
Chronic and Acute Effects on Skin Temperature from a Sport Consisting of Repetitive Impacts from Hitting a Ball with the Hands
 , , , , and
, , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Experimental Protocol
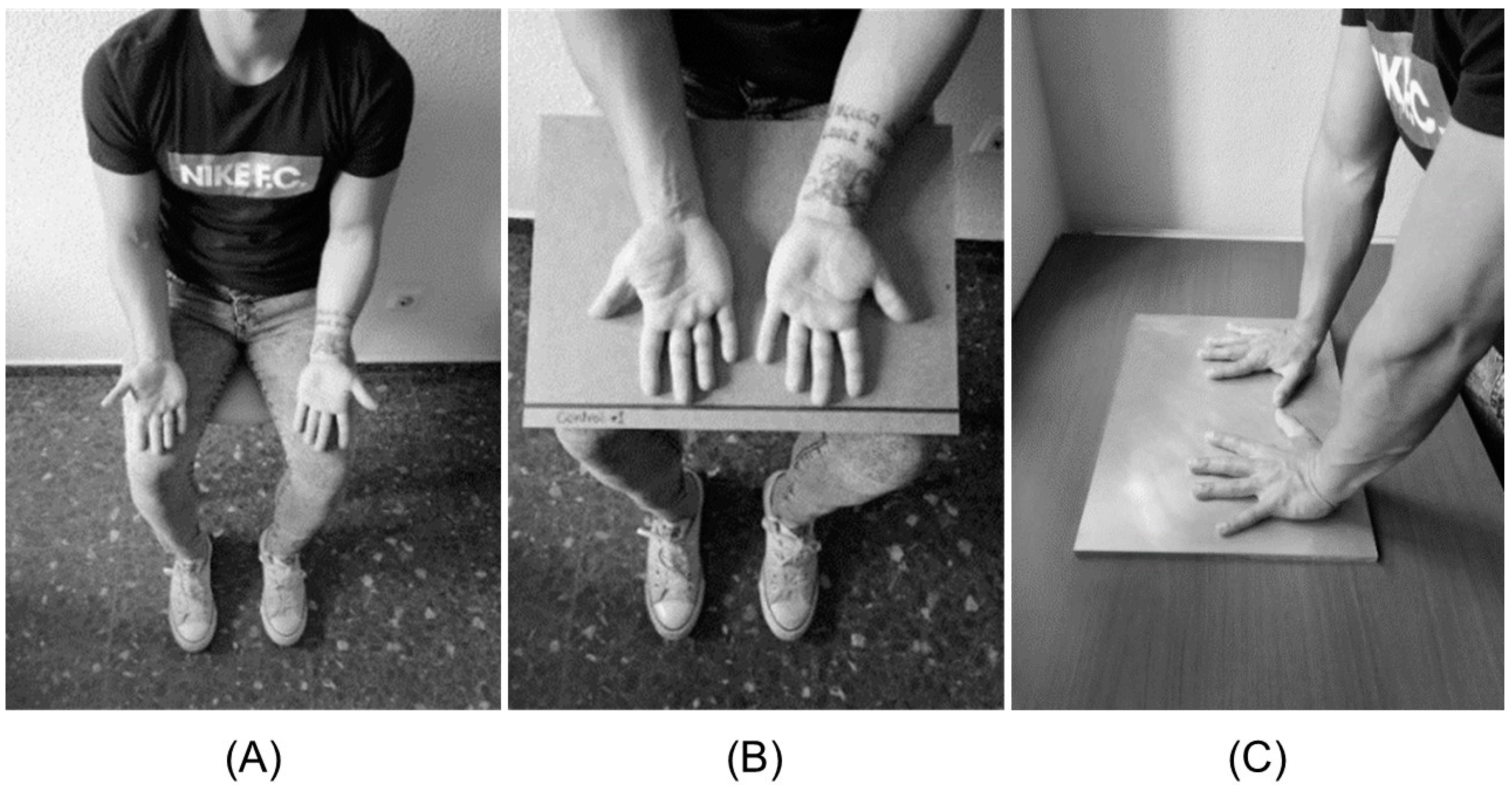
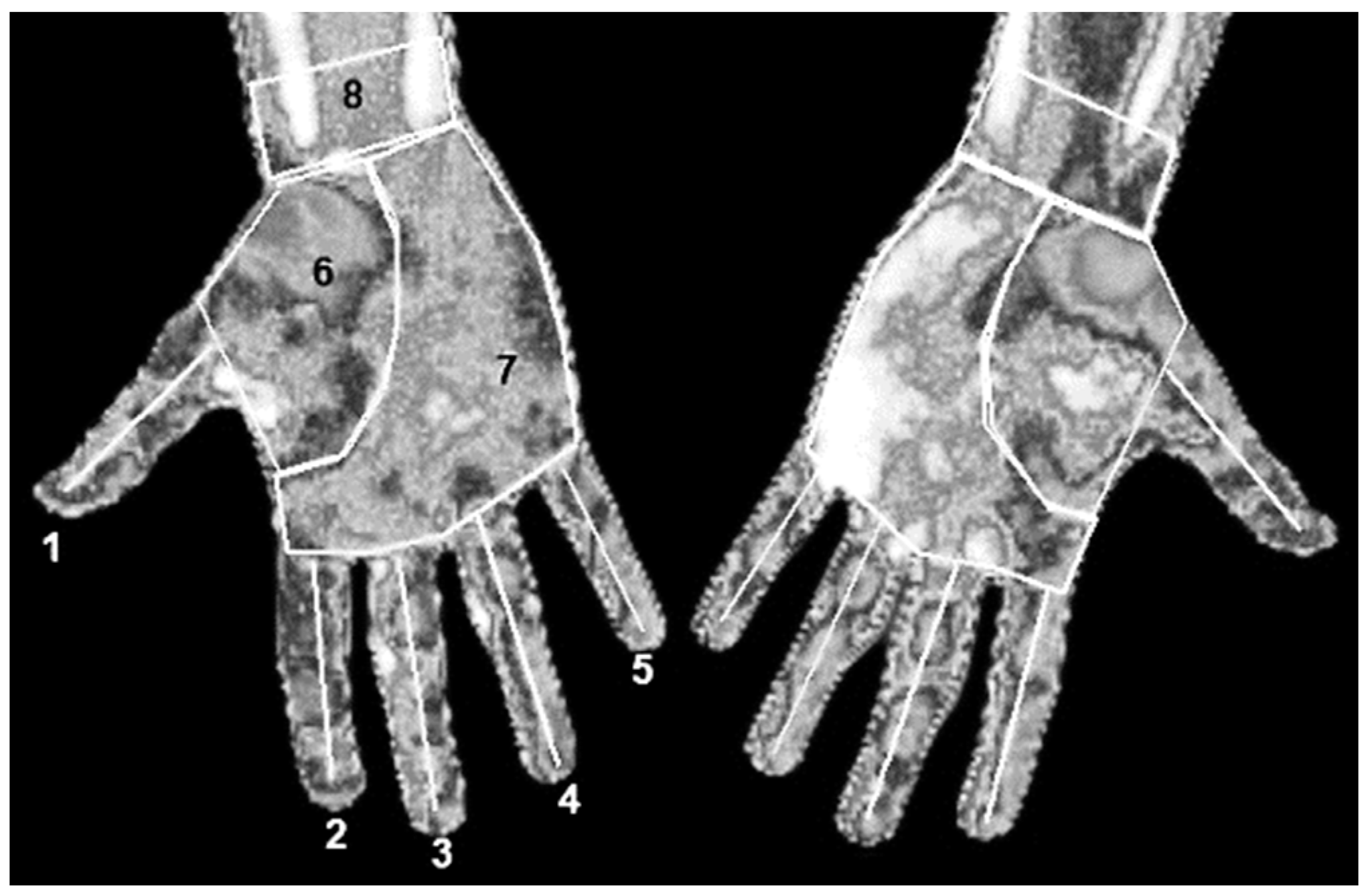
2.3. Procedures
2.4. Statistical Analysis
3. Results
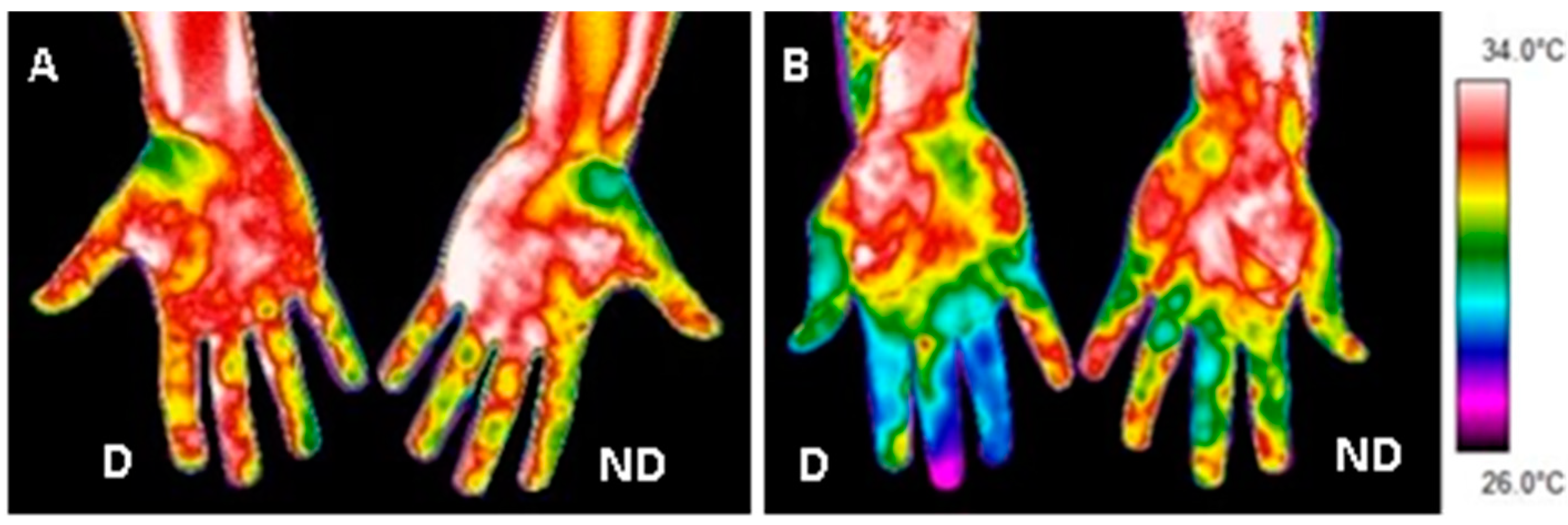
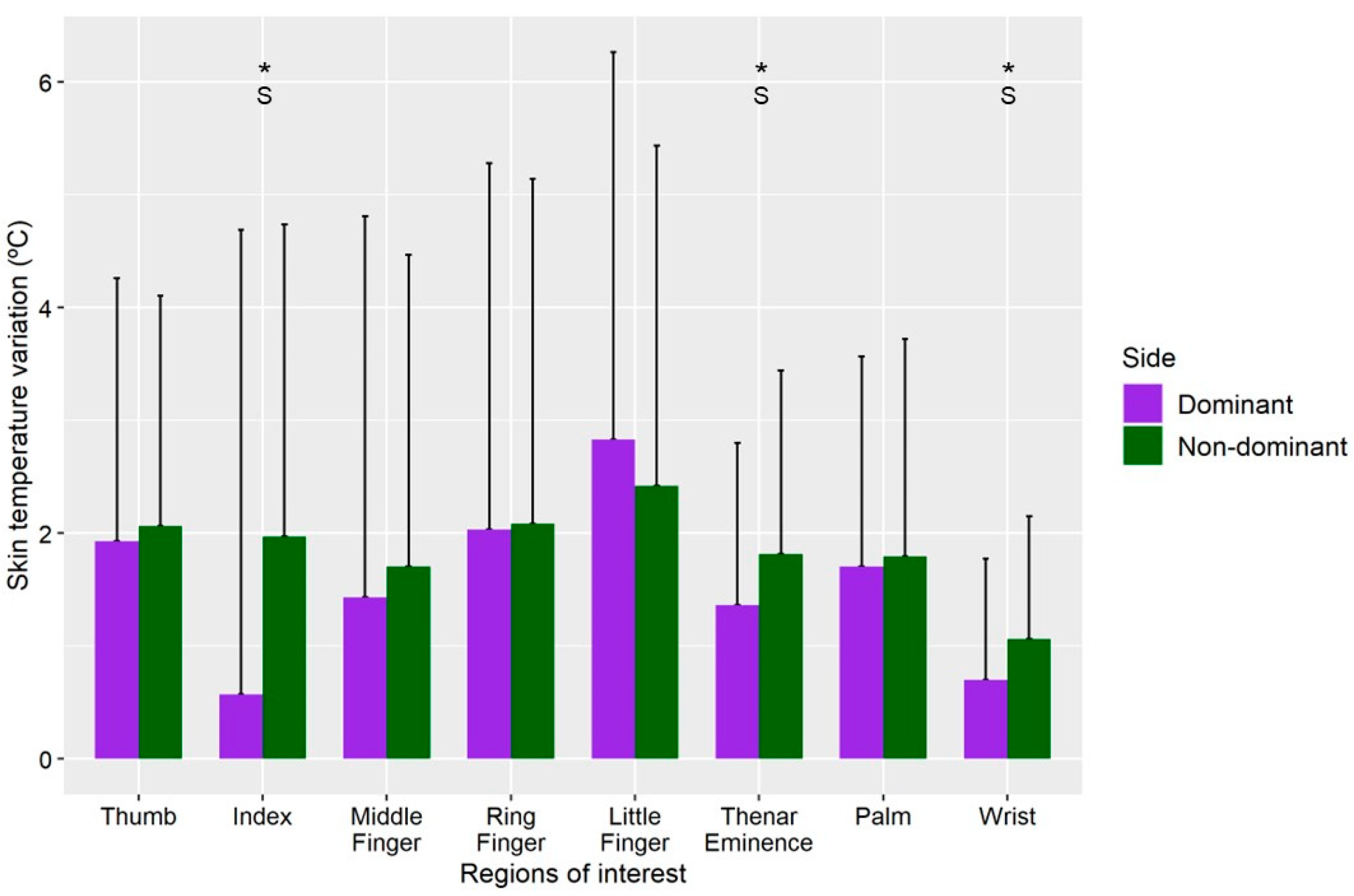
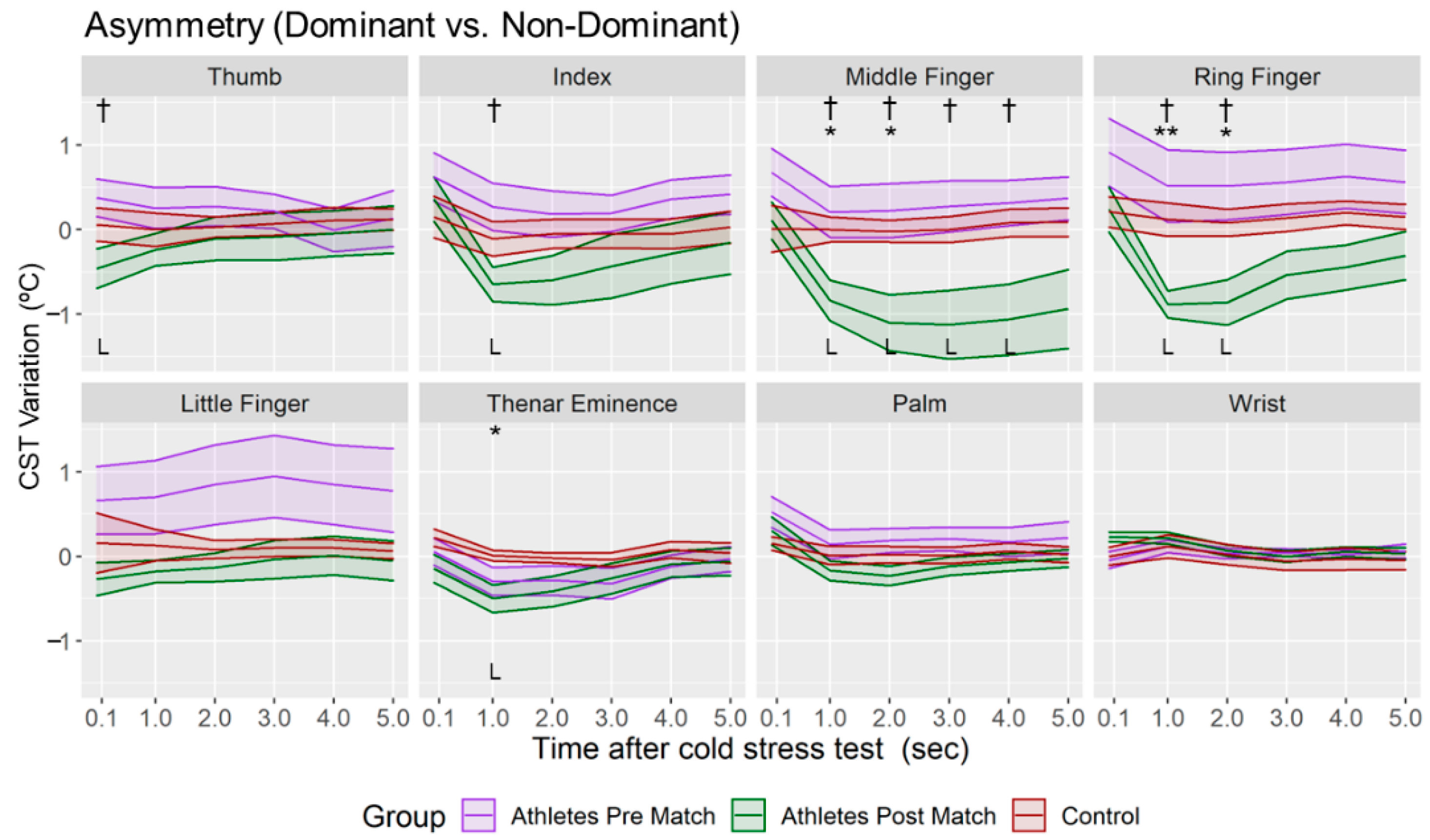
3.1. Thermal Asymmetry Analysis
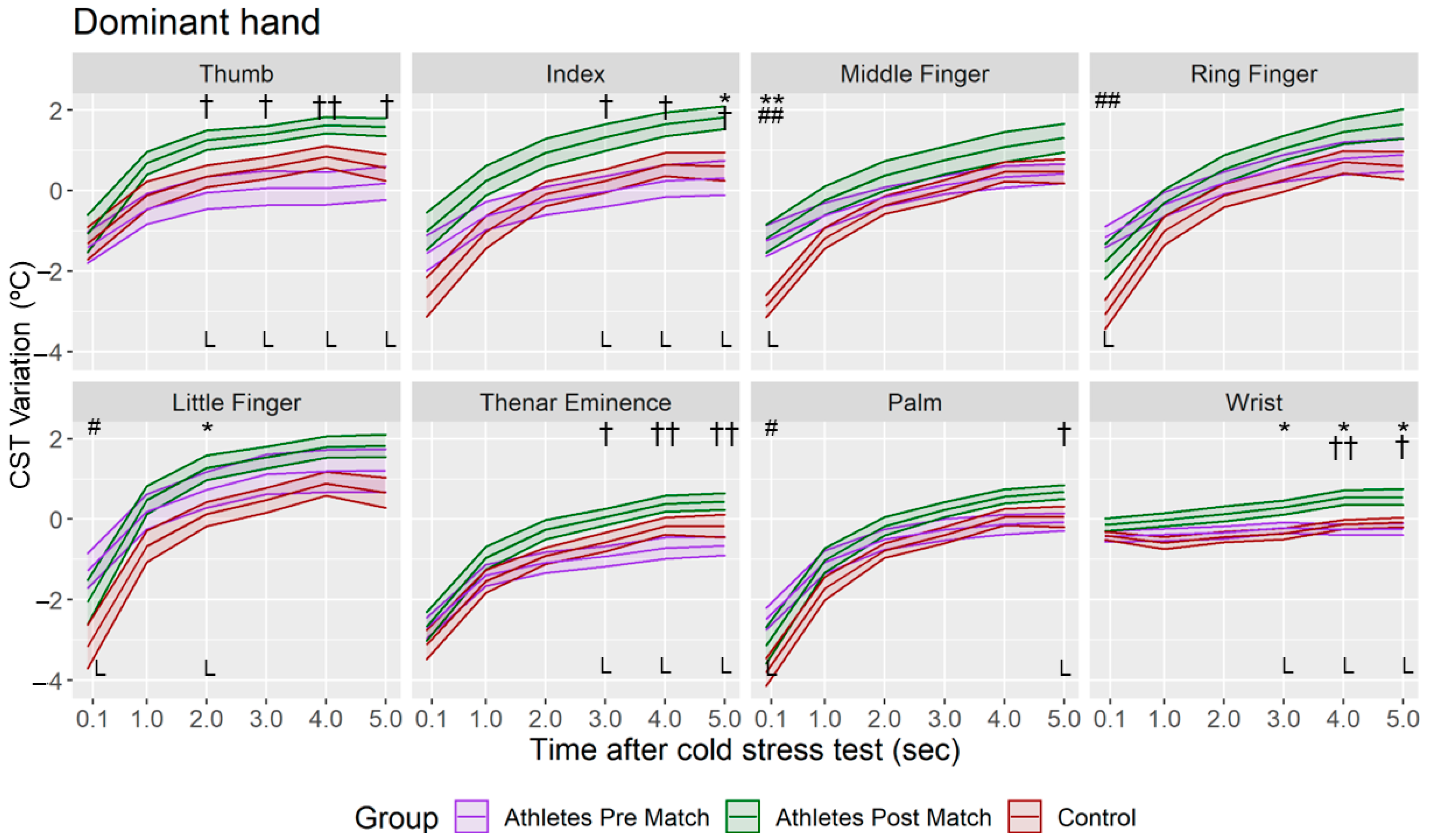
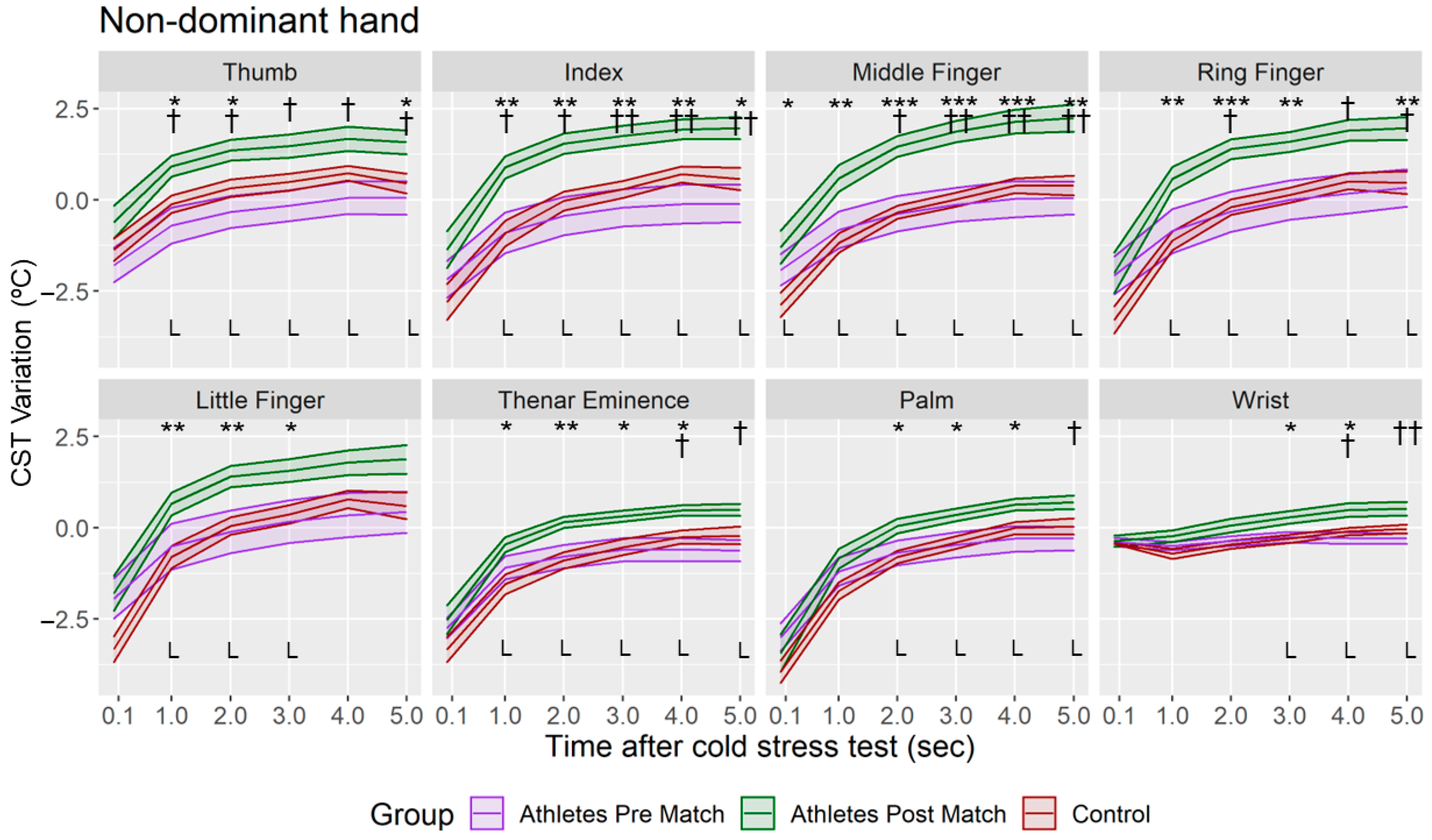
3.2. Thermal Stress Protocol
3.3. Relationship between Tsk Variation and Hand Hitting Count
4. Discussion
4.1. Thermal Asymmetry Analysis
4.2. Thermal Stress Protocol
4.3. Relationship between Tsk Variation and Hand Hitting Count
4.4. Limitations of the Study and future studies
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Montaner, C.; Llana, S.; Gámez, J.; Alcántara, E. Especificaciones de diseño para el desarrollo de un guante de pilota valenciana. Rev. Int. Med. Y Cienc. La Act. Física Y El Deport. 2012, 12, 405–429. [Google Scholar]
- Montaner, A.; Llana, S.; Gámez, J.; Montaner, C. Estudio epidemiológico en pelota valenciana. Rev. Int. Med. Y Cienc. La Act. Física Y El Deport. 2013, 13, 235–255. [Google Scholar]
