
Continuous Monitoring of Health and Mobility Indicators in Patients with Cardiovascular Disease: A Review of Recent Technologies

Abstract
:1. Introduction
2. Physical Activity Monitoring
2.1. Step Counting
2.2. Raw Accelerometer Data
2.3. Gyroscope Data
2.4. Magnetometer Data
3. Indoor Home Tracking
3.1. Localisation Techniques
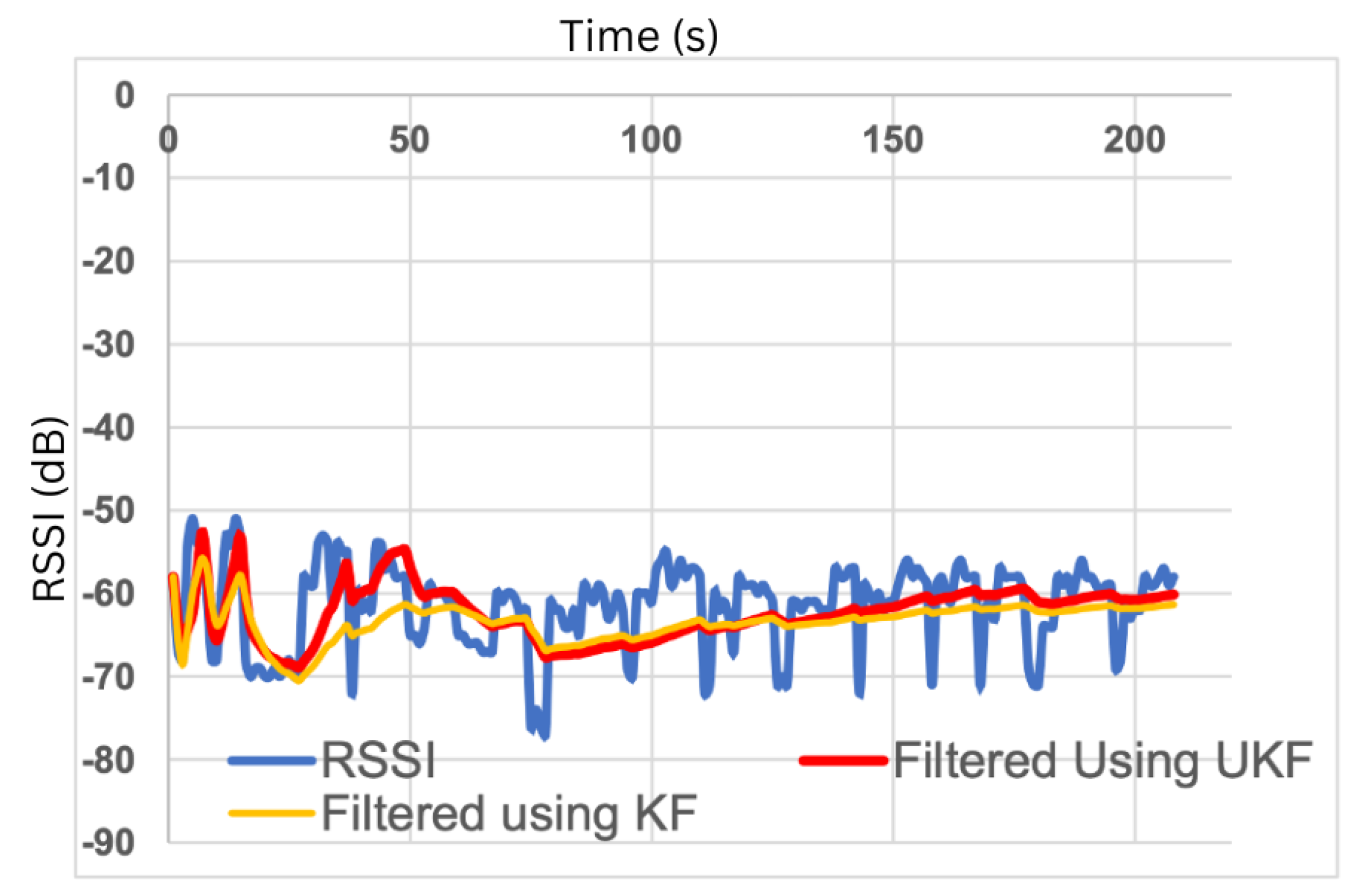
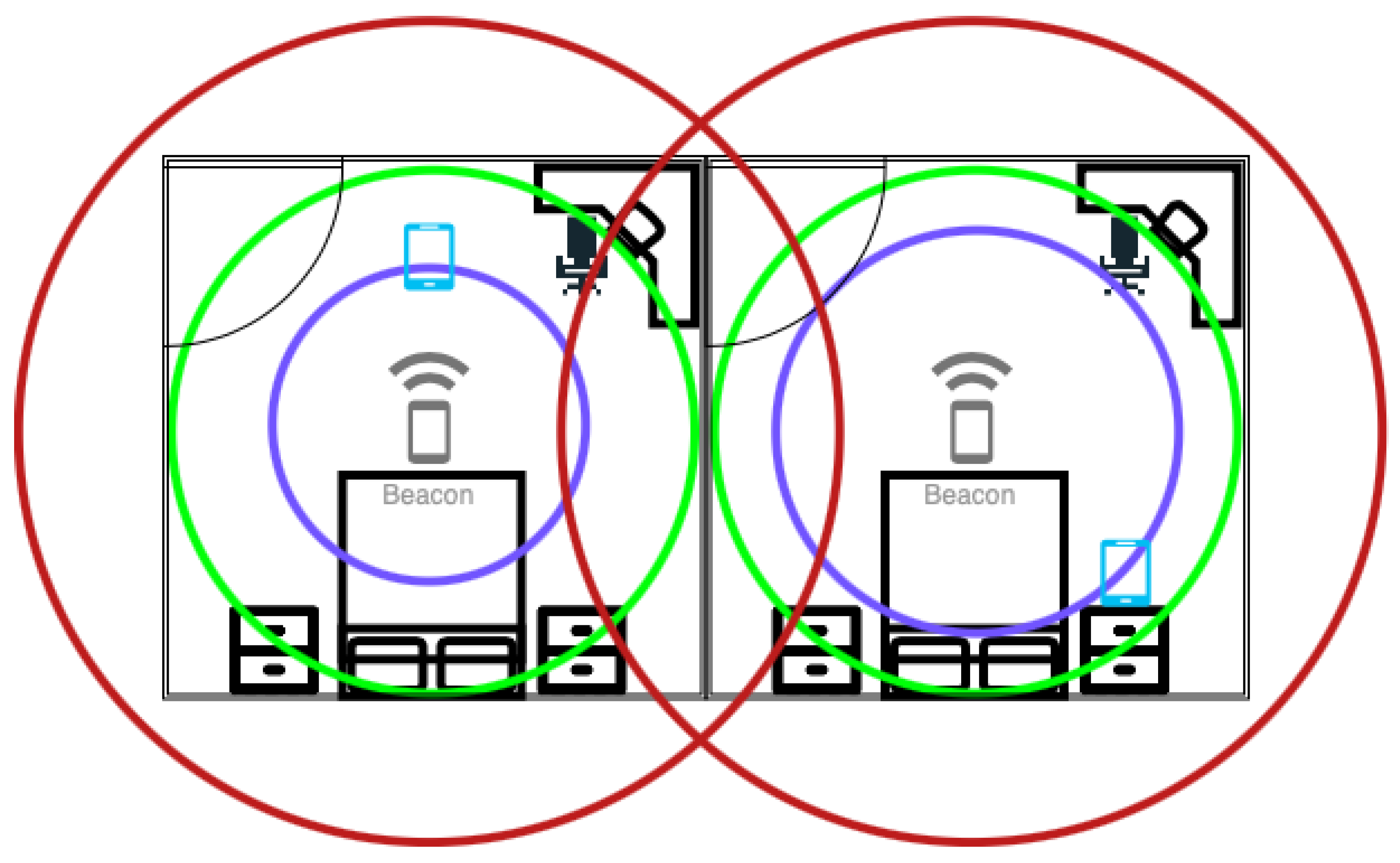
3.1.1. Received Signal Strength Indicator (RSSI)
3.1.2. Channel State Information (CSI)
3.1.3. Angle of Arrival (AoA)
3.1.4. Time of Arrival (ToA)
3.1.5. Return Time of Flight (RToF)
3.1.6. Time Difference of Arrival (TDoA)
3.2. Localisation Methods
3.2.1. Range-Based Method
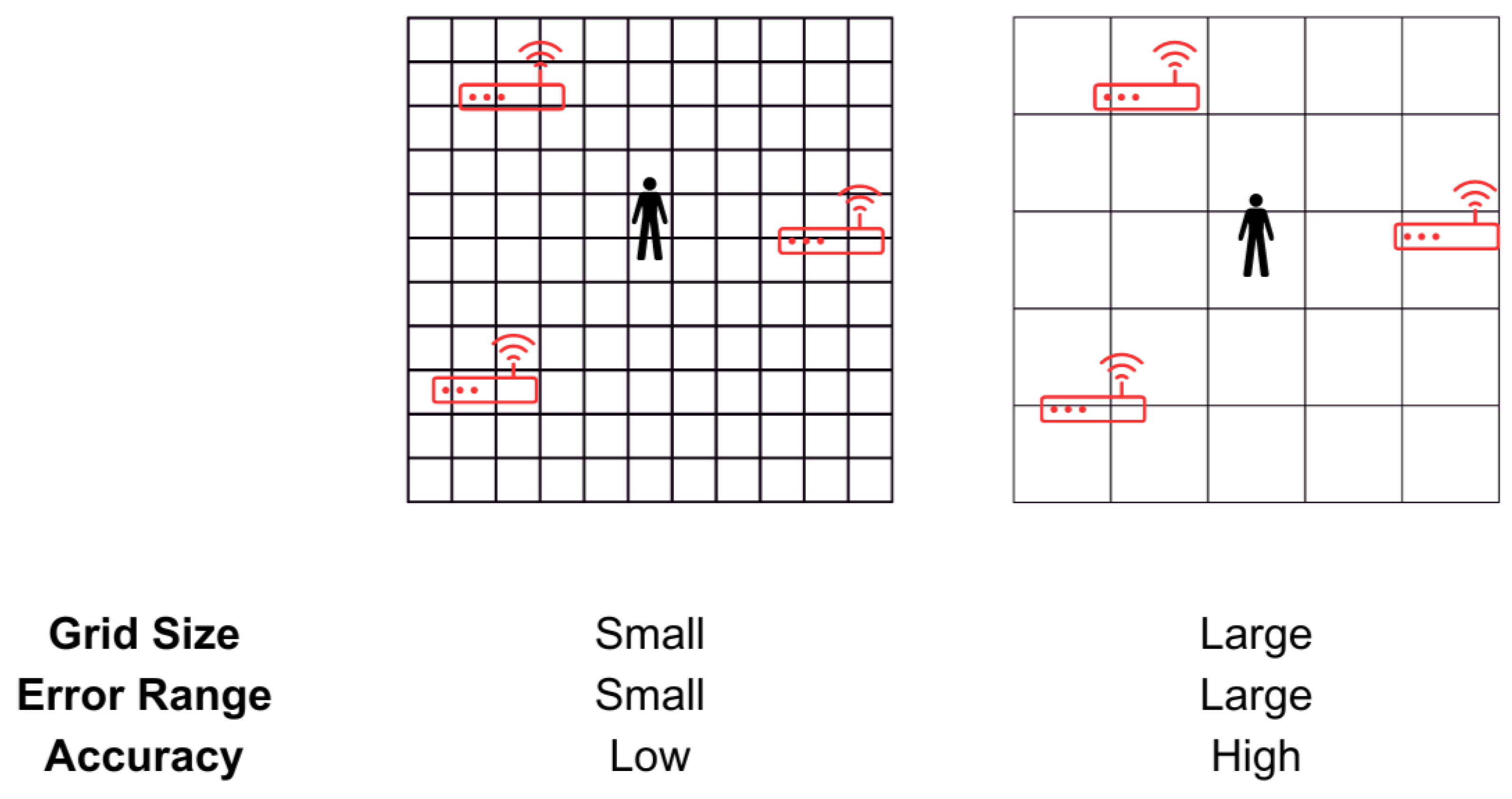
3.2.2. Fingerprinting Method
3.3. Indoor Localisation Technologies
