
Reliability and Validity of a Wearable Sensing System and Online Gait Analysis Report in Persons after Stroke
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measurement System
2.2. Cloud-Based Gait Analysis Report
- Speed in meters per second was defined as the average walking pace of the gait recording.
- Steps were defined as the total number of steps identified in both legs based on heel strike detection.
- Step length in centimeters was defined as the distance between the heel strike position of the first foot and the heel strike of the opposite foot.
- Step width in centimeters was defined as the medial lateral distance between the heel strikes of the corresponding foot.
- Swing phase in seconds was defined as the time required from toe off to heel strike of one leg.
- Stance phase in seconds was defined as the time elapsed from heel strike to toe off in one leg.
- Hip flexion/extension in degrees were defined as the absolute range of motion from the minimum to the maximum hip joint angle in the sagittal plane.
- Knee flexion/extension in degrees were defined as the absolute range of motion from the minimum to the maximum knee joint angle in the sagittal plane.
- Ankle flexion/extension in degrees were defined as the absolute range of motion from the minimum to the maximum ankle joint angle in the sagittal plane.
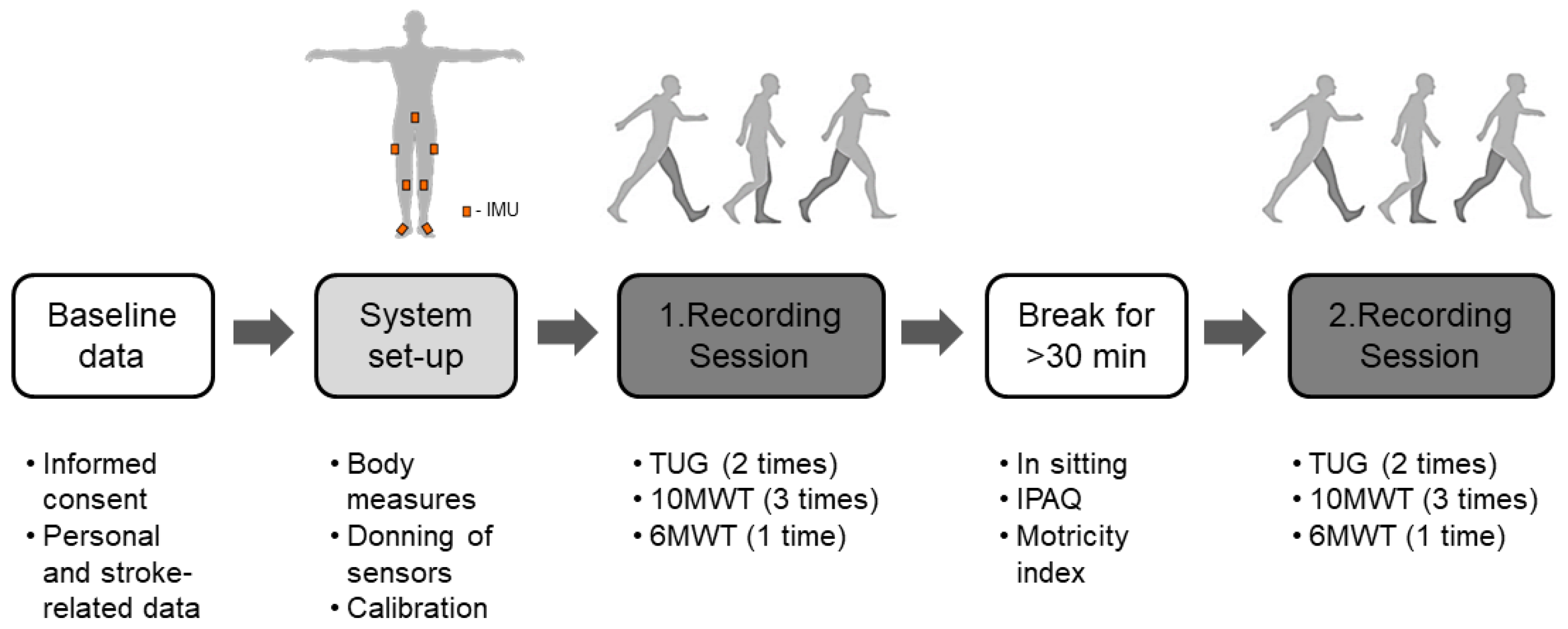
2.3. Experimental Protocol
2.4. Statistical Analysis
3. Results
3.1. System Usability
3.2. Test-Retest Reliability
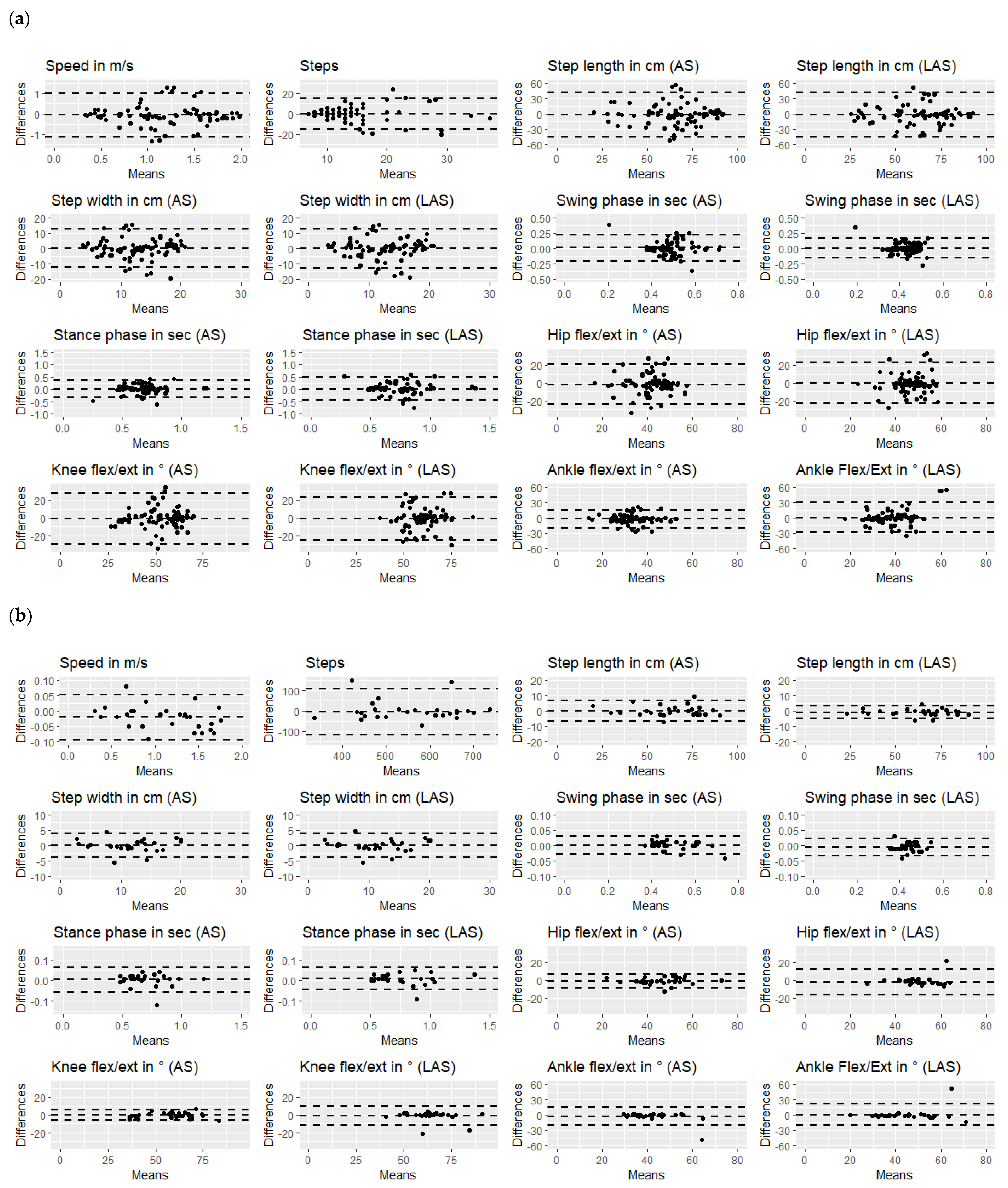
3.3. Hypothesis Testing Reliability
3.4. Discriminability between Affected and Less-Affected Leg and 10MWT and 6MWT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khan, F.; Chevidikunnan, M.F. Prevalence of Balance Impairment and Factors Associated with Balance among Patients with Stroke. A Cross Sectional Retrospective Case Control Study. Healthcare 2021, 9, 320. [Google Scholar] [CrossRef] [PubMed]
- Duncan, P.W.; Zorowitz, R.; Bates, B.; Choi, J.Y.; Glasberg, J.J.; Graham, G.D.; Katz, R.C.; Lamberty, K.; Reker, D. Management of Adult Stroke Rehabilitation Care. Stroke 2005, 36, e100-43. [Google Scholar] [CrossRef] [PubMed]
- Selves, C.; Stoquart, G.; Lejeune, T. Gait Rehabilitation after Stroke: Review of the Evidence of Predictors, Clinical Outcomes and Timing for Interventions. Acta Neurol. Belg. 2020, 120, 783–790. [Google Scholar] [CrossRef]
- Wang, Y.; Mukaino, M.; Ohtsuka, K.; Otaka, Y.; Tanikawa, H.; Matsuda, F.; Tsuchiyama, K.; Yamada, J.; Saitoh, E. Gait Characteristics of Post-Stroke Hemiparetic Patients with Different Walking Speeds. Int. J. Rehabil. Res. 2020, 43, 69–75. [Google Scholar] [CrossRef] [PubMed]
