
IoT-Enabled Gait Assessment: The Next Step for Habitual Monitoring


{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Background: Digitizing Gait
3.1. Considerations: Prescribing
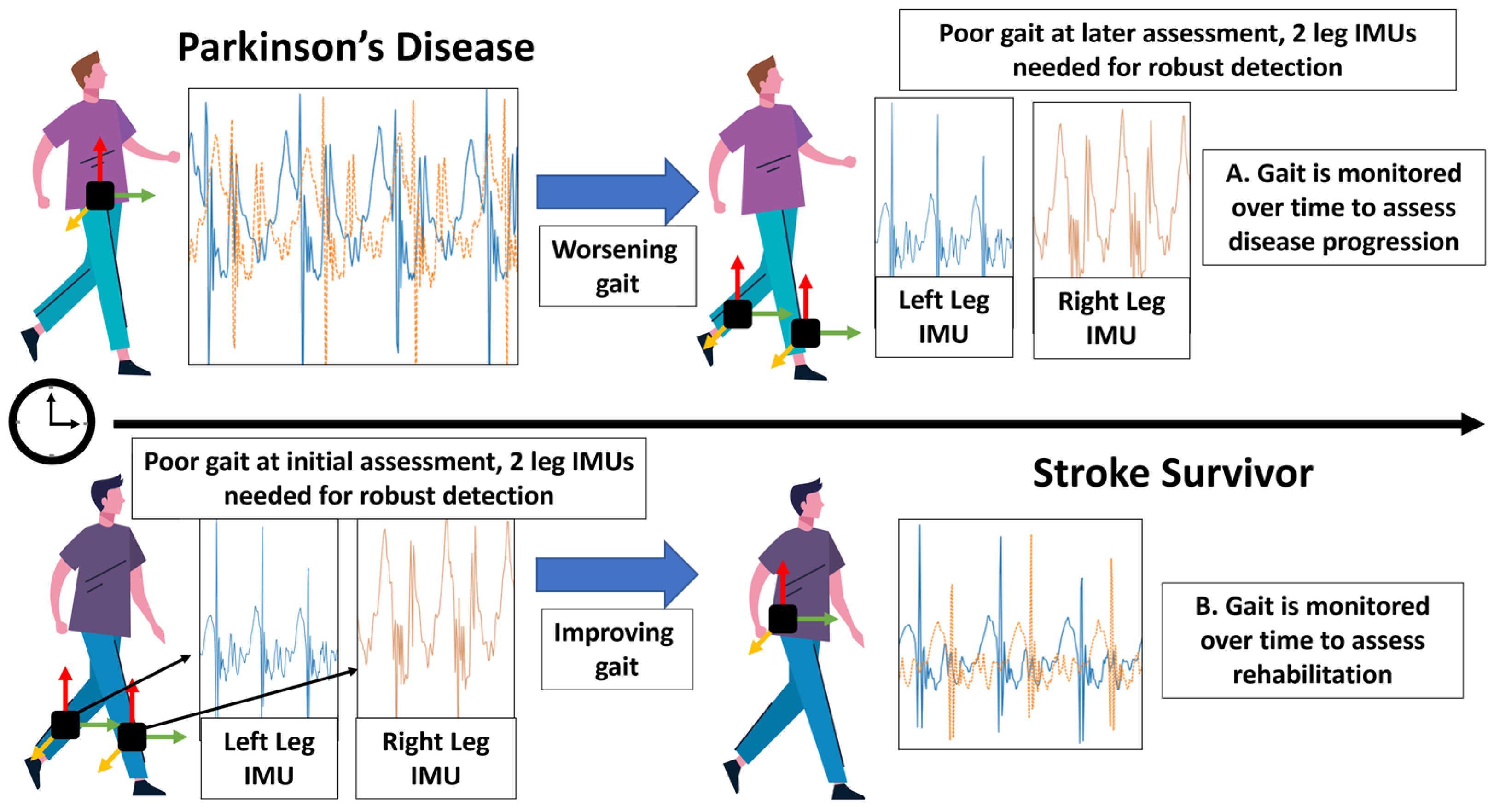
- PD gait will typically degrade over time, with incidence cohorts displaying lower step time, length, and velocity. As the disease progresses, affected individuals may be susceptible to wider gait asymmetry and bouts of freezing of gait (FOG) [53]. Additionally, a weakened pace and rhythm can be experienced within Parkinsonian gait [54].
- An increase in gait variability, as well as fluctuations in stride length and speed can be indicative of reduced cardiovascular health, often contributing to an increased risk of future health conditions [55].
- Ground contact time and the total step time show a significant increase when orthotics (shoe inserts) are used, suggesting that the latter do not interfere with running techniques and could be used as a preventive injury tool during running [56].
3.2. Instrumenting Gait: Approaches and Considerations
3.2.1. Inertial Measurement Units
3.2.2. Considerations and Limitations
3.2.3. Overcoming Obstacles
3.2.4. Smartphones
Limitations
4. IoT as an Enabler for Remote Assessment
4.1. Data Capture: Commercial Ubiquity
4.2. Local Networks: Data Handling
4.3. Edge Computing: High Frequency Data and Streaming
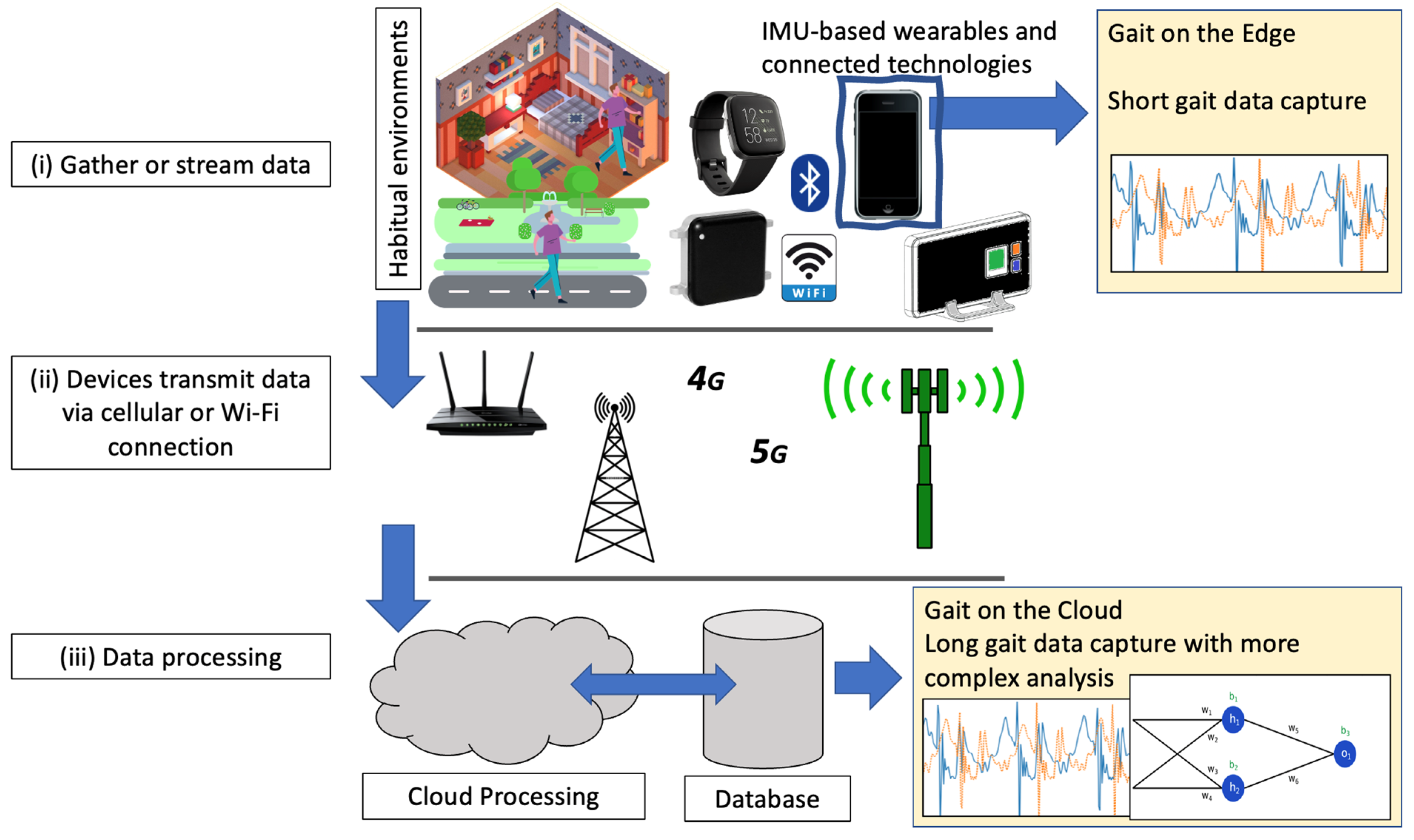
- Computationally inexpensive analyses are performed on-device to extract key features, regions of interest, and bouts of gait [101]. For example, during free-living assessment there will be periods of sedentary behavior (e.g., the person is sitting still or sleeping). As such, identifying regions of interest in the signal is paramount to provide the most relevant data for analysis. Pre-existing and validated approaches to identify gait in free-living scenarios [79,112] could be adapted for use on a smartphone due to relatively uncomplex computations (i.e., no use of deep learning). By identifying regions of interest within a high frequency signal before transmission, bandwidth/costs would be reduced by the sending of shorter signals.
