
Assessing Cerebellar Disorders with Wearable Inertial Sensor Data Using Time-Frequency and Autoregressive Hidden Markov Model Approaches


Abstract
:1. Introduction
- We demonstrate that an autoregressive hidden Markov model (AR-HMM) that allows for nonparametric extension can be used to characterize and parse movement within clinical motor assessments recorded by IMUs. To our knowledge, this paper represents the first application of such models to human motion measured by IMUs.
- We present two approaches to developing meaningful and descriptive quantifications of movement tasks recorded by IMUs, with one set learned from data based on an autoregressive hidden Markov model and another based on a time-frequency approach.
- We apply these approaches to clinical data, demonstrating excellent classification accuracy and good severity score estimation accuracy for ataxia when the AR-HMM and time-frequency features are combined and used with classical random forest machine learning approaches.
Related Work
2. Materials and Methods
2.1. Data Collection and Participants
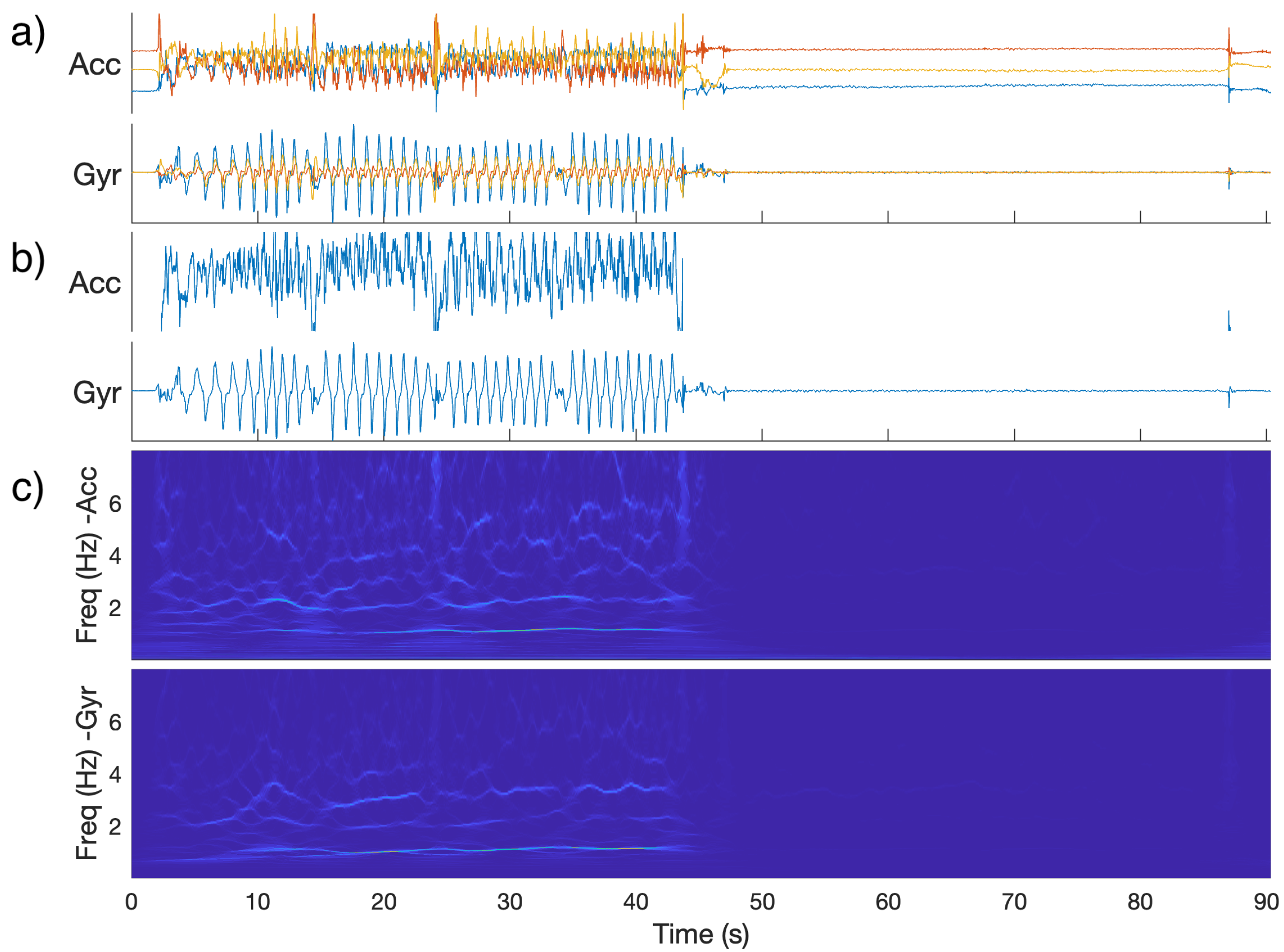
2.2. Preprocessing
2.3. Time Frequency Features
- Total power (rest and task): Power summed across all time bins and all frequencies.
- Ratio of task to rest power: Total power during task divided by total power during rest.
- Low frequency power (rest and task): Power summed across all time bins and all frequencies below the cutoff (2 or 3 Hz, depending on task).
- High frequency power (rest and task): Power summed across all time bins and all frequencies above cutoff.
- Ratio of low to high frequency power (rest and task): Low frequency power divided by high frequency power.
- Center frequency (rest and task): Weighted sum of frequency (with weights the total power for that frequency summed over time), divided by summed power over all frequencies.
- Spread of frequency (rest and task): Squared difference of frequency from center frequency, multiplied total power for that frequency and then summed over all frequencies.
- Center frequency of low frequency (task): As above, but calculated only for frequencies below cutoff.
- Center frequency of high frequency (task): As above, but calculated only for frequencies above cutoff.
