
The Validity of Ultra-Short-Term Heart Rate Variability during Cycling Exercise

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
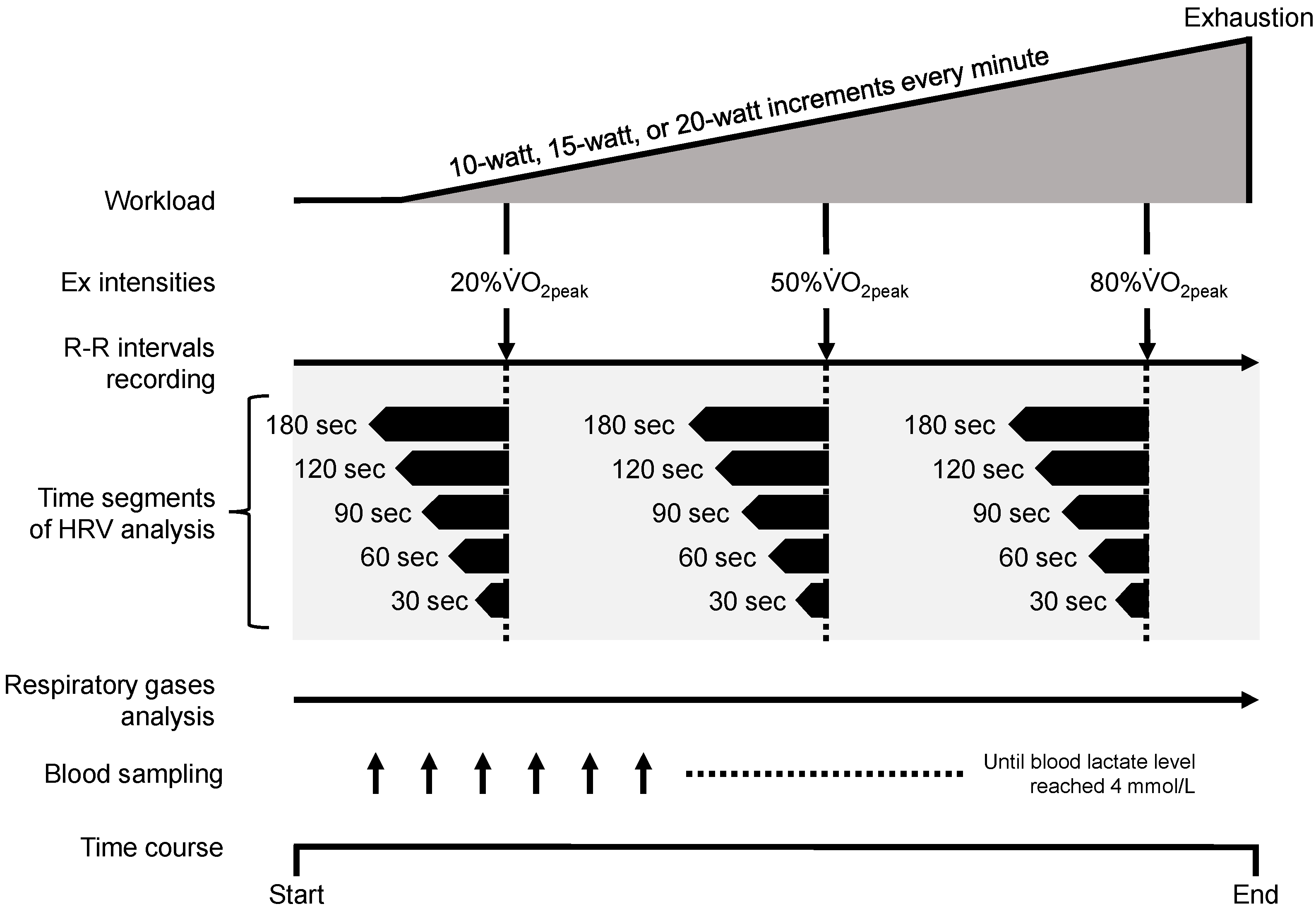
2.1. Research Methodology
2.2. Participants
2.3. Ethical Statements
2.4. The Cycling Exercise Test Procedure
2.5. Physiological Parameter Measurements
2.6. Heart Rate Variability Analysis
2.7. Additional Data Handling
2.8. Missing Data
2.9. Statistical Analysis
3. Results
3.1. Changes in Physiological Parameters during Exercise
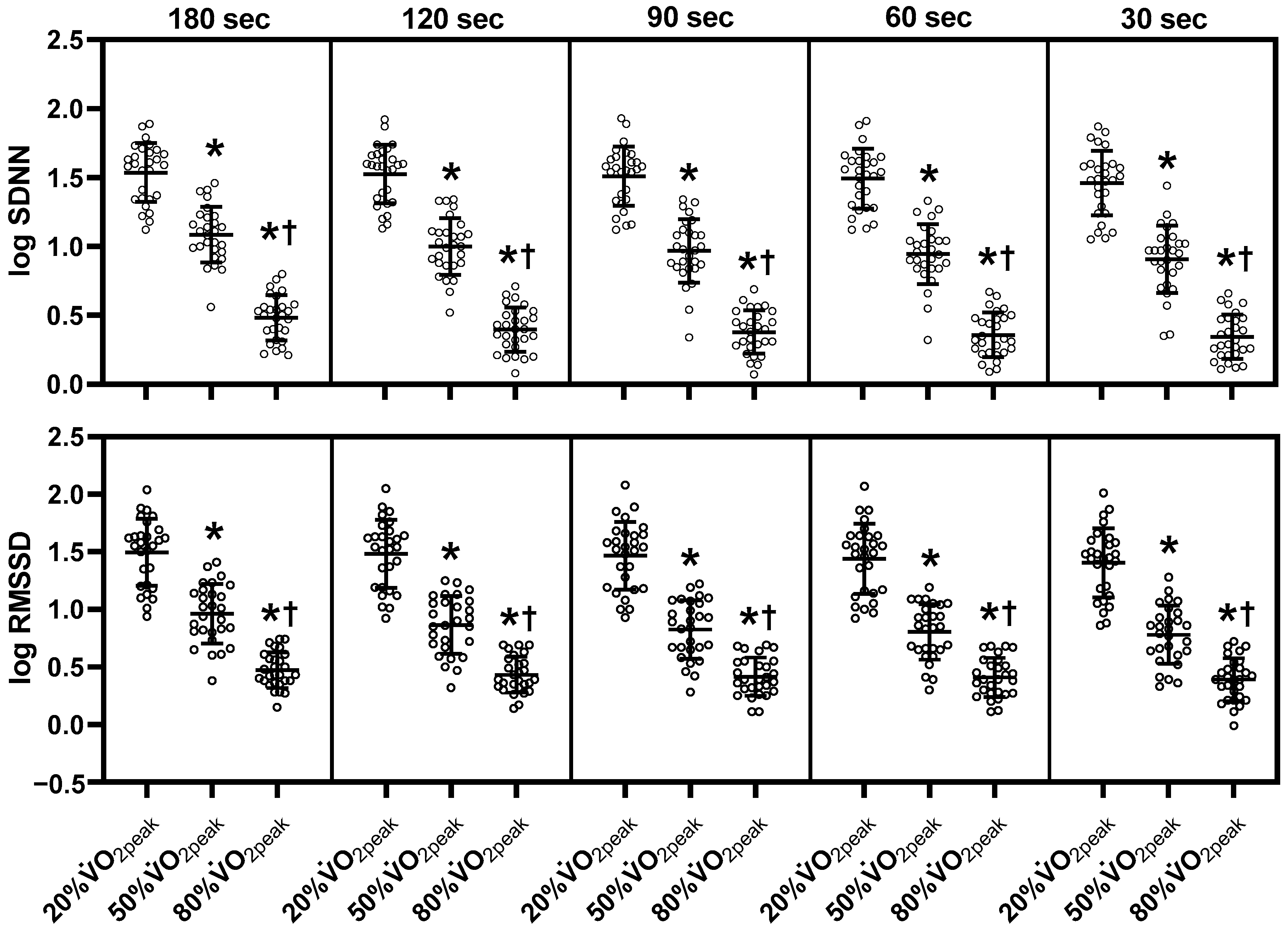
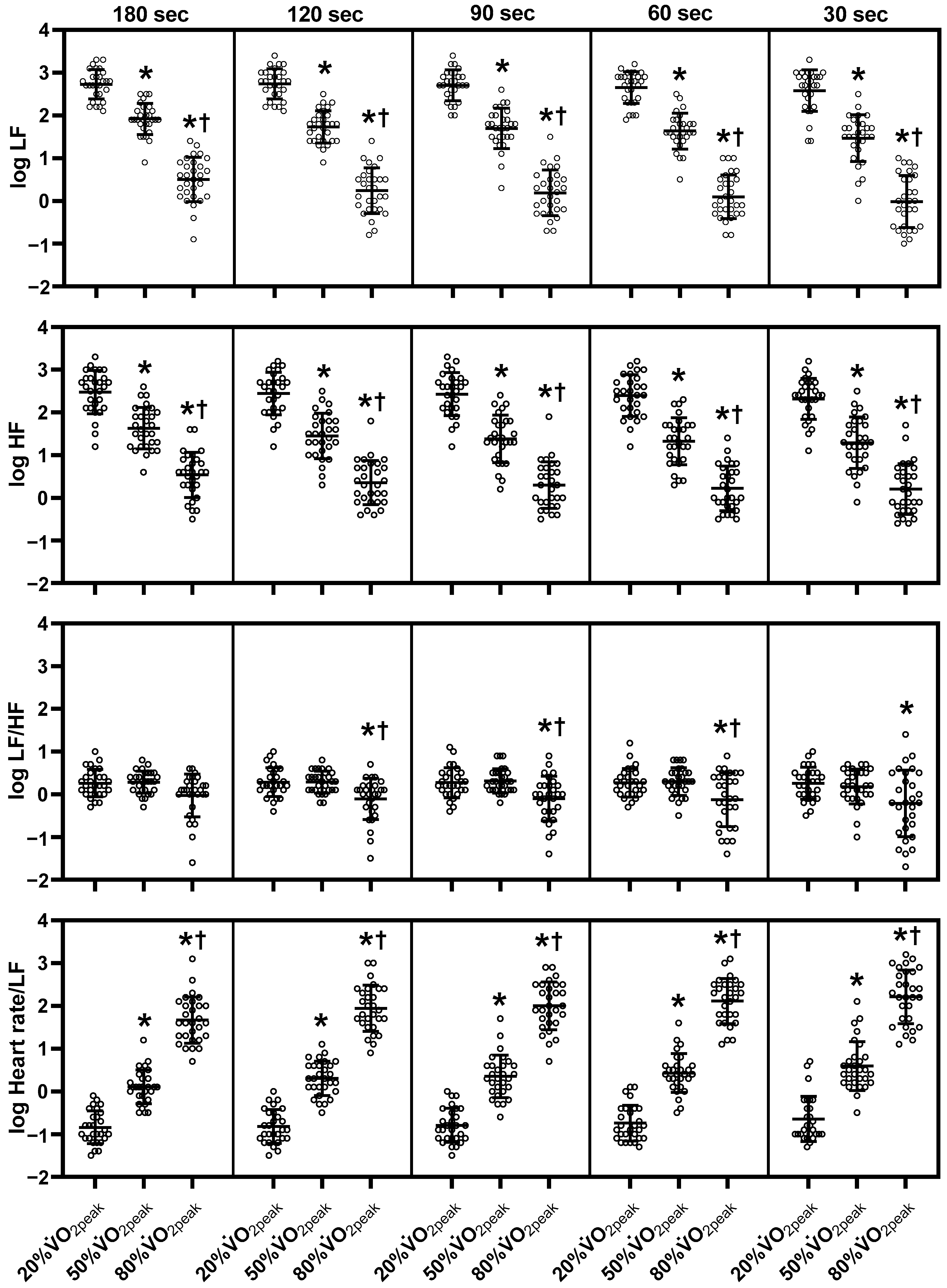
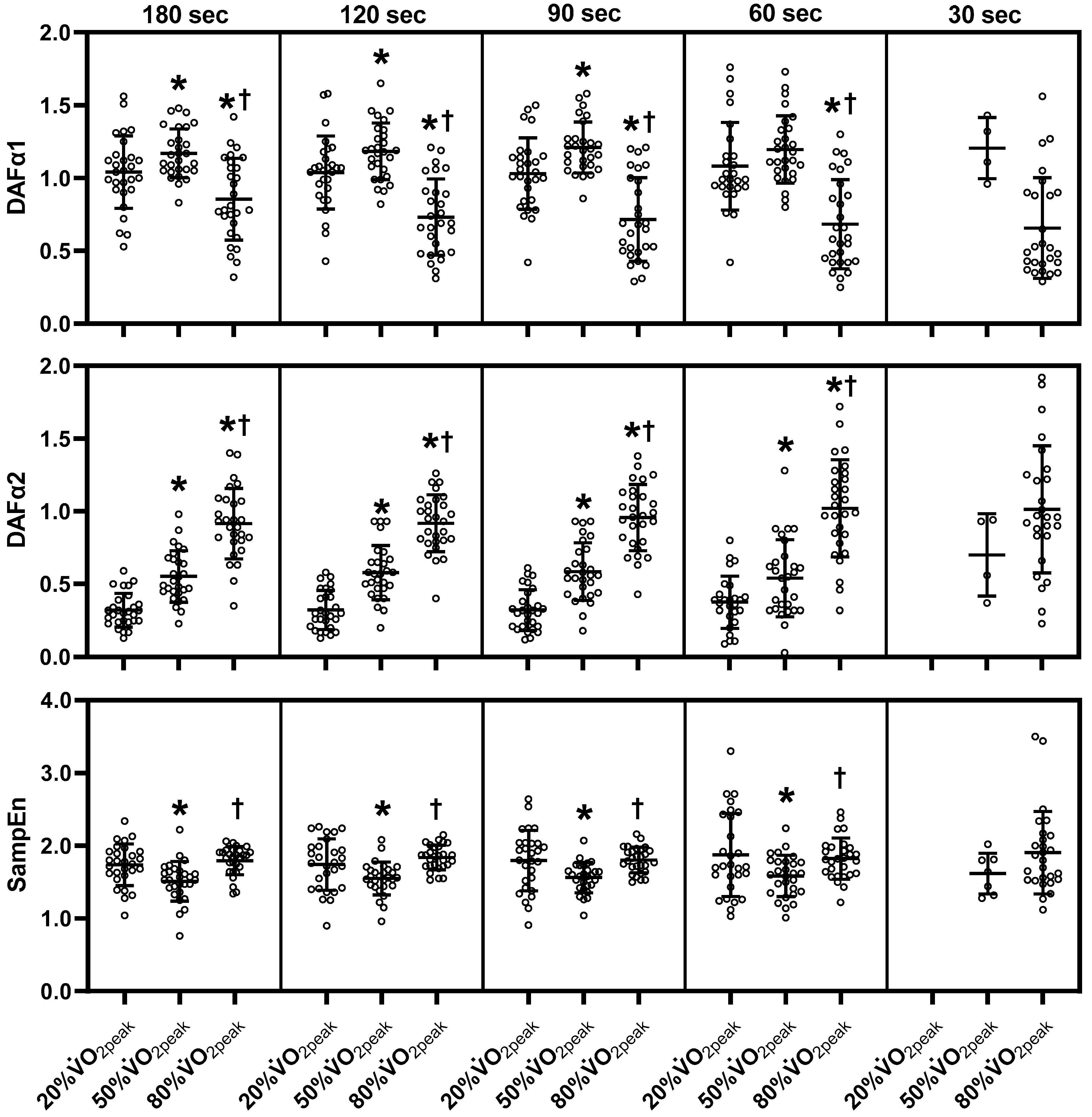
3.2. The Mean HRV Values Change during Exercise
3.3. The Correlation Coefficient
3.4. The Bias and LOA from the Different Time Segments of the HRV Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Billman, G.E. Heart rate variability—A historical perspective. Front. Physiol. 2011, 2, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, V.N.; Pierce, B.R.; Bodapati, R.K.; Brown, D.L.; Ives, D.G.; Stein, P.K. Association of Holter-Derived Heart Rate Variability Parameters with the Development of Congestive Heart Failure in the Cardiovascular Health Study. JACC Heart Fail. 2017, 5, 423–431. [Google Scholar] [CrossRef] [PubMed]
- Jarczok, M.N.; Weimer, K.; Braun, C.; William, D.P.; Thayer, J.F.; Gündel, H.O.; Balint, E.M. Heart rate variability in the prediction of mortality: A systematic review and meta-analysis of healthy and patient populations. Neurosci. Biobehav. Rev. 2022, 143, 104907. [Google Scholar] [CrossRef]
- Brown, L.; Karmakar, C.; Gray, R.; Jindal, R.; Lim, T.; Bryant, C. Heart rate variability alterations in late life depression: A meta-analysis. J. Affect. Disord. 2018, 235, 456–466. [Google Scholar] [CrossRef]
- Stephenson, M.D.; Thompson, A.G.; Merrigan, J.J.; Stone, J.D.; Hagen, J.A. Applying Heart Rate Variability to Monitor Health and Performance in Tactical Personnel: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 8143. [Google Scholar] [CrossRef]
- Altini, M.; Plews, D. What Is behind Changes in Resting Heart Rate and Heart Rate Variability? A Large-Scale Analysis of Longitudinal Measurements Acquired in Free-Living. Sensors 2021, 21, 7932. [Google Scholar] [CrossRef]
- Kiviniemi, A.M.; Hautala, A.J.; Kinnunen, H.; Tulppo, M.P. Endurance training guided individually by daily heart rate variability measurements. Eur. J. Appl. Physiol. 2007, 101, 743–751. [Google Scholar] [CrossRef]
- Muñoz-López, A.; Naranjo-Orellana, J. Individual versus team heart rate variability responsiveness analyses in a national soccer team during training camps. Sci. Rep. 2020, 10, 11726. [Google Scholar] [CrossRef]
