

Dynamic Analysis of the Coracohumeral Ligament Using Ultra-Sonography in Shoulder Contracture

 , , ,
, , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Population
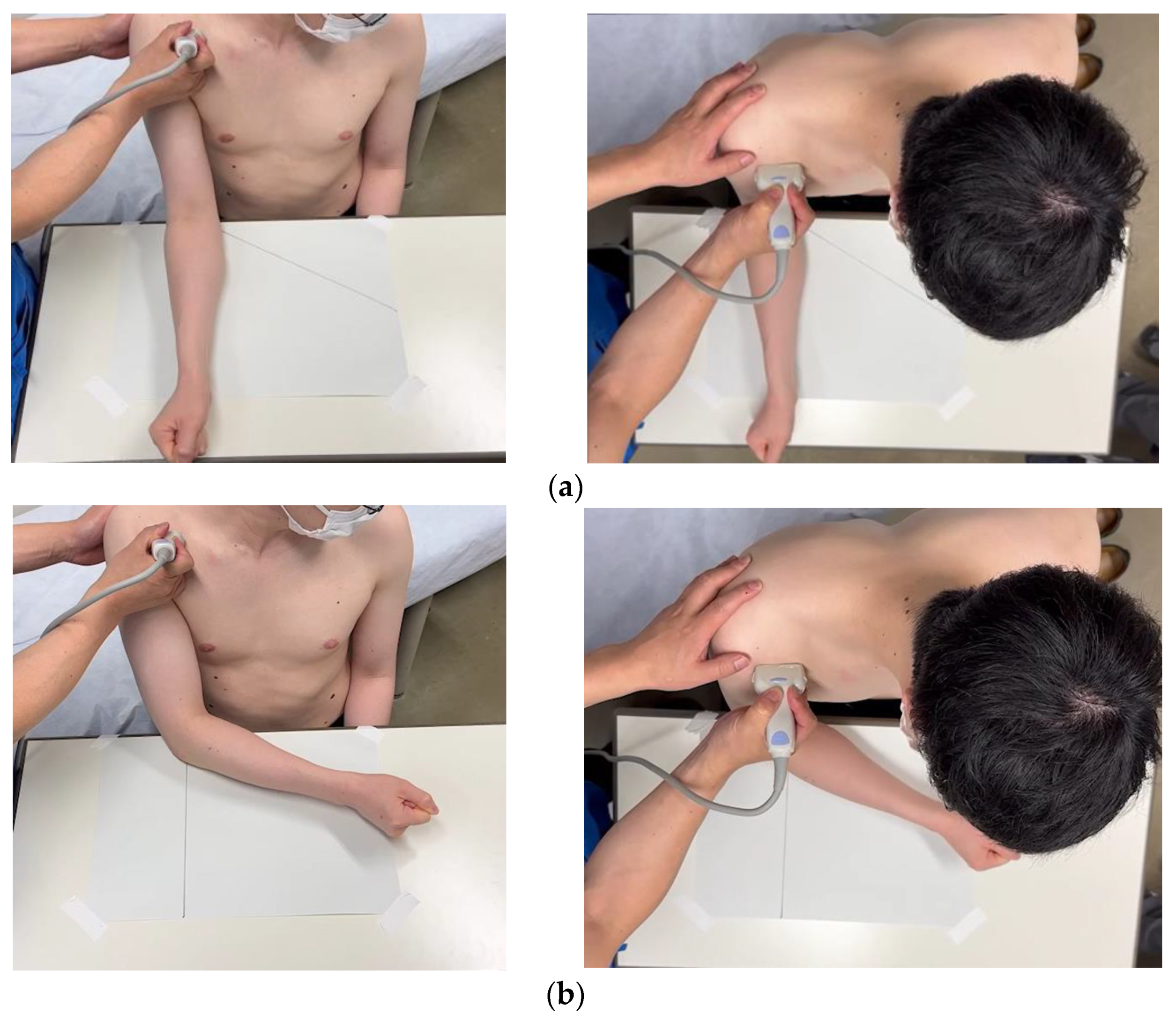
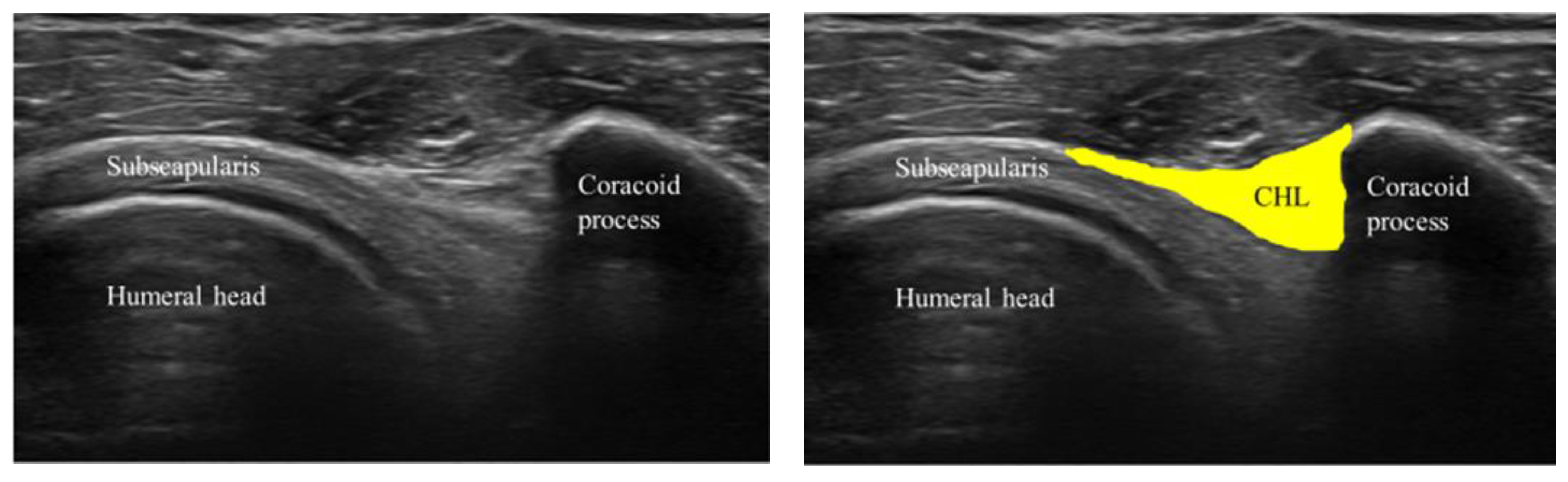
2.2. Experimental Data Acquisition and Analysis
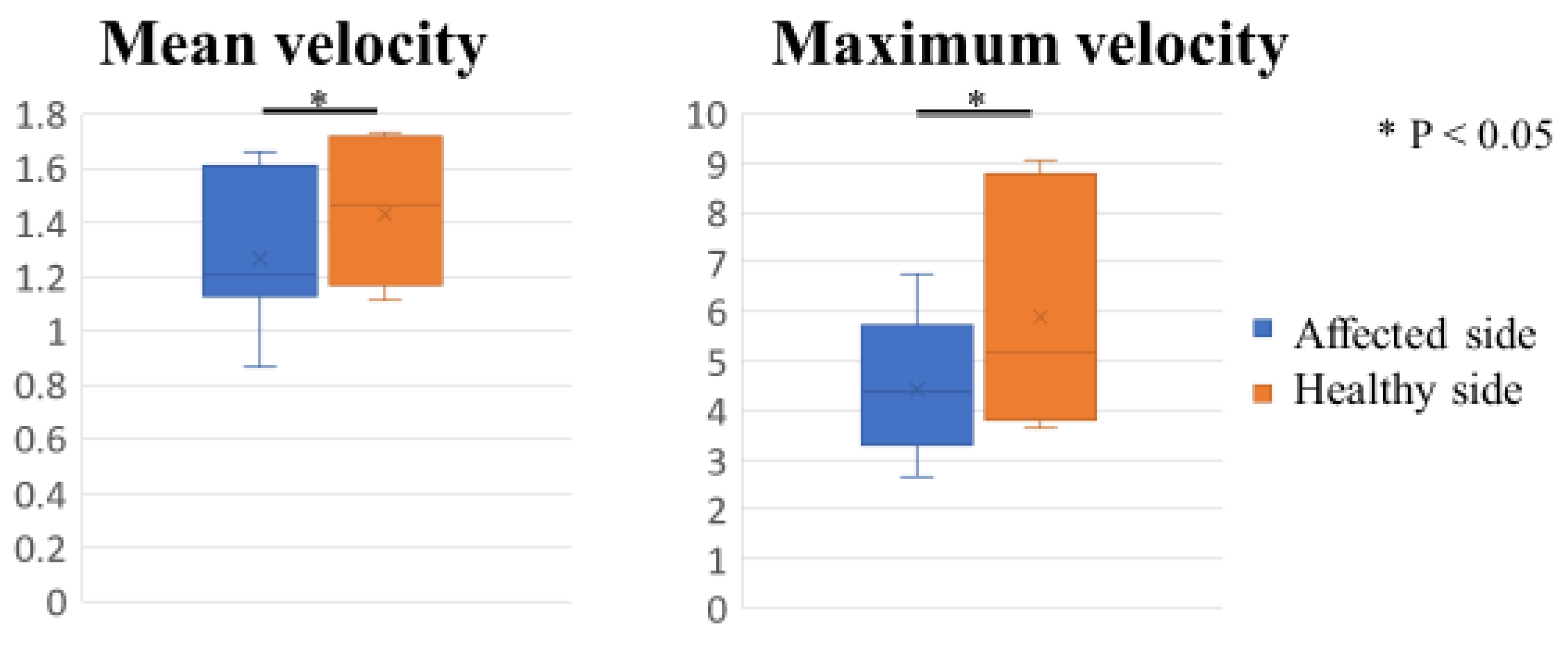
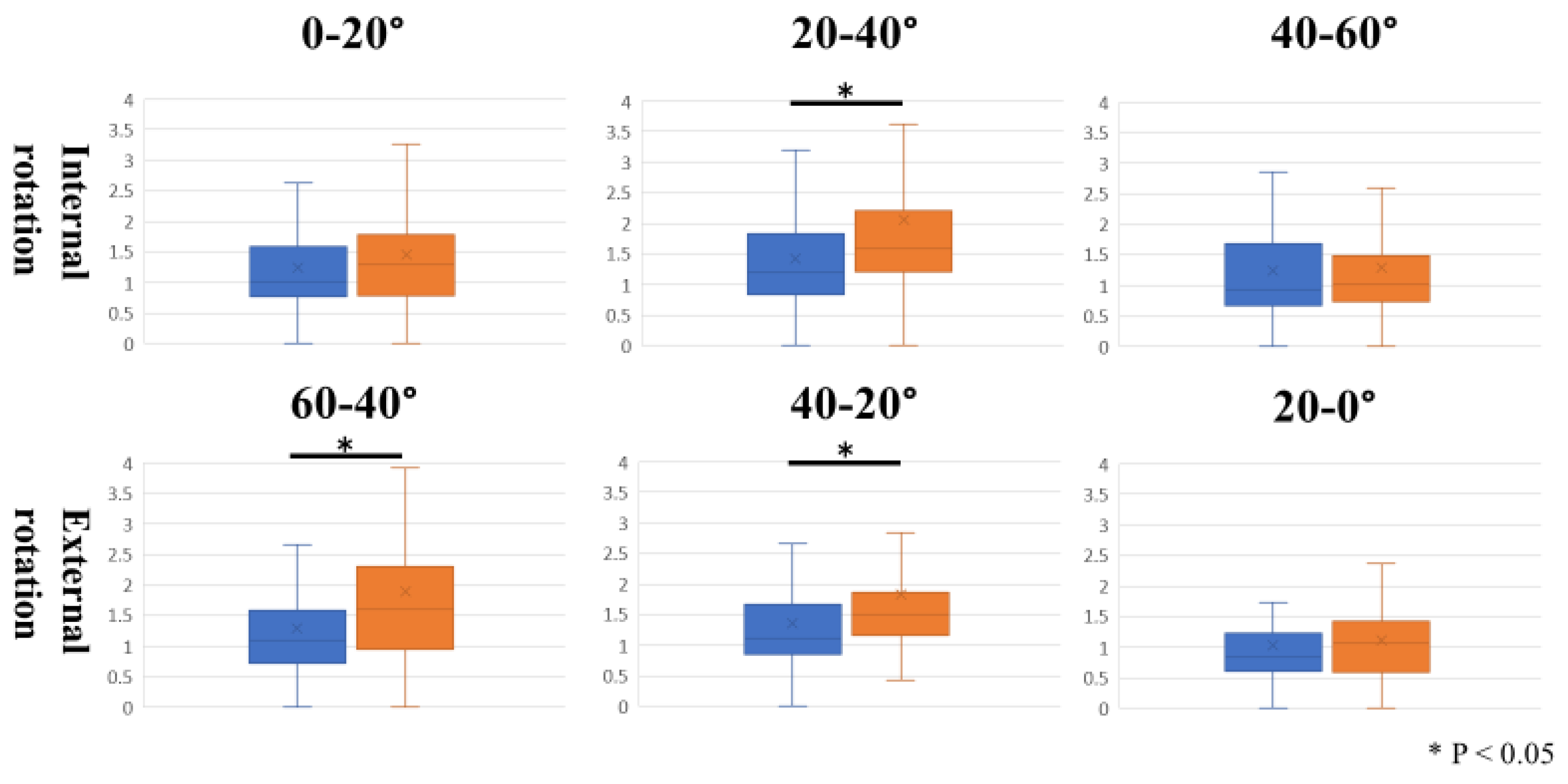
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Brand, R.A. Recurrent dislocation of the shoulder joint. Clin Orthop Relat Res. 2008, 466, 520–530. [Google Scholar] [CrossRef] [Green Version]
- Ricci, V.; Mezian, K.; Naňka, O.; Özçakar, L. Assessing/Imaging the Subcoracoid Space: From Anatomy to Dynamic So-nography. J. Ultrasound Med. 2022, 41, 2149–2155. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.-F.; Tang, K.-L.; Chen, W.; Dong, S.-W.; Jin, T.; Gong, J.-C.; Li, J.-Q.; Wang, H.-Q.; Wang, J.; Xu, J. An anatomic and histologic study of the coracohumeral ligament. J. Shoulder Elb. Surg. 2009, 18, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Boardman, N.D.; Debski, R.E.; Warner, J.J.; Taskiran, E.; Maddox, L.; Imhoff, A.B.; Fu, F.H.; Woo, S.L.