- De Andrade, A.; Dos Santos, P.R.; Brito, C.J.; De Moura, A.G.; Moreira, D.G.; Costa, C.M.A.; Sillero, M.; Marins, J.C.B. Measuring skin temperature before, during and after exercise: A comparison of thermocouples and infrared thermography. Physiol. Meas. 2014, 35, 189–203. [Google Scholar] [CrossRef] [Green Version]
- Priego, J.I.; Kunzler, M.R.; Carpes, F.P. Methodological Aspects of Infrared Thermography in Human Assessment. In Application of Infrared Thermography in Sports Science; Springer International Publishing: Valencia, Spain, 2017; pp. 49–79. ISBN 978-3-319-47409-0. [Google Scholar]
- Niu, H.H.; Lui, P.W.; Hu, J.S.; Ting, C.K.; Yin, Y.C.; Lo, Y.L.; Liu, L.; Lee, T.Y. Thermal symmetry of skin temperature: Normative data of normal subjects in Taiwan. Zhonghua Yi Xue Za Zhi (Taipei) 2001, 64, 459–468. [Google Scholar]
- Vardasca, R.; Ring, E.; Plassman, P.; Jones, C. Termal symmetry of the upper and lower extremities in healthy subjects. Thermol. Int. 2012, 22, 53–60. [Google Scholar]
- Fernández, I.; Arnáiz, J.; Escamilla, V.; Gómez, P. Infrared Thermography for the Detection of Injury in Sports Medicine. In Application of Infrared Thermography in Sports Science; Springer: Cham, Switzerland, 2017; pp. 81–109. [Google Scholar]
- Hildebrandt, C.; Raschner, C.; Ammer, K. An Overview of Recent Application of Medical Infrared Thermography in Sports Medicine in Austria. Sensors 2010, 10, 4700. [Google Scholar] [CrossRef] [Green Version]
- De Weerd, L.; Mercer, J.B.; Weum, S. Dynamic infrared thermography. Clin. Plast. Surg. 2011, 38, 277–292. [Google Scholar] [CrossRef]
