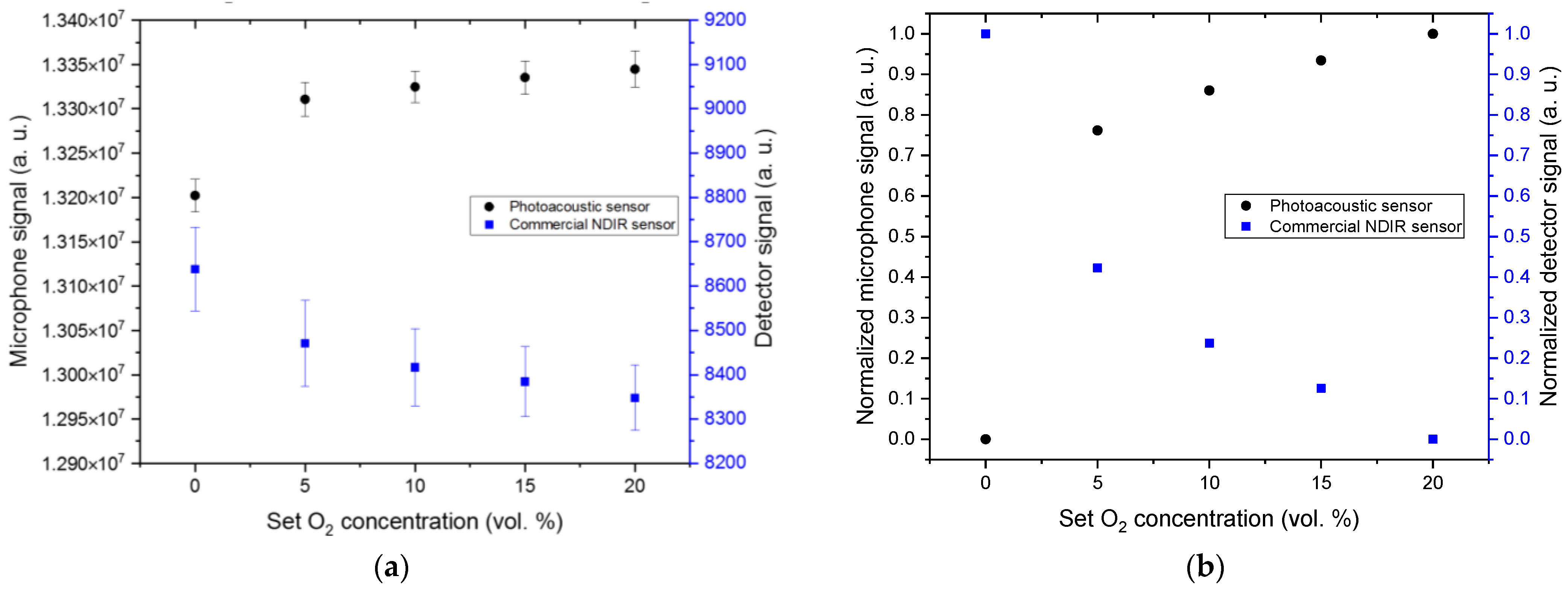
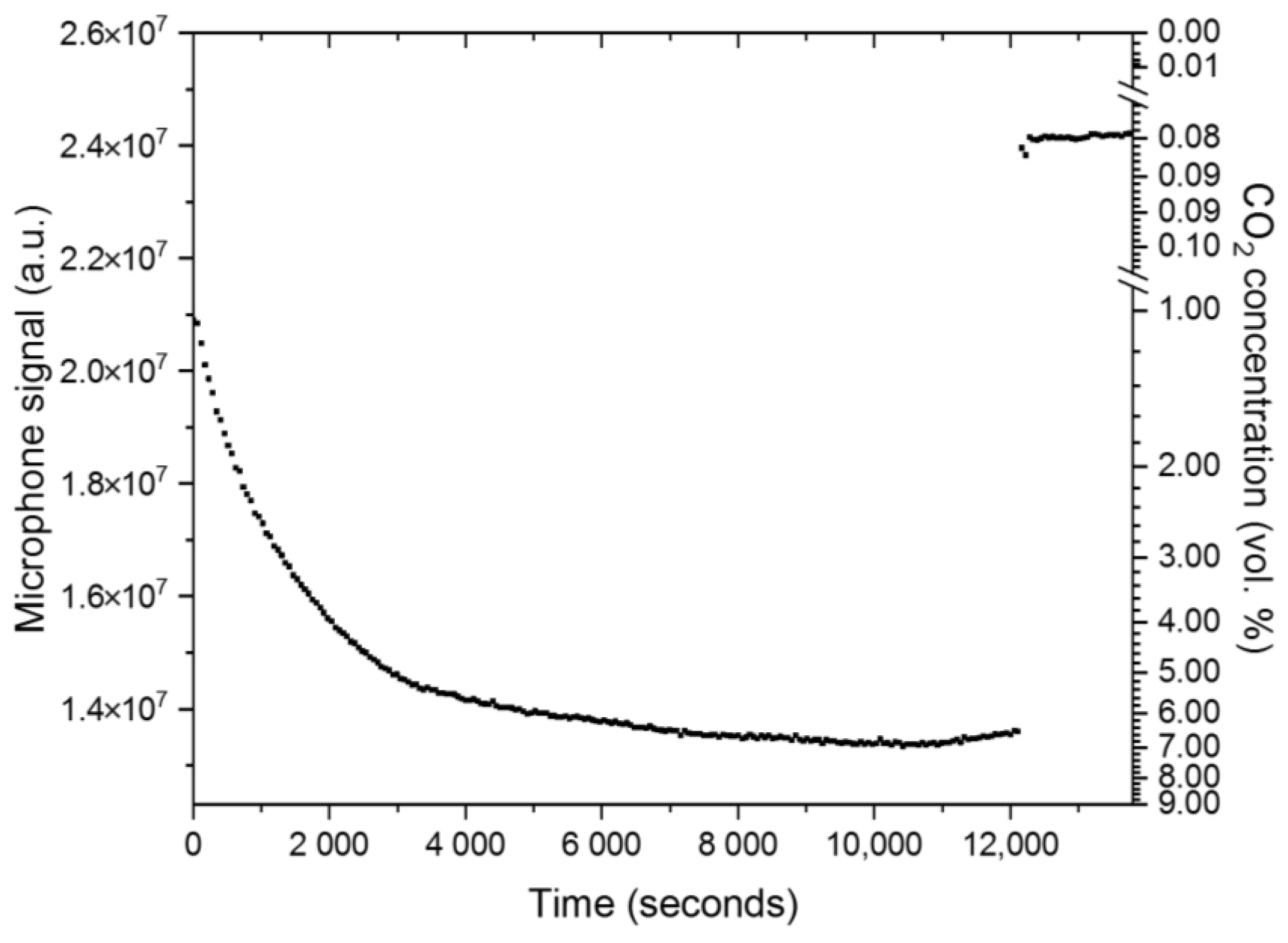
4.1. Laboratory Setup
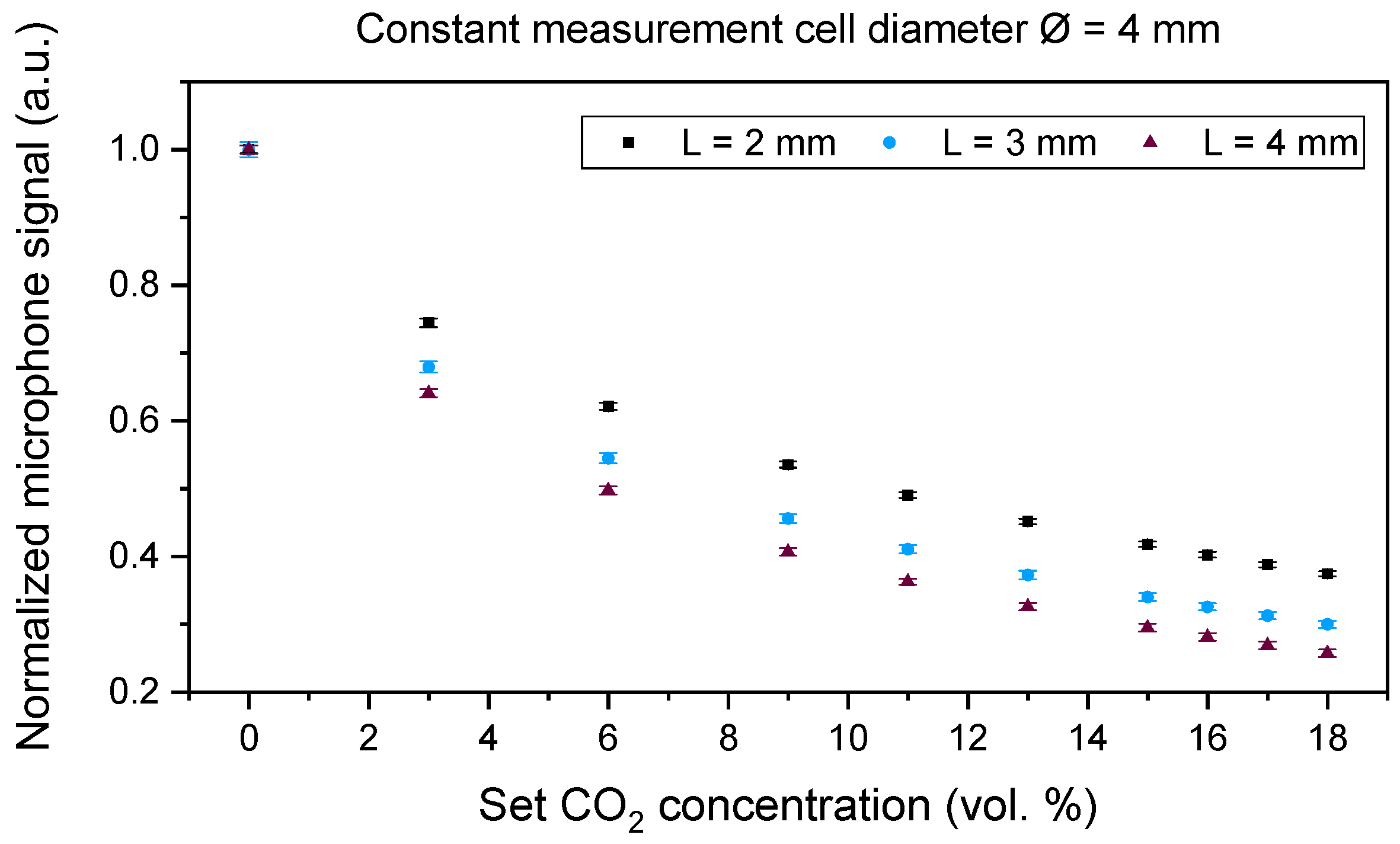
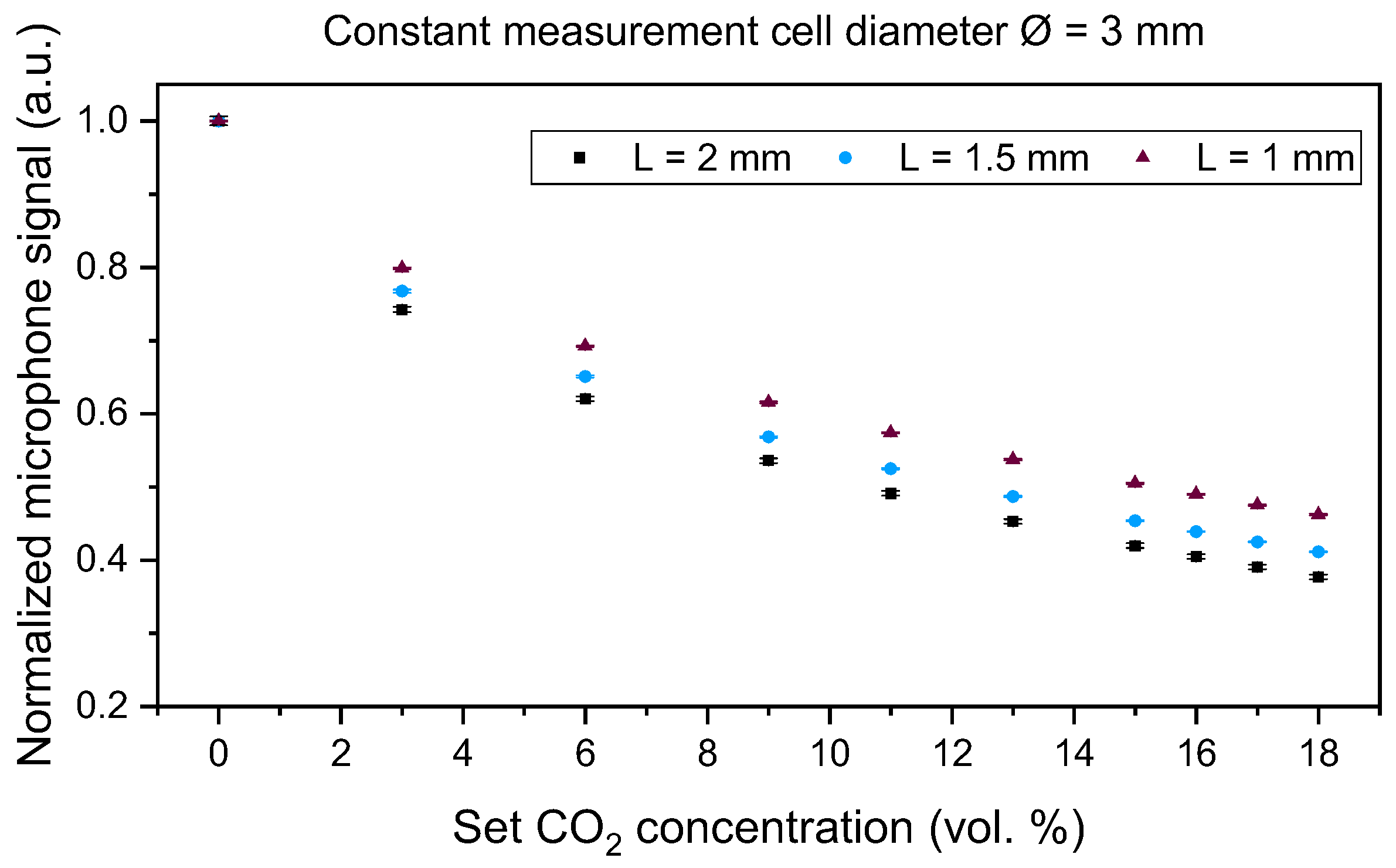
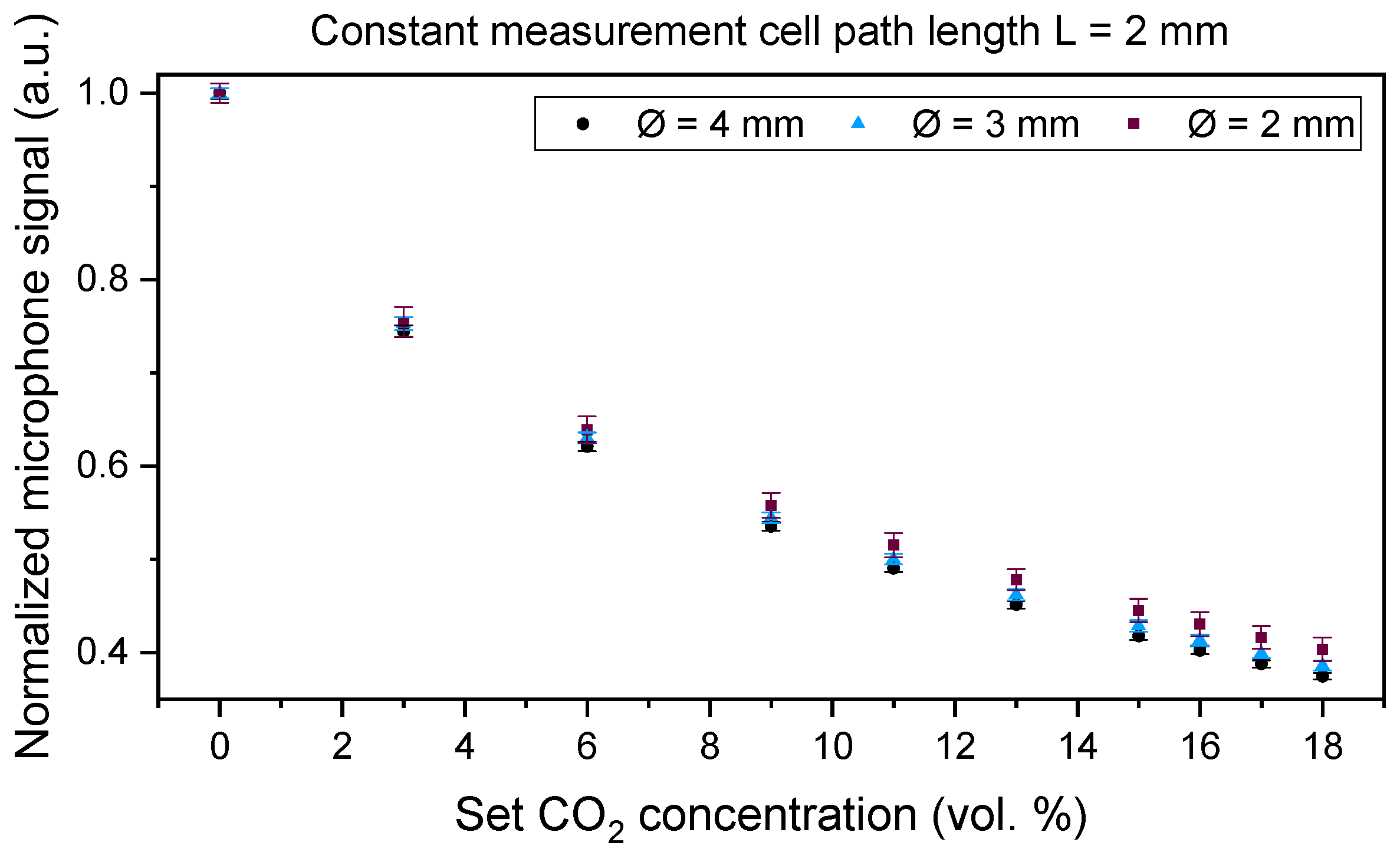
4.2. Miniaturized Sensor System
4.3. Transcutaneous Measurement on a Test Person
5. Discussion
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jonkman, A.H.; de Vries, H.J.; Heunks, L.M.A. Physiology