
Three-Dimensional Kinematics during Shoulder Scaption in Asymptomatic and Symptomatic Subjects by Inertial Sensors: A Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
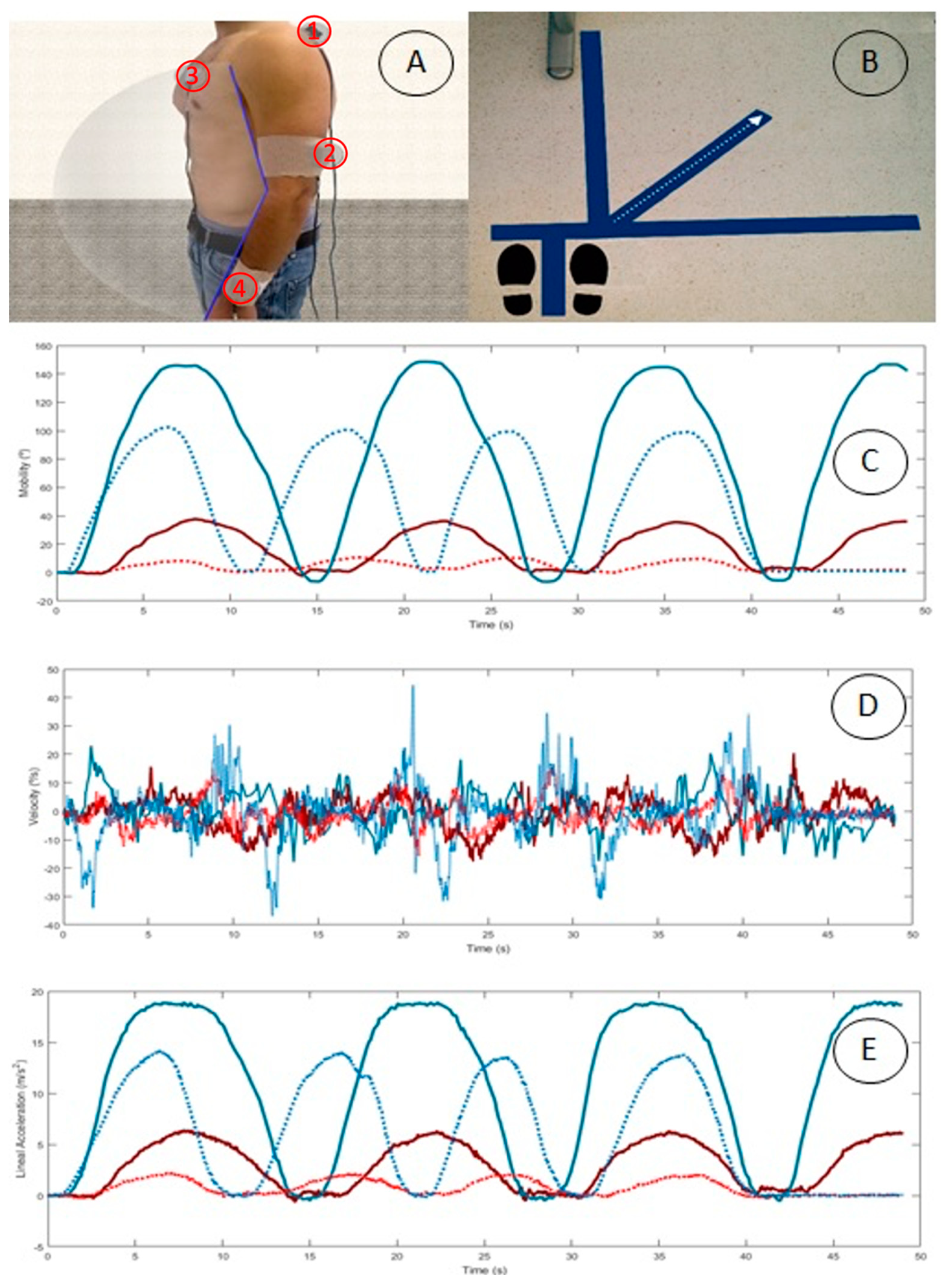
2.2. Equipment and Outcome Measures
- (1)
- the middle third of the humerus, a little posterior with the Z axis pointing against the body;
- (2)
- on the medial third of the scapular upper spine with the x axis in alignment with the cranial edge of the scapular spine;
- (3)
- on the sternum with the Z axis pointing against the body; and
- (4)
- on the distal surface of the ulna and radius with the Z axis pointing away from the wrist.