-Y. Tensile properties of the superior glenohumeral and coracohumeral ligaments. J. Shoulder Elb. Surg. 1996, 5, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Izumi, T.; Aoki, M.; Tanaka, Y.; Uchiyama, E.; Suzuki, D.; Miyamoto, S.; Fujimiya, M. Stretching positions for the coracohumeral ligament: Strain measurement during passive motion using fresh/frozen cadaver shoulders. BMC Sports Sci. Med. Rehabil. 2011, 3, 2–11. [Google Scholar] [CrossRef] [Green Version]
- Arai, R.; Nimura, A.; Yamaguchi, K.; Yoshimura, H.; Sugaya, H.; Saji, T.; Matsuda, S.; Akita, K. The anatomy of the coracohumeral ligament and its relation to the subscapularis muscle. J. Shoulder Elb. Surg. 2014, 23, 1575–1581. [Google Scholar] [CrossRef]
- Kelley, M.J.; Shaffer, M.A.; Kuhn, J.E.; Michener, L.A.; Seitz, A.L.; Uhl, T.L.; Godges, J.J.; McClure, P.W. Shoulder Pain and Mobility Deficits: Adhesive Capsulitis: Clinical Practice Guidelines Linked to the International Classification of Functioning, Disability, and Health from the Orthopaedic Section of the American Physical Therapy Association. J. Orthop. Sports Phys. Ther. 2013, 43, A1–A31. [Google Scholar] [CrossRef] [Green Version]
- Ozaki, J.; Nakagawa, Y.; Sakurai, G.; Tamai, S. Recalcitrant chronic adhesive capsulitis of the shoulder. Role of contracture of the coracohumeral ligament and rotator interval in pathogenesis and treatment. J. Bone Joint Surg. Am. 1989, 71, 1511–1515. [Google Scholar] [CrossRef]