- Cosine similarity of adjacent time bins (task): Mean cosine similarity between the vectors of powers for each frequency for adjacent time bins.
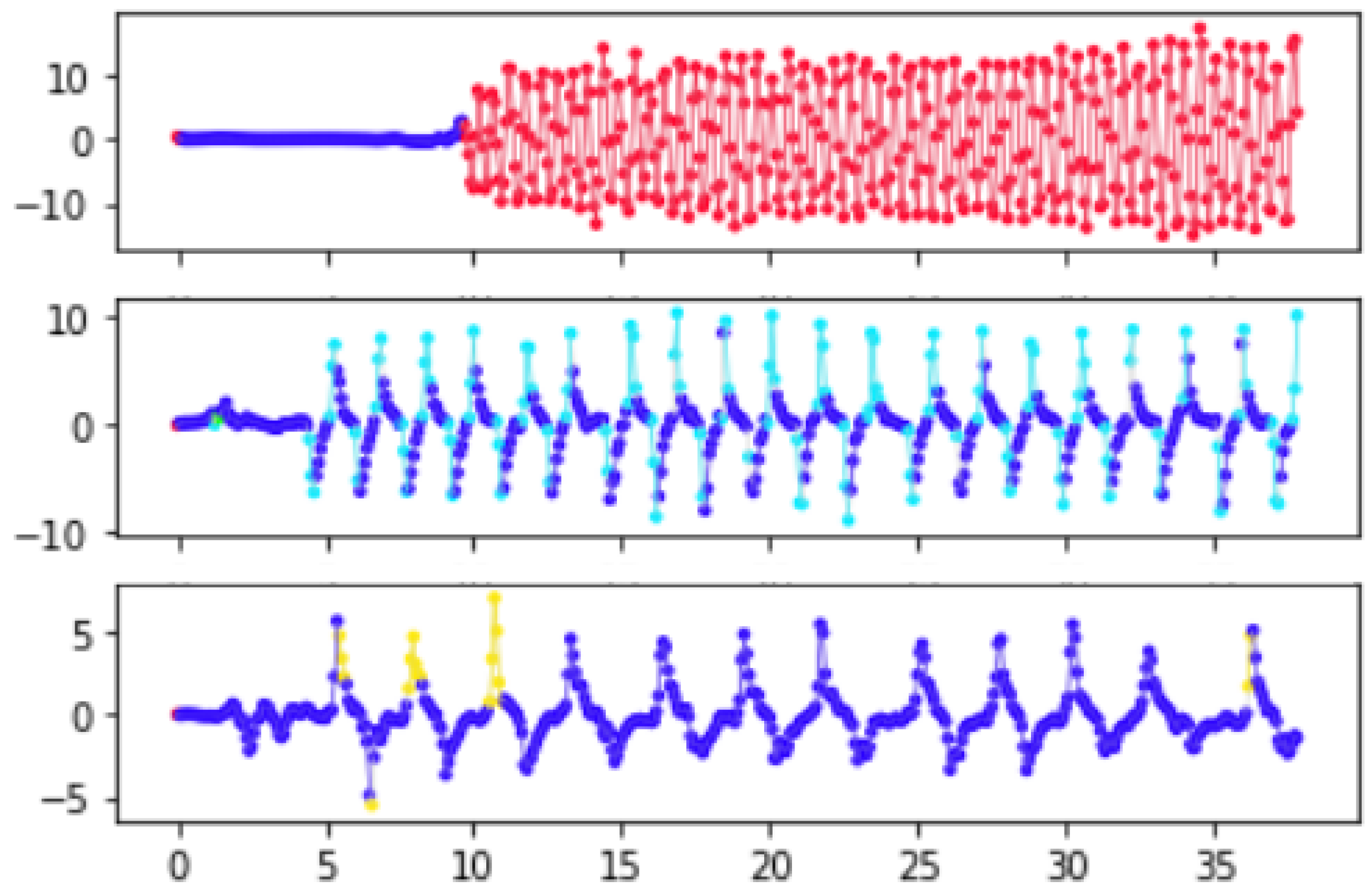
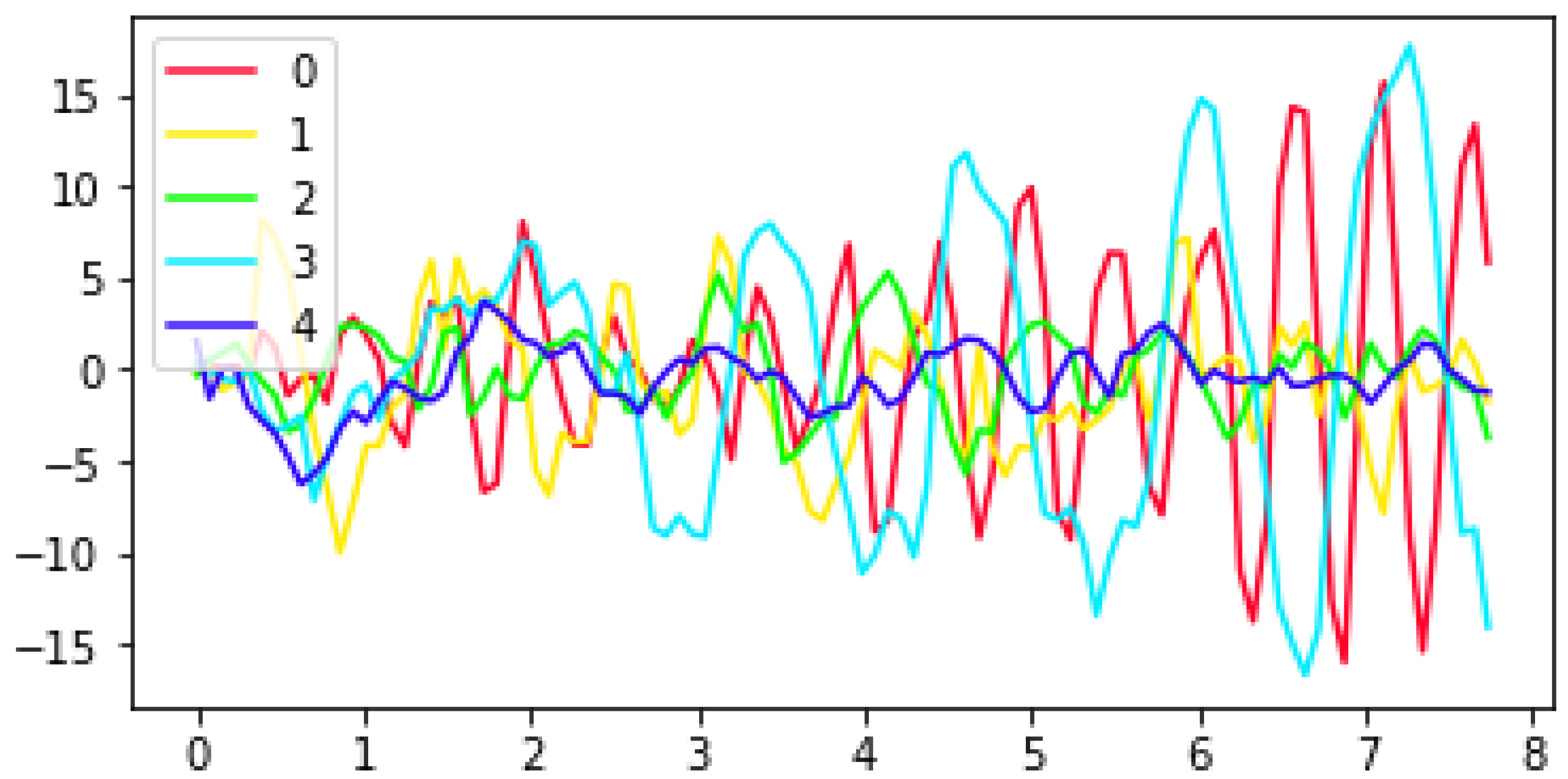
2.4. Autoregressive Hidden Markov Model
- The frequencies of each state in the data
- Each state’s estimated self-transition probability
- The mean of the the length of runs (consecutive appearances) of each state
- The standard deviation of the length of runs (consecutive appearances) of each state
- The estimated entropy rate of the state sequence as calculated from the posterior mean of the Markov transition probabilities.
- For each state, the proportion of state samples drawn that were equal to that mode was averaged over all time points for which that state was the mode
- The proportion of all state samples that were equal to their corresponding mode state in time.
2.5. Classification
2.6. Score Prediction
2.7. Cross-Validation
2.8. Code Availability
3. Results
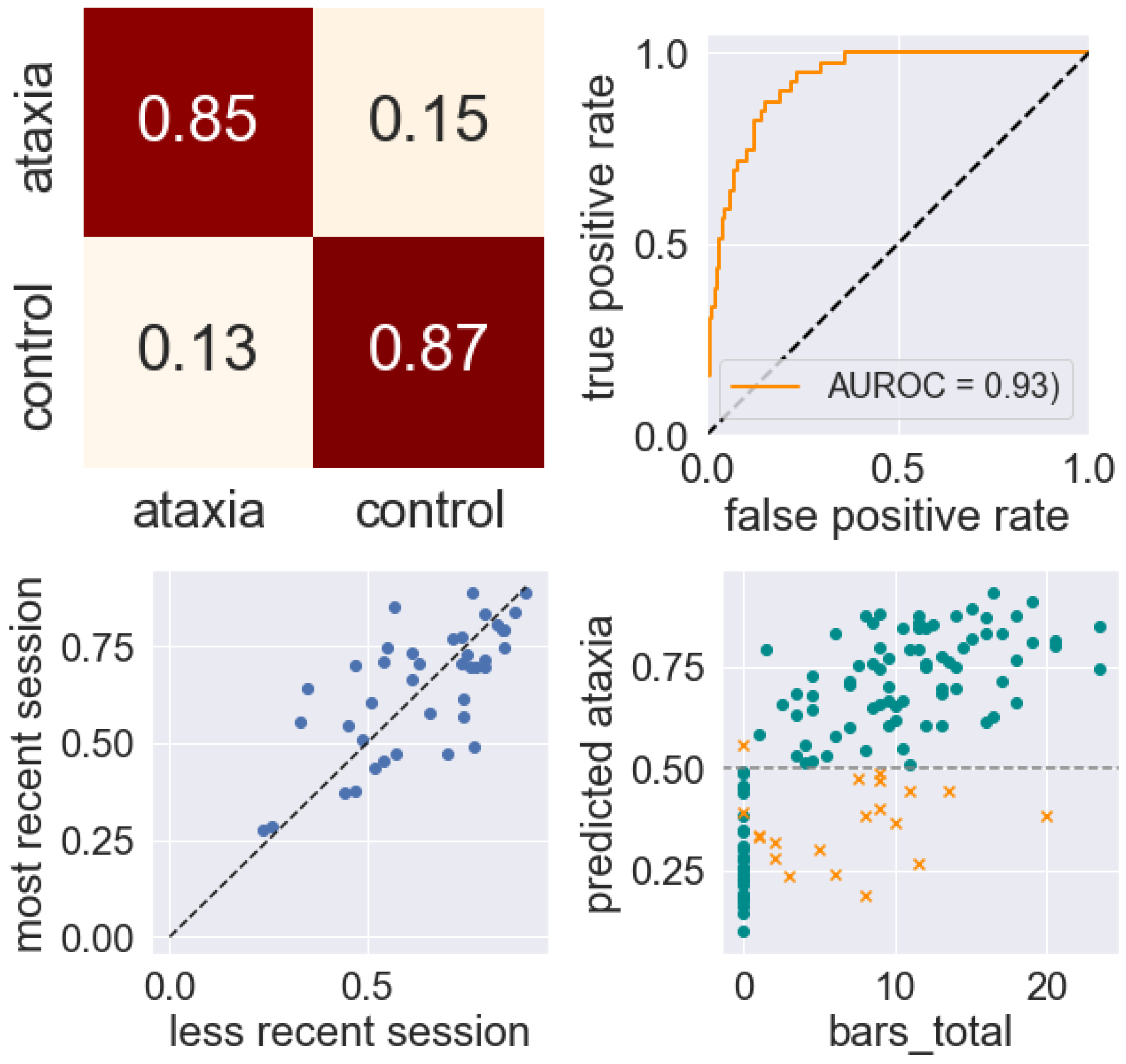
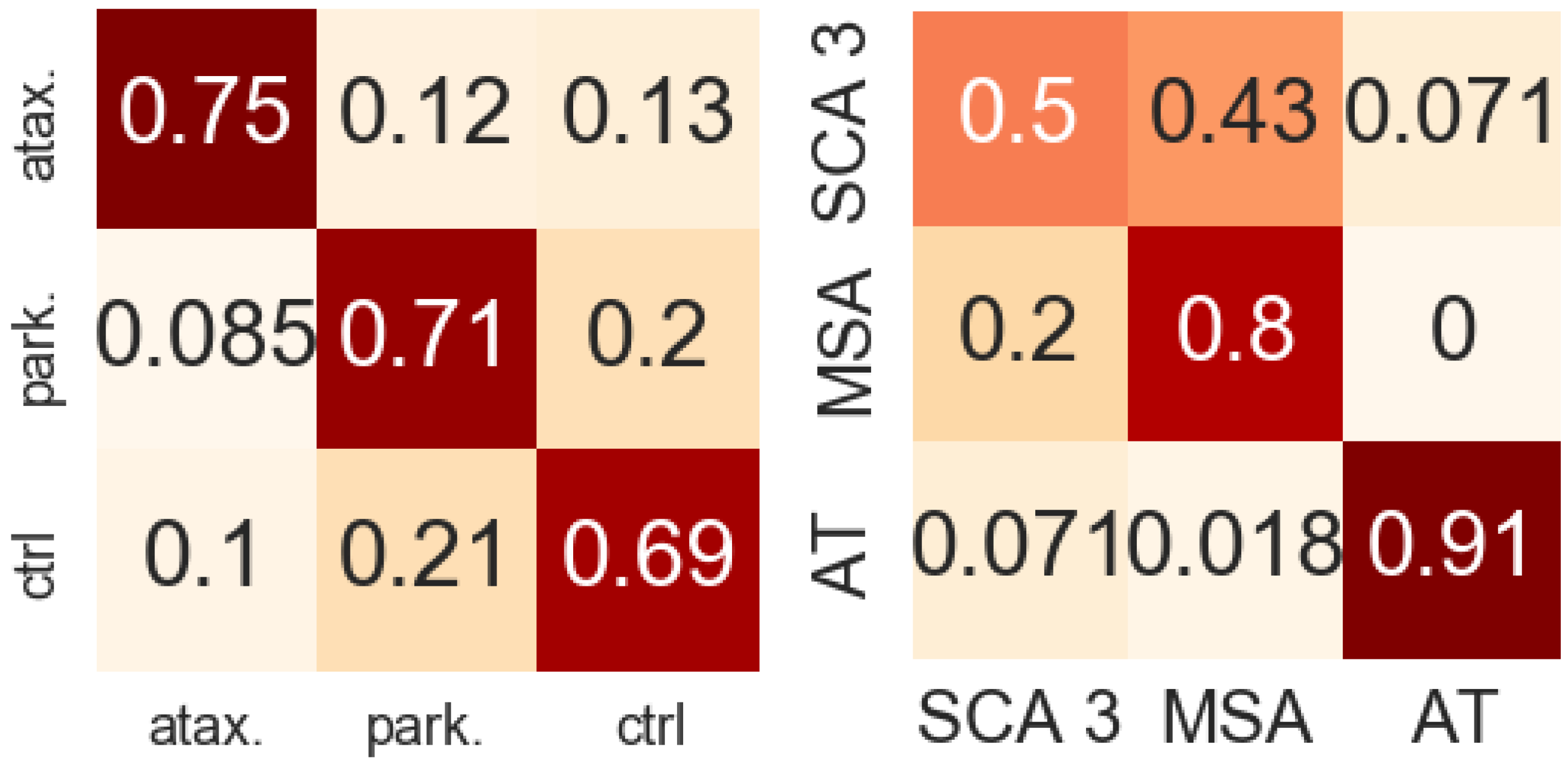
3.1. Classification Results
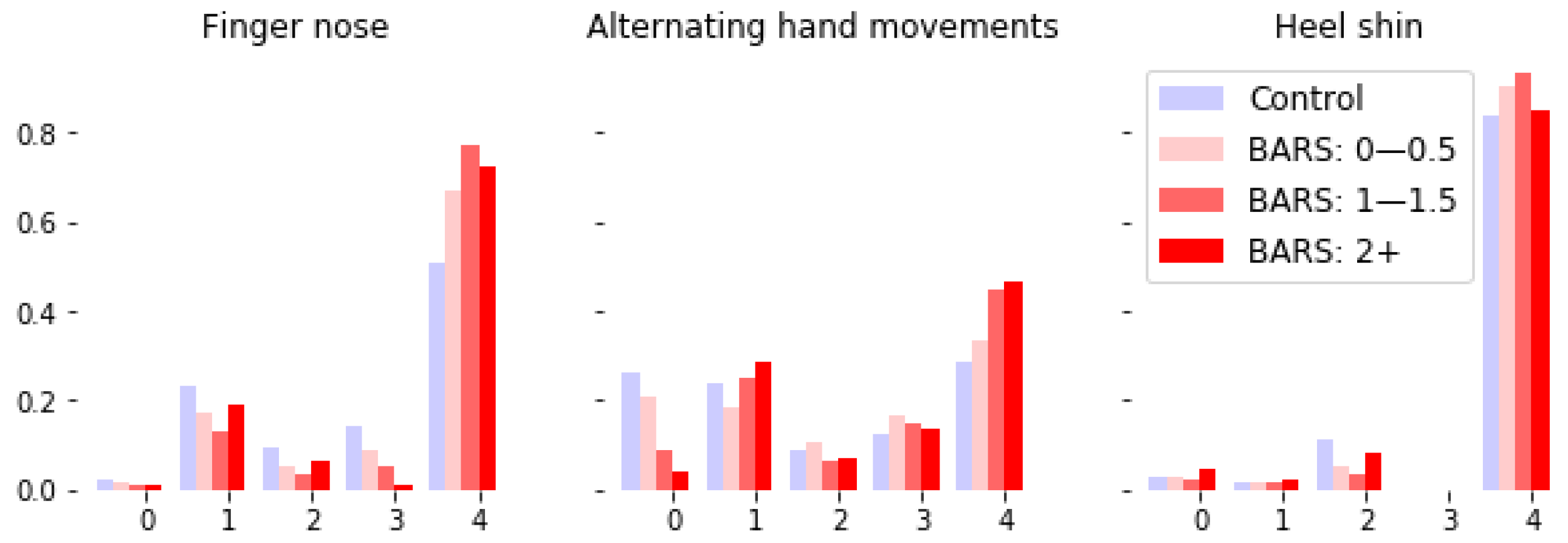
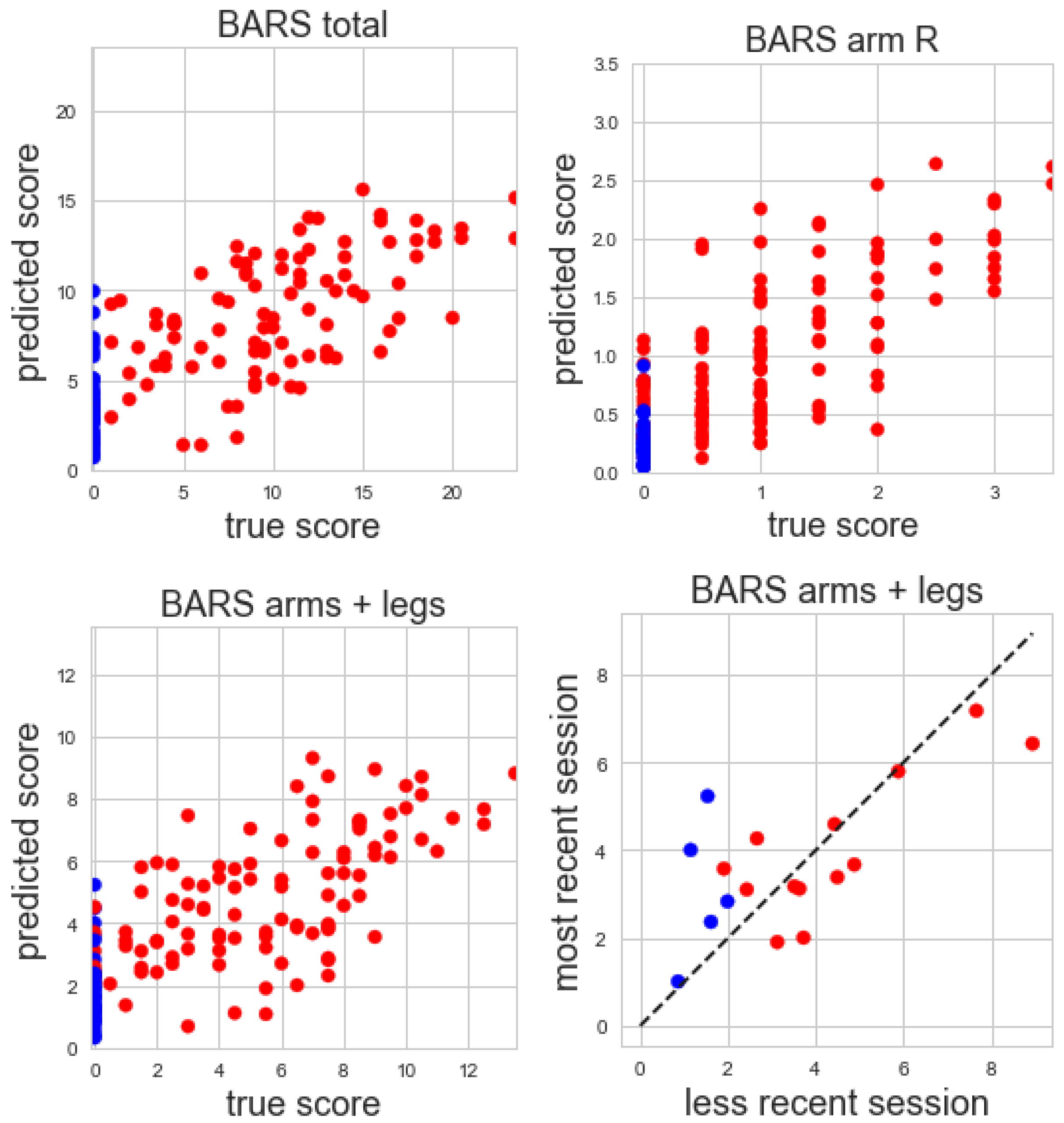
3.2. Score Prediction Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| APDM | APDM Wearable Technologies |
| AR-HMM | Autoregressive hidden Markov model |
| AT | Ataxia-telangectasia |
| BARS | Brief ataxia rating scale |
| CNN | Convolutional neural network |
| FRDA | Friedreich’s ataxia |
| HDP-HMM | Hierarchical Dirichlet process hidden Markov model |
| ICARS | International cooperative ataxia rating scale |
| ILOCA | Idiopathic late-onset cerebellar ataxia |
| IMU | Inertial measurement unit |
| MSA | Multiple system atrophy |
| MVN | Multivariate normal distribution |
