
Quantification of Error Sources with Inertial Measurement Units in Sports

Abstract
:1. Introduction
2. Materials and Methods
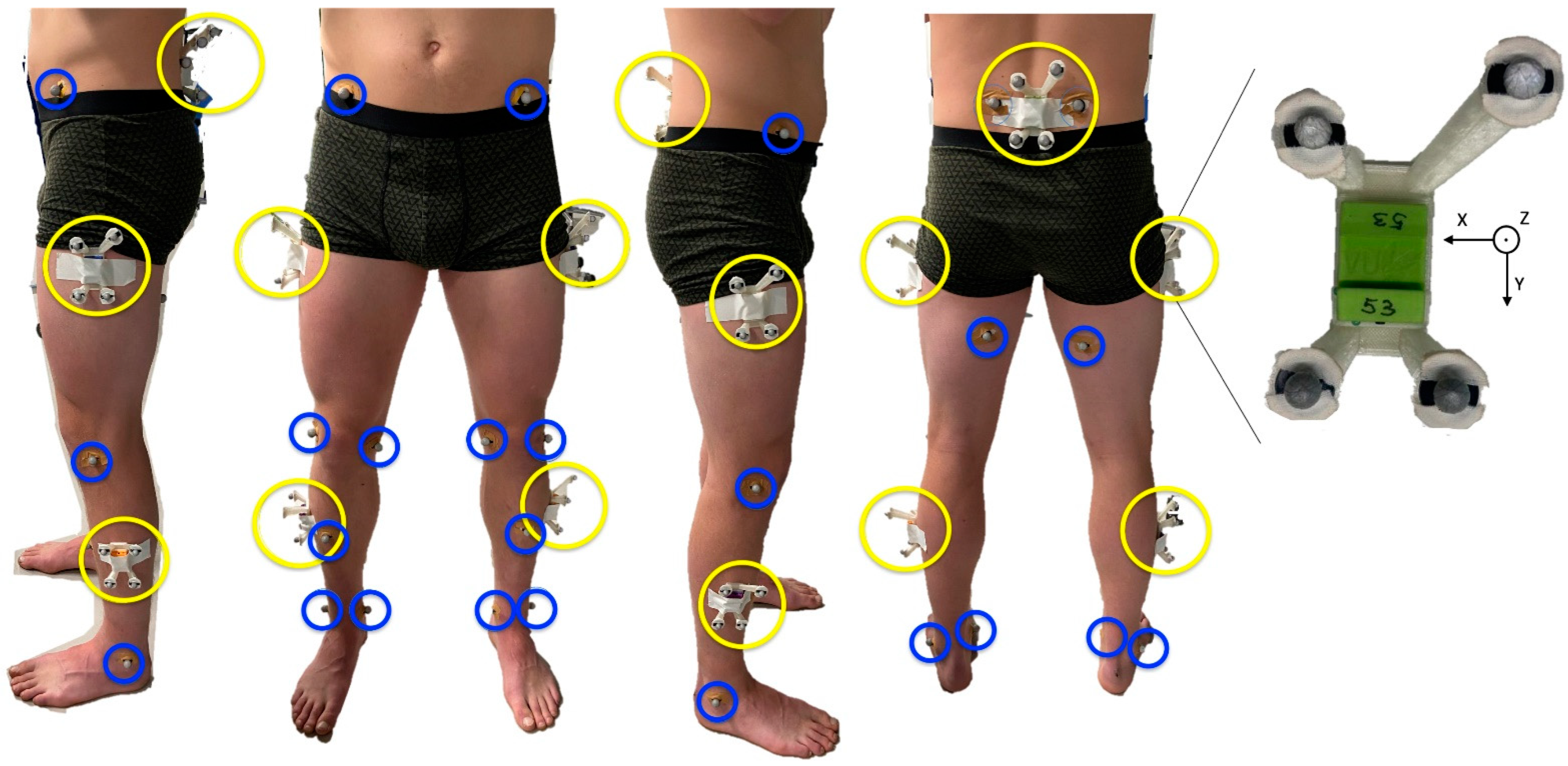
2.1. Subjects and Instrumentation
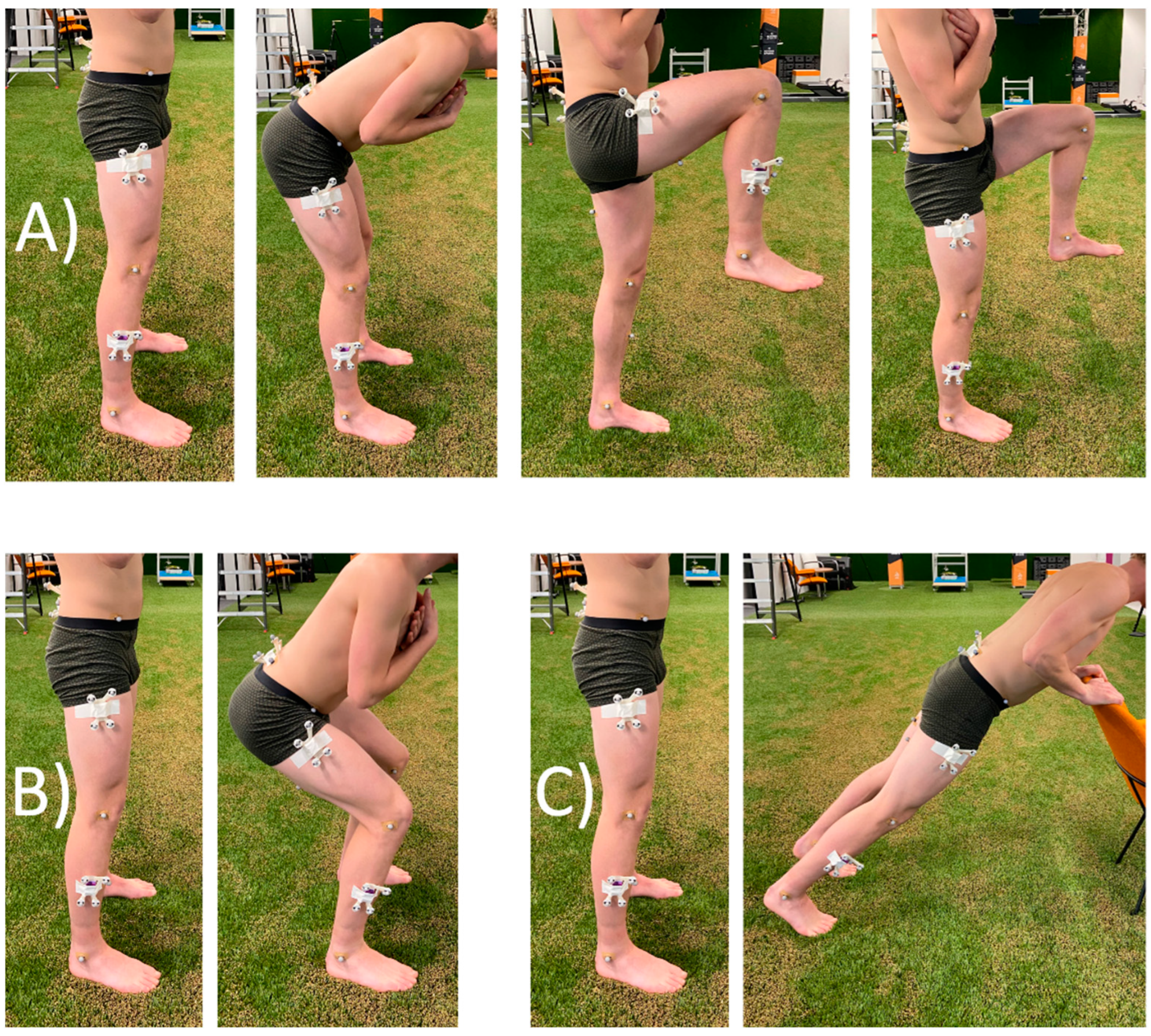
2.2. Protocol
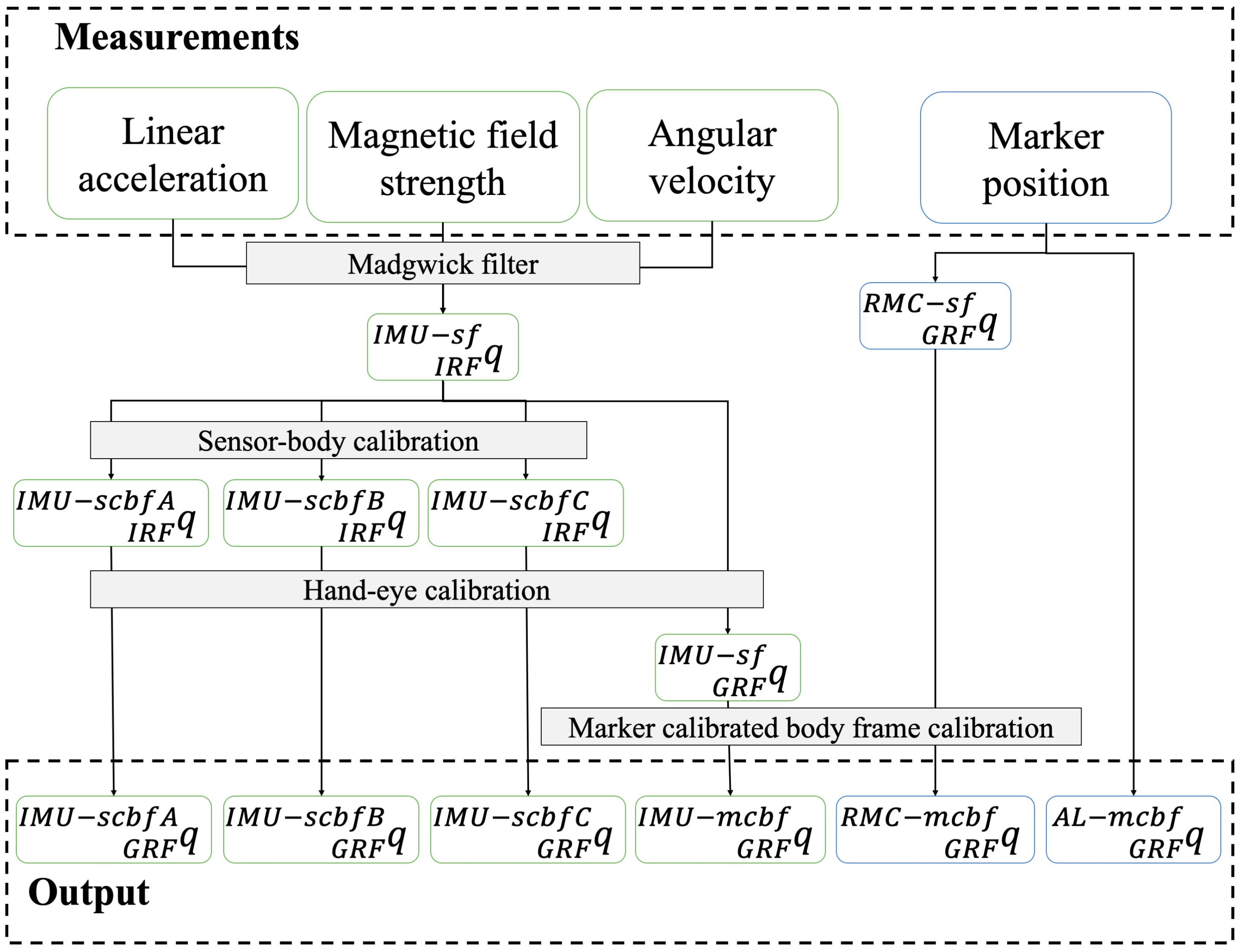
2.3. Data Processing
2.4. Data Analysis
3. Results
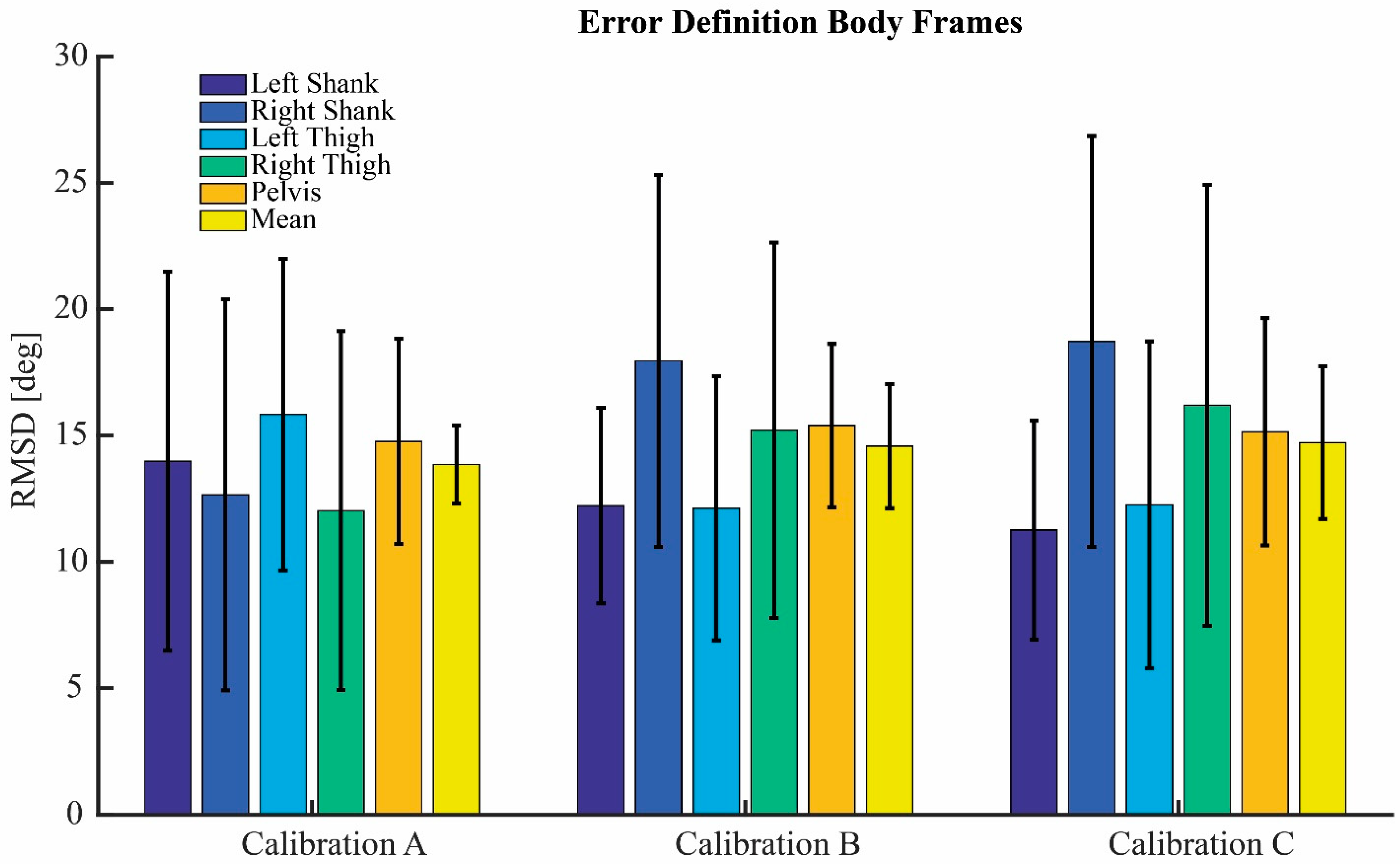
3.1. Definition Body Frames
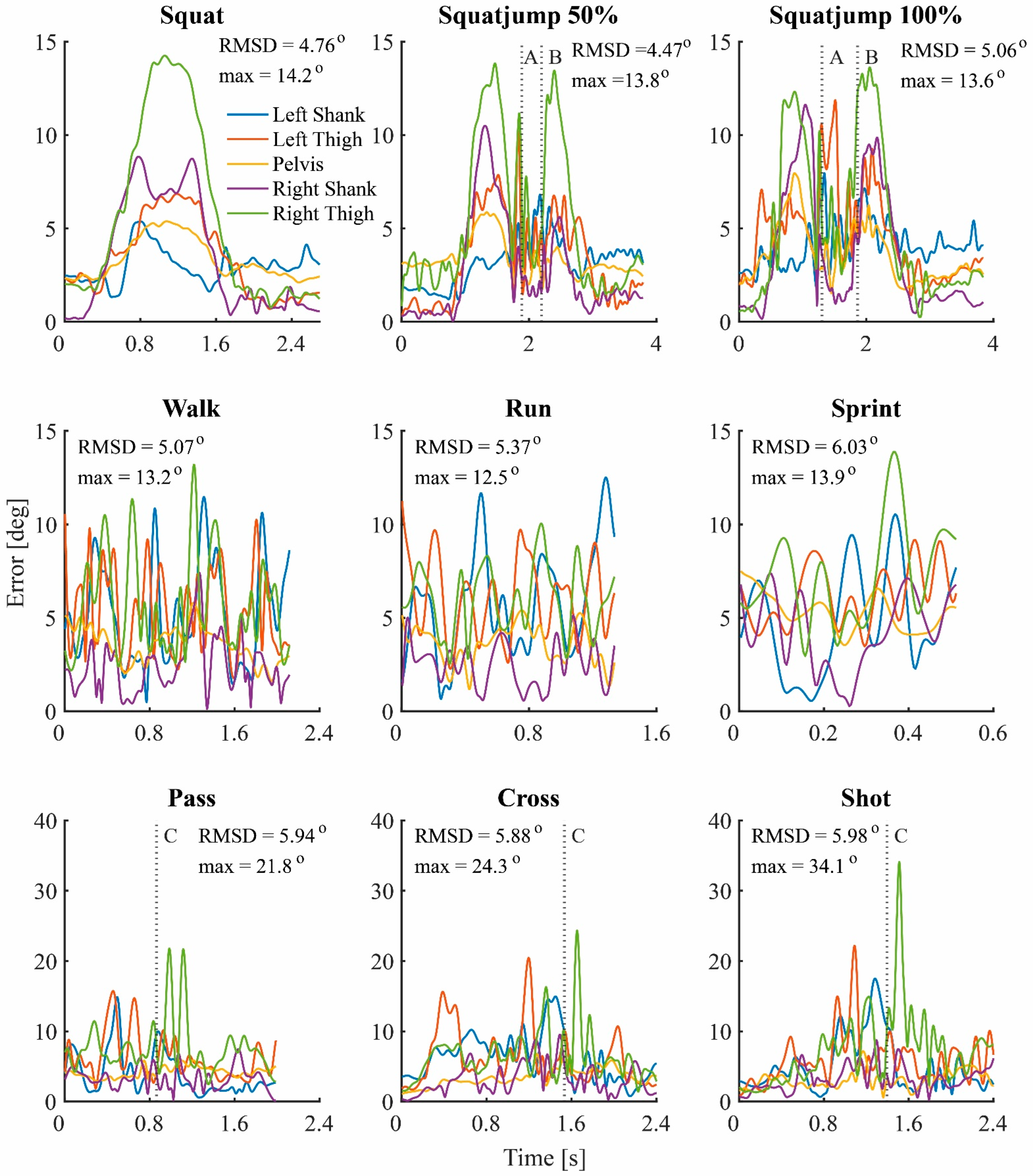
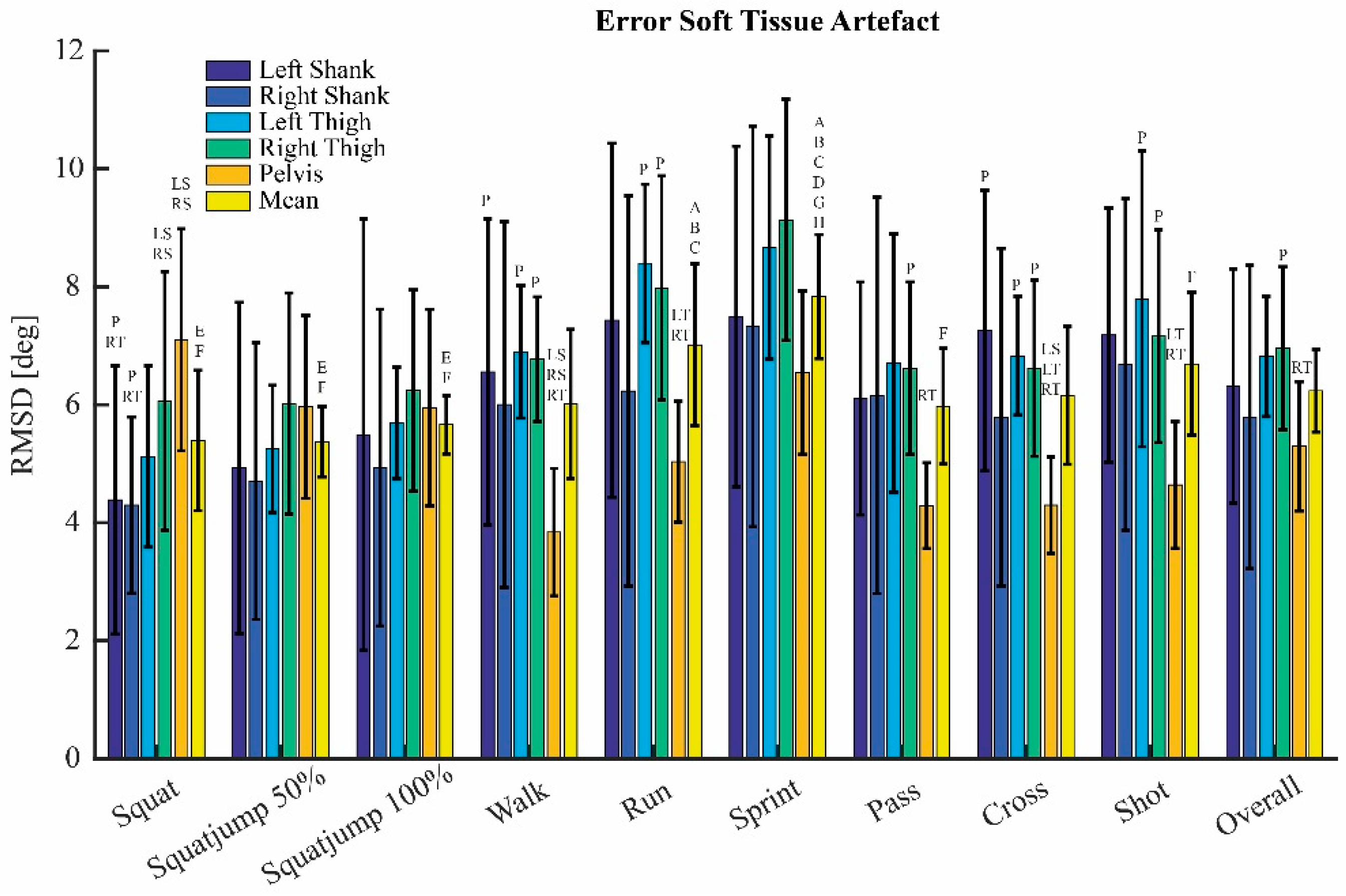
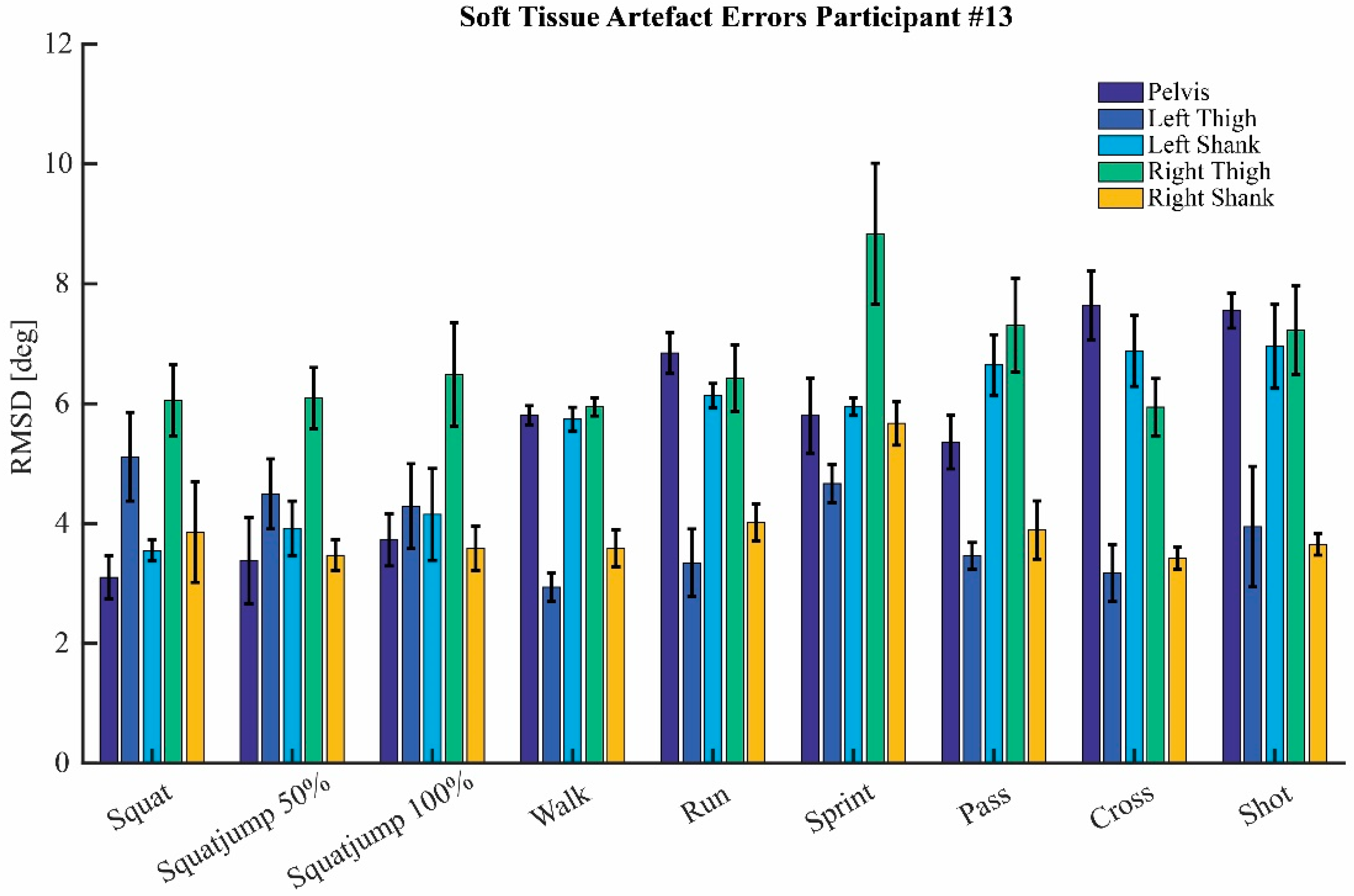
3.2. Soft Tissue Artefact
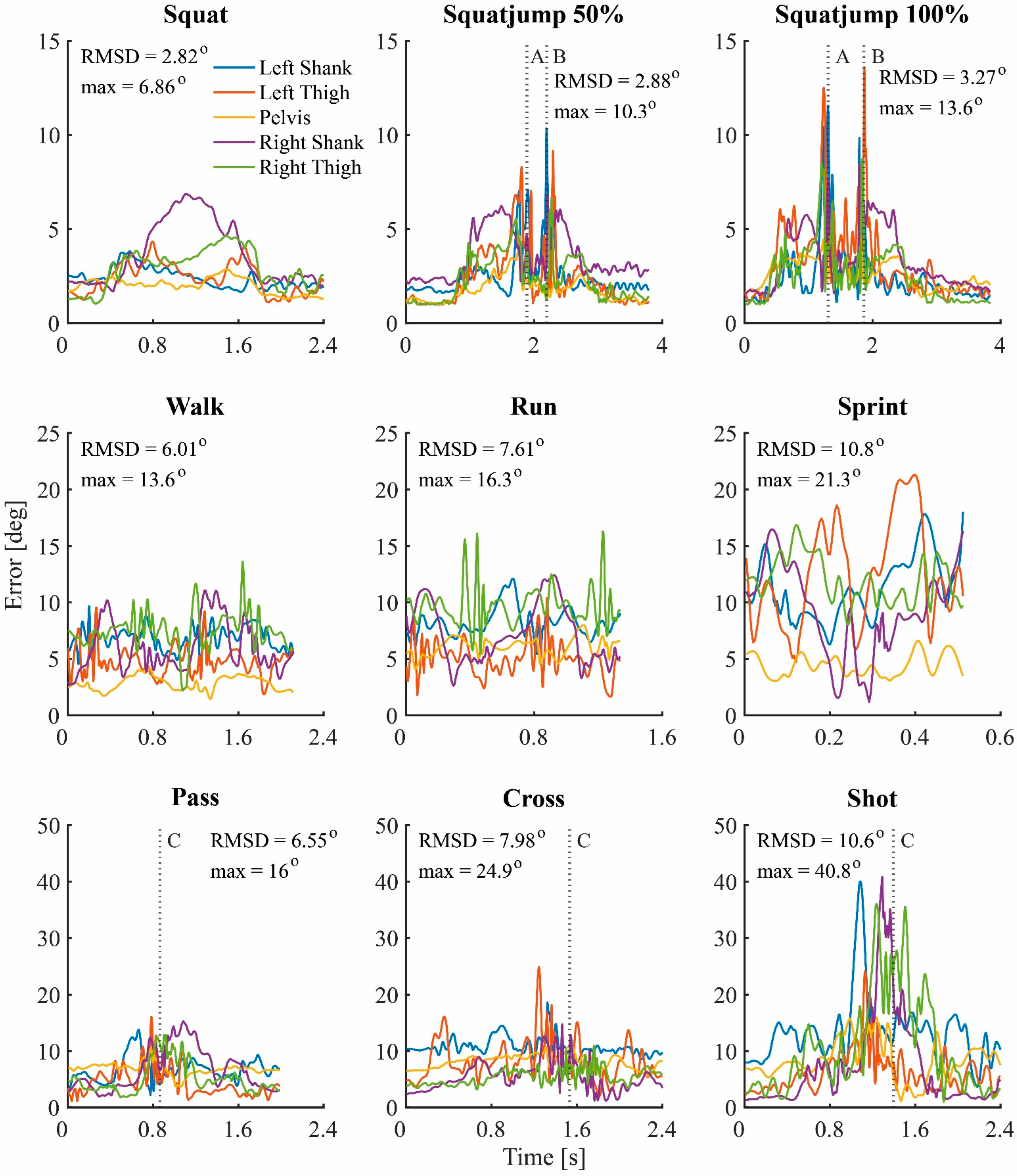
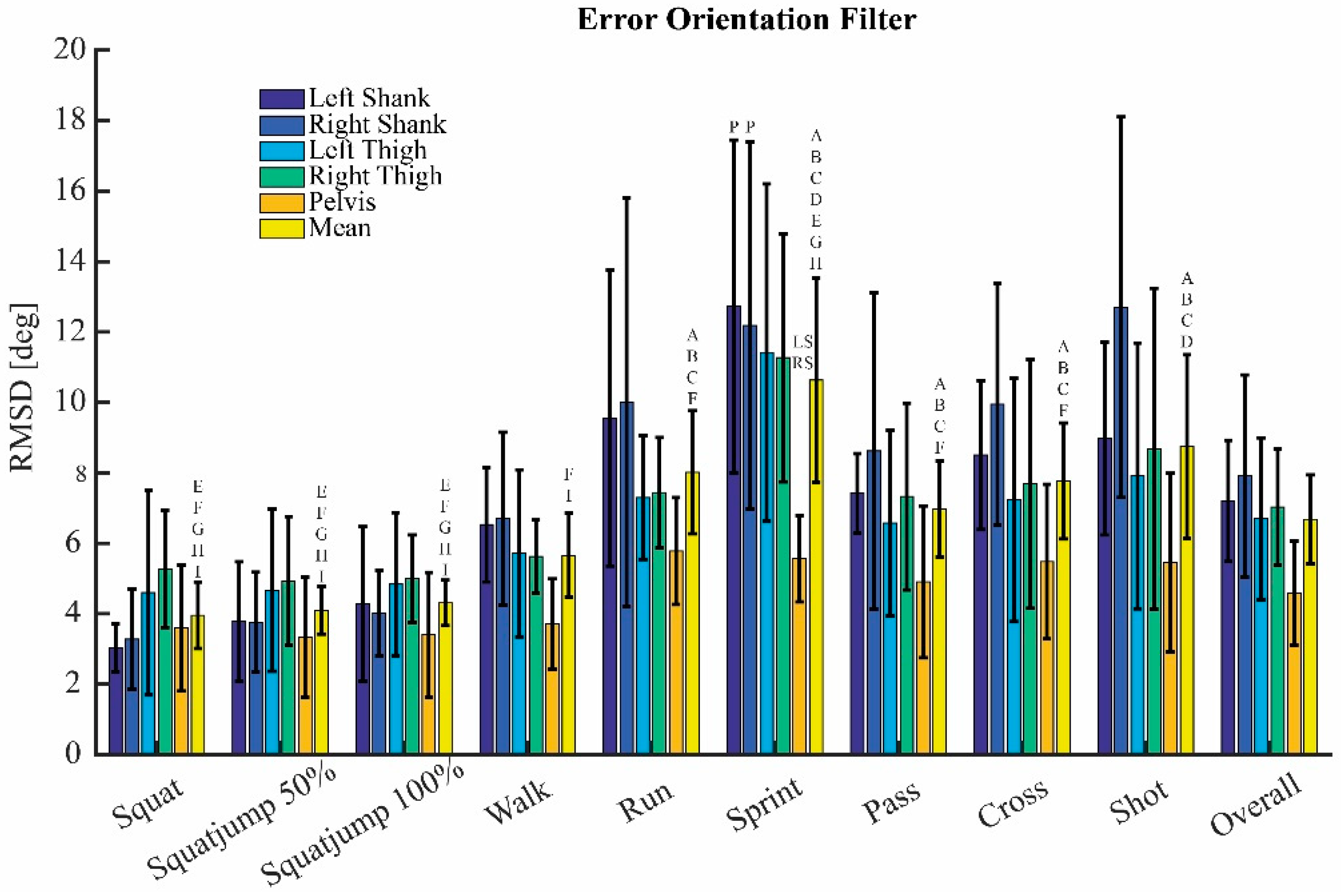
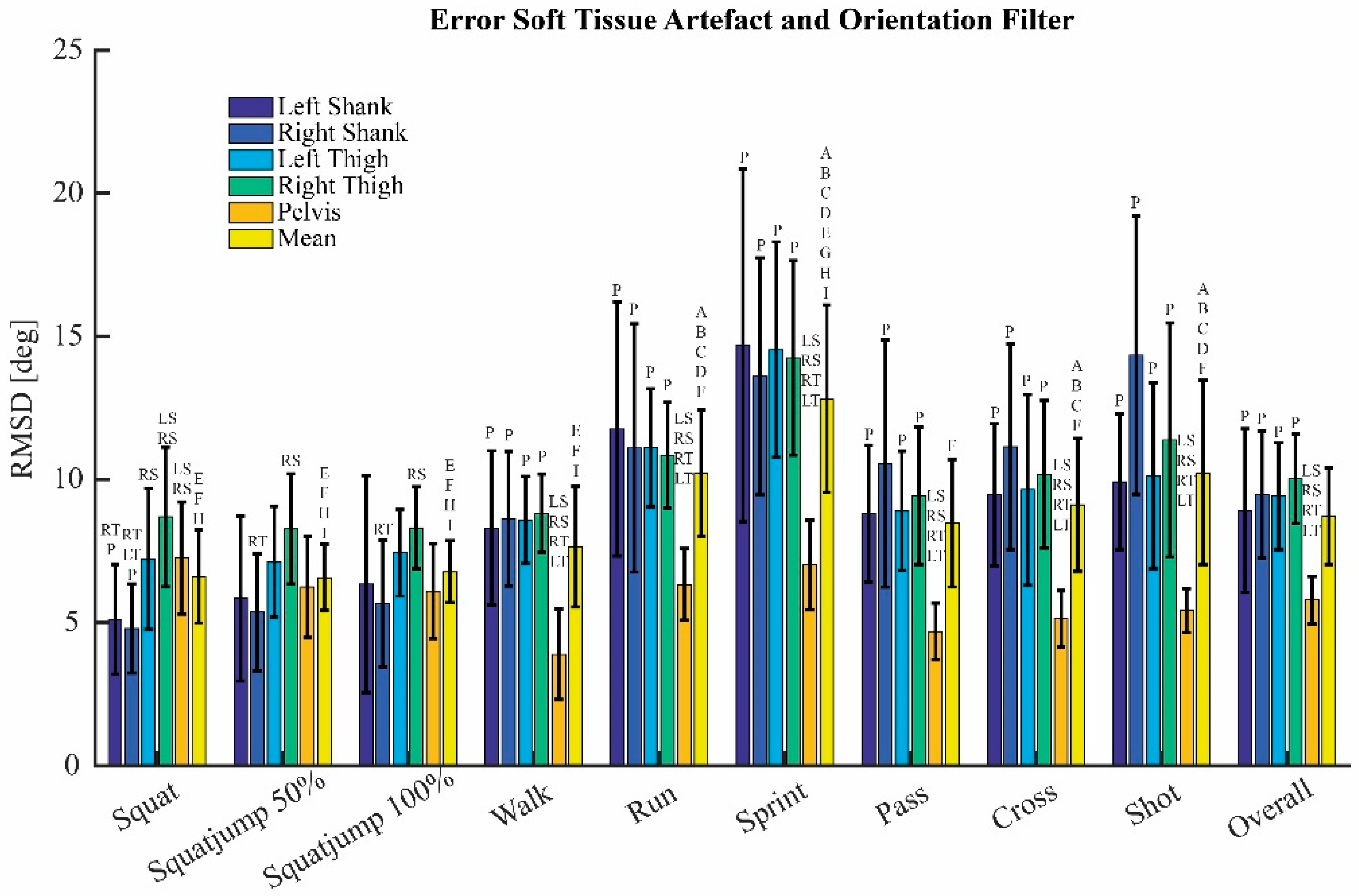
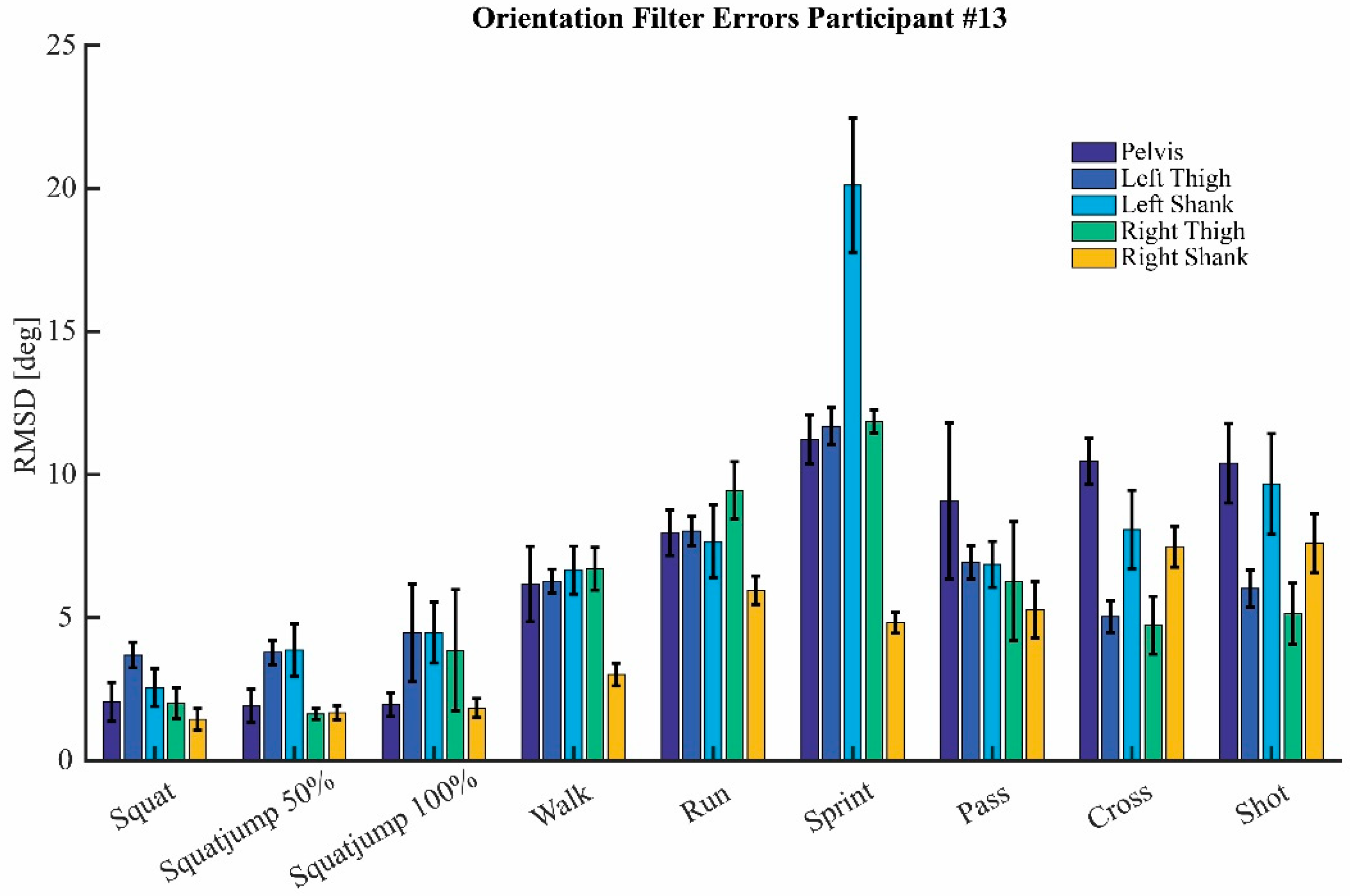
3.3. Orientation Filter
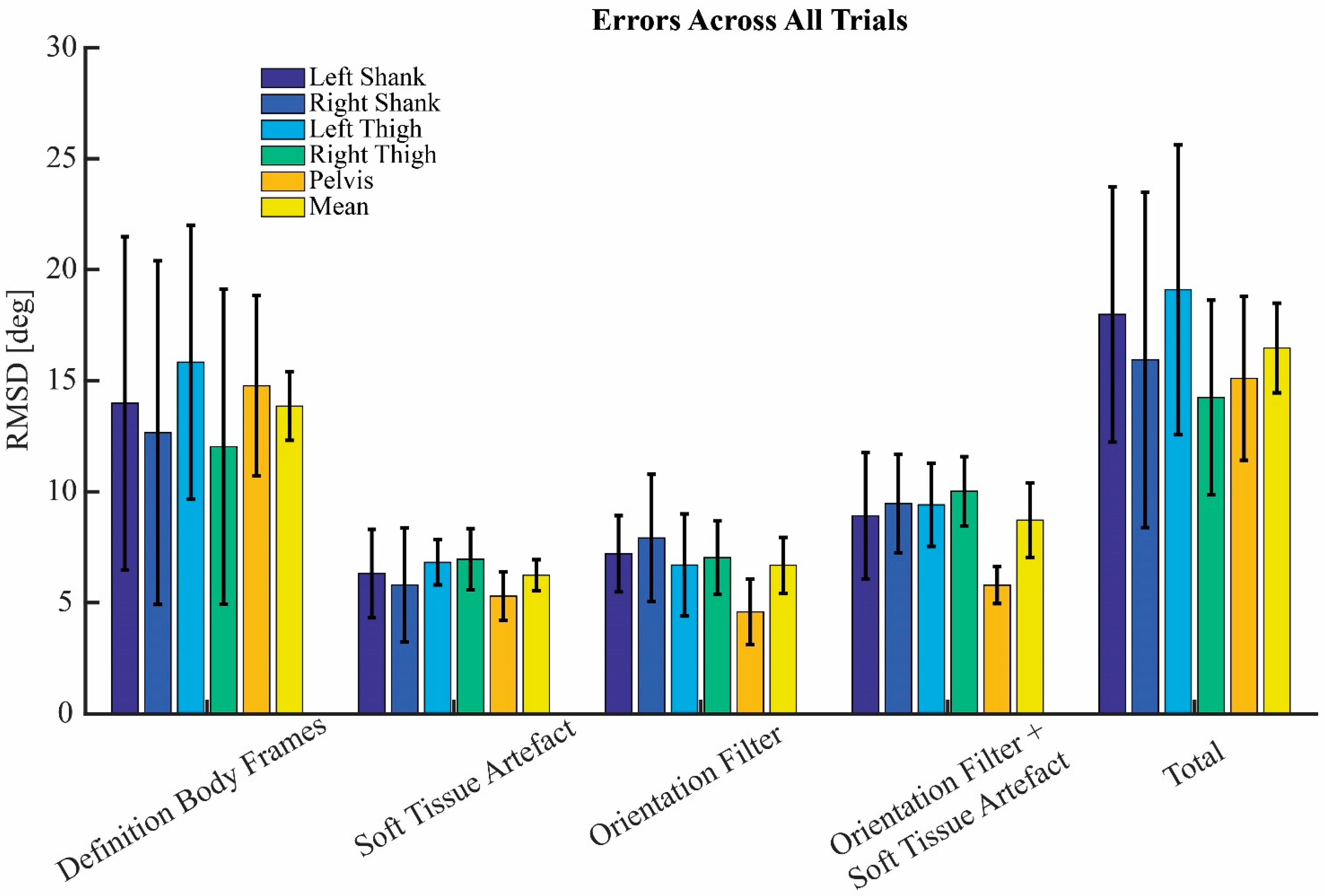
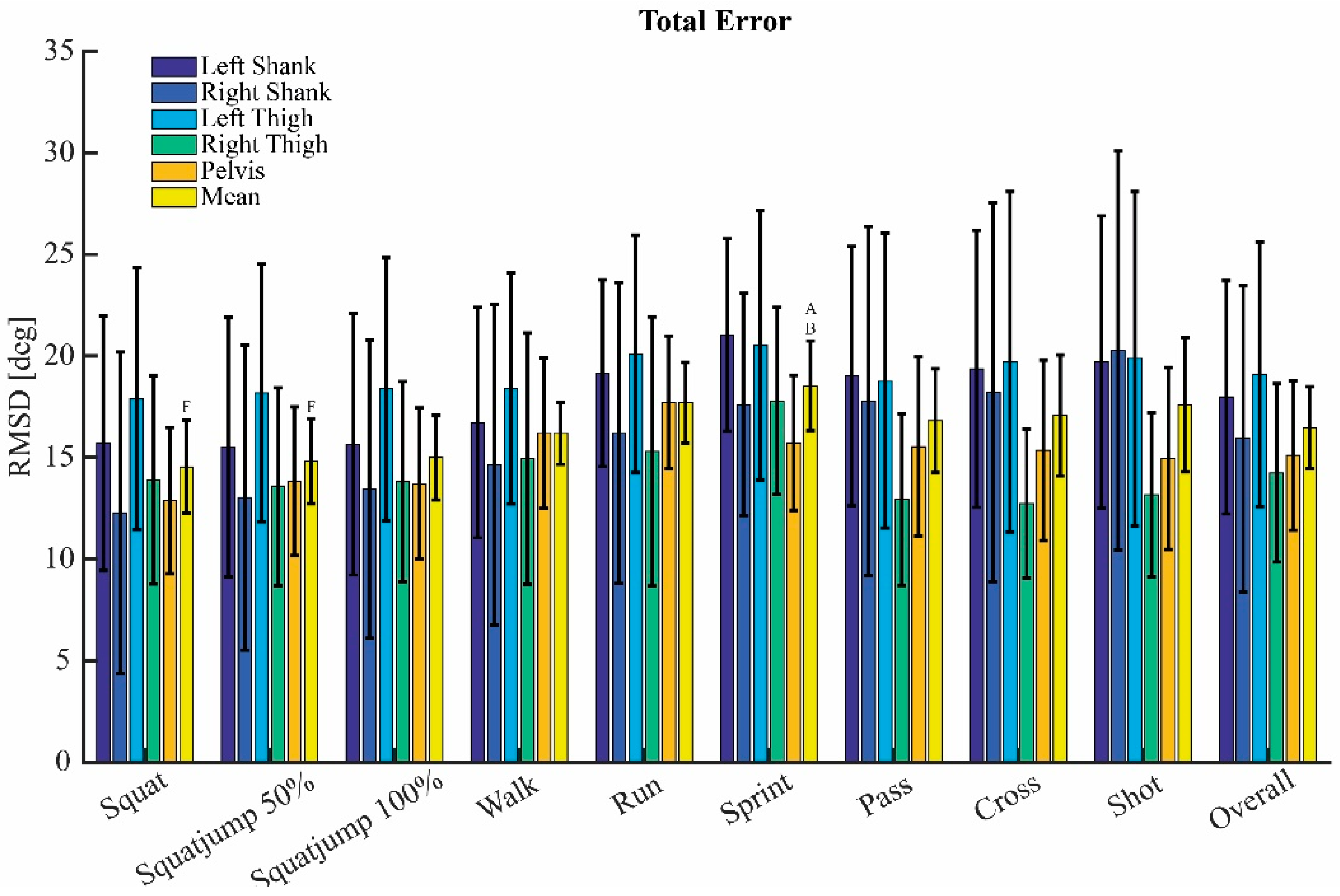
3.4. Total Error
4. Discussion
4.1. Definition Body Frames
4.2. Soft Tissue Artefact
4.3. Orientation Filter
4.4. Total Error
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A






References
- Ancillao, A. Stereophotogrammetry in Functional Evaluation: History and Modern Protocols. In Modern Functional Evaluation Methods for Muscle Strength and Gait Analysis; Springer: Berlin/Heidelberg, Germany, 2018; pp. 1–29. [Google Scholar]
