
Relationship between the Central and Regional Pulse Wave Velocity in the Assessment of Arterial Stiffness Depending on Gender in the Geriatric Population
 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Pulse Wave Velocity
1.2. Regional Pulse Wave Velocity
1.3. Cardiovascular Risk Factors
2. Materials and Methods
2.1. Design and Participants
2.2. Exclusion Criteria
2.3. Consent of the Bioethics Committee
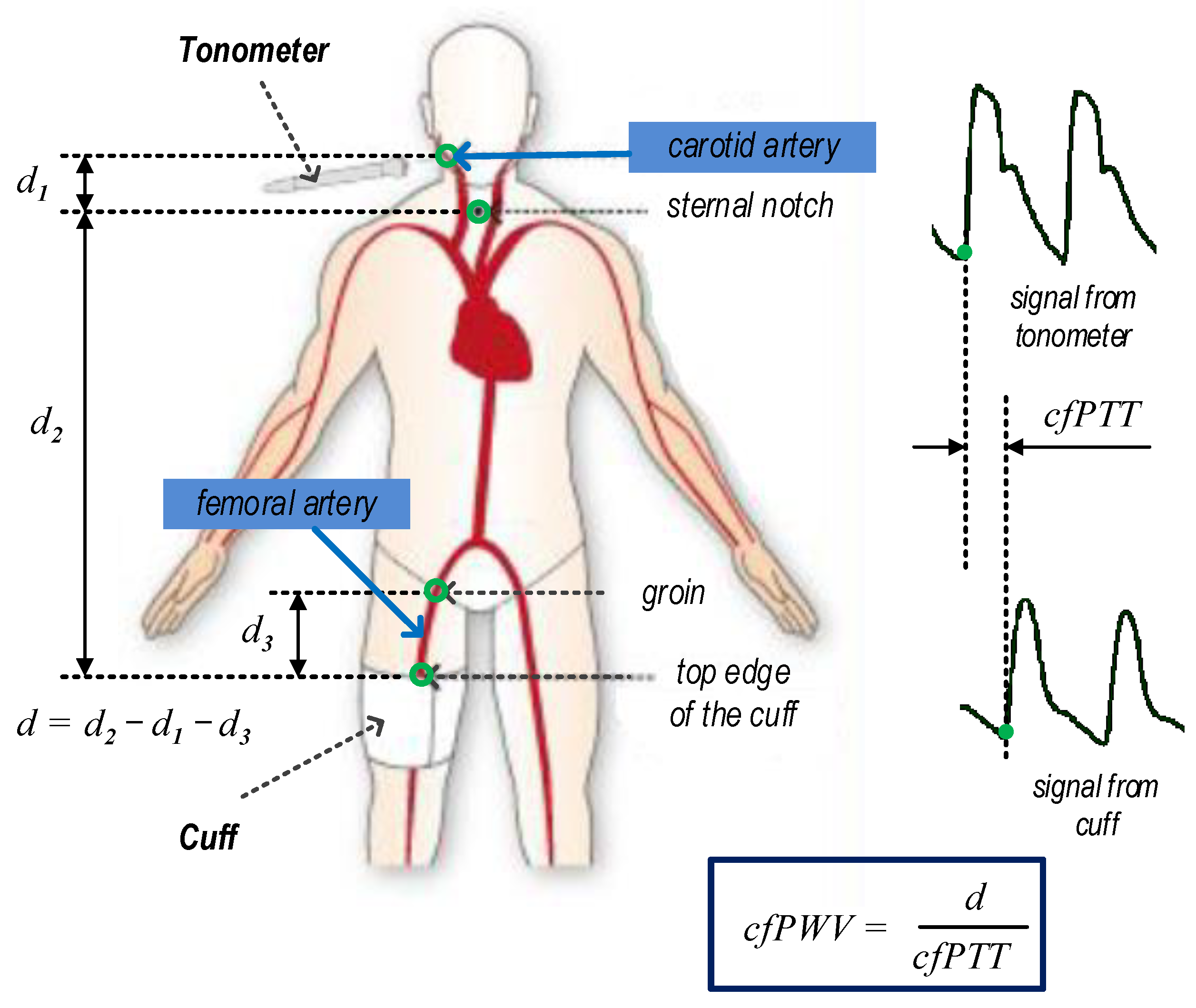
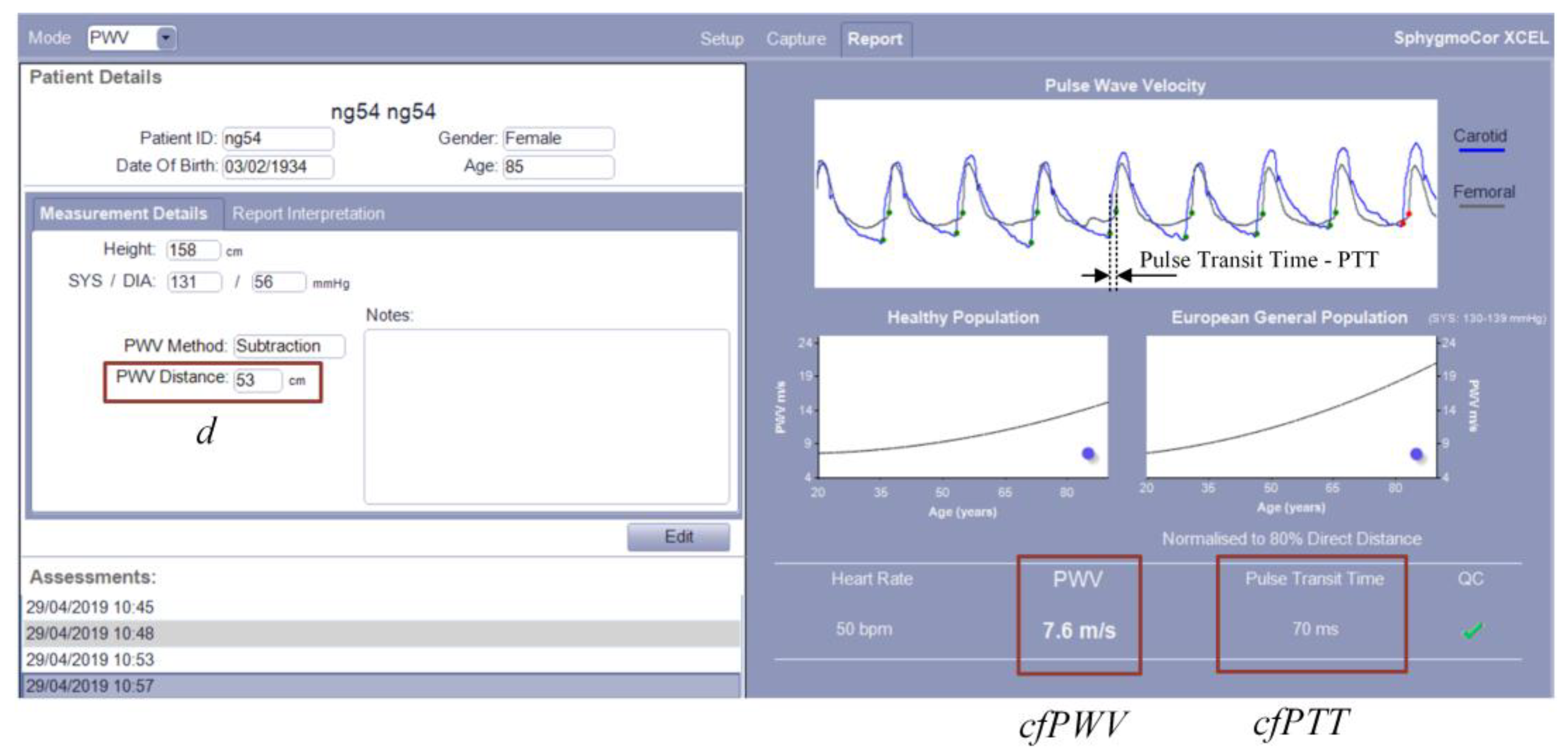
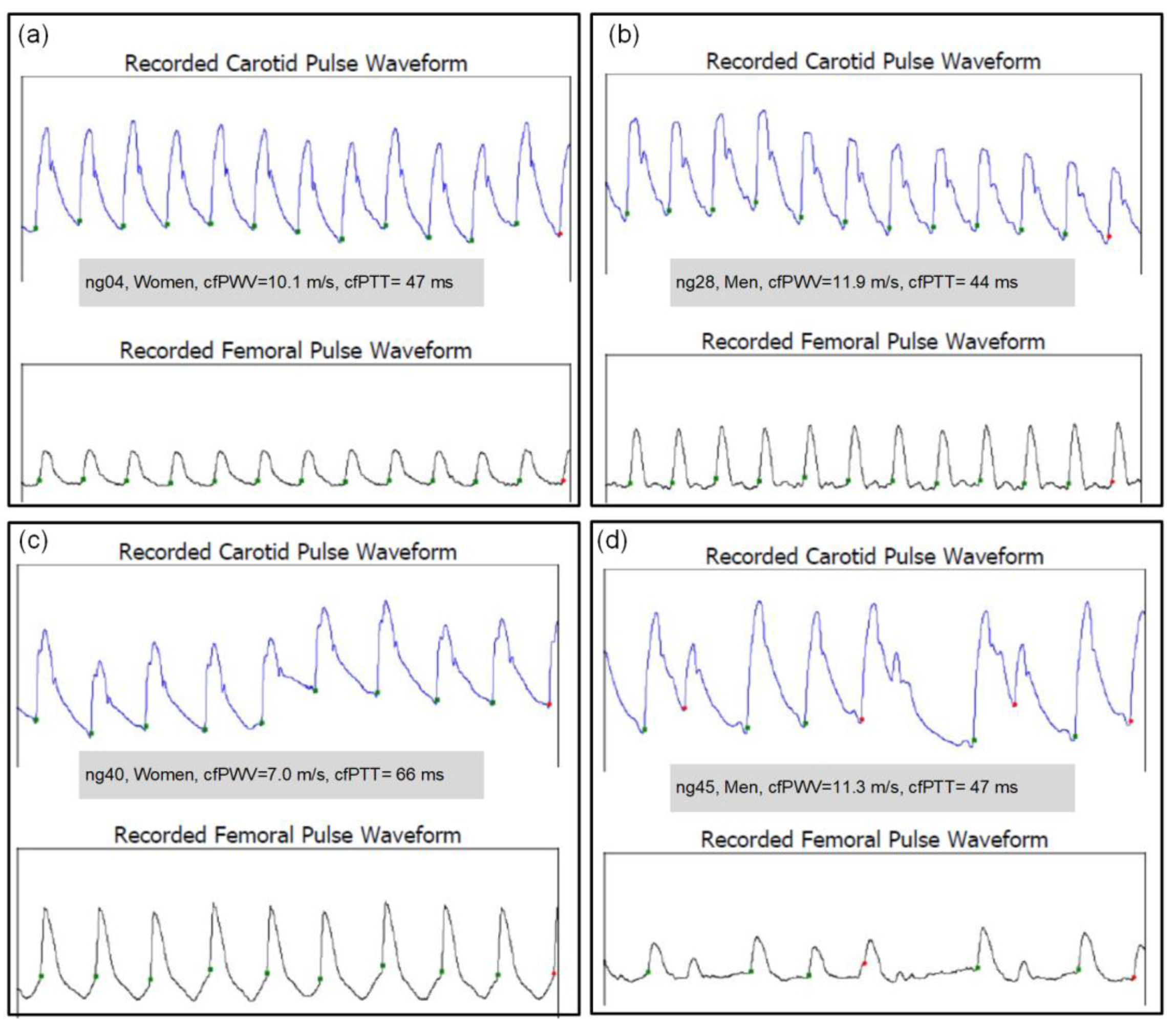
2.4. Measurement of cfPWV
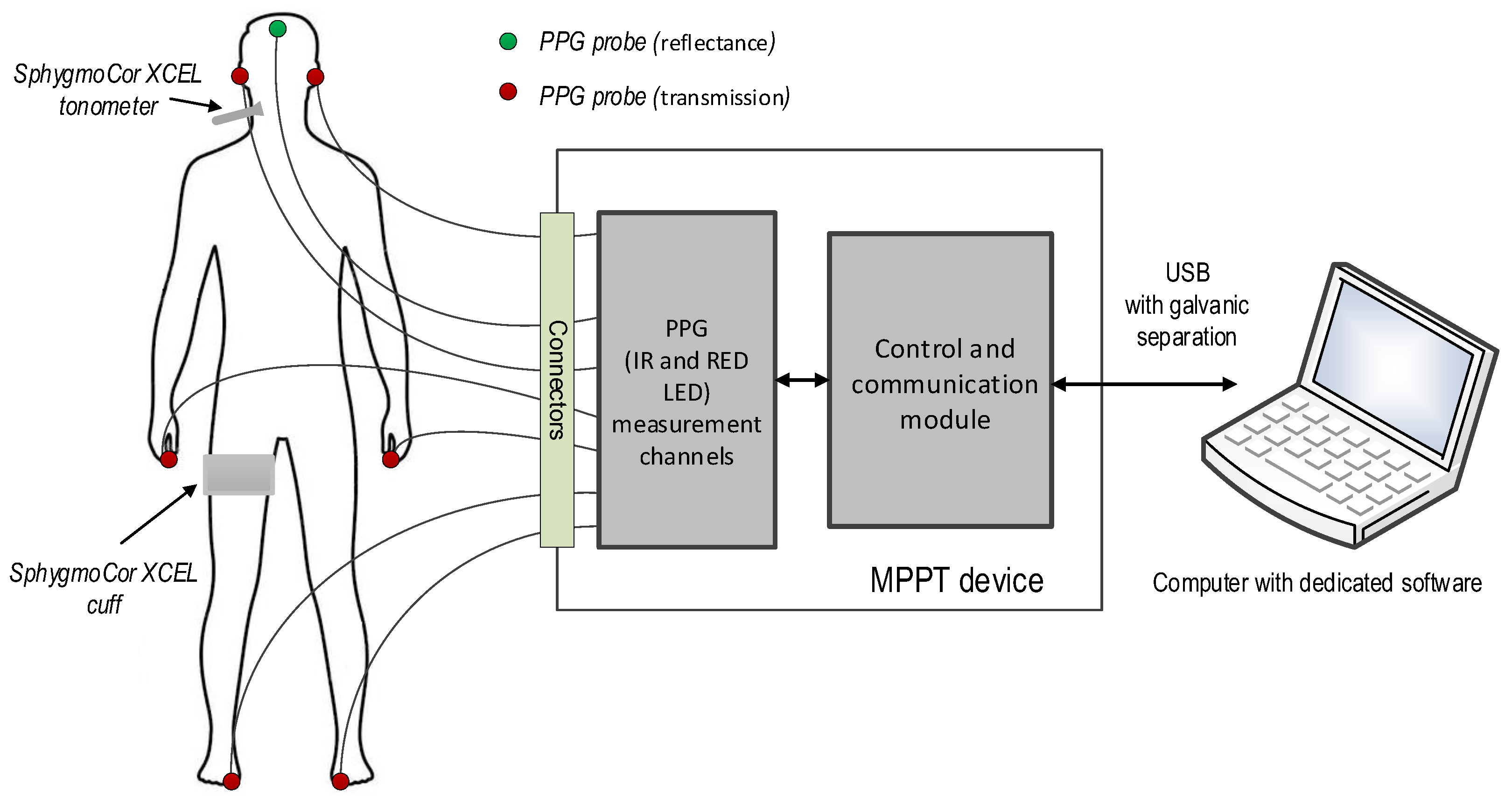
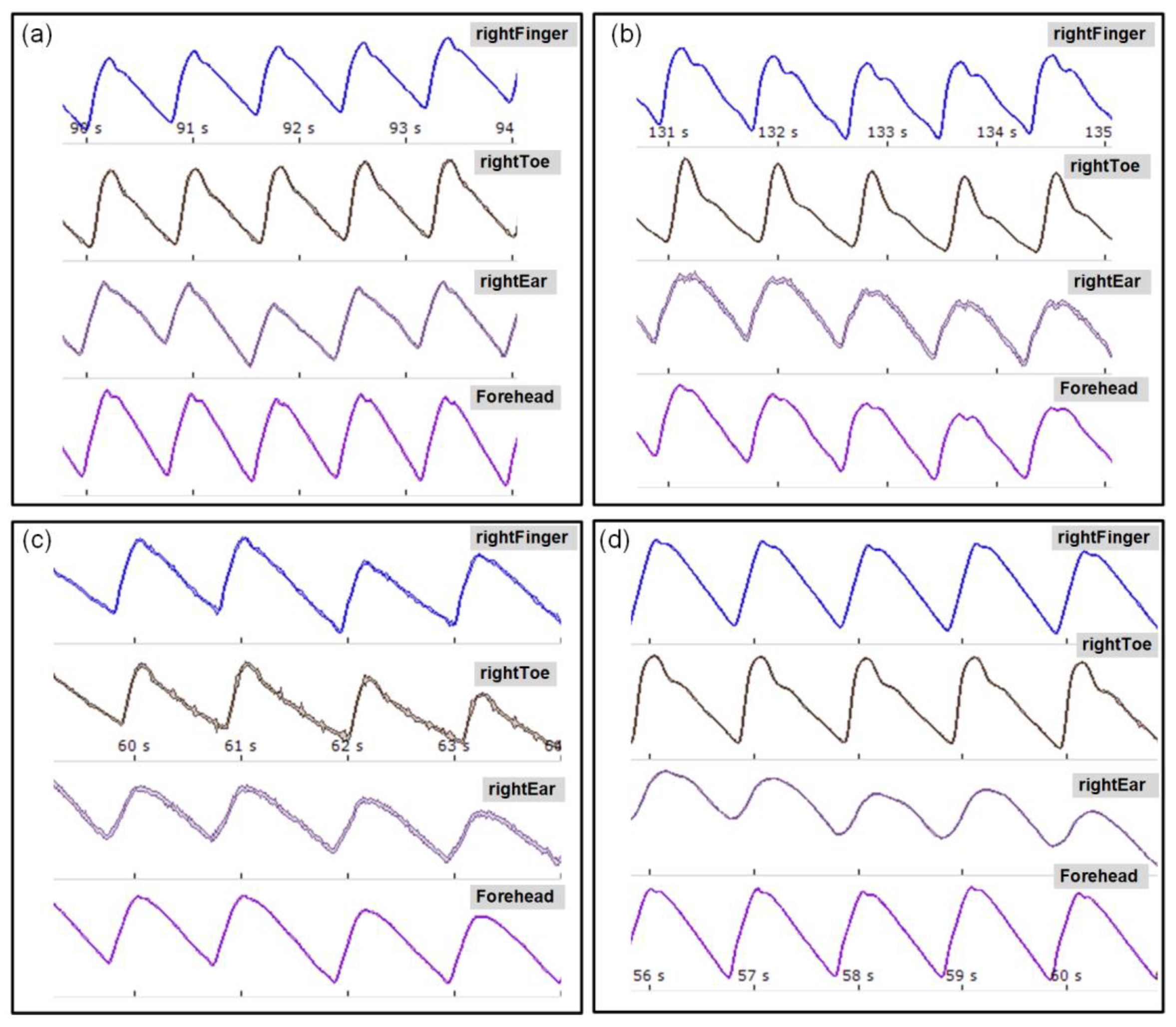
2.5. Measurement of Multi-Site PWV
2.6. Measurement Protocol
2.7. Analysis
3. Results
3.1. Characteristics of the Study Group
3.2. Gender Differences in the Analysis of the Impact of cfPWV on Selected Atherosclerosis Risk Factors and Comorbidities
3.3. Multivariable Regression—Comorbidities and Gender
3.4. Analysis of Multi-Site Regional PWV by Gender
3.5. Comparison of Central and Regional PWV
4. Discussion
4.1. Results
