
Definition of High-Risk Motion Patterns for Female ACL Injury Based on Football-Specific Field Data: A Wearable Sensors Plus Data Mining Approach

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.3. Agility Task
2.4. Data Processing and Statistical Analysis
3. Results
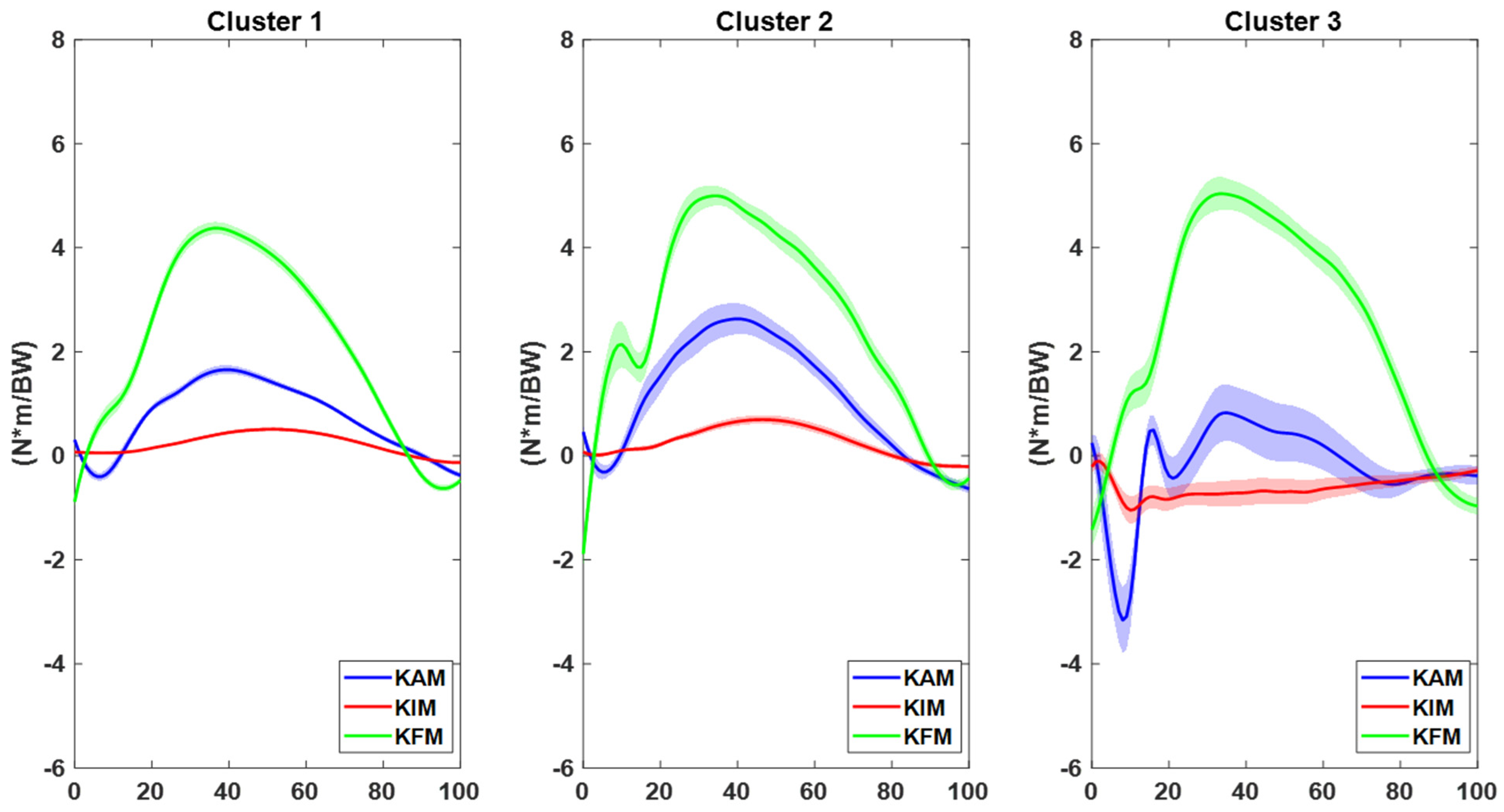
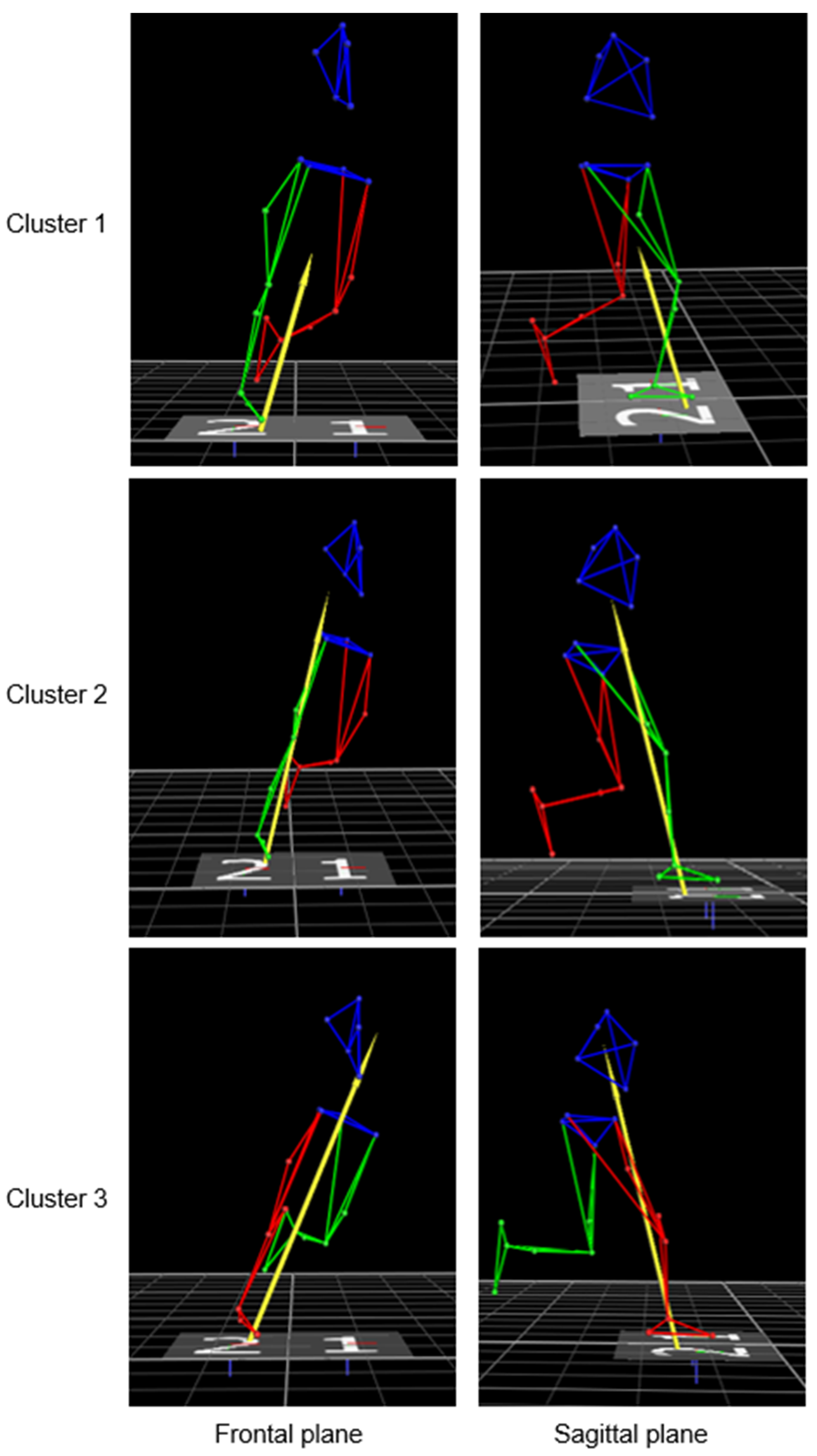
3.1. Laboratory-Based Clustering
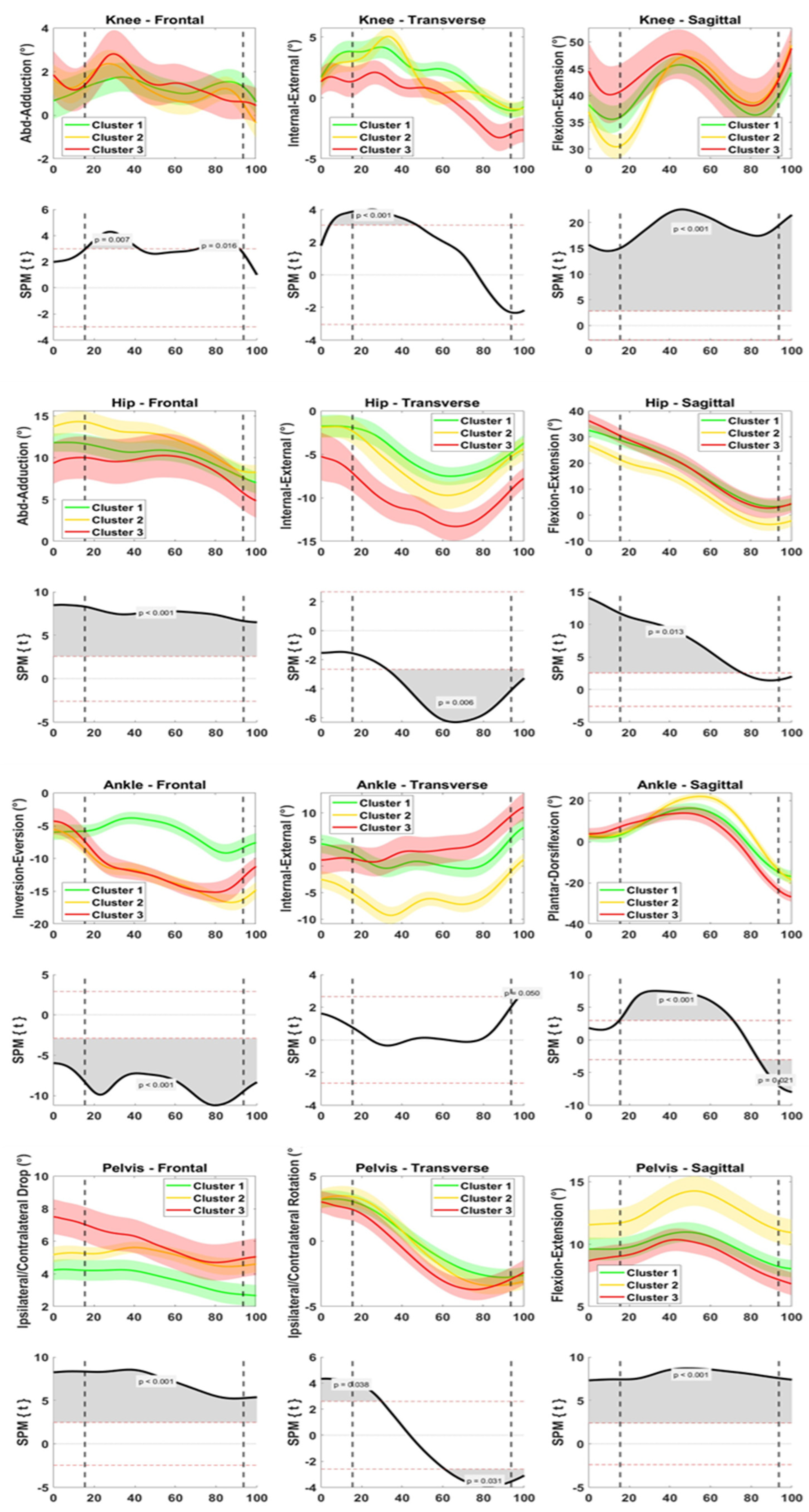
3.2. Field Data—Exercise Kinematics
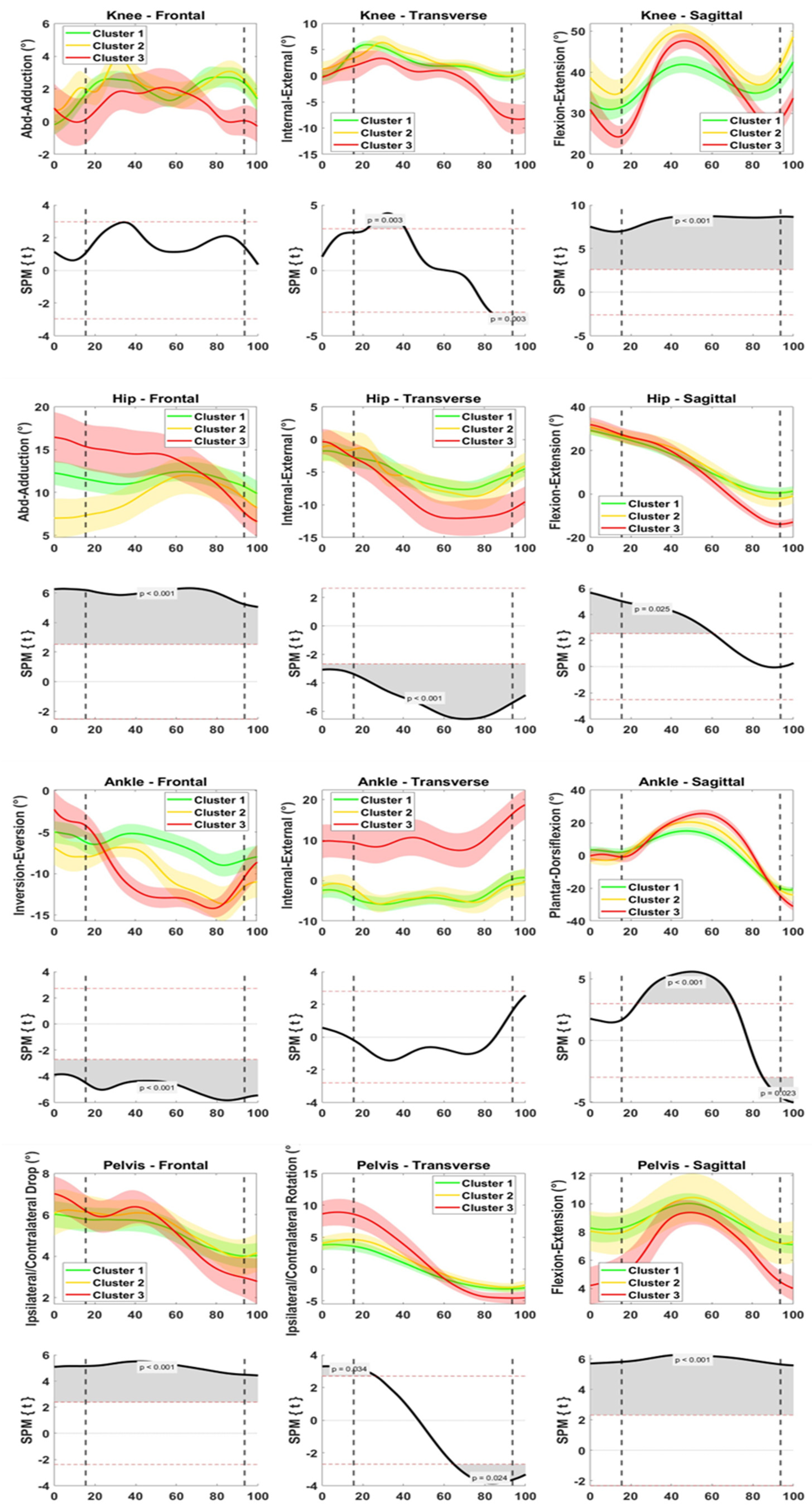
3.3. Field Data—Game Kinematics
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Agel, J.; Rockwood, T.; Klossner, D. Collegiate ACL Injury Rates Across 15 Sports: National Collegiate Athletic Association Injury Surveillance System Data Update (2004–2005 Through 2012–2013). Clin. J. Sport Med. Off. J. Can. Acad. Sport Med. 2016, 26, 518–523. [Google Scholar] [CrossRef] [PubMed]
- Aït Si Selmi, T.; Fithian, D.; Neyret, P. The Evolution of Osteoarthritis in 103 Patients with ACL Reconstruction at 17 Years Follow-Up. Knee 2006, 13, 353–358. [Google Scholar] [CrossRef] [PubMed]
- Brophy, R.H.; Stepan, J.G.; Silvers, H.J.; Mandelbaum, B.R. Defending Puts the Anterior Cruciate Ligament at Risk During Soccer: A Gender-Based Analysis. Sport. Health Multidiscip. Approach 2015, 7, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Lucarno, S.; Zago, M.; Buckthorpe, M.; Grassi, A.; Tosarelli, F.; Smith, R.; Della Villa, F. Systematic Video Analysis of Anterior Cruciate Ligament Injuries in Professional Female Soccer Players. Am. J. Sport. Med. 2021, 49, 1794–1802. [Google Scholar] [CrossRef] [PubMed]
- Bolt, R.; Heuvelmans, P.; Benjaminse, A.; Robinson, M.A.; Gokeler, A. An Ecological Dynamics Approach to ACL Injury Risk Research: A Current Opinion. Sport. Biomech. 2021, 1–14. [Google Scholar] [CrossRef]
