
Reliability and Validity of Inertial Sensor Assisted Reaction Time Measurement Tools among Healthy Young Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
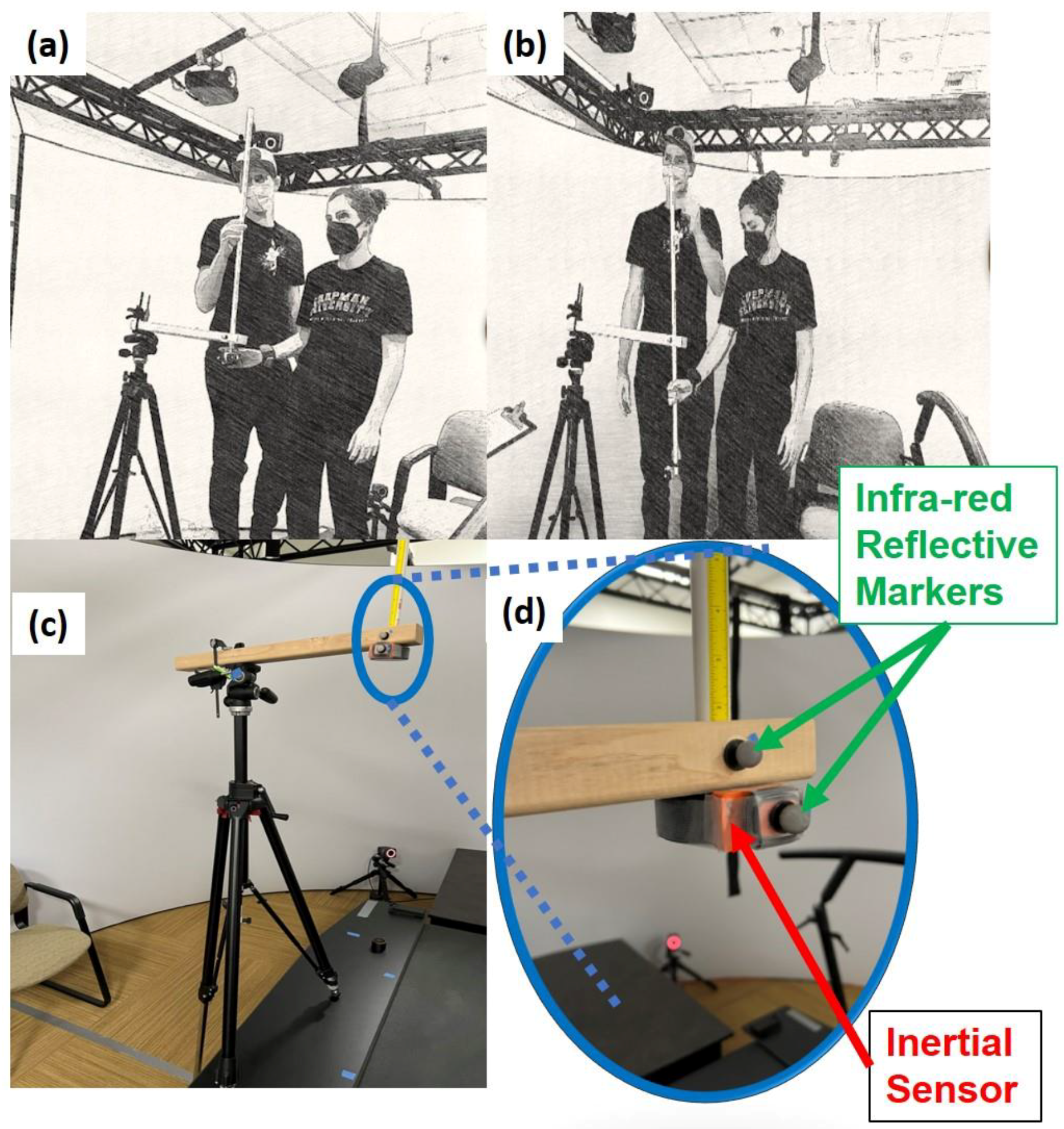
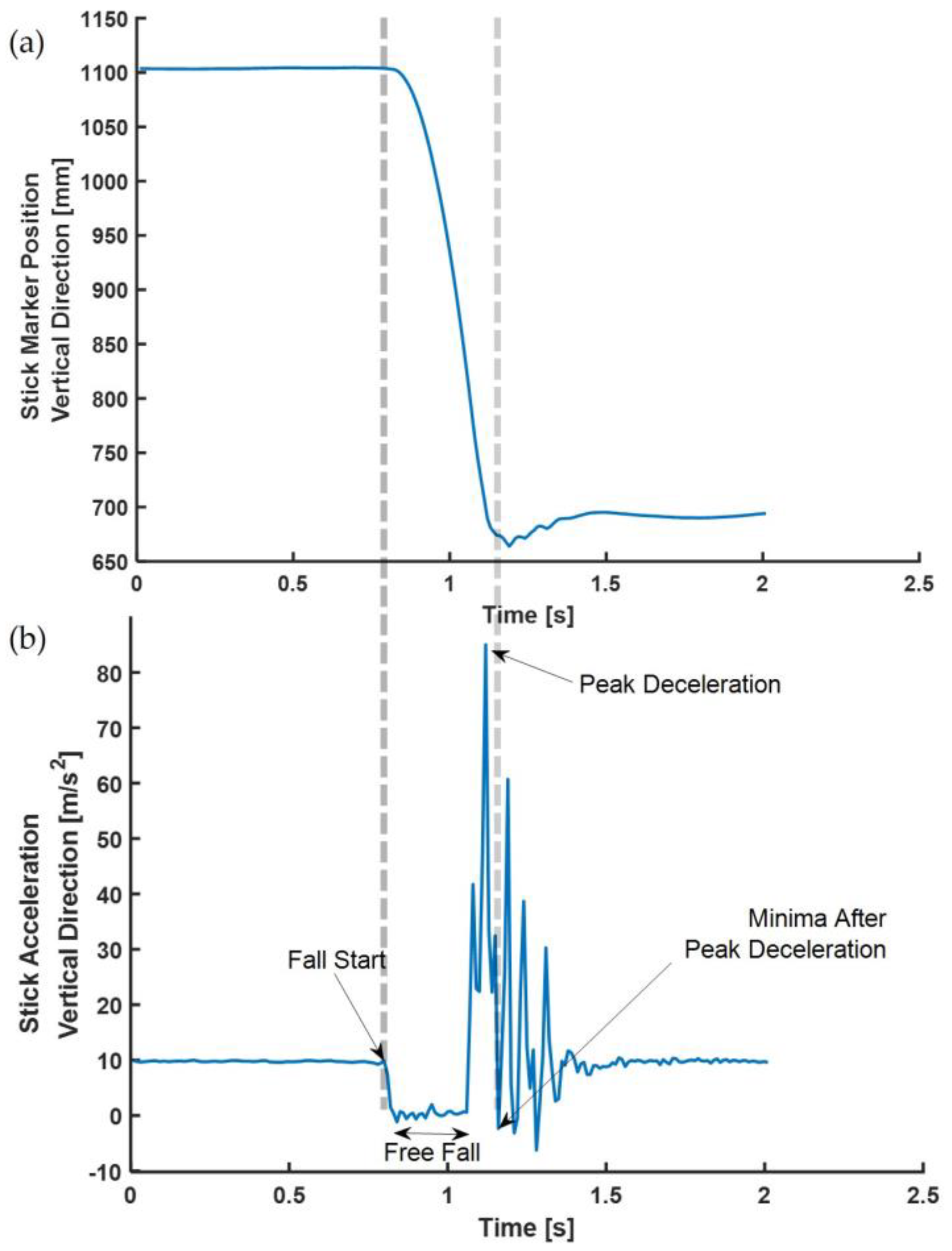
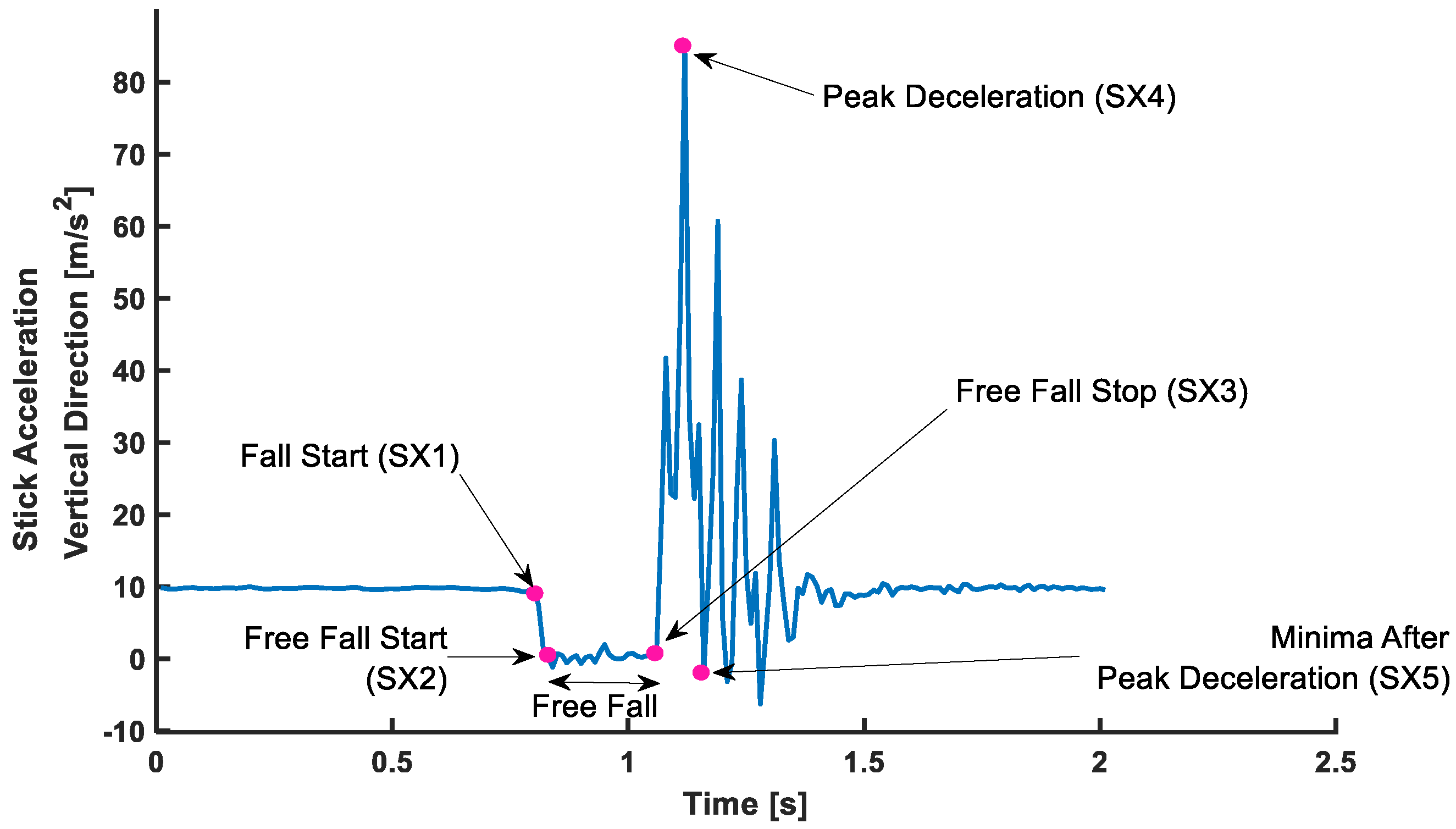
2.2.1. Drop-Stick Test System
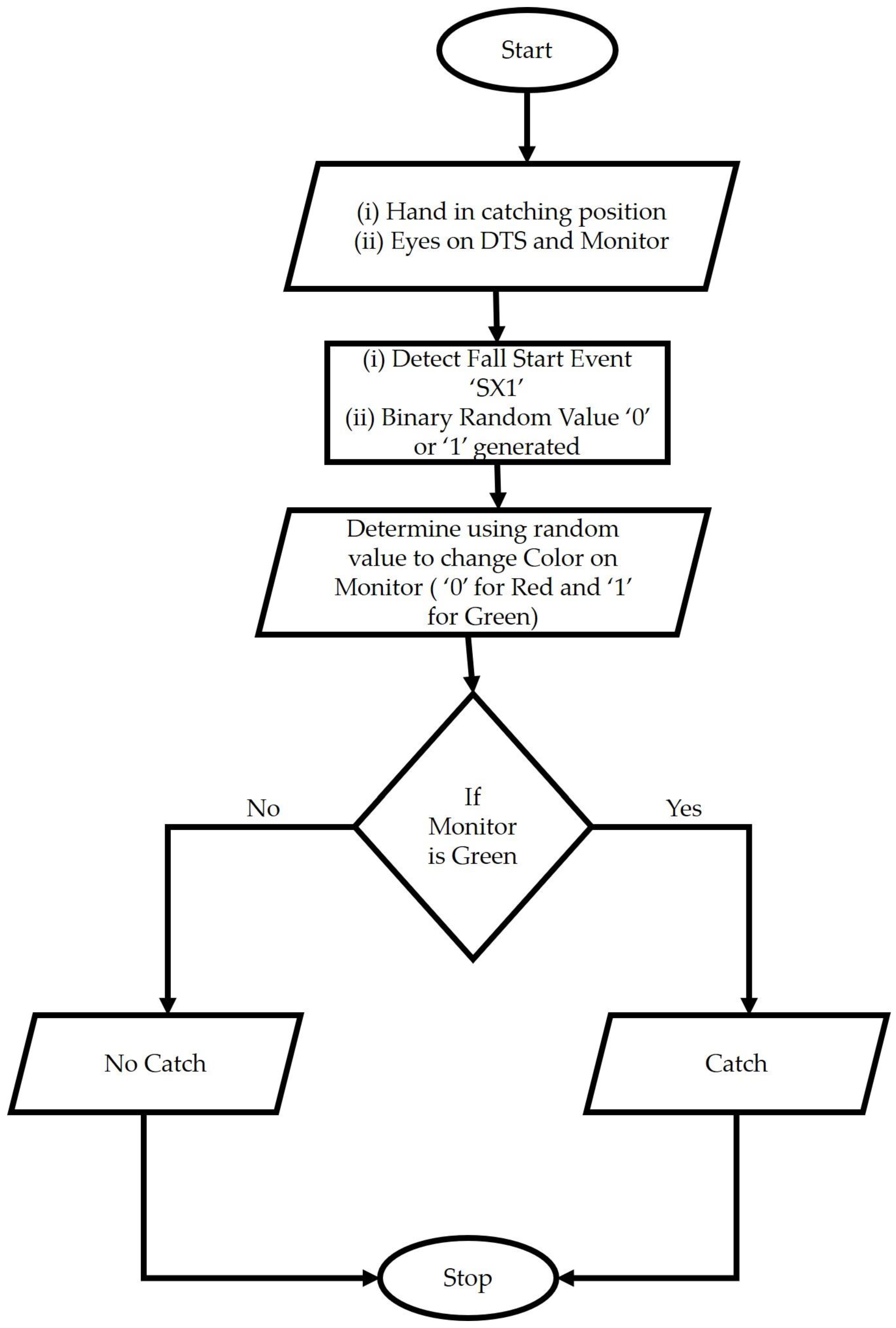
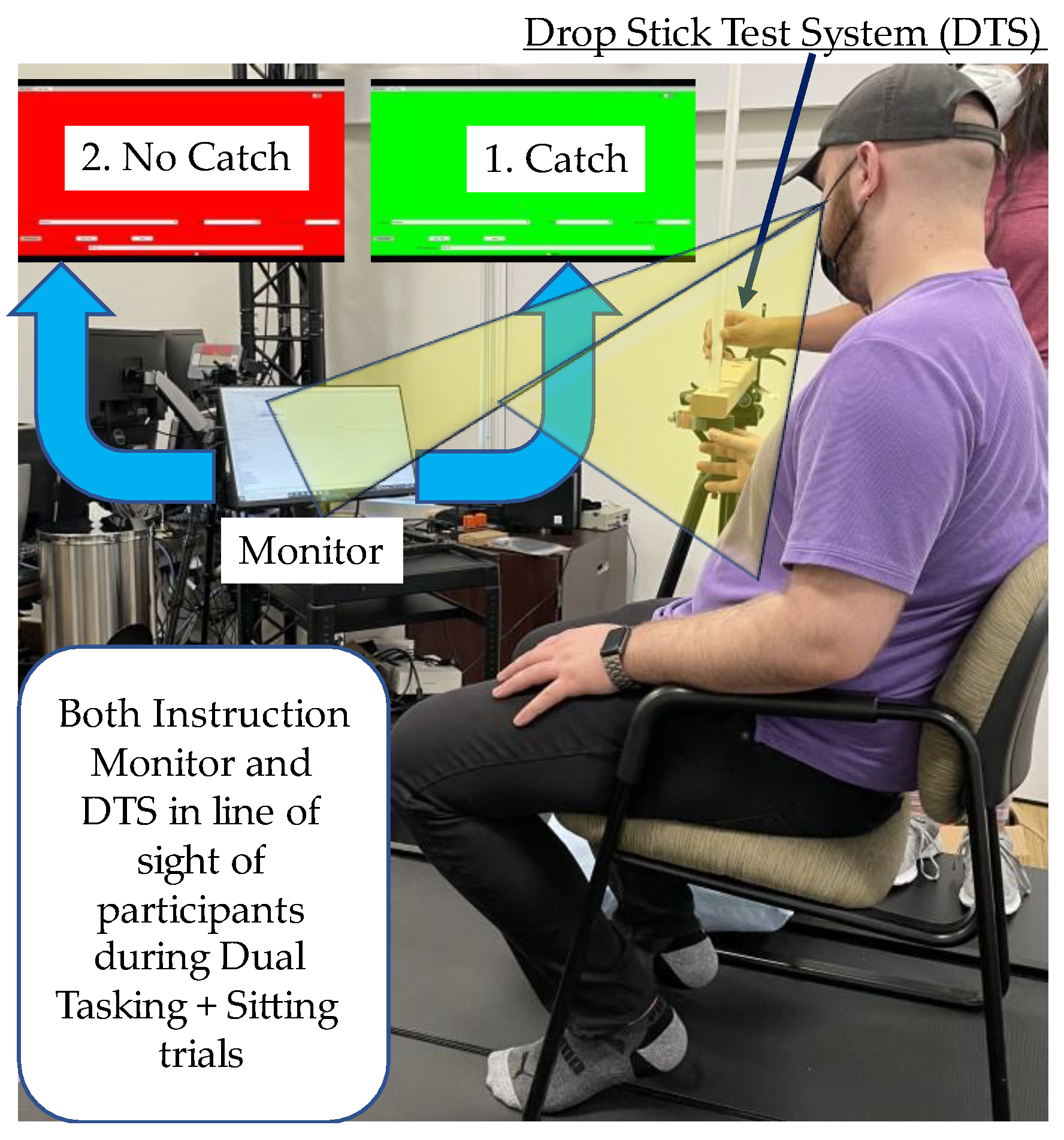
2.2.2. Dual Task Condition
2.3. Procedure and Protocol
2.3.1. Experimental Conditions
Single Task
Dual Task
Foam Stand
No Foam Stand
Sit
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mudric, M.; Cuk, I.; Nedeljkovic, A.; Jovanovic, S.; Jaric, S. Evaluation of Video-based method for the measurement of reaction time in specific sport situation. Int. J. Perform. Anal. Sport 2017, 15, 1077–1089. [Google Scholar] [CrossRef]
- Crabtree, D.A.; Antrim, L.R. Guidelines for measuring reaction time. Percept. Mot. Ski. 1988, 66, 363–370. [Google Scholar] [CrossRef] [PubMed]
- Donders, F.C. On the speed of mental processes. Acta Psychol. (Amst.) 1969, 30, 412–431. [Google Scholar] [CrossRef]