- van Dijk, M.M.; Meyer, S.; Sandstad, S.; Wiskerke, E.; Thuwis, R.; Vandekerckhove, C.; Myny, C.; Ghosh, N.; Beyens, H.; Dejaeger, E.; et al. A Cross-Sectional Study Comparing Lateral and Diagonal Maximum Weight Shift in People with Stroke and Healthy Controls and the Correlation with Balance, Gait and Fear of Falling. PLoS ONE 2017, 12, e0183020. [Google Scholar] [CrossRef] [Green Version]
- Tasseel-Ponche, S.; Yelnik, A.P.; Bonan, I.V. Motor Strategies of Postural Control after Hemispheric Stroke. Neurophysiol. Clin./Clin. Neurophysiol. 2015, 45, 327–333. [Google Scholar] [CrossRef]
- van Ooijen, M.W.; Heeren, A.; Smulders, K.; Geurts, A.C.H.; Janssen, T.W.J.; Beek, P.J.; Weerdesteyn, V.; Roerdink, M. Improved Gait Adjustments after Gait Adaptability Training Are Associated with Reduced Attentional Demands in Persons with Stroke. Exp. Brain Res. 2015, 233, 1007–1018. [Google Scholar] [CrossRef]
- Heshmatollah, A.; Darweesh, S.K.L.; Dommershuijsen, L.J.; Koudstaal, P.J.; Ikram, M.A.; Ikram, M.K. Quantitative Gait Impairments in Patients with Stroke or Transient Ischemic Attack: A Population-Based Approach. Stroke 2020, 51, 2464–2471. [Google Scholar] [CrossRef]
- Balaban, B.; Tok, F. Gait Disturbances in Patients With Stroke. PM&R 2014, 6, 635–642. [Google Scholar] [CrossRef]
- Ward, N.S.; Carmichael, S.T. Blowing up Neural Repair for Stroke Recovery. Stroke 2020, 51, 3169–3173. [Google Scholar] [CrossRef]
- Mohan, D.M.; Khandoker, A.H.; Wasti, S.A.; Ismail Ibrahim Ismail Alali, S.; Jelinek, H.F.; Khalaf, K. Assessment Methods of Post-Stroke Gait: A Scoping Review of Technology-Driven Approaches to Gait Characterization and Analysis. Front. Neurol. 2021, 12, 650024. [Google Scholar] [CrossRef] [PubMed]
- Pan, M.S.; Lin, H.W. A Step Counting Algorithm for Smartphone Users: Design and Implementation. IEEE Sens. J. 2015, 15, 2296–2305. [Google Scholar] [CrossRef]
- Lefeber, N.; Degelaen, M.; Truyers, C.; Safin, I.; Beckwee, D. Validity and Reproducibility of Inertial Physilog Sensors for Spatiotemporal Gait Analysis in Patients With Stroke. IEEE Trans. Neural. Syst. Rehabil. Eng. 2019, 27, 1865–1874. [Google Scholar] [CrossRef] [PubMed]
- Caldas, R.; Mundt, M.; Potthast, W.; Buarque de Lima Neto, F.; Markert, B. A Systematic Review of Gait Analysis Methods Based on Inertial Sensors and Adaptive Algorithms. Gait Posture 2017, 57, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Schepers, M.; Giuberti, M.; Bellusci, G. Xsens MVN: Consistent Tracking of Human Motion Using Inertial Sensing; Technical Report for Xsens Technologies B.V.: Enschede, The Netherlands, 2018. [Google Scholar] [CrossRef]
- Reenalda, J.; Maartens, E.; Homan, L.; Buurke, J.H. Continuous Three Dimensional Analysis of Running Mechanics during a Marathon by Means of Inertial Magnetic Measurement Units to Objectify Changes in Running Mechanics. J. Biomech. 2016, 49, 3362–3367. [Google Scholar] [CrossRef] [PubMed]