| SARA | Scale for the assessment and rating of ataxia |
| SCA | Spinocerebellar ataxia |
References
- Ruano, L.; Melo, C.; Silva, M.C.; Coutinho, P. The global epidemiology of hereditary ataxia and spastic paraplegia: A systematic review of prevalence studies. Neuroepidemiology 2014, 42, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Pringsheim, T.; Jette, N.; Frolkis, A.; Steeves, T.D. The prevalence of Parkinson’s disease: A systematic review and meta-analysis. Mov. Disord. 2014, 29, 1583–1590. [Google Scholar] [CrossRef] [PubMed]
- Schmitz-Hübsch, T.; du Montcel, S.T.; Baliko, L.; Berciano, J.; Boesch, S.; Depondt, C.; Giunti, P.; Globas, C.; Infante, J.; Kang, J.S.; et al. Scale for the assessment and rating of ataxia. Neurology 2006, 66, 1717–1720. [Google Scholar] [CrossRef] [PubMed]
- Trouillas, P.; Takayanagi, T.; Hallett, M.; Currier, R.; Subramony, S.; Wessel, K.; Bryer, A.; Diener, H.; Massaquoi, S.; Gomez, C.; et al. International Cooperative Ataxia Rating Scale for pharmacological assessment of the cerebellar syndrome. J. Neurol. Sci. 1997, 145, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Schmahmann, J.D.; Gardner, R.; MacMore, J.; Vangel, M.G. Development of a brief ataxia rating scale (BARS) based on a modified form of the ICARS. Mov. Disord. 2009, 24, 1820–1828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, A.S. Digital Phenotyping in Clinical Neurology. Semin. Neurol. 2022, 42, 048–059. [Google Scholar] [CrossRef]
- Khan, N.C.; Pandey, V.; Gajos, K.Z.; Gupta, A.S. Free-living motor activity monitoring in ataxia-telangiectasia. Cerebellum 2022, 21, 368–379. [Google Scholar] [CrossRef]