- Sawasaki, N.; Iwase, S.; Mano, T. Effect of skin sympathetic response to local or systemic cold exposure on thermoregulatory functions in humans. Auton. Neurosci. 2001, 87, 274–281. [Google Scholar] [CrossRef]
- Leijon, K.; Tegner, Y.; Juntti, U.; Karp, K.; Lehto, N. Hand skin temperature—Are there warm and cold rewarming patterns after cold stress test? Thermol. Int. 2016, 26, 81–87. [Google Scholar]
- del Estal, A.; Brito, C.J.; Galindo, V.E.; Lopez Diaz de Durana, A.; Franchini, E.; Sillero-Quintana, M. Asymétries thermiques en sport de combat, mesurées par thermographie infrarouge. Sci. Sport. 2017, 32, e61–e67. [Google Scholar] [CrossRef]
- Price, D.D.; McGrath, P.A.; Rafii, A.; Buckingham, B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain 1983, 17, 45–56. [Google Scholar] [CrossRef]
- Moreira, D.G.; Costello, J.T.; Brito, C.J.; Adamczyk, J.G.; Ammer, K.; Bach, A.J.E.; Costa, C.M.A.; Eglin, C.; Fernandes, A.A.; Fernández, I.; et al. Thermographic imaging in sports and exercise medicine: A Delphi study and consensus statement on the measurement of human skin temperature. J. Therm. Biol. 2017, 69, 155–162. [Google Scholar] [CrossRef]
- Ioannou, L.G.; Tsoutsoubi, L.; Mantzios, K.; Gkikas, G.; Piil, J.F.; Dinas, P.C.; Notley, S.R.; Kenny, G.P.; Nybo, L.; Flouris, A.D. The Impacts of Sun Exposure on Worker Physiology and Cognition: Multi-Country Evidence and Interventions. Int. J. Environ. Res. Public Health 2021, 18, 7698. [Google Scholar] [CrossRef]