- Lopez-Nava, I.H.; Munoz-Melendez, A. Wearable inertial sensors for human motion analysis: A review. IEEE Sens. J. 2016, 16, 7821–7834. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Mecheri, H.; Larue, C.; Plamondon, A. Validation of inertial measurement units with an optoelectronic system for whole-body motion analysis. Med. Biol. Eng. Comput. 2017, 55, 609–619. [Google Scholar] [CrossRef]
- Leardini, A.; Lullini, G.; Giannini, S.; Berti, L.; Ortolani, M.; Caravaggi, P. Validation of the angular measurements of a new inertial-measurement-unit based rehabilitation system: Comparison with state-of-the-art gait analysis. J. Neuroeng. Rehabil. 2014, 11, 136. [Google Scholar] [CrossRef] [Green Version]
- Peruzzi, A.; Della Croce, U.; Cereatti, A. Estimation of stride length in level walking using an inertial measurement unit attached to the foot: A validation of the zero velocity assumption during stance. J. Biomech. 2011, 44, 1991–1994. [Google Scholar] [CrossRef]
- Teufl, W.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Validity of inertial sensor based 3D joint kinematics of static and dynamic sport and physiotherapy specific movements. PLoS ONE 2019, 14, e0213064. [Google Scholar] [CrossRef] [Green Version]