- Held, J.P.O.; Klaassen, B.; Eenhoorn, A.; van Beijnum, B.-J.F.; Buurke, J.H.; Veltink, P.H.; Luft, A.R. Inertial Sensor Measurements of Upper-Limb Kinematics in Stroke Patients in Clinic and Home Environment. Front. Bioeng. Biotechnol. 2018, 6, 27. [Google Scholar] [CrossRef] [Green Version]
- van Meulen, F.B.; Klaassen, B.; Held, J.; Reenalda, J.; Buurke, J.H.; van Beijnum, B.-J.F.; Luft, A.; Veltink, P.H. Objective Evaluation of the Quality of Movement in Daily Life after Stroke. Front. Bioeng. Biotechnol. 2016, 3, 210. [Google Scholar] [CrossRef] [Green Version]
- Konrath, J.; Hartman, P.; Engels, C. Xsens MVN Gait Report: The Use of Inertial Motion Capture for Cloud Based Reporting of Gait Parameters; Technical Report for Xsens Technologies B.V.: Enschede, The Netherlands, 2021. [Google Scholar]
- Al-Amri, M.; Nicholas, K.; Button, K.; Sparkes, V.; Sheeran, L.; Davies, J.L. Inertial Measurement Units for Clinical Movement Analysis: Reliability and Concurrent Validity. Sensors 2018, 18, 719. [Google Scholar] [CrossRef] [Green Version]
- Podsiadlo, D.; Richardson, S. The Timed “Up & Go”: A Test of Basic Functional Mobility for Frail Elderly Persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Bohannon, R.W. Reference Values for the Timed Up and Go Test. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Barry, E.; Galvin, R.; Keogh, C.; Horgan, F.; Fahey, T. Is the Timed Up and Go Test a Useful Predictor of Risk of Falls in Community Dwelling Older Adults: A Systematic Review and Meta- Analysis. BMC Geriatr. 2014, 14, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Persson, C.U.; Danielsson, A.; Sunnerhagen, K.S.; Grimby-Ekman, A.; Hansson, P.-O. Timed Up & Go as a Measure for Longitudinal Change in Mobility after Stroke—Postural Stroke Study in Gothenburg (POSTGOT). J. Neuroeng. Rehabil. 2014, 11, 83. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, J.E.; Crowner, B.E.; Kluding, P.M.; Nichols, D.; Rose, D.K.; Yoshida, R.; Pinto Zipp, G. Outcome Measures for Individuals With Stroke: Process and Recommendations From the American Physical Therapy Association Neurology Section Task Force. Phys. Ther. 2013, 93, 1383–1396. [Google Scholar] [CrossRef] [PubMed]
- Collen, F.M.; Wade, D.T.; Bradshaw, C.M. Mobility after Stroke: Reliability of Measures of Impairment and Disability. Int. Disabil. Stud. 1990, 12, 6–9. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R.W. Comfortable and Maximum Walking Speed of Adults Aged 20–79 Years: Reference Values and Determinants. Age Ageing 1997, 26, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Lexell, J.; Flansbjer, U.-B.; Holmbäck, A.M.; Downham, D.; Patten, C. Reliability of gait performance tests in men and women with hemiparesis after stroke. J. Rehabil. Med. 2005, 37, 75–82. [Google Scholar] [CrossRef] [Green Version]