- Karapetian, G.K.; Engels, H.J.; Gretebeck, R.J. Use of heart rate variability to estimate LT and VT. Int. J. Sports Med. 2008, 29, 652–657. [Google Scholar] [CrossRef]
- Shiraishi, Y.; Katsumata, Y.; Sadahiro, T.; Azuma, K.; Akita, K.; Isobe, S.; Yashima, F.; Miyamoto, K.; Nishiyama, T.; Tamura, Y.; et al. Real-Time Analysis of the Heart Rate Variability During Incremental Exercise for the Detection of the Ventilatory Threshold. J. Am. Heart Assoc. 2018, 7, e006612. [Google Scholar] [CrossRef] [Green Version]
- Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Circulation 1996, 93, 1043–1065. [Google Scholar] [CrossRef] [Green Version]
- Berntson, G.G.; Bigger, J.T., Jr.; Eckberg, D.L.; Grossman, P.; Kaufmann, P.G.; Malik, M.; Nagaraja, H.N.; Porges, S.W.; Saul, J.P.; Stone, P.H.; et al. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology 1997, 34, 623–648. [Google Scholar] [CrossRef] [PubMed]
- Moak, J.P.; Goldstein, D.S.; Eldadah, B.A.; Saleem, A.; Holmes, C.; Pechnik, S.; Sharabi, Y. Supine low-frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation. Heart Rhythm 2007, 4, 1523–1529. [Google Scholar] [CrossRef]
- Rahman, F.; Pechnik, S.; Gross, D.; Sewell, L.; Goldstein, D.S. Low frequency power of heart rate variability reflects baroreflex function, not cardiac sympathetic innervation. Clin. Auton. Res. 2011, 21, 133–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martelli, D.; Silvani, A.; McAllen, R.M.; May, C.N.; Ramchandra, R. The low frequency power of heart rate variability is neither a measure of cardiac sympathetic tone nor of baroreflex sensitivity. Am. J. Physiol. Heart Circ. Physiol. 2014, 307, H1005-12. [Google Scholar] [CrossRef]
- Penttilä, J.; Helminen, A.; Jartti, T.; Kuusela, T.; Huikuri, H.V.; Tulppo, M.P.; Coffeng, R.; Scheinin, H. Time domain, geometrical and frequency domain analysis of cardiac vagal outflow: Effects of various respiratory patterns. Clin. Physiol. 2001, 21, 365–376. [Google Scholar] [CrossRef]
- Sassi, R.; Cerutti, S.; Lombardi, F.; Malik, M.; Huikuri, H.V.; Peng, C.K.; Schmidt, G.; Yamamoto, Y. Advances in heart rate variability signal analysis: Joint position statement by the e-Cardiology ESC Working Group and the European Heart Rhythm Association co-endorsed by the Asia Pacific Heart Rhythm Society. Europace 2015, 17, 1341–1353. [Google Scholar] [CrossRef]
- Costa, M.; Goldberger, A.L.; Peng, C.K. Multiscale entropy analysis of biological signals. Phys. Rev. E 2005, 71, 021906. [Google Scholar] [CrossRef] [Green Version]