- Rastogi, S.K.; Gupta, B.N.; Husain, T. Wet-bulb globe temperature index: A predictor of physiological strain in hot environments. Occup. Med. 1992, 42, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.; Nilsson, H.; Holmér, I. Finger cooling by contact with cold aluminium surfaces—Effects of pressure, mass and whole body thermal balance. Eur. J. Appl. Physiol. Occup. Physiol. 1994, 69, 55–60. [Google Scholar] [CrossRef] [PubMed]
- Jay, O.; Havenith, G. Finger skin cooling on contact with cold materials: A comparison between male and female responses during short-term exposures. Eur. J. Appl. Physiol. 2004, 91, 373–381. [Google Scholar] [CrossRef] [Green Version]
- House, C.M.; Taylor, R.J.; Oakley, E.H.N. Repeatability of a cold stress test to assess cold sensitization. Occup. Med. 2015, 65, 578–584. [Google Scholar] [CrossRef] [Green Version]
- Steketee, J. Spectral emissivity of skin and pericardium. Phys. Med. Biol. 1973, 18, 686–694. [Google Scholar] [CrossRef]
- Hedges, L.V. Estimation of effect size from a series of independent experiments. Psychol. Bull. 1982, 92, 490–499. [Google Scholar] [CrossRef]
- Montaner, C. Diseño de un Guante de Protección para Jugar a Pilota Valenciana en Función de la Opinión de los Usuarios y de Criterios Epidemiológicos y Biomecánicos. Ph.D. Thesis, Universitat de València, Dialnet, Valencia, Spain, 2012. [Google Scholar]