- Wilmes, E.; de Ruiter, C.J.; Bastiaansen, B.J.; Zon, J.F.v.; Vegter, R.J.; Brink, M.S.; Goedhart, E.A.; Lemmink, K.A.; Savelsbergh, G.J. Inertial sensor-based motion tracking in football with movement intensity quantification. Sensors 2020, 20, 2527. [Google Scholar] [CrossRef]
- Bergamini, E.; Guillon, P.; Camomilla, V.; Pillet, H.; Skalli, W.; Cappozzo, A. Trunk inclination estimate during the sprint start using an inertial measurement unit: A validation study. J. Appl. Biomech. 2013, 29, 622–627. [Google Scholar] [CrossRef] [Green Version]
- Morrow, M.M.; Lowndes, B.; Fortune, E.; Kaufman, K.R.; Hallbeck, M.S. Validation of inertial measurement units for upper body kinematics. J. Appl. Biomech. 2017, 33, 227–232. [Google Scholar] [CrossRef]
- Morton, L.; Baillie, L.; Ramirez-Iniguez, R. Pose calibrations for inertial sensors in rehabilitation applications. In Proceedings of the 2013 IEEE 9th International Conference on Wireless and Mobile Computing, Networking and Communications (WiMob), Lyon, France, 7–9 October 2013; pp. 204–211. [Google Scholar]