2.3. Procedure
2.4. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kapandji, A. The Physiology of the Joints—Volume 1: The Upper Limb; Handspring Publishing Limited: Pencaitland, Scotland, 2019; ISBN 978-1-912085-59-0. [Google Scholar]
- Clarkson, H.M.; Hurabielle, J.; Doy, K.; Marlowe, J.D. Proceso Evaluativo Musculoesquelético: Amplitud Del Movimiento Articular Y Test Manual de Fuerza Muscular; Editorial Paidotribo: Badalona, Spain, 2003; ISBN 978-84-8019-671-0. [Google Scholar]
- Greene, D.P.; Roberts, S.L. Kinesiology: Movement in the Context of Activity; Elsevier Health Sciences: Amsterdam, The Netherlands, 2015; ISBN 978-0-323-29889-6. [Google Scholar]
- Codman, E.A. The Shoulder: Rupture of the Supraspinatus Tendon and Other Lesions in or about the Subacromial Bursa; Thomas Todd Copany: Boston, MA, USA, 1934. [Google Scholar]
- Kibler, W.B.; Ludewig, P.M.; McClure, P.W.; Michener, L.A.; Bak, K.; Sciascia, A.D. Clinical Implications of Scapular Dyskinesis in Shoulder Injury: The 2013 Consensus Statement from the “Scapular Summit”. Br. J. Sports Med. 2013, 47, 877–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kibler, W.B.; Sciascia, A.; Wilkes, T. Scapular Dyskinesis and Its Relation to Shoulder Injury. J. Am. Acad. Orthop. Surg. 2012, 20, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Ludewig, P.M.; Reynolds, J.F. The Association of Scapular Kinematics and Glenohumeral Joint Pathologies. J. Orthop. Sports Phys. Ther. 2009, 39, 90–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjelle, A. Epidemiology of Shoulder Problems. Baillieres Clin. Rheumatol. 1989, 3, 437–451. [Google Scholar] [CrossRef]
- Gonçalves, D.H.M.; de Oliveira, A.S.; Freire, L.C.; Silva, A.B.M.; Garbelotti, S.A.; Lucareli, P.R.G. Three-Dimensional Kinematic Analysis of Upper Limb Movements between Individuals with and without Subacromial Shoulder Pain Exploring the Statistical Parametric Mapping. J. Biomech. 2021, 129, 110806. [Google Scholar] [CrossRef]
- Muir, S.W.; Corea, C.L.; Beaupre, L. Evaluating Change in Clinical Status: Reliability and Measures of Agreement for the Assessment of Glenohumeral Range of Motion. N. Am. J. Sports Phys. Ther. NAJSPT 2010, 5, 98–110. [Google Scholar]
- Cuesta-Vargas, A.I.; Galán-Mercant, A.; Williams, J.M. The Use of Inertial Sensors System for Human Motion Analysis. Phys. Ther. Rev. 2010, 15, 462–473. [Google Scholar] [CrossRef] [Green Version]
- Luo, H.; Gao, B. Development of Smart Wearable Sensors for Life Healthcare. Eng. Regen. 2021, 2, 163–170. [Google Scholar] [CrossRef]
- Wong, W.Y.; Wong, M.S.; Lo, K.H. Clinical Applications of Sensors for Human Posture and Movement Analysis: A Review. Prosthet. Orthot. Int. 2007, 31, 62–75. [Google Scholar] [CrossRef]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The Reliability of Three-Dimensional Kinematic Gait Measurements: A Systematic Review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef]
- Kontaxis, A.; Cutti, A.G.; Johnson, G.R.; Veeger, H.E.J. A Framework for the Definition of Standardized Protocols for Measuring Upper-Extremity Kinematics. Clin. Biomech. 2009, 24, 246–253. [Google Scholar] [CrossRef] [PubMed]