- De Baets, L.; Matheve, T.; Dierickx, C.; Bijnens, E.; Jans, D.; Timmermans, A. Are clinical outcomes of frozen shoulder linked to pain, structural factors or pain-related cognitions? An explorative cohort study. Musculoskelet. Sci. Pract. 2020, 50, 102270. [Google Scholar] [CrossRef]
- Kanazawa, K.; Hagiwara, Y.; Sekiguchi, T.; Fujita, R.; Suzuki, K.; Koide, M.; Ando, A.; Yabe, Y. Correlations Between Range of Motion and Elasticity of the Coracohumeral Ligament Evaluated with Shear-Wave Elastography. J. Sport Rehabil. 2021, 30, 9–15. [Google Scholar] [CrossRef] [Green Version]
- Medero, R.; Falk, K.; Rutkowski, D.; Johnson, K.; Roldán-Alzate, A. In Vitro Assessment of Flow Variability in an Intracranial Aneurysm Model Using 4D Flow MRI and Tomographic PIV. Ann. Biomed. Eng. 2020, 48, 2484–2493. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Dong, J.; Tian, L.; Inthavong, K.; Tu, J. Numerical and Experimental Analysis of Inhalation Airflow Dynamics in a Human Pharyngeal Airway. Int. J. Environ. Res. Public Health 2020, 17, 1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawanishi, K.; Kudo, S.; Yokoi, K. Relationship Between Gliding and Lateral Femoral Pain in Patients with Trochanteric Fracture. Arch. Phys. Med. Rehabil. 