- Salbach, N.M.; Brooks, D.; Romano, J.; Woon, L.; Dolmage, T.E. Cardiorespiratory Responses during the 6-Minute Walk and Ramp Cycle Ergometer Tests and Their Relationship to Physical Activity in Stroke. Neurorehabil. Neural Repair 2014, 28, 111–119. [Google Scholar] [CrossRef]
- De Assis Pereira Cacau, L.; de Santana-Filho, V.J.; Maynard, L.G.; Neto, M.G.; Fernandes, M.; Carvalho, V.O. Reference Values for the Six-Minute Walk Test in Healthy Children and Adolescents: A Systematic Review. Braz. J. Cardiovasc. Surg. 2016, 31, 381–388. [Google Scholar] [CrossRef] [Green Version]
- Borg, G.A. Psychophysical Bases of Perceived Exertion. Med. Sci. Sport. Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International Physical Activity Questionnaire: 12-Country Reliability and Validity. Med. Sci. Sport. Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Rosenberg, D.E.; Bull, F.C.; Marshall, A.L.; Sallis, J.F.; Bauman, A.E. Assessment of Sedentary Behavior With the International Physical Activity Questionnaire. J. Phys. Act. Health. 2008, 5, S30–S44. [Google Scholar] [CrossRef] [PubMed]
- Demeurisse, G.; Demol, O.; Robaye, E. Motor Evaluation in Vascular Hemiplegia. Eur. Neurol. 1980, 19, 382–389. [Google Scholar] [CrossRef] [PubMed]
- Fayazi, M.; Dehkordi, S.N.; Dadgoo, M.; Salehi, M. Test-Retest Reliability of Motricity Index Strength Assessments for Lower Extremity in Post Stroke Hemiparesis. Orig. Res. Med. J. Islam. Repub. Iran 2012, 26, 27–30. [Google Scholar]
- Cameron, D.; Bohannon, R.W. Criterion Validity of Lower Extremity Motricity Index Scores. Clin. Rehabil. 2000, 14, 208–211. [Google Scholar] [CrossRef] [PubMed]
- Mokkink, L.B.; Prinsen, C.A.C.; Bouter, L.M.; de Vet, H.C.W.; Terwee, C.B. The COnsensus-Based Standards for the Selection of Health Measurement INstruments (COSMIN) and How to Select an Outcome Measurement Instrument. Braz. J. Phys. Ther. 2016, 20, 105–113. [Google Scholar] [CrossRef] [Green Version]
- Shrout, P.E.; Fleiss, J.L. Intraclass Correlations: Uses in Assessing Rater Reliability. Psychol. Bull. 1979, 86, 420–428. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Bland, J.M.; Altman, D.G. Measuring Agreement in Method Comparison Studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef]
- Furlan, L.; Sterr, A. The Applicability of Standard Error of Measurement and Minimal Detectable Change to Motor Learning Research—A Behavioral Study. Front. Hum. Neurosci. 2018, 12, 95. [Google Scholar] [CrossRef]
- Akoglu, H. User’s Guide to Correlation Coefficients. Turk. J. Emerg. Med. 2018, 18, 91–93. [Google Scholar] [CrossRef]
- An, S.; Lee, Y.; Shin, H.; Lee, G. Gait Velocity and Walking Distance to Predict Community Walking after Stroke. Nurs. Health Sci. 2015, 17, 533–538. [Google Scholar] [CrossRef]