- Cutti, A.G.; Giovanardi, A.; Rocchi, L.; Davalli, A.; Sacchetti, R. Ambulatory Measurement of Shoulder and Elbow Kinematics through Inertial and Magnetic Sensors. Med. Biol. Eng. Comput. 2008, 46, 169–178. [Google Scholar] [CrossRef] [PubMed]
- Parel, I.; Cutti, A.G.; Fiumana, G.; Porcellini, G.; Verni, G.; Accardo, A.P. Ambulatory Measurement of the Scapulohumeral Rhythm: Intra- and Inter-Operator Agreement of a Protocol Based on Inertial and Magnetic Sensors. Gait Posture 2012, 35, 636–640. [Google Scholar] [CrossRef] [PubMed]
- Shumway-Cook, A.; Woollacott, M.H. Motor Control: Translating Research into Clinical Practice; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2007; ISBN 978-0-7817-6691-3. [Google Scholar]
- De Baets, L.; van der Straaten, R.; Matheve, T.; Timmermans, A. Shoulder Assessment According to the International Classification of Functioning by Means of Inertial Sensor Technologies: A Systematic Review. Gait Posture 2017, 57, 278–294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jobe, F.W.; Pink, M. Shoulder Injuries in the Athlete: The Instability Continuum and Treatment. J. Hand Ther. 1991, 4, 69–73. [Google Scholar] [CrossRef]
- Youdas, J.W.; Carey, J.R.; Garrett, T.R.; Suman, V.J. Reliability of Goniometric Measurements of Active Arm Elevation in the Scapular Plane Obtained in a Clinical Setting. Arch. Phys. Med. Rehabil. 1994, 75, 1137–1144. [Google Scholar] [CrossRef]
- Day, J.M.; Jones, T.; Eiben, K.; Berger, Y. Scapular Motion Is Accelerated in Asymptomatic Individuals with Dyskinesis: An Observational Study. J. Bodyw. Mov. Ther. 2021, 26, 134–140. [Google Scholar] [CrossRef]
- Roy, J.-S.; Braën, C.; Leblond, J.; Desmeules, F.; Dionne, C.E.; MacDermid, J.C.; Bureau, N.J.; Frémont, P. Diagnostic Accuracy of Ultrasonography, MRI and MR Arthrography in the Characterisation of Rotator Cuff Disorders: A Systematic Review and Meta-Analysis. Br. J. Sports Med. 2015, 49, 1316–1328. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-Y.; Kim, J.; Seo, B.H.; Yu, H.D.; Sim, J.H.; Lee, J.H.; Oh, K.S.; Chung, S.W. Three-Dimensional Analysis of Scapular Kinematics During Arm Elevation in Baseball Players With Scapular Dyskinesis: Comparison of Dominant and Nondominant Arms. J. Sport Rehabil. 2020, 29, 93–101. [Google Scholar] [CrossRef]
- Hervás, M.T.; Navarro Collado, M.J.; Peiró, S.; Rodrigo Pérez, J.L.; López Matéu, P.; Martínez Tello, I. Spanish Version of the DASH Questionnaire. Cross-Cultural Adaptation, Reliability, Validity and Responsiveness. Med. Clínica 2006, 127, 441–447. [Google Scholar]
- Cuesta-Vargas, A.I.; Gabel, P.C. Cross-Cultural Adaptation, Reliability and Validity of the Spanish Version of the Upper Limb Functional Index. Health Qual. Life Outcomes 2013, 11, 126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neer, C.S. Impingement Lesions. Clin. Orthop. 1983, 173, 70–77. [Google Scholar] [CrossRef]
- MacDonald, P.B.; Clark, P.; Sutherland, K. An Analysis of the Diagnostic Accuracy of the Hawkins and Neer Subacromial Impingement Signs. J. Shoulder Elbow Surg. 2000, 9, 299–301. [Google Scholar] [CrossRef] [PubMed]