- As seen in other domains such as autonomous vehicles [115], full datasets (i.e., not pre-processed on-device to define regions of interest) could be uploaded to a cloud instance for storage at less-regular intervals where data bandwidth was not of concern, e.g., if a Wi-Fi signal was available.
4.4. Data on the Cloud: Storage and Security
4.4.1. Data Storage
4.4.2. Data Security
Identity and Anonymity
Subjectivity and Resistance to Malicious Attacks
4.5. Data Processing in the Cloud
5. IoT-Enabled Multi-Modal Remote Gait Assessment
5.1. Computer Vision and Gait Assessment
Considerations
5.2. A Proposed Approach: The Complementarity of IMU and Computer Vision
5.2.1. Wireless-Enabled IMU
5.2.2. Smartphone as a Central Communication Node
5.2.3. Environmental Context
5.2.4. Data Transmission, Storage, and Cloud Infrastructure
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Friedl, K.E.; Looney, D.P. With life there is motion. Activity biomarkers signal important health and performance outcomes. J. Sci. Med. Sport 2023, in press. [Google Scholar] [CrossRef] [PubMed]
- Fritz, S.; Lusardi, M. White paper: “Walking speed: The sixth vital sign”. J. Geriatr. Phys. Ther. 2009, 32, 2–5. [Google Scholar] [CrossRef]
- Atrsaei, A.; Corrà, M.F.; Dadashi, F.; Vila-Chã, N.; Maia, L.; Mariani, B.; Maetzler, W.; Aminian, K. Gait speed in clinical and daily living assessments in Parkinson’s disease patients: Performance versus capacity. NPJ Park. Dis. 2021, 7, 24. [Google Scholar] [CrossRef] [PubMed]
- Merchant, R.A.; Goh, J.; Chan, Y.; Lim, J.; Vellas, B. Slow gait, subjective cognitive decline and motoric cognitive RISK syndrome: Prevalence and associated factors in community dwelling older adults. J. Nutr. Health Aging 2021, 25, 48–56. [Google Scholar] [CrossRef]
- Ozsoy, I.; Kodak, M.I.; Zerman, N.; Karartı, C.; Ozsoy, G.; Erturk, A. Gait speed predictors and gait-speed cut-off score to discriminate asthma control status and physical activity in patients with asthma. Adv. Respir. Med. 2022, 90, 164–170. [Google Scholar] [CrossRef] [PubMed]
- Montero-Odasso, M.; Pieruccini-Faria, F.; Bartha, R.; Black, S.E.; Finger, E.; Freedman, M.; Greenberg, B.; Grimes, D.A.; Hegele, R.A.; Hudson, C. Motor phenotype in neurodegenerative disorders: Gait and balance platform study design protocol for the Ontario neurodegenerative research initiative (ONDRI). J. Alzheimer’s Dis. 2017, 59, 707–721. [Google Scholar] [CrossRef]
- Ezzati, A.; Katz, M.J.; Lipton, M.L.; Lipton, R.B.; Verghese, J. The association of brain structure with gait velocity in older adults: A quantitative volumetric analysis of brain MRI. Neuroradiology 2015, 57, 851–861. [Google Scholar] [CrossRef]
- Braak, H.; Braak, E. Staging of Alzheimer’s disease-related neurofibrillary changes. Neurobiol. Aging 1995, 16, 271–278. [Google Scholar] [CrossRef]
- Kyröläinen, H.; Belli, A.; Komi, P.V. Biomechanical factors affecting running economy. Med. Sci. Sport. Exerc. 2001, 33, 1330–1337. [Google Scholar] [CrossRef]
- Saleh, M.; Murdoch, G. In defence of gait analysis. Observation and measurement in gait assessment. J. Bone Jt. Surg. Br. Vol. 1985, 67, 237–241. [Google Scholar] [CrossRef]
- Lord, S.; Halligan, P.; Wade, D. Visual gait analysis: The development of a clinical assessment and scale. Clin. Rehabil. 1998, 12, 107–119. [Google Scholar] [CrossRef] [PubMed]
- Read, H.S.; Hazlewood, M.E.; Hillman, S.J.; Prescott, R.J.; Robb, J.E. Edinburgh visual gait score for use in cerebral palsy. J. Pediatr. Orthop. 2003, 23, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Rathinam, C.; Bateman, A.; Peirson, J.; Skinner, J. Observational gait assessment tools in paediatrics–A systematic review. Gait Posture 2014, 40, 279–285. [Google Scholar] [CrossRef] [PubMed]
- Toro, B.; Nester, C.; Farren, P. A review of observational gait assessment in clinical practice. Physiother. Theory Pract. 2003, 19, 137–149. [Google Scholar] [CrossRef]
- Kluge, F.; Gaßner, H.; Hannink, J.; Pasluosta, C.; Klucken, J.; Eskofier, B.M. Towards mobile gait analysis: Concurrent validity and test-retest reliability of an inertial measurement system for the assessment of spatio-temporal gait parameters. Sensors 2017, 17, 1522. [Google Scholar] [CrossRef]
- Baskwill, A.J.; Belli, P.; Kelleher, L. Evaluation of a gait assessment module using 3D motion capture technology. Int. J. Ther. Massage Bodyw. 2017, 10, 3. [Google Scholar]
- Albert, J.A.; Owolabi, V.; Gebel, A.; Brahms, C.M.; Granacher, U.; Arnrich, B. Evaluation of the pose tracking performance of the azure kinect and kinect v2 for gait analysis in comparison with a gold standard: A pilot study. Sensors 2020, 20, 5104. [Google Scholar] [CrossRef]
- Jakob, V.; Küderle, A.; Kluge, F.; Klucken, J.; Eskofier, B.M.; Winkler, J.; Winterholler, M.; Gassner, H. Validation of a Sensor-Based Gait Analysis System with a Gold-Standard Motion Capture System in Patients with Parkinson’s Disease. Sensors 2021, 21, 7680. [Google Scholar] [CrossRef]
- Schlagenhauf, F.; Sreeram, S.; Singhose, W. Comparison of kinect and vicon motion capture of upper-body joint angle tracking. In Proceedings of the 2018 IEEE 14th International Conference on Control and Automation (ICCA), Anchorage, AK, USA, 12–15 June 2018; pp. 674–679. [Google Scholar]
- Sharma, S.; Verma, S.; Kumar, M.; Sharma, L. Use of motion capture in 3D animation: Motion capture systems, challenges, and recent trends. In Proceedings of the 2019 International Conference on Machine Learning, Big Data, Cloud and Parallel Computing (COMITCon), Faridabad, India, 14–16 February 2019; pp. 289–294. [Google Scholar]
- Zhao, H.; Wang, Z.; Qiu, S.; Shen, Y.; Wang, J. IMU-based gait analysis for rehabilitation assessment of patients with gait disorders. In Proceedings of the 2017 4th International Conference on Systems and Informatics (ICSAI), Hangzhou, China, 11–13 November 2017; pp. 622–626. [Google Scholar]
- Young, F.; Coulby, G.; Watson, I.; Downs, C.; Stuart, S.; Godfrey, A. Just find it: The Mymo approach to recommend running shoes. IEEE Access 2020, 8, 109791–109800. [Google Scholar] [CrossRef]
- Ahmad, N.; Ghazilla, R.A.R.; Khairi, N.M.; Kasi, V. Reviews on various inertial measurement unit (IMU) sensor applications. Int. J. Signal Process. Syst. 2013, 1, 256–262. [Google Scholar] [CrossRef]
- Bo, F.; Yerebakan, M.; Dai, Y.; Wang, W.; Li, J.; Hu, B.; Gao, S. IMU-Based Monitoring for Assistive Diagnosis and Management of IoHT: A Review. Healthcare 2022, 10, 1210. [Google Scholar] [CrossRef]
- Young, F.; Stuart, S.; Morris, R.; Downs, C.; Coleman, M.; Godfrey, A. Validation of an inertial-based contact and swing time algorithm for running analysis from a foot mounted IoT enabled wearable. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Virtual, 1–5 November 2021; pp. 6818–6821. [Google Scholar]
