1. Introduction
Joint quasi-stiffness [
1], referred to by some as joint stiffness [
2], represents the relationship between a person’s internal moment and angular change for a certain plane of a joint. This relationship not only provides a characterization of the joint mechanical properties but also represents a lower-order model approximation of the neural mechanisms of human motor control [
3]. In particular, researchers have made efforts in determining how joint quasi-stiffness during gait differs by gender [
4], age [
2,
4,
5], body dimensions [
6,
7,
8], walking speeds [
2,
5], ground surface conditions [
9], and body loads [
10,
11]. However, it should be mentioned that quasi-stiffness has been more characterized in the literature at the ankle joint [
2,
4,
5,
8,
10,
11] and knee joint [
2,
7,
9,
10] than at the hip joint [
2,
6,
10].
This basic science understanding of joint quasi-stiffness has also been applied to help make clinical decisions [
12,
13], describe dynamic joint function [
4], and advance hardware designs of wearable assistive devices [
5,
9]. With respect to the latter, recent advances in assistive devices known as exoskeletons (exos) often use this knowledge of joint quasi-stiffness to determine control methods which can cooperatively interact with the user in order to provide assistance for desired movements [
14,
15]. With that being said, achieving assistance can be challenging, as all exos introduce some changes to the wearer’s biomechanics via the influence of the device’s added mass magnitudes and body locations [
16,
17,
18,
19]. As hip exos add the device’s mass closer to the wearer’s center of body mass, there is an assumption that hip exos will have reduced influence on the wearer’s biomechanics and, therefore, hip exos have recently gained interest [
20]. However, this added mass distribution effect on human motor control, or joint quasi-stiffness, has not received enough attention to make such an assumption. In a review of the literature, if mass amounts are exceeded at specific limb locations, even for those of hip exo designs, then wearer adaptations can result in significant changes in their hip angular and moment profiles, which are related to hip joint quasi-stiffness [
17,
18,
21,
22]. Specifically, among healthy young adults, walking with as little as 10.8 lb added mass around the pelvis increased hip flexion angles during the majority of the gait cycle and hip extension moment during the first half of the gait cycle [
17,
18]. In addition, walking with a backpack or vest [
21,
23], or with weights around the pelvis and/or thighs bilaterally [
18,
19,
24], also changed other lower-limb joint angular and/or moment profiles. Thus, hip exo physical designs, and their controllers, can benefit from incorporating knowledge of such responses by the wearer with respect to quasi-stiffness at the hip joint during walking. A reasonable starting point is with understanding the actual influence of wearing added mass that is representative of hip exos and then extending this to increased walking speeds, as that is a common goal of exo assistance [
20,
25].
While all exos have the intention of providing assistance, a hip exo achieves this by altering the resultant torque at the wearer’s hip joint. Thus, depending on the design, the change in the resultant torque at the hip joint can lower or increase the stiffness felt by the hip exo wearer. Both passive and active hip exo designs can benefit from knowing the response of the wearer, specifically regarding their hip joint quasi-stiffness at different phases of the gait cycle [
26,
27,
28,
29,
30,
31,
32,
33]. For instance, passive hip exos, with components such as springs, can be designed to be lightweight and therefore are thought to minimize the added mass effect on biomechanics. However, overall they do not change the net mechanical energy at the actuated joints, but instead provide assistance by selectively storing and returning mechanical energy only at specified times of the gait cycle [
20]. Thus, mechanical tuning is critical to the success of passive hip exos. Parallel research has focused on active exos, which have the primary advantage of being able to change the net mechanical energy at the actuated joints during their wearer’s movement. These devices tend to be heavier and thus more likely to change the wearer’s biomechanics due to added mass [
20]. However, their potential for tailoring the assistance of varying profiles has made them quite versatile to tuning for assistance. With respect to developing their control algorithms, a popular one is assist-as-needed (AAN) [
15,
34,
35,
36], where the exo provides only necessary, or intermittent, assistance to the wearer in order to achieve predefined gait profiles. Thus, the wearer remains in complete control of their movement when not active and must adapt accordingly to the presence of wearing the device. Another popular algorithm is impedance control [
37], which alters the total resistance of the exo and the wearer’s joint by varying the assistance to match the desired model parameters of inertia, damping, and stiffness. For both algorithms and many others like them, estimates of what profiles the wearer would naturally impose for their movement is critical to their tuning. For example, two active hip exos [
38,
39] presented in a recent exo review paper [
25] exerted net mechanical energy only during hip flexion and/or extension phases of the gait cycle. To further tune such active control algorithms or even passive hip exo designs, knowledge of the quasi-stiffness during these phases would allow for better cooperative control. Specifically, the quasi-stiffness in the mid-to-late-stance phase, when a person exerts higher internal hip joint moments near the maximum hip extension angle, could be incorporated into the tuning parameters, and likewise the timing relationship during the pre-swing phase after that [
40].