- Fox, E.B.; Sudderth, E.B.; Jordan, M.I.; Willsky, A.S. An HDP-HMM for systems with state persistence. In Proceedings of the 25th International Conference on Machine Learning, Helsinki, Finland, 5–9 July 2008; pp. 312–319. [Google Scholar]
- Fox, E.; Sudderth, E.B.; Jordan, M.I.; Willsky, A.S. Nonparametric Bayesian learning of switching linear dynamical systems. In Proceedings of the Advances in Neural Information Processing Systems, Vancouver, BC, Canada, 7–10 December 2009; pp. 457–464. [Google Scholar]
- Rovini, E.; Maremmani, C.; Cavallo, F. How wearable sensors can support Parkinson’s disease diagnosis and treatment: A systematic review. Front. Neurosci. 2017, 11, 555. [Google Scholar] [CrossRef]
- Maetzler, W.; Domingos, J.; Srulijes, K.; Ferreira, J.J.; Bloem, B.R. Quantitative wearable sensors for objective assessment of Parkinson’s disease. Mov. Disord. 2013, 28, 1628–1637. [Google Scholar] [CrossRef]
- Klucken, J.; Barth, J.; Kugler, P.; Schlachetzki, J.; Henze, T.; Marxreiter, F.; Kohl, Z.; Steidl, R.; Hornegger, J.; Eskofier, B.; et al. Unbiased and mobile gait analysis detects motor impairment in Parkinson’s disease. PLoS ONE 2013, 8, e56956. [Google Scholar] [CrossRef]
- Barrantes, S.; Egea, A.J.S.; Rojas, H.A.G.; Martí, M.J.; Compta, Y.; Valldeoriola, F.; Mezquita, E.S.; Tolosa, E.; Valls-Solè, J. Differential diagnosis between Parkinson’s disease and essential tremor using the smartphone’s accelerometer. PLoS ONE 2017, 12, e0183843. [Google Scholar] [CrossRef] [PubMed]
- Lonini, L.; Dai, A.; Shawen, N.; Simuni, T.; Poon, C.; Shimanovich, L.; Daeschler, M.; Ghaffari, R.; Rogers, J.A.; Jayaraman, A. Wearable sensors for Parkinson’s disease: Which data are worth collecting for training symptom detection models. NPJ Digit. Med. 2018, 1, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butt, A.H.; Rovini, E.; Esposito, D.; Rossi, G.; Maremmani, C.; Cavallo, F. Biomechanical parameter assessment for classification of Parkinson’s disease on clinical scale. Int. J. Distrib. Sens. Netw. 2017, 13, 1550147717707417. [Google Scholar] [CrossRef] [Green Version]