- Benson, L.C.; Räisänen, A.M.; Clermont, C.A.; Ferber, R. Is This the Real Life, or Is This Just Laboratory? A Scoping Review of IMU-Based Running Gait Analysis. Sensors 2022, 22, 1722. [Google Scholar] [CrossRef]
- Mc Ardle, R.; Morris, R.; Hickey, A.; Del Din, S.; Koychev, I.; Gunn, R.N.; Lawson, J.; Zamboni, G.; Ridha, B.; Sahakian, B.J. Gait in mild Alzheimer’s disease: Feasibility of multi-center measurement in the clinic and home with body-worn sensors: A pilot study. J. Alzheimer’s Dis. 2018, 63, 331–341. [Google Scholar] [CrossRef]
- Webster, K.E.; Merory, J.R.; Wittwer, J.E. Gait variability in community dwelling adults with Alzheimer disease. Alzheimer Dis. Assoc. Disord. 2006, 20, 37–40. [Google Scholar] [CrossRef]
- Belghali, M.; Chastan, N.; Cignetti, F.; Davenne, D.; Decker, L.M. Loss of gait control assessed by cognitive-motor dual-tasks: Pros and cons in detecting people at risk of developing Alzheimer’s and Parkinson’s diseases. Geroscience 2017, 39, 305–329. [Google Scholar] [CrossRef] [PubMed]
- Brodie, M.A.; Lovell, N.H.; Canning, C.G.; Menz, H.B.; Delbaere, K.; Redmond, S.J.; Latt, M.; Sturnieks, D.L.; Menant, J.; Smith, S.T. Gait as a biomarker? Accelerometers reveal that reduced movement quality while walking is associated with Parkinson’s disease, ageing and fall risk. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 26–30 August 2014; pp. 5968–5971. [Google Scholar]
- Buckley, C.; Galna, B.; Rochester, L.; Mazzà, C. Upper body accelerations as a biomarker of gait impairment in the early stages of Parkinson’s disease. Gait Posture 2019, 71, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Koller, W.C.; Trimble, J. The gait abnormality of Huntington’s disease. Neurology 1985, 35, 1450. [Google Scholar] [CrossRef] [PubMed]
- Gaßner, H.; Jensen, D.; Marxreiter, F.; Kletsch, A.; Bohlen, S.; Schubert, R.; Muratori, L.M.; Eskofier, B.; Klucken, J.; Winkler, J. Gait variability as digital biomarker of disease severity in Huntington’s disease. J. Neurol. 2020, 267, 1594–1601. [Google Scholar] [CrossRef] [PubMed]
- Mirek, E.; Filip, M.; Chwała, W.; Banaszkiewicz, K.; Rudzinska-Bar, M.; Szymura, J.; Pasiut, S.; Szczudlik, A. Three-Dimensional Trunk and Lower Limbs Characteristics during Gait in Patients with Huntington’s Disease. Front. Neurosci. 2017, 11, 566. [Google Scholar] [CrossRef]
- Mason, R.; Pearson, L.T.; Barry, G.; Young, F.; Lennon, O.; Godfrey, A.; Stuart, S. Wearables for Running Gait Analysis: A Systematic Review. Sport. Med. 2023, 53, 241–268. [Google Scholar] [CrossRef]
- Young, F.; Mason, R.; Wall, C.; Morris, R.; Stuart, S.; Godfrey, A. Examination of a foot mounted IMU-based methodology for a running gait assessment. Front. Sport. Act. Living 2022, 4, 956889. [Google Scholar] [CrossRef]
- Zhang, H.; Yin, Y.; Chen, Z.; Zhang, Y.; Rao, A.K.; Guo, Y.; Zanotto, D. Wearable Biofeedback System to Induce Desired Walking Speed in Overground Gait Training. Sensors 2020, 20, 4002. [Google Scholar] [CrossRef]
- Celik, Y.; Powell, D.; Woo, W.L.; Stuart, S.; Godfrey, A. A feasibility study towards instrumentation of the Sport Concussion Assessment Tool (iSCAT). In Proceedings of the 2020 42nd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Montreal, QC, Canada, 20–24 July 2020; pp. 4624–4627. [Google Scholar]
- Beauchet, O.; Allali, G.; Launay, C.; Herrmann, F.; Annweiler, C. Gait variability at fast-pace walking speed: A biomarker of mild cognitive impairment? J. Nutr. Health Aging 2013, 17, 235–239. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Stone, E.; Skubic, M.; Keller, J.M.; Abbott, C.; Rantz, M. Toward a passive low-cost in-home gait assessment system for older adults. IEEE J. Biomed. Health Inform. 2013, 17, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Stone, E.E.; Skubic, M. Capturing habitual, in-home gait parameter trends using an inexpensive depth camera. In Proceedings of the 2012 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 28 August–1 September 2012; pp. 5106–5109. [Google Scholar]
- Bongartz, M.; Kiss, R.; Lacroix, A.; Eckert, T.; Ullrich, P.; Jansen, C.-P.; Feißt, M.; Mellone, S.; Chiari, L.; Becker, C. Validity, reliability, and feasibility of the uSense activity monitor to register physical activity and gait performance in habitual settings of geriatric patients. Physiol. Meas. 2019, 40, 095005. [Google Scholar] [CrossRef]
- Godfrey, A. Wearables for independent living in older adults: Gait and falls. Maturitas 2017, 100, 16–26. [Google Scholar] [CrossRef]
- Strozzi, N.; Parisi, F.; Ferrari, G. Impact of on-body IMU placement on inertial navigation. IET Wirel. Sens. Syst. 2017, 8, 3–9. [Google Scholar] [CrossRef]
- Garai, Á.; Péntek, I.; Adamkó, A. Revolutionizing healthcare with IoT and cognitive, cloud-based telemedicine. Acta Polytech. Hung 2019, 16, 163–181. [Google Scholar]
- Abdellatif, M.M.; Mohamed, W. Telemedicine: An IoT Based Remote Healthcare System. Int. J. Online Biomed. Eng. 2020, 16. [Google Scholar] [CrossRef]
- Nguyen, H.H.; Mirza, F.; Naeem, M.A.; Nguyen, M. A review on IoT healthcare monitoring applications and a vision for transforming sensor data into real-time clinical feedback. In Proceedings of the 2017 IEEE 21st International Conference on Computer Supported Cooperative Work in Design (CSCWD), Wellington, New Zealand, 26–28 April 2017; pp. 257–262. [Google Scholar]
- Barata, J.J.R.; Munoz, R.; Silva, R.D.D.C.; Rodrigues, J.J.; De Albuquerque, V.H.C. Internet of Things based on electronic and mobile health systems for blood glucose continuous monitoring and management. IEEE Access 2019, 7, 175116–175125. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef]
- Morris, R.; Lord, S.; Bunce, J.; Burn, D.; Rochester, L. Gait and cognition: Mapping the global and discrete relationships in ageing and neurodegenerative disease. Neurosci. Biobehav. Rev. 2016, 64, 326–345. [Google Scholar] [CrossRef]
- Celik, Y.; Stuart, S.; Woo, W.L.; Godfrey, A. Gait analysis in neurological populations: Progression in the use of wearables. Med. Eng. Phys. 2020, 87, 9–29. [Google Scholar] [CrossRef] [PubMed]
- Von Schroeder, H.P.; Coutts, R.D.; Lyden, P.D.; Billings, E.; Nickel, V.L. Gait parameters following stroke: A practical assessment. J. Rehabil. Res. Dev. 1995, 32, 25. [Google Scholar] [PubMed]
- Moore, O.; Peretz, C.; Giladi, N. Freezing of gait affects quality of life of peoples with Parkinson’s disease beyond its relationships with mobility and gait. Mov. Disord. Off. J. Mov. Disord. Soc. 2007, 22, 2192–2195. [Google Scholar] [CrossRef]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in Parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef] [PubMed]