- Palermo, E.; Rossi, S.; Marini, F.; Patanè, F.; Cappa, P. Experimental evaluation of accuracy and repeatability of a novel body-to-sensor calibration procedure for inertial sensor-based gait analysis. Measurement 2014, 52, 145–155. [Google Scholar] [CrossRef]
- Teufl, W.; Lorenz, M.; Miezal, M.; Taetz, B.; Fröhlich, M.; Bleser, G. Towards inertial sensor based mobile gait analysis: Event-detection and spatio-temporal parameters. Sensors 2018, 19, 38. [Google Scholar] [CrossRef]
- De Vries, W.; Veeger, H.; Cutti, A.; Baten, C.; Van Der Helm, F. Functionally interpretable local coordinate systems for the upper extremity using inertial & magnetic measurement systems. J. Biomech. 2010, 43, 1983–1988. [Google Scholar]
- Favre, J.; Aissaoui, R.; Jolles, B.M.; de Guise, J.A.; Aminian, K. Functional calibration procedure for 3D knee joint angle description using inertial sensors. J. Biomech. 2009, 42, 2330–2335. [Google Scholar] [CrossRef]
- Peters, A.; Galna, B.; Sangeux, M.; Morris, M.; Baker, R. Quantification of soft tissue artifact in lower limb human motion analysis: A systematic review. Gait Posture 2010, 31, 1–8. [Google Scholar] [CrossRef]