3.3.1. Bluetooth Low Energy (BLE)
3.3.2. WiFi
3.3.3. Radio Frequency Identification Device (RFID)
3.3.4. ZigBee
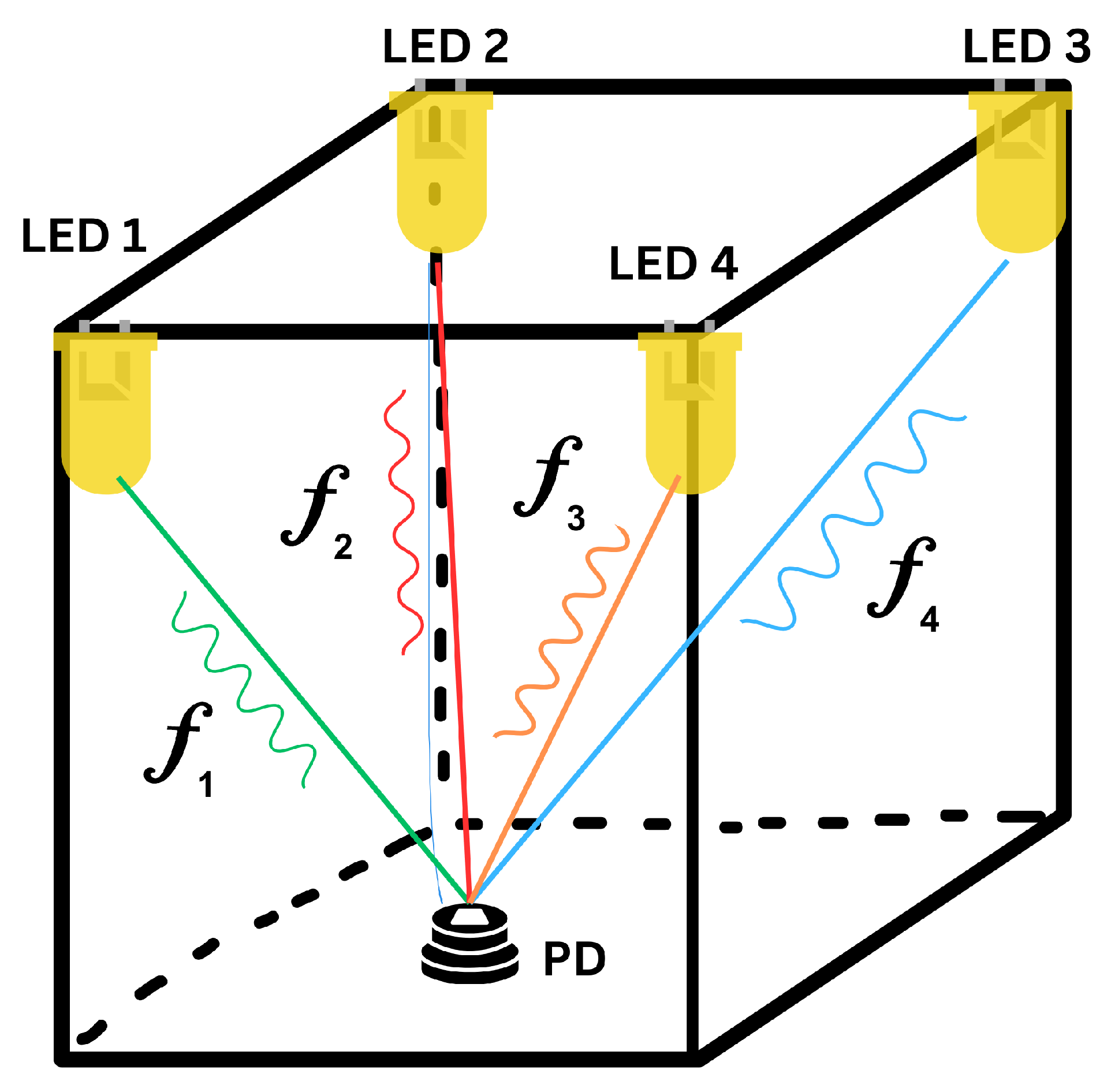
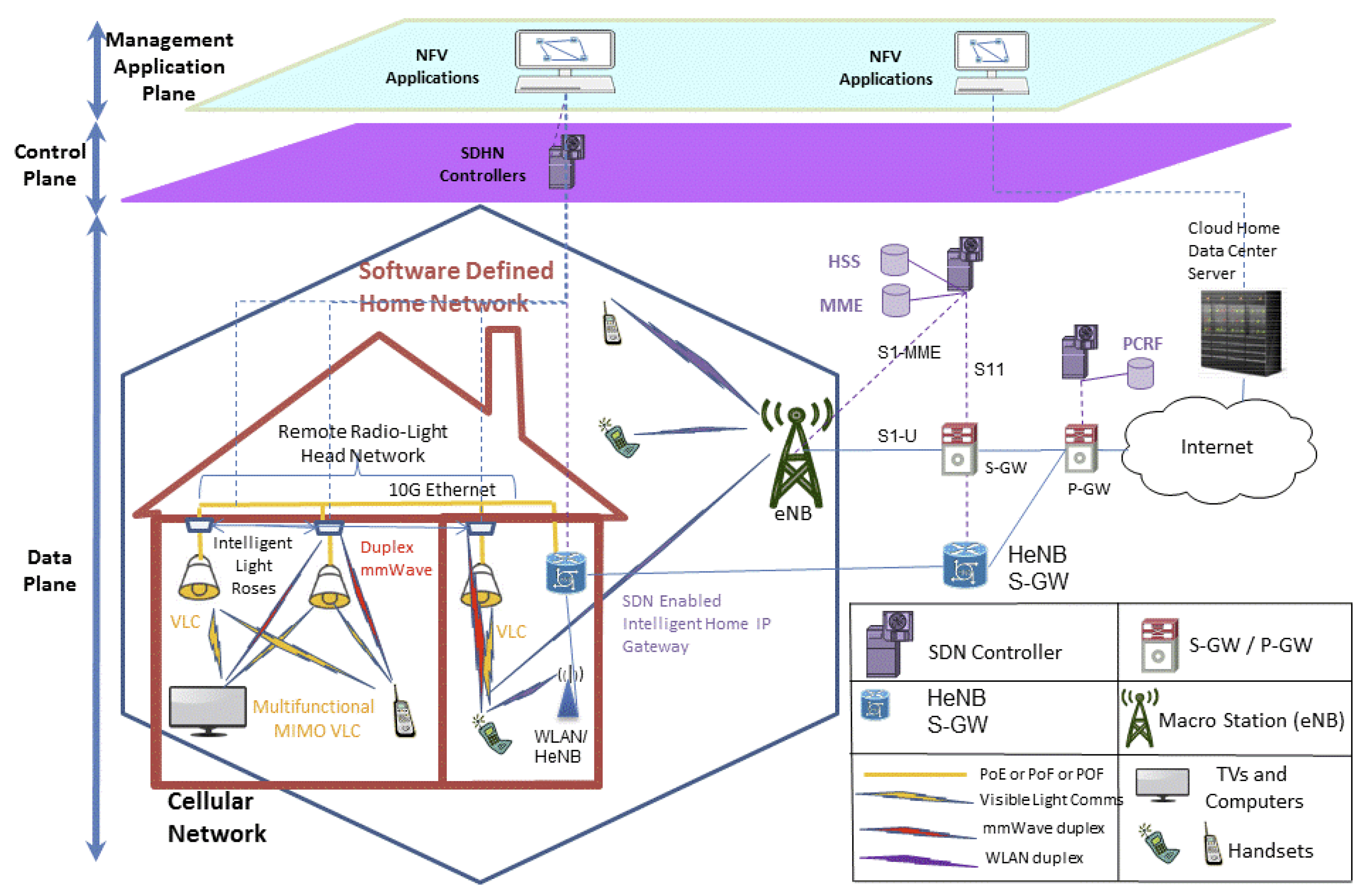
3.3.5. Visible Light Communication (VLC)
3.3.6. Acoustic Signal
3.3.7. Ultrasound
3.3.8. Ultrawideband (UWB)
3.3.9. The Fifth Generation of Mobile Communications (5G)
3.3.10. Light Detection and Ranging (LiDAR)
3.4. Requirements for Combining Different Methods
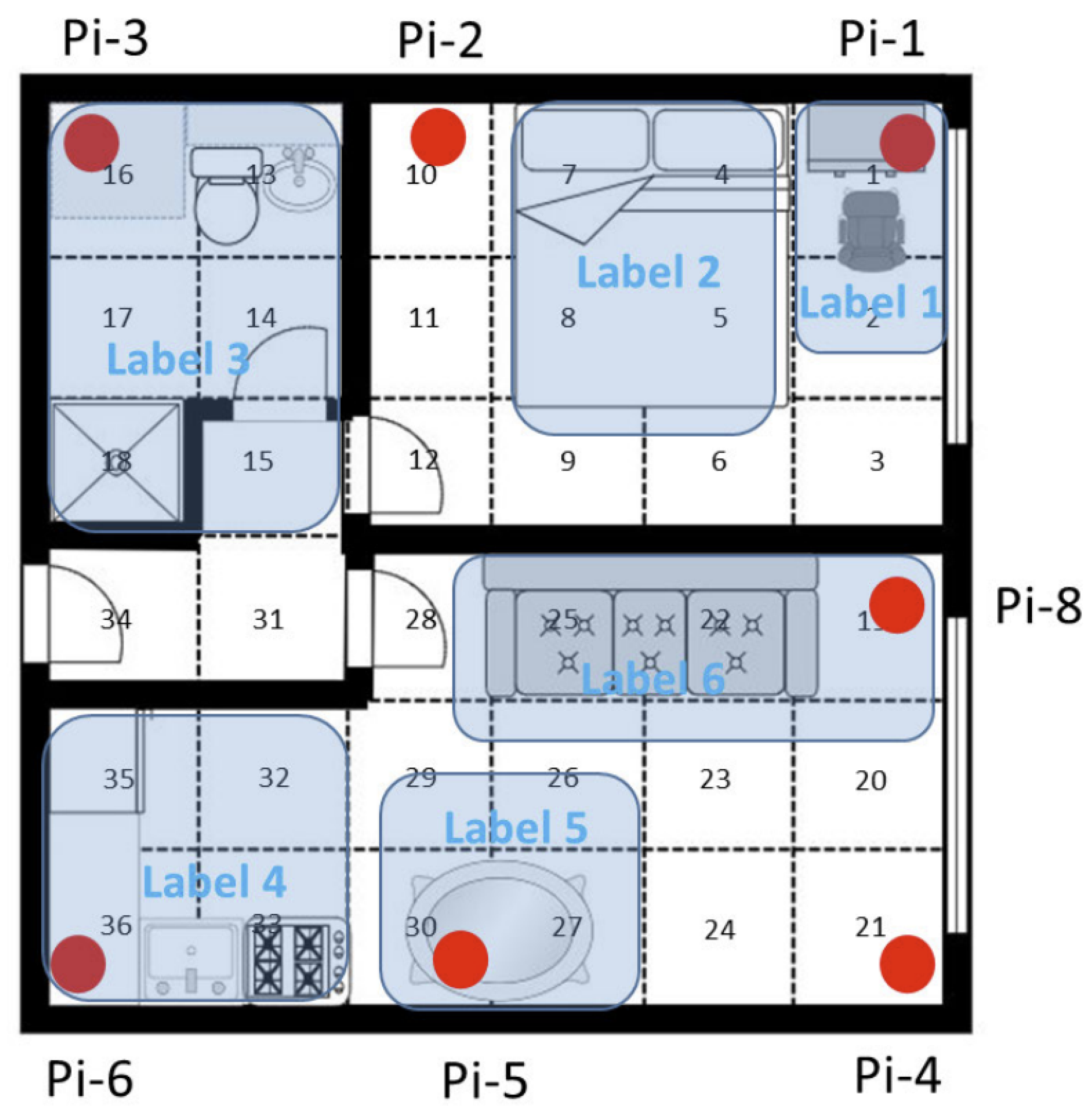
3.5. Examples of Indoor Localisation Systems Used within the Healthcare Domain
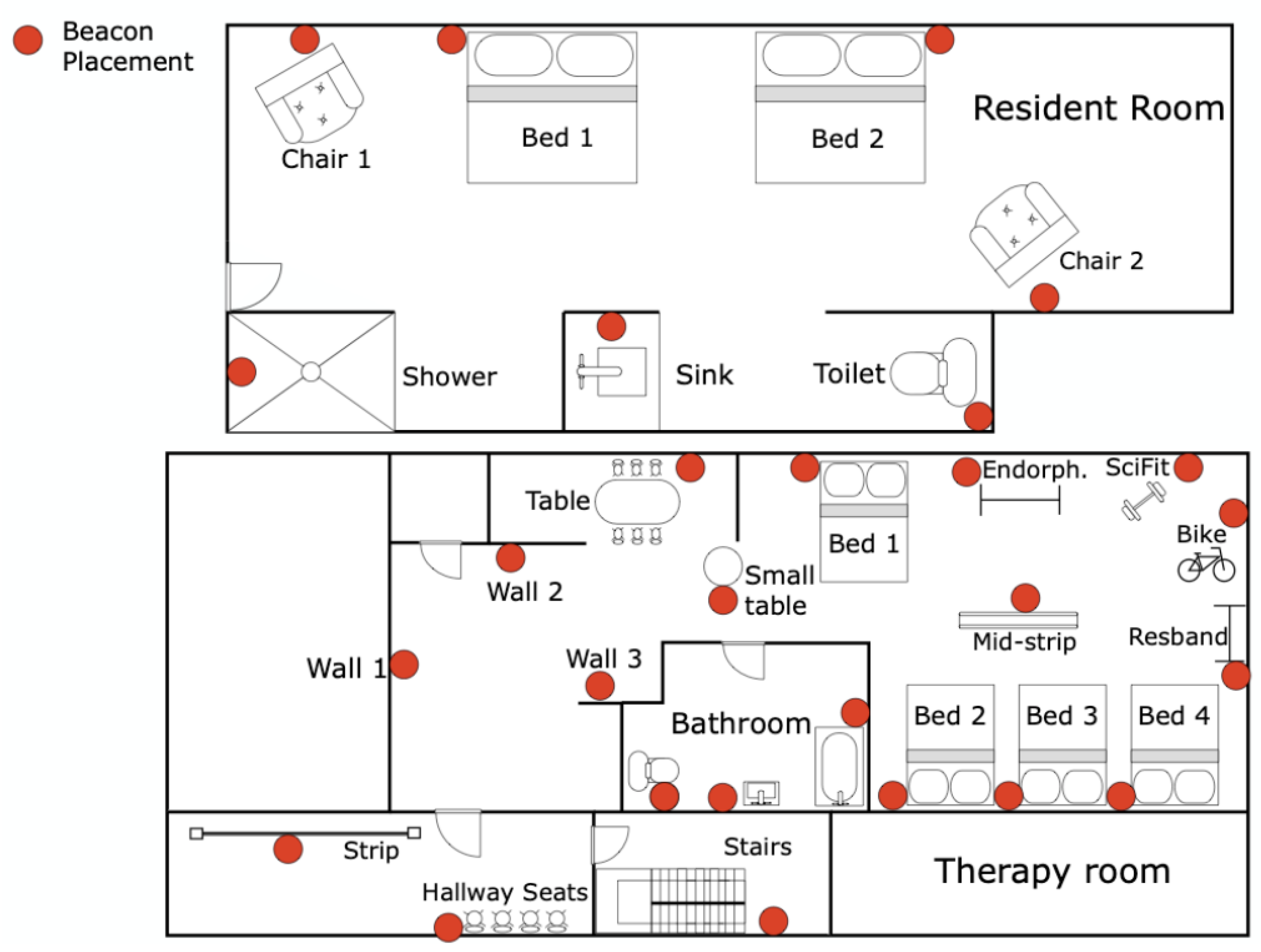
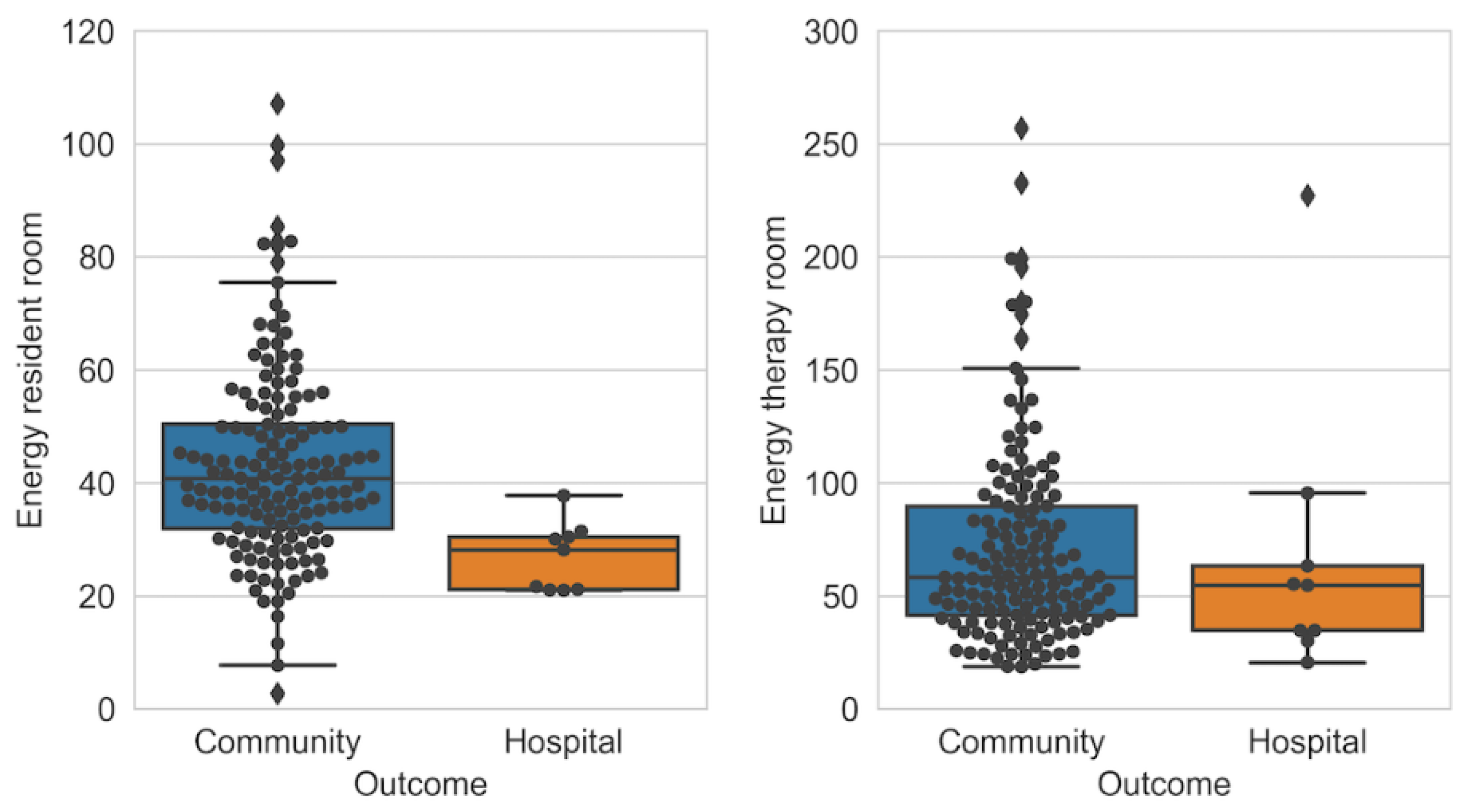
3.5.1. Tracking Patients in a Post-Acute Rehabilitation Centre
3.5.2. Vesta: Tracking Patients Undergoing Heart Valve Surgery
4. Physiological Parameters