To date, aspects of the relationships between hip joint quasi-stiffness and walking speed, body mass, and body height have all been quantified for the hip extension and flexion phases of the gait cycle [
6]. In particular, walking at an increased speed was found to increase hip joint quasi-stiffness during the early stance and swing phases [
3]. Furthermore, a positive correlation has been found between body mass and hip joint quasi-stiffness during the “resilient loading phase” around the terminal stance phase [
6]. Similarly, a more recent study emulating reduced gravity showed that hip joint quasi-stiffness increases during pre-swing hip flexion when walking at 0.8 and 1.2 m/s with reduced vertical weight support through a harness. It also confirmed that walking at a faster speed increases hip joint quasi-stiffness during the pre-swing phase [
10]. This increased joint quasi-stiffness due to greater added mass or faster walking speed has been observed at other lower-limb joints as well. With as low as 15% body mass added to the upper body of young adults during walking, quasi-stiffness at the ankle joint was found to increase during both the ankle dorsiflexion and plantarflexion phases [
11]. A similar effect was observed for older adults who increased their ankle joint quasi-stiffness during late stance when walking faster [
5]. It should be noted that age-related muscle loss may influence joint quasi-stiffness in older adults [
41].
Overall, quasi-stiffness studies have focused less on the hip than the ankle and knee, and those studies evaluating hip joint quasi-stiffness have been mostly focused on young adults [
3,
6,
10]. As middle-aged or older adults are more likely to be the target population for hip exos, it would be valuable to examine whether such age groups adopt similar hip joint quasi-stiffness relationships as young adults. One prior study compared young and middle-aged adults walking at multiple speeds and found no significant difference between the two age groups in hip/knee/ankle joint quasi-stiffness during the braking phase of stance, despite there existing differences in joint mechanical work [
2]. Other prior studies have shown that the amplitude of hip joint mechanical work during walking increased among both young [
42] and middle-aged adults under increased walking speeds [
2]. Likewise, the amplitude of hip joint mechanical work during walking increased among young adults with added mass, but the result is currently unknown for other age groups [
21,
42]. Given that exos are likely to alter walking speeds and added mass to the user, reporting on both quasi-stiffness and mechanical work across multiple age groups may help to establish whether clear relationships exist between the two or not. Such information is important as exos have the potential to assist aging adults in achieving higher mobility and thus improve their quality of life and independence [
43].
To summarize, knowledge of joint quasi-stiffness during emulated hip exo conditions can improve a person’s mobile performance. Previous studies have characterized hip joint quasi-stiffness during walking between the terminal stance phase and early swing phase [
3,
6], or across different time windows during the stance phase with reduced gravity [
10]. Some have focused on other joints [
11,
42], and some have focused on a different phase of the gait [
2]. However, to our knowledge, the hip joint quasi-stiffness response to changes in walking speeds and with added mass around the pelvis and thighs, emulating a hip exo, has not yet been characterized. To maximize the translational impact of this study, we propose to analyze the sagittal plane hip joint quasi-stiffness during the hip extension phase and the hip flexion phase for both young and middle-aged, healthy adults. To emulate hip exos with different mass amounts and mass distributions, various amounts of added mass were attached to the participants’ lower body (pelvis and both thighs). Specifically, the total added mass, 0 to ~10 kg, was representative of the mass range of most recent exos with hip joint actuation [
20,
25]. The sagittal plane hip joint mechanical work generated during the two phases was also evaluated to observe whether any relationships could be described between quasi-stiffness and the mechanical energy consumption, or generation, at the hip joint. The two phases analyzed were chosen because, during these gait timings, the magnitude of the hip joint moment is high, and the hip joint has been shown to exhibit “spring-like” properties [
3,
6,
10]. The “spring-like” properties imply that the hip joint moment–angle relation is expected to have relatively linear slopes during these stages, making for good fits of the hip joint quasi-stiffness. Equally important is that these timings are when exos have been designed to store/absorb and release/generate mechanical energy at the hip joint [
16].
Based on previous reports [
2,
3,
5,
6,
9,
10,
11,
21,
42], for this study the following hypotheses were tested during the hip extension and hip flexion phases, respectively: (1) when walking at a higher speed, healthy adults would increase their hip joint quasi-stiffness; (2) when wearing hip-exo-like added mass on the pelvis and thighs, healthy adults would increase their hip joint quasi-stiffness. Lastly, comparisons of hip joint quasi-stiffness and hip joint mechanical work between young adults and middle-aged adults were performed to provide a better understanding of how age influences the response to these factors of walking speed and added mass.
