1. Introduction
Cardiovascular disease is now the principal threat to human health worldwide [
1] and has become a serious challenge to the medical systems of many countries. In recent years, more young people are facing this threat [
2]. Unfortunately, many cardiovascular diseases do not give rise to obvious symptoms in their early stages, often leading to delayed diagnosis. However, certain physiological variables, such as heart rate and heart rate variability (HRV), exhibit early changes before other symptoms are seen [
3]. Therefore, the monitoring of heart rate and its short-term variability in daily life can be of clinical value in detecting cardiovascular disease at a stage when early treatment is beneficial.
HRV refers to the minor difference between beat-to-beat heart intervals. It may reflect the activity of the sympathetic nervous system (SNS) and parasympathetic nervous system (PNS) in the autonomic nervous system (ANS) [
4]. The regular activity of the healthy heart is maintained by the interaction between the sympathetic and parasympathetic nervous systems, but an imbalance in this interaction can lead to cardiovascular dysfunction. It has been known for at least 50 years that changes in HRV are strongly associated with cardiovascular diseases, such as heart failure, coronary artery disease, acute myocardial infarction and essential hypertension, and more recent studies have confirmed this [
5,
6,
7,
8]. Therefore, HRV analysis has become important in the screening of human cardiovascular function.
The gold standard for assessing HRV is the analysis of the R-R interval of the ECG signal, followed by the calculation of various descriptive parameters. In clinical practice, the 24-h ECG is generally analyzed because it can accurately and comprehensively reflect the patient’s cardiac activity under a range of conditions [
1]. On the other hand, most studies focusing on HRV, rather than the characteristics of the ECG signal itself, have used data collected in the short-term (5-min) [
9,
10,
11,
12,
13].
The Pulse Wave (PW), detected, for instance, by photoplethysmography or tonometry, is often used for the noninvasive assessment of the cardiovascular system but can also be used as an alternative source to the ECG to record and analyze HRV. Strictly speaking, since pulse signals are used, the results should be referred to as pulse rate variability (PRV). Compared with ECG, the equipment used to acquire the PW signal is simpler and more convenient to use, and is, therefore, more suitable for routine monitoring, providing a good alternative to ECG-based HRV analysis [
14,
15].
Ballistocardiography (BCG) is a technique that records the force caused by the ejection of blood by the heart into the arteries [
16]. The force signal can be acquired noninvasively using polyvinylidene fluoride (PVDF) or ElectroMechanical Film (EMFi) sensors. By recording the force and work of the heartbeats, as well as their timing, BCG signals can also be used to evaluate hemodynamic changes in the cardiovascular system. In recent years, a variety of BCG signal acquisition systems for health monitoring have been designed and developed, most of which come in the form of a mattress, chair, or weighing scale [
9,
16,
17]. Unlike ECG, the BCG signal can be acquired by non-contact sensors with less discomfort and inconvenience. Ease of operation is also an important feature of BCG-monitoring equipment. Overall, the recording of BCG signals is relatively simple and unobtrusive, so that the user is essentially unaware of its presence.
BCG signals have been considered an alternative method for HRV analysis in various studies [
2,
10,
11,
12,
13]. Alba et al. [
10] explored the feasibility of HRV analysis using the J-J, I-I, K-K, and H-H intervals of BCG signals. The results showed that the J-J intervals were largely consistent with simultaneously recorded ECG signals. Jan et al. [
11] compared BCG and ECG signals to monitor heart rate. However, only the beat-to-beat intervals were analyzed, without further analysis of any HRV parameters. Brueser et al. [
12] discussed the HRV parameters calculated from BCG signals; they chose a set such as pNN50, SDNN, RMSSD, LF, HF and LF/HF. Jae et al. [
13] assessed virtually all the widely used HRV parameters, including AVNN, SDNN, RMSSD, pNN50, LF, HF, SD1, SD2, etc. However, they only analyzed the correlation between short-term BCG and ECG signals and the number of subjects was small.
In many studies, there is no consensus regarding the validity of using BCG instead of ECG for HRV analysis. Ville et al. reported that all the time-domain and frequency-domain HRV parameters calculated from BCG and ECG agreed well [
18]. However, Christoph et al. found that only for the parameter LF/HF did the BCG and ECG signals show a good correlation [
12], whereas Cao et al. found significant differences between pNN50, LF/HF and SD1 [
17]. A likely explanation for these different findings is that they used different statistical methods to analyze their results. Most studies used the Pearson correlation and the relative error [
10,
11,
12,
13,
19]. However, both are measures of correlation rather than agreement between variables, and they are not, therefore, an appropriate means of assessing agreement. While it is true that the results from tests that agree well will have a high Pearson correlation and low relative error, the converse is not always true [
20,
21].
Studies have shown that the PRV can be often used as an alternative for HRV analysis in healthy subjects [
19]. However, a wearable sensor is required to record the pulse signals [
22], whereas this is not needed to record the BCG signal. We have previously investigated the use of the pulse wave to replace the ECG for HRV analysis and found that the degree of concordance between the two methods varies for different groups of people. In healthy adolescents, the two signals can replace each other for HRV analysis. However, in elderly subjects, and patients with cardiovascular disease, some parameters (pNN50, RMSSD, LF, HF) are not consistent and cannot be substituted for each other [
23].
To comprehensively analyze the potential concordance or disagreement between results based on BCG and Pulse wave (PW) signals, we adopted a wider range of statistical methods, including the coefficient of variation, Bland-Altman analysis, and Lin’s concordance correlation coefficient.
The main contributions of this article are as follows:
- (a)
A comprehensive statistical analysis, as outlined in the preceding paragraph.
- (b)
A comparison of the pros and cons of BCG and PW signals as a substitute for ECG when analyzing HRV in young adults.
The remainder of the paper is organized as follows.
Section 2 presents the design of the experiment, data collection equipment and the data analysis methods.
Section 3 describes and demonstrates the experimental results. In
Section 4, we analyze the consistency of the HRV analysis based on BCG signals and compare the pros and cons of BCG signals and PW signals for HRV calculation. Finally, we summarize our findings and outline our aims for future work.
2. Materials and Methods
A total of 50 healthy young adult volunteers (age 26.2 ± 5.5 years, 22 females and 28 males) were recruited. The exclusion criteria included the use of medication and any medical condition associated with abnormal heart rate signals. This study has been approved by the research ethics committee of Northeastern University. Study number: NEU-EC-20208015S.
The experiment was divided into two parts. In the first, we collected short-term data (5 min) consisting of ECG, BCG, and PW signals from all 50 subjects to assess the feasibility of calculating HRV parameters based on BCG and PW signals. In the second part, we collected data over a longer time interval (100 min) from three subjects only, to explore the stability of BCG signals in calculating medium-term HRV parameters. The aim was to verify whether BCG and PW signals can be used for medium- to longer-term HRV analysis.