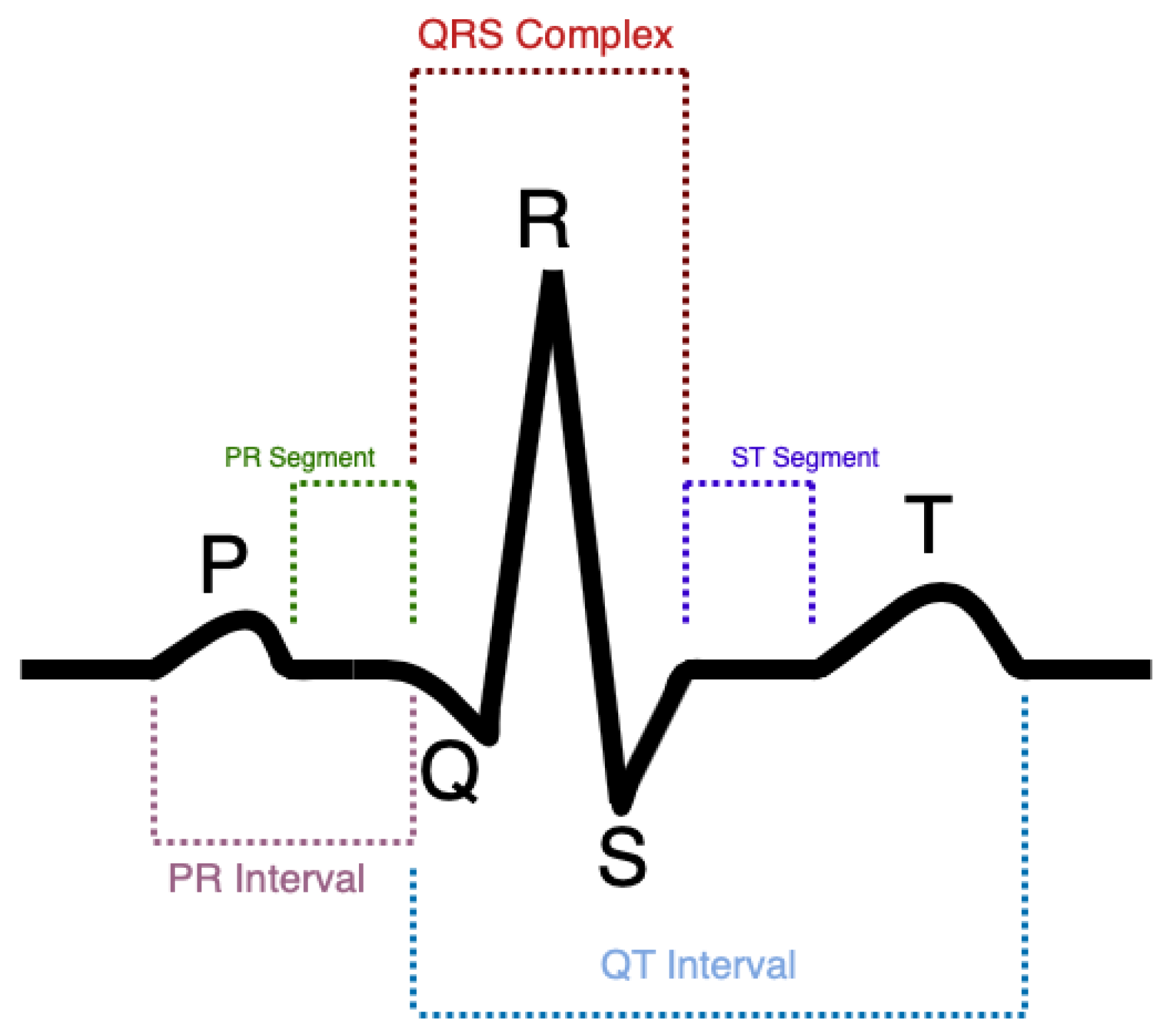
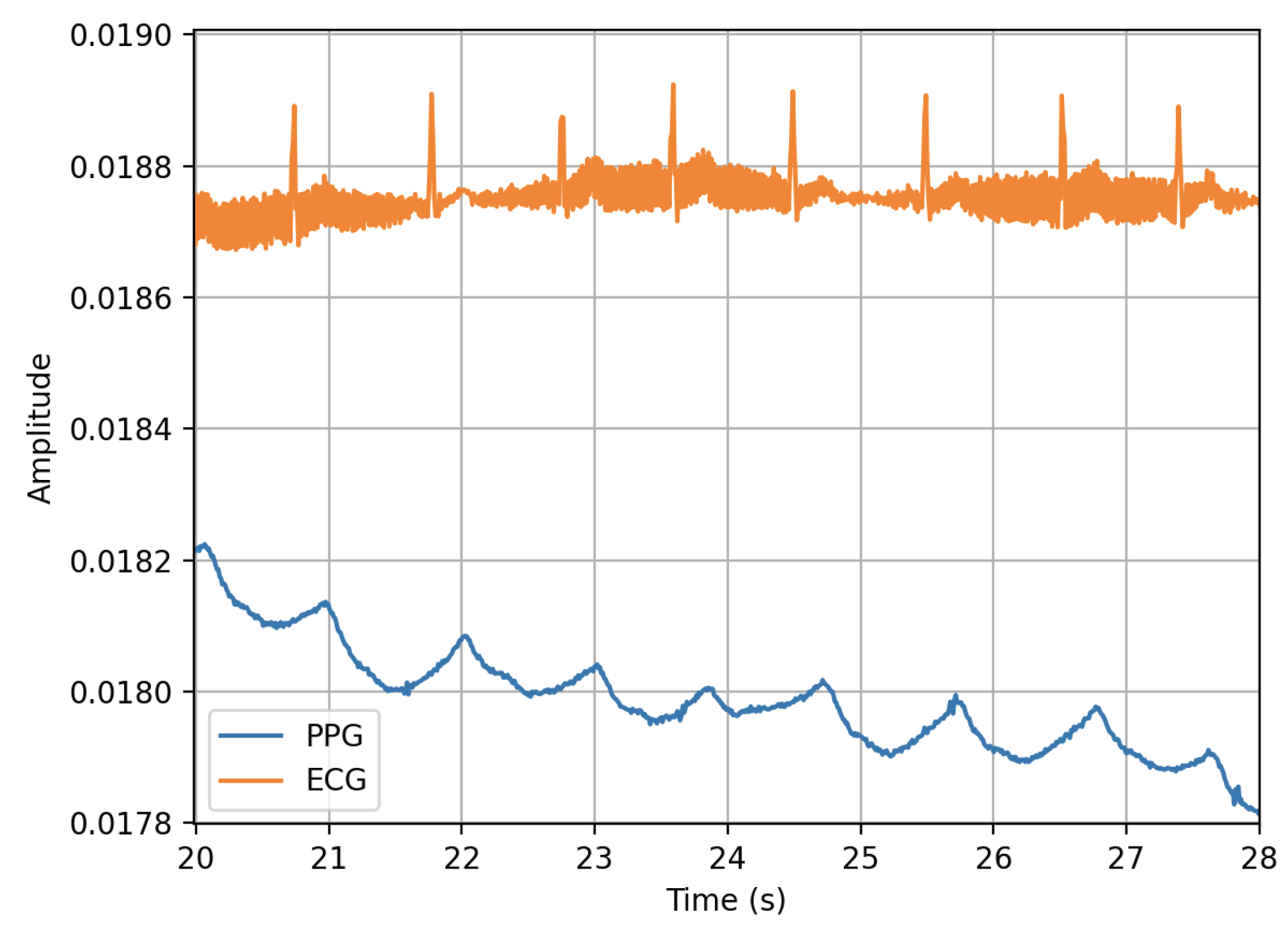
4.1. Electrocardiogram
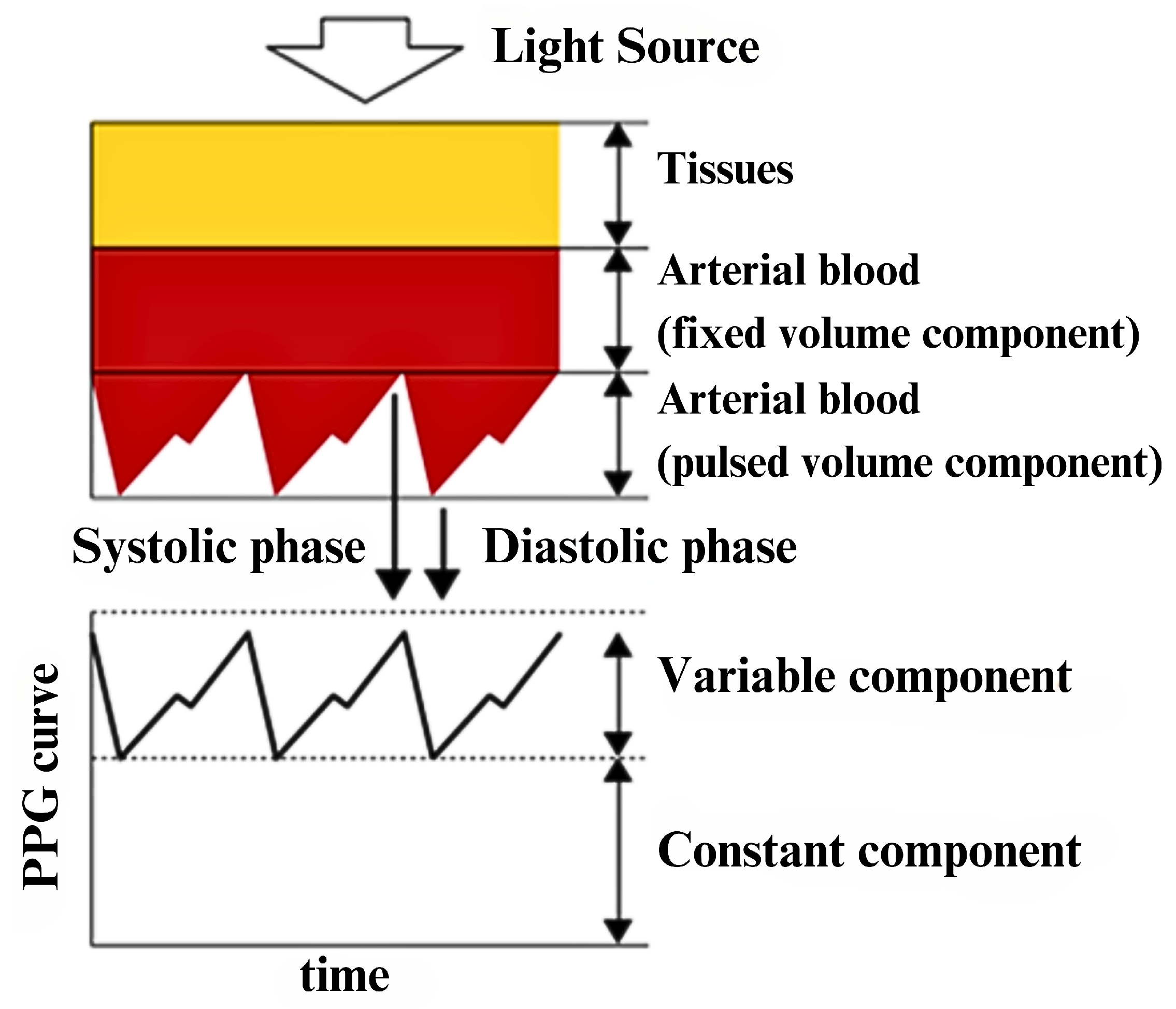
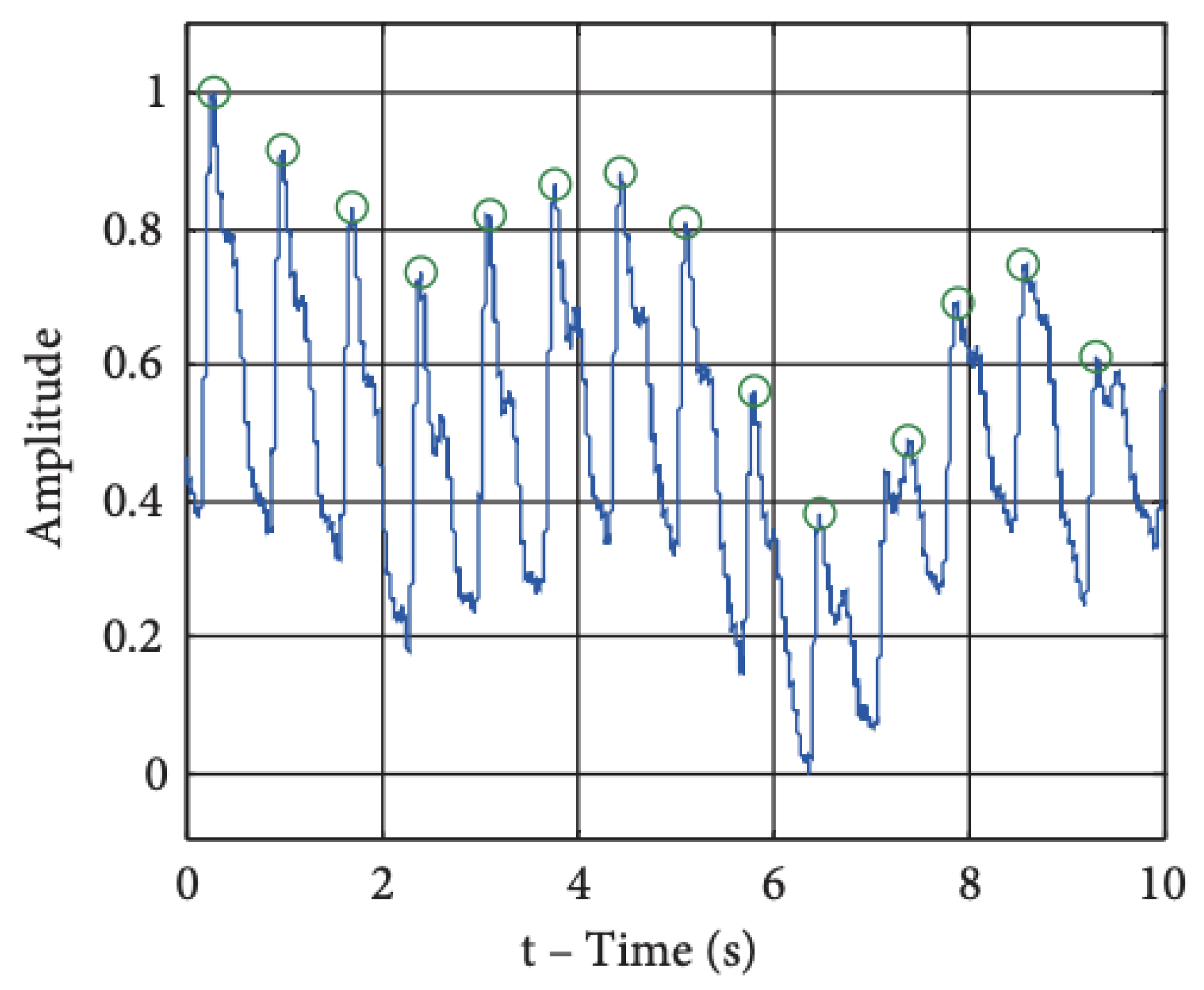
4.2. Photoplethysmography (PPG)
4.3. Heart Rate
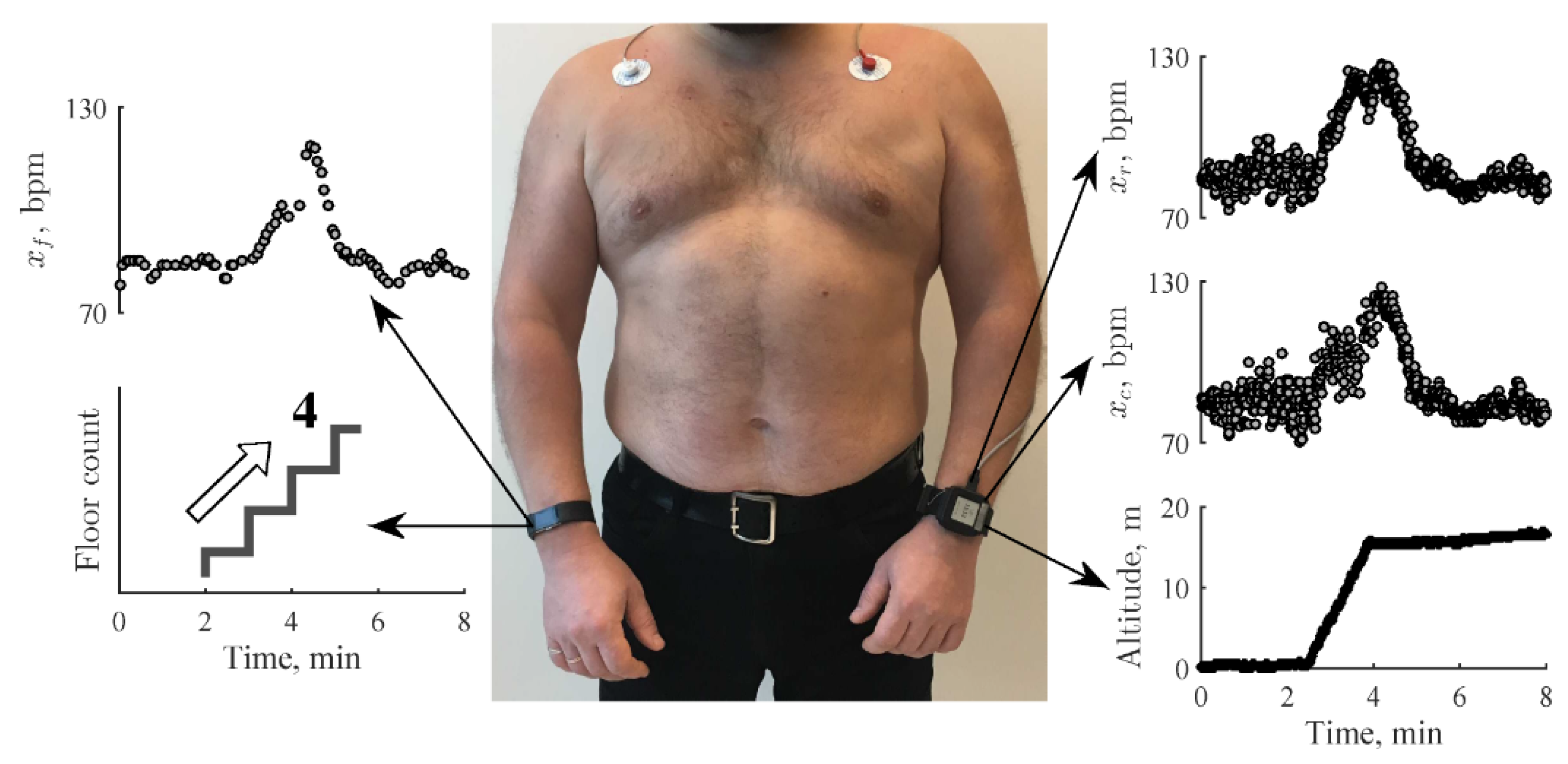
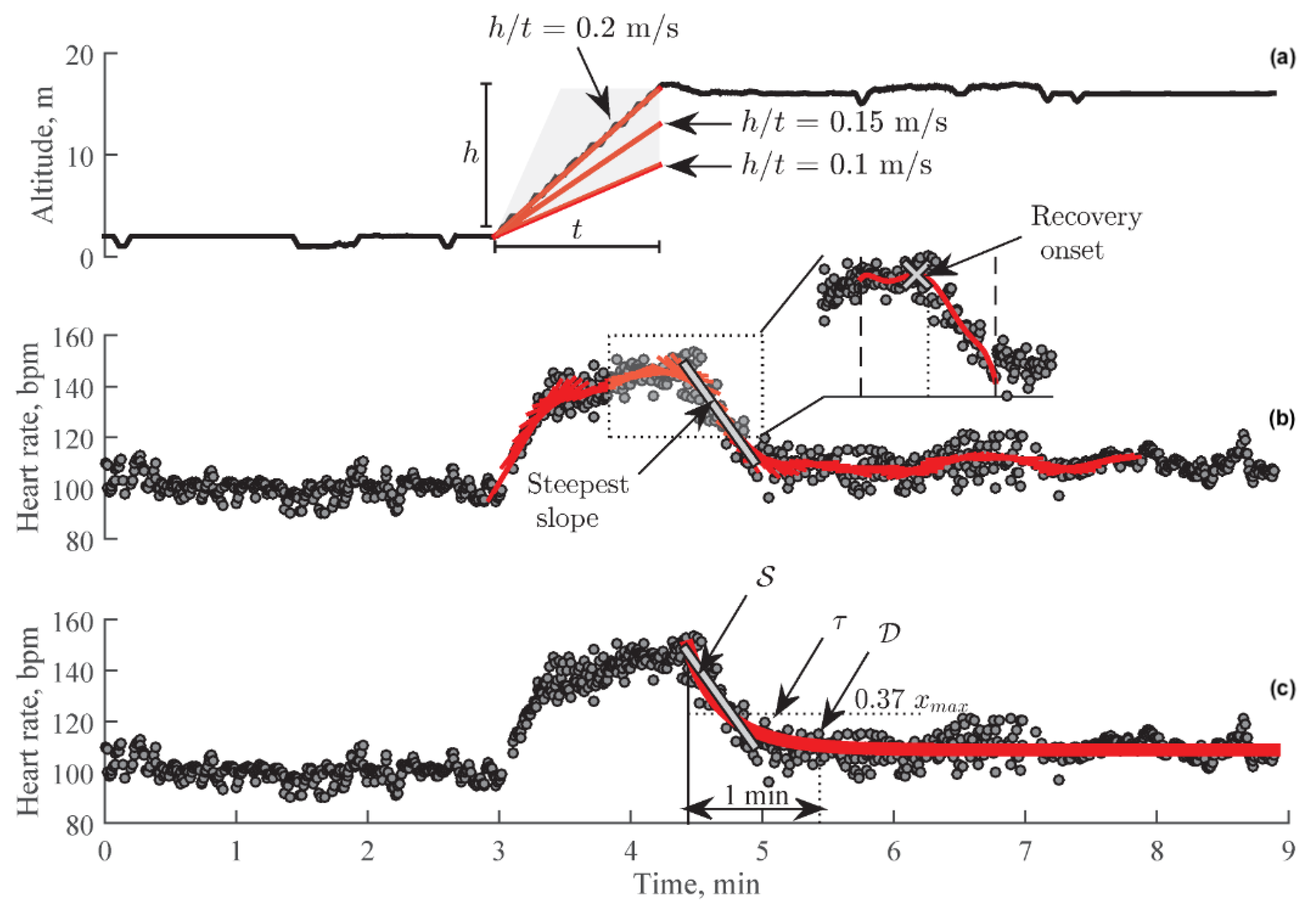
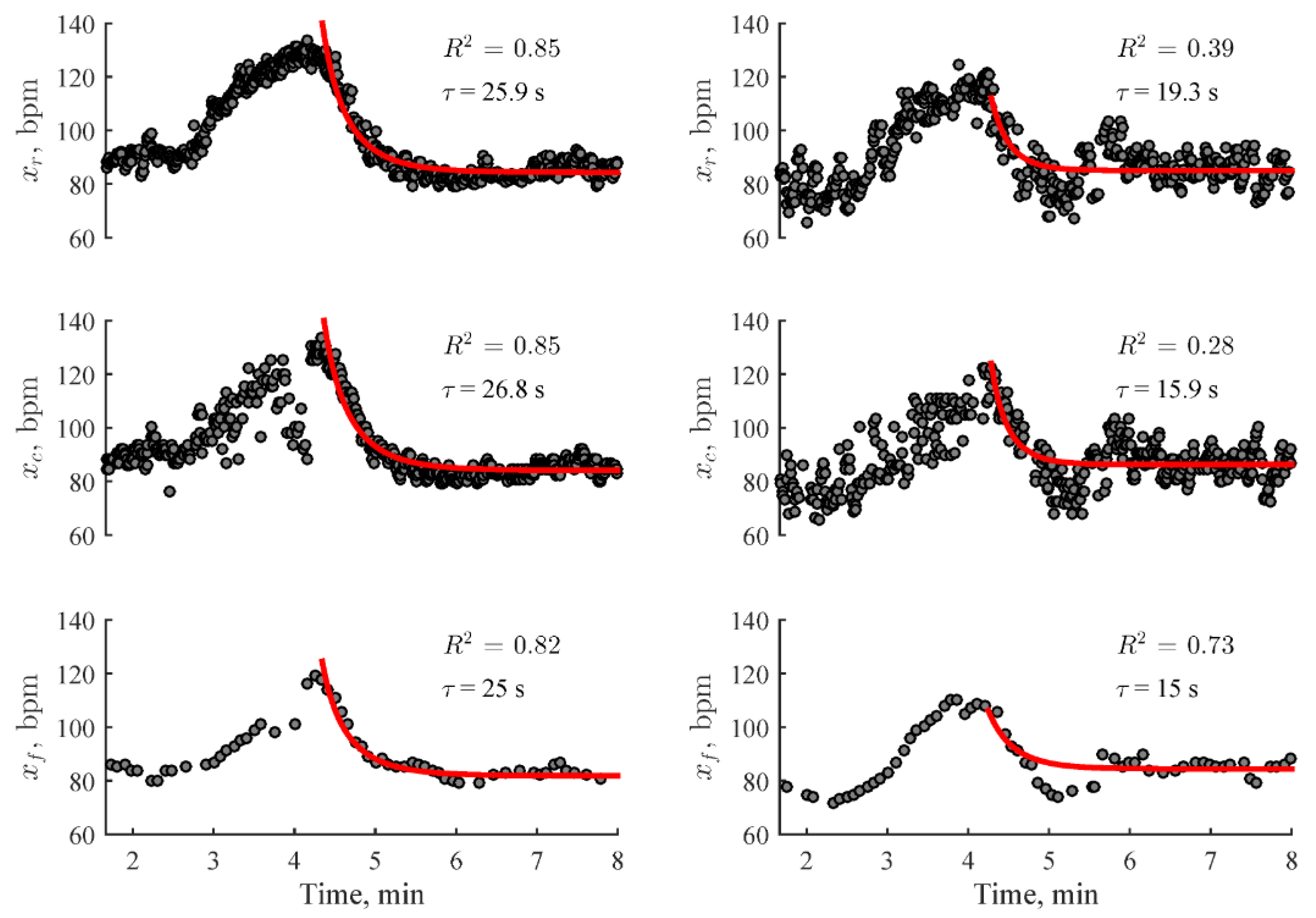
4.4. Heart Rate Recovery (HRR)
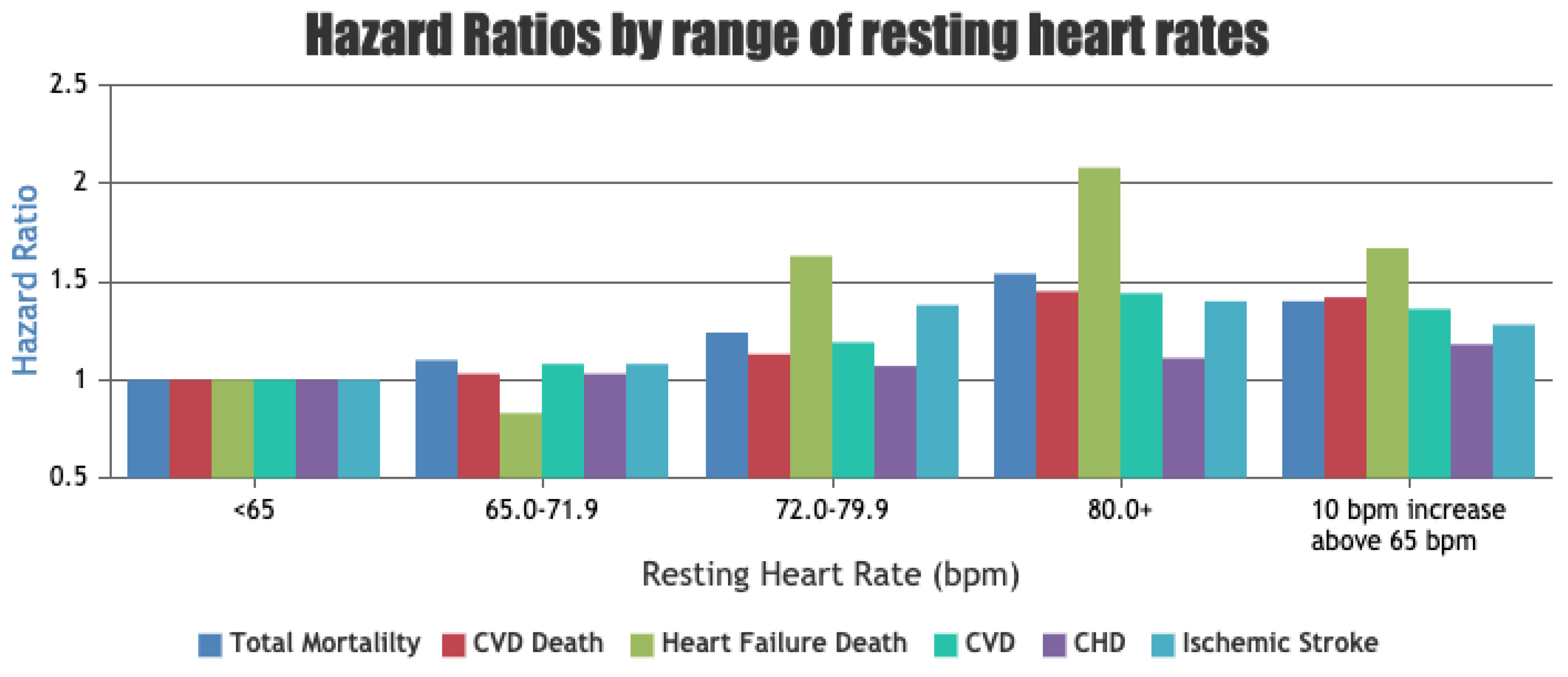
4.5. Resting Heart Rate (RHR)
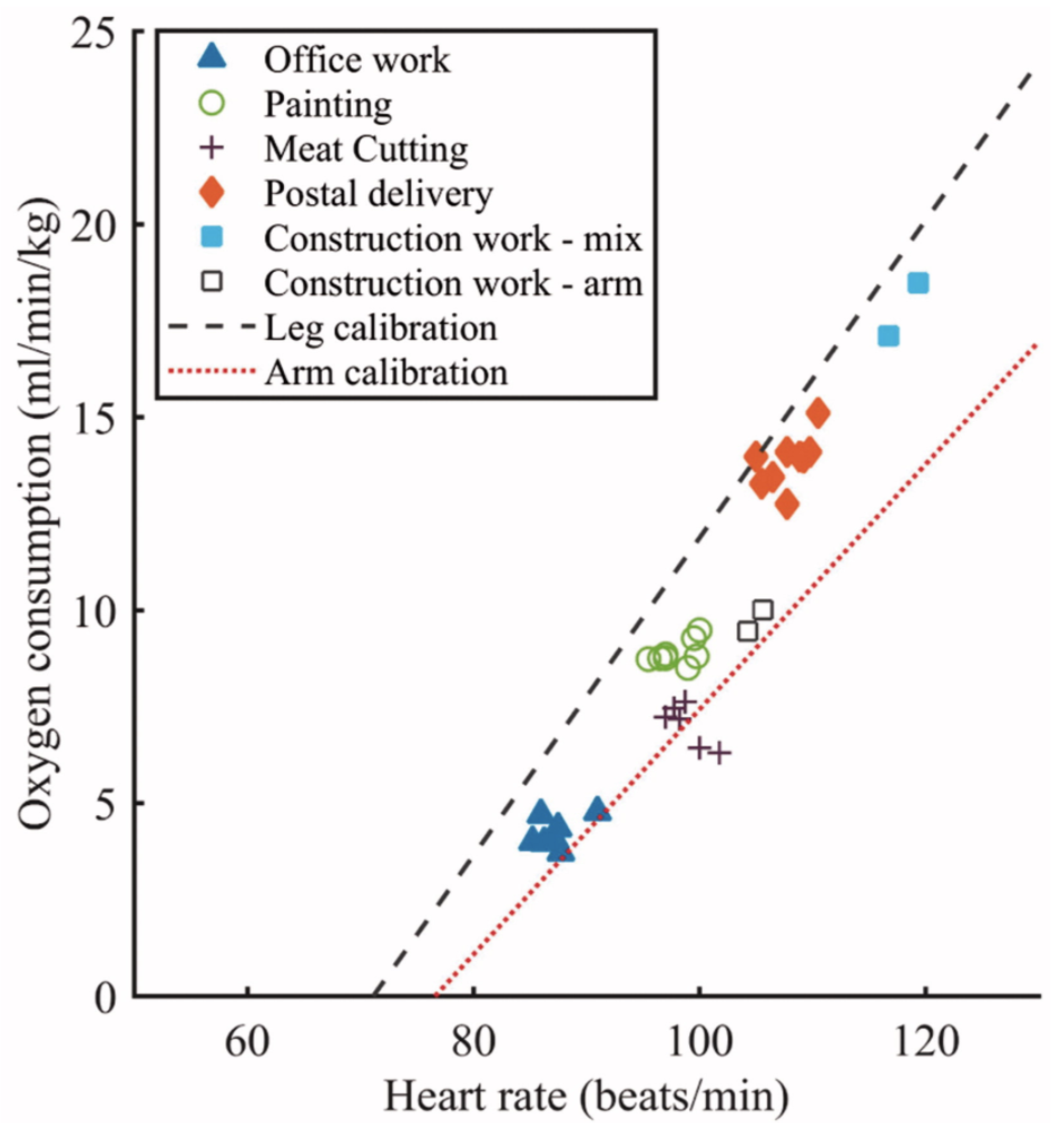
4.6. Energy Expenditure Using HR
4.6.1. PAI—Personalised Activity Intelligence
4.6.2. Beta-Blocker Patient Model
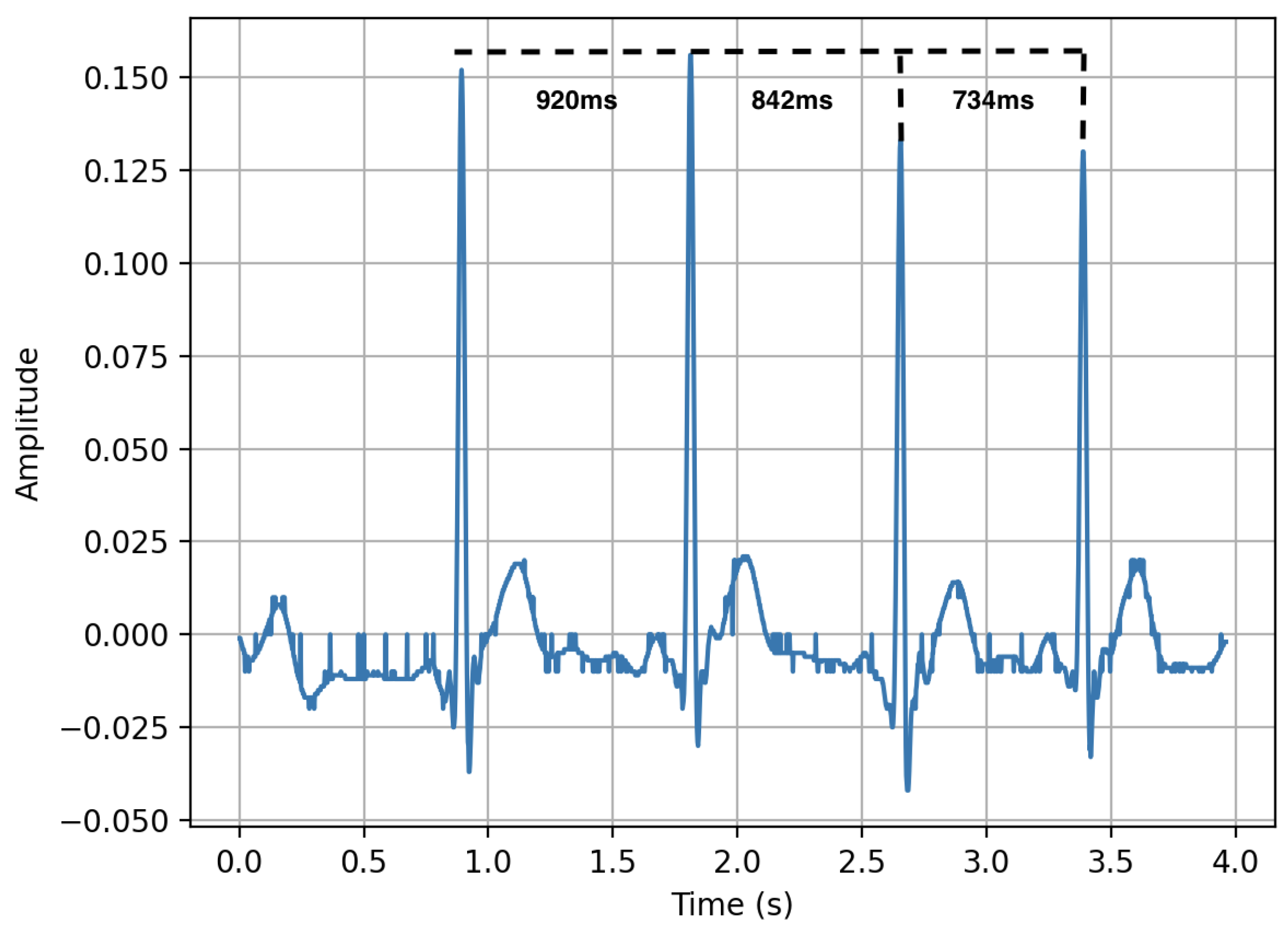
4.7. Heart Rate Variability (HRV)
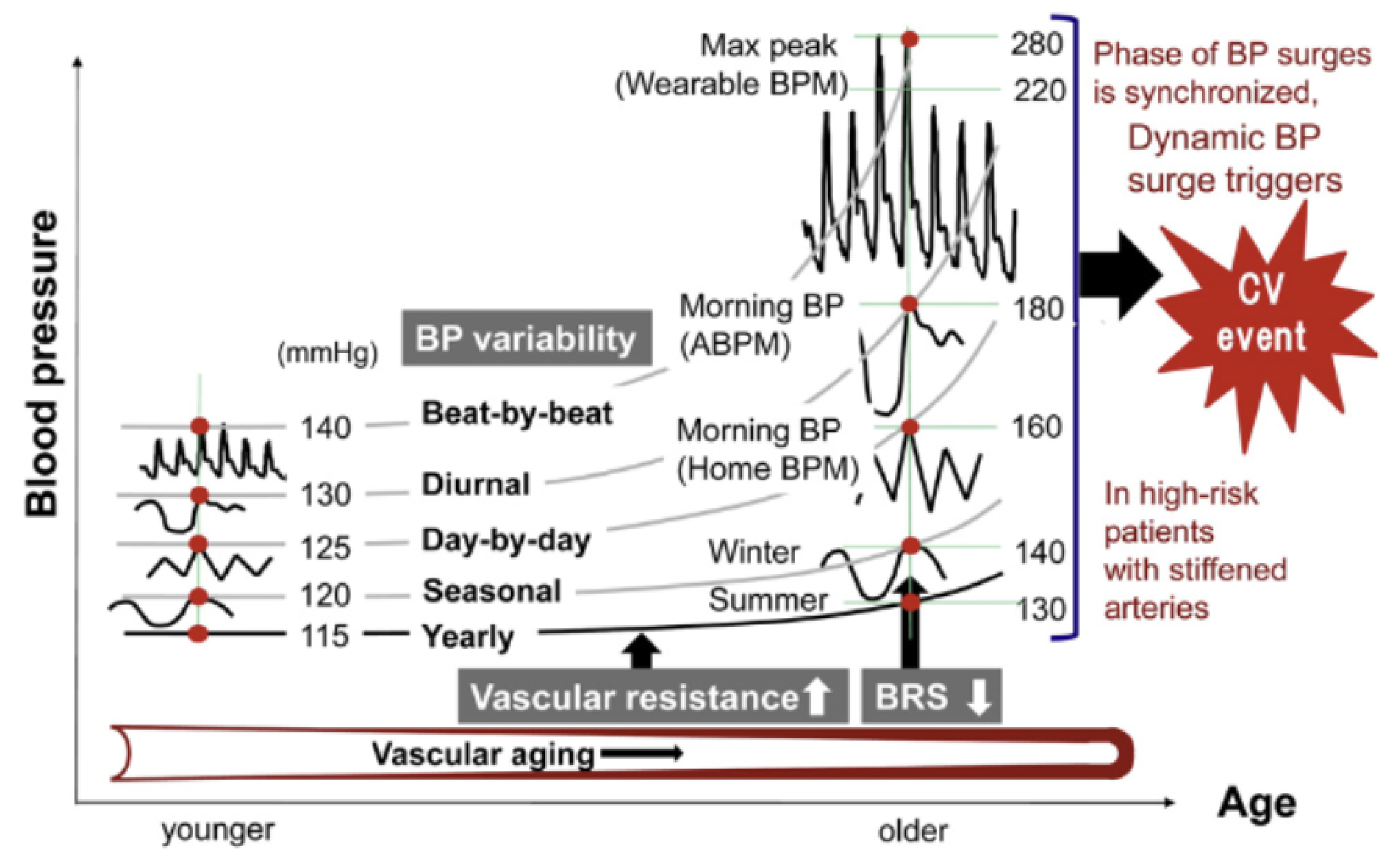
4.8. Blood Pressure—Ambulatory BP
PPG for BP Monitoring