- Cole, M.H.; van den Hoorn, W.; Kavanagh, J.K.; Morrison, S.; Hodges, P.W.; Smeathers, J.E.; Kerr, G.K. Concurrent Validity of Accelerations Measured Using a Tri-Axial Inertial Measurement Unit While Walking on Firm, Compliant and Uneven Surfaces. PloS ONE 2014, 9, e98395. [Google Scholar] [CrossRef]
- Jasiewicz, J.M.; Treleaven, J.; Condie, P.; Jull, G. Wireless Orientation Sensors: Their Suitability to Measure Head Movement for Neck Pain Assessment. Man. Ther. 2007, 12, 380–385. [Google Scholar] [CrossRef]
- Roldán-Jiménez, C.; Martin-Martin, J.; Cuesta-Vargas, A.I. Reliability of a Smartphone Compared With an Inertial Sensor to Measure Shoulder Mobility: Cross-Sectional Study. JMIR MHealth UHealth 2019, 7, e13640. [Google Scholar] [CrossRef]
- Höglund, G.; Grip, H.; Öhberg, F. The Importance of Inertial Measurement Unit Placement in Assessing Upper Limb Motion. Med. Eng. Phys. 2021, 92, 1–9. [Google Scholar] [CrossRef]
- Hudak, P.L.; Amadio, P.C.; Bombardier, C. Development of an Upper Extremity Outcome Measure: The DASH (Disabilities of the Arm, Shoulder and Hand) [Corrected]. The Upper Extremity Collaborative Group (UECG). Am. J. Ind. Med. 1996, 29, 602–608. [Google Scholar] [CrossRef]
- Gummesson, C.; Atroshi, I.; Ekdahl, C. The Disabilities of the Arm, Shoulder and Hand (DASH) Outcome Questionnaire: Longitudinal Construct Validity and Measuring Self-Rated Health Change after Surgery. BMC Musculoskelet. Disord. 2003, 4, 11. [Google Scholar] [CrossRef] [Green Version]
- Gabel, C.P.; Michener, L.A.; Burkett, B.; Neller, A. The Upper Limb Functional Index: Development and Determination of Reliability, Validity, and Responsiveness. J. Hand Ther. Off. J. Am. Soc. Hand Ther. 2006, 19, 328–348. [Google Scholar] [CrossRef]
- McClure, P.W.; Michener, L.A.; Karduna, A.R. Shoulder Function and 3-Dimensional Scapular Kinematics in People with and without Shoulder Impingement Syndrome. Phys. Ther. 2006, 86, 1075–1090. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Routledge: England, UK, 1988; ISBN 978-0-8058-0283-2. [Google Scholar]
- Keshavarz, R.; Bashardoust Tajali, S.; Mir, S.M.; Ashrafi, H. The Role of Scapular Kinematics in Patients with Different Shoulder Musculoskeletal Disorders: A Systematic Review Approach. J. Bodyw. Mov. Ther. 2017, 21, 386–400. [Google Scholar] [CrossRef] [PubMed]
- Matsuki, K.; Sugaya, H.; Hoshika, S.; Takahashi, N.; Kenmoku, T.; Banks, S.A. Scaption Kinematics of Reverse Shoulder Arthroplasty Do Not Change after the Sixth Postoperative Month. Clin. Biomech. 2018, 58, 1–6. [Google Scholar] [CrossRef] [PubMed]
- López-Pascual, J.; Page, Á.; Serra-Añó, P. Dynamic Thoracohumeral Kinematics Are Dependent upon the Etiology of the Shoulder Injury. PloS ONE 2017, 12, e0183954. [Google Scholar] [CrossRef] [Green Version]
- McKenna, L.; Cornwall, X.; Williams, S. Differences in Scapular Orientation Between Standing and Sitting Postures at Rest and in 120° Scaption: A Cross-Sectional Study. PM R 2017, 9, 579–587. [Google Scholar] [CrossRef] [Green Version]