- Gokeler, A.; Benjaminse, A.; Della Villa, F.; Tosarelli, F.; Verhagen, E.; Baumeister, J. Anterior Cruciate Ligament Injury Mechanisms through a Neurocognition Lens: Implications for Injury Screening. BMJ Open Sport Exerc. Med. 2021, 7, e001091. [Google Scholar] [CrossRef]
- McLean, S.G.; Huang, X.; van den Bogert, A.J. Association between Lower Extremity Posture at Contact and Peak Knee Valgus Moment during Sidestepping: Implications for ACL Injury. Clin. Biomech. 2005, 20, 863–870. [Google Scholar] [CrossRef] [Green Version]
- Sigward, S.M.; Powers, C.M. The Influence of Gender on Knee Kinematics, Kinetics and Muscle Activation Patterns during Side-Step Cutting. Clin. Biomech. 2006, 21, 41–48. [Google Scholar] [CrossRef]
- Cortes, N.; Blount, E.; Ringleb, S.; Onate, J.A. Soccer-Specific Video Simulation for Improving Movement Assessment. Sport. Biomech. 2011, 10, 22–34. [Google Scholar] [CrossRef]
- Lee, M.J.C.; Lloyd, D.G.; Lay, B.S.; Bourke, P.D.; Alderson, J.A. Effects of Different Visual Stimuli on Postures and Knee Moments during Sidestepping. Med. Sci. Sport. Exerc. 2013, 45, 1740–1748. [Google Scholar] [CrossRef]
- McGuckian, T.B.; Cole, M.H.; Pepping, G.-J. A Systematic Review of the Technology-Based Assessment of Visual Perception and Exploration Behaviour in Association Football. J. Sport. Sci. 2018, 36, 861–880. [Google Scholar] [CrossRef] [PubMed]
- Krosshaug, T.; Steffen, K.; Kristianslund, E.; Nilstad, A.; Mok, K.-M.; Myklebust, G.; Andersen, T.E.; Holme, I.; Engebretsen, L.; Bahr, R. The Vertical Drop Jump Is a Poor Screening Test for ACL Injuries in Female Elite Soccer and Handball Players: A Prospective Cohort Study of 710 Athletes. Am. J. Sport. Med. 2016, 44, 874–883. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Paolo, S.; Nijmeijer, E.; Bragonzoni, L.; Dingshoff, E.; Gokeler, A.; Benjaminse, A. Comparing Lab and Field Agility Kinematics in Young Talented Female Football Players: Implications for ACL Injury Prevention. Eur. J. Sport Sci. 2022, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Newell, K.M.; Van Emmerik, R.E.A.; McDonald, P.V. Biomechanical Constraints and Action Theory. Hum. Mov. Sci. 1989, 8, 403–409. [Google Scholar] [CrossRef]
- Vicon Motion Systems. Vicon Nexus User Guide. Available online: https://docs.vicon.com/display/Nexus212/Vicon+Nexus+User+Guide/ (accessed on 9 February 2023).
- Kadaba, M.P.; Ramakrishnan, H.K.; Wooten, M.E.; Gainey, J.; Gorton, G.; Cochran, G.V.B. Repeatability of Kinematic, Kinetic, and EMG Data in Normal Adult Gait. J. Orthop. Res. 1989, 7, 849–860. [Google Scholar]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The Reliability of Three-Dimensional Kinematic Gait Measurements: A Systematic Review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef]
- Dos’Santos, T.; Thomas, C.; Jones, P.A. The Effect of Angle on Change of Direction Biomechanics: Comparison and Inter-Task Relationships. J. Sport. Sci. 2021, 39, 2618–2631. [Google Scholar] [CrossRef]
- Koga, H.; Nakamae, A.; Shima, Y.; Iwasa, J.; Myklebust, G.; Engebretsen, L.; Bahr, R.; Krosshaug, T. Mechanisms for Noncontact Anterior Cruciate Ligament Injuries: Knee Joint Kinematics in 10 Injury Situations from Female Team Handball and Basketball. Am. J. Sport. Med. 2010, 38, 2218–2225. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Heidt, R.S.; Colosimo, A.J.; McLean, S.G.; Van Den Bogert, A.J.; Paterno, M.V.; Succop, P. Biomechanical Measures of Neuromuscular Control and Valgus Loading of the Knee Predict Anterior Cruciate Ligament Injury Risk in Female Athletes: A Prospective Study. Am. J. Sport. Med. 2005, 33, 492–501. [Google Scholar] [CrossRef] [Green Version]