- Zhan, A.; Mohan, S.; Tarolli, C.; Schneider, R.B.; Adams, J.L.; Sharma, S.; Elson, M.J.; Spear, K.L.; Glidden, A.M.; Little, M.A.; et al. Using smartphones and machine learning to quantify Parkinson disease severity: The mobile Parkinson disease score. JAMA Neurol. 2018, 75, 876–880. [Google Scholar] [CrossRef] [PubMed]
- Battista, L.; Romaniello, A. A novel device for continuous monitoring of tremor and other motor symptoms. Neurol. Sci. 2018, 39, 1333–1343. [Google Scholar] [CrossRef] [PubMed]
- Heijmans, M.; Habets, J.; Kuijf, M.; Kubben, P.; Herff, C. Evaluation of Parkinson’s Disease at Home: Predicting Tremor from Wearable Sensors. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 584–587. [Google Scholar]
- Hickey, A.; Gunn, E.; Alcock, L.; Del Din, S.; Godfrey, A.; Rochester, L.; Galna, B. Validity of a wearable accelerometer to quantify gait in spinocerebellar ataxia type 6. Physiol. Meas. 2016, 37, N105. [Google Scholar] [CrossRef] [Green Version]
- LeMoyne, R.; Heerinckx, F.; Aranca, T.; De Jager, R.; Zesiewicz, T.; Saal, H.J. Wearable body and wireless inertial sensors for machine learning classification of gait for people with Friedreich’s ataxia. In Proceedings of the 2016 IEEE 13th International Conference on Wearable and Implantable Body Sensor Networks (BSN), San Francisco, CA, USA, 14–17 June 2016; pp. 147–151. [Google Scholar]
- Phan, D.; Nguyen, N.; Pathirana, P.N.; Horne, M.; Power, L.; Szmulewicz, D. A random forest approach for quantifying gait ataxia with truncal and peripheral measurements using multiple wearable sensors. IEEE Sens. J. 2019, 20, 723–734. [Google Scholar] [CrossRef]