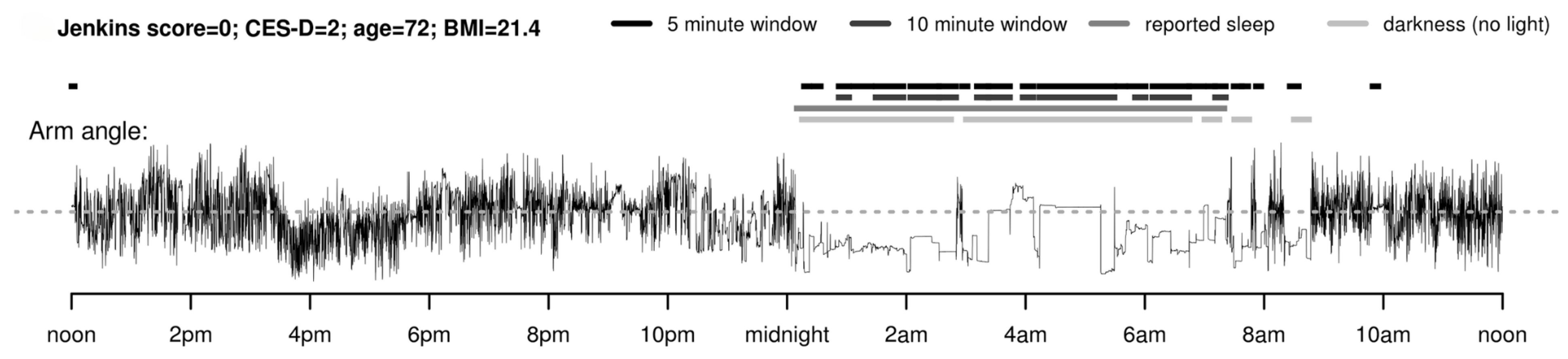
4.9. Sleep
4.10. Patient-Reported Outcome Measures (PROMs) and Ecological Momentary Assessment (EMA)
5. Where Might Such Technologies Fit into Cardiovascular Healthcare?
5.1. Arrhythmia
5.2. Heart Failure
5.3. Valvular Heart Disease
5.4. Practical Implications
6. Conclusions and Future Direction
Future Direction
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ageing and Health. Available online: https://www.who.int/news-room/fact-sheets/detail/952ageing-and-health (accessed on 1 March 2021).
- Cardiovascular Diseases. Available online: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_2 (accessed on 8 March 2021).
- Myers, J. Exercise and Cardiovascular Health. Circulation 2003, 107, e2–e5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Afilalo, J.; Karunananthan, S.; Eisenberg, M.J.; Alexander, K.P.; Bergman, H. Role of Frailty in Patients With Cardiovascular Disease. Am. J. Cardiol. 2009, 103, 1616–1621. [Google Scholar] [CrossRef] [PubMed]
- Kan, C.W.; Lam, Y.L. Future trend in wearable electronics in the textile industry. Appl. Sci. 2021, 11, 3914. [Google Scholar] [CrossRef]
- Loncar-Turukalo, T.; Zdravevski, E.; da Silva, J.M.; Chouvarda, I.; Trajkovik, V. Literature on Wearable Technology for Connected Health: Scoping Review of Research Trends, Advances, and Barriers. J. Med. Internet Res. 2019, 21, e14017. [Google Scholar] [CrossRef] [PubMed]
- PwC. The Wearable Life 2.0: Connected Living in a Wearable World. Technical Report. 2016. Available online: https://www.pwc.se/sv/pdf-reports/the-wearable-life-2-0.pdf (accessed on 10 June 2021).