- Sternberg, S. Memory-scanning: Mental processes revealed by reaction-time experiments. Am. Sci. 1969, 57, 421–457. [Google Scholar] [PubMed]
- Friston, K.J.; Price, C.J.; Fletcher, P.; Moore, C.; Frackowiak, R.S.; Dolan, R.J. The trouble with cognitive subtraction. Neuroimage 1996, 4, 97–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanders, A.F. Elements of Human Performance: Reaction Processes and Attention in Human Skill; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1998. [Google Scholar]
- Lee, T.D.; Schmidt, R.A. Motor Control and Learning: A Behavioral Emphasis; Human Kinetics: Champaign, IL, USA, 2005. [Google Scholar]
- Polechoński, J.; Langer, A. Assessment of the Relevance and Reliability of Reaction Time Tests Performed in Immersive Virtual Reality by Mixed Martial Arts Fighters. Sensors 2022, 22, 4762. [Google Scholar] [CrossRef]
- Mirifar, A.; Luan, M.; Ehrlenspiel, F. Effects of unilateral dynamic handgrip on reaction time and error rate. Cogn. Process. 2022, 23, 169–178. [Google Scholar] [CrossRef]
- Sadler, C.M.; Peters, K.J.; Santangelo, C.M.; Maslovat, D.; Carlsen, A.N. Retrospective composite analysis of StartReact data indicates sex differences in simple reaction time are not attributable to response preparation. Behav. Brain Res. 2022, 426, 113839. [Google Scholar] [CrossRef]
- Reicker, L.; Tombaugh, T.; Walker, L.; Freedman, M. Reaction time: An alternative method for assessing the effects of multiple sclerosis on information processing speed. Arch. Clin. Neuropsychol. 2007, 22, 655–664. [Google Scholar] [CrossRef] [Green Version]
- Klimesch, W.; Doppelmayr, M.; Schimke, H.; Pachinger, T. Alpha Frequency, Reaction Time, and the Speed of Processing Information. J. Clin. Neurophysiol. 1996, 13, 511–518. [Google Scholar] [CrossRef]
- Wong, A.L.; Goldsmith, J.; Forrence, A.D.; Haith, A.M.; Krakauer, J.W. Reaction times can reflect habits rather than computations. eLife 2017, 6, e28075. [Google Scholar] [CrossRef] [PubMed]