- Abellan-Aynes, O.; Naranjo-Orellana, J.; Manonelles, P.; Alacid, F. Multiscale Entropy and Multiscale Time Irreversibility Analysis of Rr Time Series Depending on Ambient Temperature. J. Mech. Med. Biol. 2020, 20, 2050029. [Google Scholar] [CrossRef]
- Thong, T.; Li, K.; McNames, J.; Aboy, M.; Goldstein, B. Accuracy of ultra-short heart rate variability measures. In Proceedings of the 25th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Cancun, Mexico, 17–21 September 2003; IEEE: New York, NY, USA, 2003; pp. 2424–2427. [Google Scholar]
- Schroeder, E.B.; Whitsel, E.A.; Evans, G.W.; Prineas, R.J.; Chambless, L.E.; Heiss, G. Repeatability of heart rate variability measures. J. Electrocardiol. 2004, 37, 163–172. [Google Scholar] [CrossRef]
- Esco, M.R.; Flatt, A.A. Ultra-short-term heart rate variability indexes at rest and post-exercise in athletes: Evaluating the agreement with accepted recommendations. J. Sports Sci. Med. 2014, 13, 535–541. [Google Scholar] [PubMed]
- Baek, H.J.; Cho, C.H.; Cho, J.; Woo, J.M. Reliability of ultra-short-term analysis as a surrogate of standard 5-min analysis of heart rate variability. Telemed. J. E Health 2015, 21, 404–414. [Google Scholar] [CrossRef] [PubMed]
- Munoz, M.L.; van Roon, A.; Riese, H.; Thio, C.; Oostenbroek, E.; Westrik, I.; de Geus, E.J.; Gansevoort, R.; Lefrandt, J.; Nolte, I.M.; et al. Validity of (Ultra-)Short Recordings for Heart Rate Variability Measurements. PLoS ONE 2015, 10, e0138921. [Google Scholar] [CrossRef] [Green Version]
- Pereira, L.A.; Flatt, A.A.; Ramirez-Campillo, R.; Loturco, I.; Nakamura, F.Y. Assessing Shortened Field-Based Heart-Rate-Variability-Data Acquisition in Team-Sport Athletes. Int. J. Sport. Physiol. Perform. 2016, 11, 154–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bourdillon, N.; Schmitt, L.; Yazdani, S.; Vesin, J.M.; Millet, G.P. Minimal Window Duration for Accurate HRV Recording in Athletes. Front. Neurosci. 2017, 11, 456. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, B.; Flatt, A.A.; Silva, L.E.V.; Mlynczak, M.; Baranowski, R.; Dziedzic, E.; Werner, B.; Gasior, J.S. A Pilot Study of the Reliability and Agreement of Heart Rate, Respiratory Rate and Short-Term Heart Rate Variability in Elite Modern Pentathlon Athletes. Diagnostics 2020, 10, 833. [Google Scholar] [CrossRef] [PubMed]
- Shaffer, F.; Meehan, Z.M.; Zerr, C.L. A Critical Review of Ultra-Short-Term Heart Rate Variability Norms Research. Front. Neurosci. 2020, 14, 594880. [Google Scholar] [CrossRef]