4. Discussion
4.1. Hip Joint Quasi-Stiffness
The goal of this study was to investigate the influence of the combination of increased walking speeds and added mass on hip joint quasi-stiffness among healthy adults. Based on the results of this study and prior studies [
3,
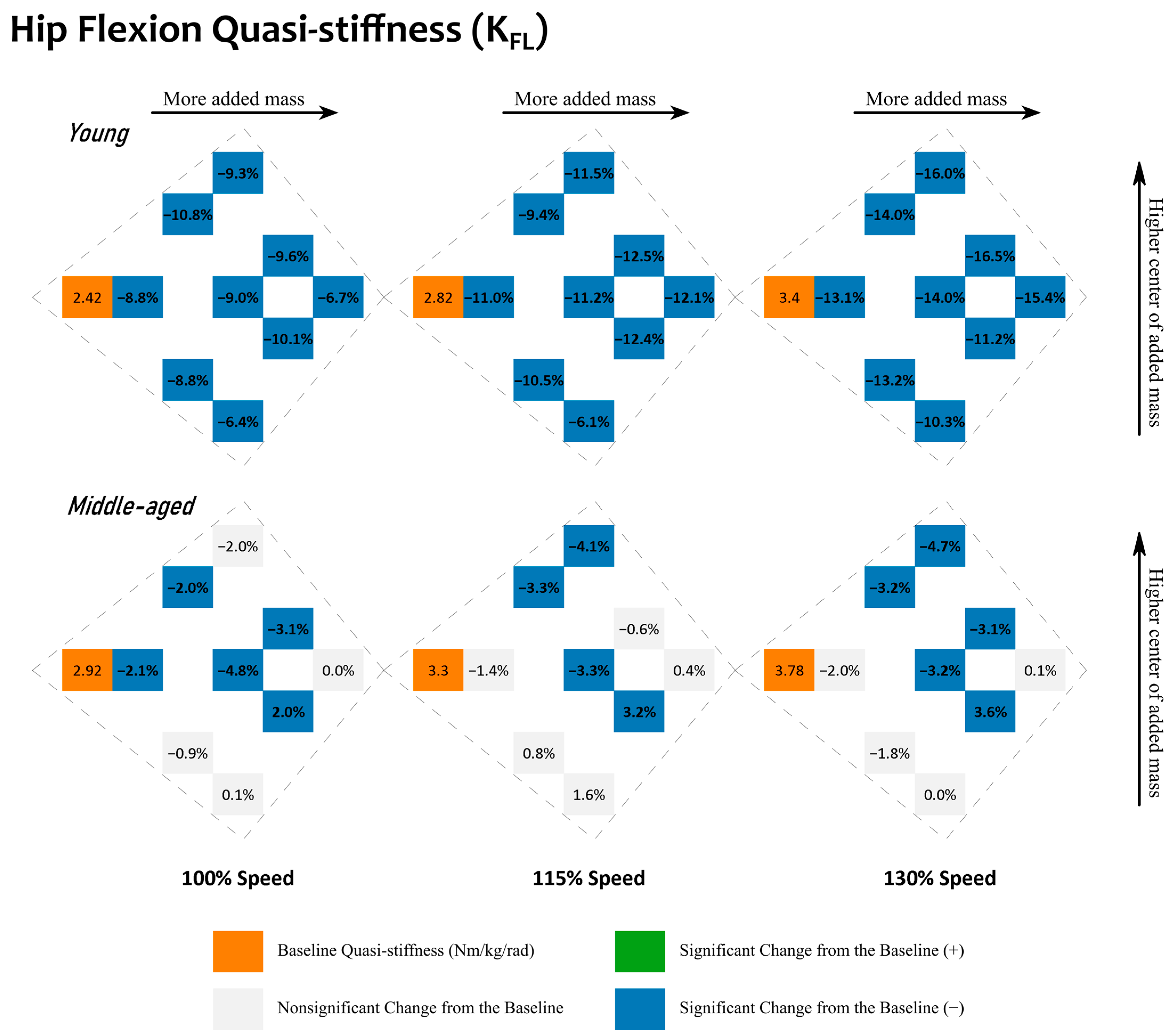
10], the hypothesis that increasing the walking speed will increase quasi-stiffness appears to be validated for both young and middle-aged adults. However, the hypothesis that quasi-stiffness increases with emulated hip exo added mass is more complex. In this study, we found that young adults support this hypothesis during hip extension, but the opposite, a reduction from baseline, occurs for hip flexion. Middle-aged adults showed mixed results for both hip extension and flexion changes that did not support such a generalization but instead required knowledge of the added mass amounts and locations on the body.