4.2. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2016 Mortality Collaborators. Global, regional, and national under-5 mortality, adult mortality, age-specific mortality, and life expectancy, 1970–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1084–1150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benjamin, E.J.; Virani, S.S.; Callaway, C.W.; Chamberlain, A.M.; Chang, A.R.; Cheng, S.; Chiuve, S.E.; Cushman, M.; Delling, F.N.; Deo, R.; et al. Heart Disease and Stroke Statistics-2018 Update: A Report From the American Heart Association. Circulation 2018, 137, e67–e492. [Google Scholar] [CrossRef] [PubMed]
- Piepoli, M.F.; Hoes, A.W.; Agewall, S.; Albus, C.; Brotons, C.; Catapano, A.L.; Cooney, M.-T.; Corrà, U.; Cosyns, B.; Deaton, C.; et al. 2016 European Guidelines on cardiovascular disease prevention in clinical practice: The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of 10 societies and by invited experts) Developed with the special contribution of the European Association for Cardiovascular Prevention & Rehabilitation (EACPR). Eur. Heart J. 2016, 37, 2315–2381. [Google Scholar] [CrossRef] [PubMed]
- Lusis, A.J. Atherosclerosis. Nature 2000, 407, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.Y.; Oh, B.H. Aging and arterial stiffness. Circ. J. 2010, 74, 2257–2262. [Google Scholar] [CrossRef] [Green Version]
- Kubalski, P.; Manitius, J. Sztywność tętnic, ciśnienie centralne, współczynnik wzmocnienia—Kompendium nie tylko dla hipertensjologa. Chor. Serca Naczyń 2008, 5, 61–67. (In Polish) [Google Scholar]
- Van Bortel, L.M.; Laurent, S.; Boutouyrie, P.; Chowienczyk, P.; Cruickshank, J.; De Backer, T.; Filipovsky, J.; Huybrechts, S.; Mattace-Raso, F.U.; Protogerou, A.D.; et al. Expert consensus document on the measurement of aortic stiffness in daily practice using carotid-femoral pulse wave velocity. J. Hypertens. 2012, 30, 445–448. [Google Scholar] [CrossRef] [Green Version]
- Williams, B.; Mancia, G.; Spiering, W.; Agabiti Rosei, E.; Azizi, M.; Burnier, M.; Clement, D.L.; Coca, A.; de Simone, G.; Dominiczak, A.; et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur. Heart J. 2018, 39, 3021–3104. [Google Scholar] [CrossRef] [Green Version]
