
DRU-Net: Pulmonary Artery Segmentation via Dense Residual U-Network with Hybrid Loss Function


Abstract
:1. Introduction
- 1.
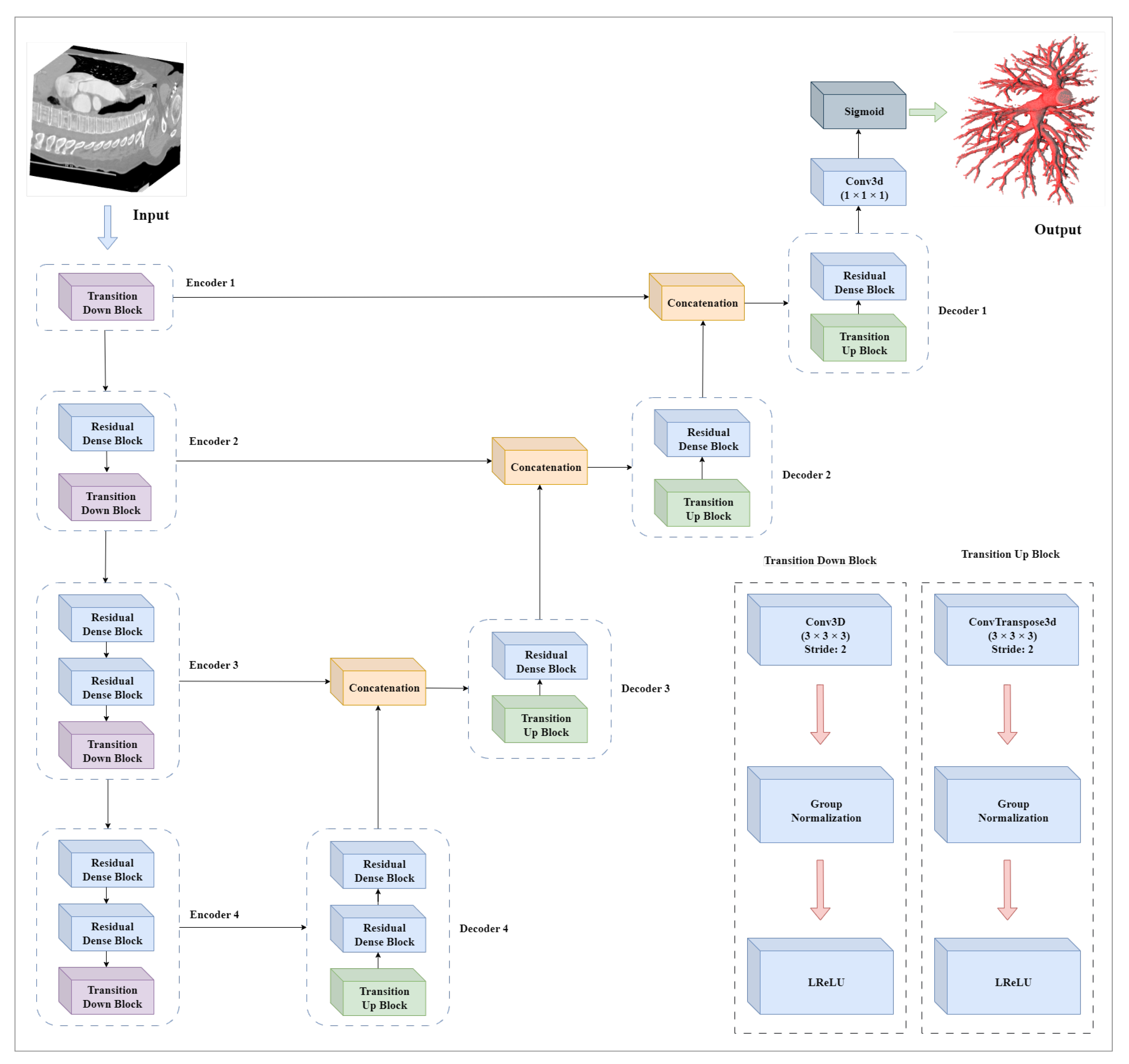
- For pulmonary artery segmentation, DRU-Net is proposed, which consists of dense connections, residual blocks, and U-Net structure. The proposed network will address the problem of gradient vanishing and will increase the information flow throughout the network for better segmentation.