- Roren, A.; Lefevre-Colau, M.-M.; Poiraudeau, S.; Fayad, F.; Pasqui, V.; Roby-Brami, A. A New Description of Scapulothoracic Motion during Arm Movements in Healthy Subjects. Man. Ther. 2015, 20, 46–55. [Google Scholar] [CrossRef] [Green Version]
- Wassinger, C.A.; Sole, G.; Osborne, H. Clinical Measurement of Scapular Upward Rotation in Response to Acute Subacromial Pain. J. Orthop. Sports Phys. Ther. 2013, 43, 199–203. [Google Scholar] [CrossRef] [Green Version]
- Lawrence, R.L.; Braman, J.P.; Laprade, R.F.; Ludewig, P.M. Comparison of 3-Dimensional Shoulder Complex Kinematics in Individuals with and without Shoulder Pain, Part 1: Sternoclavicular, Acromioclavicular, and Scapulothoracic Joints. J. Orthop. Sports Phys. Ther. 2014, 44, 634–645, A1-8. [Google Scholar] [CrossRef] [Green Version]
- Theodoridis, D.; Ruston, S. The Effect of Shoulder Movements on Thoracic Spine 3D Motion. Clin. Biomech. Bristol Avon 2002, 17, 418–421. [Google Scholar] [CrossRef]
- Lefèvre-Colau, M.-M.; Nguyen, C.; Palazzo, C.; Srour, F.; Paris, G.; Vuillemin, V.; Poiraudeau, S.; Roby-Brami, A.; Roren, A. Kinematic Patterns in Normal and Degenerative Shoulders. Part II: Review of 3-D Scapular Kinematic Patterns in Patients with Shoulder Pain, and Clinical Implications. Ann. Phys. Rehabil. Med. 2018, 61, 46–53. [Google Scholar] [CrossRef]
- Duckworth, D.G.; Smith, K.L.; Campbell, B.; Matsen, F.A. Self-Assessment Questionnaires Document Substantial Variability in the Clinical Expression of Rotator Cuff Tears. J. Shoulder Elbow Surg. 1999, 8, 330–333. [Google Scholar] [CrossRef]
- Via, A.G.; De Cupis, M.; Spoliti, M.; Oliva, F. Clinical and Biological Aspects of Rotator Cuff Tears. Muscles Ligaments Tendons J. 2013, 3, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Matthewson, G.; Beach, C.J.; Nelson, A.A.; Woodmass, J.M.; Ono, Y.; Boorman, R.S.; Lo, I.K.Y.; Thornton, G.M. Partial Thickness Rotator Cuff Tears: Current Concepts. Adv. Orthop. 2015, 2015, 458786. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ludewig, P.M.; Kamonseki, D.H.; Staker, J.L.; Lawrence, R.L.; Camargo, P.R.; Braman, J.P. Changing Our Diagnostic Paradigm: Movement System Diagnostic Classification. Int. J. Sports Phys. Ther. 2017, 12, 884–893. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’hondt, N.E.; Kiers, H.; Pool, J.J.M.; Hacquebord, S.T.; Terwee, C.B.; Veeger, D.H.E.J. Reliability of Performance-Based Clinical Measurements to Assess Shoulder Girdle Kinematics and Positioning: Systematic Review. Phys. Ther. 2017, 97, 124–144. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S.; Valentine, R.E. The Pectoralis Minor Length Test: A Study of the Intra-Rater Reliability and Diagnostic Accuracy in Subjects with and without Shoulder Symptoms. BMC Musculoskelet. Disord. 2007, 8, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hickey, B.W.; Milosavljevic, S.; Bell, M.L.; Milburn, P.D. Accuracy and Reliability of Observational Motion Analysis in Identifying Shoulder Symptoms. Man. Ther. 2007, 12, 263–270. [Google Scholar] [CrossRef]
- Lewis, J. Rotator Cuff Related Shoulder Pain: Assessment, Management and Uncertainties. Man. Ther. 2016, 23, 57–68. [Google Scholar] [CrossRef] [Green Version]