- Jannasz, I.; Sondej, T.; Targowski, T.; Dobrowolski, A.; Olszewski, R. Pomiar prędkości fali tętna—Użyteczne narzędzie w ocenie sztywności tętnic [Pulse wave velocity—A useful tool in assessing the stiffness of the arteries]. Pol. Merkur. Lek. 2019, 46, 257–262. [Google Scholar]
- Kim, H.L.; Kim, S.H. Pulse Wave Velocity in Atherosclerosis. Front. Cardiovasc. Med. 2019, 6, 41. [Google Scholar] [CrossRef]
- Segers, P.; Rietzschel, E.R.; Chirinos, J.A. How to Measure Arterial Stiffness in Humans. Arterioscler. Thromb. Vasc. Biol. 2020, 40, 1034–1043. [Google Scholar] [CrossRef] [Green Version]
- Nabeel, P.M.; Kiran, V.R.; Joseph, J.; Abhidev, V.V.; Sivaprakasam, M. Local Pulse Wave Velocity: Theory, Methods, Advancements, and Clinical Applications. IEEE Rev. Biomed. Eng. 2020, 13, 74–112. [Google Scholar] [CrossRef]
- OECD. Life Expectancy at Birth (Indicator). 2020. Available online: https://www.oecd-ilibrary.org/social-issues-migration-health/life-expectancy-at-birth/indicator/english_27e0fc9d-en (accessed on 8 May 2020).