- Kim, J.; Marcusson-Clavertz, D.; Yoshiuchi, K.; Smyth, J.M. Potential benefits of integrating ecological momentary assessment data into mHealth care systems. Biopsychosoc. Med. 2019, 13, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, L.; Ciravegna, F.; Bond, R.; Mulvenna, M. A Low Cost Indoor Positioning System Using Bluetooth Low Energy. IEEE Access 2020, 8, 136858–136871. [Google Scholar] [CrossRef]
- Lopez-Jimenez, F.; Attia, Z.; Arruda-Olson, A.M.; Carter, R.; Chareonthaitawee, P.; Jouni, H.; Kapa, S.; Lerman, A.; Luong, C.; Medina-Inojosa, J.R.; et al. Artificial Intelligence in Cardiology: Present and Future. Mayo Clin. Proc. 2020, 95, 1015–1039. [Google Scholar] [CrossRef]
- Krittanawong, C.; Rogers, A.J.; Johnson, K.W.; Wang, Z.; Turakhia, M.P.; Halperin, J.L.; Narayan, S.M. Integration of novel monitoring devices with machine learning technology for scalable cardiovascular management. Nat. Rev. Cardiol. 2021, 18, 75–91. [Google Scholar] [CrossRef]
- Zafari, F.; Gkelias, A.; Leung, K.K. A Survey of Indoor Localization Systems and Technologies. IEEE Commun. Surv. Tutor. 2019, 21, 2568–2599. [Google Scholar] [CrossRef] [Green Version]
- Paul, A.K.; Sato, T. Localization in wireless sensor networks: A survey on algorithms, measurement techniques, applications and challenges. J. Sens. Actuator Netw. 2017, 6, 24. [Google Scholar] [CrossRef] [Green Version]
- Wang, Z.; Yang, Z.; Dong, T. A review of wearable technologies for elderly care that can accurately track indoor position, recognize physical activities and monitor vital signs in real time. Sensors 2017, 17, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choi, B.C.; Pak, A.W.; Choi, J.C.; Choi, E.C. Daily step goal of 10,000 steps: A literature review. Clin. Investig. Med. 2007, 30, E146–E151. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayabe, M.; Brubaker, P.H.; Dobrosielski, D.; Miller, H.S.; Kiyonaga, A.; Shindo, M.; Tanaka, H. Target Step Count for the Secondary Prevention of Cardiovascular Disease. Circ. J. 2008, 72, 299–303. [Google Scholar] [CrossRef] [Green Version]
- Thorup, C.; Hansen, J.; Grønkjær, M.; Andreasen, J.J.; Nielsen, G.; Sørensen, E.E.; Dinesen, B.I. Cardiac patients’ walking activity determined by a step counter in cardiac telerehabilitation: Data from the intervention arm of a randomized controlled trial. J. Med. Internet Res. 2016, 18, e5191. [Google Scholar] [CrossRef]
- Qiu, S.; Cai, X.; Ju, C.; Sun, Z.; Yin, H.; Zügel, M.; Otto, S.; Steinacker, J.M.; Schumann, U. Step Counter Use and Sedentary Time in Adults. Medicine 2015, 94, e1412. [Google Scholar] [CrossRef]
- Qiu, S.; Cai, X.; Chen, X.; Yang, B.; Sun, Z. Step counter use in type 2 diabetes: A meta-analysis of randomized controlled trials. BMC Med. 2014, 12, 36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, D.; Morton, A.; Arguello, D.; Lyden, K.; Bassett, D. “What is a step?” Differences in how a step is detected among three popular activity monitors that have impacted physical activity research. Sensors 2018, 18, 1206. [Google Scholar] [CrossRef] [Green Version]
- Baril, J.F.; Bromberg, S.; Moayedi, Y.; Taati, B.; Manlhiot, C.; Ross, H.J.; Cafazzo, J. Use of free-living step count monitoring for heart failure functional classification: Validation study. JMIR Cardio 2019, 3, e12122. [Google Scholar] [CrossRef]
- Pepera, G.K.; Sandercock, G.R.; Sloan, R.; Cleland, J.J.; Ingle, L.; Clark, A.L. Influence of step length on 6-minute walk test performance in patients with chronic heart failure. Physiotherapy 2012, 98, 325–329. [Google Scholar] [CrossRef]
- Thorup, C.B.; Andreasen, J.J.; Sørensen, E.E.; Grønkjær, M.; DInesen, B.I.; Hansen, J. Accuracy of a step counter during treadmill and daily life walking by healthy adults and patients with cardiac disease. BMJ Open 2017, 7, e011742. [Google Scholar] [CrossRef]
- Vetrovsky, T.; Siranec, M.; Marencakova, J.; Tufano, J.J.; Capek, V.; Bunc, V.; Belohlavek, J. Validity of six consumer-level activity monitors for measuring steps in patients with chronic heart failure. PLoS ONE 2019, 14, e0222569. [Google Scholar] [CrossRef] [Green Version]
- Wilson, K.; Bell, C.; Wilson, L.; Witteman, H. Agile research to complement agile development: A proposal for an mHealth research lifecycle. NPJ Digit. Med. 2018, 1, 46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramezani, R.; Zhang, W.; Xie, Z.; Shen, J.; Elashoff, D.; Roberts, P.; Stanton, A.; Eslami, M.; Wenger, N.; Sarrafzadeh, M.; et al. A combination of indoor localization and wearable sensor–based physical activity recognition to assess older patients undergoing subacute rehabilitation: Baseline study results. JMIR mHealth uHealth 2019, 7, e14090. [Google Scholar] [CrossRef]
- Kheirkhahan, M.; Nair, S.; Davoudi, A.; Rashidi, P.; Wanigatunga, A.A.; Corbett, D.B.; Mendoza, T.; Manini, T.M.; Ranka, S. A smartwatch-based framework for real-time and online assessment and mobility monitoring. J. Biomed. Inform. 2019, 89, 29–40. [Google Scholar] [CrossRef]
- Chen, L.; Nugent, C.D.; Wang, H. A knowledge-driven approach to activity recognition in smart homes. IEEE Trans. Knowl. Data Eng. 2012, 24, 961–974. [Google Scholar] [CrossRef]
- Mostafa, M.S.; Slim, S.O.; Atia, A.; Elfattah, M.M.A.; Mostafa, M.S.M. Survey on Human Activity Recognition based on Acceleration Data. Int. J. Adv. Comput. Sci. Appl. 2019, 10. [Google Scholar] [CrossRef] [Green Version]
- Merrilees, J. Activities of Daily Living. In Encyclopedia of the Neurological Sciences; Elsevier Inc.: Amsterdam, The Netherlands, 2014; pp. 47–48. [Google Scholar] [CrossRef]
- Odhiambo, C.; Wright, P.; Corbett, C.; Valafar, H. MedSensor: Medication Adherence Monitoring Using Neural Networks on Smartwatch Accelerometer Sensor Data. arXiv 2021, arXiv:2105.08907. [Google Scholar]
- Atallah, L.; Lo, B.; King, R.; Yang, G.Z. Sensor placement for activity detection using wearable accelerometers. In Proceedings of the 2010 International Conference on Body Sensor Networks, BSN 2010, Singapore, 7–9 June 2010; pp. 24–29. [Google Scholar] [CrossRef]
- Ceron, J.D.; Lopez, D.M.; Ramirez, G.A. A mobile system for sedentary behaviors classification based on accelerometer and location data. Comput. Ind. 2017, 92–93, 25–31. [Google Scholar] [CrossRef]
- Rhudy, M.B.; Mahoney, J.M. A comprehensive comparison of simple step counting techniques using wrist- and ankle-mounted accelerometer and gyroscope signals. J. Med. Eng. Technol. 2018, 42, 236–243. [Google Scholar] [CrossRef]
- Shoaib, M.; Bosch, S.; Durmaz Incel, O.; Scholten, H.; Havinga, P.J. Fusion of Smartphone Motion Sensors for Physical Activity Recognition. Sensors 2014, 14, 10146–10176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Twomey, N.; Diethe, T.; Fafoutis, X.; Elsts, A.; McConville, R.; Flach, P.; Craddock, I. A Comprehensive Study of Activity Recognition Using Accelerometers. Informatics 2018, 5, 27. [Google Scholar] [CrossRef] [Green Version]
- Ganea, R.; Paraschiv-Ionescu, A.; Büla, C.; Rochat, S.; Aminian, K. Multi-parametric evaluation of sit-to-stand and stand-to-sit transitions in elderly people. Med. Eng. Phys. 2011, 33, 1086–1093. [Google Scholar] [CrossRef]
- Puthoff, M.L.; Saskowski, D. Reliability and Responsiveness of Gait Speed, Five Times Sit to Stand, and Hand Grip Strength for Patients in Cardiac Rehabilitation. Cardiopulm. Phys. Ther. J. 2013, 24, 31–37. [Google Scholar] [CrossRef] [Green Version]
- Horsman, H.M.; Tzeng, Y.C.; Galletly, D.C.; Peebles, K.C. The repeated sit-to-stand maneuver is a superior method for cardiac baroreflex assessment: A comparison with the modified Oxford method and Valsalva maneuver. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2014, 307, R1345–R1352. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Chen, Y.; Hao, S.; Peng, X.; Hu, L. Deep Learning for Sensor-based Activity Recognition: A Survey. arXiv 2017, arXiv:1707.03502. [Google Scholar] [CrossRef] [Green Version]
- Barnes, C.M.; Clark, C.C.T.; Rees, P.; Stratton, G.; Summers, H.D. Objective profiling of varied human motion based on normative assessment of magnetometer time series data. Physiol. Meas. 2018, 39, 45007. [Google Scholar] [CrossRef] [Green Version]
- Chen, M.A. Frailty and cardiovascular disease: Potential role of gait speed in surgical risk stratification in older adults. J. Geriatr. Cardiol. 2015, 12, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Tzoumas, A.; Kokkinidis, D.G.; Giannopoulos, S.; Giannakoulas, G.; Palaiodimos, L.; Avgerinos, D.V.; Kampaktsis, P.N. Frailty in patients undergoing transcatheter aortic valve replacement: From risk scores to frailty-based management. J. Geriatr. Cardiol. 2021, 18, 479–486. [Google Scholar] [CrossRef] [PubMed]
- Schenk, A.K.; Witbrodt, B.C.; Hoarty, C.A.; Carlson, R.H.; Goulding, E.H.; Potter, J.F.; Bonasera, S.J. Cellular telephones measure activity and lifespace in community-dwelling adults: Proof of principle. J. Am. Geriatr. Soc. 2011, 59, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Peel, C.; Baker, P.S.; Roth, D.L.; Brown, C.J.; Bodner, E.V.; Allman, R.M. Assessing Mobility in Older Adults: The UAB Study of Aging Life-Space Assessment. Phys. Ther. 2005, 85, 1008–1019. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinrichs, T.; Zanda, A.; Fillekes, M.P.; Bereuter, P.; Portegijs, E.; Rantanen, T.; Schmidt-Trucksäss, A.; Zeller, A.W.; Weibel, R. Map-based assessment of older adults’ life space: Validity and reliability. Eur. Rev. Aging Phys. Act. 2020, 17, 21. [Google Scholar] [CrossRef] [PubMed]
- Baronti, P.; Barsocchi, P.; Chessa, S.; Mavilia, F.; Palumbo, F. Indoor Bluetooth Low Energy Dataset for Localization, Tracking, Occupancy, and Social Interaction. Sensors 2018, 18, 4462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oosterlinck, D.; Benoit, D.F.; Baecke, P.; Van de Weghe, N. Bluetooth tracking of humans in an indoor environment: An application to shopping mall visits. Appl. Geogr. 2017, 78, 55–65. [Google Scholar] [CrossRef] [Green Version]
- Frisby, J.; Smith, V.; Traub, S.; Patel, V.L. Contextual Computing: A Bluetooth based approach for tracking healthcare providers in the emergency room. J. Biomed. Inform. 2017, 65, 97–104. [Google Scholar] [CrossRef] [PubMed]
- Alhomayani, F.; Mahoor, M.H. Deep learning methods for fingerprint-based indoor positioning: A review. J. Locat. Based Serv. 2020, 14, 129–200. [Google Scholar] [CrossRef]
- Yang, J.; Chen, Y.; Martin, R.P.; Trappe, W.; Gruteser, M. On the Performance of Wireless Indoor Localization Using Received Signal Strength. In Handbook of Position Location; John Wiley & Sons, Ltd.: Hoboken, NJ, USA, 2018; Chapter 12; pp. 405–433. [Google Scholar] [CrossRef]
- Farid, Z.; Nordin, R.; Ismail, M. Recent advances in wireless indoor localization techniques and system. J. Comput. Netw. Commun. 2013, 2013, 185138. [Google Scholar] [CrossRef]
- Lin, X.Y.; Ho, T.W.; Fang, C.C.; Yen, Z.S.; Yang, B.J.; Lai, F. A mobile indoor positioning system based on iBeacon technology. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Milan, Italy, 25–29 August 2015; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2015; pp. 4970–4973. [Google Scholar] [CrossRef]
- Benaissa, B.; Hendrichovsky, F.; Yishida, K.; Köppen, M.; Sinčák, P. Phone Application for Indoor Localization Based on Ble Signal Fingerprint. In Proceedings of the 2018 9th IFIP International Conference on New Technologies, Mobility and Security, NTMS 2018, Paris, France, 26–28 February 2018; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2018; pp. 1–5. [Google Scholar] [CrossRef]
- Bullmann, M.; Fetzer, T.; Ebner, F.; Ebner, M.; Deinzer, F.; Grzegorzek, M. Comparison of 2.4 GHz WiFi FTM- and RSSI-Based Indoor Positioning Methods in Realistic Scenarios. Sensors 2020, 20, 4515. [Google Scholar] [CrossRef]
- Zhang, G.; Wang, P.; Chen, H.; Zhang, L. Wireless Indoor Localization Using Convolutional Neural Network and Gaussian Process Regression. Sensors 2019, 19, 2508. [Google Scholar] [CrossRef] [Green Version]
- Kumar, P.; Reddy, L.; Varma, S. Distance measurement and error estimation scheme for RSSI based localization in wireless sensor networks. In Proceedings of the 5th International Conference on Wireless Communication and Sensor Networks, WCSN-2009, Allahabad, India, 15–19 December 2009; pp. 80–83. [Google Scholar] [CrossRef]
- Murata, M.; Ahmetovic, D.; Sato, D.; Takagi, H.; Kitani, K.M.; Asakawa, C. Smartphone-based Indoor Localization for Blind Navigation across Building Complexes. In Proceedings of the 2018 IEEE International Conference on Pervasive Computing and Communications, PerCom 2018, Athens, Greece, 19–23 March 2018; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2018. [Google Scholar] [CrossRef]
- Chuku, N.; Nasipuri, A. RSSI-Based Localization Schemes for Wireless Sensor Networks Using Outlier Detection. J. Sens. Actuator Netw. 2021, 10, 10. [Google Scholar] [CrossRef]
- Fuada, S.; Adiono, T.; Prasetiyo, P. Accuracy Improvement of RSSI-based Distance Localization using Unscented Kalman Filter (UKF) Algorithm for Wi-Fi Tracking Application. Int. J. Interact. Mob. Technol. 2020, 14, 225–233. [Google Scholar] [CrossRef]