- Salbach, N.; Author, L.; Professor, A.; Bayley, M.; Brooks, D.; Howe, J.-A.; Educator, C.; MacKay-Lyons, M.; McDonald, A.; Specialist, C.; et al. IWalk a Guide to an Evidence-Informed Approach to Using the 10-Meter and 6-Minute Walk Tests Post-Stroke; University of Toronto: Toronto, ON, Canada, 2018. [Google Scholar]
- Konrath, J.M.; Karatsidis, A.; Martin Schepers, H.; Bellusci, G.; de Zee, M.; Andersen, M.S. Estimation of the Knee Adduction Moment and Joint Contact Force during Daily Living Activities Using Inertial Motion Capture. Sensors 2019, 19, 1681. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, W.; Smuck, M.; Legault, C.; Ith, M.A.; Muaremi, A.; Aminian, K. Gait Symmetry Assessment with a Low Back 3d Accelerometer in Post-Stroke Patients. Sensors 2018, 18, 3322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buurke, J.H.; Nene, A.V.; Kwakkel, G.; Erren-Wolters, V.; IJzerman, M.J.; Hermens, H.J. Recovery of Gait After Stroke: What Changes? Neurorehabil. Neural Repair 2008, 22, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Patterson, S.L.; Forrester, L.W.; Rodgers, M.M.; Ryan, A.S.; Ivey, F.M.; Sorkin, J.D.; Macko, R.F. Determinants of Walking Function After Stroke: Differences by Deficit Severity. Arch. Phys. Med. Rehabil. 2007, 88, 115–119. [Google Scholar] [CrossRef] [PubMed]
- Wüest, S.; Massé, F.; Aminian, K.; Gonzenbach, R.; de Bruin, E.D. Reliability and Validity of the Inertial Sensor-Based Timed “Up and Go” Test in Individuals Affected by Stroke. J. Rehabil. Res. Dev. 2016, 53, 599–610. [Google Scholar] [CrossRef] [PubMed]
- Olney, S.J.; Richardsb, C. Hemiparetic Gait Following Stroke. Part I: Characteristics. Gait Posture 1996, 4, 136–148. [Google Scholar] [CrossRef]
- Pollet, J.; Buraschi, R.; Villafañe, J.H.; Piovanelli, B.; Negrini, S. Gait Parameters Assessed with Inertial Measurement Unit during 6-Minute Walk Test in People after Stroke. Int. J. Rehabil. Res. 2021, 44, 358–363. [Google Scholar] [CrossRef]
- Teufl, W.; Miezal, M.; Taetz, B.; Frohlichi, M.; Bleser, G. Validity of Inertial Sensor Based 3D Joint Kinematics of Static and Dynamic Sport and Physiotherapy Specific Movements. PLoS ONE 2019, 14, e0213064. [Google Scholar] [CrossRef] [Green Version]
- Karatsidis, A.; Richards, R.E.; Konrath, J.M.; van den Noort, J.C.; Schepers, H.M.; Bellusci, G.; Harlaar, J.; Veltink, P.H. Validation of Wearable Visual Feedback for Retraining Foot Progression Angle Using Inertial Sensors and an Augmented Reality Headset. J. Neuroeng. Rehabil. 2018, 15, 78. [Google Scholar] [CrossRef]