- Rodgers, J.L.; Jones, J.; Bolleddu, S.I.; Vanthenapalli, S.; Rodgers, L.E.; Shah, K.; Karia, K.; Panguluri, S.K. Cardiovascular Risks Associated with Gender and Aging. J. Cardiovasc. Dev. Dis. 2019, 6, 19. [Google Scholar] [CrossRef] [Green Version]
- Conde-Sala, J.L.; Garre-Olmo, J.; Calvó-Perxas, L.; Turró-Garriga, O.; Vilalta-Franch, J.; López-Pousa, S. CAUSES, mortality rates and risk factors of death in community-dwelling Europeans aged 50 years and over: Results from the Survey of Health, Ageing and Retirement in Europe 2013–2015. Arch. Gerontol. Geriatr. 2020, 89, 104035. [Google Scholar] [CrossRef]
- Ogola, B.O.; Zimmerman, M.A.; Clark, G.L.; Abshire, C.M.; Gentry, K.M.; Miller, K.S.; Lindsey, S.H. New insights into arterial stiffening: Does sex matter? Am. J. Physiol. Heart Circ. Physiol. 2018, 315, H1073–H1087. [Google Scholar] [CrossRef] [Green Version]
- Available online: https://atcormedical.com/technology/sphygmocor/ (accessed on 22 May 2020).
- Wilkinson, I.B.; McEniery, C.M.; Schillaci, G.; Boutouyrie, P.; Segers, P.; Donald, A.; Chowienczyk, P.J. ARTERY Society guidelines for validation of non-invasive haemodynamic measurement devices: Part 1, arterial pulse wave velocity. Artery Res. 2010, 4, 34–40. [Google Scholar] [CrossRef]
- Rajzer, M.W.; Wojciechowska, W.; Klocek, M.; Palka, I.; Brzozowska-Kiszka, M.; Kawecka-Jaszcz, K. Comparison of aortic pulse wave velocity measured by three techniques: Complior, SphygmoCor and Arteriograph. J. Hypertens. 2008, 26, 2001–2007. [Google Scholar] [CrossRef]
- Butlin, M.; Qasem, A. Large Artery Stiffness Assessment Using SphygmoCor Technology. Pulse 2017, 4, 180–192. [Google Scholar] [CrossRef] [Green Version]
- Sondej, T.; Sieczkowski, K.; Olszewski, R.; Dobrowolski, A. Simultaneous multi-site measurement system for the assessment of pulse wave delays. Biocybern. Biomed. Eng. 2019, 39, 488–502. [Google Scholar] [CrossRef]
- Sondej, T.; Jannasz, I.; Sieczkowski, K.; Dobrowolski, A.; Obiała, K.; Targowski, T.; Olszewski, R. Validation of a new device for photoplethysmographic measurement of multi-site arterial pulse wave velocity. Biocybern. Biomed. Eng. 2021, 41, 1664–1684. [Google Scholar] [CrossRef]
- Mozos, I.; Maidana, J.P.; Stoian, D.; Stehlik, M. Gender Differences of Arterial Stiffness and Arterial Age in Smokers. Int. J. Environ. Res. Public Health 2017, 14, 565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lan, Y.; Liu, H.; Liu, J.; Zhao, H.; Wang, H. Gender Difference of the Relationship between Arterial Stiffness and Blood Pressure Variability in Participants in Prehypertension. Int. J. Hypertens. 2019, 2019, 7457385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zemtsovskaja, G.; Abina, J.; Meigas, K.; Pilt, K.; Viigimaa, M. Pulse wave velocity and its gender-related associations with cardiovascular risk factors in a high cardiovascular risk population. Arch. Med. Sci. Atheroscler. Dis. 2018, 3, e99–e105. [Google Scholar] [CrossRef] [PubMed]
- Łoboz-Rudnicka, M.; Jaroch, J.; Kruszyńska, E.; Bociąga, Z.; Rzyczkowska, B.; Dudek, K.; Szuba, A.; Łoboz-Grudzień, K. Gender-related differences in the progression of carotid stiffness with age and in the influence of risk factors on carotid stiffness. Clin. Interv. Aging 2018, 13, 1183–1191. [Google Scholar] [CrossRef] [Green Version]
- Mil, S.R.; Biter, L.U.; Geijn, G.J.M.; Birnie, E.; Dunkelgrun, M.; Ijzermans, J.N.M.; Meulen, N.; Mannaerts, G.H.H.; Cabezas, M.C. The effect of sex and menopause on carotid intima-media thickness and pulse wave velocity in morbid obesity. Eur. J. Clin. Investig. 2019, 49, e13118. [Google Scholar] [CrossRef]
