
Feasibility of a Novel Therapist-Assisted Feedback System for Gait Training in Parkinson’s Disease


 , ,
, , _Carlson-Kuhta.jpg) ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Design
2.2.1. Overground Walking
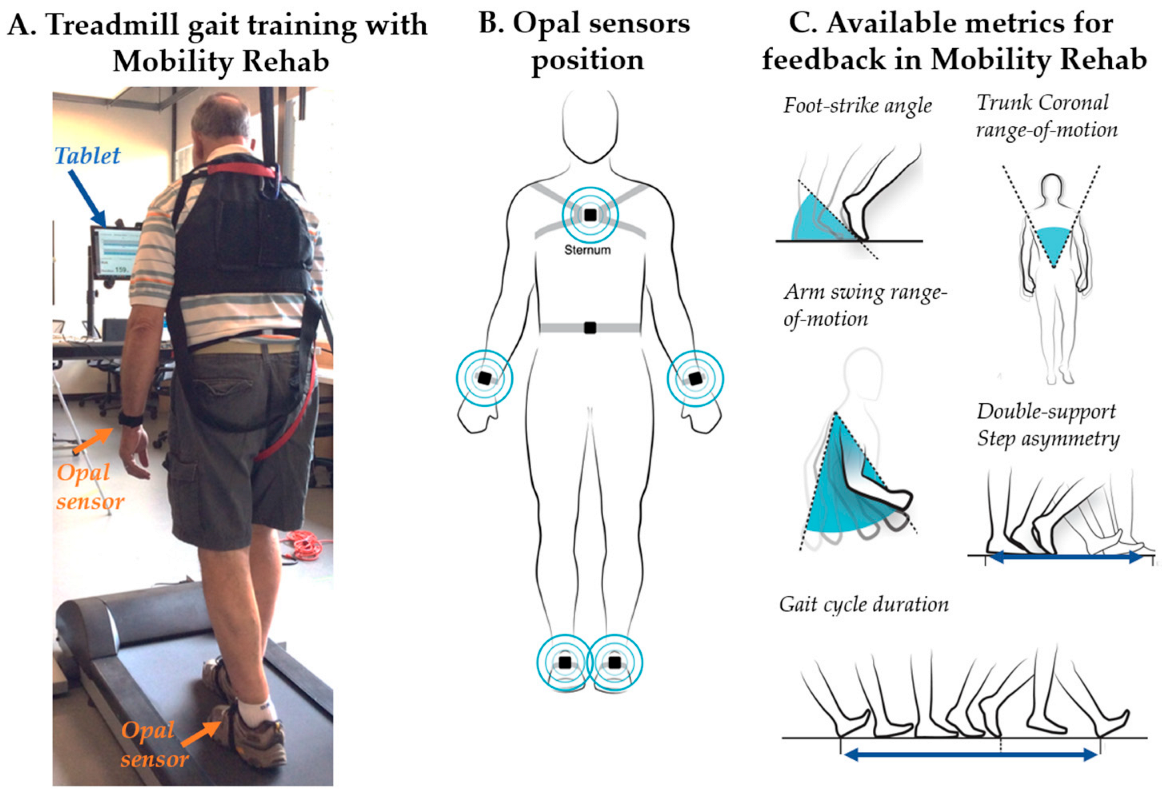
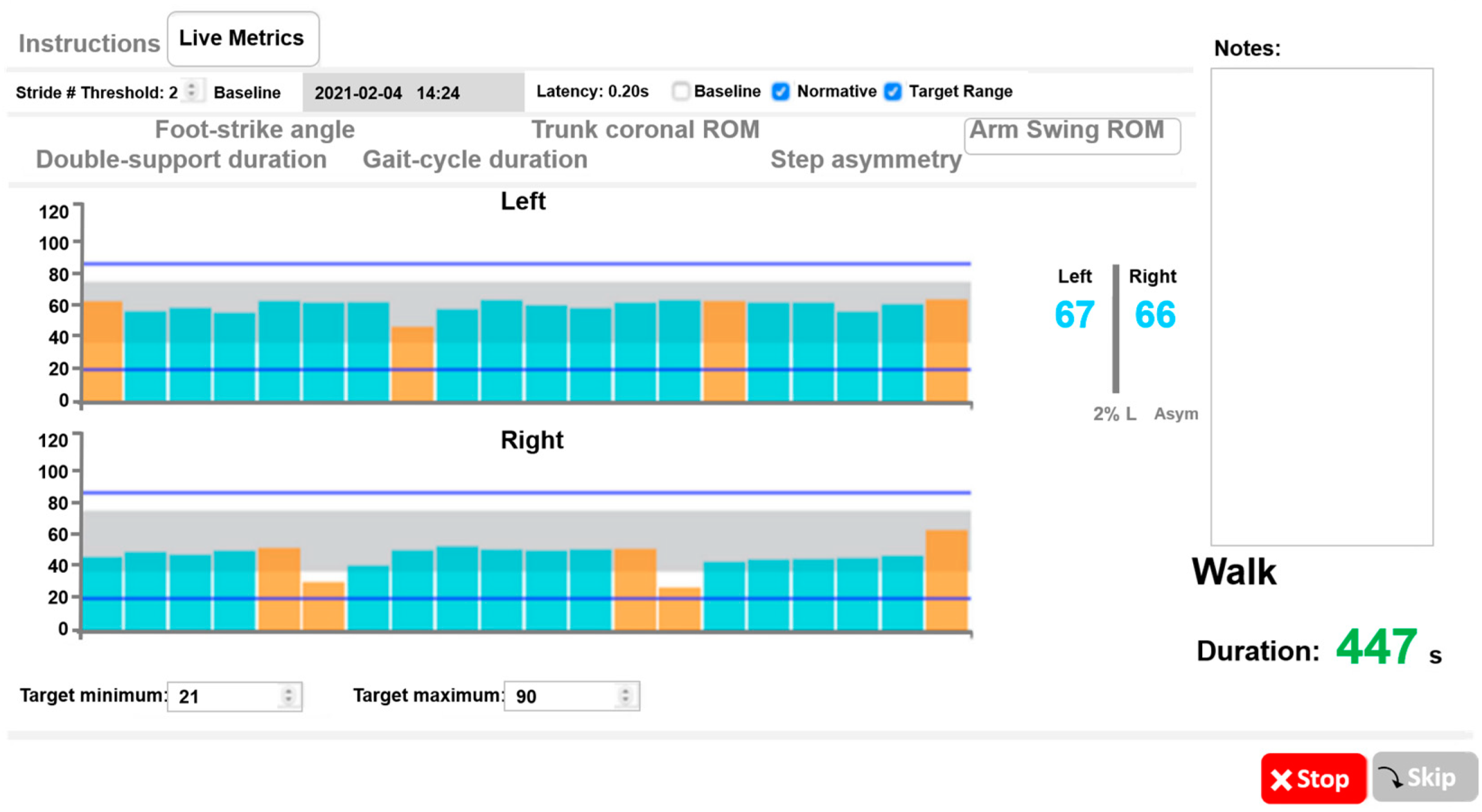
2.2.2. Treadmill Gait Training with Mobility Rehab
2.3. Data Analysis
3. Results
3.1. Participants
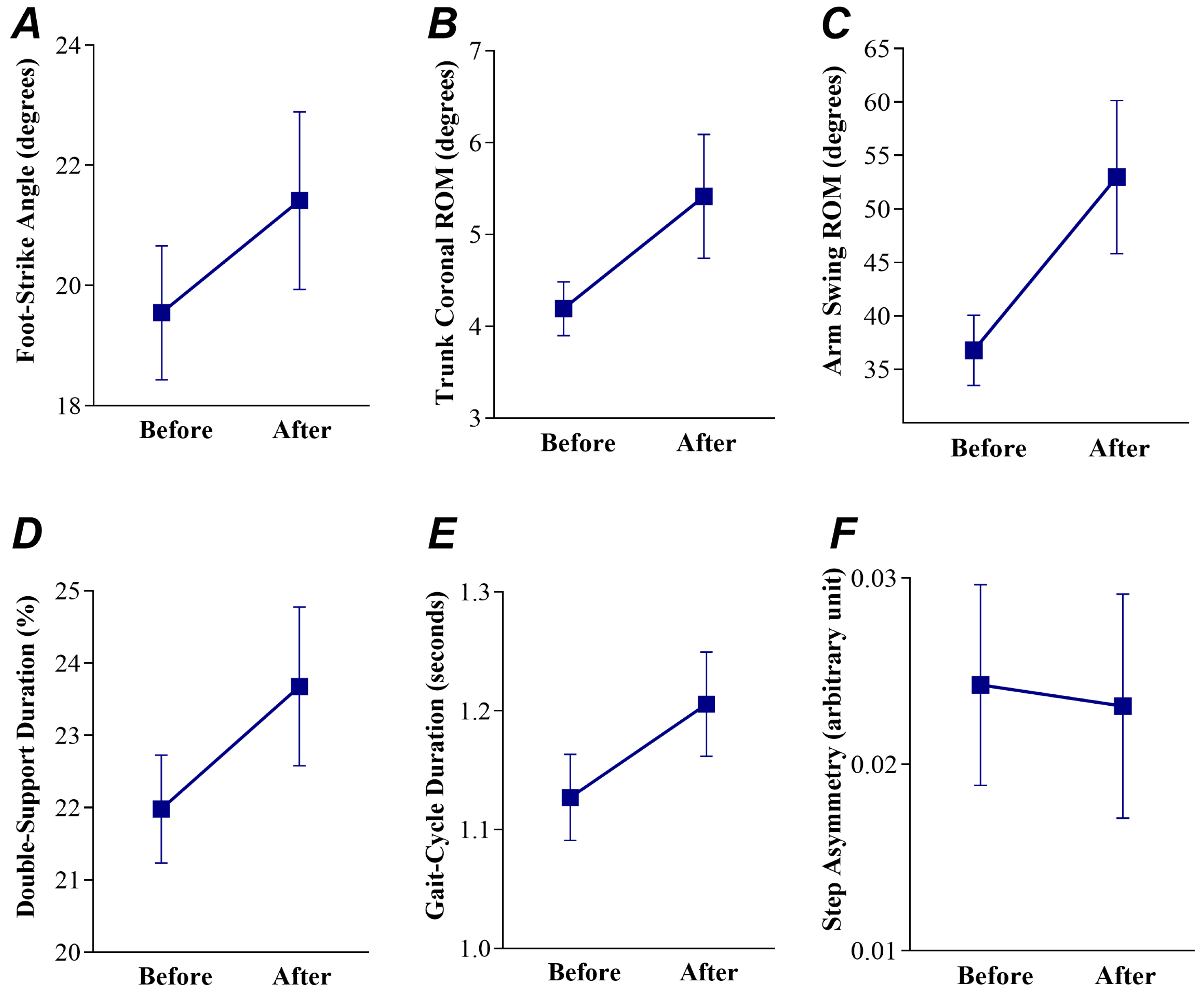
3.2. Treadmill Gait Training with Mobility Rehab Showed Moderate to Large Effect Sizes on Overground Upper and Lower Body Gait Metrics
3.3. Treadmill Gait Training with Mobility Rehab Showed a Safe Gait Pattern on Overground Lower Body Gait Metrics
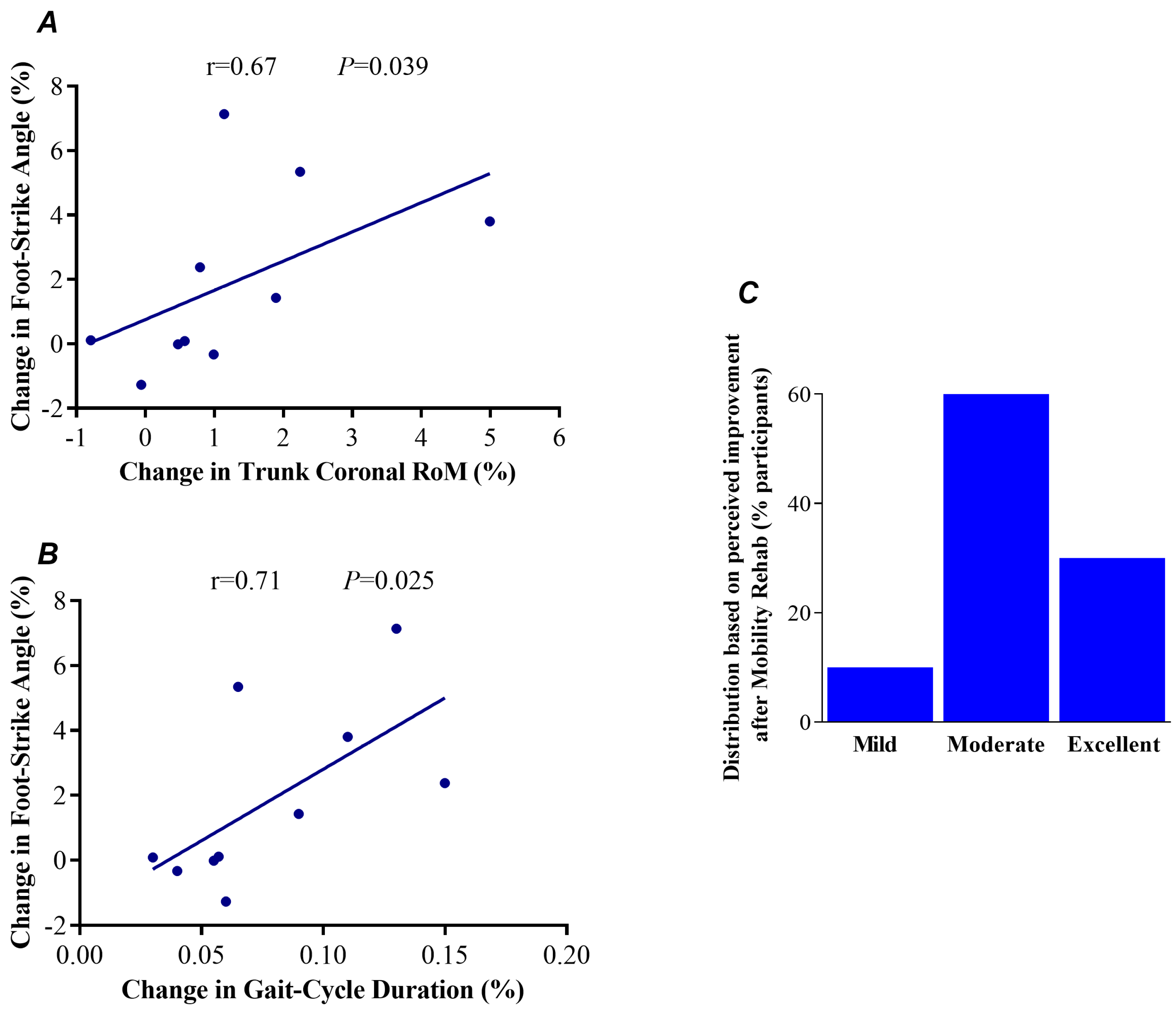
3.4. Changes in Foot-Strike Angle Are Associated with Changes in Upper and Lower Body Gait Metrics following Treadmill Gait Training with Mobility Rehab
3.5. Distribution of Rate Perceived
4. Discussion
4.1. Treadmill Gait Training with Mobility Rehab Is Feasible for Patients with PD
4.2. People with PD Showed a Safe Gait Pattern after Treadmill Gait Training with Mobility Rehab
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gray, P.; Hildebrand, K. Fall risk factors in Parkinson’s disease. J. Neurosci. Nurs. 2000, 32, 222–228. [Google Scholar] [CrossRef] [PubMed]
- Lewis, G.N.; Byblow, W.D.; Walt, S.E. Stride length regulation in Parkinson’s disease: The use of extrinsic, visual cues. Brain 2000, 123 Pt 10, 2077–2090. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, N.; Shah, V.V.; Carlson-Kuhta, P.; Nutt, J.G.; Horak, F.B.; Mancini, M. How to Select Balance Measures Sensitive to Parkinson’s Disease from Body-Worn Inertial Sensors-Separating the Trees from the Forest. Sensors 2019, 19, 3320. [Google Scholar] [CrossRef] [Green Version]