- Rosano, C.; Brach, J.; Studenski, S.; Longstreth, W., Jr.; Newman, A.B. Gait variability is associated with subclinical brain vascular abnormalities in high-functioning older adults. Neuroepidemiology 2007, 29, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Florenciano Restoy, J.L.; Solé-Casals, J.; Borràs-Boix, X. IMU-Based Effects Assessment of the Use of Foot Orthoses in the Stance Phase during Running and Asymmetry between Extremities. Sensors 2021, 21, 3277. [Google Scholar] [CrossRef]
- Hobert, M.A.; Nussbaum, S.; Heger, T.; Berg, D.; Maetzler, W.; Heinzel, S. Progressive gait deficits in Parkinson’s disease: A wearable-based biannual 5-year prospective study. Front. Aging Neurosci. 2019, 11, 22. [Google Scholar] [CrossRef]
- Hsu, W.-C.; Sugiarto, T.; Lin, Y.-J.; Yang, F.-C.; Lin, Z.-Y.; Sun, C.-T.; Hsu, C.-L.; Chou, K.-N. Multiple-wearable-sensor-based gait classification and analysis in patients with neurological disorders. Sensors 2018, 18, 3397. [Google Scholar] [CrossRef]
- Zhou, L.; Fischer, E.; Tunca, C.; Brahms, C.M.; Ersoy, C.; Granacher, U.; Arnrich, B. How we found our imu: Guidelines to IMU selection and a comparison of seven IMUs for pervasive healthcare applications. Sensors 2020, 20, 4090. [Google Scholar] [CrossRef]
- Weizman, Y.; Tirosh, O.; Fuss, F.K.; Tan, A.M.; Rutz, E. Recent State of Wearable IMU Sensors Use in People Living with Spasticity: A Systematic Review. Sensors 2022, 22, 1791. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, N.F.; Santos, C.P. Inertial measurement units: A brief state of the art on gait analysis. In Proceedings of the 2017 IEEE 5th Portuguese Meeting on Bioengineering (ENBENG), Coimbra, Portugal, 16–18 February 2017; pp. 1–4. [Google Scholar]
- Sabatini, A.M.; Martelloni, C.; Scapellato, S.; Cavallo, F. Assessment of walking features from foot inertial sensing. IEEE Trans. Biomed. Eng. 2005, 52, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Niswander, W.; Wang, W.; Kontson, K. Optimization of IMU sensor placement for the measurement of lower limb joint kinematics. Sensors 2020, 20, 5993. [Google Scholar] [CrossRef] [PubMed]
- Klieme, E.; Tietz, C.; Meinel, C. Beware of smombies: Verification of users based on activities while walking. In Proceedings of the 2018 17th IEEE International Conference on Trust, Security and Privacy in Computing and Communications/12th IEEE International Conference on Big Data Science and Engineering (TrustCom/BigDataSE), New York, NY, USA, 1–3 August 2018; pp. 651–660. [Google Scholar]
- Bet, P.; Castro, P.C.; Ponti, M.A. Fall detection and fall risk assessment in older person using wearable sensors: A systematic review. Int. J. Med. Inform. 2019, 130, 103946. [Google Scholar] [CrossRef]
- Diaz, E.M.; Heirich, O.; Khider, M.; Robertson, P. Optimal sampling frequency and bias error modeling for foot-mounted IMUs. In Proceedings of the International Conference on Indoor Positioning and Indoor Navigation, Nantes, France, 24–27 September 2018; pp. 1–9. [Google Scholar]
- Gujarathi, T.; Bhole, K. Gait analysis using imu sensor. In Proceedings of the 2019 10th International Conference on Computing, Communication and Networking Technologies (ICCCNT), Kanpur, India, 6–8 July 2019; pp. 1–5. [Google Scholar]
- Vargas-Valencia, L.S.; Elias, A.; Rocon, E.; Bastos-Filho, T.; Frizera, A. An IMU-to-body alignment method applied to human gait analysis. Sensors 2016, 16, 2090. [Google Scholar] [CrossRef]
- Bolink, S.; Naisas, H.; Senden, R.; Essers, H.; Heyligers, I.; Meijer, K.; Grimm, B. Validity of an inertial measurement unit to assess pelvic orientation angles during gait, sit–stand transfers and step-up transfers: Comparison with an optoelectronic motion capture system. Med. Eng. Phys. 2016, 38, 225–231. [Google Scholar] [CrossRef]
- Dehzangi, O.; Taherisadr, M.; ChangalVala, R. IMU-based gait recognition using convolutional neural networks and multi-sensor fusion. Sensors 2017, 17, 2735. [Google Scholar] [CrossRef]
- McCamley, J.; Donati, M.; Grimpampi, E.; Mazzà, C. An enhanced estimate of initial contact and final contact instants of time using lower trunk inertial sensor data. Gait Posture 2012, 36, 316–318. [Google Scholar] [CrossRef]
- Del Din, S.; Godfrey, A.; Rochester, L. Validation of an accelerometer to quantify a comprehensive battery of gait characteristics in healthy older adults and Parkinson’s disease: Toward clinical and at home use. IEEE J. Biomed. Health Inform. 2015, 20, 838–847. [Google Scholar] [CrossRef]
- Czech, M.D.; Patel, S. GaitPy: An open-source python package for gait analysis using an accelerometer on the lower back. J. Open Source Softw. 2019, 4, 1778. [Google Scholar] [CrossRef]
- Zijlstra, W.; Hof, A.L. Assessment of spatio-temporal gait parameters from trunk accelerations during human walking. Gait Posture 2003, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Powell, D.; Stuart, S.; Fearn, D.; Bowen, S.; Steel, H.; Jones, T.; Godfrey, A. Wearables as objective tools in sport-related concussion: A protocol for more informed player management. Physiotherapy 2020, 107, e142–e143. [Google Scholar] [CrossRef]
- Chen, Y.; Hu, W.; Yang, Y.; Hou, J.; Wang, Z. A method to calibrate installation orientation errors of inertial sensors for gait analysis. In Proceedings of the 2014 IEEE International Conference on Information and Automation (ICIA), Hailar, China, 28–30 July 2014; pp. 598–603. [Google Scholar]
- Mancini, M.; Horak, F.B. Potential of APDM mobility lab for the monitoring of the progression of Parkinson’s disease. Expert Rev. Med. Devices 2016, 13, 455–462. [Google Scholar] [CrossRef] [PubMed]
- Godfrey, A.; Del Din, S.; Barry, G.; Mathers, J.C.; Rochester, L. Within trial validation and reliability of a single tri-axial accelerometer for gait assessment. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Diego, CA, USA, 26–30 August 2014; pp. 5892–5895. [Google Scholar]
- Hickey, A.; Del Din, S.; Rochester, L.; Godfrey, A. Detecting free-living steps and walking bouts: Validating an algorithm for macro gait analysis. Physiol. Meas. 2016, 38, N1. [Google Scholar] [CrossRef]
- Doherty, A.; Jackson, D.; Hammerla, N.; Plötz, T.; Olivier, P.; Granat, M.H.; White, T.; Van Hees, V.T.; Trenell, M.I.; Owen, C.G. Large scale population assessment of physical activity using wrist worn accelerometers: The UK Biobank Study. PLoS ONE 2017, 12, e0169649. [Google Scholar] [CrossRef]
- Leite, P.; Postolache, O.; Pereira, J.D.; Postolache, G. Gait rehabilitation monitor. Proc. J. Phys. Conf. Ser. 2019, 1379, 012071. [Google Scholar] [CrossRef]
- Gowthami, S.; Kumar, S. Impact of smartphone: A pilot study on positive and negative effects. Int. J. Sci. Eng. Appl. Sci. 2016, 2, 473–478. [Google Scholar]