of the Respiratory Drive in ICU Patients: Implications for Diagnosis and Treatment. Crit. Care 2020, 24, 104. [Google Scholar] [CrossRef] [PubMed]
- Mairbäurl, H.; Weber, R.E. Oxygen transport by hemoglobin. Compr. Physiol. 2012, 2, 1463–1489. [Google Scholar]
- Harvey, J.W. The Erythrocyte: Physiology, Metabolism, and Biochemical Disorders. In Clinical Biochemistry of Domestic Animals, 6th ed.; Kaneko, J., Harvey, J., Bruss, M., Eds.; Academic Press (Imprint of Elsevier): Cambridge, MA, USA, 2008; pp. 173–240. [Google Scholar]
- Feher, J. Oxygen and Carbon Dioxide Transport. In Quantitative Human Physiology: An Introduction, 1st ed.; Feher, J., Ed.; Academic Press (Imprint of Elsevier): Cambridge, MA, USA, 2017; pp. 586–594. [Google Scholar]
- Bromley, I. Transcutaneous monitoring–understanding the principles. Infant 2008, 4, 95–98. [Google Scholar]
- Nassar, B.S.; Schmidt, G.A. Estimating Arterial Partial Pressure of Carbon Dioxide in Ventilated Patients: How Valid Are Surrogate Measures? Ann. Am. Thorac. Soc. 2017, 14, 1005–1014. [Google Scholar] [CrossRef] [PubMed]
- Baermann, A.; Grey, K.; Hein, U.; Schwabbauer, N.; Ullrich, L.; Vonier, R.; Wilpsbäumer, S. Atmung, Atemtherapie, Beatmung. In Intensivpflege und Anästhesie, 3rd ed.; Ullreich, L., Stolecki, D., Eds.; Georg Thieme Verlag: Stuttgart, Germany, 2015; pp. 156–170. [Google Scholar]
- Heath, D.A.; Burri, P.H.; Weibel, E.R.; Klocke, R.A.; Elliott, D.H.; Cherniack, N.S.; Siebens, A.A.; Beers, M.F.; Human respiratory system. Encycl. Brit. 2023. Available online: https://www.britannica.com/science/human-respiratory-system (accessed on 5 January 2023).
