
Acoustic Environmental Conditions (Do Not?) Affect the Static Posturography Diagnostic Accuracy: A Test–Retest Reliability Study

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Sample Size Calculation
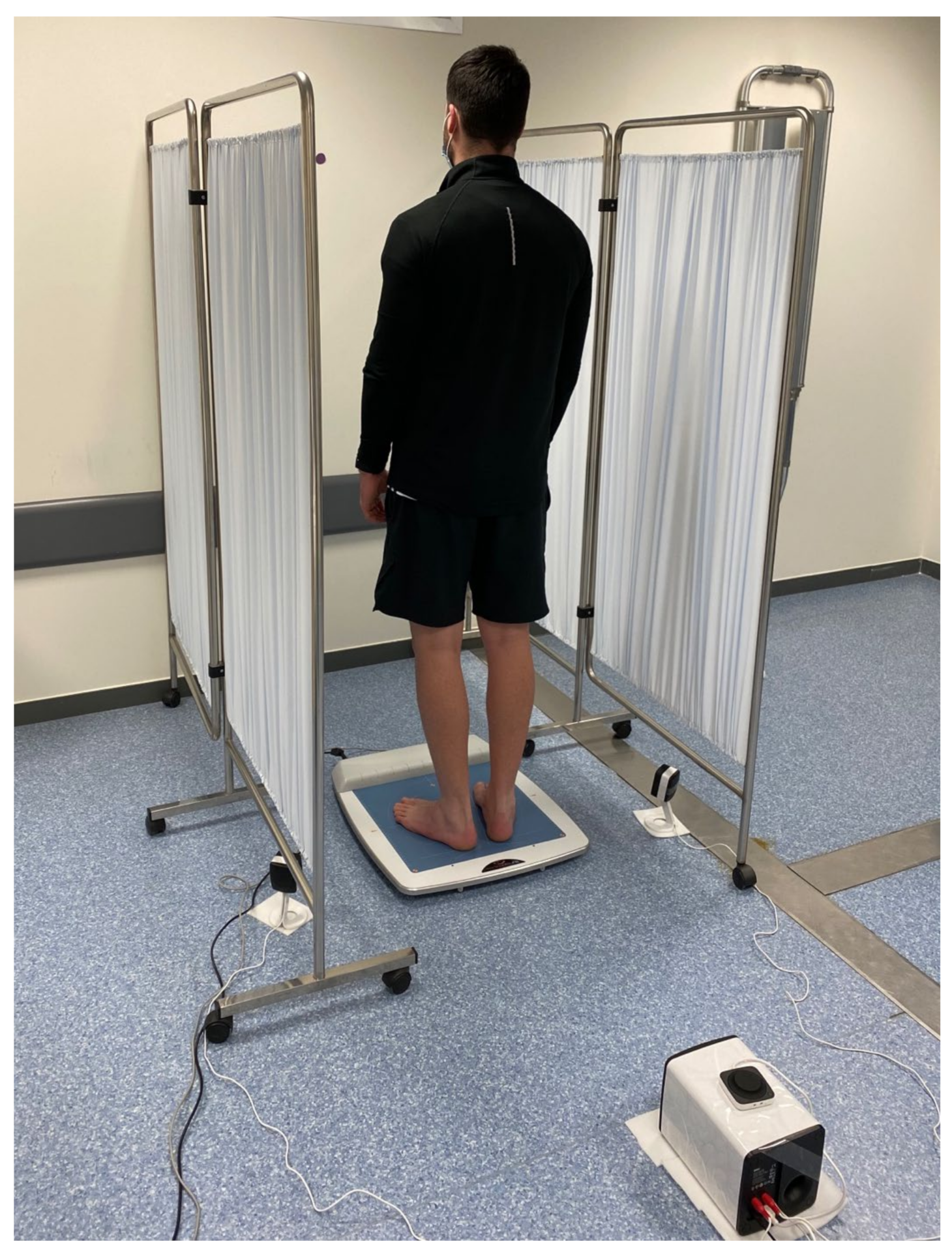
2.4. Procedures
2.5. Variables
2.6. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cuccia, A.; Caradonna, C. The relationship between the stomatognathic system and body posture. Clinics 2009, 64, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Lipworth, W.L.; Hooker, C.; Carter, S.M. Balance, balancing, and health. Qual. Health Res. 2011, 21, 714–725. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pineda, R.C.; Krampe, R.T.; Vanlandewijck, Y.; Van Biesen, D. Reliability of center of pressure excursion as a measure of postural control in bipedal stance of individuals with intellectual disability: A pilot study. PLoS ONE 2020, 15, e0240702. [Google Scholar] [CrossRef]
- Lackner, J.R.; DiZio, P.A. Aspects of body self-calibration. Trends Cogn. Sci. 2000, 4, 279–288. [Google Scholar] [CrossRef]
- Oyarzo, C.A.; Villagrán, C.R.; Silvestre, R.E.; Carpintero, P.; Berral, F.J. Postural control and low back pain in elite athletes comparison of static balance in elite athletes with and without low back pain. J. Back Musculoskelet. Rehabil. 2014, 27, 141–146. [Google Scholar] [CrossRef]
- Howcroft, J.; Lemaire, E.D.; Kofman, J.; McIlroy, W.E. Elderly fall risk prediction using static posturography. PLoS ONE 2017, 12, e0172398. [Google Scholar] [CrossRef]
- Li, L.; Zhang, S.; Dobson, J. The contribution of small and large sensory afferents to postural control in patients with peripheral neuropathy. J. Sport Health Sci. 2019, 8, 218–227. [Google Scholar] [CrossRef]
- Vuong, K.; Canning, C.G.; Menant, J.C.; Loy, C.T. Gait, balance, and falls in Huntington disease. Handb. Clin. Neurol. 2018, 159, 251–260. [Google Scholar] [CrossRef]
- Wang, R.; Wang, H.; Roman, H.E.; Wang, Y.; Xu, D. A cooperative medium access control protocol for mobile clusters in wireless body area networks. In Proceedings of the 2013 First International Symposium on Future Information and Communication Technologies for Ubiquitous HealthCare (Ubi-HealthTech), Jinhua, China, 1–3 July 2013; pp. 1–4. [Google Scholar] [CrossRef]
- Domènech-Vadillo, E.; Aguilera-Aguilera, G.; Sánchez-Blanco, C.; Batuecas-Caletrio, Á.; Guajardo, C.; Pérez, N.; Trinidad-Ruiz, G.; Gimeno, C.; Rama, J.; Rossi-Izquierdo, M.; et al. Normative data for static balance testing in healthy individuals using open source computerized posturography. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 41–48. [Google Scholar] [CrossRef]