- 2.
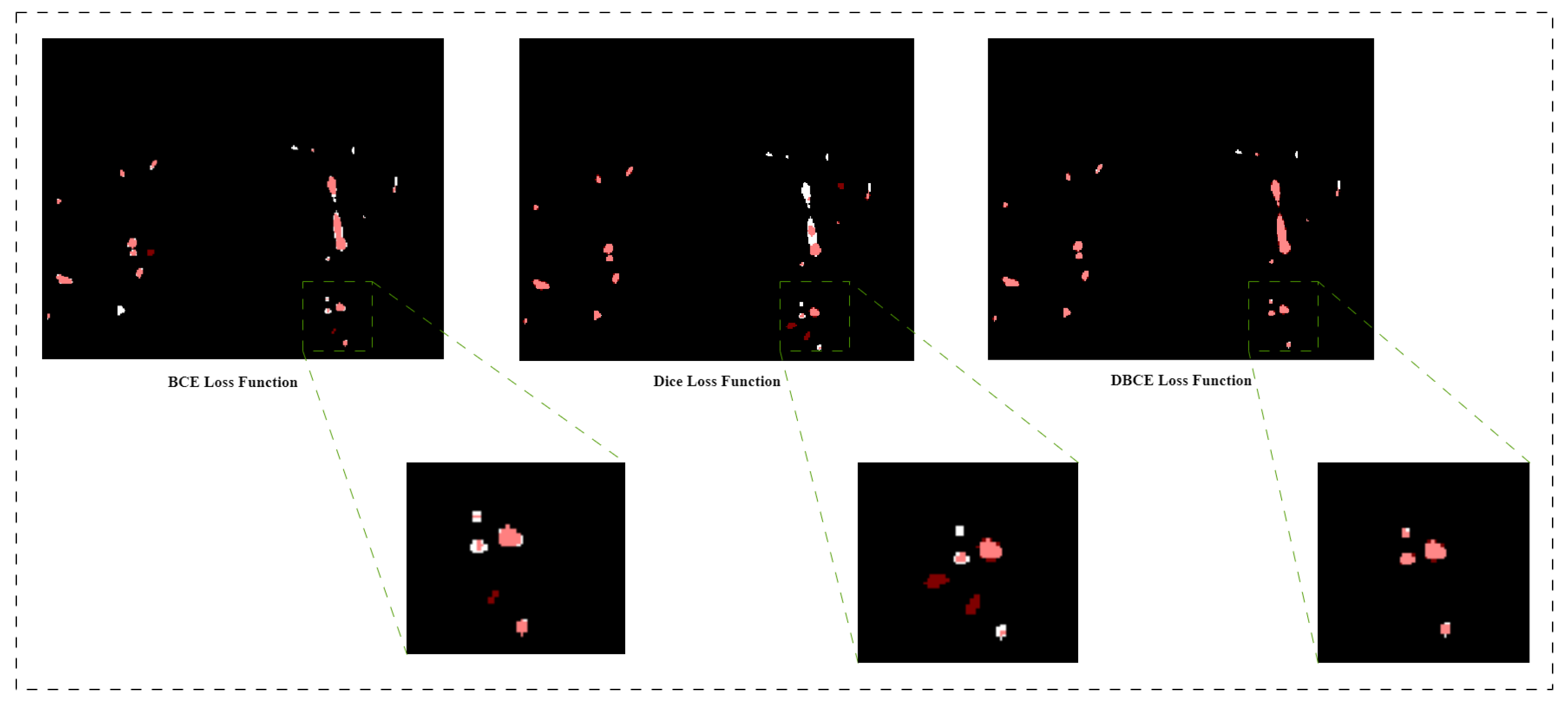
- A hybrid loss function is introduced, which will optimize network performance by stabilizing the loss function and will assist the network in segmenting fine details.
2. Methods
2.1. Dataset Description
2.2. Prepossessing
- 1.
- In order to target the lung area, Intensities are clipped to [−800, 500] HU. Due to the nature of CT data, clipping is required. The range of HU values is wider than what can be displayed. The use of clipping ensures that the same structures are assigned similar values after the operation, regardless of the CT scanner on which they were collected. By limiting the intensities to [−800, 500] HU, we focus on the range that is more likely to capture pulmonary vessels and reduce the impact of unrelated structures or artifacts Figure 1.