- Antunes, A.; Carnide, F.; Matias, R. Real-Time Kinematic Biofeedback Improves Scapulothoracic Control and Performance during Scapular-Focused Exercises: A Single-Blind Randomized Controlled Laboratory Study. Hum. Mov. Sci. 2016, 48, 44–53. [Google Scholar] [CrossRef]
- López-Pascual, J.; Page, Á.; Serra-Añó, P. Movement Variability Increases With Shoulder Pain When Compensatory Strategies of the Upper Body Are Constrained. J. Mot. Behav. 2018, 50, 510–516. [Google Scholar] [CrossRef] [Green Version]
- Smith, K.L.; Harryman, D.T.; Antoniou, J.; Campbell, B.; Sidles, J.A.; Matsen, F.A. A Prospective, Multipractice Study of Shoulder Function and Health Status in Patients with Documented Rotator Cuff Tears. J. Shoulder Elbow Surg. 2000, 9, 395–402. [Google Scholar] [CrossRef] [PubMed]
- Habechian, F.A.P.; Rosa, D.P.; Haik, M.N.; Camargo, P.R. Sex-Related Differences in Scapular Kinematics During Elevation of the Arm in Asymptomatic Children and Adults. J. Appl. Biomech. 2016, 32, 513–519. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Surface Placement | Humerus | Ulna and Radius | Scapula | Sternum |
|---|---|---|---|---|
| Anatomical Segment Represented Axis | Humerus | Forearm | Scapula | Thorax |
| X | IN-EX | PR-SU | AN-PO | Axial rotation |
| Y | AB-AD | FL-EX | PR-RE | Flexion and extension |
| Z | FL-EX | Carrying angle | ME-LA | Lateral rotation |
| Mobility (°) | Velocity (°/s) | Linear Acceleration (m/s2) | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asymptomatic | Symptomatic | ANOVA (F,p) | Cohens’d (95% C.I) | Asymptomatic | Symptomatic | ANOVA (F,p) | Cohens’d (95% C.I) | Asymptomatic | Symptomatic | ANOVA (F,p) | Cohens’d (95% C.I) | ||
| HUMERUS | AB-AD | 138.98 (13.55) | 88.80 (38.92) | 20.104 (<0.001) | 1.556 (0.864–2.267) | 84.78 (37.59) | 90.22 (155.9) | 0.015 (0.903) | −0.043 (−0.062–0.575) | 17.90 (2.61) | 12.28 (6.20) | 9.676 (0.004) | 1.084 (0.425–1.744) |
| FL-EX | 57.24 (27.08) | 38.62 (38.03) |
2.453 (0.126) | 0.541 (−088–1.17) | 181.76 (49.63) | 106.09 (58.77) | 15.676 (<0.0001) | 1.316 (0.679–2.043) | 10.90 (2.97) | 8.73 (8.78) | 0.741 (0.395) | 0.307 (−0.321–0.922) | |
| IN-EX | 60.29 (50.20) | 41.55 (28.28) | 2.186 (0.148) | 0.496 (−0.131–1.123) | 72.15 (31.66) | 71.58 (63.01) | 0.001, (0.976) | 0.011 (−0.608–0.629) | 5.23 (1.76) | 5.71 (4.83) | 0.120 (0.731) | −0.12 (−0.739–0.499) | |
| SCAPULA | AN-PO | 18.85 (10.17) | 7.81 (8.66) | 11.576 (0.002) | 1.195 (0.527–1.863) | 50.19 (13.89) | 30.83 (26.49) | 5.580 (0.024) | 0.853 (0.209–1.497) | 3.15 (1.12) | 2.48 (3.74) | 0.360 (0.552) | 0.219 (−0.401–0.839) |
| ME-LA | 5.38 (3.69) | 5.47 (4.01) | 0.005 (0.946) | −0.023 (−0.641–0.595) | 44.06 (13.61) | 28.37 (19.22) | 6.351 (0.017) | 0.903 (0.256–1.55) | 4.32 (2.44) | 3.31 (3.27) | 0.893 (0.351) | 0.337 (−0.285–0.96) | |
| PR-RE | 31.89 (8.63) | 10.03 (8) | 56.663 (<0.001) | 2.654 (1.819–3.489) | 48.99 (20.37) | 27.33 (18.20) | 10.468 (0.003) | 1.139 (0.475–1.802) | 5.85 (1.43) | 4.50 (4.91) | 0.867 (0.358) | 0.337 (−0.285–0.96) | |
| Mobility (°) | Velocity (°/s) | Linear Acceleration (m/s2) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asymptomatic | Symptomatic | ANOVA (F,p) | Cohens’d (95% C.I) | Asymptomatic | Symptomatic | ANOVA (F,p) | Cohens’d (95% C.I) | Asymptomatic | Symptomatic | ANOVA (F,p) | Cohens’d (95% C.I) | |