- Hoffman, L.; Wisniewski, H.; Hays, R.; Henson, P.; Vaidyam, A.; Hendell, V.; Keshavan, M.; Torous, J. Digital Opportunities for Outcomes in Recovery Services (DOORS): A pragmatic hands-on group approach toward increasing digital health and smartphone competencies, autonomy, relatedness, and alliance for those with serious mental illness. J. Psychiatr. Pract. 2020, 26, 80. [Google Scholar] [CrossRef] [PubMed]
- Pratap, A.; Grant, D.; Vegesna, A.; Tummalacherla, M.; Cohan, S.; Deshpande, C.; Mangravite, L.; Omberg, L. Evaluating the utility of smartphone-based sensor assessments in persons with multiple sclerosis in the real-world using an app (elevateMS): Observational, prospective pilot digital health study. JMIR Mhealth Uhealth 2020, 8, e22108. [Google Scholar] [CrossRef]
- Kim, J.H.; Choi, W.S.; Song, J.Y.; Yoon, Y.K.; Kim, M.J.; Sohn, J.W. The role of smart monitoring digital health care system based on smartphone application and personal health record platform for patients diagnosed with coronavirus disease 2019. BMC Infect. Dis. 2021, 21, 229. [Google Scholar] [CrossRef]
- Bhavsar, K.; Singhal, S.; Chandel, V.; Samal, A.; Khandelwal, S.; Ahmed, N.; Ghose, A. Digital Biomarkers: Using Smartwatch Data For Clinically Relevant Outcomes. In Proceedings of the 2021 IEEE International Conference on Pervasive Computing and Communications Workshops and other Affiliated Events (PerCom Workshops), Kassel, Germany, 22–26 March 2021; pp. 630–635. [Google Scholar]
- Erdem, N.S.; Ersoy, C.; Tunca, C. Gait analysis using smartwatches. In Proceedings of the 2019 IEEE 30th International Symposium on Personal, Indoor and Mobile Radio Communications (PIMRC Workshops), Istanbul, Turkey, 8 September 2019; pp. 1–6. [Google Scholar]
- Yu-Huei, C.; Ja-Shen, C.; Ming-Chao, W. Why do older adults use wearable devices: A case study adopting the Senior Technology Acceptance Model (STAM). In Proceedings of the 2019 Portland International Conference on Management of Engineering and Technology (PICMET), Portland, OR, USA, 25–29 August 2019; pp. 1–8. [Google Scholar]
- Miao, B.Y.; Arneson, D.; Wang, M.; Butte, A.J. Open challenges in developing digital therapeutics in the United States. PLOS Digit. Health 2022, 1, e0000008. [Google Scholar] [CrossRef] [PubMed]
- Breitinger, F.; Tully-Doyle, R.; Hassenfeldt, C. A survey on smartphone user’s security choices, awareness and education. Comput. Secur. 2020, 88, 101647. [Google Scholar] [CrossRef]
- Chia, C.; Choo, K.-K.; Fehrenbacher, D. How Cyber-Savvy are Older Mobile Device Users? In Mobile Security and Privacy; Elsevier: Amsterdam, The Netherlands, 2017; pp. 67–83. [Google Scholar]
- Greco, L.; Percannella, G.; Ritrovato, P.; Tortorella, F.; Vento, M. Trends in IoT based solutions for health care: Moving AI to the edge. Pattern Recognit. Lett. 2020, 135, 346–353. [Google Scholar] [CrossRef]
- Greco, L.; Ritrovato, P.; Xhafa, F. An edge-stream computing infrastructure for real-time analysis of wearable sensors data. Future Gener. Comput. Syst. 2019, 93, 515–528. [Google Scholar] [CrossRef]
- Uddin, M.Z. A wearable sensor-based activity prediction system to facilitate edge computing in smart healthcare system. J. Parallel Distrib. Comput. 2019, 123, 46–53. [Google Scholar] [CrossRef]
- Kumar, P.M.; Gandhi, U.D. A novel three-tier Internet of Things architecture with machine learning algorithm for early detection of heart diseases. Comput. Electr. Eng. 2018, 65, 222–235. [Google Scholar] [CrossRef]
- Coulby, G.; Clear, A.; Jones, O.; Young, F.; Stuart, S.; Godfrey, A. Towards remote healthcare monitoring using accessible IoT technology: State-of-the-art, insights and experimental design. BioMedical Eng. OnLine 2020, 19, 80. [Google Scholar] [CrossRef]
- Farahani, B.; Firouzi, F.; Chakrabarty, K. Healthcare iot. In Intelligent Internet of Things; Springer: Berlin/Heidelberg, Germany, 2020; pp. 515–545. [Google Scholar]
- Muthu, B.; Sivaparthipan, C.; Manogaran, G.; Sundarasekar, R.; Kadry, S.; Shanthini, A.; Dasel, A. IOT based wearable sensor for diseases prediction and symptom analysis in healthcare sector. Peer-to-Peer Netw. Appl. 2020, 13, 2123–2134. [Google Scholar] [CrossRef]
- Ladha, C.; Del Din, S.; Nazarpour, K.; Hickey, A.; Morris, R.; Catt, M.; Rochester, L.; Godfrey, A. Toward a low-cost gait analysis system for clinical and free-living assessment. In Proceedings of the 2016 38th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Orlando, FL, USA, 16–20 August 2016; pp. 1874–1877. [Google Scholar]
- Li, Y.; Zhang, P.; Zhang, Y.; Miyazaki, K. Gait Analysis Using Stereo Camera in Daily Environment. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 1471–1475. [Google Scholar]
- Steins, D.; Sheret, I.; Dawes, H.; Esser, P.; Collett, J. A smart device inertial-sensing method for gait analysis. J. Biomech. 2014, 47, 3780–3785. [Google Scholar] [CrossRef]
- David, R.; Duke, J.; Jain, A.; Janapa Reddi, V.; Jeffries, N.; Li, J.; Kreeger, N.; Nappier, I.; Natraj, M.; Wang, T. Tensorflow lite micro: Embedded machine learning for tinyml systems. Proc. Mach. Learn. Syst. 2021, 3, 800–811. [Google Scholar]
- Moyle, W.; Jones, C.; Murfield, J.; Dwan, T.; Ownsworth, T. ‘We don’t even have Wi-Fi’: A descriptive study exploring current use and availability of communication technologies in residential aged care. Contemp. Nurse 2018, 54, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Anderson, M.; Perrin, A. Tech adoption climbs among older Americans. Pew Res. Cent. Internet Sci. Tech 2017. [Google Scholar]
- Jones, P.; Comfort, D. A commentary on the rollout of 5g mobile in the UK. J. Public Aff. 2020, 20, e1993. [Google Scholar] [CrossRef]
- Jenal, C.; Endreß, S.; Kühne, O.; Zylka, C. Technological Transformation Processes and Resistance—On the Conflict Potential of 5G Using the Example of 5G Network Expansion in Germany. Sustainability 2021, 13, 13550. [Google Scholar] [CrossRef]
- Medin, M.; Louie, G. The 5G Ecosystem: Risks and Opportunities for DoD; Defense Innovation Board: Washington, DC, USA, 2019. [Google Scholar]
- Shorgin, S.; Samouylov, K.; Gudkova, I.; Galinina, O.; Andreev, S. On the benefits of 5G wireless technology for future mobile cloud computing. In Proceedings of the 2014 International Science and Technology Conference (Modern Networking Technologies)(MoNeTeC), Moscow, Russia, 28–29 October 2014; pp. 1–4. [Google Scholar]
- Celik, Y.; Stuart, S.; Woo, W.L.; Sejdic, E.; Godfrey, A. Multi-modal gait: A wearable, algorithm and data fusion approach for clinical and free-living assessment. Inf. Fusion 2022, 78, 57–70. [Google Scholar] [CrossRef]
- Del Din, S.; Galna, B.; Godfrey, A.; Bekkers, E.M.; Pelosin, E.; Nieuwhof, F.; Mirelman, A.; Hausdorff, J.M.; Rochester, L. Analysis of free-living gait in older adults with and without Parkinson’s disease and with and without a history of falls: Identifying generic and disease-specific characteristics. J. Gerontol. Ser. A 2019, 74, 500–506. [Google Scholar] [CrossRef]