- Wu, L.; Shi, P.; Yu, H.; Liu, Y. An optimization study of the ultra-short period for HRV analysis at rest and post-exercise. J. Electrocardiol. 2020, 63, 57–63. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-S.; Clemente, F.M.; Bezerra, P.; Lu, Y.-X. Ultra-Short-Term and Short-Term Heart Rate Variability Recording during Training Camps and an International Tournament in U-20 National Futsal Players. Int. J. Environ. Res. Public Health 2020, 17, 775. [Google Scholar] [CrossRef] [Green Version]
- Burma, J.S.; Graver, S.; Miutz, L.N.; Macaulay, A.; Copeland, P.V.; Smirl, J.D. The validity and reliability of ultra-short-term heart rate variability parameters and the influence of physiological covariates. J. Appl. Physiol. 2021, 130, 1848–1867. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.S.; Pagaduan, J.C.; Bezerra, P.; Crowley-McHattan, Z.J.; Kuo, C.D.; Clemente, F.M. Agreement of Ultra-Short-Term Heart Rate Variability Recordings During Overseas Training Camps in under-20 National Futsal Players. Front. Psychol. 2021, 12, 621399. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Seok, H.S.; Shin, H. Is Ultra-Short-Term Heart Rate Variability Valid in Non-static Conditions? Front. Physiol. 2021, 12, 596060. [Google Scholar] [CrossRef]
- Abellán-Aynés, O.; López-Plaza, D.; Alacid, F.; Naranjo-Orellana, J.; Manonelles, P. Recovery of Heart Rate Variability after Exercise Under Hot Conditions: The Effect of Relative Humidity. Wilderness Environ. Med. 2019, 30, 260–267. [Google Scholar] [CrossRef] [Green Version]
- Michael, S.; Graham, K.S.; Davis, G.M.O. Cardiac Autonomic Responses during Exercise and Post-exercise Recovery Using Heart Rate Variability and Systolic Time Intervals-A Review. Front. Physiol. 2017, 8, 301. [Google Scholar] [CrossRef] [Green Version]
- Rogers, B.; Giles, D.; Draper, N.; Hoos, O.; Gronwald, T. A New Detection Method Defining the Aerobic Threshold for Endurance Exercise and Training Prescription Based on Fractal Correlation Properties of Heart Rate Variability. Front. Physiol. 2020, 11, 596567. [Google Scholar] [CrossRef]
- Tanoue, Y.; Komatsu, T.; Nakashima, S.; Matsuda, T.; Michishita, R.; Higaki, Y.; Uehara, Y. The ratio of heart rate to heart rate variability reflects sympathetic activity during incremental cycling exercise. Eur. J. Sport Sci. 2021, 22, 1714–1723. [Google Scholar] [CrossRef]
- Hirano, M.; Yamada, Y.; Hibi, M.; Katashima, M.; Higaki, Y.; Kiyonaga, A.; Tanaka, H. Simultaneous multiple-subject analysis of respiratory gas exchange in humans. J. Phys. Fit. Sport. Med. 2014, 3, 269–279. [Google Scholar] [CrossRef] [Green Version]