It is worth noting, before going into a discussion regarding the exact details of the influence of walking speeds and added mass on quasi-stiffness, that the approximations of such metrics using linearization were validated as being acceptable for both hip extension and flexion; see
Supplementary Tables S5 and S6.
4.2. Comparisons between Young and Middle-Aged Adults
Considering all of the experimental conditions during extension, young adults did not exhibit a different quasi-stiffness from that of middle-aged adults; see
Table 2. This lack of significant differences in quasi-stiffness between the two age groups during extension has been observed previously over the braking phase as well [
2]. A similar observation was made for the mechanical work during hip extension, though with a greater relative difference (9.5% for W
EX vs. 0.8% for K
EX) between the two age groups.
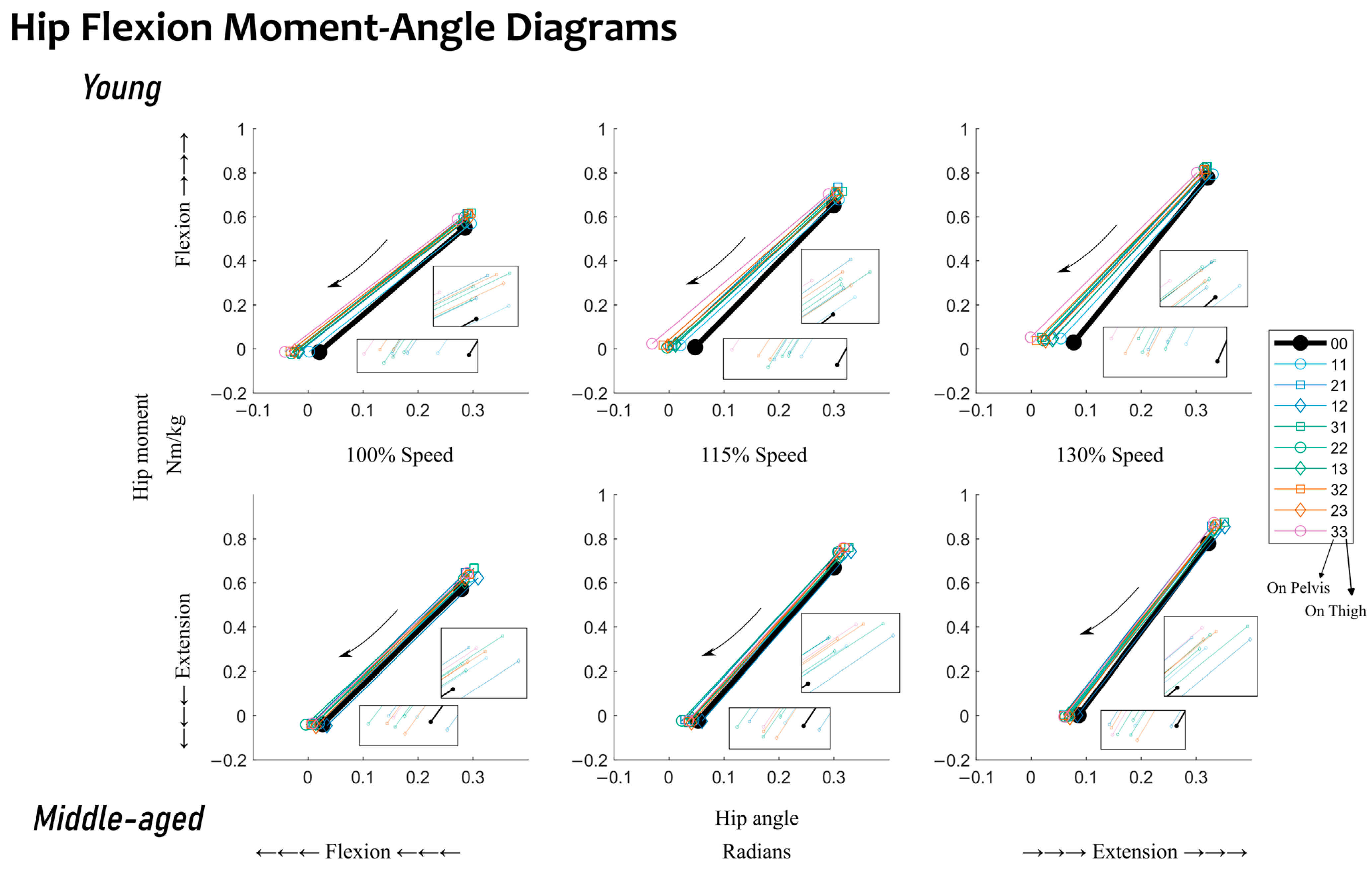
During hip flexion, a statistical difference between quasi-stiffness in young and middle-aged adults was observed; see
Table 2. Middle-aged adults’ quasi-stiffness was 27.4% higher than that of young adults. The moment–angle diagrams show that the difference in quasi-stiffness can be attributed to differences in the hip angle at the end point (toe-off) between the two age groups (
Figure 5). No statistical differences were observed between the two groups in work during hip flexion when mechanical work was generated at the hip joint. Given the statistical differences observed between the two groups, the following discussion will be split into the influences of walking speed and added mass within each age group.