- Cereatti, A.; Bonci, T.; Akbarshahi, M.; Aminian, K.; Barré, A.; Begon, M.; Benoit, D.L.; Charbonnier, C.; Dal Maso, F.; Fantozzi, S. Standardization proposal of soft tissue artefact description for data sharing in human motion measurements. J. Biomech. 2017, 62, 5–13. [Google Scholar] [CrossRef] [Green Version]
- Madgwick, S.O.; Harrison, A.J.; Vaidyanathan, A. Estimation of IMU and MARG orientation using a gradient descent algorithm. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011. [Google Scholar] [CrossRef]
- De Vries, W.; Veeger, H.; Baten, C.; Van Der Helm, F. Magnetic distortion in motion labs, implications for validating inertial magnetic sensors. Gait Posture 2009, 29, 535–541. [Google Scholar] [CrossRef]
- de Ruiter, C.J.; van Dieën, J.H. Stride and step length obtained with inertial measurement units during maximal sprint acceleration. Sports 2019, 7, 202. [Google Scholar] [CrossRef] [Green Version]
- Cappozzo, A.; Catani, F.; Della Croce, U.; Leardini, A. Position and orientation in space of bones during movement: Anatomical frame definition and determination. Clin. Biomech. 1995, 10, 171–178. [Google Scholar] [CrossRef]