- Laporte, G. Patología de la mano del pelotari. Arch. Med. Del Deport. 1972, 3, 31–42. [Google Scholar]
- Gatt, A.; Formosa, C.; Cassar, K.; Camilleri, K.P.; De Raffaele, C.; Mizzi, A.; Azzopardi, C.; Mizzi, S.; Falzon, O.; Cristina, S.; et al. Thermographic patterns of the upper and lower limbs: Baseline data. Int. J. Vasc. Med. 2015, 2015, 831369. [Google Scholar] [CrossRef] [Green Version]
- Miziołek, B.; Lis-Święty, A.; Kucharz, E.; Pieczyrak, R.; Polak, K.; Szczepanek, M.; Bergler-Czop, B. Clinical assessment of patients with systemic sclerosis: Is there a place for thermography? Arch. Dermatol. Res. 2022, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Li, W.W.; Carter, M.J.; Mashiach, E.; Guthrie, S.D. Vascular assessment of wound healing: A clinical review. Int. Wound J. 2017, 14, 460–469. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, M.H.; Pugh, N.; Wright, I.; Brownlee, M. A vascular basis for repetitive strain injury. Rheumatology 1999, 38, 636–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tirloni, A.S.; Dos Reis, D.C.; Ramos, E.; Moro, A.R.P. Thermographic Evaluation of the Hands of Pig Slaughterhouse Workers Exposed to Cold Temperatures. Int. J. Environ. Res. Public Health 2017, 14, 838. [Google Scholar] [CrossRef] [PubMed]