4.3. Effects of Walking Speed on Young and Middle-Aged Adults
For both young and middle-aged adults, walking at a higher speed increased hip joint quasi-stiffness. Thus, the hypothesis that walking faster increases quasi-stiffness was further validated in this study within both groups. Specifically, increased walking speed significantly and consistently altered the quasi-stiffness during both extension and flexion; see
Table 3. The changes were such that a 30% increase in walking speed increased the mechanical work by almost 60% during hip flexion for young adults. This significant impact from increased walking speed aligns with what has been reported at the ankle joint by a previous study [
5].
The speed-induced quasi-stiffness increases observed in this study are comparable to those reported in previous studies with predominantly healthy, young adults [
6,
10]. To be specific, this study had both young and middle-aged participants walking on average at 1.058–1.375 m/s (100% and 130% speeds), which resulted in a quasi-stiffness range of 0.873–6.437 Nm/kg/rad during hip extension, and 0.560–9.157 Nm/kg/rad during hip flexion. Compared to the literature, a prior study assessed quasi-stiffness at walking speeds from 0.75 m/s to 2.6 m/s and also reported higher mean quasi-stiffness with faster walking speeds [
6]. The quasi-stiffness range for that study yielded 1.029–23.386 Nm/kg/rad for hip extension and 0.145–16.336 Nm/kg/rad for hip flexion. Additionally, a different prior study reported hip flexion quasi-stiffness to increase from 2.750 Nm/kg/rad at a walking speed of 0.8 m/s to 4.354 Nm/kg/rad at 1.2 m/s [
10]. Thus, this study expands upon what is known in the literature on the effect of walking speed on hip quasi-stiffness, as it shows that such an effect is consistent across both young and middle-aged groups.
4.4. Effects of Added Mass on Young Adults
The influence of added mass on quasi-stiffness is consistent for young adults: increases during hip extension and decreases during hip flexion. Adding mass to the lower body increased quasi-stiffness and kinetic energy absorption during hip extension (~30–55% of the gait cycle) and decreased quasi-stiffness with a higher kinetic energy generation during hip flexion (~55–65% of the gait cycle). However, increasing the amount of added mass does not always amplify those influences. When more added mass is transferred from the pelvis to the thighs, the quasi-stiffness mostly decreases during extension, and increases during flexion. This transfer of added mass from the pelvis to the thighs also reduces kinetic energy absorption during extension and kinetic energy generation during flexion.