- Wu, K.; Xiao, J.; Yi, Y.; Chen, D.; Luo, X.; Ni, L.M. CSI-based indoor localization. IEEE Trans. Parallel Distrib. Syst. 2013, 24, 1300–1309. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Wang, X.; Mao, S. Deep Convolutional Neural Networks for Indoor Localization with CSI Images. IEEE Trans. Netw. Sci. Eng. 2020, 7, 316–327. [Google Scholar] [CrossRef]
- Laska, M.; Blankenbach, J. DeepLocBox: Reliable Fingerprinting-Based Indoor Area Localization. Sensors 2021, 21, 2000. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Gao, L.; Mao, S.; Pandey, S. CSI-Based Fingerprinting for Indoor Localization: A Deep Learning Approach. IEEE Trans. Veh. Technol. 2017, 66, 763–776. [Google Scholar] [CrossRef] [Green Version]
- Chen, H.C.; Lin, T.H.; Kung, H.T.; Lin, C.K.; Gwon, Y. Determining RF angle of arrival using COTS antenna arrays: A field evaluation. In Proceedings of the IEEE Military Communications Conference MILCOM, Orlando, FL, USA, 29 October–1 November 2012. [Google Scholar] [CrossRef]
- Obeidat, H.; Shuaieb, W.; Obeidat, O.; Abd-Alhameed, R. A Review of Indoor Localization Techniques and Wireless Technologies. Wirel. Pers. Commun. 2021, 119, 289–327. [Google Scholar] [CrossRef]
- Dargie, W.; Poellabauer, C. Fundamentals of Wireless Sensor Networks: Theory and Practice; Wiley: Hoboken, NJ, USA, 2010. [Google Scholar]
- Pešić, S.; Radovanović, M.; Tošić, M.; Ivanović, M.; Iković, O.; Bošković, D. GEMAT—Internet of things solution for indoor security geofencing. In Proceedings of the ACM International Conference Proceeding Series, New York, NY, USA, 26–28 September 2019; pp. 1–8. [Google Scholar] [CrossRef]
- Yang, Z.; Zhou, Z.; Liu, Y. From RSSI to CSI: Indoor localization via channel response. Acm Comput. Surv. 2013, 46, 1–32. [Google Scholar] [CrossRef]
- Njima, W.; Ahriz, I.; Zayani, R.; Terre, M.; Bouallegue, R. Deep CNN for Indoor Localization in IoT-Sensor Systems. Sensors 2019, 19, 3127. [Google Scholar] [CrossRef] [Green Version]
- Hou, Y.; Yang, X.; Abbasi, Q. Efficient AoA-Based Wireless Indoor Localization for Hospital Outpatients Using Mobile Devices. Sensors 2018, 18, 3698. [Google Scholar] [CrossRef] [Green Version]
- McConville, R.; Archer, G.; Craddock, I.; Kozłowski, M.; Piechocki, R.; Pope, J.; Santos-Rodriguez, R. Vesta: A digital health analytics platform for a smart home in a box. Future Gener. Comput. Syst. 2021, 114, 106–119. [Google Scholar] [CrossRef]
- Bouchard, K.; Ramezani, R.; Naeim, A. Features based proximity localization with Bluetooth emitters. In Proceedings of the 2016 IEEE 7th Annual Ubiquitous Computing, Electronics and Mobile Communication Conference, UEMCON 2016, New York, NY, USA, 20–22 October 2016; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2016. [Google Scholar] [CrossRef]
- Renaudin, O.; Zemen, T.; Burgess, T. Ray-Tracing Based Fingerprinting for Indoor Localization. In Proceedings of the IEEE Workshop on Signal Processing Advances in Wireless Communications, SPAWC, Kalamata, Greece, 25–28 June 2018; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2018. [Google Scholar] [CrossRef]
- Tabbakha, N.E.; Ooi, C.P.; Tan, W.H.; Fei Tan, Y. A wearable device for machine learning based elderly’s activity tracking and indoor location system. Bull. Electr. Eng. Inform. 2021, 10, 927–939. [Google Scholar] [CrossRef]
- Konings, D.; Alam, F.; Noble, F.; Lai, E.M. SpringLoc: A Device-Free Localization Technique for Indoor Positioning and Tracking Using Adaptive RSSI Spring Relaxation. IEEE Access 2019, 7, 56960–56973. [Google Scholar] [CrossRef]
- Gu, Y.; Chen, M.; Ren, F.; Li, J. HED: Handling environmental dynamics in indoor WiFi fingerprint localization. In Proceedings of the IEEE Wireless Communications and Networking Conference, WCNC, Doha, Qatar, 3–6 April 2016; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2016. [Google Scholar] [CrossRef]
- Baronti, P.; Pillai, P.; Chook, V.W.; Chessa, S.; Gotta, A.; Hu, Y.F. Wireless sensor networks: A survey on the state of the art and the 802.15.4 and ZigBee standards. Comput. Commun. 2007, 30, 1655–1695. [Google Scholar] [CrossRef]
- Bianchi, V.; Ciampolini, P.; De Munari, I. RSSI-Based Indoor Localization and Identification for ZigBee Wireless Sensor Networks in Smart Homes. IEEE Trans. Instrum. Meas. 2019, 68, 566–575. [Google Scholar] [CrossRef]
- Maheepala, M.; Kouzani, A.Z.; Joordens, M.A. Light-Based Indoor Positioning Systems: A Review. IEEE Sens. J. 2020, 20, 3971–3995. [Google Scholar] [CrossRef]
- Tran, H.Q.; Ha, C. Fingerprint-Based Indoor Positioning System Using Visible Light Communication—A Novel Method for Multipath Reflections. Electronics 2019, 8, 63. [Google Scholar] [CrossRef] [Green Version]
- Kuo, Y.S.; Pannuto, P.; Hsiao, K.J.; Dutta, P. Luxapose: Indoor positioning with mobile phones and visible light. In Proceedings of the Annual International Conference on Mobile Computing and Networking, MOBICOM, New York, NY, USA, 7–11 September 2014; pp. 447–458. [Google Scholar] [CrossRef] [Green Version]
- Liu, K.; Liu, X.; Li, X. Guoguo: Enabling fine-grained indoor localization via smartphone. In Proceedings of the MobiSys 201311th Annual International Conference on Mobile Systems, Applications, and Services, Taipei Taiwan, 25–28 June 2013; pp. 235–248. [Google Scholar] [CrossRef]
- Hazas, M.; Hopper, A. Broadband ultrasonic location systems for improved indoor positioning. IEEE Trans. Mob. Comput. 2006, 5, 536–547. [Google Scholar] [CrossRef] [Green Version]
- Deng, Z.; Wang, H.; Zheng, X.; Yin, L. Base Station Selection for Hybrid TDOA/RTT/DOA Positioning in Mixed LOS/NLOS Environment. Sensors 2020, 20, 4132. [Google Scholar] [CrossRef]
- Menta, E.Y.; Malm, N.; Jantti, R.; Ruttik, K.; Costa, M.; Leppanen, K. On the Performance of AoA-Based Localization in 5G Ultra-Dense Networks. IEEE Access 2019, 7, 33870–33880. [Google Scholar] [CrossRef]
- Del Peral-Rosado, J.A.; Raulefs, R.; López-Salcedo, J.A.; Seco-Granados, G. Survey of Cellular Mobile Radio Localization Methods: From 1G to 5G. IEEE Commun. Surv. Tutor. 2018, 20, 1124–1148. [Google Scholar] [CrossRef]
- Oguntala, G.; Abd-Alhameed, R.; Jones, S.; Noras, J.; Patwary, M.; Rodriguez, J. Indoor location identification technologies for real-time IoT-based applications: An inclusive survey. Comput. Sci. Rev. 2018, 30, 55–79. [Google Scholar] [CrossRef]
- Perry, T.S. Look Out for Apple’s AR Glasses: With head-up displays, cameras, inertial sensors, and lidar on board, Apple’s augmented-reality glasses could redefine wearables. IEEE Spectr. 2021, 58, 26–54. [Google Scholar] [CrossRef]
- Li, J.; He, X.; Li, J. 2D LiDAR and camera fusion in 3D modeling of indoor environment. In Proceedings of the 2015 National Aerospace and Electronics Conference (NAECON), Dayton, OH, USA, 15–19 June 2015; pp. 379–383. [Google Scholar] [CrossRef]
- Zhen, W.; Hu, Y.; Liu, J.; Scherer, S. A Joint Optimization Approach of LiDAR-Camera Fusion for Accurate Dense 3-D Reconstructions. IEEE Robot. Autom. Lett. 2019, 4, 3585–3592. [Google Scholar] [CrossRef] [Green Version]
- Kolakowski, J.; Djaja-Josko, V.; Kolakowski, M.; Broczek, K. UWB/BLE tracking system for elderly people monitoring. Sensors 2020, 20, 1574. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Surian, D.; Kim, V.; Menon, R.; Dunn, A.G.; Sintchenko, V.; Coiera, E. Tracking a moving user in indoor environments using Bluetooth low energy beacons. J. Biomed. Inform. 2019, 98, 103288. [Google Scholar] [CrossRef] [PubMed]
- Internet of Radio Light—IoRL. Available online: https://iorl.5g-ppp.eu/ (accessed on 10 September 2021).
- Zhang, H.; Cui, J.; Feng, L.; Yang, A.; Lv, H.; Lin, B.; Huang, H. High-Precision Indoor Visible Light Positioning Using Modified Momentum Back Propagation Neural Network with Sparse Training Point. Sensors 2019, 19, 2324. [Google Scholar] [CrossRef] [Green Version]
- European Comission. Periodic Reporting for Period 2—IoRL (Internet of Radio Light)|H2020|CORDIS|European Commission. 2018. Available online: https://cordis.europa.eu/project/id/761992/reporting (accessed on 26 October 2022). [CrossRef]
- Pope, J.; McConville, R.; Kozlowski, M.; Fafoutis, X.; Santos-Rodriguez, R.; Piechocki, R.J.; Craddock, I. SPHERE in a Box: Practical and Scalable EurValve Activity Monitoring Smart Home Kit. In Proceedings of the 2017 IEEE 42nd Conference on Local Computer Networks Workshops, LCN Workshops 2017, Singapore, 9 October 2017; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2017; pp. 128–135. [Google Scholar] [CrossRef] [Green Version]
- Li, X.; Dunn, J.; Salins, D.; Zhou, G.; Zhou, W.; Schüssler-Fiorenza Rose, S.M.; Perelman, D.; Colbert, E.; Runge, R.; Rego, S.; et al. Digital Health: Tracking Physiomes and Activity Using Wearable Biosensors Reveals Useful Health-Related Information. PLoS Biol. 2017, 15, e2001402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hampton, J.R.; Hampton, J. The ECG Made Easy, 9th ed.; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Electrocardiogram (ECG) Test|BHF. Available online: https://www.bhf.org.uk/informationsupport/tests/ecg (accessed on 27 April 2021).
- Samol, A.; Bischof, K.; Luani, B.; Pascut, D.; Wiemer, M.; Kaese, S. Single-lead ECG recordings including einthoven and wilson leads by a smartwatch: A new era of patient directed early ECG differential diagnosis of cardiac diseases? Sensors 2019, 19, 4377. [Google Scholar] [CrossRef] [Green Version]
- KardiaMobile 6L—AliveCor, UK. Available online: https://store.alivecor.co.uk/products/1255/kardiamobile6l (accessed on 8 March 2021).
- Brasier, N.; Raichle, C.J.; Dörr, M.; Becke, A.; Nohturfft, V.; Weber, S.; Bulacher, F.; Salomon, L.; Noah, T.; Birkemeyer, R.; et al. Detection of atrial fibrillation with a smartphone camera: First prospective, international, two-centre, clinical validation study (DETECT AF PRO). Europace 2019, 21, 41–47. [Google Scholar] [CrossRef]
- Hickey, K.T.; Hauser, N.R.; Valente, L.E.; Riga, T.C.; Frulla, A.P.; Creber, R.M.; Whang, W.; Garan, H.; Jia, H.; Sciacca, R.R.; et al. A single-center randomized, controlled trial investigating the efficacy of a mHealth ECG technology intervention to improve the detection of atrial fibrillation: The iHEART study protocol. BMC Cardiovasc. Disord. 2016, 16, 152. [Google Scholar] [CrossRef] [Green Version]
- Soni, A.; Karna, S.; Patel, H.; Fahey, N.; Raithatha, S.; Handorf, A.; Bostrom, J.; Bashar, S.; Talati, K.; Shah, R.; et al. Study protocol for Smartphone Monitoring for A trial fibrillation in Real- Time in India (SMART-India): A community-based screening and referral programme. BMJ Open 2017, 7, e017668. [Google Scholar] [CrossRef] [Green Version]
- Allen, J. Photoplethysmography and its application in clinical physiological measurement Related content. Physiol. Meas. 2007, 28, R1. [Google Scholar] [CrossRef] [Green Version]
- Botman, S.; Borchevkin, D.; Petrov, V.; Bogdanov, E.; Patrushev, M.; Shusharina, N. Photoplethysmography-Based Device Designing for Cardiovascular System Diagnostics. Int. J. Biomed. Biol. Eng. 2015, 9, 689–693. [Google Scholar] [CrossRef]
- Nelson, B.W.; Allen, N.B. Accuracy of consumer wearable heart rate measurement during an ecologically valid 24-hour period: Intraindividual validation study. JMIR mHealth uHealth 2019, 7, e10828. [Google Scholar] [CrossRef] [PubMed]
- Bhowmick, S.; Kundu, P.K.; Das Mandal, D. HRV Performance Analysis in Photoplethysmography and Electrocardiography. In Proceedings of the 2020 IEEE Calcutta Conference, CALCON 2020, Kolkata, India, 28–29 February 2020; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2020; pp. 342–345. [Google Scholar] [CrossRef]
- Han, J.; Ou, W.; Xiong, J.; Feng, S. Remote Heart Rate Estimation by Pulse Signal Reconstruction Based on Structural Sparse Representation. Electronics 2022, 11, 3738. [Google Scholar] [CrossRef]
- Hu, Q.; Zeng, W.; Sheng, Y.; Xu, J.; Ou, W.; Tan, R. Study on Real-Time Heart Rate Detection Based on Multi-People. Comput. Syst. Sci. Eng. 2023, 44, 1397–1408. [Google Scholar] [CrossRef]
- Spinsante, S.; Porfiri, S.; Scalise, L. Accuracy of Heart Rate Measurements by a Smartwatch in Low Intensity Activities. In Proceedings of the Medical Measurements and Applications, MeMeA 2019—Symposium Proceedings, Istanbul, Turkey, 26–28 June 2019; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA, 2019. [Google Scholar] [CrossRef]
- Falter, M.; Budts, W.; Goetschalckx, K.; Cornelissen, V.; Buys, R. Accuracy of apple watch measurements for heart rate and energy expenditure in patients with cardiovascular disease: Cross-sectional study. JMIR mHealth uHealth 2019, 7, e11889. [Google Scholar] [CrossRef]
- Bent, B.; Goldstein, B.A.; Kibbe, W.A.; Dunn, J.P. Investigating sources of inaccuracy in wearable optical heart rate sensors. NPJ Digit. Med. 2020, 3, 18. [Google Scholar] [CrossRef] [Green Version]
- Heart Rate: What Is a Normal Heart Rate? Available online: https://www.medicalnewstoday.com/articles/235710 (accessed on 25 March 2021).
- Heart Rate: What’s Normal?—Mayo Clinic. Available online: https://www.mayoclinic.org/healthy-lifestyle/fitness/expert-answers/heart-rate/faq-20057979 (accessed on 25 March 2021).