- 2.
- The dataset is normalized between the values [0, 1] for the training of the network.
- 3.
- Each sample in the dataset is divided into 9 patches of the size 256 × 256 × number of slices. A patch-based approach is employed as high resolution volumes cannot be processed at their original resolution due to a GPU memory constraint. Furthermore, the patch-based method synthetically generates “more” data by dividing input volumes into patches with varied centers.
2.3. Network Architecture
Hybrid Loss Function
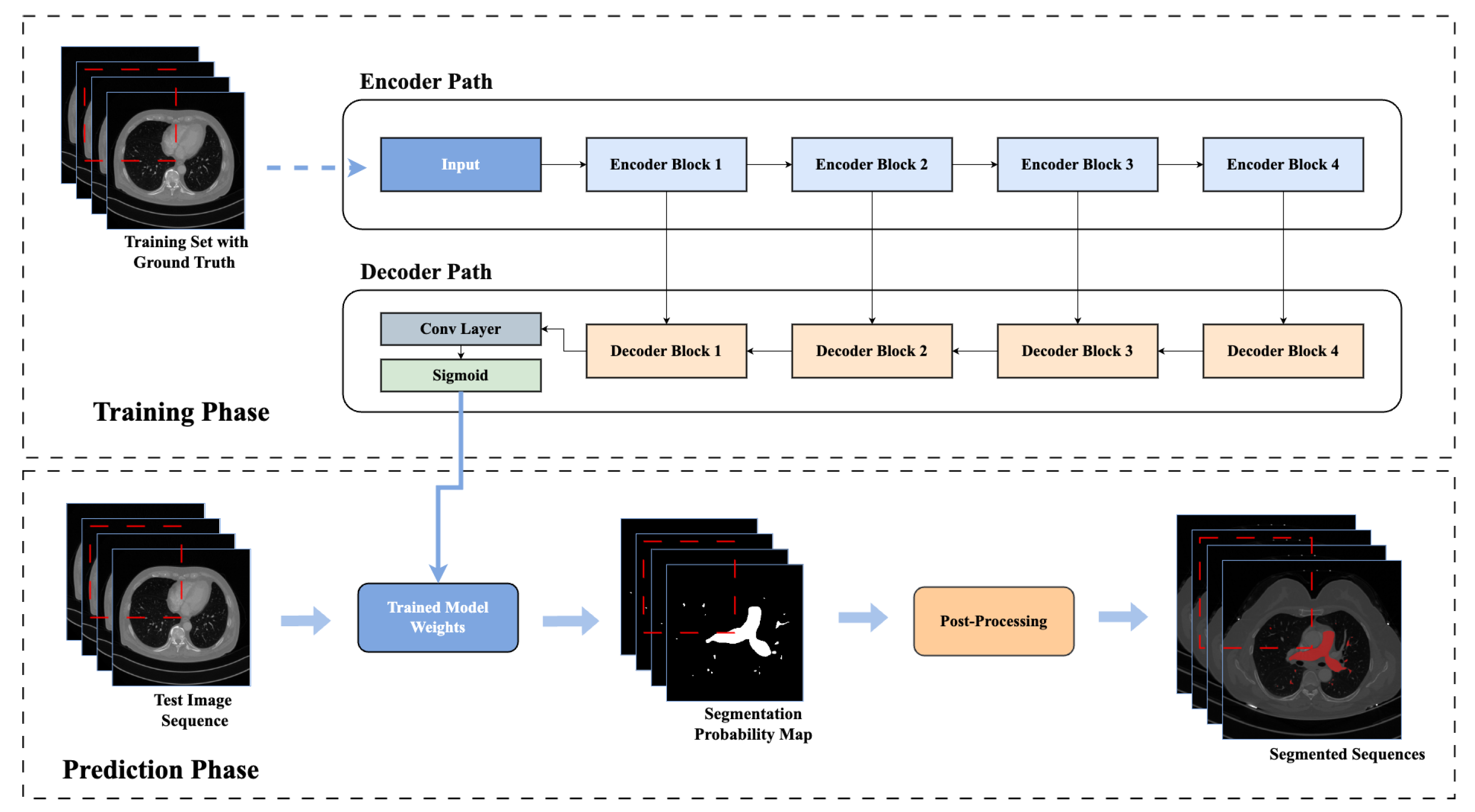
2.4. Post-Processing
2.5. Network Training and Testing
2.6. Evaluation Metrics
- 1.