- Sahara, H.; Ezoe, K.; Fukuoka, H.; Ohtomo, N.; Tanaka, Y.; Takahashi, N.; Sato, N.; Kikuchi, K. Periodicity of Ovarian Follicular Dynamics in Postpartum Cows Demonstrated Using Time-Series Analysis Based on the Maximum Entropy Method. J. Reprod. Dev. 1996, 42, 117–124. [Google Scholar] [CrossRef]
- Sawada, Y.; Ohtomo, N.; Tanaka, Y.; Tanaka, G.; Yamakoshi, K.; Terachi, S.; Shimamoto, K.; Nakagawa, M.; Satoh, S.; Kuroda, S.; et al. New technique for time series analysis combining the maximum entropy method and non-linear least squares method: Its value in heart rate variability analysis. Med. Biol. Eng. Comput. 1997, 35, 318–322. [Google Scholar] [CrossRef] [PubMed]
- Tarvainen, M.P.; Niskanen, J.-P.; Lipponen, J.A.; Ranta-Aho, P.O.; Karjalainen, P.A. Kubios HRV—Heart rate variability analysis software. Comput. Methods Programs Biomed. 2014, 113, 210–220. [Google Scholar] [CrossRef]
- Pecchia, L.; Castaldo, R.; Montesinos, L.; Melillo, P. Are ultra-short heart rate variability features good surrogates of short-term ones? State-of-the-art review and recommendations. Healthc. Technol. Lett. 2018, 5, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Earlbaum Associates: New York, NY, USA, 1988. [Google Scholar]
- Breuer, H.W.; Skyschally, A.; Schulz, R.; Martin, C.; Wehr, M.; Heusch, G. Heart rate variability and circulating catecholamine concentrations during steady state exercise in healthy volunteers. Heart 1993, 70, 144–149. [Google Scholar] [CrossRef]
- Tulppo, M.P.; Mäkikallio, T.H.; Seppänen, T.; Laukkanen, R.T.; Huikuri, H.V. Vagal modulation of heart rate during exercise: Effects of age and physical fitness. Am. J. Physiol. 1998, 274, H424-9. [Google Scholar] [CrossRef]
- Casties, J.F.; Mottet, D.; Le Gallais, D. Non-linear analyses of heart rate variability during heavy exercise and recovery in cyclists. Int. J. Sports Med. 2006, 27, 780–785. [Google Scholar] [CrossRef] [PubMed]
- Leicht, A.S.; Sinclair, W.H.; Spinks, W.L. Effect of exercise mode on heart rate variability during steady state exercise. Eur. J. Appl. Physiol. 2008, 102, 195–204. [Google Scholar] [CrossRef]
- Gąsior, J.S.; Hoffmann, B.; Silva, L.E.V.; Małek, Ł.; Flatt, A.A.; Baranowski, R.; Werner, B. Changes in Short-Term and Ultra-Short Term Heart Rate, Respiratory Rate, and Time-Domain Heart Rate Variability Parameters during Sympathetic Nervous System Activity Stimulation in Elite Modern Pentathlonists—A Pilot Study. Diagnostics 2020, 10, 1104. [Google Scholar] [CrossRef]