2019, 101, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Shinohara, I.; Inui, A.; Mifune, Y.; Nishimoto, H.; Yamaura, K.; Mukohara, S.; Yoshikawa, T.; Kato, T.; Furukawa, T.; Hoshino, Y.; et al. Motion Analysis of Triangular Fibrocartilage Complex by Using Ultrasonography Images: Preliminary Analysis. Sensors 2022, 22, 345. [Google Scholar] [CrossRef]
- Tanaka, S.; Inui, A.; Mifune, Y.; Nishimoto, H.; Yoshikawa, T.; Shinohara, I.; Furukawa, T.; Kato, T.; Kusunose, M.; Kuroda, R. Motion Analysis of the Extensor Carpi Ulnaris in Triangular Fibrocartilage Complex Injury Using Ultrasonography Images. Sensors 2022, 22, 8216. [Google Scholar] [CrossRef]
- Kim, Y.-S.; Kim, J.-M.; Bigliani, L.U.; Kim, H.-J.; Jung, H.-W. In vivo strain analysis of the intact supraspinatus tendon by ultrasound speckles tracking imaging. J. Orthop. Res. 2011, 29, 1931–1937. [Google Scholar] [CrossRef]
- Shinohara, I.; Mifune, Y.; Inui, A.; Nishimoto, H.; Yamaura, K.; Mukohara, S.; Yoshikawa, T.; Kato, T.; Furukawa, T.; Hoshino, Y.; et al. Advanced glycation end products are associated with limited range of motion of the shoulder joint in patients with rotator cuff tears associated with diabetes mellitus. BMC Musculoskelet. Disord. 2022, 23, 1–10. [Google Scholar] [CrossRef]
- Do, J.G.; Hwang, J.T.; Yoon, K.J.; Lee, Y.-T. Correlation of Ultrasound Findings with Clinical Stages and Impairment in Adhesive Capsulitis of the Shoulder. Orthop. J. Sports Med. 2021, 9, 23259671211003675. [Google Scholar] [CrossRef]