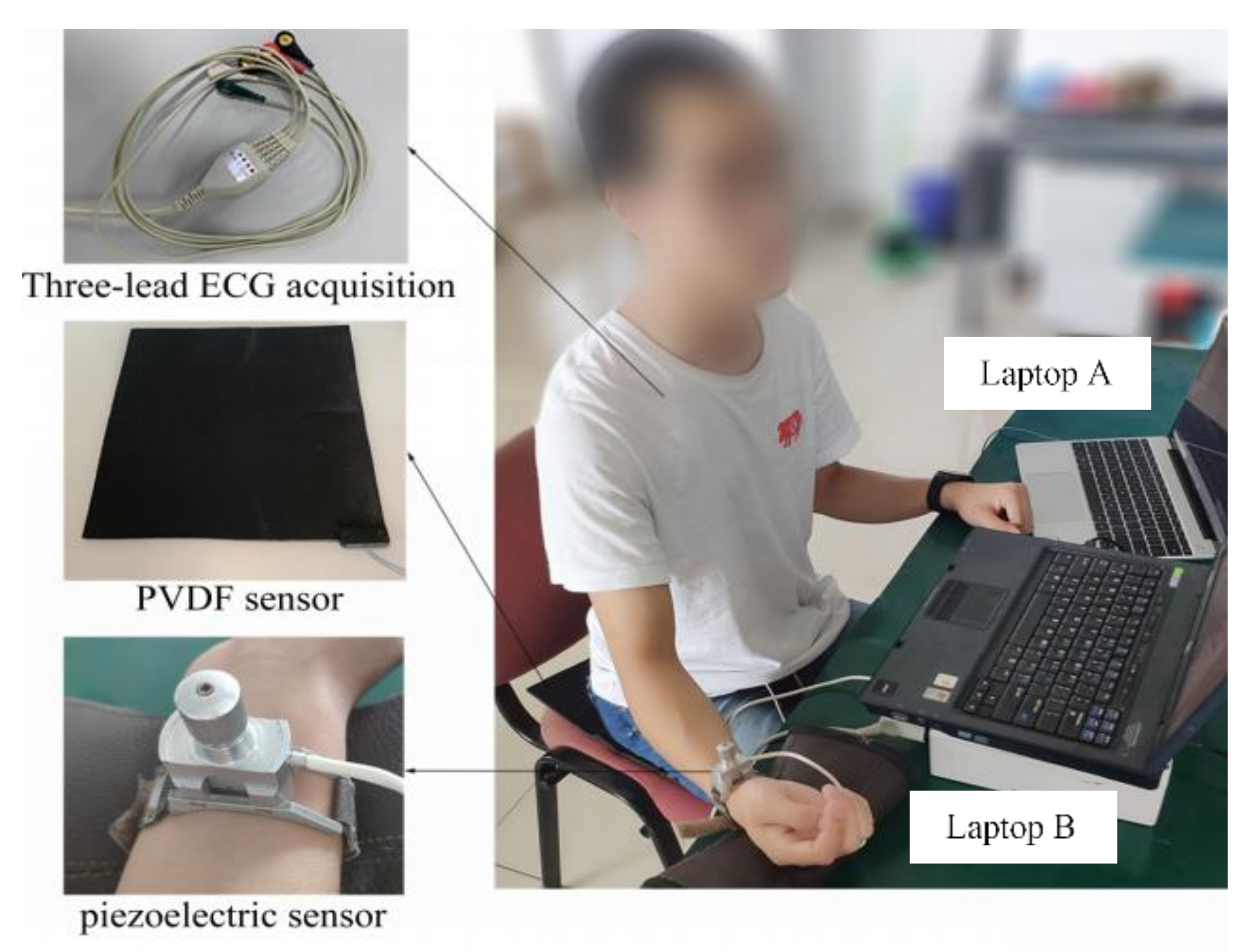
A device was developed by BOBO Technology (Hangzhou, China) to acquire the BCG signal. It consisted of a poly-vinylidene fluoride (PVDF), piezoelectric film sensor (33 cm × 30 cm), integrated into an ESP32 board, combined with a 12-bit SAR ADC and TP1562AL1 rail-to-rail CMOS operational amplifier, set in a smart cushion (type LS-ADA). The device for the synchronous recording of ECG and PW signals was designed in our laboratory; the ECG was detected with Ag/AgCl electrodes on the chest and ankle. A piezoresistive strain gauge sensor (PESG) was used as a tonometer to convert pressure signals into a change in strain-dependent resistance. This was converted, in a bridge circuit, to a varying voltage, which corresponded to the pulse wave signal [
24,
25,
26].
All three signals were recorded at a sampling rate of 1 kHz: the bandwidth of the ECG signal ranged from 0.05 Hz to 100 Hz [
27], that of the PW signals was 0.2 Hz to 40 Hz [
28], and for the BCG signals, it was 4 Hz to 10 Hz [
29]. The two acquisition devices are shown in
Figure 1: laptop A was used to record the BCG signals, and laptop B was used to record the PW and ECG signals simultaneously. The synchronization of recordings from the two computers is described below.
Long-term recordings used to monitor HRV are generally continued for 24 h to account for the effect of circadian rhythm. For practical purposes, we designed a BCG signal acquisition device in the form of a seat, which can be used for daily health monitoring. Sitting for 24 h is obviously unreasonable. Therefore, in order to compare the HRV obtained by the three modalities over a sufficient time period to allow for medium-term variation in cardiovascular control mechanisms, we chose 100 min, and defined this as a “medium-term” data acquisition period.
At the start of the recording session, subjects were asked to relax for 1 min before data collection to reduce the effect of body movement on the BCG signal. In the process of collecting data, the subjects were asked to keep as still as possible. For each subject, the signal was recorded for a total of 100 min, but this period was divided into 20 5-min intervals, each followed by a 2-min rest period. Although this procedure helped to reduce movement artefacts, they were not entirely eliminated, and the signals required further processing (see below for more details).
As mentioned above and shown in
Figure 1, we used two independent signal acquisition devices, so precise synchronization of all the data was not possible in real time. Synchronization was realized off-line before further signal processing by finding the maximum of the cross correlation between the BCG and ECG signals. The PW signals were band-pass filtered (cut-off frequencies 0.5 Hz and 10 Hz), the ECG signals were passed through a 50 Hz notch filter, and the noise in the BCG signal was removed with a 5th-order ‘db4’ wavelet filter using its default threshold. All processing was performed in MATLAB R2018a).
Studies have shown that there are slight differences in the measured beat-to-beat intervals obtained from different types of recording devices. However, the R-R interval, as a measure of heart interval, has become the gold standard in current research [
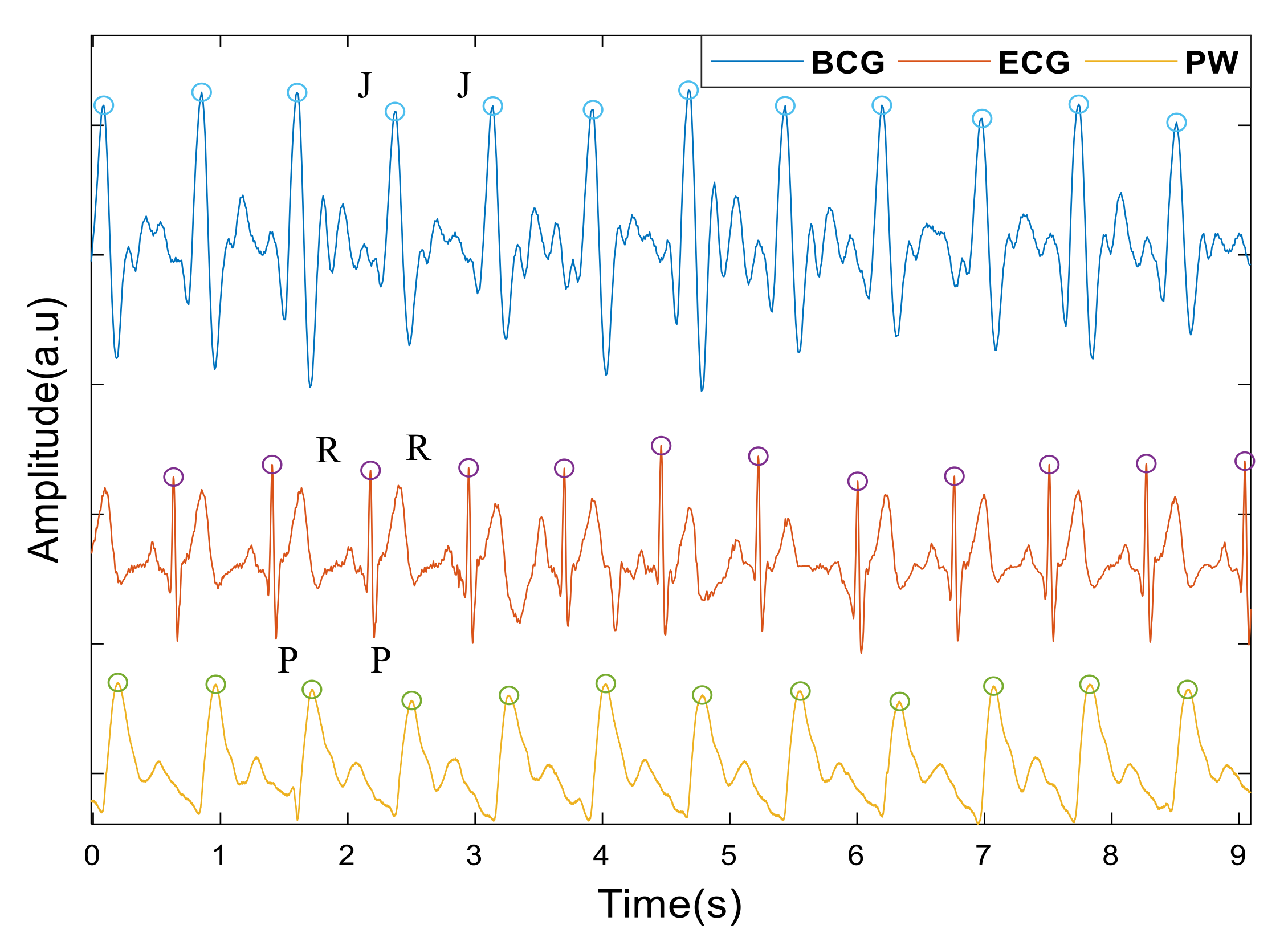
30]. In this study, we chose R-R, P-P, J-J intervals to calculate the heartrate from the ECG, the PW and BCG, respectively. The J wave of the BCG and the first peak of PW signals were taken as the maximum amplitude points in each period. For the ECG, we detected the R wave by first finding the maximum value of the first derivative and then using this as a marker to find the maximum value of the points in the undifferentiated signal immediately following this.
Figure 2 shows the peaks detected from a typical set of signals. Intervals less than 350 ms or greater than 1500 ms, or those differing by more than 20% of the value of the preceding and subsequent interval, were treated as artefacts, defined as spurious and replaced by a linear interpolation of the values derived from the neighboring peaks [
7],
Table 1 lists the number of spurious peaks detected by each signal.