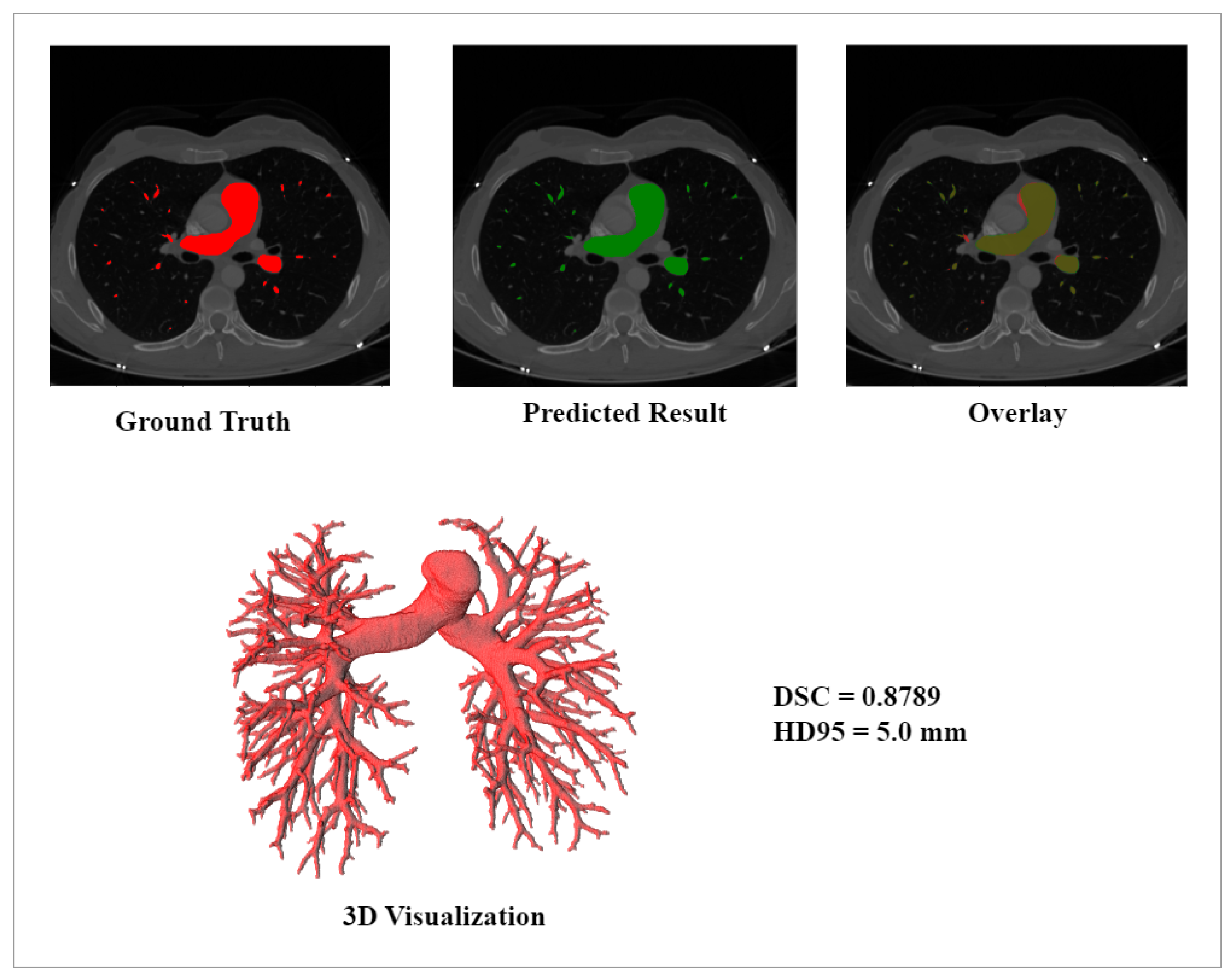
- Dice Similarity Coefficient (DSC): The DSC represents the overlap between the predicted results and the ground truth based on Equation (4), where P represents the predictions and G shows the ground truth.