- Wu, G.; Siegler, S.; Allard, P.; Kirtley, C.; Leardini, A.; Rosenbaum, D.; Whittle, M.; D’Lima, D.D.; Cristofolini, L.; Witte, H. ISB recommendation on definitions of joint coordinate system of various joints for the reporting of human joint motion—Part I: Ankle, hip, and spine. J. Biomech. 2002, 35, 543–548. [Google Scholar] [CrossRef]
- Kok, M.; Schön, T.B. Magnetometer calibration using inertial sensors. IEEE Sens. J. 2016, 16, 5679–5689. [Google Scholar] [CrossRef] [Green Version]
- Tedaldi, D.; Pretto, A.; Menegatti, E. A robust and easy to implement method for IMU calibration without external equipments. In Proceedings of the 2014 IEEE International Conference on Robotics and Automation (ICRA), Hong Kong, China, 31 May–7 June 2014; pp. 3042–3049. [Google Scholar]
- Hol, J.D. Sensor Fusion and Calibration of Inertial Sensors, Vision, Ultra-Wideband and GPS; Linköping University Electronic Press: Linköping, Sweden, 2011. [Google Scholar]
- Roetenberg, D.; Luinge, H.; Slycke, P. Xsens MVN: Full 6DOF human motion tracking using miniature inertial sensors. Xsens Motion Technol. BV Tech. Rep. 2009, 1, 1–7. [Google Scholar]