- Hayward, C.S.; Kelly, R.P.; Collins, P. The roles of gender, the menopause and hormone replacement on cardiovascular function. Cardiovasc. Res. 2000, 46, 28–49. [Google Scholar] [CrossRef] [Green Version]
- Moreau, K.L. Modulatory influence of sex hormones on vascular aging. Am. J. Physiol. Heart Circ. Physiol. 2019, 316, H522–H526. [Google Scholar] [CrossRef]
- Pawlik, A.; Januszek, R.; Ruzsa, Z.; Óriás, V.; Kleczyński, P.; Wojtasik-Bakalarz, J.; Arif, S.; Nyerges, A.; Chyrchel, M.; Stanek, A.; et al. Gender differences and long-term clinical outcomes in patients with chronic total occlusions of infrainguinal lower limb arteries treated from retrograde access with peripheral vascular interventions. Adv. Med. Sci. 2020, 65, 197–201. [Google Scholar] [CrossRef]
- Meaume, S.; Benetos, A.; Henry, O.; Rudnichi, A.; Safar, M. Aortic pulse wave velocity predicts cardiovascular mortality in subjects >70 years of age. Arterioscler. Thromb. Vasc. Biol. 2001, 21, 2046–2050. [Google Scholar] [CrossRef]
- Campos-Staffico, A.M.; Freitas, W.M.; Carvalho, L.S.F.; Coelho-Filho, O.; Nadruz, W.; de Oliveira, R.B.; Sposito, A.C. Lower bone mass is associated with subclinical atherosclerosis, endothelial dysfunction and carotid thickness in the very elderly. Atherosclerosis 2020, 292, 70–74. [Google Scholar] [CrossRef] [Green Version]
- Sawabe, M.; Takahashi, R.; Matsushita, S.; Ozawa, T.; Arai, T.; Hamamatsu, A.; Nakahara, K.-I.; Chida, K.; Yamanouchi, H.; Murayama, S.; et al. Aortic pulse wave velocity and the degree of atherosclerosis in the elderly: A pathological study based on 304 autopsy cases. Atherosclerosis 2005, 179, 345–351. [Google Scholar] [CrossRef]
- Heffernan, K.S.; Stoner, L.; London, A.S.; Augustine, J.A.; Lefferts, W.K. Estimated pulse wave velocity as a measure of vascular aging. PLoS ONE 2023, 18, e0280896. [Google Scholar] [CrossRef]
- Almarshad, M.A.; Islam, M.S.; Al-Ahmadi, S.; BaHammam, A.S. Diagnostic Features and Potential Applications of PPG Signal in Healthcare: A Systematic Review. Healthcare 2022, 10, 547. [Google Scholar] [CrossRef]
- Zieff, G.; Stone, K.; Paterson, C.; Fryer, S.; Diana, J.; Blackwell, J.; Meyer, M.L.; Stoner, L. Pulse-wave velocity assessments derived from a simple photoplethysmography device: Agreement with a referent device. Front. Cardiovasc. Med. 2023, 10, 1108219. [Google Scholar] [CrossRef]
- Soukup, L.; Jurak, P.; Halamek, J.; Viscor, I.; Matejkova, M.; Leinveber, P.; Vondra, V. Arterial Aging Best Reflected in Pulse Wave Velocity Measured from Neck to Lower Limbs: A Whole-Body Multichannel Bioimpedance Study. Sensors 2022, 22, 1910. [Google Scholar] [CrossRef]
- Cho, J.; Baek, H.J. A Comparative Study of Brachial-Ankle Pulse Wave Velocity and Heart-Finger Pulse Wave Velocity in Korean Adults. Sensors 2020, 20, 2073. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Women (n = 83) | Men (n = 35) | p-Value | |
|---|---|---|---|
| cfPWV (m/s) | 9.36 (8.28–10.63) | 10.52 (9.18–11.65) | 0.001 |
| Age (years) | 77 (72–83) | 76 (69–86) | 0.810 |
| TC (mg/dL) | 199 (165–226) | 167 (135–224) | 0.051 |
| HDL-C (mg/dL) | 63 (54–72) | 51 (39–61) | <0.001 |
| LDL-C (mg/dL) | 107.8 (84.0–138.2) | 98.4 (64.2–145.0) | 0.208 |
| TG (mg/dL) | 111 (82–150) | 107 (87–170) | 0.874 |
| FPG (mg/dL) | 95 (87–109) | 95 (88–107) | 0.751 |
| NTproBNP (pg/mL) | 225.4 (128.6–410.0) | 322.1 (213.0–1183.0) | 0.047 |
| eGFR (mL/min) | 62.53 (47.53–80.77) | 83.04 (47.57–86.14) | 0.819 |
| Uric acid (mg/dL) | 5.0 (4.4–5.8) | 6.0 (5.3–6.7) | <0.001 |
| CRP (mg/L) | 6 (5–11) | 5 (5–7) | 0.047 |