- Myer, G.D.; Ford, K.R.; Di Stasi, S.L.; Foss, K.D.B.; Micheli, L.J.; Hewett, T.E. High Knee Abduction Moments Are Common Risk Factors for Patellofemoral Pain (PFP) and Anterior Cruciate Ligament (ACL) Injury in Girls: Is PFP Itself a Predictor for Subsequent ACL Injury? Br. J. Sport. Med. 2015, 49, 118–122. [Google Scholar] [CrossRef] [Green Version]
- Dicesare, C.A.; Minai, A.A.; Riley, M.A.; Ford, K.R.; Hewett, T.E.; Myer, G.D. Distinct Coordination Strategies Associated with the Drop Vertical Jump Task. Med. Sci. Sport. Exerc. 2020, 52, 1088–1098. [Google Scholar] [CrossRef] [PubMed]
- Sigurðsson, H.B.; Briem, K. Cluster Analysis Successfully Identifies Clinically Meaningful Knee Valgus Moment Patterns: Frequency of Early Peaks Reflects Sex-Specific ACL Injury Incidence. J. Exp. Orthop. 2019, 6, 37. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigurðsson, H.B.; Karlsson, J.; Snyder-Mackler, L.; Briem, K. Kinematics Observed during ACL Injury Are Associated with Large Early Peak Knee Abduction Moments during a Change of Direction Task in Healthy Adolescents. J. Orthop. Res. 2021, 39, 2281–2290. [Google Scholar] [CrossRef] [PubMed]
- Della Villa, F.; Buckthorpe, M.; Grassi, A.; Nabiuzzi, A.; Tosarelli, F.; Zaffagnini, S.; Della Villa, S. Systematic Video Analysis of ACL Injuries in Professional Male Football (Soccer): Injury Mechanisms, Situational Patterns and Biomechanics Study on 134 Consecutive Cases. Br. J. Sport. Med. 2020, 54, 1423–1432. [Google Scholar] [CrossRef]
- Dix, C.; Arundale, A.; Silvers-Granelli, H.; Marmon, A.; Zarzycki, R.; Snyder-Mackler, L. Biomechanical Measures during Two Sport-Specific Tasks Differentiate between Soccer Players Who Go on to Anterior Cruciate Ligament Injury and Those Who Do Not: A Prospective Cohort Analysis. Int. J. Sport. Phys. Ther. 2020, 15, 928–935. [Google Scholar] [CrossRef]