- Martini, D.N.; Morris, R.; Madhyastha, T.M.; Grabowski, T.J.; Oakley, J.; Hu, S.C.; Zabetian, C.P.; Edwards, K.L.; Hiller, A.; Chung, K.; et al. Relationships between Sensorimotor Inhibition and Mobility in Older Adults with and without Parkinson’s Disease. J. Gerontol. Ser. A Biol. Sci. Med. Sci. 2021, 76, 630–637. [Google Scholar] [CrossRef]
- Callais Franco do Nascimento, T.; Martins Gervasio, F.; Pignolo, A.; Augusto Santos Bueno, G.; Araujo do Carmo, A.; Martins Ribeiro, D.; D’Amelio, M.; Augusto Dos Santos Mendes, F. Assessment of the Kinematic Adaptations in Parkinson’s Disease Using the Gait Profile Score: Influences of Trunk Posture, a Pilot Study. Brain Sci. 2021, 11, 1605. [Google Scholar] [CrossRef]
- Cano-de-la-Cuerda, R.; Vela-Desojo, L.; Miangolarra-Page, J.C.; Macias-Macias, Y. Axial rigidity is related to the risk of falls in patients with Parkinson’s disease. NeuroRehabilitation 2017, 40, 569–577. [Google Scholar] [CrossRef]
- Curtze, C.; Nutt, J.G.; Carlson-Kuhta, P.; Mancini, M.; Horak, F.B. Levodopa Is a Double-Edged Sword for Balance and Gait in People with Parkinson’s Disease. Mov. Disord. 2015, 30, 1361–1370. [Google Scholar] [CrossRef] [PubMed]
- Mirelman, A.; Bonato, P.; Camicioli, R.; Ellis, T.D.; Giladi, N.; Hamilton, J.L.; Hass, C.J.; Hausdorff, J.M.; Pelosin, E.; Almeida, Q.J. Gait impairments in Parkinson’s disease. Lancet Neurol. 2019, 18, 697–708. [Google Scholar] [CrossRef]