- Kanazawa, K.; Hagiwara, Y.; Kawai, N.; Sekiguchi, T.; Koide, M.; Ando, A.; Sugaya, H.; Itoi, E. Correlations of coracohumeral ligament and range of motion restriction in patients with recurrent anterior glenohumeral instability evaluated by magnetic resonance arthrography. J. Shoulder Elb. Surg. 2016, 26, 233–240. [Google Scholar] [CrossRef]
- Park, J.H.; Yang, S.H.; Rhee, S.M.; Oh, J.H. The effect of concomitant coracohumeral ligament release in arthroscopic rotator cuff repair to prevent postoperative stiffness: A retrospective comparative study. Knee Surg. Sport. Traumatol. Arthrosc. 2019, 27, 3881–3889. [Google Scholar] [CrossRef]
- Yukata, K.; Goto, T.; Sakai, T.; Fujii, H.; Hamawaki, J.; Yasui, N. Ultrasound-guided coracohumeral ligament release. Orthop. Traumatol. Surg. Res. 2018, 104, 823–827. [Google Scholar] [CrossRef] [PubMed]
- Koide, M.; Hamada, J.; Hagiwara, Y.; Kanazawa, K.; Suzuki, K. A Thickened Coracohumeral Ligament and Superomedial Capsule Limit Internal Rotation of the Shoulder Joint: Report of Three Cases. Case Rep. Orthop. 