| ESR (mm/h) | 17 (11–27) | 13 (5–22) | 0.050 |
| TSH (mlU/L) | 1.50 (0.94–2.35) | 1.27 (0.68–1.87) | 0.292 |
| BMI (kg/m2) | 29.38 ± 5.13 | 27.31 ± 4.67 | 0.053 |
| Ac (cm) | 28 (26–31) | 27 (26–30) | 0.976 |
| LLc (cm) | 35 (33–38) | 34 (31–37) | 0.135 |
| bSBP | 136.54 ± 17.97 | 134.26 ± 19.23 | 0.538 |
| bDBP | 69.12 ± 9.92 | 70.49 ± 10.47 | 0.503 |
| bMAP | 91.58 ± 10.79 | 91.8 ± 12.44 | 0.923 |
| aSBP | 124.19 ± 15.99 | 121.09 ± 16.75 | 0.346 |
| aDBP | 70.22 ± 10.05 | 71.76 ± 10.25 | 0.451 |
| aPP | 51.6 (43.5–63.8) | 48.7 (42.1–55.7) | 0.075 |
| aMAP | 90.87 ± 10.82 | 89.55 ± 12.3 | 0.563 |
| aHR | 67.38 ± 9.57 | 64.61 ± 8.4 | 0.141 |
| Hypertension | 70 (84%) | 33 (94%) | 0.238 |
| Diabetes mellitus | 22 (27%) | 13 (37%) | 0.248 |
| MS | 33 (40%) | 15 (43%) | 0.754 |
| COPD | 8 (10%) | 4 (11%) | 0.968 |
| HF | 58 (77%) | 26 (84%) | 0.623 |
| VES 13 | 5.29 ± 2.78 | 5.169 ± 3.53 | 0.739 |
| ADL | 5.539 ± 0.71 | 5.429 ± 1.06 | 0.957 |
| I ADL | 21.499 ± 3.56 | 19.529 ± 5.45 | 0.100 |
| MMSE | 26.619 ± 2.81 | 25.469 ± 5.19 | 0.935 |
| CDT | 8.669 ± 2.00 | 8.889 ± 2.29 | 0.244 |
| Parameter | Total | Men (n = 35) | Women (n = 85) | |||
|---|---|---|---|---|---|---|
| r | p-Value | r | p-Value | r | p-Value | |
| Age | 0.341 | <0.001 | 0.194 | 0.265 | 0.430 | <0.001 |
| HDL-C | −0.196 | 0.033 | −0.132 | 0.448 | −0.076 | 0.493 |
| LDL-C | −0.042 | 0.653 | 0.012 | 0.944 | −0.008 | 0.946 |
| TC | −0.090 | 0.332 | 0.118 | 0.500 | −0.095 | 0.393 |
| TG | 0.160 | 0.083 | 0.466 | 0.005 | 0.056 | 0.618 |
| FPG | 0.108 | 0.247 | 0.413 | 0.014 | 0.080 | 0.472 |
| NTproBNP | 0.347 | <0.001 | 0.296 | 0.106 | 0.329 | 0.004 |
| Uric acid | 0.339 | <0.001 | 0.108 | 0.536 | 0.335 | 0.002 |
| CRP | 0.147 | 0.113 | 0.018 | 0.919 | 0.242 | 0.028 |
| ESR | 0.128 | 0.171 | 0.262 | 0.128 | 0.166 | 0.135 |
| TSH | 0.088 | 0.344 | 0.053 | 0.764 | 0.150 | 0.177 |
| eGFR | −0.212 | 0.021 | −0.051 | 0.771 | −0.300 | 0.006 |
| BMI | 0.097 | 0.309 | 0.352 | 0.052 | 0.113 | 0.318 |
| Ac | 0.035 | 0.713 | 0.192 | 0.301 | 0.023 | 0.839 |
| LLc | −0.013 | 0.890 | 0.070 | 0.707 | 0.032 | 0.775 |
| bSBP | 0.443 | <0.001 | 0.466 | 0.005 | 0.500 | <0.001 |
| bDBP | 0.229 | 0.013 | 0.196 | 0.259 | 0.232 | 0.035 |
| bMAP | 0.374 | <0.001 | 0.347 | 0.041 | 0.413 | <0.001 |
| aSBP | 0.411 | <0.001 | 0.450 | 0.007 | 0.471 | <0.001 |
| aDBP | 0.255 | 0.005 | 0.223 | 0.197 | 0.255 | 0.020 |
| aPP | 0.311 | <0.001 | 0.488 | 0.003 | 0.357 | 0.001 |
| aMAP | 0.353 | <0.001 | 0.351 | 0.039 | 0.409 | <0.001 |
| AorticHR | 0.009 | 0.922 | −0.044 | 0.801 | 0.089 | 0.425 |
| TOTAL GROUP Variable | Unstandardized Coefficients | Standardized Coefficients | p-Value | ||
|---|---|---|---|---|---|
| β | SE | β | SE | ||
| Age | 0.053 | 0.017 | 0.250 | 0.081 | 0.003 |
| NTproBNP | 0.000 | 0.000 | 0.119 | 0.085 | 0.165 |
| Uric Acid | 0.201 | 0.093 | 0.172 | 0.080 | 0.034 |
| bSBP | 0.037 | 0.007 | 0.398 | 0.077 | <0.001 |
| gender (male) | 0.464 | 0.151 | 0.251 | 0.081 | 0.003 |
| WOMEN GROUP variable | Unstandardized coefficients | Standardized coefficients | p-value | ||
| β | SE | β | SE | ||
| Age | 0.059 | 0.021 | 0.276 | 0.098 | 0.006 |
| NTproBNP | 0.000 | 0.000 | 0.208 | 0.096 | 0.034 |
| Uric Acid | 0.273 | 0.104 | 0.240 | 0.091 | 0.010 |
| bSBP | 0.033 | 0.009 | 0.355 | 0.093 | <0.001 |
| MEN GROUP variable | Unstandardized coefficients | Standardized coefficients | p-value | ||
| β | SE | β | SE | ||
| TG | 0.007 | 0.004 | 0.332 | 0.173 | 0.064 |
| FPG | 0.008 | 0.010 | 0.138 | 0.175 | 0.435 |
| bSBP | 0.031 | 0.011 | 0.394 | 0.143 | 0.010 |