- Phan, D.; Nguyen, N.; Pathirana, P.N.; Horne, M.; Power, L.; Szmulewicz, D. Quantitative Assessment of Ataxic Gait using Inertial Sensing at Different Walking Speeds. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 4600–4603. [Google Scholar]
- Ilg, W.; Seemann, J.; Giese, M.; Traschütz, A.; Schöls, L.; Timmann, D.; Synofzik, M. Real-life gait assessment in degenerative cerebellar ataxia: Toward ecologically valid biomarkers. Neurology 2020, 95, e1199–e1210. [Google Scholar] [CrossRef]
- Lee, J.; Oubre, B.; Daneault, J.F.; Stephen, C.D.; Schmahmann, J.D.; Gupta, A.S.; Lee, S.I. Analysis of Gait Sub-Movements to Estimate Ataxia Severity using Ankle Inertial Data. IEEE Trans. Biomed. Eng. 2022, 69, 2314–2323. [Google Scholar] [CrossRef]
- Tran, H.; Pathirana, P.N.; Horne, M.; Power, L.; Szmulewicz, D.J. Automated Evaluation of Upper Limb Motor Impairment of Patient with Cerebellar Ataxia. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 6846–6849. [Google Scholar]
- Nguyen, K.D.; Pathirana, P.N.; Horne, M.; Power, L.; Szmulewicz, D. Quantitative Assessment of Cerebellar Ataxia with Kinematic Sensing During Rhythmic Tapping. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 1098–1101. [Google Scholar]
- Oubre, B.; Daneault, J.F.; Whritenour, K.; Khan, N.C.; Stephen, C.D.; Schmahmann, J.D.; Lee, S.I.; Gupta, A.S. Decomposition of reaching movements enables detection and measurement of ataxia. Cerebellum 2021, 20, 811–822. [Google Scholar] [CrossRef]