2016, 2016, 9384974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tandon, A.; Dewan, S.; Bhatt, S.; Jain, A.K.; Kumari, R. Sonography in diagnosis of adhesive capsulitis of the shoulder: A case–control study. J. Ultrasound 2017, 20, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Suda, M.; Kobayashi, T.; Suzuki, S.; Fukui, S.; Obata, H. Effectiveness of ultrasound-guided fascia hydrorelease on the coracohumeral ligament in patients with global limitation of the shoulder range of motion: A pilot study. Sci. Rep. 2022, 12, 19782. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kato, T.; Inui, A.; Mifune, Y.; Nishimoto, H.; Yoshikawa, T.; Shinohara, I.; Furukawa, T.; Tanaka, S.; Kusunose, M.; Kuroda, R. Dynamic Analysis of the Coracohumeral Ligament Using Ultra-Sonography in Shoulder Contracture. Sensors 2023, 23, 4015. https://doi.org/10.3390/s23084015
Kato T, Inui A, Mifune Y, Nishimoto H, Yoshikawa T, Shinohara I, Furukawa T, Tanaka S, Kusunose M, Kuroda R. Dynamic Analysis of the Coracohumeral Ligament Using Ultra-Sonography in Shoulder Contracture. Sensors. 2023; 23(8):4015. https://doi.org/10.3390/s23084015
Chicago/Turabian StyleKato, Tatsuo, Atsuyuki Inui, Yutaka Mifune, Hanako Nishimoto, Tomoya Yoshikawa, Issei Shinohara, Takahiro Furukawa, Shuya Tanaka, Masaya Kusunose, and Ryosuke Kuroda. 2023. "Dynamic Analysis of the Coracohumeral Ligament Using Ultra-Sonography in Shoulder Contracture" Sensors 23, no. 8: 4015. https://doi.org/10.3390/s23084015