| Carrying angle | 44.22 (47.59) | 47.17 (25.45) | 0.060 (0.809) | 0.084 (−0.702–0.535) | 173.03 (46.62) | 112.41 (74.21) | 6.638 (0.015) | 0.926 (0.277–1.574) | 11.64 (3.21) | 7.70 (2.39) | 17.214 (<0.001) | 1.426 (0.738–2.114) |
| FL-EX | 150.44 (10.95) | 94.26 (36.35) | 27.066 (<0.001) | 1.892 (1.156–2.628) | 116.58 (38.53) | 94.38 (68.50) | 1.079 (0.306) | 0.374 (−0.249–0.998) | 19.23 (3.07) | 12.98 (5.72) | 12.387 (0.001) | 1.271 (0.596–1.945) |
| PR-SU | 73.61 (62.62) | 43.70 (31.11) | 6.638 (0.015) | 0.661 (0.027–1.295) | 102.84 (26.10) | 81.73 (36.70) | 3.149 (0.085) | 0.636 (0.003–1.268) | 6.29 (1.70) | 5.59 (1.73) | 1.307 (0.261) | 0.407 (−0.217–1.032) |
| Mobility (°) | Velocity (°/s) | Linear Acceleration (m/s2) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Asymptomatic | Symptomatic | ANOVA (F,p) | Cohens’d (95% C.I) | Asymptomatic | Symptomatic | ANOVA (F,p) | Cohens’d (95% C.I) | Asymptomatic | Symptomatic | ANOVA (F,p) | Cohens’d (95% C.I) | |
| Lateral rotation | 15.72 (9.38) | 6.25 (8.12) | 10.285 (0.003) | 1.101 (0.44–1.762) | 24.05 (8.46) | 14.58 (9.61) | 8.852 (0.05) | 1.029 (0.373–1.684) | 2.01 (0.75) | 1.32 (0.85) | 5.952 (0.020) | 0.847 (0.203–1.491) |
| Flexion and extension | 4.71 (2.60) | 1.29 (2.14) | 18.438 (<0.001) | 1.475 (0.782–2.167) | 21.44 (5.59) | 15.30 (10.72) | 3.677 (0.63) | 0.669 (0.034–1.303) | 1.38 (0.657) | 0.65 (0.37) | 18.967 (<0.001) | 1.476 (0.783–2.168) |
| Axial rotation | 14.98 (6.34) | 5.87 (7.01) | 15.173 (<0.001) | 1.345 (0.665–2.026) | 19.43 (5.67) | 11.55 (5.33) | 17.604 (<0.001) | 1.444 (0.754–2.134) | 1.09 (0.34) | 0.73 (0.38) | 7.997 (0.008) | 0.984 (0.332–1.636) |
| Humerus Mobility | Scapula Mobility | Humerus Velocity | Scapula Velocity | Humerus Acceleration | Scapula Acceleration | |||||||
| R Value | p Value | R Value | p Value | R Value | p Value | R Value | p Value | R Value | p Value | R Value | p Value | |
| ULFI100 | −0.690 | ˂0.005 | −0.766 | 3.259 | −0.327 | 0.095 | −0.401 | 0.038 | −0.493 | 0.009 | −0.556 | ˂0.005 |
| DASH100 | −0.682 | ˂0.005 | −0.845 | 3.030 | −0.277 | 0.161 | −0.393 | 0.042 | −0.458 | 0.016 | −0.487 | 0.010 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Roldán-Jiménez, C.; Cuesta-Vargas, A.I.; Martín-Martín, J. Three-Dimensional Kinematics during Shoulder Scaption in Asymptomatic and Symptomatic Subjects by Inertial Sensors: A Cross-Sectional Study. Sensors 2022, 22, 3081. https://doi.org/10.3390/s22083081
Roldán-Jiménez C, Cuesta-Vargas AI, Martín-Martín J. Three-Dimensional Kinematics during Shoulder Scaption in Asymptomatic and Symptomatic Subjects by Inertial Sensors: A Cross-Sectional Study. Sensors. 2022; 22(8):3081. https://doi.org/10.3390/s22083081
Chicago/Turabian StyleRoldán-Jiménez, Cristina, Antonio I. Cuesta-Vargas, and Jaime Martín-Martín. 2022. "Three-Dimensional Kinematics during Shoulder Scaption in Asymptomatic and Symptomatic Subjects by Inertial Sensors: A Cross-Sectional Study" Sensors 22, no. 8: 3081. https://doi.org/10.3390/s22083081