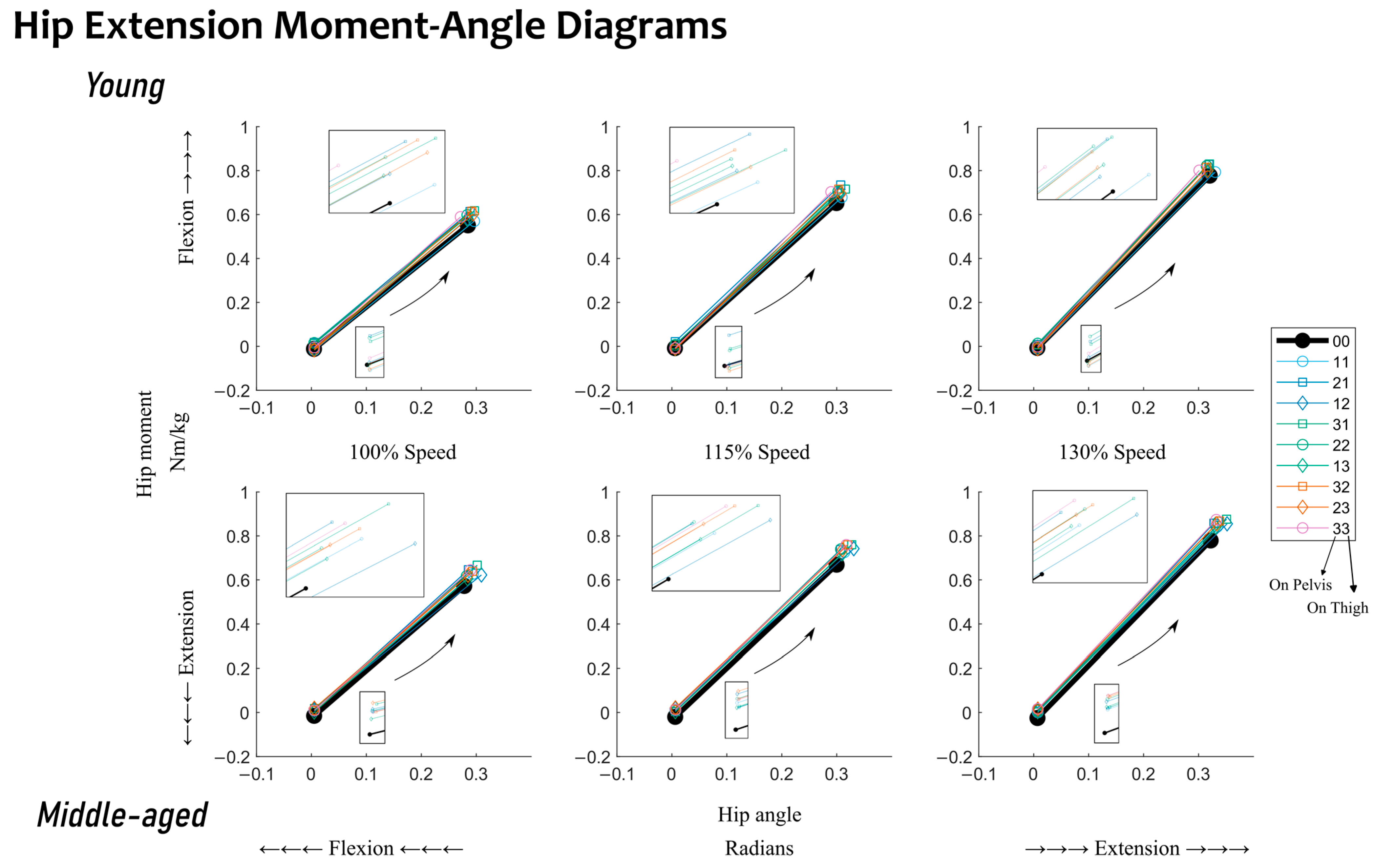
The hypothesis that added mass increases quasi-stiffness is validated during hip extension for young adults. The changes are almost all statistically significant; see
Figure 2. When relating to the moment–angle diagrams, the starting point is nominally the same but the end point (at the maximum extension angle) is often increased more by the moment than the angle; see
Figure 4. Analyzing this further, during extension, increased quasi-stiffness will absorb more kinetic energy over a small angular change. An increased rate of kinetic energy absorption leads to increased kinetic energy absorption at the hip during extension; see
Supplementary Figure S1.
Both the amount and the distribution of added mass play a role in quasi-stiffness for young adults. During hip extension, when added mass is evenly distributed across the pelvis and thighs (mass conditions: “11”, “22”, and “33”), the higher the amount of added mass, the greater its influence on quasi-stiffness. With total added mass of <14.4 lb, young adults steadily increased their quasi-stiffness when more added mass was added unevenly across the pelvis and thighs (mass conditions: “31”, “22”, and “13”). However, the patterns after this were not consistent. The potential reasoning for this can be that increased quasi-stiffness during extension has a negative impact from a kinetic energy point of view, as it would absorb more kinetic energy over a shorter angular change.
Given that young adults reduced their quasi-stiffness with added mass during hip flexion, see
Figure 3, the hypothesis that added mass increases quasi-stiffness is not supported. When relating to the moment–angle diagrams, the observed reduction in quasi-stiffness can be best attributed to the fact that the starting point has less changes than the angular shift towards flexion at the end point, toe-off; see
Figure 5. During this stage of returning kinetic energy, demonstrated via positive mechanical work, see
Supplementary Figure S2, with reduced quasi-stiffness, the hip joint generates greater mechanical work over the same angular change.
During hip flexion, the presumption that heavier added mass would result in larger changes was not fully supported. An added mass as little as 7.2 lb (mass condition: “11”) reduced the young adults’ quasi-stiffness by 8.8–13.1% compared to the baseline, whereas a larger added mass (21.6 lb) reduced it by 6.7–15.4%, indicating that reducing the mass added from 21.6 lb to 7.2 lb would not proportionally reduce its influence on quasi-stiffness during flexion.