- Cohen, H.S. A review on screening tests for vestibular disorders. J. Neurophysiol. 2019, 122, 81–92. [Google Scholar] [CrossRef]
- Huurnink, A.; Fransz, D.P.; Kingma, I.; van Dieën, J.H. Comparison of a laboratory grade force platform with a Nintendo Wii Balance Board on measurement of postural control in single-leg stance balance tasks. J. Biomech. 2013, 46, 1392–1395. [Google Scholar] [CrossRef] [Green Version]
- Asai, M. International standardization in clinical stabilometry and problems in Japan. Equilib. Res. 2016, 75, 135–141. [Google Scholar] [CrossRef] [Green Version]
- Yamamoto, M.; Ishikawa, K.; Aoki, M.; Mizuta, K.; Ito, Y.; Asai, M.; Shojaku, H.; Yamanaka, T.; Fujimoto, C.; Murofushi, T.; et al. Japanese standard for clinical stabilometry assessment: Current status and future directions. Auris Nasus Larynx 2018, 45, 201–206. [Google Scholar] [CrossRef]
- Reutimann, S.; Hill-Strathy, M.; Krewer, C.; Bergmann, J.; Müller, F.; Jahn, K.; Rauen, K. Influence of footwear on postural sway: A systematic review and meta-analysis on barefoot and shod bipedal static posturography in patients and healthy subjects. Gait Posture 2021, 92, 302–314. [Google Scholar] [CrossRef]
- Rodríguez-Rubio, P.; Bagur-Calafat, C.; López-De-Celis, C.; Bueno-Gracía, E.; Cabanas-Valdés, R.; Herrera-Pedroviejo, E.; Girabent-Farrés, M. Validity and Reliability of the Satel 40 Hz Stabilometric Force Platform for Measuring Quiet Stance and Dynamic Standing Balance in Healthy Subjects. Int. J. Environ. Res. Public Health 2020, 17, 7733. [Google Scholar] [CrossRef] [PubMed]
- Ernst, A.; Basta, D.; Mittmann, P.; Seidl, R.O. Can hearing amplification improve presbyvestibulopathy and/or the risk-to-fall? Eur. Arch. Otorhinolaryngol. 2021, 278, 2689–2694. [Google Scholar] [CrossRef]
- Kottner, J.; Audigé, L.; Brorson, S.; Donner, A.; Gajewski, B.J.; Hróbjartsson, A.; Streiner, D.L. Guidelines for Reporting Reliability and Agreement Studies (GRRAS) were pro- posed. Int. J. Nurs. Stud. 2011, 48, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Simera, I.; Moher, D.; Hoey, J.; Schulz, K.F.; Altman, D.G. A catalogue of reporting guidelines for health research. Eur. J. Clin. Investig. 2010, 40, 35–53. [Google Scholar] [CrossRef] [PubMed]
- Walter, S.D.; Eliasziw, M.; Donner, A. Sample size and optimal de- signs for reliability studies. Stat. Med. 1998, 17, 101–110. [Google Scholar] [CrossRef]
- Nagymáté, G.; Orlovits, Z.; Kiss, R.M. Reliability analysis of a sensitive and independent stabilometry parameter set. PLoS ONE 2018, 13, e0195995. [Google Scholar] [CrossRef] [Green Version]
- Nordahl, S.H.; Aasen, T.; Dyrkorn, B.M.; Eidsvik, S.; Molvaer, O.I. Static stabilometry and repeated testing in a normal population. Aviat. Space Environ. Med. 2000, 71, 889–893. [Google Scholar]