- Chang, J.T.; Ganz, D.A. Quality indicators for falls and mobility problems in vulnerable elders. J. Am. Geriatr. Soc. 2007, 55 (Suppl. S2), S327–S334. [Google Scholar] [CrossRef] [PubMed]
- Gordt, K.; Gerhardy, T.; Najafi, B.; Schwenk, M. Effects of Wearable Sensor-Based Balance and Gait Training on Balance, Gait, and Functional Performance in Healthy and Patient Populations: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Gerontology 2018, 64, 74–89. [Google Scholar] [CrossRef]
- Byl, N.; Zhang, W.; Coo, S.; Tomizuka, M. Clinical impact of gait training enhanced with visual kinematic biofeedback: Patients with Parkinson’s disease and patients stable post stroke. Neuropsychologia 2015, 79 Pt B, 332–343. [Google Scholar] [CrossRef] [Green Version]
- Morris, R.; Stuart, S.; McBarron, G.; Fino, P.C.; Mancini, M.; Curtze, C. Validity of Mobility Lab (version 2) for gait assessment in young adults, older adults and Parkinson’s disease. Physiol. Meas. 2019, 40, 095003. [Google Scholar] [CrossRef] [PubMed]
- Ni, M.; Hazzard, J.B.; Signorile, J.F.; Luca, C. Exercise Guidelines for Gait Function in Parkinson’s Disease: A Systematic Review and Meta-analysis. Neurorehabil. Neural Repair 2018, 32, 872–886. [Google Scholar] [CrossRef]
- Hasegawa, N.; Shah, V.V.; Harker, G.; Carlson-Kuhta, P.; Nutt, J.G.; Lapidus, J.A.; Jung, S.H.; Barlow, N.; King, L.A.; Horak, F.B.; et al. Responsiveness of Objective vs. Clinical Balance Domain Outcomes for Exercise Intervention in Parkinson’s Disease. Front. Neurol. 2020, 11, 940. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.J.; Daniel, S.E.; Kilford, L.; Lees, A.J. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: A clinico-pathological study of 100 cases. J. Neurol. Neurosurg. Psychiatry 1992, 55, 181–184. [Google Scholar] [CrossRef] [Green Version]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology; Management Information Systems Research Center, University of Minnesota: Minneapolis, MN, USA, 1989; Volume 18, pp. 319–340. [Google Scholar]
- Rhea, M.R. Determining the magnitude of treatment effects in strength training research through the use of the effect size. J. Strength Condit. Res. 2004, 18, 918–920. [Google Scholar] [CrossRef]
- Lixandrao, M.E.; Ugrinowitsch, C.; Laurentino, G.; Libardi, C.A.; Aihara, A.Y.; Cardoso, F.N.; Tricoli, V.; Roschel, H. Effects of exercise intensity and occlusion pressure after 12 weeks of resistance training with blood-flow restriction. Eur. J. Appl. Physiol. 2015, 115, 2471–2480. [Google Scholar] [CrossRef] [PubMed]
- Nakagawa, S.; Cuthill, I.C. Effect size, confidence interval and statistical significance: A practical guide for biologists. Biol. Rev. Camb. Philos. Soc. 2007, 82, 591–605. [Google Scholar] [CrossRef]
- Rothman, K.J. No adjustments are needed for multiple comparisons. Epidemiology 1990, 1, 43–46. [Google Scholar] [CrossRef] [Green Version]
- Almeida, L.R.; Valenca, G.T.; Negreiros, N.N.; Pinto, E.B.; Oliveira-Filho, J. Comparison of Self-report and Performance-Based Balance Measures for Predicting Recurrent Falls in People with Parkinson Disease: Cohort Study. Phys. Ther. 2016, 96, 1074–1084. [Google Scholar] [CrossRef]