- Gavriel, C.; Thomik, A.A.; Lourenço, P.R.; Nageshwaran, S.; Athanasopoulos, S.; Sylaidi, A.; Festenstein, R.; Faisal, A.A. Towards neurobehavioral biomarkers for longitudinal monitoring of neurodegeneration with wearable body sensor networks. In Proceedings of the 2015 7th International IEEE/EMBS Conference on Neural Engineering (NER), Montpellier, France, 22–24 April 2015; pp. 348–351. [Google Scholar]
- Oung, Q.W.; Muthusamy, H.; Basah, S.N.; Lee, H.; Vijean, V. Empirical wavelet transform based features for classification of Parkinson’s disease severity. J. Med. Syst. 2018, 42, 29. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, T.; Hamahata, K.; Iwahashi, N. Unsupervised segmentation of human motion data using a sticky hierarchical dirichlet process-hidden markov model and minimal description length-based chunking method for imitation learning. Adv. Robot. 2011, 25, 2143–2172. [Google Scholar] [CrossRef]
- Wiltschko, A.B.; Johnson, M.J.; Iurilli, G.; Peterson, R.E.; Katon, J.M.; Pashkovski, S.L.; Abraira, V.E.; Adams, R.P.; Datta, S.R. Mapping sub-second structure in mouse behavior. Neuron 2015, 88, 1121–1135. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiltschko, A.B.; Tsukahara, T.; Zeine, A.; Anyoha, R.; Gillis, W.F.; Markowitz, J.E.; Peterson, R.E.; Katon, J.; Johnson, M.J.; Datta, S.R. Revealing the structure of pharmacobehavioral space through motion sequencing. Nat. Neurosci. 2020, 23, 1433–1443. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.R.; Gommers, R.; Waselewski, F.; Wohlfahrt, K.; O’Leary, A. PyWavelets: A Python package for wavelet analysis. J. Open Source Softw. 2019, 4, 1237. [Google Scholar] [CrossRef]
- Daubechies, I.; Lu, J.; Wu, H.T. Synchrosqueezed wavelet transforms: An empirical mode decomposition-like tool. Appl. Comput. Harmon. Anal. 2011, 30, 243–261. [Google Scholar] [CrossRef] [Green Version]
- MATLAB Wavelet Toolbox; The MathWorks: Natick, MA, USA, 2018.