- Gagey, P.M.; Weber, B. Study of intra-subject random variations of stabilometric parameters. Med. Biol. Eng. Comput. 2010, 48, 833–835. [Google Scholar] [CrossRef] [PubMed]
- Crossley, E.; Biggs, T.; Brown, P.; Singh, T. The Accuracy of iPhone Applications to Monitor Environmental Noise Levels. Laryngoscope 2021, 131, E59–E62. [Google Scholar] [CrossRef] [PubMed]
- Delgado-Delgado, R.; Valera-Calero, J.A.; Gowie, A.E.; Calvo-Moreno, S.O.; Centenera-Centenera, M.B.; Gallego-Sendarrubias, G.M. Is Any Feature of the Stabilometric Evaluation Clinically Relevant in Patients with Temporomandibular Disorders?A Cross-Sectional Study. Appl. Sci. 2021, 11, 4473. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Howell, D.R.; Hanson, E.; Sugimoto, D.; Stracciolini, A.; Meehan, W.P., 3rd. Assessment of the Postural Stability of Female and Male Athletes. Clin. J. Sport Med. 2017, 27, 444–449. [Google Scholar] [CrossRef]
- Medical Advisory Secretariat. Prevention of falls and fall-related injuries in community-dwelling seniors: An evidence-based analysis. Ont. Health Technol. Assess. Ser. 2008, 8, 1–78. [Google Scholar]
- Olivier, B.; Taljaard, T.; Burger, E.; Brukner, P.D.; Orchard, J.; Gray, J.; Botha, N.; Stewart, A.; McKinon, W. Which Extrinsic and Intrinsic Factors are Associated with Non-Contact Injuries in Adult Cricket Fast Bowlers? Sports Med. 2016, 46, 79–101. [Google Scholar] [CrossRef]
- Granacher, U.; Gollhofer, A. Is there an association between variables of postural control and strength in adolescents? J. Strength Cond. Res. 2011, 25, 1718–1725. [Google Scholar] [CrossRef]
- Paillard, T.; Zéronian, S.; Noé, F. The optimal exploitation of sensory electrical stimulation for regulating postural balance depends on participants’ intrinsic balance abilities. J. Clin. Neurosci. 2021, 93, 88–91. [Google Scholar] [CrossRef]
- Amiri, P.; Kearney, R.E. Ankle intrinsic stiffness changes with postural sway. J. Biomech. 2019, 85, 50–58. [Google Scholar] [CrossRef] [PubMed]
- Solis-Escalante, T.; van der Cruijsen, J.; de Kam, D.; van Kordelaar, J.; Weerdesteyn, V.; Schouten, A.C. Cortical dynamics during preparation and execution of reactive balance responses with distinct postural demands. Neuroimage 2019, 188, 557–571. [Google Scholar] [CrossRef] [PubMed]
- Iqbal, K. Mechanisms and models of postural stability and control. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 7837–7840. [Google Scholar] [CrossRef]
- Noronha, M.; França, L.C.; Haupenthal, A.; Nunes, G.S. Intrinsic predictive factors for ankle sprain in active university students: A prospective study. Scand. J. Med. Sci. Sports 2013, 23, 541–547. [Google Scholar] [CrossRef] [PubMed]