- Schwenk, M.; Grewal, G.S.; Honarvar, B.; Schwenk, S.; Mohler, J.; Khalsa, D.S.; Najafi, B. Interactive balance training integrating sensor-based visual feedback of movement performance: A pilot study in older adults. J. Neuroeng. Rehabil. 2014, 11, 164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ginis, P.; Nieuwboer, A.; Dorfman, M.; Ferrari, A.; Gazit, E.; Canning, C.G.; Rocchi, L.; Chiari, L.; Hausdorff, J.M.; Mirelman, A. Feasibility and effects of home-based smartphone-delivered automated feedback training for gait in people with Parkinson’s disease: A pilot randomized controlled trial. Parkinsonism Relat. Disord. 2016, 22, 28–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elm, J.J.; Daeschler, M.; Bataille, L.; Schneider, R.; Amara, A.; Espay, A.J.; Afek, M.; Admati, C.; Teklehaimanot, A.; Simuni, T. Feasibility and utility of a clinician dashboard from wearable and mobile application Parkinson’s disease data. NPJ Digit. Med. 2019, 2, 95. [Google Scholar] [CrossRef] [Green Version]
- Contin, M.; Riva, R.; Martinelli, P.; Balboni, M.; Tonello, C.; Albani, F.; Baruzzi, A. Objective assessment of foot strike in Parkinson’s disease. Eur. J. Neurol. 1996, 3, 221–226. [Google Scholar] [CrossRef]
- Zampieri, C.; Salarian, A.; Carlson-Kuhta, P.; Aminian, K.; Nutt, J.G.; Horak, F.B. The instrumented timed up and go test: Potential outcome measure for disease modifying therapies in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2010, 81, 