- 2.
- 95% Hausdorff distance (HD95): The Hausdorff Distance (HD) is a metric used to compute the maximum distance between two structures.In Equation (5), X and Y represent the boundaries of two different structures. shows the maximum distance from the calculated minimum distances from the boundary X to the boundary Y, while represents the maximum distance from the calculated minimum distances from boundary Y to boundary X. The Hausdorff distance (HD) is extremely sensitive to outliers [30]. As a result, in the field of medical science, HD95 is used. HD95 is the 95th percentile of the Hausdroff Distance. The objective of HD95 is to reduce the impact of a very small subset of outliers.
3. Results
4. Discussion
5. Conclusions
- 1.
- The dense residual network is designed and consists of residual blocks, dense connections, and a U-Net structure. The proposed network addressed the challenges of the vanishing gradient problem and integrated the feature reuse property in the deep neural network.
- 2.
- The hybrid loss function combining dice loss and binary cross entropy is introduced to precisely segment fine details in the pulmonary artery.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aboyans, V.; Causes of Death Collaborators. Global, regional, and national age–sex specific all-cause and cause-specific mortality for 240 causes of death, 1990–2013: A systematic analysis for the global burden of disease study 2013. Lancet 2015, 385, 117–171. [Google Scholar]
- Reduced lung-cancer mortality with low-dose computed tomographic screening. N. Engl. J. Med. 2011, 365, 395–409. [CrossRef] [Green Version]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [Green Version]
- Weiss, A.; Neubauer, M.C.; Yerabolu, D.; Kojonazarov, B.; Schlueter, B.C.; Neubert, L.; Jonigk, D.; Baal, N.; Ruppert, C.; Dorfmuller, P.; et al. Targeting cyclin-dependent kinases for the treatment of pulmonary arterial hypertension. Nat. Commun. 2019, 10, 2204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schermuly, R.T.; Ghofrani, H.A.; Wilkins, M.R.; Grimminger, F. Mechanisms of disease: Pulmonary arterial hypertension. Nat. Rev. Cardiol. 2011, 8, 443–455. [Google Scholar] [CrossRef] [PubMed]
- Fréchette, É.; Deslauriers, J. Surgical anatomy of the bronchial tree and pulmonary artery. Semin. Thorac. Cardiovasc. Surg. 2006, 18, 77–84. [Google Scholar] [CrossRef]
- Shahin, Y.; Alabed, S.; Alkhanfar, D.; Tschirren, J.; Rothman, A.M.; Condliffe, R.; Wild, J.M.; Kiely, D.G.; Swift, A.J. Quantitative CT evaluation of small pulmonary vessels has functional and prognostic value in pulmonary hypertension. Radiology 2022, 305, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Poletti, J.; Bach, M.; Yang, S.; Sexauer, R.; Stieltjes, B.; Rotzinger, D.C.; Bremerich, J.; Walter Sauter, A.; Weikert, T. Automated Lung Vessel Segmentation reveals blood vessel volume redistribution in viral pneumonia. Eur. J. Radiol. 2022, 150, 110259. [Google Scholar] [CrossRef] [PubMed]
- Meinel, F.G.; Nance, J.W.; Schoepf, U.J.; Hoffmann, V.S.; Thierfelder, K.M.; Costello, P.; Goldhaber, S.Z.; Bamberg, F. Predictive value of computed tomography in acute pulmonary embolism: Systematic review and meta-analysis. Am. J. Med. 2015, 128, 747–759. [Google Scholar] [CrossRef]