HRV analysis includes time domain methods, frequency domain methods and nonlinear analysis. In this paper, we chose the time domain parameters mean, SDNN, pNN50 and RMSSD; the frequency domain parameters LF, HF and LF/HF; and the non-linear analysis parameters SD1 and SD2, derived from Poincaré plots. However, SD1 and RMSSD are essentially equivalent, as are SD2 and SDNN [
31,
32]. Therefore, only RMSSD and SDNN were analyzed here, in place of SD1 and SD2. On the other hand, the results of nonlinear analysis are affected by many factors, such as the method used to preprocess the data, parameter settings, inconsistent algorithms for calculating the parameters, individual differences between subjects, etc. For example, entropy is a commonly used index in HRV nonlinear analysis and in all entropy measurement methods, the embedding dimension and delay time play a decisive role as initialization parameters. However, there is no standard for the optimal value of initialization parameters, which are mainly determined according to a priori knowledge and data structure. This means that, under different initialization parameters, the results of the entropy measurement will be different [
33]. Furthermore, agreement concerning the clinical significance of HRV nonlinear analysis has yet to be reached [
34,
35,
36,
37]. Therefore, before the clinical importance of nonlinear HRV parameters is widely accepted, it is of little significance to use them to analyze the consistency of the results.
Table 2 lists and defines the parameters used in this study.