- Donelon, T.A.; Dos’Santos, T.; Pitchers, G.; Brown, M.; Jones, P.A. Biomechanical Determinants of Knee Joint Loads Associated with Increased Anterior Cruciate Ligament Loading During Cutting: A Systematic Review and Technical Framework. Sport. Med.-Open 2020, 6, 53. [Google Scholar] [CrossRef]
- Leppänen, M.; Pasanen, K.; Krosshaug, T.; Kannus, P.; Vasankari, T.; Kujala, U.M.; Bahr, R.; Perttunen, J.; Parkkari, J. Sagittal Plane Hip, Knee, and Ankle Biomechanics and the Risk of Anterior Cruciate Ligament Injury: A Prospective Study. Orthop. J. Sport. Med. 2017, 5, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Bates, N.A.; Myer, G.D.; Hale, R.F.; Schilaty, N.D.; Hewett, T.E. Prospective Frontal Plane Angles Used to Predict ACL Strain and Identify Those at High Risk for Sports-Related ACL Injury. Orthop. J. Sport. Med. 2020, 8, 232596712095764. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Kiefer, A.W.; Ford, K.R. Longitudinal Increases in Knee Abduction Moments in Females during Adolescent Growth. Med. Sci. Sport. Exerc. 2015, 47, 2579–2585. [Google Scholar] [CrossRef]
- Di Paolo, S.; Bragonzoni, L.; Della Villa, F.; Grassi, A.; Zaffagnini, S. Do Healthy Athletes Exhibit At-Risk Biomechanics for Anterior Cruciate Ligament Injury during Pivoting Movements? Sport. Biomech. 2022, 1–14. [Google Scholar] [CrossRef]
- Alentorn-Geli, E.; Myer, G.D.; Silvers, H.J.; Samitier, G.; Romero, D.; Lázaro-Haro, C.; Cugat, R. Prevention of Non-Contact Anterior Cruciate Ligament Injuries in Soccer Players. Part 1: Mechanisms of Injury and Underlying Risk Factors. Knee Surg. Sport. Traumatol. Arthrosc. 2009, 17, 705–729. [Google Scholar] [CrossRef]