- Houck, J.; Yack, H.J.; Cuddeford, T. Validity and comparisons of tibiofemoral orientations and displacement using a femoral tracking device during early to mid stance of walking. Gait Posture 2004, 19, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Gao, B.; Conrad, B.; Zheng, N. Comparison of skin error reduction techniques for skeletal motion analysis. J. Biomech. 2007, 40, S551. [Google Scholar] [CrossRef]
- Cavallo, A.; Cirillo, A.; Cirillo, P.; De Maria, G.; Falco, P.; Natale, C.; Pirozzi, S. Experimental comparison of sensor fusion algorithms for attitude estimation. IFAC Proc. Vol. 2014, 47, 7585–7591. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comparisons | Frame 1 | Frame 2 | Error |
|---|---|---|---|
| #1 | IMU-scbfA | IMU-mcbf | Error definition body frames A |
| #2 | IMU-scbfB | IMU-mcbf | Error definition body frames B |
| #3 | IMU-scbfC | IMU-mcbf | Error definition body frames C |
| #4 | RMC-mcbf | AL-mcbf | Soft Tissue Artefact |
| #5 | IMU-mcbf | RMC-mcbf | Error orientation filter |
| #6 | IMU-mcbf | AL-mcbf | Error orientation filter + Soft Tissue Artefact |
| #7 | IMU-scbfA | AL-mcbf | Total error with calibration A |
| #8 | IMU-scbfB | AL-mcbf | Total error with calibration B |
| #9 | IMU-scbfC | AL-mcbf | Total error with calibration C |
| Error STA | Error Orientation Filter | Total Error | ||||