- Prause, G.; Hetz, H.; Lauda, P.; Pojer, H.; Smolle-Juettner, F.; Smolle, J. A comparison of the end-tidal-CO2 documented by capnometry and the arterial pCO2 in emergency patients. Resuscitation 1997, 35, 145–148. [Google Scholar] [CrossRef]
- Von Rueden, K.T. Noninvasive assessment of gas exchange in the critically ill patient. AACN Clin. Issues Crit. Care Nurs. 1990, 1, 239–247. [Google Scholar] [CrossRef]
- Wahba, R.W.M.; Tessler, M.J. Misleading end-tidal CO2 tensions. Can. J. Anaesth. 1996, 43, 862–866. [Google Scholar] [CrossRef]
- Hoffman, R.A.; Krieger, B.P.; Kramer, M.R.; Segel, S.; Bizousky, F.; Gazeroglu, H.; Sackner, M.A. End-tidal carbon dioxide in critically ill patients during changes in mechanical ventilation. Am. Rev. Respir. Dis. 2012, 140, 1265–1268. [Google Scholar] [CrossRef]
- Yosefy, C.; Hay, E.; Nasri, Y.; Magen, E.; Reisin, L. End tidal carbon dioxide as a predictor of the arterial PCO2 in the emergency department setting. Emerg. Med. J. 2004, 21, 557–559. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, R. Smoking, age and the arterial-end-tidal PCO2 difference during anaesthesia and controlled ventilation. Acta Anaesthesiol. Scand. 1987, 31, 355–356. [Google Scholar] [CrossRef]
- Eberhard, P. The design, use, and results of transcutaneous carbon dioxide analysis: Current and future directions. Anesth. Anal. 2007, 105, S48–S52. [Google Scholar] [CrossRef] [PubMed]
- Zhan, C.; Xu, K.; Liu, K.; Xu, J.; Zhen, Z. Metal oxide resistive sensors for carbon dioxide detection. Coord. Chem. Rev. 2022, 472, 214758. [Google Scholar] [CrossRef]
- Cascales, J.P.; Li, X.; Roussakis, E.; Evans, C.L. A Patient-Ready Wearable Transcutaneous CO2 Sensor. Biosensors 2022, 12, 333. [Google Scholar] [CrossRef] [PubMed]
- Bozóki, Z.; Pogány, A.; Szabó, G. Photoacoustic instruments for practical applications: Present, potentials, and future challenges. Appl. Spectrosc. 2011, 46, 1–37. [Google Scholar] [CrossRef]
- Swart, H.C.; Motaung, D.E. LED-based gas sensors: A review. Curr. Opin. Environ. Sci. Technol. 2023, 36, 100506. [Google Scholar] [CrossRef]
- Swinehart, D.F. The Beer-Lambert Law. J. Chem. Educ. 1962, 39, 333. [Google Scholar] [CrossRef]
- Dinh, T.-V.; Choi, I.-Y.; Son, Y.-S.; Kim, J.-C. A review on non-dispersive infrared gas sensors: Improvement of sensor detection limit and interference correction. Sens. Actuators B 2016, 231, 529–538. [Google Scholar] [CrossRef]
- Sun, Y.W.; Liu, C.; Chan, K.L.; Xie, P.H.; Liu, W.Q.; Zeng, Y.; Wang, S.M.; Huang, S.H.; Chen, J.; Wang, Y.P. Stack emission monitoring using non-dispersive infrared spectroscopy with an optimized nonlinear absorption cross interference correction algorithm. Atmos. Meas. Technol. 2013, 6, 1993–2005. [Google Scholar] [CrossRef]
- Barritault, P.; Brun, M.; Gidon, S.; Nicoletti, S. Mid-IR source based on a free-standing microhotplate for autonomous CO2 sensing in indoor applications. Sens. Actuators A 2011, 172, 379–385. [Google Scholar] [CrossRef]
- Tezcan, D.S.; Eminoglu, S.; Akin, T. A low-cost uncooled infrared microbolometer detector in standard CMOS technology. IEEE Trans. Electron Devices 2003, 50, 494–502. [Google Scholar] [CrossRef]