- Pagani, M.; Lombardi, F.; Guzzetti, S.; Rimoldi, O.; Furlan, R.; Pizzinelli, P.; Sandrone, G.; Malfatto, G.; Dell’Orto, S.; Piccaluga, E.; et al. Power spectral analysis of heart rate and arterial pressure variabilities as a marker of sympatho-vagal interaction in man and conscious dog. Circ. Res. 1986, 59, 178–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arai, Y.; Saul, J.P.; Albrecht, P.; Hartley, L.H.; Lilly, L.S.; Cohen, R.J.; Colucci, W.S. Modulation of cardiac autonomic activity during and immediately after exercise. Am. J. Physiol. 1989, 256, H132–H141. [Google Scholar] [CrossRef]
- Pichon, A.P.; de Bisschop, C.; Roulaud, M.; Denjean, A.; Papelier, Y. Spectral analysis of heart rate variability during exercise in trained subjects. Med. Sci. Sports Exerc. 2004, 36, 1702–1708. [Google Scholar] [CrossRef] [PubMed]
- Hautala, A.J.; Mäkikallio, T.H.; Seppänen, T.; Huikuri, H.V.; Tulppo, M.P. Short-term correlation properties of R-R interval dynamics at different exercise intensity levels. Clin. Physiol. Funct. Imaging. 2003, 23, 215–223. [Google Scholar] [CrossRef] [PubMed]
- Gronwald, T.; Rogers, B.; Hoos, O. Fractal Correlation Properties of Heart Rate Variability: A New Biomarker for Intensity Distribution in Endurance Exercise and Training Prescription? Front. Physiol. 2020, 11, 550572. [Google Scholar] [CrossRef] [PubMed]
- Volpes, G.; Barà, C.; Busacca, A.; Stivala, S.; Javorka, M.; Faes, L.; Pernice, R. Feasibility of Ultra-Short-Term Analysis of Heart Rate and Systolic Arterial Pressure Variability at Rest and during Stress via Time-Domain and Entropy-Based Measures. Sensors 2022, 22, 9149. [Google Scholar] [CrossRef] [PubMed]
- Sacha, J.; Pluta, W. Alterations of an average heart rate change heart rate variability due to mathematical reasons. Int. J. Cardiol. 2008, 128, 444–447. [Google Scholar] [CrossRef] [PubMed]
- Monfredi, O.; Lyashkov, A.E.; Johnsen, A.B.; Inada, S.; Schneider, H.; Wang, R.; Nirmalan, M.; Wisloff, U.; Maltsev, V.A.; Lakatta, E.G.; et al. Biophysical characterization of the underappreciated and important relationship between heart rate variability and heart rate. Hypertension 2014, 64, 1334–1343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakamura, F.Y.; Antunes, P.; Nunes, C.; Costa, J.A.; Esco, M.R.; Travassos, B. Heart Rate Variability Changes from Traditional vs. Ultra-Short-Term Recordings in Relation to Preseason Training Load and Performance in Futsal Players. J. Strength Cond. Res. 2020, 34, 2974–2981. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | 20% | 50% | 80% |
|---|---|---|---|
| Workload (watts) | 29 ± 11 | 100 ± 21 * | 173 ± 30 *† |
| VO2 (ml/kg/min) | 8.5 ± 1.4 | 21.3 ± 3.5 * | 34.1 ± 5.7 *† |
| Vt (L) | 0.8 ± 0.2 | 1.3 ± 0.3 * | 1.8 ± 0.4 *† |
| Respiratory rate (breath/min) | 20.4 ± 3.7 | 24.4 ± 5.3 * | 33.8 ± 7.1 *† |
| Blood lactate (mmol/L) | 1.0 ± 0.3 | 1.5 ± 0.4 * | 3.6 ± 0.7 *† |