- Priego, J.I.; Lucas, A.G.; Gil, M.; Giménez, J.V.; Aparicio, I.; Cibrián Ortiz de Anda, R.M.; Salvador, R.; Llana, S.; Pérez, P. Effects of graduated compression stockings on skin temperature after running. J. Therm. Biol. 2015, 52, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Cuevas, I.; Bouzas Marins, J.C.; Arnáiz Lastras, J.; Gómez Carmona, P.M.; Piñonosa Cano, S.; García-Concepción, M.Á.; Sillero-Quintana, M. Classification of factors influencing the use of infrared thermography in humans: A review. Infrared Phys. Technol. 2015, 71, 28–55. [Google Scholar] [CrossRef]
- Binzoni, T.; Tchernin, D.; Richiardi, J.; Van De Ville, D.; Hyacinthe, J.N. Haemodynamic responses to temperature changes of human skeletal muscle studied by laser-Doppler flowmetry. Physiol. Meas. 2012, 33, 1181. [Google Scholar] [CrossRef] [Green Version]
- Clegg, D.; Mauvais, F. An integrated view of sex differences in metabolic physiology and disease. Mol. Metab. 2018, 15, 1–2. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Athletes Group (n = 13) | Control Group (n = 10) | p-Value | |
|---|---|---|---|
| Age (years) | 24 ± 4 | 26 ± 3 | 0.27 |
| Height (m) | 1.80 ± 0.05 | 1.78 ± 0.04 | 0.15 |
| Body mass (kg) | 80.7 ± 6.9 | 75.2 ± 8.2 | 0.95 |
| BMI (kg/m2) | 24.91 ± 1.87 | 23.70 ± 2.40 | 0.25 |
| Blood pressure (mmHg) | 122/77 ± 9/7 | 120/75 ± 9/8 | 0.61/0.83 |
| ROI | Dominant Hand | Non-Dominant Hand | |||
|---|---|---|---|---|---|
| Mean (°C) | SD (°C) | Mean (°C) | SD (°C) | ||