Although there does not seem to be a one-size-fits-all observation for the influence of the amount of added mass on young adults, some added mass distributions may be more ideal than others. For example, when the center of added mass was lower (closer to the thighs), we observed smaller increases in quasi-stiffness during extension and smaller reductions in quasi-stiffness during flexion, as demonstrated in
Figure 2 and
Figure 3. A smaller increase in extension quasi-stiffness, see
Figure 2, shows that the mechanical work is distributed more evenly over a larger angular change, whereas a smaller reduction in flexion quasi-stiffness, see
Figure 3, shows that the mechanical work is distributed less evenly, and more mechanical work will be generated at the beginning of hip flexion. A lower center of added mass means that equal or more tungsten bars were added to the thighs than the pelvis. In
Figure 2 and
Figure 3 and
Supplementary Figures S1 and S2, this falls in the lower half of each cluster (mass conditions: “11”, “12”, “13”, “22”, “23”, and “33”).
One possible reason leading to increased quasi-stiffness during extension is that a higher center of added mass also places more of the added mass closer to the center of mass of the body. During hip extension, the center of mass of the body has just moved in front of the leg and keeps moving forward, while the thigh swings backward, dragging the center of body mass. Since more added mass is placed closer to the center of body mass, the hip joint must increase its quasi-stiffness to slow down the center of body mass. The turning point is when the plantarflexion moment at the ankle joint provides the propulsive force at the center of body mass through the hip joint, while the thigh swings forward. However, reduced hip joint quasi-stiffness during flexion indicates that young adults experienced more difficulty swinging the thigh forward during this phase.
4.5. Effects of Added Mass on Middle-Aged Adults
In response to added mass, middle-aged adults performed very differently in comparison to the young adults. Specifically, (1) when walking at the same speeds, middle-aged adults had higher quasi-stiffness during both hip extension (~35–55% of the gait cycle) and flexion (~55–65% of the gait cycle); (2) middle-aged adults had smaller relative changes in their quasi-stiffness when wearing added mass on the lower limb; and (3) middle-aged adults showed higher variability in quasi-stiffness and mechanical work. A smaller number of significant quasi-stiffness changes in response to added mass indicates that middle-aged adults do not systematically alter their quasi-stiffness. However, given the higher variability, predicting quasi-stiffness changes for middle-aged exo users may be difficult. Additionally, variability in quasi-stiffness reduced with most added mass combinations, indicating that although it can be more difficult to predict the quasi-stiffness changes for middle-aged adults, added mass of a hip exo may make such predictions easier by narrowing the range down.
Our results support our hypothesis that added mass increases hip joint quasi-stiffness for middle-aged adults during extension. However, in contrast to the young adults, these changes are smaller, and only apply to limited added mass conditions. In comparison to an added 7.2 lb (mass condition: “11”) where both age groups retained their quasi-stiffness compared to the baseline, the largest changes were caused by 10.8 lb (mass conditions: “12” and “21”). More specifically, these changes were 3.9–4.8%, and even heavier mass conditions did not result in a larger change. For middle-aged adults, the mass condition “12” was unique in that a quasi-stiffness reduction was observed during extension across all speeds. During flexion, however, middle-aged adults did alter their quasi-stiffness more with added mass of higher amounts, but only when the total added mass was no more than 14.4 lb and the center of added mass was not closer to the thighs. As observed in young adults, this should be beneficial for middle-aged adults to retain their kinetic energy at the hip joints by absorbing less while returning less.
Middle-aged adults experienced higher hip joint quasi-stiffness. When comparing the detailed quasi-stiffness values, see
Supplementary Tables S1–S4, the relative changes in the quasi-stiffness were different between the two age groups. In response to added mass, although at all walking speeds both groups increased the quasi-stiffness during extension and decreased it during flexion, the ranges were different. During extension, middle-aged adults started with higher quasi-stiffness at baseline. Walking at 100% speed, they had an average quasi-stiffness of 2.40 Nm/kg/rad, which was increased to 2.51 Nm/kg/rad at most with added mass. However, for young adults walking at the 100% speed, they started with a lower quasi-stiffness (2.24 Nm/kg/rad) and were able to increase their quasi-stiffness to a similar maximum value (2.50 Nm/kg/rad) with added mass. The same trends were observed at both the 115% and 130% speeds. For example, at 130% speed, young adults started at 2.75 Nm/kg/rad, and managed to increase the quasi-stiffness to a maximum of 2.99 Nm/kg/rad, whereas middle-aged adults started higher, at 2.83 Nm/kg/rad, and only peaked at 2.92 Nm/kg/rad.