| Adrenaline (ng/mL) | 0.05 ± 0.04 | 0.07 ± 0.05 | 0.21 ± 0.25 *† |
| Noradrenaline (ng/mL) | 0.42 ± 0.16 | 0.59 ± 0.23 * | 1.15 ± 0.75 *† |
| Variable | Exercise Intensity | Coefficient of Correlation | |||
|---|---|---|---|---|---|
| 180 sec vs. 120 sec | 180 sec vs. 90 sec | 180 sec vs. 60 sec | 180 sec vs. 30 sec | ||
| Time-domain | |||||
| log SDNN | 20% | 0.993 * | 0.972 * | 0.953 * | 0.906 * |
| 50% | 0.938 * | 0.917 * | 0.895 * | 0.832 * | |
| 80% | 0.917 * | 0.890 * | 0.831 * | 0.792 * | |
| log RMSSD | 20% | 0.996 * | 0.981 * | 0.957 * | 0.917 * |
| 50% | 0.960 * | 0.936 * | 0.921 * | 0.884 * | |
| 80% | 0.950 * | 0.918 * | 0.884 * | 0.835 * | |
| Frequency-domain | |||||
| log LF | 20% | 0.982 * | 0.936 * | 0.926 *a | 0.814 *a |
| 50% | 0.883 * | 0.867 * | 0.797 * | 0.655 * | |
| 80% | 0.906 * | 0.898 * | 0.818 * | 0.738 * | |
| log HF | 20% | 0.992 * | 0.969 * | 0.950 * | 0.910 * |
| 50% | 0.934 * | 0.908 * | 0.819 * | 0.730 * | |
| 80% | 0.911 * | 0.859 * | 0.836 * | 0.825 * | |
| log LF/HF | 20% | 0.959 * | 0.868 * | 0.735 *a | 0.476 *a |
| 50% | 0.799 * | 0.736 * | 0.725 * | 0.362 | |
| 80% | 0.821 *a | 0.771 *a | 0.769 *a | 0.725 *a | |
| log Heart rate/LF | 20% | 0.984 * | 0.944 * | 0.924 * | 0.837 * |
| 50% | 0.895 * | 0.878 * | 0.815 * | 0.693 * | |
| 80% | 0.911 * | 0.903 * | 0.829 * | 0.747 * | |
| Non-linear analysis | |||||
| DFAα1 | 20% | 0.942 * | 0.839 * | 0.717 *a | - |
| 50% | 0.703 * | 0.525 * | 0.549 * | 0.083 | |
| 80% | 0.906 * | 0.911 *a | 0.864 *a | 0.733 *a | |
| DFAα2 | 20% | 0.818 * | 0.673 * | 0.364 | - |
| 50% | 0.698 * | 0.570 * | 0.474 * | −0.946 | |
| 80% | 0.529 * | 0.218 | 0.403 * | −0.116 | |
| SampEn | 20% | 0.898 * | 0.768 * | 0.707 * | - |
| 50% | 0.846 * | 0.739 * | 0.731 * | −0.036 | |
| 80% | 0.605 *a | 0.517 *a | 0.319 a | 0.332 a | |
| Variable | Exercise Intensity | Statistical Metrics | |
|---|---|---|---|
| Correlation Coefficient | Effect Size (Bias) | ||
| Time-domain | |||
| log SDNN | 20% | 30 sec | n/a |
| 50% | 30 sec | n/a | |
| 80% | 60 sec | n/a | |
| log RMSSD | 20% | 30 sec | 120 sec |
| 50% | 30 sec | n/a | |
| 80% | 30 sec | n/a | |
| Frequency-domain | |||
| log LF | 20% | 30 sec | 30 sec |
| 50% | 90 sec | n/a | |
| 80% | 60 sec | n/a | |
| log HF | 20% | 30 sec | 90 sec |
| 50% | 60 sec | n/a | |
| 80% | 30 sec | n/a | |
| log LF/HF | 20% | 90 sec | 30 sec |
| 50% | n/a | 30 sec | |
| 80% | 120 sec | 30 sec | |
| log Heart rate/LF | 20% | 30 sec | 90 sec |
| 50% | 60 sec | n/a | |
| 80% | 60 sec | n/a | |
| Non-linear analysis | |||
| DFAα1 | 20% | 90 sec | 60 sec |