To quantify the agreement between the HRV variables extracted from the intervals between successive beats in the BCG, ECG and PW signals, we applied several measures. First, the relative variability between the HRV measurements extracted from the intervals was compared by calculating the differences between the coefficient of variation (CV), calculated from the means and standard deviations (SD) of each pair of HRV features. We defined the quality of the agreement as follows [
22]: the absolute value of CV difference < 2%, excellent agreement; 5% > the absolute value of CV difference ≥ 2%, substantial agreement and the absolute value of CV difference ≥ 5%, poor agreement.
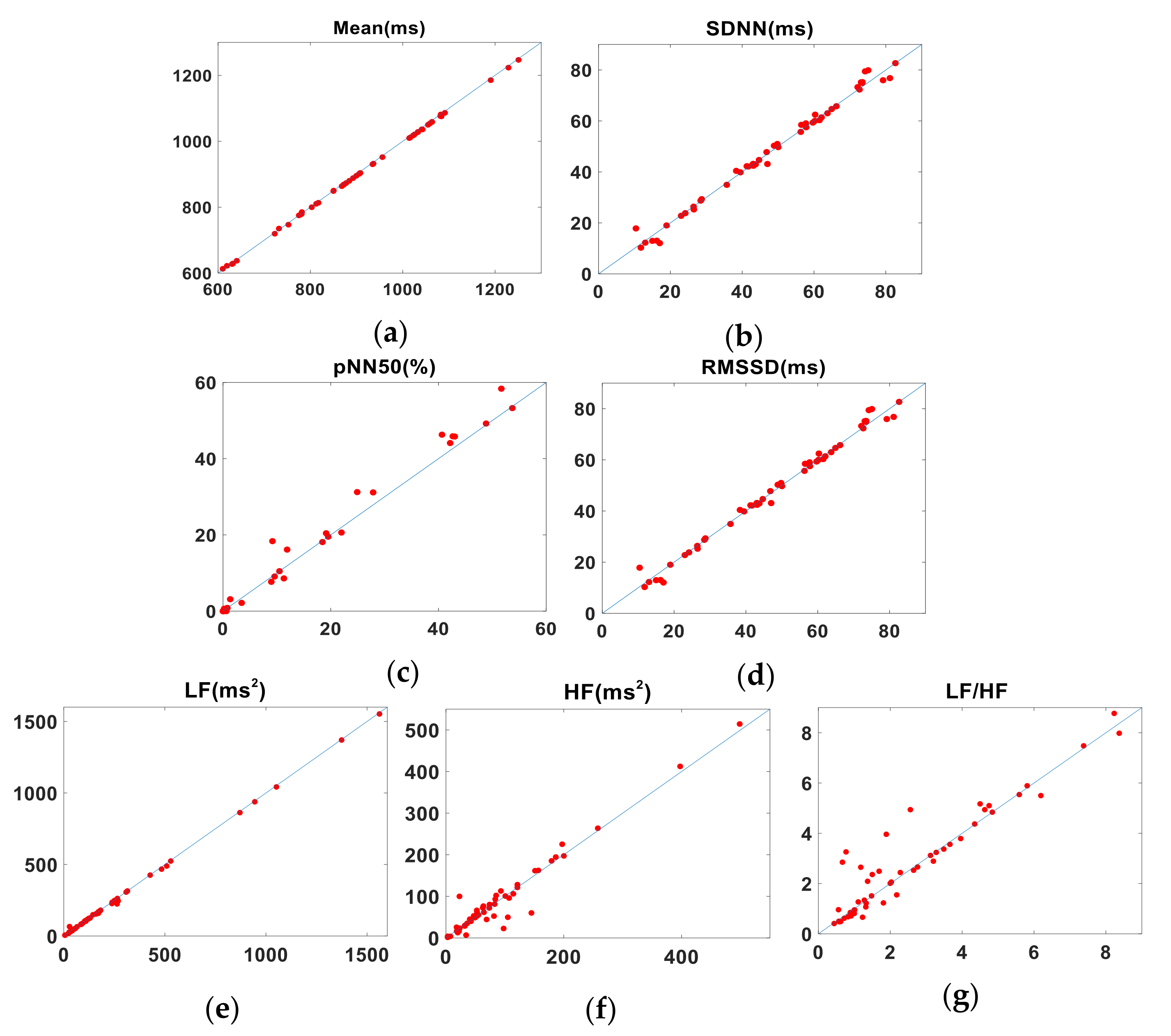
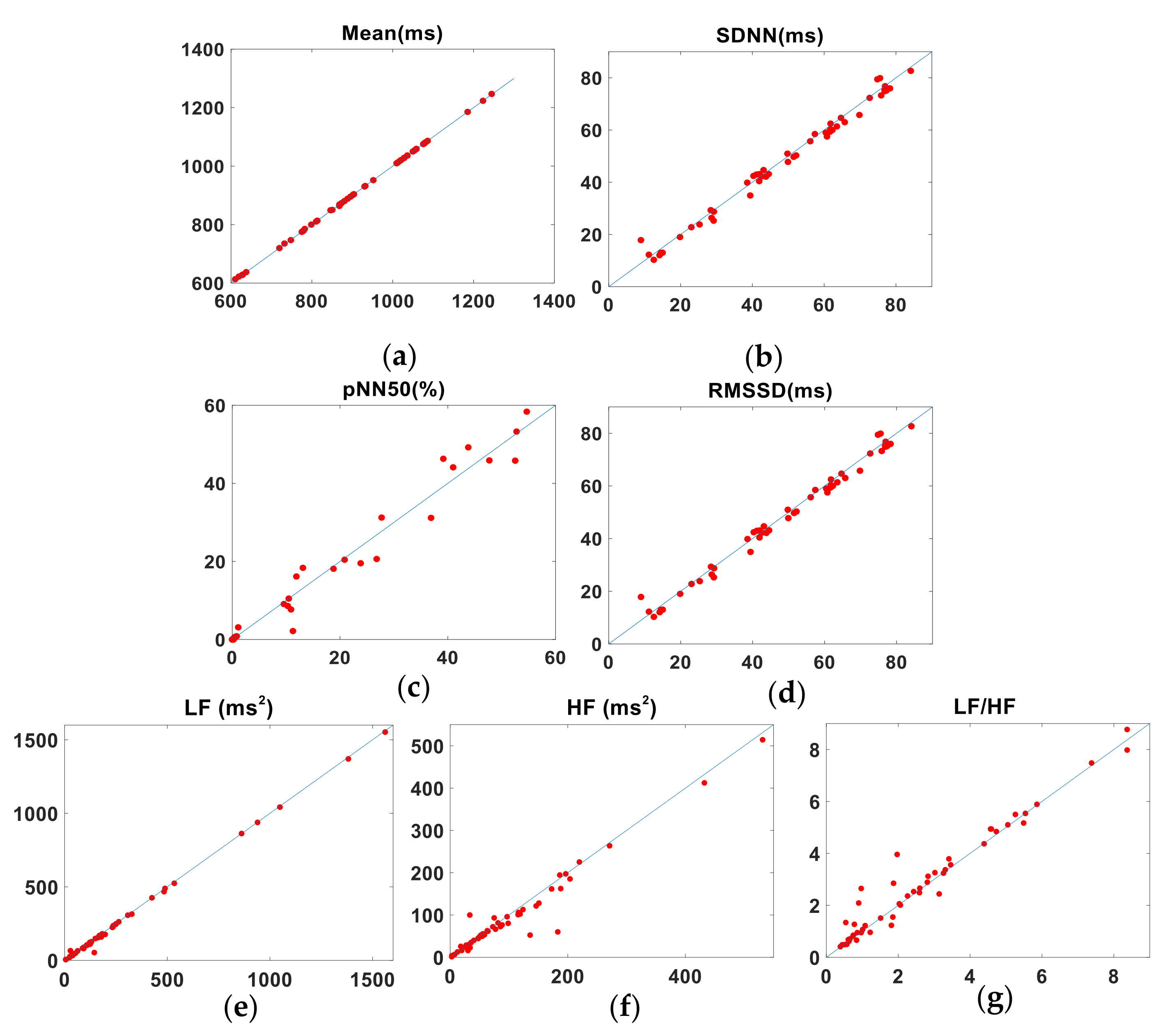
Lin’s Concordance Correlation Coefficient (LCCC) was used to evaluate the agreement between each pair of readings by measuring the perpendicular distance between each pair and the line of identity that would result if the two methods agreed perfectly [
38,
39]. In contrast to the figures given in Reference [
40], we applied a more conservative approach [
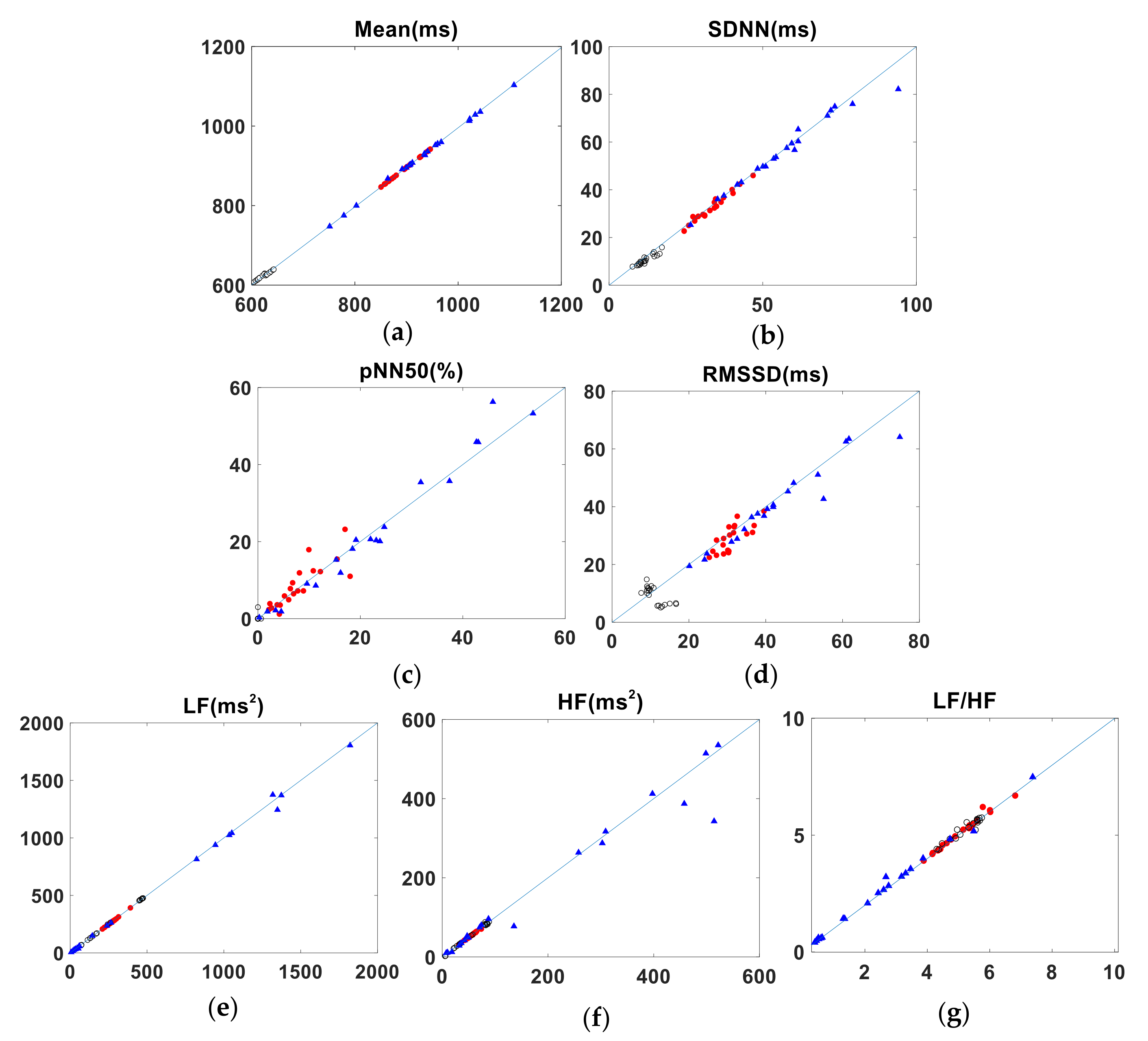
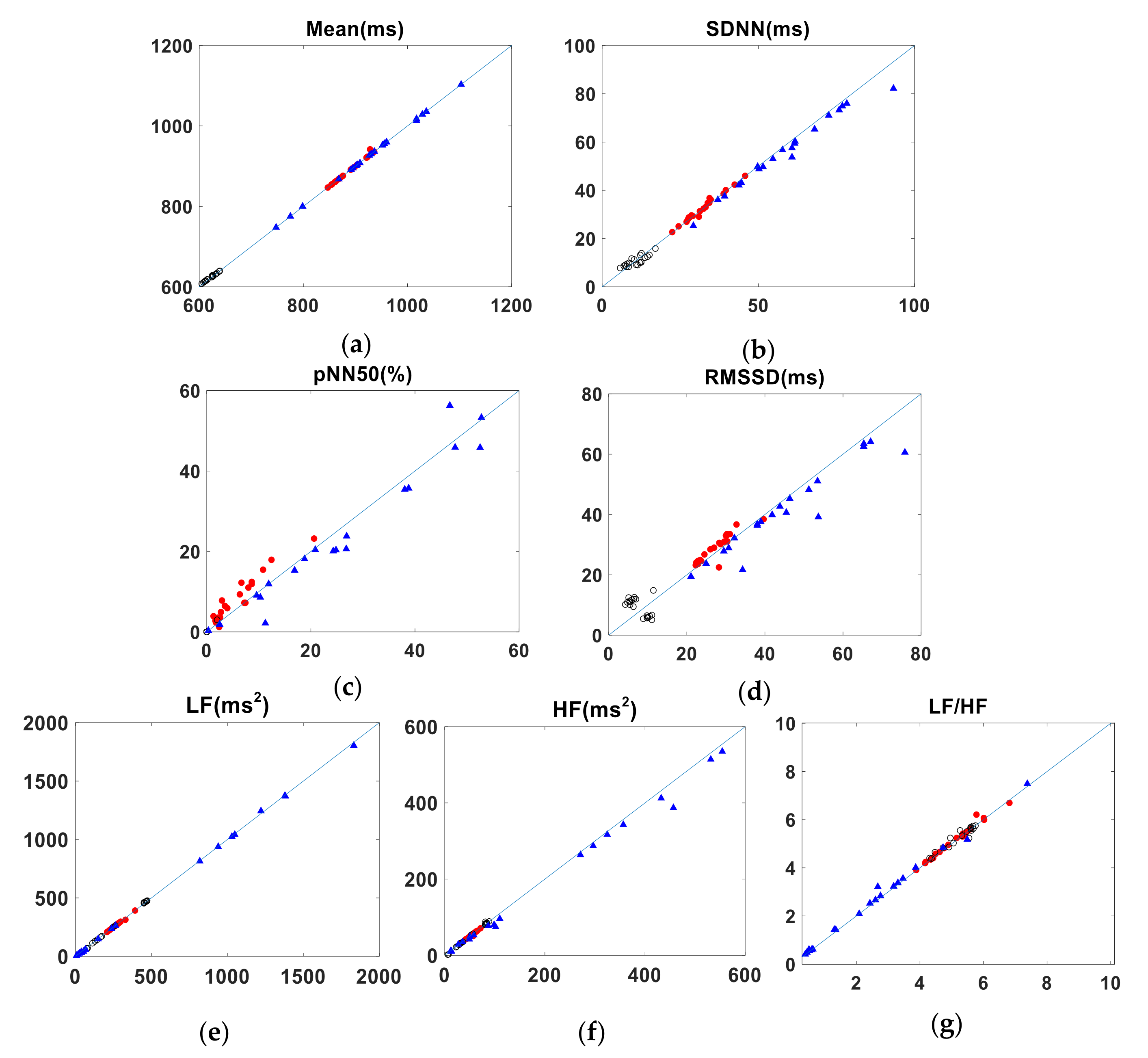
12], and defined the quality of the agreement as follows: excellent agreement if LCCC > 0.99, substantial agreement if 0.99 ≥ LCCC > 0.95; and poor agreement if LCCC ≤ 0.95. As a graphical representation of the concordance between each of the test methods and the gold standard (ECG), we plotted all pairs of heart intervals against the 45° line.