- Goulermas, J.Y.; Findlow, A.H.; Nester, C.J.; Liatsis, P.; Zeng, X.-J.; Kenney, L.; Tresadern, P.; Thies, S.B.; Howard, D. An Instance-Based Algorithm With Auxiliary Similarity Information for the Estimation of Gait Kinematics From Wearable Sensors. IEEE Trans. Neural Netw. 2008, 19, 1574–1582. [Google Scholar] [CrossRef] [PubMed]
- Findlow, A.; Goulermas, J.Y.; Nester, C.; Howard, D.; Kenney, L.P.J. Predicting Lower Limb Joint Kinematics Using Wearable Motion Sensors. Gait Posture 2008, 28, 120–126. [Google Scholar] [CrossRef] [PubMed]
- Hansen, C.; Ortlieb, C.; Romijnders, R.; Warmerdam, E.; Welzel, J.; Geritz, J.; Maetzler, W. Reliability of IMU-Derived Temporal Gait Parameters in Neurological Diseases. Sensors 2022, 22, 2304. [Google Scholar] [CrossRef] [PubMed]
- Posada-Ordax, J.; Cosin-Matamoros, J.; Losa-Iglesias, M.E.; Becerro-de-Bengoa-Vallejo, R.; Esteban-Gonzalo, L.; Martin-Villa, C.; Calvo-Lobo, C.; Rodriguez-Sanz, D. Accuracy and Repeatability of Spatiotemporal Gait Parameters Measured with an Inertial Measurement Unit. J. Clin. Med. 2021, 10, 1804. [Google Scholar] [CrossRef] [PubMed]
- Chia Bejarano, N.; Ambrosini, E.; Pedrocchi, A.; Ferrigno, G.; Monticone, M.; Ferrante, S. A Novel Adaptive, Real-Time Algorithm to Detect Gait Events From Wearable Sensors. IEEE Trans. Neural Syst. Rehabil. Eng. 2015, 23, 413–422. [Google Scholar] [CrossRef]
- Kroneberg, D.; Elshehabi, M.; Meyer, A.-C.; Otte, K.; Doss, S.; Paul, F.; Nussbaum, S.; Berg, D.; Kühn, A.A.; Maetzler, W.; et al. Less Is More—Estimation of the Number of Strides Required to Assess Gait Variability in Spatially Confined Settings. Front. Aging Neurosci. 2019, 10, 435. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Francisco, G.E.; Zhou, P. Post-Stroke Hemiplegic Gait: New Perspective and Insights. Front. Physiol. 2018, 9, 1021. [Google Scholar] [CrossRef] [Green Version]
- Allen, J.L.; Kautz, S.A.; Neptune, R.R. Step Length Asymmetry Is Representative of Compensatory Mechanisms Used in Post-Stroke Hemiparetic Walking. Gait Posture 2011, 33, 538–543. [Google Scholar] [CrossRef] [Green Version]
- Garland, S.J.; Willems, D.A.; Ivanova, T.D.; Miller, K.J. Recovery of Standing Balance and Functional Mobility after Stroke. Arch. Phys. Med. Rehabil. 2003, 84, 1753–1759. [Google Scholar] [CrossRef]
- Hagströmer, M.; Oja, P.; Sjöström, M. The International Physical Activity Questionnaire (IPAQ): A Study of Concurrent and Construct Validity. Public Health Nutr. 2006, 9, 755–762. [Google Scholar] [CrossRef]
- Hollman, J.H.; McDade, E.M.; Petersen, R.C. Normative Spatiotemporal Gait Parameters in Older Adults. Gait Posture 2011, 34, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bouchalová, V.; Houben, E.; Tancsik, D.; Schaekers, L.; Meuws, L.; Feys, P. The Influence of an Ankle-Foot Orthosis on the Spatiotemporal Gait Parameters and Functional Balance in Chronic Stroke Patients. J. Phys. Ther. Sci. 2016, 28, 1621–1628. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, X.; Tsujimoto, T.; Kim, B.; Tanaka, K. Association of Arch Height with Ankle Muscle Strength and Physical Performance in Adult Men. Biol. Sport 2017, 2, 119–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, D.; Li, Z.; Xie, W.; Li, D.; Li, Z.; Li, Y. Applications of Nanogenerator-Based Wearable Devices in Orthopedics. Nano Energy 2022, 103, 107762. [Google Scholar] [CrossRef]
- Li, L.; He, R.; Soares, M.S.; Savovic, S.; Hu, X.; Marques, C.; Min, R.; Li, X. Embedded FBG-Based Sensor for Joint Movement Monitoring. IEEE Sens. J. 2021, 21, 26793–26798. [Google Scholar] [CrossRef]
- Moore, S.A.; Boyne, P.; Fulk, G.; Verheyden, G.; Fini, N.A. Walk the Talk: Current Evidence for Walking Recovery After Stroke, Future Pathways and a Mission for Research and Clinical Practice. Stroke 2022, 53, 3494–3505. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | N = 28 |
|---|---|
| Sex, female/male | 9/19 |
| Age in years, mean (SD) | 62.04 (11.68) |
| Body height in cm, mean (SD) | 172.3 (9.89) |
| Body mass index in kg/m2, mean (SD) | 25.76 (3.30) |
| Paretic body side, left/right | 15/13 |
| Months since stroke, mean (SD) | 63.71 (51.85) |
| Initial stroke severity NIHSS, median (Q1-Q3), N = 23 | 8.5 (6–10) |
| Household ambulators (<0.4 m/s), n (%) | 2 (7.14) |
| Limited community ambulators (0.4–0.8 m/s), n (%) | 6 (21.43) |
| Community ambulators (>0.8 m/s), n (%) | 8 (28.57) |
| Normal ambulators (>1.1 m/s), n (%) | 12 (42.86) |
| Assistive device, n (%) | 9 (32) |
| Foot orthoses, n (%) | 4 (14) |
| MI-LE Total, median (Q1–Q3) | 75 (60–83)/100 |
| TUG in seconds, mean (SD) | 15.42 (7.76) |
| 10MWT mean speed in m/s, mean (SD) | 1.03 (0.45) |
| 6MWT in meters, mean (SD) | 384.3 (156.4) |
| IPAQ in MET/week, mean (SD) | 2493 (2014) |
| Gait Metric | 10MWT | 6MWT | ||||
|---|---|---|---|---|---|---|
| Mean SD | ICC (95% CI) | SEM | Mean SD | ICC (95% CI) | SEM | |
| Speed (m/s) | 1.19 ± 0.52 | 0.84 (0.73–0.92) | 0.21 | 1.11 ± 0.45 | 0.99 (0.99–0.99) | 0.03 |
| Steps | 14 ± 7.13 | 0.82 (0.71–0.91) | 3.02 | 554.4 ± 105.08 | 0.86 (0.73–0.93) | 38.92 |
| Step length, cm (AS) | 65.39 ± 20.19 | 0.88 (0.80–0.94) | 6.95 | 62.57 ± 17.40 | 0.98 (0.96–0.99) | 2.25 |
| Step length, cm (LAS) | 63.05 ± 20.26 | 0.87 (0.81–0.92) | 7.94 | 62.26 ± 17.67 | 0.99 (0.98–0.99) | 1.56 |
| Step width, cm (AS) | 12.89 ± 5.44 | 0.80 (0.71–0.87) | 1.80 | 11.34 ± 4.91 | 0.92 (0.84–0.96) | 1.37 |
| Step width, cm (LAS) | 12.81 ± 5.49 | 0.80 (0.71–0.87) | 1.83 | 11.34 ± 4.91 | 0.92 (0.84–0.96) | 1.38 |
| Swing phase, s (AS) | 0.48 ± 0.10 | 0.60 (0.43–0.78) | 0.06 | 0.49 ± 0.09 | 0.99 (0.97–0.99) | 0.01 |
| Swing phase, s (LAS) | 0.43 ± 0.07 | 0.46 (0.28–0.67) | 0.05 | 0.44 ± 0.05 | 0.95 (0.90–0.98) | 0.01 |