- Carrick, F.R.; Hankir, A.; Zaman, R.; Wright, C.H.G. Metrological Performance of Instruments used in Clinical Evaluation of Balance. Psychiatr. Danub. 2019, 31 (Suppl. 3), 324–330. [Google Scholar] [PubMed]
- Nishiwaki, Y.; Takebayashi, T.; Imai, A.; Yamamoto, M.; Omae, K. Difference by instructional set in stabilometry. J. Vestib. Res. 2000, 10, 157–161. [Google Scholar] [CrossRef]
- Kubryak, O.V.; Markov, N.M.; Krechina, E.K.; Pogabalo, I.V.; Rozhnova, E.V. Achievement of consensus and standardization of methods in dentistry on the example of studies of support reactions (posturography, stabilometry). Stomatologiia 2019, 98, 103–106. [Google Scholar] [CrossRef]
- Scoppa, F.; Capra, R.; Gallamini, M.; Shiffer, R. Clinical stabilometry standardization: Basic definitions—Acquisition interval—Sampling frequency. Gait Posture 2013, 37, 290–292. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Total Sample (n = 27) | Males (n = 12) | Females (n = 15) | Between Group Differences |
|---|---|---|---|---|
| Age (years) | 20.1 ± 2.8 | 21.1 ± 3.8 | 19.3 ± 1.5 | 1.8 (−0.5; 3.9) p = 0.116 |
| Height (m) | 1.70 ± 0.07 | 1.76 ± 0.05 | 1.65 ± 0.04 | 0.11 (0.08; 0.15) p < 0.001 |
| Weight (kg) | 70.2 ± 11.8 | 75.6 ± 9.2 | 65.9 ± 12.1 | 9.7 (1.0; 18.4) p = 0.030 |
| Body Mass Index (kg/m2) | 24.2 ± 3.5 | 24.3 ± 3.2 | 24.1 ± 3.8 | 0.1 (−2.6; 3.0) p = 0.923 |
| Foot size (European shoe size) | 40.6 ± 2.3 | 42.6 ± 1.6 | 39.1 ± 1.3 | 0.1 (−2.7; 3.0) p < 0.001 |
| Variables | Mean ± SD | Absolute Error | ICC2,1 (95% CI) | SEM | MDC95 |
|---|---|---|---|---|---|
| 35–40 dB | |||||
| Oscillation Surface (mm2) | 195.6 ± 117.2 | 53.4 ± 49.4 | 0.903 (0.787; 0.956) | 34.9 | 96.7 |
| Total Oscillation Length (mm) | 373.6 ± 79.6 | 53.2 ± 39.8 | 0.837 (0.642; 0.926) | 28.1 | 77.8 |
| ML-Length absolute deviation (mm) | 5.0 ± 2.4 | 2.9 ± 2.0 | 0.453 (−0.200; 0.751) | 1.4 | 3.8 |
| AP-Length absolute deviation (mm) | 42.5 ± 13.8 | 4.4 ± 3.0 | 0.962 (0.917; 0.983) | 2.1 | 5.8 |
| LFS | 0.65 ± 0.12 | 0.07 ± 0.07 | 0.840 (0.649; 0.927) | 0.04 | 0.11 |
| SVFAP | 52.8 ± 35.7 | 7.9 ± 5.4 | 0.829 (0.625; 0.922) | 3.8 | 10.5 |
| ASV (mm/s) | 50.4 ± 14.7 | 8.6 ± 5.8 | 0.871 (0.717; 0.941) | 4.1 | 11.3 |
| Mean Speed (mm/s) | 12.4 ± 2.7 | 1.8 ± 1.3 | 0.839 (0.647; 0.927) | 0.9 | 2.5 |
| 85–90 dB | |||||
| Oscillation Surface (mm2) | 209.0 ± 124.5 | 77.6 ± 77.2 | 0.804 (0.570; 0.911) | 54.5 | 151.0 |
| Total Oscillation Length (mm) | 378.8 ± 81.8 | 53.8 ± 40.0 | 0.859 (0.690; 0.936) | 28.2 | 78.1 |
| ML-Length absolute deviation (mm) | 4.0 ± 3.0 | 2.9 ± 2.2 | 0.621 (0.168; 0.827) | 1.5 | 4.1 |
| AP-Length absolute deviation (mm) | 44.5 ± 13.3 | 4.4 ± 3.7 | 0.952 (0.895; 0.978) | 2.6 | 7.2 |
