
Wearable Immersive Virtual Reality Device for Promoting Physical Activity in Parkinson’s Disease Patients




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Wearable Device
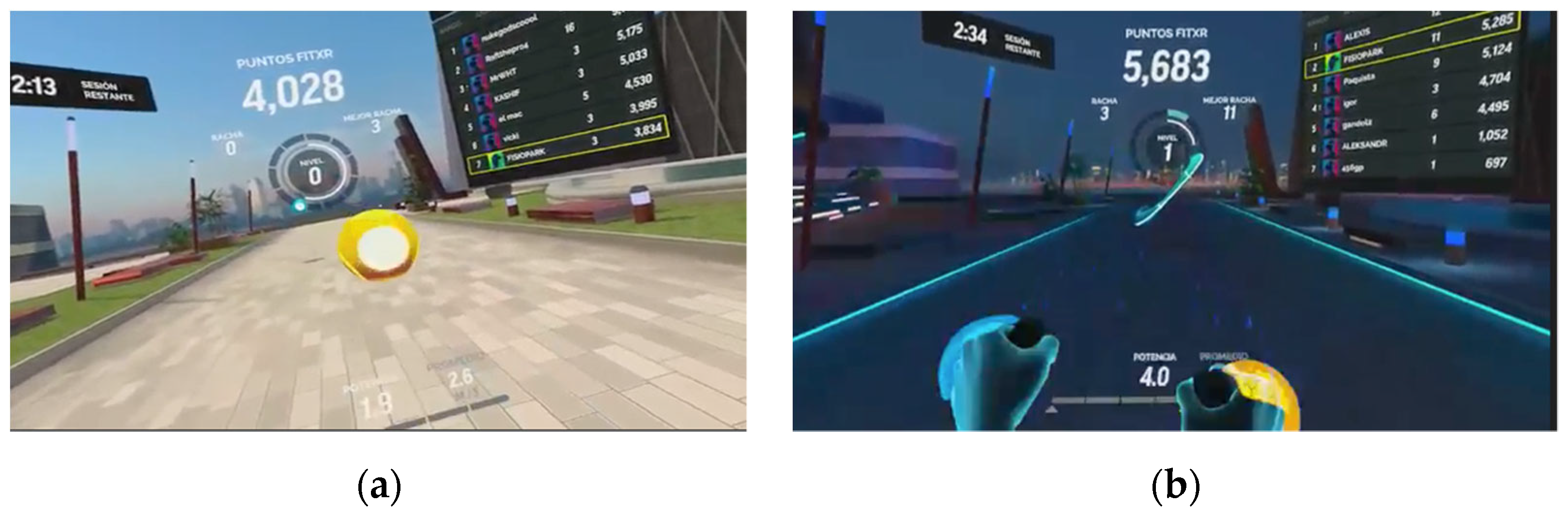
2.3. The Exergame
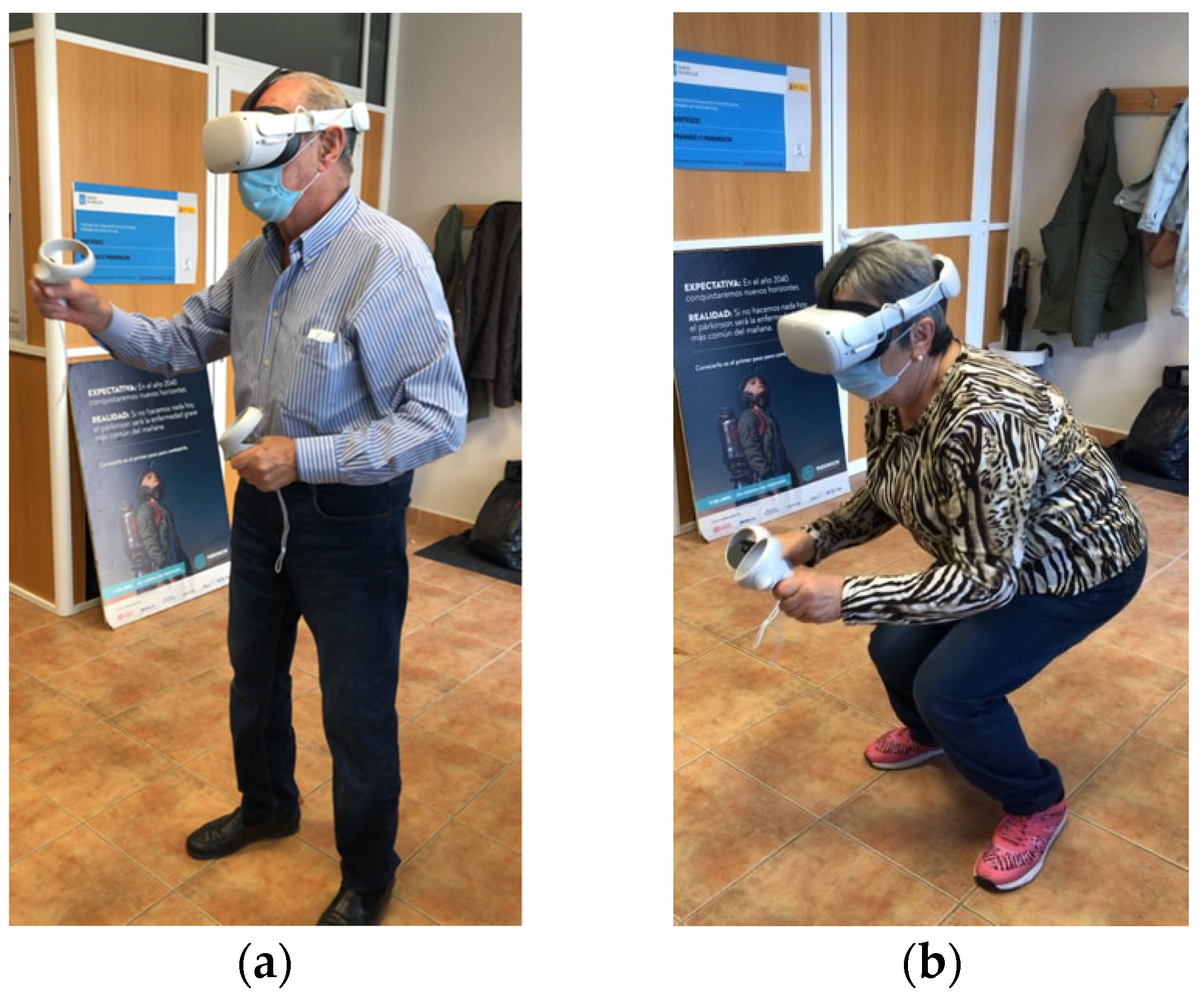
2.4. Intervention
2.5. Assessments
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dorsey, E.R.; Bloem, B.R. The Parkinson Pandemic—A Call to Action. JAMA Neurol. 2018, 75, 9. [Google Scholar] [CrossRef]
- Keus, S.H.J.; Bloem, B.R.; Hendriks, E.J.M.; Bredero-Cohen, A.B.; Munneke, M.; and on behalf of the Practice Recommendations Development Group. Evidence-based analysis of physical therapy in Parkinson’s disease with recommendations for practice and research. Mov. Disord. 2007, 22, 451–460. [Google Scholar] [CrossRef]
- Goodwin, V.A.; Richards, S.H.; Taylor, R.S.; Taylor, A.H.; Campbell, J.L. The effectiveness of exercise interventions for people with Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2008, 23, 631–640. [Google Scholar] [CrossRef] [PubMed]