- Teh, Y.W.; Jordan, M.I.; Beal, M.J.; Blei, D.M. Sharing clusters among related groups: Hierarchical Dirichlet processes. In Proceedings of the Advances in Neural Information Processing Systems, Vancouver, BC, Canada, 5–8 December 2005; pp. 1385–1392. [Google Scholar]
- Chen, C.; Liaw, A.; Breiman, L. Using Random Forest to Learn Imbalanced Data; Technical Report; University of California: Berkeley, CA, USA, 2004; Volume 110, p. 24. [Google Scholar]
- Lemaître, G.; Nogueira, F.; Aridas, C.K. Imbalanced-learn: A Python Toolbox to Tackle the Curse of Imbalanced Datasets in Machine Learning. J. Mach. Learn. Res. 2017, 18, 1–5. [Google Scholar]
- Pedregosa, F.; Varoquaux, G.; Gramfort, A.; Michel, V.; Thirion, B.; Grisel, O.; Blondel, M.; Prettenhofer, P.; Weiss, R.; Dubourg, V.; et al. Scikit-learn: Machine Learning in Python. J. Mach. Learn. Res. 2011, 12, 2825–2830. [Google Scholar]
- Goetz, C.G.; Tilley, B.C.; Shaftman, S.R.; Stebbins, G.T.; Fahn, S.; Martinez-Martin, P.; Poewe, W.; Sampaio, C.; Stern, M.B.; Dodel, R.; et al. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Scale presentation and clinimetric testing results. Mov. Disord. Off. J. Mov. Disord. Soc. 2008, 23, 2129–2170. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | Age | Women | Men | Severity Score | |
|---|---|---|---|---|---|
| Subjects, Sessions | Mean (SD) | Mean (SD) | |||
| Total | 195, 242 | 46.9 (24.1) | 78 | 117 | n/a |
| Ataxia (all) | 109, 144 | 43.1 (23.8) | 49 | 60 | 10.3 (5.3) |
| AT | 34, 56 | 12.4 (6.1) | 13 | 21 | 11.3 (5.7) |
| Episodic Ataxia | 2, 2 | 50.0 (28.0) | 0 | 2 | 1.2 (0.2) |
| FA | 2, 2 | 55.5 (5.5) | 1 | 1 | 16.2 (2.8) |
| MSA | 5, 6 | 60.4 (5.2) | 2 | 3 | 12.2 (3.8) |
| SCA 1 | 4, 8 | 49.0 (14.1) | 3 | 1 | 8.1 (2.0) |
| SCA 2 | 2, 2 | 61.0 (6.0) | 1 | 1 | 12.0 (1.5) |
| SCA 3 | 11, 14 | 51.0 (10.6) | 9 | 2 | 9.5 (3.3) |
| SCA 6 | 8, 9 | 69.0 (6.0) | 3 | 5 | 12.8 (6.1) |
| SPG 7 | 2, 2 | 58.0 (2.0) | 0 | 2 | 9.0 (1.0) |
| Transient Ataxia | 2, 2 | 72.5 (2.5) | 1 | 1 | 1.0 (0.0) |
| Ataxia (other) | 36, 40 | 55.8 (14.0) | 16 | 20 | 10.6 (5.7) |
| Parkisonism | 52, 59 | 67.6 (7.9) | 14 | 38 | 16.5 (9.7) |
| Control | 34, 39 | 27.5 (18.4) | 15 | 19 | n/a |
| AUROC | Sensitivity | Specificity | Test-Retest Correlation (# Sessions) | |
|---|---|---|---|---|
| Ataxia/control | 0.93 | 0.85 | 0.87 | 0.70 (35) |
| Ataxia/control (AR-HMM only) | 0.89 | 0.81 | 0.80 | 0.51 (35) |
| Ataxia/control (time-freq only) | 0.93 | 0.86 | 0.90 | 0.74 (35) |
| Mild ataxia/control | 0.87 | 0.76 | 0.82 | 0.62 (12) |
| Mild ataxia/control (AR-HMM only) | 0.80 | 0.78 | 0.78 | 0.61 (12) |
| Mild ataxia/control (time-freq only) | 0.87 | 0.78 | 0.79 | 0.52 (12) |
| Pediatric ataxia/control | 0.95 | 0.90 | 0.93 | 0.84 (20) |
| Adult ataxia/control | 0.90 | 0.80 | 0.80 | 0.46 (15) |
| Ataxia/parkinsonism | 0.93 | 0.88 | 0.83 | 0.94 (35) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knudson, K.C.; Gupta, A.S. Assessing Cerebellar Disorders with Wearable Inertial Sensor Data Using Time-Frequency and Autoregressive Hidden Markov Model Approaches. Sensors 2022, 22, 9454. https://doi.org/10.3390/s22239454
Knudson KC, Gupta AS. Assessing Cerebellar Disorders with Wearable Inertial Sensor Data Using Time-Frequency and Autoregressive Hidden Markov Model Approaches. Sensors. 2022; 22(23):9454. https://doi.org/10.3390/s22239454
Chicago/Turabian StyleKnudson, Karin C., and Anoopum S. Gupta. 2022. "Assessing Cerebellar Disorders with Wearable Inertial Sensor Data Using Time-Frequency and Autoregressive Hidden Markov Model Approaches" Sensors 22, no. 23: 9454. https://doi.org/10.3390/s22239454