Similar behavior happened during hip flexion as well. Both young and middle-aged adults reduced their quasi-stiffness due to added mass. Under the most extreme case, when walking at 130% speed, young adults started at 3.40 Nm/kg/rad, and reduced to a minimum of 2.84 Nm/kg/rad, whereas middle-aged adults started with 3.78 Nm/kg/rad, and only managed to reduce their quasi-stiffness to 3.61 Nm/kg/rad. This was a 0.56 Nm/kg/rad reduction for young adults, and only a 0.17 Nm/kg/rad reduction for middle-aged adults. Furthermore, middle-aged adults consistently showed higher standard deviations, with condition standard deviations ranging from 0.93 to 1.33 Nm/kg/rad, as opposed to young adults’ 0.58 to 1.07 Nm/kg/rad; see
Supplementary Table S2. Their hip joint mechanical work during hip extension had a standard deviation of 0.7 to 0.8 W/kg across all of the conditions, as opposed to young adults’ 0.03 to 0.05 W/kg; see
Supplementary Table S3. This indicates that middle-aged adults had higher quasi-stiffness and mechanical work variabilities during both extension and flexion.
4.6. Implications to Hip Exo Control
In this work, hip joint quasi-stiffness serves as an approximation of hip joint stiffness. For a hip exo with cooperative impedance control, to calculate the required torque output, the exo needs to first acquire an estimate of the wearer’s joint stiffness, which in this case was the hip joint quasi-stiffness. Here, it is worth noting that all quasi-stiffness quantifications discussed in this study were in the sagittal plane only, and so results will not directly translate to other planes such as the frontal plane. With that said, in this study, both young and middle-aged adults significantly increased both extension and flexion quasi-stiffness at faster walking speeds. This suggests that a hip exo should increase its stiffness support during the extension stage to help to absorb the kinetic energy. Similarly, in the flexion stage, a hip exo should increase its joint stiffness to provide hip flexion assistance in order to propel the center of body mass.
With hip-exo-like added mass, responses of young and middle-aged adults differed depending on mass amounts and distributions. Young adults had a majority of the mass conditions yield significant changes and so were generally predictable in their quasi-stiffness response to a hip exo’s added mass: during extension, there was larger quasi-stiffness with heavier added mass and a higher center of added mass; during flexion, there was smaller quasi-stiffness with added mass but not in any generalizable pattern with mass amounts or distributions. In contrast, middle-aged adults had approximately half of the mass conditions yield significant changes with respect to quasi-stiffness and so were much less generalizable. This leads to hip exo designers being able to use this information to intentionally design for the added mass amounts and locations on the body to target this age group. For example, designers could take advantage of the findings that there exist several added mass combinations which will result in a minimal shift of the wearer’s quasi-stiffness, at least under certain walking speeds, and furthermore, these combinations are not necessarily the lightest. With that being said, such mass combinations could still induce a different hip joint angle profile, as the workload is different because of the added mass, and so control algorithms may need to incorporate this information as well. Highlighting another example, hip exo designers could use the findings that since middle-aged adults have a smaller range of quasi-stiffness, estimation errors in a hip exo would be lower for middle-aged adults than for young adults, even if the hip exo control does not make the correct hip joint quasi-stiffness estimate. Thus, this study highlights that designing mass distributions for hip exos based only on information from young adults is not necessarily translational to older populations, even those as close in age as the middle-aged.
5. Conclusions
This study supports that both walking speed and added mass on the pelvis and thighs change the sagittal plane hip joint quasi-stiffness during hip extension and flexion among both young and middle-aged adults. The changes were more consistent with walking speed for both age groups, in that they increased their quasi-stiffness during both extension and flexion with higher speeds. The mechanical work also increased with faster walking speeds for both age groups, but by different relative amounts in comparison to quasi-stiffness.
In response to added mass, only extension quasi-stiffness was found to have similarities between the two age groups. Specifically, for both age groups, extension quasi-stiffness remained the same or increased when either the distribution on the pelvis and thighs was even or was biased to the pelvis. However, with added mass biased to the thighs, middle-aged adults had extension quasi-stiffness stay the same or decrease, while for young adults it increased. For flexion quasi-stiffness, young adults exhibited a decrease with added mass but not in any generalizable pattern with respect to the mass amounts or distributions. Conversely, middle-aged adults were found to have flexion quasi-stiffness remain the same or decrease with either an even distribution on the pelvis and thighs or biased to the pelvis, while no change occurred if biased to the thighs. While changes in quasi-stiffness did not always follow the same patterns with added mass amounts or distribution, mechanical work increased for both young and middle-aged adults during hip extension and flexion. Overall, middle-aged adults maintained a higher quasi-stiffness than young adults for all of the conditions but with a smaller range, indicating that their motor control output was elevated but did not tend to vary.
Given that the added mass in this study reflected the mass of a hip exo, we expect similar responses to be observed when a person wears a hip exo. Furthermore, this study found that middle-aged adults showed different added mass adaptations with respect to young adults. In conclusion, this study emphasizes the importance of studying the intended user populations, as parameters for age-specialized hip exos are likely different for achieving effective cooperative control design.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}