- Gibson, D.; MacGregor, C. A novel solid state non-dispersive infrared CO2 gas sensor compatible with wireless and portable deployment. Sensors 2013, 13, 7079–7103. [Google Scholar] [CrossRef] [PubMed]
- Kimmig, L. Method and Device for Measuring the Concentration of a Detector Gas in a Measuring Gas Containing an Interfering Gas. U.S. Patent 5,563,330, 8 October 1996. [Google Scholar]
- Luft, K.F. Über eine neue Methode der registrierenden Gasanalyse mit Hilfe der Absorption ultraroter Strahlen ohne spektrale Zerlegung. Z. Tech. Phys 1943, 24, 97–104. [Google Scholar]
- Jia, X.; Roels, J.; Baets, R.; Roelkens, G. A Miniaturised, Fully Integrated NDIR CO2 Sensor On-Chip. Sensors 2021, 21, 5347. [Google Scholar] [CrossRef] [PubMed]
- Scholz, L.; Ortiz Perez, A.; Bierer, B.; Eaksen, P.; Wöllenstein, J.; Palzer, S. Miniature Low-Cost Carbon Dioxide Sensor for Mobile Devices. IEEE Sens. J. 2017, 17, 2889–2895. [Google Scholar] [CrossRef]
- Rouxel, J.; Coutard, J.-G.; Gidon, S.; Lartigue, O.; Nicoletti, S.; Parvitte, B.; Vallon, R.; Zéninari, V.; Glière, A. Development of a miniaturized differential photoacoustic gas sensor. Proc. Eng. 2015, 120, 396–399. [Google Scholar] [CrossRef]
- Ortiz Perez, A.; Bierer, B.; Scholz, L.; Wöllenstein, J.; Palzer, S. A Wireless Gas Sensor Network to Monitor Indoor Environmental Quality in Schools. Sensors 2018, 18, 4345. [Google Scholar] [CrossRef]
- Principles of Lock-in Detection. Available online: https://www.zhinst.com/europe/en/resources/principles-of-lock-in-detection (accessed on 8 January 2024).
- El-Safoury, M.; Dufner, M.; Weber, C.; Schmitt, K.; Pernau, H.-F.; Willing, B.; Wöllenstein, J. On-Board Monitoring of SO2 Ship Emissions Using Resonant Photoacoustic Gas Detection in the UV Range. Sensors 2021, 21, 4468. [Google Scholar] [CrossRef] [PubMed]
- Gordon, I.E.; Rothman, L.S.; Hill, C.; Kochanov, R.V.; Tan, Y.; Bernath, P.F.; Birk, M.; Boudon, V.; Campargue, A.; Chance, K.V.; et al. The HITRAN2016 molecular spectroscopic database. J. Quant. Spectrosc. Radiat. Transf. 2017, 203, 3–69. [Google Scholar] [CrossRef]
- Riecke, B.; Neuhaus, P.; Stockmann, M. Major Influence of Oxygen Supply on 13CO2: 12CO2 Ratio Measurement by Nondispersive Isotope-Selective Infrared Spectroscopy. Helicobacter 2005, 10, 620–622. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Length L | Ø = 2.0 mm | Ø = 2.5 mm | Ø = 3.0 mm | Ø = 4.0 mm |
|---|---|---|---|---|
| 1.0 mm | X | |||
| 1.5 mm | X | |||
| 2.0 mm | X | X | X | X |
| 3.0 mm | X | |||
| 4.0 mm | X |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
El-Safoury, M.; Weber, C.; Yassine, H.; Wöllenstein, J.; Schmitt, K. Towards a Miniaturized Photoacoustic Sensor for Transcutaneous CO2 Monitoring. Sensors 2024, 24, 457. https://doi.org/10.3390/s24020457
El-Safoury M, Weber C, Yassine H, Wöllenstein J, Schmitt K. Towards a Miniaturized Photoacoustic Sensor for Transcutaneous CO2 Monitoring. Sensors. 2024; 24(2):457. https://doi.org/10.3390/s24020457
Chicago/Turabian StyleEl-Safoury, Mahmoud, Christian Weber, Hassan Yassine, Jürgen Wöllenstein, and Katrin Schmitt. 2024. "Towards a Miniaturized Photoacoustic Sensor for Transcutaneous CO2 Monitoring" Sensors 24, no. 2: 457. https://doi.org/10.3390/s24020457