- Mak, M.K.; Wong-Yu, I.S.; Shen, X.; Chung, C.L. Long-term effects of exercise and physical therapy in people with Parkinson disease. Nat. Rev. Neurol. 2017, 13, 689–703. [Google Scholar] [CrossRef] [PubMed]
- Chen, Z.; Li, G.; Liu, J. Autonomic dysfunction in Parkinson’s disease: Implications for pathophysiology, diagnosis, and treatment. Neurobiol. Dis. 2020, 134, 104700. [Google Scholar] [CrossRef] [PubMed]
- Bouça-Machado, R.; Gonçalves, N.; Lousada, I.; Patriarca, M.A.; Costa, P.; Nunes, R.; Dias, S.; Castro Caldas, A.; Valdas, A.; Pita Lobo, P.; et al. Patients and Health Professional’s Perspective of Functional Mobility in Parkinson’s Disease. Front. Neurol. 2020, 11, 575811. [Google Scholar] [CrossRef]
- Keus, S.; Munneke, M.; Graziano, M.; Paltamaa, J.; Pelosin, E.; Domingos, J.; Brühlmann, S.; Ramaswamy, B.; Prins, J.; Struiksma, C.; et al. European Physiotherapy Guideline for Parkinson’s Disease, 1st ed.; KNGF/ParkinsonNet: Nijmegen, The Netherlands, 2014; Available online: http://www.fizioterapeitiem.lv/attachments/article/307/4_eu_guideline_parkinson_201412-development.pdf (accessed on 23 January 2022).