| Stance phase, s (AS) | 0.66 ± 0.18 | 0.67 (0.50–0.82) | 0.10 | 0.69 ± 0.17 | 0.98 (0.97–0.99) | 0.02 |
| Stance phase, s (LAS) | 0.71 ± 0.23 | 0.64 (0.47–0.80) | 0.13 | 0.75 ± 0.22 | 0.99 (0.98–0.99) | 0.02 |
| Hip flex/ext, ° (AS) | 41.28 ± 9.96 | 0.87 (0.79–0.94) | 3.53 | 46.31 ± 10.34 | 0.93 (0.86–0.97) | 2.73 |
| Hip flex/ext, ° (LAS) | 46.46 ± 9.33 | 0.73 (0.58–0.86) | 4.85 | 51.55 ± 10.72 | 0.76 (0.54–0.88) | 5.28 |
| Knee flex/ext, ° (AS) | 51.76 ± 13.22 | 0.88 (0.80–0.94) | 4.54 | 58.10 ± 12.84 | 0.97 (0.94–0.99) | 2.09 |
| Knee flex/ext, ° (LAS) | 59.44 ± 10.72 | 0.84 (0.74–0.92) | 4.25 | 64.21 ± 11.03 | 0.89 (0.78–0.95) | 3.69 |
| Ankle flex/ext, ° (AS) | 33.21 ± 8.78 | 0.88 (0.79–0.94) | 3.05 | 42.71 ± 10.77 | 0.63 (0.35–0.81) | 6.56 |
| Ankle flex/ext, ° (LAS) | 38.81 ± 11.20 | 0.70 (0.54–0.84) | 6.13 | 44.86 ± 12.74 | 0.68 (0.42–0.84) | 7.19 |
| Gait Metric | 10MWT | 6MWT | Levene | ANOVA | |||
|---|---|---|---|---|---|---|---|
| Affected Leg | Less-Affected Leg | Affected Leg | Less-Affected Leg | Leg | Test | ||
| Mean SD | Mean SD | Mean SD | Mean SD | p-Value | p-Value | p-Value | |
| Step length, cm | 65.39 ± 20.19 | 63.05 ± 20.26 | 62.57 ± 17.4 | 62.26 ± 17.67 | 0.178 | 0.335 | 0.400 |
| Step width, cm | 12.89 ± 5.44 | 12.81 ± 5.49 | 11.34 ± 4.91 | 11.34 ± 4.91 | 0.452 | 0.905 | 0.010 |
| Swing phase, s | 0.48 ± 0.1 | 0.43 ± 0.07 | 0.49 ± 0.09 | 0.44 ± 0.05 | <0.001 | <0.001 | 0.126 |
| Stance phase, s | 0.66 ± 0.18 | 0.71 ± 0.22 | 0.69 ± 0.17 | 0.74 ± 0.22 | 0.017 | 0.007 | 0.135 |
| Hip flex/ext, ° | 41.28 ± 9.96 | 46.46 ± 9.33 | 46.31 ± 10.34 | 51.55 ± 10.72 | 0.214 | <0.001 | <0.001 |
| Knee flex/ext, ° | 51.76 ± 13.22 | 59.44 ± 10.72 | 58.1 ± 12.84 | 64.21 ± 11.03 | <0.001 | <0.001 | <0.001 |
| Ankle flex/ext, ° | 33.21 ± 8.78 | 38.81 ± 11.2 | 42.71 ± 10.77 | 44.86 ± 12.74 | 0.157 | <0.001 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schwarz, A.; Al-Haj Husain, A.; Einaudi, L.; Thürlimann, E.; Läderach, J.; Awai Easthope, C.; Held, J.P.O.; Luft, A.R. Reliability and Validity of a Wearable Sensing System and Online Gait Analysis Report in Persons after Stroke. Sensors 2023, 23, 624. https://doi.org/10.3390/s23020624
Schwarz A, Al-Haj Husain A, Einaudi L, Thürlimann E, Läderach J, Awai Easthope C, Held JPO, Luft AR. Reliability and Validity of a Wearable Sensing System and Online Gait Analysis Report in Persons after Stroke. Sensors. 2023; 23(2):624. https://doi.org/10.3390/s23020624
Chicago/Turabian StyleSchwarz, Anne, Adib Al-Haj Husain, Lorenzo Einaudi, Eva Thürlimann, Julia Läderach, Chris Awai Easthope, Jeremia P. O. Held, and Andreas R. Luft. 2023. "Reliability and Validity of a Wearable Sensing System and Online Gait Analysis Report in Persons after Stroke" Sensors 23, no. 2: 624. https://doi.org/10.3390/s23020624