- Reginya, S.; Meigal, A.Y.; Gerasimova-Meigal, L.I.; Prokhorov, K.; Moschevikin, A. Using smartphone inertial measurement unit for analysis of human gait. Int. J. Embed. Real-Time Commun. Syst. 2019, 10, 101–117. [Google Scholar] [CrossRef]
- Lyons, G.; Culhane, K.; Hilton, D.; Grace, P.; Lyons, D. A description of an accelerometer-based mobility monitoring technique. Med. Eng. Phys. 2005, 27, 497–504. [Google Scholar] [CrossRef]
- Nieto-Hidalgo, M.; Ferrández-Pastor, F.J.; Valdivieso-Sarabia, R.J.; Mora-Pascual, J.; García-Chamizo, J.M. Gait analysis using computer vision based on cloud platform and mobile device. Mob. Inf. Syst. 2018, 2018, 7381264. [Google Scholar] [CrossRef]
- Castiglione, A.; Choo, K.-K.R.; De Marsico, M.; Mecca, A. Walking on the cloud: Gait recognition, a wearable solution. In Proceedings of the International Conference on Network and System Security, Hong Kong, China, 27–29 August 2018; pp. 174–186. [Google Scholar]
- Khan, Z.; Prehofer, C. Efficient and Selective Upload of Data from Connected Vehicles. In Proceedings of the 6th International Conference on Vehicle Technology and Intelligent Transport Systems (VEHITS 2020), Online, 2–4 May 2020; pp. 559–566. [Google Scholar]
- Yu, W.; Liang, F.; He, X.; Hatcher, W.G.; Lu, C.; Lin, J.; Yang, X. A survey on the edge computing for the Internet of Things. IEEE Access 2017, 6, 6900–6919. [Google Scholar] [CrossRef]
- Nouredanesh, M.; Godfrey, A.; Howcroft, J.; Lemaire, E.D.; Tung, J. Fall risk assessment in the wild: A critical examination of wearable sensors use in free-living conditions. Gait Posture 2020, 85, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.U.; Stenholm, S.; Metter, E.J.; Ferrucci, L. Age-associated gait patterns and the role of lower extremity strength—Results from the Baltimore Longitudinal Study of Aging. Arch. Gerontol. Geriatr. 2012, 55, 474–479. [Google Scholar] [CrossRef]
- Dever, A.; Powell, D.; Graham, L.; Mason, R.; Das, J.; Marshall, S.J.; Vitorio, R.; Godfrey, A.; Stuart, S. Gait impairment in traumatic brain injury: A systematic review. Sensors 2022, 22, 1480. [Google Scholar] [CrossRef] [PubMed]
- Muir, S.W.; Speechley, M.; Wells, J.; Borrie, M.; Gopaul, K.; Montero-Odasso, M. Gait assessment in mild cognitive impairment and Alzheimer’s disease: The effect of dual-task challenges across the cognitive spectrum. Gait Posture 2012, 35, 96–100. [Google Scholar] [CrossRef]
- Furtado, S.; Godfrey, A.; Del Din, S.; Rochester, L.; Gerrand, C. Are Accelerometer-based Functional Outcome Assessments Feasible and Valid After Treatment for Lower Extremity Sarcomas? Clin Orthop. Relat. Res. 2020, 478, 482–503. [Google Scholar] [CrossRef]
- Zhang, P.; Schmidt, D.C.; White, J.; Lenz, G. Blockchain Technology Use Cases in Healthcare. In Advances in Computers; Elsevier: Amsterdam, The Netherlands, 2018; Volume 111, pp. 1–41. [Google Scholar]
- Espay, A.; Dwivedi, A.; Payne, M.; Gaines, L.; Vaughan, J.; Maddux, B.; Slevin, J.; Gartner, M.; Sahay, A.; Revilla, F. Methylphenidate for gait impairment in Parkinson disease: A randomized clinical trial. Neurology 2011, 76, 1256–1262. [Google Scholar] [CrossRef]
- Celesti, A.; Lay-Ekuakille, A.; Wan, J.; Fazio, M.; Celesti, F.; Romano, A.; Bramanti, P.; Villari, M. Information management in IoT cloud-based tele-rehabilitation as a service for smart cities: Comparison of NoSQL approaches. Measurement 2020, 151, 107218. [Google Scholar] [CrossRef]
- Martins, P.; Abbasi, M.; Sá, F. A Study over NoSQL Performance. In New Knowledge in Information Systems and Technologies; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 603–611. [Google Scholar]
- Alharam, A.K.; El-madany, W. Complexity of cyber security architecture for IoT healthcare industry: A comparative study. In Proceedings of the 2017 5th international conference on future internet of things and cloud workshops (FiCloudW), Prague, Czech Republic, 21–23 August 2017; pp. 246–250. [Google Scholar]
- Chacko, A.; Hayajneh, T. Security and privacy issues with IoT in healthcare. EAI Endorsed Trans. Pervasive Health Technol. 2018, 4, e2. [Google Scholar] [CrossRef]
- Bhuiyan, M.N.; Rahman, M.M.; Billah, M.M.; Saha, D. Internet of things (IoT): A review of its enabling technologies in healthcare applications, standards protocols, security, and market opportunities. IEEE Internet Things J. 2021, 8, 10474–10498. [Google Scholar] [CrossRef]
- Khan, S.; Parkinson, S.; Grant, L.; Liu, N.; Mcguire, S. Biometric systems utilising health data from wearable devices: Applications and future challenges in computer security. ACM Comput. Surv. (CSUR) 2020, 53, 1–29. [Google Scholar] [CrossRef]
- Barua, A.; Al Alamin, M.A.; Hossain, M.S.; Hossain, E. Security and privacy threats for bluetooth low energy in iot and wearable devices: A comprehensive survey. IEEE Open J. Commun. Soc. 2022, 3, 251–281. [Google Scholar] [CrossRef]
- Awotunde, J.B.; Jimoh, R.G.; Folorunso, S.O.; Adeniyi, E.A.; Abiodun, K.M.; Banjo, O.O. Privacy and Security Concerns in IoT-based Healthcare Systems. In The Fusion of Internet of Things, Artificial Intelligence, and Cloud Computing in Health Care; Springer: Berlin/Heidelberg, Germany, 2021; pp. 105–134. [Google Scholar]
- Pataky, T.C.; Mu, T.; Bosch, K.; Rosenbaum, D.; Goulermas, J.Y. Gait recognition: Highly unique dynamic plantar pressure patterns among 104 individuals. J. R. Soc. Interface 2012, 9, 790–800. [Google Scholar] [CrossRef]
- Zhang, Y.; Huang, Y.; Wang, L.; Yu, S. A comprehensive study on gait biometrics using a joint CNN-based method. Pattern Recognit. 2019, 93, 228–236. [Google Scholar] [CrossRef]
- Baek, S.; Seo, S.-H.; Kim, S. Preserving patient’s anonymity for mobile healthcare system in IoT environment. Int. J. Distrib. Sens. Netw. 2016, 12, 2171642. [Google Scholar] [CrossRef]
- Masud, M.; Gaba, G.S.; Choudhary, K.; Hossain, M.S.; Alhamid, M.F.; Muhammad, G. Lightweight and anonymity-preserving user authentication scheme for IoT-based healthcare. IEEE Internet Things J. 2021, 9, 2649–2656. [Google Scholar] [CrossRef]
- Bhatia, T.; Verma, A.K.; Sharma, G. Towards a secure incremental proxy re-encryption for e-healthcare data sharing in mobile cloud computing. Concurr. Comput. Pract. Exp. 2020, 32, e5520. [Google Scholar] [CrossRef]
- Delgado-Santos, P.; Tolosana, R.; Guest, R.; Vera-Rodriguez, R.; Deravi, F.; Morales, A. GaitPrivacyON: Privacy-preserving mobile gait biometrics using unsupervised learning. Pattern Recognit. Lett. 2022, 161, 30–37. [Google Scholar] [CrossRef]
- Ravi, A.R.; Nair, R.R. Cybersecurity threats and solutions in the current ehealthcare environment: A situational analysis. Med.-Leg. Update 2019, 19, 141–144. [Google Scholar] [CrossRef]
- Azure. Azure Health Data Services. Available online: https://azure.microsoft.com/en-us/products/health-data-services (accessed on 19 January 2023).