171–176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, V.V.; McNames, J.; Mancini, M.; Carlson-Kuhta, P.; Spain, R.I.; Nutt, J.G.; El-Gohary, M.; Curtze, C.; Horak, F.B. Laboratory versus daily life gait characteristics in patients with multiple sclerosis, Parkinson’s disease, and matched controls. J. Neuroeng. Rehabil. 2020, 17, 159. [Google Scholar] [CrossRef] [PubMed]
- Winter, D.A. Human balance and posture control during standing and walking. Gait Posture 1995, 3, 193–214. [Google Scholar] [CrossRef]
- Kavanagh, J.J.; Barrett, R.S.; Morrison, S. Age-related differences in head and trunk coordination during walking. Hum. Mov. Sci. 2005, 24, 574–587. [Google Scholar] [CrossRef]
- Kavanagh, J.J.; Morrison, S.; Barrett, R.S. Coordination of head and trunk accelerations during walking. Eur. J. Appl. Physiol. 2005, 94, 468–475. [Google Scholar] [CrossRef]
- Wright, W.G.; Gurfinkel, V.S.; Nutt, J.; Horak, F.B.; Cordo, P.J. Axial hypertonicity in Parkinson’s disease: Direct measurements of trunk and hip torque. Exp. Neurol. 2007, 208, 38–46. [Google Scholar] [CrossRef]
- Mirelman, A.; Bernad-Elazari, H.; Thaler, A.; Giladi-Yacobi, E.; Gurevich, T.; Gana-Weisz, M.; Saunders-Pullman, R.; Raymond, D.; Doan, N.; Bressman, S.B.; et al. Arm swing as a potential new prodromal marker of Parkinson’s disease. Mov. Disord. 2016, 31, 1527–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zijlstra, A.; Mancini, M.; Chiari, L.; Zijlstra, W. Biofeedback for training balance and mobility tasks in older populations: A systematic review. J. Neuroeng. Rehabil. 2010, 7, 58. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participants | Range | |
|---|---|---|