| LFS | 0.65 ± 0.12 | 0.07 ± 0.08 | 0.831 (0.628; 0.923) | 0.05 | 0.13 |
| SVFAP | 37.4 ± 12.1 | 6.8 ± 5.5 | 0.873 (0.721; 0.942) | 3.88 | 10.7 |
| ASV (mm/s) | 52.6 ± 14.9 | 7.5 ± 5.7 | 0.902 (0.784; 0.955) | 4.0 | 11.1 |
| Mean Speed (mm/s) | 14.1 ± 7.6 | 1.8 ± 1.3 | 0.858 (0.689; 0.935) | 0.9 | 2.5 |
| Variables | Differences between Mean Scores from 2 and 3 Measurements | |
|---|---|---|
| 40 dB | 90 dB | |
| Oscillation Surface (mm2) | 0.5 (−60.5; 61.5) p = 0.986 | 4.7 (−59.0; 68.5) p = 0.881 |
| Total Oscillation Length (mm) | 4.9 (−36.7; 46.5) p = 0.815 | 4.6 (−38.9; 48.2) p = 0.833 |
| ML-Length absolute deviation (mm) | 0.1 (−1.1; 1.4) p = 0.805 | 0.2 (1.3; 1.7) p = 0.784 |
| AP-Length absolute deviation (mm) | 0.2 (−7.1; 7.6) p = 0.941 | 0.4 (−6.8; 7.7) p = 0.902 |
| LFS | 0.00 (−0.05; 0.07) p = 0.767 | 0.00 (−0.06; 0.07) p = 0.831 |
| SVFAP | 0.6 (−6.3; 7.4) p = 0.866 | 0.1 (−6.5; 6.8) p = 0.966 |
| ASV (mm/s) | 0.4 (−7.5; 8.3) p = 0.921 | 0.2 (−8.0; 8.5) p = 0.950 |
| Mean Speed (mm/s) | 0.2 (−0.7; 1.2) p = 0.817 | 0.2 (−1.3; 1.6) p = 0.833 |
| Variables | Differences between both Acoustic Conditions |
|---|---|
| Oscillation Surface (mm2) | 8.1 (−50.3; 66.7) p = 0.780 |
| Total Oscillation Length (mm) | 5.5 (35.6; 46.6) p = 0.790 |
| ML-Length absolute deviation (mm) | 0.6 (−0.8; 1.9) p = 0.378 |
| AP-Length absolute deviation (mm) | 2.2 (−5.0; 9.5) p = 0.545 |
| LFS | 0.00 (−0.05; 0.06) p = 0.876 |
| SVFAP | 1.5 (−5.0; 8.1) p = 0.634 |
| ASV (mm/s) | 2.1 (−6.0; 10.1) p = 0.610 |
| Mean Speed (mm/s) | 0.2 (−1.2; 1.5) p = 0.797 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calvo-Moreno, S.O.; Rodríguez-López, E.S.; Varol, U.; Benito-de-Pedro, M.; Anós-Merino, E.; Conde-Vázquez, O.; Fernández-de-las-Peñas, C.; Valera-Calero, J.A. Acoustic Environmental Conditions (Do Not?) Affect the Static Posturography Diagnostic Accuracy: A Test–Retest Reliability Study. Sensors 2022, 22, 2365. https://doi.org/10.3390/s22062365
Calvo-Moreno SO, Rodríguez-López ES, Varol U, Benito-de-Pedro M, Anós-Merino E, Conde-Vázquez O, Fernández-de-las-Peñas C, Valera-Calero JA. Acoustic Environmental Conditions (Do Not?) Affect the Static Posturography Diagnostic Accuracy: A Test–Retest Reliability Study. Sensors. 2022; 22(6):2365. https://doi.org/10.3390/s22062365
Chicago/Turabian StyleCalvo-Moreno, Sofía Olivia, Elena Sonsoles Rodríguez-López, Umut Varol, María Benito-de-Pedro, Elena Anós-Merino, Orlando Conde-Vázquez, César Fernández-de-las-Peñas, and Juan Antonio Valera-Calero. 2022. "Acoustic Environmental Conditions (Do Not?) Affect the Static Posturography Diagnostic Accuracy: A Test–Retest Reliability Study" Sensors 22, no. 6: 2365. https://doi.org/10.3390/s22062365