- Shultz, S.J.; Schmitz, R.J. Effects of Transverse and Frontal Plane Knee Laxity on Hip and Knee Neuromechanics during Drop Landings. Am. J. Sport. Med. 2009, 37, 1821–1830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leppänen, M.; Pasanen, K.; Kujala, U.M.; Vasankari, T.; Kannus, P.; Äyrämö, S.; Krosshaug, T.; Bahr, R.; Avela, J.; Perttunen, J.; et al. Stiff Landings Are Associated With Increased ACL Injury Risk in Young Female Basketball and Floorball Players. Am. J. Sport. Med. 2017, 45, 386–393. [Google Scholar] [CrossRef]
- Paterno, M.V.; Kiefer, A.W.; Bonnette, S.; Riley, M.A.; Schmitt, L.C.; Ford, K.R.; Myer, G.D.; Shockley, K.; Hewett, T.E. Prospectively Identified Deficits in Sagittal Plane Hip–Ankle Coordination in Female Athletes Who Sustain a Second Anterior Cruciate Ligament Injury after Anterior Cruciate Ligament Reconstruction and Return to Sport. Clin. Biomech. 2015, 30, 1094–1101. [Google Scholar] [CrossRef] [Green Version]
- Silvers-Granelli, H.J.; Bizzini, M.; Arundale, A.; Mandelbaum, B.R.; Snyder-Mackler, L. Does the FIFA 11+ Injury Prevention Program Reduce the Incidence of ACL Injury in Male Soccer Players? Clin. Orthop. 2017, 475, 2447–2455. [Google Scholar] [CrossRef] [PubMed]
- Slauterbeck, J.R.; Choquette, R.; Tourville, T.W.; Krug, M.; Mandelbaum, B.R.; Vacek, P.; Beynnon, B.D. Implementation of the FIFA 11+ Injury Prevention Program by High School Athletic Teams Did Not Reduce Lower Extremity Injuries: A Cluster Randomized Controlled Trial. Am. J. Sport. Med. 2019, 47, 2844–2852. [Google Scholar] [CrossRef]
- Heidarnia, E.; Letafatkar, A.; Khaleghi-Tazji, M.; Grooms, D.R. Comparing the Effect of a Simulated Defender and Dual-Task on Lower Limb Coordination and Variability during a Side-Cut in Basketball Players with and without Anterior Cruciate Ligament Injury. J. Biomech. 2022, 133, 110965. [Google Scholar] [CrossRef]
- Olivares-Jabalera, J.; Fílter-Ruger, A.; Dos’Santos, T.; Afonso, J.; Della Villa, F.; Morente-Sánchez, J.; Soto-Hermoso, V.M.; Requena, B. Exercise-Based Training Strategies to Reduce the Incidence or Mitigate the Risk Factors of Anterior Cruciate Ligament Injury in Adult Football (Soccer) Players: A Systematic Review. Int. J. Environ. Res. Public. Health 2021, 18, 13351. [Google Scholar] [CrossRef]