| 50% | n/a | 30 sec | |
| 80% | 60 sec | n/a | |
| DFAα2 | 20% | 120 sec | 60 sec |
| 50% | n/a | 30 sec | |
| 80% | n/a | 30 sec | |
| SampEn | 20% | 120 sec | 60 sec |
| 50% | 120 sec | 60 sec | |
| 80% | n/a | 30 sec | |
| Variable | Exercise Intensity | Effect Size | |||
|---|---|---|---|---|---|
| 180 sec vs. 120 sec | 180 sec vs. 90 sec | 180 sec vs. 60 sec | 180 sec vs. 30 sec | ||
| Time-domain | |||||
| log SDNN | 20% | 0.502 | 0.552 | 0.659 | 0.775 |
| 50% | 1.212 | 1.287 | 1.445 | 1.331 | |
| 80% | 1.266 | 1.367 | 1.309 | 1.312 | |
| log RMSSD | 20% | 0.475 | 0.526 | 0.636 | 0.754 |
| 50% | 1.354 | 1.496 | 1.554 | 1.487 | |
| 80% | 0.834 | 0.862 | 0.810 | 0.798 | |
| Frequency-domain | |||||
| log LF | 20% | 0.162 | 0.310 | 0.435 a | 0.491 a |
| 50% | 1.011 | 0.924 | 1.107 | 1.062 | |
| 80% | 1.122 | 1.328 | 1.331 | 1.224 | |
| log HF | 20% | 0.417 | 0.389 | 0.523 | 0.741 |
| 50% | 1.027 | 1.140 | 0.993 | 0.835 | |
| 80% | 0.812 | 0.859 | 1.044 | 0.986 | |
| log LF/HF | 20% | −0.172 | −0.049 | −0.065 a | −0.043 a |
| 50% | −0.061 | −0.192 | −0.100 | −0.250 | |
| 80% | 0.343 a | 0.291 a | 0.251 a | 0.315 a | |
| log Heart rate/LF | 20% | −0.218 | −0.360 | −0.594 | −0.620 |
| 50% | −1.077 | −1.004 | −1.198 | −1.143 | |
| 80% | −1.174 | −1.401 | −1.409 | −1.298 | |
| Non-linear analysis | |||||
| DFAα1 | 20% | 0.036 | 0.072 | 0.127 a | - |
| 50% | −0.085 | −0.239 | −0.125 | 0.477 | |
| 80% | 1.040 | −0.775 a | −0.753 a | −0.705 a | |
| DFAα2 | 20% | −0.034 | −0.009 | −0.267 | - |
| 50% | −0.187 | −0.190 | 0.052 | 0.112 | |
| 80% | −0.008 | −0.142 | −0.322 | −0.143 | |
| SampEn | 20% | −0.028 | −0.224 | −0.322 | - |
| 50% | −0.276 | −0.276 | −0.356 | −0.597 | |
| 80% | −0.181 a | −0.034 a | −0.052 a | −0.097 a | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanoue, Y.; Nakashima, S.; Komatsu, T.; Kosugi, M.; Kawakami, S.; Kawakami, S.; Michishita, R.; Higaki, Y.; Uehara, Y. The Validity of Ultra-Short-Term Heart Rate Variability during Cycling Exercise. Sensors 2023, 23, 3325. https://doi.org/10.3390/s23063325
Tanoue Y, Nakashima S, Komatsu T, Kosugi M, Kawakami S, Kawakami S, Michishita R, Higaki Y, Uehara Y. The Validity of Ultra-Short-Term Heart Rate Variability during Cycling Exercise. Sensors. 2023; 23(6):3325. https://doi.org/10.3390/s23063325
Chicago/Turabian StyleTanoue, Yukiya, Shihoko Nakashima, Tomohiro Komatsu, Miki Kosugi, Saki Kawakami, Shotaro Kawakami, Ryoma Michishita, Yasuki Higaki, and Yoshinari Uehara. 2023. "The Validity of Ultra-Short-Term Heart Rate Variability during Cycling Exercise" Sensors 23, no. 6: 3325. https://doi.org/10.3390/s23063325