| Parameters | Unstandardized Coefficients | Standardized Coefficients | p-Value | ||
|---|---|---|---|---|---|
| β | SE | β | SE | ||
| Hypertension | 0.542 | 0.244 | 0.196 | 0.089 | 0.029 |
| Diabetes Mellitus | 0.508 | 0.162 | 0.279 | 0.089 | 0.002 |
| COPD | 0.048 | 0.238 | 0.017 | 0.086 | 0.842 |
| Heart failure | 0.288 | 0.180 | 0.139 | 0.087 | 0.113 |
| Gender | 0.465 | 0.160 | 0.251 | 0.086 | 0.005 |
| Measured Site-Dependent PWV (Regional PWV) | Women Mean [Min–Max] | Men Mean [Min–Max] | p Value |
|---|---|---|---|
| forehead–right toe, htPWV | 9.40 [6.70–14.10] | 9.34 [6.10–13.00] | 0.660 |
| forehead–left toe, htPWV | 9.51 [6.10–14.10] | 9.63 [6.80–14.00] | 0.858 |
| right ear–right toe, etPWV | 9.41 [7.00–13.50] | 9.64 [6.70–13.90] | 0.951 |
| left ear–left toe, etPWV | 9.25 [6.10–13.70] | 9.79 [7.00–13.30] | 0.180 |
| right finger–right toe, ftPWV | 10.01 [6.10–15.30] | 9.43 [6.10–14.40] | 0.336 |
| left finger–left toe, ftPWV | 9.49 [6.20–13.60] | 9.20 [6.50–14.40] | 0.286 |
| TOTAL GROUP Variable | Central PWV (cfPWV) Mean [Min–Max] | Regional PWV Mean [Min–Max] | Mean Difference | p-Value |
|---|---|---|---|---|
| forehead–right toe, htPWV | 9.86 [6.32–14.14] | 9.38 [6.10–14.10] | 0.48 | 0.028 |
| forehead–left toe, htPWV | 9.55 [6.10–14.10] | 0.25 | 0.060 | |
| right ear–right toe, etPWV | 9.48 [6.70–13.90] | 0.44 | 0.015 | |
| left ear–left toe, etPWV | 9.41 [6.10–13.70] | 0.42 | 0.021 | |
| right finger–right toe, ftPWV | 9.85 [6.10–15.30] | 0.03 | 0.409 | |
| left finger–left toe, ftPWV | 9.40 [6.20–14.40] | 0.55 | 0.038 | |
| WOMEN GROUP variable | central PWV (cfPWV) | regional PWV | mean difference | p-value |
| forehead–right toe, htPWV | 9.36 [6.32–13.02] | 9.40 [6.70–14.10] | 0.07 | 0.046 |
| forehead–left toe, htPWV | 9.51 [6.10–14.10] | 0.12 | 0.166 | |
| right ear–right toe, etPWV | 9.41 [7.00–13.50] | 0.17 | 0.534 | |
| left ear–left toe, etPWV | 9.25 [6.10–13.70] | 0.26 | 0.345 | |
| right finger–right toe, ftPWV | 10.01 [6.10–15.30] | 0.46 | 0.181 | |
| left finger–left toe, ftPWV | 9.49 [6.20–13.60] | 0.12 | 0.185 | |
| MEN GROUP variable | central PWV (cfPWV) | regional PWV | mean difference | p-value |
| forehead–right toe, htPWV | 10.52 [8.12–14.14] | 9.34 [6.10–13.00] | 1.37 | 0.001 |
| forehead–left toe, htPWV | 9.63 [6.80–14.00] | 1.01 | 0.012 | |
| right ear–right toe, etPWV | 9.64 [6.70–13.90] | 1.07 | 0.005 | |
| left ear–left toe, etPWV | 9.79 [7.00–13.30] | 0.81 | 0.029 | |
| right finger–right toe, ftPWV | 9.43 [6.10–14.40] | 1.33 | 0.011 | |
| left finger–left toe, ftPWV | 9.20 [6.50–14.40] | 1.49 | 0.004 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jannasz, I.; Sondej, T.; Targowski, T.; Mańczak, M.; Obiała, K.; Dobrowolski, A.P.; Olszewski, R. Relationship between the Central and Regional Pulse Wave Velocity in the Assessment of Arterial Stiffness Depending on Gender in the Geriatric Population. Sensors 2023, 23, 5823. https://doi.org/10.3390/s23135823
Jannasz I, Sondej T, Targowski T, Mańczak M, Obiała K, Dobrowolski AP, Olszewski R. Relationship between the Central and Regional Pulse Wave Velocity in the Assessment of Arterial Stiffness Depending on Gender in the Geriatric Population. Sensors. 2023; 23(13):5823. https://doi.org/10.3390/s23135823
Chicago/Turabian StyleJannasz, Iwona, Tadeusz Sondej, Tomasz Targowski, Małgorzata Mańczak, Karolina Obiała, Andrzej Piotr Dobrowolski, and Robert Olszewski. 2023. "Relationship between the Central and Regional Pulse Wave Velocity in the Assessment of Arterial Stiffness Depending on Gender in the Geriatric Population" Sensors 23, no. 13: 5823. https://doi.org/10.3390/s23135823