- Davis, K.; Williams, J.L.; Sanford, B.A.; Zucker-Levin, A. Assessing Lower Extremity Coordination and Coordination Variability in Individuals with Anterior Cruciate Ligament Reconstruction during Walking. Gait Posture 2019, 67, 154–159. [Google Scholar] [CrossRef]
- Weir, G.; van Emmerik, R.; Jewell, C.; Hamill, J. Coordination and Variability during Anticipated and Unanticipated Sidestepping. Gait Posture 2019, 67, 1–8. [Google Scholar] [CrossRef]
- Shao, E.; Mei, Q.; Ye, J.; Ugbolue, U.C.; Chen, C.; Gu, Y. Predicting Coordination Variability of Selected Lower Extremity Couplings during a Cutting Movement: An Investigation of Deep Neural Networks with the LSTM Structure. Bioengineering 2022, 9, 411. [Google Scholar] [CrossRef] [PubMed]
- Di Paolo, S.; Santillozzi, F.; Zinno, R.; Barone, G.; Bragonzoni, L. On-Field Biomechanical Assessment of High and Low Dive in Competitive 16-Year-Old Goalkeepers through Wearable Sensors and Principal Component Analysis. Sensors 2022, 22, 7519. [Google Scholar] [CrossRef] [PubMed]
- Federolf, P.A. A Novel Approach to Study Human Posture Control: “Principal Movements” Obtained from a Principal Component Analysis of Kinematic Marker Data. J. Biomech. 2016, 49, 364–370. [Google Scholar] [CrossRef] [Green Version]
- Smeets, A.; Verheul, J.; Vanrenterghem, J.; Staes, F.; Vandenneucker, H.; Claes, S.; Verschueren, S. Single-Joint and Whole-Body Movement Changes in Anterior Cruciate Ligament Athletes Returning to Sport. Med. Sci. Sport. Exerc. 2020, 52, 1658–1667. [Google Scholar] [CrossRef] [PubMed]
- FIFA Medical Assessment and Research Centre. Fifa11+Manual. Available online: https://www.fifa.com/ (accessed on 9 February 2023).