- Erhardsson, M.; Alt Murphy, M.; Sunnerhagen, K.S. Commercial head-mounted display virtual reality for upper extremity rehabilitation in chronic stroke: A single-case design study. J. Neuroeng. Rehabil. 2020, 17, 154. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Santos-García, D.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Current status of immersive virtual reality as a tool for physsical and functional rehabilitation in patients with Parkinson´s disease: Systematic review. Rev. Neurol. 2021, 73, 358–367. [Google Scholar] [CrossRef]
- Bouça-Machado, R.; Rosário, A.; Caldeira, D.; Castro Caldas, A.; Guerreiro, D.; Venturelli, M.; Tinazzi, M.; Schena, F.J.; Ferreira, J. Physical Activity, Exercise, and Physiotherapy in Parkinson’s Disease: Defining the Concepts. Mov. Disord. Clin. Pract. 2019, 7, 7–15. [Google Scholar] [CrossRef]
- Morales-Gómez, S.; Elizagaray-García, I.; Yepes-Rojas, Ó.; De la Puente-Ranea, L.; Gil-Martínez, A. Efectividad de los programas de inmersión virtual en los pacientes con Enfermedad de Parkinson. Revisión sistemática. Rev. Neurol. 2018, 66, 69–80. [Google Scholar] [CrossRef]
- De Keersmaecker, E.; Lefeber, N.; Geys, M.; Jespers, E.; Kerckhofs, E.; Swinnen, E. Virtual reality during gait training: Does it improve gait function in persons with central nervous system movement disorders? A systematic review and meta-analysis. NeuroRehabilitation 2019, 44, 43–66. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Shen, M.; Wang, Y.X.; He, Z.W.; Chi, S.Q.; Yang, Z.H. Effect of virtual reality on balance and gait ability in patients with Parkinson’s disease: A systematic review and meta-analysis. Clin. Rehabil. 2019, 33, 1130–1138. [Google Scholar] [CrossRef] [PubMed]
- Marsh, R.; Hao, X.; Xu, D.; Wang, Z.; Duan, Y.; Liu, J.; Kangarlu, A.; Martinez, D.; Garcia, F.; Tau, G.Z.; et al. A virtual reality-based FMRI study of reward-based spatial learning. Neuropsychologia 2010, 48, 2912–2921. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, D.A.; Pajaro-Blazquez, M.; Daneault, J.F.; Gallegos, J.G.; Pons, J.; Fregni, F.; Bonato, P.; Zafonte, R. Combining Dopaminergic Facilitation with Robot-Assisted Upper Limb Therapy in Stroke Survivors: A Focused Review. Am. J. Phys. Med. Rehabil. 2016, 95, 459–474. [Google Scholar] [CrossRef] [PubMed]
- Benham, S.; Kang, M.; Grampurohit, N. Immersive virtual reality for the management of pain in community-dwelling older adults. OTJR Occup. Particip. Health 2019, 39, 90–96. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Can Immersive Virtual Reality Videogames Help Parkinson’s Disease Patients? A Case Study. Sensors 2021, 21, 4825. [Google Scholar] [CrossRef]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Immersive Virtual Reality Exergame Promotes the Practice of Physical Activity in Older People: An Opportunity during COVID-19. Mutimodal. Technol. Interact. 2021, 5, 52. [Google Scholar] [CrossRef]
- Combs, S.A.; Diehl, M.D.; Chrzastowski, C.; Didrick, N.; McCoin, B.; Mox, N.; Staples, W.H.; Wayman, J. Community-based Group Exercise for Persons with Parkinson Disease: A Randomized Controlled Trial. NeuroRehabilitation 2013, 32, 117–124. [Google Scholar] [CrossRef]