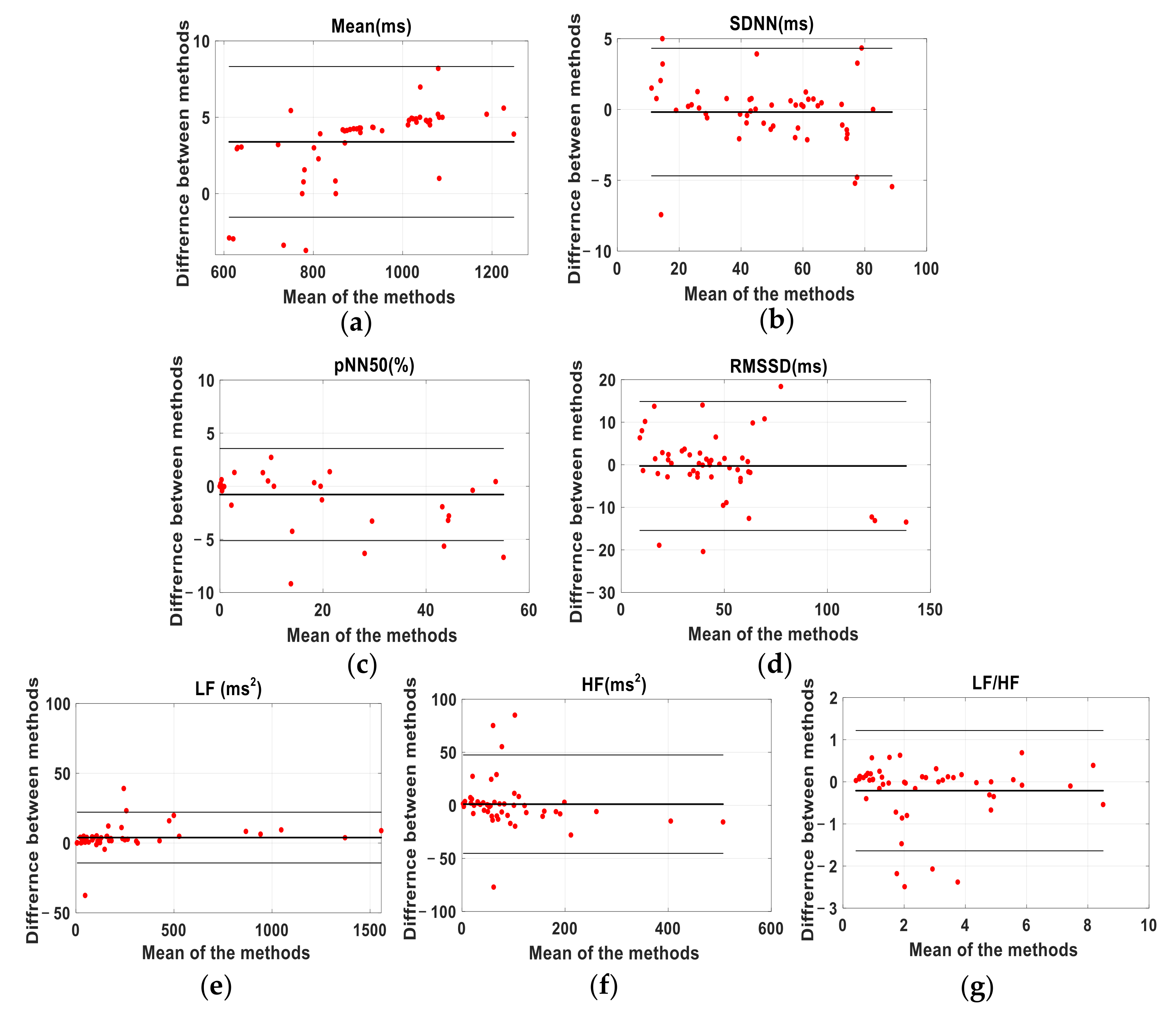
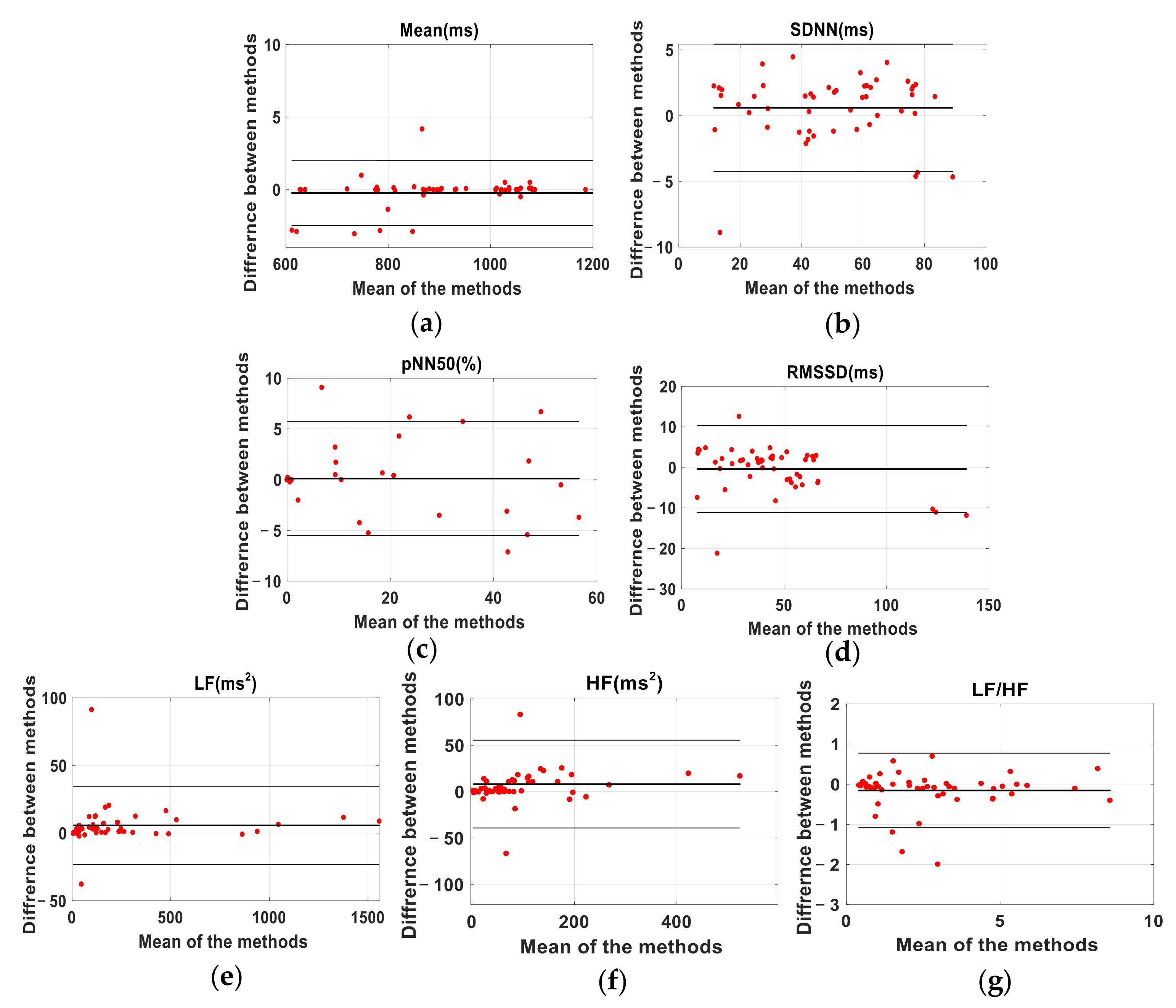
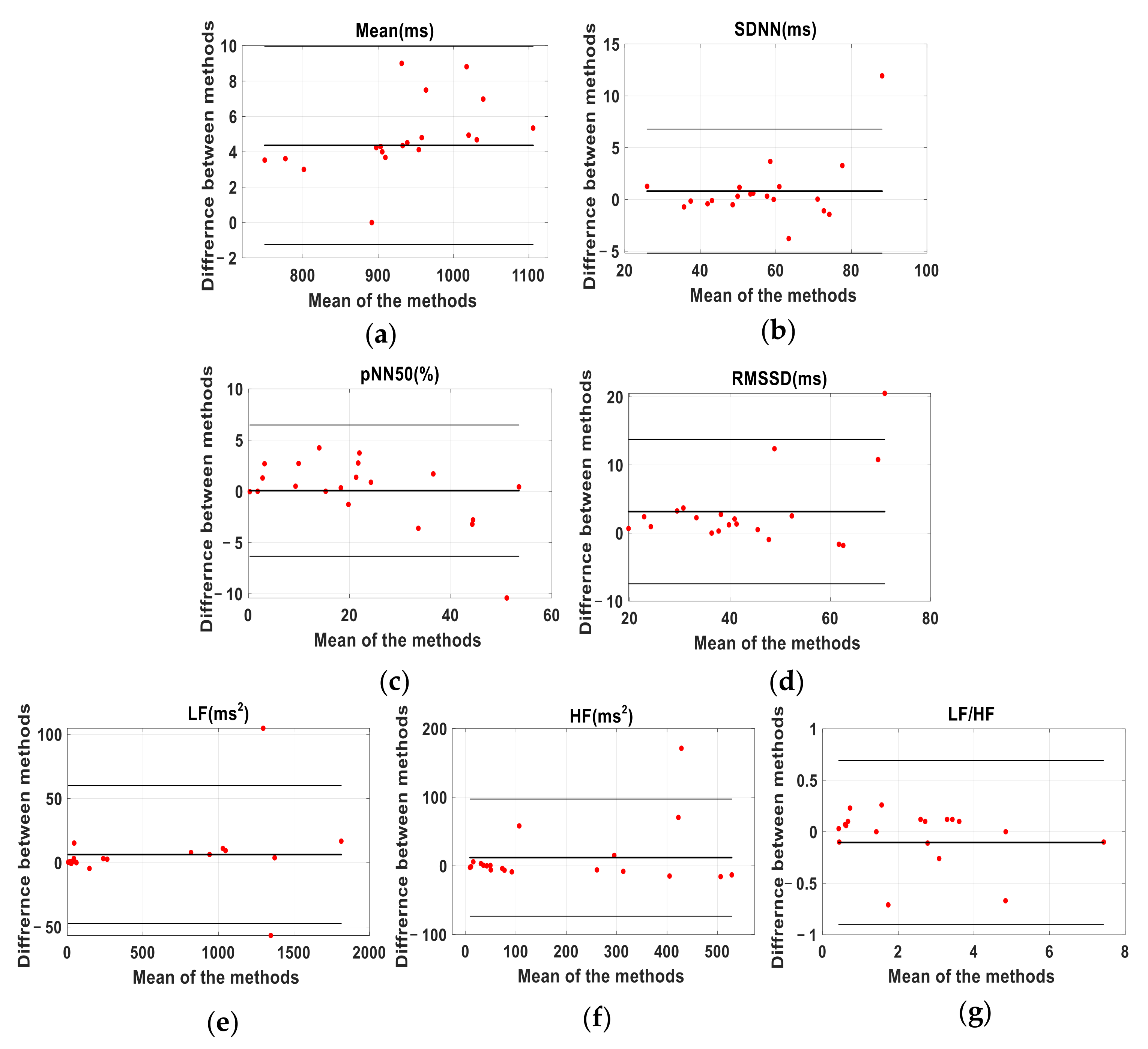
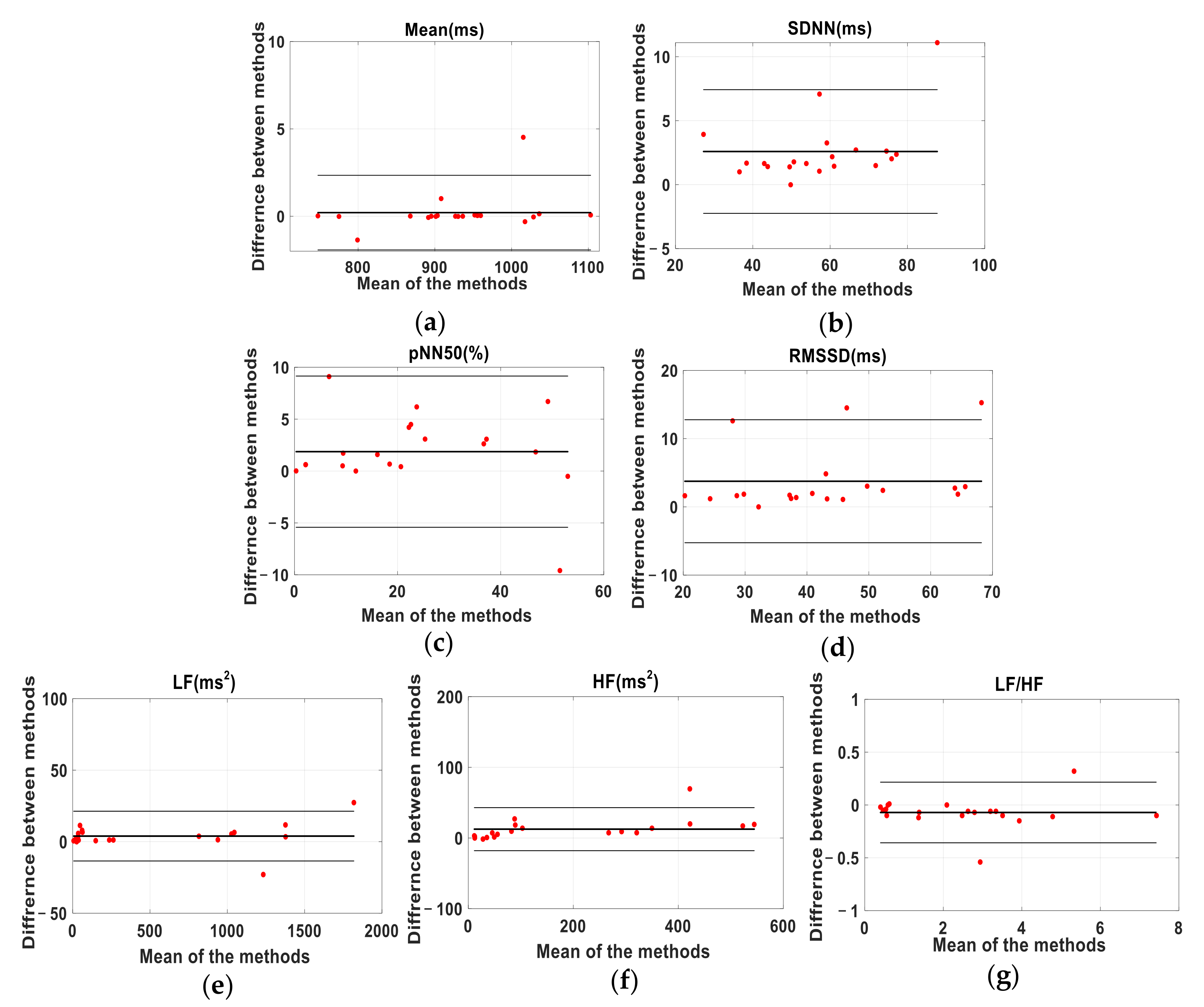
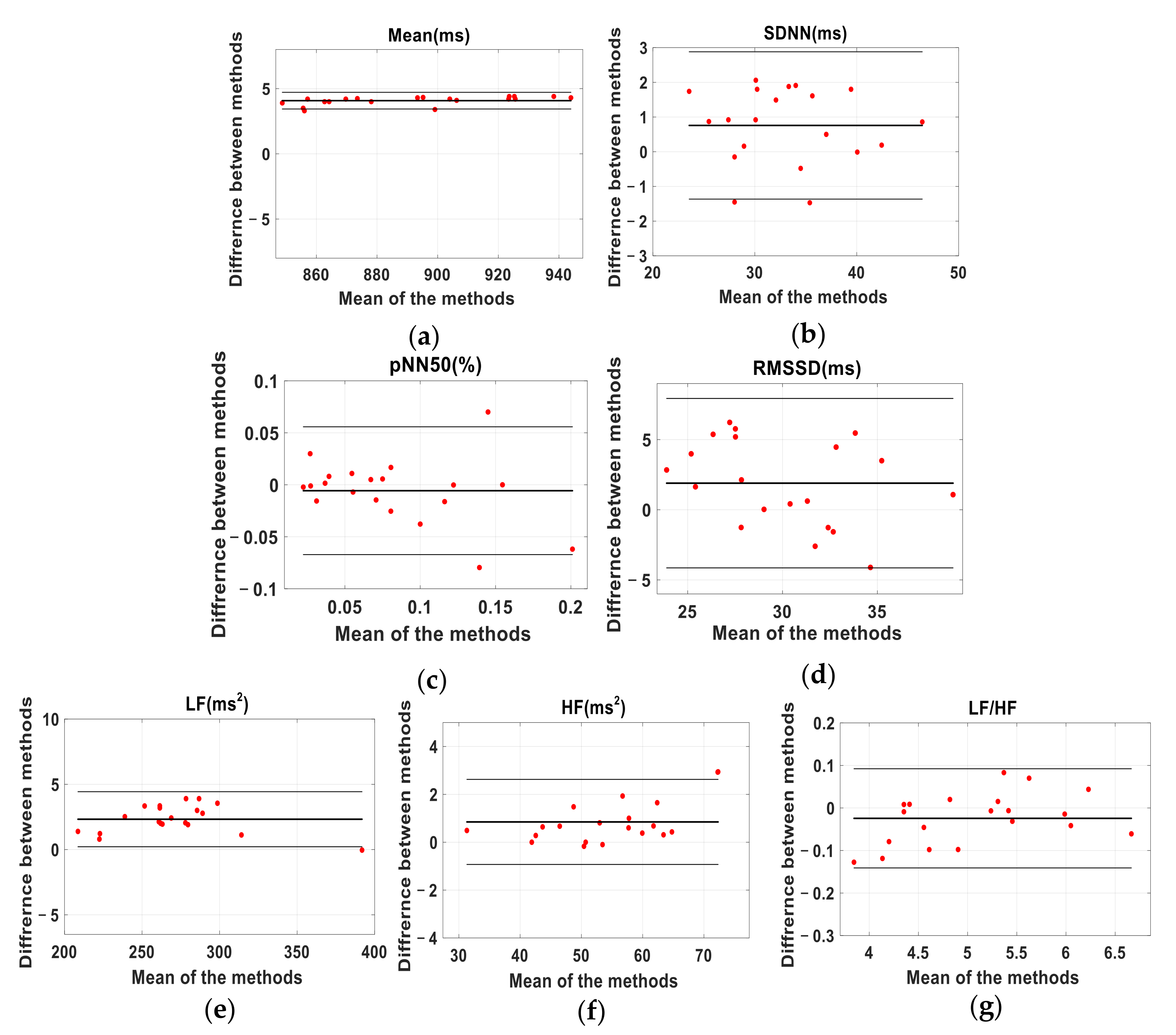
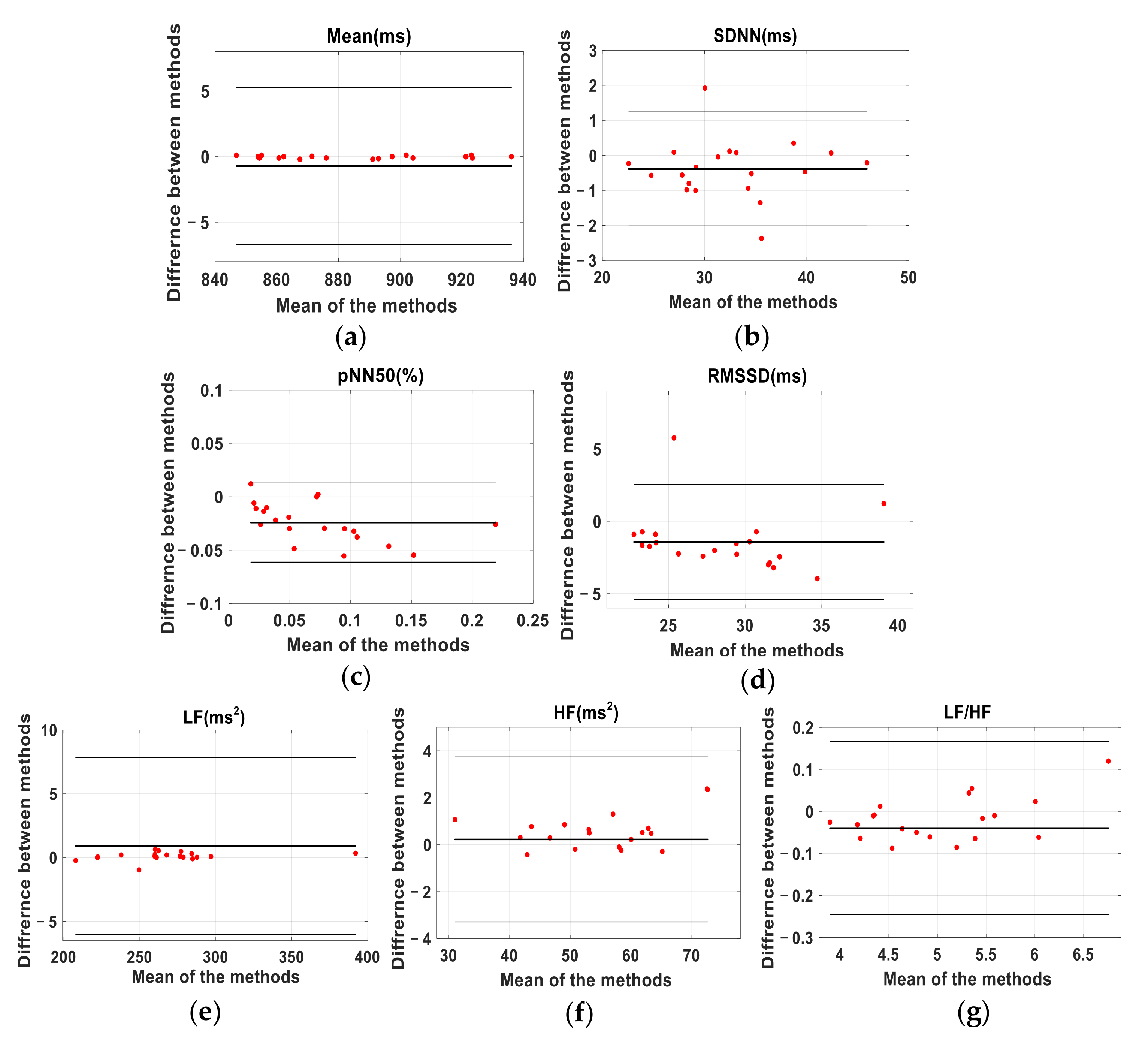
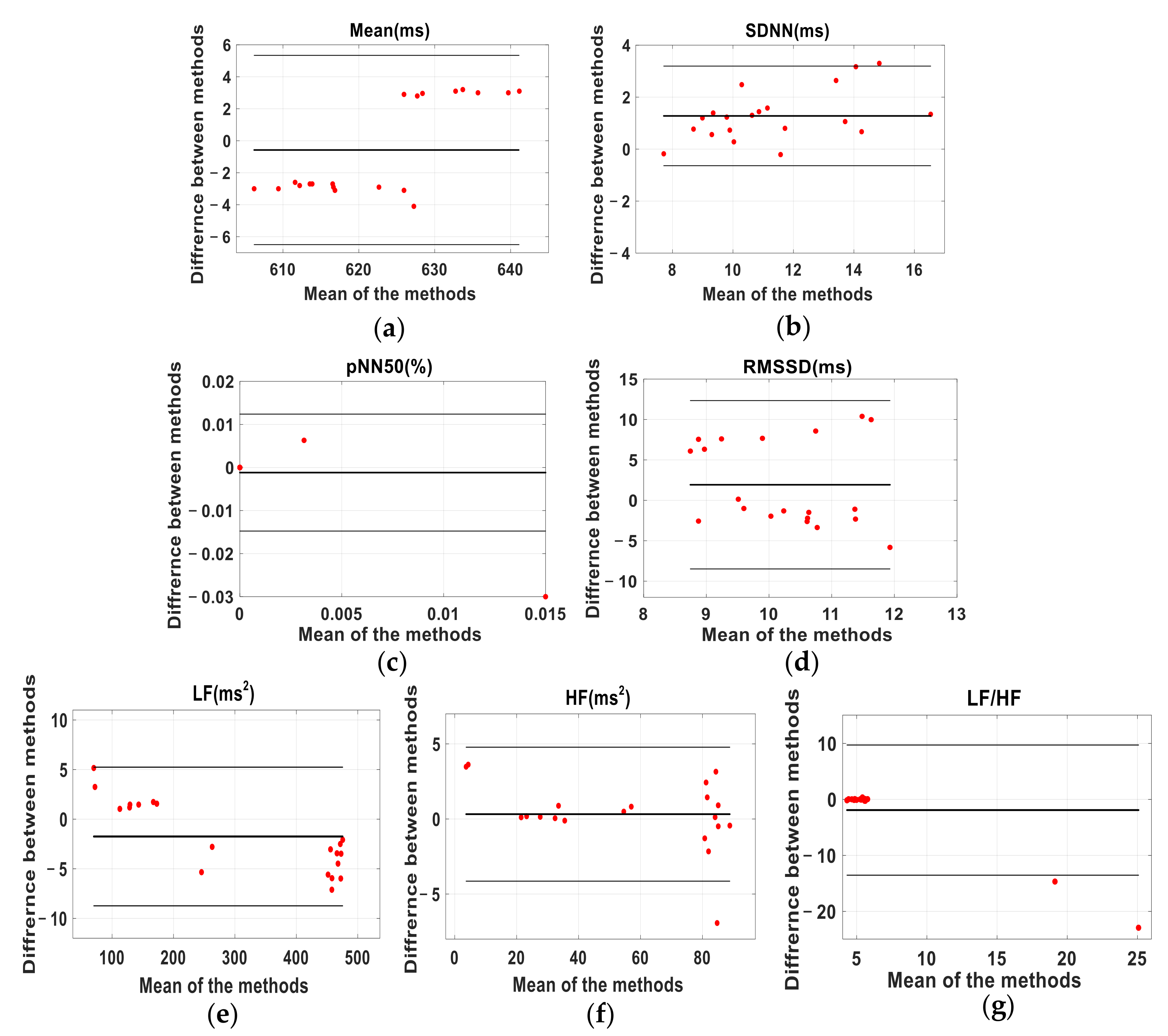
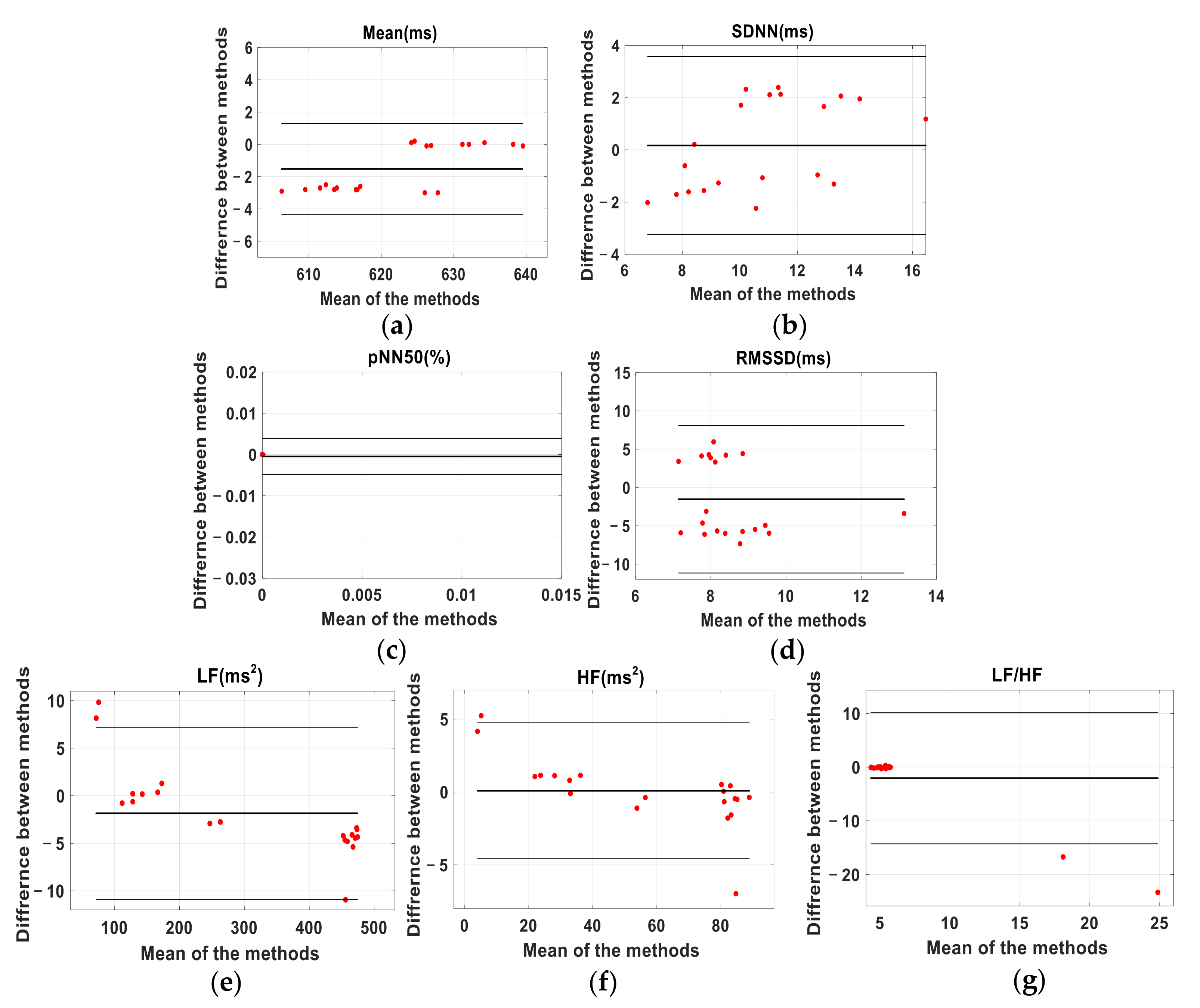
Bland-Altman analysis is often used to evaluate the concordance between two sets of quantitative data obtained by different methods [
41]. In this case, we took the ECG as the gold standard and compared each of the test methods (BCG and PW) separately against the ECG by plotting the mean of each pair of readings against the difference between them. As usual, we defined the limits of agreement (LoA) as the 95% confidence intervals of the overall mean of the differences between each pair of readings. The Bland-Altman ratio (BA ratio) was calculated by dividing half the range of the LoA by the overall mean, as defined above. The standard for evaluating the agreement between two methods based on BA ratio value, as given in References [
42,
43], is: BA ratio < 0.1, excellent agreement; 0.2 > BA ratio ≥ 0.1, moderate agreement and BA ratio ≥ 0.2, poor agreement.
If the quality of agreement given by the above methods differed, we took the worst as the result, and only considered a result to be good if all methods showed a good agreement.
4. Discussion
The need for simple, low-cost and non-invasive methods to monitor the cardiovascular system has encouraged the development of PW systems as an alternative to ECG [
14,
15,
44]. In recent years, this need has also led to the re-emergence of BCG acquisition systems [