- Gokeler, A.; Grassi, A.; Hoogeslag, R.; van Houten, A.; Lehman, T.; Bolling, C.; Buckthorpe, M.; Norte, G.; Benjaminse, A.; Heuvelmans, P.; et al. Return to Sports after ACL Injury 5 Years from Now: 10 Things We Must Do. J. Exp. Orthop. 2022, 9, 73. [Google Scholar] [CrossRef]
- Nijmeijer, E.M.; Elferink-Gemser, M.T.; Otten, E.; Benjaminse, A. Optimal and Suboptimal Video Instructions Change Movement Execution in Young Talented Basketball Players. Int. J. Sport. Sci. Coach. 2022, 174795412211188. [Google Scholar] [CrossRef]
- Di Paolo, S.; Lopomo, N.F.; Della Villa, F.; Paolini, G.; Figari, G.; Bragonzoni, L.; Grassi, A.; Zaffagnini, S. Rehabilitation and Return to Sport Assessment after Anterior Cruciate Ligament Injury: Quantifying Joint Kinematics during Complex High-Speed Tasks through Wearable Sensors. Sensors 2021, 21, 2331. [Google Scholar] [CrossRef]
- van der Kruk, E.; Reijne, M.M. Accuracy of Human Motion Capture Systems for Sport Applications; State-of-the-Art Review. Eur. J. Sport Sci. 2018, 18, 806–819. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cluster | Cluster 1 “Low-Risk” | Cluster 1 “Mid-Risk” | Cluster 3 “High-Risk” | p-Value | Eta-Squared |
|---|---|---|---|---|---|
| Exercise | |||||
| No. of trials | 48 | 44 | 19 | ||
| Speed (m/s) | 3.5 ± 0.9 | 3.2 ± 0.8 | 2.7 ± 0.7 | 0.003 | 0.11 |
| Angle (°) | 32.3 ± 14.2 | 40.4 ± 18.6 | 38.5 ± 20.6 | n.s. | 0.05 |
| Game | |||||
| No. of trials | 45 | 22 | 14 | ||
| Speed (m/s) | 3.7 ± 1.0 | 3.0 ± 0.8 | 3.2 ± 0.7 | 0.016 | 0.10 |
| Angle (°) | 29.0 ± 15.0 | 33.7 ± 17.0 | 29.6 ± 15.8 | n.s. | 0.02 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Di Paolo, S.; Nijmeijer, E.M.; Bragonzoni, L.; Gokeler, A.; Benjaminse, A. Definition of High-Risk Motion Patterns for Female ACL Injury Based on Football-Specific Field Data: A Wearable Sensors Plus Data Mining Approach. Sensors 2023, 23, 2176. https://doi.org/10.3390/s23042176
Di Paolo S, Nijmeijer EM, Bragonzoni L, Gokeler A, Benjaminse A. Definition of High-Risk Motion Patterns for Female ACL Injury Based on Football-Specific Field Data: A Wearable Sensors Plus Data Mining Approach. Sensors. 2023; 23(4):2176. https://doi.org/10.3390/s23042176
Chicago/Turabian StyleDi Paolo, Stefano, Eline M. Nijmeijer, Laura Bragonzoni, Alli Gokeler, and Anne Benjaminse. 2023. "Definition of High-Risk Motion Patterns for Female ACL Injury Based on Football-Specific Field Data: A Wearable Sensors Plus Data Mining Approach" Sensors 23, no. 4: 2176. https://doi.org/10.3390/s23042176