|---|---|---|---|---|---|---|
| Effects: | p | η2 | p | η2 | p | η2 |
| Movement type | <0.001 | 0.100 | <0.001 | 0.201 | <0.001 | 0.046 |
| Intensity | <0.001 | 0.052 | <0.001 | 0.066 | <0.001 | 0.008 |
| Segment | <0.001 | 0.154 | 0.018 | 0.104 | 0.604 * | 0.040 |
| Movement type: Intensity | <0.001 | 0.042 | <0.001 | 0.063 | 0.046 | 0.003 |
| Movement type: Segment | <0.001 | 0.132 | 0.006 | 0.055 | <0.001 | 0.038 |
| Intensity: Segment | 0.750 * | 0.004 | <0.001 | 0.019 | <0.001 | 0.008 |
| Movement type: Intensity: Segment | 0.001 | 0.025 | 0.003 | 0.012 | <0.001 | 0.009 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kamstra, H.; Wilmes, E.; van der Helm, F.C.T. Quantification of Error Sources with Inertial Measurement Units in Sports. Sensors 2022, 22, 9765. https://doi.org/10.3390/s22249765
Kamstra H, Wilmes E, van der Helm FCT. Quantification of Error Sources with Inertial Measurement Units in Sports. Sensors. 2022; 22(24):9765. https://doi.org/10.3390/s22249765
Chicago/Turabian StyleKamstra, Haye, Erik Wilmes, and Frans C. T. van der Helm. 2022. "Quantification of Error Sources with Inertial Measurement Units in Sports" Sensors 22, no. 24: 9765. https://doi.org/10.3390/s22249765