- Smelt, J.L.; Suri, T.; Valencia, O.; Jahangiri, M.; Rhode, K.; Nair, A.; Bille, A. Operative planning in thoracic surgery: A pilot study comparing imaging techniques and three-dimensional printing. Ann. Thorac. Surg. 2019, 107, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Chenyang, X.; Prince, J.L. Snakes, shapes, and gradient vector flow. IEEE Trans. Image Process. 1998, 7, 359–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, C.; Chan, H.-P.; Sahiner, B.; Hadjiiski, L.M.; Chughtai, A.; Patel, S.; Wei, J.; Ge, J.; Cascade, P.N.; Kazerooni, E.A. Automatic Multiscale Enhancement and segmentation of pulmonary vessels in CT pulmonary angiography images for CAD Applications. Med. Phys. 2007, 34, 4567–4577. [Google Scholar] [CrossRef] [Green Version]
- Shikata, H.; McLennan, G.; Hoffman, E.A.; Sonka, M. Segmentation of pulmonary vascular trees from Thoracic 3D CT Images. Int. J. Biomed. Imaging 2009, 2009, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lo, P.; van Ginneken, B.; de Bruijne, M. Vessel tree extraction using locally optimal paths. In Proceedings of the IEEE International Symposium on Biomedical Imaging: From Nano to Macro, Rotterdam, The Netherlands, 14–17 April 2010. [Google Scholar]
- Zhou, C.; Chan, H.-P.; Kuriakose, J.W.; Chughtai, A.; Wei, J.; Hadjiiski, L.M.; Guo, Y.; Patel, S.; Kazerooni, E.A. Pulmonary vessel segmentation utilizing curved planar Reformation and optimal path finding (crop) in computed tomographic pulmonary angiography (CTPA) for CAD Applications. In Proceedings of the Medical Imaging 2012: Computer-Aided Diagnosis, San Diego, CA, USA, 7–9 February 2012; SPIE: Paris, France, 2012. [Google Scholar]
- Chen, Y.; Lin, Y.; Niu, Y.; Ke, X.; Huang, T. Pyramid context contrast for semantic segmentation. IEEE Access 2019, 7, 173679–173693. [Google Scholar] [CrossRef]
- Ronneberger, O.; Fischer, P.; Brox, T. U-Net: Convolutional Networks for Biomedical Image Segmentation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2015: 18th International Conference, Munich, Germany, 5–9 October 2015; pp. 234–241. [Google Scholar]
- Liu, Z.; Song, Y.-Q.; Sheng, V.S.; Wang, L.; Jiang, R.; Zhang, X.; Yuan, D. Liver CT sequence segmentation based with improved U-Net and graph cut. Expert Syst. Appl. 2019, 126, 54–63. [Google Scholar] [CrossRef]
- Zhou, Z.; Siddiquee, M.M.; Tajbakhsh, N.; Liang, J. UNet++: Redesigning skip connections to exploit multiscale features in image segmentation. IEEE Trans. Med. Imaging 2020, 39, 1856–1867. [Google Scholar] [CrossRef] [Green Version]
- Valanarasu, J.M.; Sindagi, V.A.; Hacihaliloglu, I.; Patel, V.M. KIU-Net: Towards accurate segmentation of biomedical images using over-complete representations. In Proceedings of the Medical Image Computing and Computer Assisted Intervention—MICCAI 2020, Lima, Peru, 4–8 October 2020; pp. 363–373. [Google Scholar]
- Wang, H.-J.; Chen, L.-W.; Lee, H.-Y.; Chung, Y.-J.; Lin, Y.-T.; Lee, Y.-C.; Chen, Y.-C.; Chen, C.-M.; Lin, M.-W. Automated 3D segmentation of the aorta and pulmonary artery on non-contrast-enhanced chest computed tomography images in lung cancer patients. Diagnostics 2022, 12, 967. [Google Scholar] [CrossRef]
- Yeung, M.; Sala, E.; Schönlieb, C.-B.; Rundo, L. Unified focal loss: Generalising dice and cross entropy-based losses to handle class imbalanced medical image segmentation. Comput. Med. Imaging Graph. 2022, 95, 102026. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Li, W.; Vercauteren, T.; Ourselin, S.; Jorge Cardoso, M. Generalised dice overlap as a deep learning loss function for highly unbalanced segmentations. In Deep Learning in Medical Image Analysis and Multimodal Learning for Clinical Decision Support, Proceedings of the 3rd International Workshop, DLMIA 2017, and 7th International Workshop, ML-CDS 2017, Held in Conjunction with MICCAI 2017, Québec City, QC, Canada, 14 September 2017; Springer International Publishing: Berlin/Heidelberg, Germany; pp. 240–248.