- Bikias, T.; Iakovakis, D.; Hadjidimitriou, S.; Charisis, V.; Hadjileontiadis, L.J. DeepFoG: An IMU-based detection of freezing of gait episodes in Parkinson’s disease patients via deep learning. Front. Robot. AI 2021, 8, 537384. [Google Scholar] [CrossRef]
- Yelamarthi, K.; Aman, M.S.; Abdelgawad, A. An application-driven modular IoT architecture. Wirel. Commun. Mob. Comput. 2017, 2017, 1350929. [Google Scholar] [CrossRef]
- Aich, S.; Pradhan, P.M.; Park, J.; Sethi, N.; Vathsa, V.S.S.; Kim, H.-C. A validation study of freezing of gait (FoG) detection and machine-learning-based FoG prediction using estimated gait characteristics with a wearable accelerometer. Sensors 2018, 18, 3287. [Google Scholar] [CrossRef]
- Rehman, R.Z.U.; Del Din, S.; Shi, J.Q.; Galna, B.; Lord, S.; Yarnall, A.J.; Guan, Y.; Rochester, L. Comparison of walking protocols and gait assessment systems for machine learning-based classification of parkinson’s disease. Sensors 2019, 19, 5363. [Google Scholar] [CrossRef] [PubMed]
- Romijnders, R.; Warmerdam, E.; Hansen, C.; Schmidt, G.; Maetzler, W. A Deep Learning Approach for Gait Event Detection from a Single Shank-Worn IMU: Validation in Healthy and Neurological Cohorts. Sensors 2022, 22, 3859. [Google Scholar] [CrossRef]
- Etemadi, M.; Ghobaei-Arani, M.; Shahidinejad, A. A cost-efficient auto-scaling mechanism for IoT applications in fog computing environment: A deep learning-based approach. Clust. Comput. 2021, 24, 3277–3292. [Google Scholar] [CrossRef]
- Amin, J.; Ruthiraphong, P. Cloud-based Gait Analysis Using a Single IMU for Parkinson Disease. In Proceedings of the 2021 18th International Conference on Electrical Engineering/Electronics, Computer, Telecommunications and Information Technology (ECTI-CON), Chiang Mai, Thailand, 19–22 May 2021; pp. 1129–1132. [Google Scholar]
- Hu, B.H.; Krausz, N.E.; Hargrove, L.J. A novel method for bilateral gait segmentation using a single thigh-mounted depth sensor and IMU. In Proceedings of the 2018 7th IEEE International Conference on Biomedical Robotics and Biomechatronics (Biorob), Enschede, Netherlands, 26–29 August 2018; pp. 807–812. [Google Scholar]
- Yang, P.; Xie, L.; Wang, C.; Lu, S. IMU-Kinect: A motion sensor-based gait monitoring system for intelligent healthcare. In Proceedings of the Adjunct Proceedings of the 2019 ACM International Joint Conference on Pervasive and Ubiquitous Computing and Proceedings of the 2019 ACM International Symposium on Wearable Computers, New York, NY, USA, 9–13 September 2019; pp. 350–353. [Google Scholar]
- Lord, S.; Galna, B.; Verghese, J.; Coleman, S.; Burn, D.; Rochester, L. Independent domains of gait in older adults and associated motor and nonmotor attributes: Validation of a factor analysis approach. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2013, 68, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Iancu, I.; Iancu, B. Designing mobile technology for elderly. A theoretical overview. Technol. Forecast. Soc. Chang. 2020, 155, 119977. [Google Scholar] [CrossRef]
- Young, F.; Stuart, S.; McNicol, R.; Morris, R.; Downs, C.; Coleman, M.; Godfrey, A. Bespoke fuzzy logic design to automate a better understanding of running gait analysis. IEEE J. Biomed. Health Inform. 2022. [Google Scholar] [CrossRef] [PubMed]
- Moore, J.; Stuart, S.; Walker, R.; McMeekin, P.; Young, F.; Godfrey, A. Deep learning semantic segmentation for indoor terrain extraction: Toward better informing free-living wearable gait assessment. In Proceedings of the 2022 IEEE-EMBS International Conference on Wearable and Implantable Body Sensor Networks (BSN), Ioannina, Greece, 27–30 September 2022. [Google Scholar]
- Hundall, J.; Babu, B.A. Computer Vision and Abnormal Patient Gait Assessment a Comparison of Machine Learning Models. arXiv 2020, arXiv:2004.02810. [Google Scholar]
- Colantonio, S.; Coppini, G.; Giorgi, D.; Morales, M.-A.; Pascali, M.A. Computer Vision for Ambient Assisted Living: Monitoring Systems for Personalized Healthcare and Wellness that are Robust in the Real World and Accepted by Users, Carers, and Society. In Computer Vision for Assistive Healthcare; Elsevier: Amsterdam, The Netherlands, 2018; pp. 147–182. [Google Scholar]
- Yu, M.; Gong, L.; Kollias, S. Computer vision based fall detection by a convolutional neural network. In Proceedings of the 19th ACM International Conference on Multimodal Interaction, Glasgow, UK, 13–17 November 2017; pp. 416–420. [Google Scholar]
- Harrou, F.; Zerrouki, N.; Sun, Y.; Houacine, A. An integrated vision-based approach for efficient human fall detection in a home environment. IEEE Access 2019, 7, 114966–114974. [Google Scholar] [CrossRef]
- Young, F.; Mason, R.; Morris, R.; Stuart, S.; Godfrey, A. Internet-of-Things-Enabled Markerless Running Gait Assessment from a Single Smartphone Camera. Sensors 2023, 23, 696. [Google Scholar] [CrossRef] [PubMed]
- Essmaeel, K.; Migniot, C.; Dipanda, A.; Gallo, L.; Damiani, E.; De Pietro, G. A new 3D descriptor for human classification: Application for human detection in a multi-kinect system. Multimed. Tools Appl. 2019, 78, 22479–22508. [Google Scholar] [CrossRef]
- Springer, S.; Yogev Seligmann, G. Validity of the kinect for gait assessment: A focused review. Sensors 2016, 16, 194. [Google Scholar] [CrossRef]
- Murshed, M.S.; Verenich, E.; Carroll, J.J.; Khan, N.; Hussain, F. Hazard detection in supermarkets using deep learning on the edge. arXiv 2020, arXiv:2003.04116. [Google Scholar]
- Caraiman, S.; Morar, A.; Owczarek, M.; Burlacu, A.; Rzeszotarski, D.; Botezatu, N.; Herghelegiu, P.; Moldoveanu, F.; Strumillo, P.; Moldoveanu, A. Computer vision for the visually impaired: The sound of vision system. In Proceedings of the IEEE International Conference on Computer Vision Workshops, Venice, Italy, 22–29 October 2017; pp. 1480–1489. [Google Scholar]
- Zhang, S.; Wei, Z.; Nie, J.; Huang, L.; Wang, S.; Li, Z. A review on human activity recognition using vision-based method. J. Healthc. Eng. 2017, 2017, 3090343. [Google Scholar] [CrossRef] [PubMed]
- Long, N.; Wang, K.; Cheng, R.; Hu, W.; Yang, K. Unifying obstacle detection, recognition, and fusion based on millimeter wave radar and RGB-depth sensors for the visually impaired. Rev. Sci. Instrum. 2019, 90, 044102. [Google Scholar] [CrossRef] [PubMed]
- Cao, Z.; Hidalgo, G.; Simon, T.; Wei, S.-E.; Sheikh, Y. OpenPose: Realtime multi-person 2D pose estimation using Part Affinity Fields. IEEE Trans. Pattern Anal. Mach. Intell. 2019, 43, 172–186. [Google Scholar] [CrossRef] [PubMed]
- Torresen, J. A Robust Human Activity Recognition Approach Using OpenPose, Motion Features, and Deep Recurrent Neural Network. In Proceedings of the Image Analysis: 21st Scandinavian Conference, SCIA 2019, Norrköping, Sweden, 11–13 June 2019; p. 299. [Google Scholar]