| Control Group | Thumb | 32.82 | 1.45 | 32.83 | 1.25 |
| Index | 32.75 * | 1.41 | 32.68 | 1.29 | |
| Middle Finger | 32.67 * | 1.47 | 32.60 | 1.24 | |
| Ring Finger | 32.66 * | 1.46 | 32.77 | 1.32 | |
| Little Finger | 32.75 * | 1.42 | 32.73 | 1.40 | |
| Thenar Eminence | 32.51 | 1.40 | 32.37 | 1.35 | |
| Palm | 33.01 | 1.13 | 32.91 | 1.19 | |
| Wrist | 32.89 | 1.06 | 32.72 | 0.97 | |
| Athletes Group Pre Match | Thumb | 30.76 | 3.43 | 31.58 †† | 3.12 |
| Index | 30.34 | 3.74 | 31.09 | 4.00 | |
| Middle Finger | 29.04 | 4.22 | 30.77 † | 3.99 | |
| Ring Finger | 28.92 | 4.20 | 30.83 †† | 4.01 | |
| Little Finger | 29.81 | 4.27 | 30.78 | 4.14 | |
| Thenar Eminence | 32.11 | 1.97 | 32.47 † | 2.08 | |
| Palm | 31.68 | 2.45 | 32.26 † | 2.46 | |
| Wrist | 32.65 | 1.17 | 32.75 | 1.35 | |
| Athletes Group Post Match | Thumb | 32.7 # | 1.8 | 33.6 ## ††† | 1.8 |
| Index | 30.9 | 2.2 | 33.1 # †† | 1.8 | |
| Middle Finger | 30.5 | 2.4 | 32.5 # †† | 2.1 | |
| Ring Finger | 31.0 # | 2.5 | 32.9 # †† | 1.8 | |
| Little Finger | 32.6 # | 2.0 | 33.2 # † | 2.3 | |
| Thenar Eminence | 33.5 ## | 1.3 | 34.3 # †† | 1.0 | |
| Palm | 33.4 ## | 1.1 | 34.1 ## †† | 1.1 | |
| Wrist | 33.4 # | 1.1 | 33.8 ## †† | 1.3 | |
| Thumb | Index | Middle Finger | Ring Finger | Little Finger | Thenar Eminence | Palm | Wrist | ||
|---|---|---|---|---|---|---|---|---|---|
| % Hitting | Pearson Correlation | −0.285 | −0.137 | 0.003 | 0.051 | −0.069 | −0.056 | −0.330 | −0.152 |