45,
46,
47,
48]. However, ECG and PW systems currently require that the sensors are either applied manually to the patient’s skin or, for longer-term use, are held in position with an adhesive patch, a strap or a more elaborate mechanical device such as the one used in this study for PW measurements. In contrast, BCG sensors can be fully integrated into everyday objects such as beds, chairs or weighing scales [
49]. Furthermore, BCG signals can provide additional information about the subject, such as sleeping position, gross movement and tremor [
50].
Although BCG has been investigated as a potential surrogate for ECG in HRV analysis [
10,
11,
12,
13,
18], it is not yet widely accepted and there is currently no agreement about how best to quantify differences between the two techniques. Correlation coefficient, BA analysis or relative error is commonly used for assessment of the association between the heart intervals and the calculation of HRV. However, in some cases, the results may be well correlated, but do not necessarily closely agree. Some studies that have explored the agreement between ECG and BCG signals for calculating HRV parameters have only analyzed the heart intervals [
51]. Thus, a further detailed analysis of derived HRV parameters is still required. This study is an attempt to more comprehensively explore the agreement between the HRV parameters calculated from the J-J and R-R intervals.
Analyzing the short-term data from 50 subjects and the longer-term data from three, we can conclude that the parameters such as mean, SDNN, and LF, used to describe the agreement between HRV measured by BCG and ECG, are closely consistent with each other; pNN50 showed moderate consistency, whereas RMSSD, HF and LF/HF agree poorly. Shin et al. [
13] think that the errors in HF, LF/HF and pNN50, obtained from BCG and ECG signals, are relatively high, a similar finding to ours, except for pNN50. The reason for this slight difference is that both data analysis methods and the values of the boundaries between good, moderate and poor agreement used in the Shin study are not the same as those that we adopted. When comparing the PW and ECG results (i.e., P-P and R-R intervals), the consistency of the mean, SDNN and LF were good, while the consistency of pNN50, RMSSD, HF and LF/HF was poor. The SDNN value reflects the overall activity of the autonomic nervous system. The larger the value, the higher the overall activity and the stronger its regulatory ability. In the results presented here, the values of SDNN derived from the J-J, R-R and P-P intervals are highly consistent, which indicates that BCG and PW may perform as well as ECG in evaluating the risk of heart disease. LF is an indicator of the overall regulatory ability of the sympathetic and parasympathetic nervous system and is often used to analyze the fatigue state.
Overall, the agreement between the J-J and P-P intervals in calculating HRV parameters, was close, with both giving consistent results with the ECG measurements. For pNN50, the consistency of the J-J intervals was good, whereas the consistency of the P-P interval was poor. It is notable that the parameters RMSSD and HF, calculated from the J-J intervals do not agree well with those calculated from R-R intervals, a similar result to other reported findings [
12,
52]. This is caused by the low-frequency components of the BCG signals, which introduce inaccuracies when detecting the blunter peaks of the BCG J waves compared to the more clearly defined peaks in the ECG R-wave [
53].
A limitation to this study is the detection of spurious maxima in the BCG signal.
Table 1 lists the number of false peaks detected by each method. The errors in the BCG signals occur more frequently because it is difficult for subjects to remain still, especially during the long-term acquisition of signals. Body movement will affect the BCG signal, cause the waveform to be distorted, and render the peak detection algorithm ineffective. In general, BCG based measurements are more widely used for sleep monitoring, office health monitoring and other routine heart rate measurements. If the body motion artefacts in the BCG signals can be effectively identified and filtered, the routine monitoring of BCG signals will be more widely used. This is the focus of our future work. For instance, a DnCNN network can be used to construct a BCG signal denoising model, and residual mapping can be added to enable the neural network to learn the characteristics of the noise [
54]. Another limitation of the study is that the participants were all healthy young adults. In future work, we will analyze more subjects over a greater range of ages and, in particular, we will carry out daily monitoring of patients with heart disease.


 ,
, 








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}