- Tarniceriu, A.; Parak, J.; Renevey, P.; Nurmi, M.; Bertschi, M.; Delgado-Gonzalo, R.; Korhonen, I. Towards 24/7 continuous heart rate monitoring. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Orlando, FL, USA, 16–20 August 2016; Institute of Electrical and Electronics Engineers Inc.: Piscataway, NJ, USA; pp. 186–189. [Google Scholar] [CrossRef]
- Henriksen, A.; Mikalsen, M.H.; Woldaregay, A.Z.; Muzny, M.; Hartvigsen, G.; Hopstock, L.A.; Grimsgaard, S. Using fitness trackers and smartwatches to measure physical activity in research: Analysis of consumer wrist-worn wearables. J. Med. Internet Res. 2018, 20, e110. [Google Scholar] [CrossRef]
- Kavsaoǧlu, A.R.; Polat, K.; Bozkurt, M.R. An innovative peak detection algorithm for photoplethysmography signals: An adaptive segmentation method. Turk. J. Electr. Eng. Comput. Sci. 2016, 24, 1782–1796. [Google Scholar] [CrossRef]
- Mishra, T.; Wang, M.; Metwally, A.A.; Bogu, G.K.; Brooks, A.W.; Bahmani, A.; Alavi, A.; Celli, A.; Higgs, E.; Dagan-Rosenfeld, O.; et al. Pre-symptomatic detection of COVID-19 from smartwatch data. Nat. Biomed. Eng. 2020, 4, 1208–1220. [Google Scholar] [CrossRef]
- Zhu, G.; Li, J.; Meng, Z.; Yu, Y.; Li, Y.; Tang, X.; Dong, Y.; Sun, G.; Zhou, R.; Wang, H.; et al. Learning from Large-Scale Wearable Device Data for Predicting Epidemics Trend of COVID-19. Discret. Dyn. Nat. Soc. 2020, 2020, 6152041. [Google Scholar] [CrossRef]
- Qiu, S.; Cai, X.; Sun, Z.; Li, L.; Zuegel, M.; Steinacker, J.M.; Schumann, U. Heart rate recovery and risk of cardiovascular events and all-cause mortality: A meta-analysis of prospective cohort studies. J. Am. Heart Assoc. 2017, 6, e005505. [Google Scholar] [CrossRef] [Green Version]
- Sokas, D.; Petrėnas, A.; Daukantas, S.; Rapalis, A.; Paliakaitė, B.; Marozas, V. Estimation of Heart Rate Recovery after Stair Climbing Using a Wrist-Worn Device. Sensors 2019, 19, 2113. [Google Scholar] [CrossRef] [Green Version]
- Pierpont, G.L.; Stolpman, D.R.; Gornick, C.C. Heart rate recovery post-exercise as an index of parasympathetic activity. J. Auton. Nerv. Syst. 2000, 80, 169–174. [Google Scholar] [CrossRef]
- Bartels-Ferreira, R.; de Sousa, É.D.; Trevizani, G.A.; Silva, L.P.; Nakamura, F.Y.; Forjaz, C.L.M.; Lima, J.R.P.; Peçanha, T. Can a first-order exponential decay model fit heart rate recovery after resistance exercise? Clin. Physiol. Funct. Imaging 2015, 35, 98–103. [Google Scholar] [CrossRef]
- Woodward, M.; Webster, R.; Murakami, Y.; Barzi, F.; Lam, T.H.; Fang, X.; Suh, I.; Batty, G.D.; Huxley, R.; Rodgers, A. The association between resting heart rate, cardiovascular disease and mortality: Evidence from 112,680 men and women in 12 cohorts. Eur. J. Prev. Cardiol. 2014, 21, 719–726. [Google Scholar] [CrossRef] [PubMed]
- Fox, K.; Borer, J.S.; Camm, A.J.; Danchin, N.; Ferrari, R.; Lopez Sendon, J.L.; Steg, P.G.; Tardif, J.C.; Tavazzi, L.; Tendera, M. Resting Heart Rate in Cardiovascular Disease. J. Am. Coll. Cardiol. 2007, 50, 823–830. [Google Scholar] [CrossRef] [Green Version]
- Dunn, J.; Kidzinski, L.; Runge, R.; Witt, D.; Hicks, J.L.; Schüssler-Fiorenza Rose, S.M.; Li, X.; Bahmani, A.; Delp, S.L.; Hastie, T.; et al. Wearable sensors enable personalized predictions of clinical laboratory measurements. Nat. Med. 2021, 27, 1105–1112. [Google Scholar] [CrossRef]
- How Do I Track Heart Rate with My Fitbit Device? Available online: https://help.fitbit.com/articles/1335en_US/Help_article/1565.htm (accessed on 27 April 2021).
- Walsh, K.A.; Lin, D. A Smartwatch Heart Rate Monitor Prompts an Unusual Diagnosis. Case Rep. 2020, 2, 431–433. [Google Scholar] [CrossRef]
- Caspersen, C.; Powell, K.; Christenson, C. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Thompson, D.L. Fitness Focus Copy-and-Share What is Oxygen Consumption? ACSM’S Health Fit. J. 2010, 14, 4. [Google Scholar] [CrossRef]
- Hills, A.P.; Mokhtar, N.; Byrne, N.M. Assessment of Physical Activity and Energy Expenditure: An Overview of Objective Measures. Front. Nutr. 2014, 1, 5. [Google Scholar] [CrossRef]
- Livingstone, M.B.E. Heart-rate monitoring: The answer for assessing energy expenditure and physical activity in population studies? Br. J. Nutr. 1997, 78, 869–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, L.; Lu, K.; Forsman, M.; Lindecrantz, K.; Seoane, F.; Ekblom, Ö.; Eklund, J. Evaluation of physiological workload assessment methods using heart rate and accelerometry for a smart wearable system. Ergonomics 2019, 62, 694–705. [Google Scholar] [CrossRef] [Green Version]
- Kraal, J.J.; Sartor, F.; Papini, G.; Stut, W.; Peek, N.; Kemps, H.M.; Bonomi, A.G. Energy expenditure estimation in beta-blocker-medicated cardiac patients by combining heart rate and body movement data. Eur. J. Prev. Cardiol. 2016, 23, 1734–1742. [Google Scholar] [CrossRef] [PubMed]
- Brage, S.; Brage, N.; Franks, P.W.; Ekelund, U.; Wong, M.Y.; Andersen, L.B.; Froberg, K.; Wareham, N.J. Branched equation modeling of simultaneous accelerometry and heart rate monitoring improves estimate of directly measured physical activity energy expenditure. J. Appl. Physiol. 2004, 96, 343–351. [Google Scholar] [CrossRef] [Green Version]
- Kuo, T.B.; Li, J.Y.; Chen, C.Y.; Lin, Y.C.; Tsai, M.W.; Lin, S.P.; Yang, C.C. Influence of Accelerometer Placement and/or Heart Rate on Energy Expenditure Prediction during Uphill Exercise. J. Mot. Behav. 2018, 50, 127–133. [Google Scholar] [CrossRef] [PubMed]
- He, K.; Yao, J.X.; Chang, H.T. Estimation of Physical Activity Walking in Different Slopes Based on Accelerometer Approach. In Proceedings of the 2015 IEEE International Conference on Computer and Information Technology, Ubiquitous Computing and Communications, Dependable, Autonomic and Secure Computing, Pervasive Intelligence and Computing, Liverpool, UK, 26–28 October 2015; pp. 1372–1376. [Google Scholar] [CrossRef]
- Nes, B.M.; Gutvik, C.R.; Lavie, C.J.; Nauman, J.; Wisløff, U. Personalized Activity Intelligence (PAI) for Prevention of Cardiovascular Disease and Promotion of Physical Activity. Am. J. Med. 2017, 130, 328–336. [Google Scholar] [CrossRef] [Green Version]
- Maya, I.; Lau, M.B.; Wong, S.; Isserow, S. The science of exercise prescription: Martti Karvonen and his contributions. Br. Columbia Med. J. 2017, 59, 38–41. [Google Scholar]
- Aspenes, S.T.; Nilsen, T.I.L.; Skaug, E.A.; Bertheussen, G.F.; Ellingsen, Ø.; Vatten, L.; Wisløff, U. Peak Oxygen Uptake and Cardiovascular Risk Factors in 4631 Healthy Women and Men. Med. Sci. Sport. Exerc. 2011, 43, 1465–1473. [Google Scholar] [CrossRef]
- Krokstad, S.; Langhammer, A.; Hveem, K.; Holmen, T.; Midthjell, K.; Stene, T.; Bratberg, G.; Heggland, J.; Holmen, J. Cohort Profile: The HUNT Study, Norway. Int. J. Epidemiol. 2013, 42, 968–977. [Google Scholar] [CrossRef] [Green Version]
- Get the PAI Health App. Available online: https://www.paihealth.com/get-the-app (accessed on 8 April 2021).
- López-Sendó, J.; Swedberg, K.; McMurray, J.; Tamargo, J.; Maggioni, A.P.; Dargie, H.; Tendera, M.; Waagstein, F.; Kjekshus, J.; Lechat, P.; et al. Expert consensus document on β-adrenergic receptor blockers: The Task Force on Beta-Blockers of the European Society of Cardiology. Eur. Heart J. 2004, 25, 1341–1362. [Google Scholar] [CrossRef] [Green Version]
- DeGroot, D.W.M.; Quinn, T.J.P.; Kertzer, R.; William, B.M.D. Circuit Weight Training in Cardiac Patients: Determining Optimal Workloads for Safety and Energy Expenditure. J. Cardiopulm. Rehabil. 1998, 18, 145–152. [Google Scholar] [CrossRef]
- Medina Quero, J.; Fernández Olmo, M.; Peláez Aguilera, M.; Espinilla Estévez, M. Real-Time Monitoring in Home-Based Cardiac Rehabilitation Using Wrist-Worn Heart Rate Devices. Sensors 2017, 17, 2892. [Google Scholar] [CrossRef] [Green Version]
- What Is Heart Rate Variability?—Elite HRV. Available online: https://elitehrv.com/what-is-heart-rate-variability (accessed on 27 April 2021).
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 1987, 59, 256–262. [Google Scholar] [CrossRef]
- Kotecha, D.; New, G.; Flather, M.D.; Eccleston, D.; Pepper, J.; Krum, H. Five-minute heart rate variability can predict obstructive angiographic coronary disease. Heart 2012, 98, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Islam, S.M.S.; Maddison, R. A Comparison of Blood Pressure Data Obtained From Wearable, Ambulatory, and Home Blood Pressure Monitoring Devices: Prospective Validation Study. JMIR Data 2020, 1, e22436. [Google Scholar]
- Kario, K. Evidence and Perspectives on the 24-hour Management of Hypertension: Hemodynamic Biomarker-Initiated ‘Anticipation Medicine’ for Zero Cardiovascular Event. Prog. Cardiovasc. Dis. 2016, 59, 262–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- What is Blood Pressure?—NHS. Available online: https://www.nhs.uk/common-health-questions/lifestyle/what-is-blood-pressure (accessed on 28 April 2021).
- How to Monitor Your Blood Pressure. Available online: https://www.omron-healthcare.co.uk/health-and-lifestyle/heart-health/blood-pressure-monitoring/how-to-monitor-your-blood-pressure.html (accessed on 28 April 2021).
- HeartGuide. Available online: https://www.omron-healthcare.co.uk (accessed on 28 April 2021).
- Rachim, V.P.; Chung, W.Y. Multimodal Wrist Biosensor for Wearable Cuff-less Blood Pressure Monitoring System. Sci. Rep. 2019, 9, 7947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kario, K. Management of Hypertension in the Digital Era: Small Wearable Monitoring Devices for Remote Blood Pressure Monitoring. Hypertension 2020, 76, 640–650. [Google Scholar] [CrossRef]
- Buysse, D.J. Sleep Health: Can We Define It? Does It Matter? Sleep 2014, 37, 9–17. [Google Scholar] [CrossRef] [Green Version]
- Kawachi, I.; Colditz, G.A.; Stampfer, M.J.; Willett, W.C.; Manson, J.E.; Speizer, F.E.; Hennekens, C.H. Prospective study of shift work and risk of coronary heart disease in women. Circulation 1995, 92, 3178–3182. [Google Scholar] [CrossRef] [PubMed]
- Laugsand, L.E.; Vatten, L.J.; Platou, C.; Janszky, I. Insomnia and the risk of acute myocardial infarction: A population study. Circulation 2011, 124, 2073–2081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Appelhans, B.M.; Janssen, I.; Cursio, J.F.; Matthews, K.A.; Hall, M.; Gold, E.B.; Burns, J.W.; Kravitz, H.M. Sleep duration and weight change in midlife women: The SWAN sleep study. Obesity 2013, 21, 77–84. [Google Scholar] [CrossRef] [PubMed]
- van Hees, V.T.; Sabia, S.; Anderson, K.N.; Denton, S.J.; Oliver, J.; Catt, M.; Abell, J.G.; Kivimäki, M.; Trenell, M.I.; Singh-Manoux, A. A Novel, Open Access Method to Assess Sleep Duration Using a Wrist-Worn Accelerometer. PLoS ONE 2015, 10, e0142533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Renevey, P.; Delgado-Gonzalo, R.; Lemkaddem, A.; Proença, M.; Lemay, M.; Soì, J.; Tarniceriu, A.; Bertschi, M. Optical wrist-worn device for sleep monitoring. In IFMBE Proceedings; Springer: Singapore, 2017. [Google Scholar] [CrossRef]
- Li, Z.; Arvaneh, M.; Elphick, H.E.; Kingshott, R.N.; Mihaylova, L.S. A Dirichlet Process Mixture Model for Autonomous Sleep Apnea Detection using Oxygen Saturation Data. In Proceedings of the 2020 IEEE 23rd International Conference on Information Fusion (FUSION), Rustenburg, South Africa, 6–9 July 2020; pp. 1–8. [Google Scholar] [CrossRef]
- Tamura, T. Current progress of photoplethysmography and SPO2 for health monitoring. Biomed. Eng. Lett. 2019, 9, 21–36. [Google Scholar] [CrossRef]
- Holmes, C.; Briffa, N. Patient-Reported Outcome Measures (PROMS) in patients undergoing heart valve surgery: Why should we measure them and which instruments should we use? Open Heart 2016, 3, e000315. [Google Scholar] [CrossRef] [Green Version]
- Keszei, A.P.; Novak, M.; Streiner, D.L. Introduction to health measurement scales. J. Psychosom. Res. 2010, 68, 319–323. [Google Scholar] [CrossRef]
- Guess, M.; Zavanelli, N.; Yeo, W.H. Recent Advances in Materials and Flexible Sensors for Arrhythmia Detection. Materials 2022, 15, 724. [Google Scholar] [CrossRef]
- Sadrawi, M.; Lin, C.H.; Lin, Y.T.; Hsieh, Y.; Kuo, C.C.; Chien, J.C.; Haraikawa, K.; Abbod, M.F.; Shieh, J.S. Arrhythmia Evaluation in Wearable ECG Devices. Sensors 2017, 17, 2445. [Google Scholar] [CrossRef] [Green Version]
- Shelbaya, K.; Claggett, B.; Dorbala, P.; Skali, H.; Solomon, S.D.; Matsushita, K.; Konety, S.; Mosley, T.H.; Shah, A.M. Stages of Valvular Heart Disease among Older Adults in the Community: The Atherosclerosis Risk in Communities Study. Circulation 2023, 147, 638–649. [Google Scholar] [CrossRef]
































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Activity Monitor | Release Year | Mean Daily Steps (HF) | MAPE (HF) | Mean Daily Steps (Healthy) | MAPE (Healthy) |
|---|---|---|---|---|---|
| Withings Go | 2016 | 4516 | 18% | Not Reported | Not Reported |
| Omron HJ-322U | 2014 | 4297 | 12% | 8480 | 8% |
| SmartLab Walk+ | 2014 | 4299 | 13% | 8573 | 8% |
| Garmin Vivofit 1 | 2014 | 5921 | 18% | 8562 | 10% |
| Garmin Vivofit 3 | 2016 | 5671 | 13% | 8393 | 7% |
| Fitbit Charge 2 | 2016 | 6796 | 46% | 10876 | 12% |
| Criterion | Description | Value |
|---|---|---|
| Accuracy | 2d position compared to reference | 0.5–1 m |
| Installation complexity | Time to install system in a flat | <1 h |
| User acceptance | Quantitative measure of invasiveness | Noninvasive |
| Coverage | Area of typical flat | 90 m2 |
| Update rate | Sampling interval of system | 0.5 s |
| Operating time | Battery life | Not assessed |
| Availability | The time a system is active and responsive | >90% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shiwani, M.A.; Chico, T.J.A.; Ciravegna, F.; Mihaylova, L. Continuous Monitoring of Health and Mobility Indicators in Patients with Cardiovascular Disease: A Review of Recent Technologies. Sensors 2023, 23, 5752. https://doi.org/10.3390/s23125752
Shiwani MA, Chico TJA, Ciravegna F, Mihaylova L. Continuous Monitoring of Health and Mobility Indicators in Patients with Cardiovascular Disease: A Review of Recent Technologies. Sensors. 2023; 23(12):5752. https://doi.org/10.3390/s23125752
Chicago/Turabian StyleShiwani, Muhammad Ali, Timothy J. A. Chico, Fabio Ciravegna, and Lyudmila Mihaylova. 2023. "Continuous Monitoring of Health and Mobility Indicators in Patients with Cardiovascular Disease: A Review of Recent Technologies" Sensors 23, no. 12: 5752. https://doi.org/10.3390/s23125752