| Bilateral Significance | 0.344 | 0.655 | 0.992 | 0.869 | 0.824 | 0.855 | 0.271 | 0.620 | |
| F Hitting | Pearson Correlation | −0.130 | −0.140 | 0.108 | −0.299 | −0.328 | −0.425 | −0.740 | −0.184 |
| Bilateral Significance | 0.673 | 0.648 | 0.725 | 0.321 | 0.274 | 0.148 | 0.004 ** | 0.547 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Jiménez, J.L.; Tejero-Pastor, R.; Calzadillas-Valles, M.d.C.; Jimenez-Perez, I.; Cibrián Ortiz de Anda, R.M.; Salvador-Palmer, R.; Priego-Quesada, J.I. Chronic and Acute Effects on Skin Temperature from a Sport Consisting of Repetitive Impacts from Hitting a Ball with the Hands. Sensors 2022, 22, 8572. https://doi.org/10.3390/s22218572
Sánchez-Jiménez JL, Tejero-Pastor R, Calzadillas-Valles MdC, Jimenez-Perez I, Cibrián Ortiz de Anda RM, Salvador-Palmer R, Priego-Quesada JI. Chronic and Acute Effects on Skin Temperature from a Sport Consisting of Repetitive Impacts from Hitting a Ball with the Hands. Sensors. 2022; 22(21):8572. https://doi.org/10.3390/s22218572
Chicago/Turabian StyleSánchez-Jiménez, Jose Luis, Robert Tejero-Pastor, María del Carmen Calzadillas-Valles, Irene Jimenez-Perez, Rosa Maria Cibrián Ortiz de Anda, Rosario Salvador-Palmer, and Jose Ignacio Priego-Quesada. 2022. "Chronic and Acute Effects on Skin Temperature from a Sport Consisting of Repetitive Impacts from Hitting a Ball with the Hands" Sensors 22, no. 21: 8572. https://doi.org/10.3390/s22218572