- Combs, S.A.; Diehl, M.D.; Staples, W.H.; Conn, L.; Davis, K.; Lewis, N.; Schaneman, K. Boxing Training for Patients With Parkinson Disease: A Case Series. Phys. Ther. 2011, 91, 132–142. [Google Scholar] [CrossRef] [Green Version]
- Campo-Prieto, P.; Rodríguez-Fuentes, G.; Cancela-Carral, J.M. Translation and cross-cultural adaptation to Spanish of the Simulator Sickness Questionnaire. Retos 2021, 43, 503–509. [Google Scholar] [CrossRef]
- Brooke, J. SUS-A quick and dirty usability scale. In Usability Evaluation in Industry; Jordan, P.W., Thomas, B., Weerdmeester, B.A., McClelland, I.L., Eds.; Taylor & Francis: London, UK, 1996; pp. 189–194. [Google Scholar]
- IJsselsteijn, W.A.; de Kort, Y.A.W.; Poels, K. The Game Experience Questionnaire; Technische Universiteit Eindhoven: Eindhoven, The Netherlands, 2013. [Google Scholar]
- Penko, A.L.; Barkley, J.E.; Koop, M.M.; Alberts, J.L. Borg scale is valid for ratings of perceived exertion for individuals with Parkinson’s disease. Int. J. Exerc. Sci. 2017, 10, 76–86. [Google Scholar] [PubMed]
- Kim, A.; Darakjian, N.; Finley, J.M. Walking in fully immersive virtual environments: An evaluation of potential adverse effects in older adults and individuals with Parkinson’s disease. J. Neuroeng. Rehabil. 2017, 14, 16. [Google Scholar] [CrossRef] [Green Version]
- Bank, P.J.M.; Cidota, M.A.; Ouwehand, P.W.; Lukosch, S.G. Patient-Tailored Augmented Reality Games for Assessing Upper Extremity Motor Impairments in Parkinson’s Disease and Stroke. J. Med. Syst. 2018, 42, 246. [Google Scholar] [CrossRef] [Green Version]
- Chen, W.; Bang, M.; Krivonos, D.; Schimek, H.; Naval, A. An Immersive Virtual Reality Exergame for People with Parkinson’s Disease. In Computers Helping People with Special Needs; Miesenberger, K., Manduchi, R., Covarrubias Rodriguez, M., Peňáz, P., Eds.; Springer International Publishing: Lecco, Italy, 2020; pp. 138–145. [Google Scholar] [CrossRef]
- Cikajlo, I.; Peterlin Potisk, K. Advantages of using 3D virtual reality based training in persons with Parkinson’s disease: A parallel study. J. Neuroeng. Rehabil. 2019, 16, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poewe, W. The natural history of Parkinson’s disease. J. Neurol. 2006, 253, vii2–vii6. [Google Scholar] [CrossRef] [PubMed]
- Stanica, I.-C.; Moldoveanu, F.; Portelli, G.-P.; Dascalu, M.-I.; Moldoveanu, A.; Ristea, M.G. Flexible Virtual Reality System for Neurorehabilitation and Quality of Life Improvement. Sensors 2020, 20, 6045. [Google Scholar] [CrossRef]
- Stanica, I.-C.; Dascalu, M.-I.; Portelli, G.-P.; Moldoveanu, F.; Moldoveanu, A. Parkinson’s Disease—How Virtual Reality Exercises can Improve the Neurorehabilitation Process. In Proceedings of the 2019 E-Health and Bioengineering Conference (EHB), Iasi, Romania, 21–23 November 2019; pp. 1–4. [Google Scholar] [CrossRef]