- Luo, G.; Wang, K.; Liu, J.; Li, S.; Liang, X.; Li, X.; Gan, S.; Wang, W.; Dong, S.; Wang, W.; et al. Efficient automatic segmentation for multi-level pulmonary arteries: The PARSE challenge. arXiv 2023, arXiv:2304.03708. [Google Scholar]
- Çiçek, Ö.; Abdulkadir, A.; Lienkamp, S.S.; Brox, T.; Ronneberger, O. 3D U-Net: Learning dense volumetric segmentation from sparse annotation. In Proceedings of the Medical Image Computing and Computer-Assisted Intervention—MICCAI 2016, Athens, Greece, 17–21 October 2016; pp. 424–432. [Google Scholar]
- Wu, Y.; He, K. Group normalization. Int. J. Comput. Vis. 2019, 128, 742–755. [Google Scholar] [CrossRef]
- Lei, X.; Sun, L.; Xia, Y. Lost data reconstruction for structural health monitoring using deep convolutional generative Adversarial Networks. Struct. Health Monit. 2021, 20, 2069–2087. [Google Scholar] [CrossRef]
- Milletari, F.; Navab, N.; Ahmadi, S.-A. V-net: Fully convolutional neural networks for volumetric medical image segmentation. In Proceedings of the 4th International Conference on 3D Vision (3DV), Stanford, CA, USA, 25–28 October 2016. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A method for stochastic optimization. arXiv 2014, arXiv:1412.6980. [Google Scholar]
- Begum, N.; Badshah, N.; Rada, L.; Ademaj, A.; Ashfaq, M.; Atta, H. An improved multi-modal joint segmentation and Registration Model based on Bhattacharyya Distance measure. Alex. Eng. J. 2022, 61, 12353–12365. [Google Scholar] [CrossRef]
- Parse2022—Grand Challenge. Available online: https://parse2022.grand-challenge.org/result/ (accessed on 22 February 2023).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Samples | Age | Gender (F/M) | Pixel Spacing (mm) | Slice Nums |
|---|---|---|---|---|
| 100 | 29–71 (56.3) | 79/21 | 0.5039–0.9238 (0.6740) | 228–390 (303) |
| Folds | DSC | HD95 (mm) |
|---|---|---|
| Fold 1 | 0.8841 | 4.7503 |
| Fold 2 | 0.8784 | 3.7708 |
| Fold 3 | 0.8762 | 3.7247 |
| Fold 4 | 0.8723 | 3.5432 |
| Fold 5 | 0.8812 | 5.2830 |
| Fold 6 | 0.8720 | 4.8999 |
| Fold 7 | 0.8827 | 4.2403 |
| Fold 8 | 0.8773 | 4.1121 |
| Fold 9 | 0.8785 | 4.022 |
| Fold 10 | 0.8730 | 4.2786 |
| Loss Functions | DSC | HD95 (mm) |
|---|---|---|
| Dice Loss Function | 0.8770 | 4.3666 |
| Binary Cross Entropy (BCE) Loss Function | 0.8765 | 5.5597 |
| Hybrid Loss Function | 0.8775 | 4.2624 |
| Teams | DSC | HD95 (mm) |
|---|---|---|
| Infervision medical technology co. Ltd. [31] | 0.7969 | 5.2607 |
| SenseTime China [31] | 0.7968 | 4.7538 |
| Beijing Institute of Technology [31] | 0.7980 | 5.3612 |
| 3D U-Net | 0.8313 | 11.6697 |
| DRU-Net (Proposed Method) | 0.8775 | 4.2624 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zulfiqar, M.; Stanuch, M.; Wodzinski, M.; Skalski, A. DRU-Net: Pulmonary Artery Segmentation via Dense Residual U-Network with Hybrid Loss Function. Sensors 2023, 23, 5427. https://doi.org/10.3390/s23125427
Zulfiqar M, Stanuch M, Wodzinski M, Skalski A. DRU-Net: Pulmonary Artery Segmentation via Dense Residual U-Network with Hybrid Loss Function. Sensors. 2023; 23(12):5427. https://doi.org/10.3390/s23125427
Chicago/Turabian StyleZulfiqar, Manahil, Maciej Stanuch, Marek Wodzinski, and Andrzej Skalski. 2023. "DRU-Net: Pulmonary Artery Segmentation via Dense Residual U-Network with Hybrid Loss Function" Sensors 23, no. 12: 5427. https://doi.org/10.3390/s23125427