| Characteristics | (n = 10) | |
| Men/women (number) | 7/3 | - |
| Age (years) | 69.3 (5.6) | 60 to 75 |
| Educational level (years) | 16.0 (3.1) | 12 to 20 |
| Body mass (kg) | 87.5 (2.8) | 83 to 91 |
| Height (cm) | 1.7 (7.5) | 1.6 to 1.8 |
| Body mass index (kg/m2) | 28.8 (3.0) | 25 to 34 |
| Years since diagnosis (years) | 8.4 (3.7) | 3 to 14 |
| Hoehn and Yahr staging scale (a.u) | ||
| 2 | 9 | - |
| 3 | 1 | - |
| Symptom-dominant side (R/L) | 4/6 | - |
| MDS-UPDRS-III (scores) | 41.3 (6.8) | 29 to 53 |
| ABC (scores) | 88.1 (5.8) | 80 to 96 |
| L-Dopa equivalent units (mg·day−1) | 789.6 (295.3) | 375 to 1200 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva-Batista, C.; Harker, G.; Vitorio, R.; Horak, F.B.; Carlson-Kuhta, P.; Pearson, S.; VanDerwalker, J.; El-Gohary, M.; Mancini, M. Feasibility of a Novel Therapist-Assisted Feedback System for Gait Training in Parkinson’s Disease. Sensors 2023, 23, 128. https://doi.org/10.3390/s23010128
Silva-Batista C, Harker G, Vitorio R, Horak FB, Carlson-Kuhta P, Pearson S, VanDerwalker J, El-Gohary M, Mancini M. Feasibility of a Novel Therapist-Assisted Feedback System for Gait Training in Parkinson’s Disease. Sensors. 2023; 23(1):128. https://doi.org/10.3390/s23010128
Chicago/Turabian StyleSilva-Batista, Carla, Graham Harker, Rodrigo Vitorio, Fay B. Horak, Patricia Carlson-Kuhta, Sean Pearson, Jess VanDerwalker, Mahmoud El-Gohary, and Martina Mancini. 2023. "Feasibility of a Novel Therapist-Assisted Feedback System for Gait Training in Parkinson’s Disease" Sensors 23, no. 1: 128. https://doi.org/10.3390/s23010128