- Thapa, N.; Park, H.J.; Yang, J.-G.; Son, H.; Jang, M.; Lee, J.; Kang, S.W.; Park, K.W.; Park, H. The Effect of a Virtual Reality-Based Intervention Program on Cognition in Older Adults with Mild Cognitive Impairment: A Randomized Control Trial. J. Clin. Med. 2020, 9, 1283. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Mean | SD | % | ||
|---|---|---|---|---|
| Age (years) | 71.50 | 11.80 | ||
| Gender | Female | 21.9% | ||
| Male | 78.1% | |||
| Height (m) | 1.67 | 0.08 | ||
| Weight (kg) | 75.88 | 13.37 | ||
| BMI (m/kg2) | 27.20 | 5.08 | ||
| H&Y stage | 2 | 1 | ||
| Time since diagnosis (years) | 5.97 | 5.53 | ||
| First symptom | Tremor | 40.6% | ||
| Bradykinesia-rigidity | 43.8% | |||
| Postural instability | 6.3% | |||
| Other | 9.4% | |||
| Motor fluctuation | 46.9% | |||
| Dyskinesias | 9.4% | |||
| Freezing | 37.5% | |||
| Mean | SD | |
|---|---|---|
| SSQ_ST | 0.00 | 0.00 |
| SUS_ST | 75.16/100 | 7.46 |
| GEQ-post game (Positives experiences) | 2.18/4 | 0.66 |
| GEQ-post game (Negative experiences) | 0.01/4 | 0.03 |
| GEQ-post game (Tiredness) | 0.09/4 | 0.30 |
| GEQ-post game (Return to reality) | 0.03/4 | 0.13 |
| Mean | SD | |
|---|---|---|
| Total FIT-XR score (Session 1) | 6973 | 10,887 |
| Borg score (Session 1) | 4 | 2 |
| Total FIT-XR score (Session 2) | 14,797 | 17,999 |
| Borg score (Session 2) | 5 | 2 |
| Stage | I | II | III | ANOVA | |||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | ||
| FIT-XR score (Session 1) | 13,189 $ | 13,733 | 3756 | 5822 | 729 | 1124 | F = 5.266; * p = 0.011 |
| Borg score (Session 1) | 4 | 2 | 3 | 2 | 4 | 2 | F = 0.376; p = 0.690 |
| FIT-XR score (Session 2) | 23,876 $ | 20,550 | 9945 | 13,202 | 2640 | 3271 | F = 4.701; * p = 0.019 |
| Borg score (Session 2) | 5 | 2 | 6 | 3 | 5 | 2 | F = 0.413; p = 0.666 |
| First Symptom Diagnosed | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Tremor | Bradykinesia Rigidity | Postural Instability | Other | ANOVA | |||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| FIT-XR score (Session 1) | 5309 | 8433 | 9707 | 14,060 | 221 # | 156 | 5920 | 2787 | F = 2.939; * p = 0.040 |
| Borg score (Session 1) | 3 | 2 | 5 | 2 | 5 | 1 | 2 | 1 | F = 0.659; p = 0.585 |
| FIT-XR score (Session 2) | 14,130 | 15,898 | 18,546 | 21,861 | 269 # | 117 | 10,459 | 6004 | F = 3.012; * p = 0.043 |
| Borg score (Session 2) | 5 | 2 | 5 | 2 | 6 | 3 | 3 | 1 | F = 1.093; p = 0.371 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Campo-Prieto, P.; Cancela-Carral, J.M.; Rodríguez-Fuentes, G. Wearable Immersive Virtual Reality Device for Promoting Physical Activity in Parkinson’s Disease Patients. Sensors 2022, 22, 3302. https://doi.org/10.3390/s22093302
Campo-Prieto P, Cancela-Carral JM, Rodríguez-Fuentes G. Wearable Immersive Virtual Reality Device for Promoting Physical Activity in Parkinson’s Disease Patients. Sensors. 2022; 22(9):3302. https://doi.org/10.3390/s22093302
Chicago/Turabian StyleCampo-Prieto, Pablo, José Mª Cancela-Carral, and Gustavo Rodríguez-Fuentes. 2022. "Wearable Immersive Virtual Reality Device for Promoting Physical Activity in Parkinson’s Disease Patients" Sensors 22, no. 9: 3302. https://doi.org/10.3390/s22093302