- Riaz, H.; Uzair, M.; Ullah, H.; Ullah, M. Anomalous human action detection using a cascade of deep learning models. In Proceedings of the 2021 9th European Workshop on Visual Information Processing (EUVIP), Paris, France, 23–25 June 2021; pp. 1–5. [Google Scholar]
- Chen, W.; Jiang, Z.; Guo, H.; Ni, X. Fall detection based on key points of human-skeleton using openpose. Symmetry 2020, 12, 744. [Google Scholar] [CrossRef]
- Viswakumar, A.; Rajagopalan, V.; Ray, T.; Parimi, C. Human Gait Analysis Using OpenPose. In Proceedings of the 2019 Fifth International Conference on Image Information Processing (ICIIP), Shimla, India, 15–17 November 2019; pp. 310–314. [Google Scholar]
- Cleland, B.T.; Arshad, H.; Madhavan, S. Concurrent validity of the GAITRite electronic walkway and the 10-m walk test for measurement of walking speed after stroke. Gait Posture 2019, 68, 458–460. [Google Scholar] [CrossRef]
- Calvache, D.A.; Bernal, H.A.; Guarín, J.F.; Aguía, K.; Orjuela-Cañón, A.D.; Perdomo, O.J. Automatic estimation of pose and falls in videos using computer vision model. In Proceedings of the 16th International Symposium on Medical Information Processing and Analysis, Lima, Peru, 3–4 October 2020; p. 115830W. [Google Scholar]
- Eloy, S.; Dias, L.; Ourique, L.; Dias, M.S. Home mobility hazards detected via object recognition in augmented reality. In Proceedings of the 37th eCAADe and 23rd SIGraDi Conference, Porto, Portugal, 11–13 September 2019; pp. 415–422. [Google Scholar]
- Esteva, A.; Chou, K.; Yeung, S.; Naik, N.; Madani, A.; Mottaghi, A.; Liu, Y.; Topol, E.; Dean, J.; Socher, R. Deep learning-enabled medical computer vision. NPJ Digit. Med. 2021, 4, 5. [Google Scholar] [CrossRef]
- Mihailidis, A.; Carmichael, B.; Boger, J. The use of computer vision in an intelligent environment to support aging-in-place, safety, and independence in the home. IEEE Trans. Inf. Technol. Biomed. 2004, 8, 238–247. [Google Scholar] [CrossRef]
- Leo, M.; Medioni, G.; Trivedi, M.; Kanade, T.; Farinella, G.M. Computer vision for assistive technologies. Comput. Vis. Image Underst. 2017, 154, 1–15. [Google Scholar] [CrossRef]
- Lemonnier, N. Ethical Issues Using Artificial Intelligence in Healthcare. 2021. Available online: https://jyx.jyu.fi/bitstream/handle/123456789/75832/URN%3aNBN%3afi%3ajyu-202105213093.pdf?sequence=1&isAllowed=y (accessed on 23 January 2023).
- Blank, A.L. Computer Vision Machine Learning and Future-Oriented Ethics. 2019. Available online: https://digitalcommons.spu.edu/honorsprojects/107/ (accessed on 12 December 2022).
- Senior, A.; Pankanti, S.; Hampapur, A.; Brown, L.; Tian, Y.-L.; Ekin, A.; Connell, J.; Shu, C.F.; Lu, M. Enabling video privacy through computer vision. IEEE Secur. Priv. 2005, 3, 50–57. [Google Scholar] [CrossRef]
- Vishwamitra, N.; Knijnenburg, B.; Hu, H.; Kelly Caine, Y.P. Blur vs. block: Investigating the effectiveness of privacy-enhancing obfuscation for images. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition Workshops, Honolulu, HI, USA, 21–26 July 2017; pp. 39–47. [Google Scholar]
- Li, J.; Han, L.; Chen, R.; Zhang, H.; Han, B.; Wang, L.; Cao, X. Identity-preserving face anonymization via adaptively facial attributes obfuscation. In Proceedings of the Proceedings of the 29th ACM International Conference on Multimedia, Virtual, 20–24 October 2021; pp. 3891–3899. [Google Scholar]
- Moore, J.; Stuart, S.; McMeekin, P.; Walker, R.; Celik, Y.; Pointon, M.; Godfrey, A. Enhancing Free-Living Fall Risk Assessment: Contextualizing Mobility Based IMU Data. Sensors 2023, 23, 891. [Google Scholar] [CrossRef]
- Langheinrich, M. Privacy by design—Principles of privacy-aware ubiquitous systems. In Proceedings of the International conference on Ubiquitous Computing, Atlanta, GA, USA, 30 September–2 October 2001; pp. 273–291. [Google Scholar]
- Lim, H.; Kim, B.; Park, S. Prediction of lower limb kinetics and kinematics during walking by a single IMU on the lower back using machine learning. Sensors 2019, 20, 130. [Google Scholar] [CrossRef] [PubMed]
- Portuese, E.; Buscaglione, S.; Formica, D.; Lanaro, D. Assessment of running training sessions using IMU sensors: Evaluation of existing parameters and choice of new indicators. In Proceedings of the 2020 IEEE International Workshop on Metrology for Industry 4.0 & IoT, Roma, Italy, 3–5 June 2020; pp. 121–124. [Google Scholar]
- Panero, E.; Digo, E.; Dimanico, U.; Artusi, C.A.; Zibetti, M.; Gastaldi, L. Effect of Deep Brain Stimulation Frequency on Gait Symmetry, Smoothness and Variability using IMU. In Proceedings of the 2021 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Lausanne, Switzerland, 23–25 June 2021; pp. 1–6. [Google Scholar]
- Perez-Ibarra, J.C.; Siqueira, A.A.; Krebs, H.I. Real-time identification of gait events in impaired subjects using a single-IMU foot-mounted device. IEEE Sens. J. 2019, 20, 2616–2624. [Google Scholar] [CrossRef]
- Hwang, T.-H.; Reh, J.; Effenberg, A.O.; Blume, H. Validation of Real Time Gait Analysis Using a Single Head-Worn IMU. In Proceedings of the Europe-Korea Conference on Science and Technology, Vienna, Austria, 15–19 July 2019; pp. 87–97. [Google Scholar]
- Zoetewei, D.; Herman, T.; Brozgol, M.; Ginis, P.; Thumm, P.C.; Ceulemans, E.; Decaluwé, E.; Palmerini, L.; Ferrari, A.; Nieuwboer, A. Protocol for the DeFOG trial: A randomized controlled trial on the effects of smartphone-based, on-demand cueing for freezing of gait in Parkinson’s disease. Contemp. Clin. Trials Commun. 2021, 24, 100817. [Google Scholar] [CrossRef] [PubMed]
- Ren, L.; Peng, Y. Research of fall detection and fall prevention technologies: A systematic review. IEEE Access 2019, 7, 77702–77722. [Google Scholar] [CrossRef]
- Tao, W.; Liu, T.; Zheng, R.; Feng, H. Gait analysis using wearable sensors. Sensors 2012, 12, 2255–2283. [Google Scholar] [CrossRef]
- Kunda, D.; Phiri, H. A comparative study of nosql and relational database. Zamb. ICT J. 2017, 1, 1–4. [Google Scholar] [CrossRef]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Young, F.; Mason, R.; Morris, R.E.; Stuart, S.; Godfrey, A. IoT-Enabled Gait Assessment: The Next Step for Habitual Monitoring. Sensors 2023, 23, 4100. https://doi.org/10.3390/s23084100
Young F, Mason R, Morris RE, Stuart S, Godfrey A. IoT-Enabled Gait Assessment: The Next Step for Habitual Monitoring. Sensors. 2023; 23(8):4100. https://doi.org/10.3390/s23084100
Chicago/Turabian StyleYoung, Fraser, Rachel Mason, Rosie E. Morris, Samuel Stuart, and Alan Godfrey. 2023. "IoT-Enabled Gait Assessment: The Next Step for Habitual Monitoring" Sensors 23, no. 8: 4100. https://doi.org/10.3390/s23084100