- Erlanger, D.; Saliba, E.; Barth, J.; Almquist, J.; Webright, W.; Freeman, J. Monitoring Resolution of Postconcussion Symptoms in Athletes: Preliminary Results of a Web-Based Neuropsychological Test Protocol. J. Athl. Train. 2001, 36, 280–287. [Google Scholar]
- Harpham, J.A.; Mihalik, J.P.; Littleton, A.C.; Frank, B.S.; Guskiewicz, K.M. The Effect of Visual and Sensory Performance on Head Impact Biomechanics in College Football Players. Ann. Biomed. Eng. 2013, 42, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mihalik, J.P.; Blackburn, J.T.; Greenwald, R.M.; Cantu, R.C.; Marshall, S.W.; Guskiewicz, K.M. Collision type and player anticipation affect head impact severity among youth ice hockey players. Pediatrics 2010, 125, e1394–e1401. [Google Scholar] [CrossRef] [PubMed]
- Eckner, J.T.; Lipps, D.B.; Kim, H.; Richardson, J.K.; Ashton-Miller, J.A. Can a clinical test of reaction time predict a functional head-protective response? Med. Sci. Sport Exerc. 2011, 43, 382–387. [Google Scholar] [CrossRef] [Green Version]
- Honda, J.; Chang, S.H.; Kim, K. The effects of vision training, neck musculature strength, and reaction time on concussions in an athletic population. J. Exerc. Rehabil. 2018, 14, 706–712. [Google Scholar] [CrossRef]
- Blackwell, C.; Cary, K.; Holst, K.; Mandle, K.; Dryg, L.; Clemens, S.; Lemke, J.H.; Castro, S.; Hendricks, E.; Kelly, R. Dynavision Normative Data for Healthy Adults: Reaction Test Program. Am. J. Occup. 2020, 74, 7401185060p1–7401185060p6. [Google Scholar] [CrossRef]
- Soangra, R.; Lockhart, T. Smartphone-Based Prediction Model for Postoperative Cardiac Surgery Outcomes Using Preoperative Gait and Posture Measures. Sensors 2021, 21, 1704. [Google Scholar] [CrossRef]
- Soangra, R.; Lockhart, T.E. Inertial Sensor-Based Variables Are Indicators of Frailty and Adverse Post-Operative Outcomes in Cardiovascular Disease Patients. Sensors 2018, 18, 1792. [Google Scholar] [CrossRef] [Green Version]
- Soangra, R.; Lockhart, T.E. Agreement in gait speed from smartphone and stopwatch for five meter walk in laboratory and clinical environments. Biomed. Sci. Instrum. 2014, 50, 254–264. [Google Scholar]
- Soangra, R.; Lockhart, T.E.; Frames, C.W.; Zhang, J.; Moon, S.H.; Park, J. Potential for using Smartphone Accelerometers in Non-laboratory Environments. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2014, 58, 1672–1675. [Google Scholar] [CrossRef] [Green Version]
- Mercer, V.S.; Hankins, C.C.; Spinks, A.J.; Tedder, D.D. Reliability and validity of a clinical test of reaction time in older adults. J. Geriatr. Phys. 2009, 32, 103–110. [Google Scholar] [CrossRef] [PubMed]
- Eckner, J.T.; Whitacre, R.D.; Kirsch, N.L.; Richardson, J.K. Evaluating a Clinical Measure of Reaction Time: An Observational Study. Percept. Mot. Ski. 2009, 108, 717–720. [Google Scholar] [CrossRef]
- Eckner, J.T.; Kutcher, J.S.; Broglio, S.P.; Richardson, J.K. Effect of sport-related concussion on clinically measured simple reaction time. Br. J. Sport Med. 2014, 48, 112–118. [Google Scholar] [CrossRef] [Green Version]
- Eckner, J.T.; Kutcher, J.S.; Richardson, J.K. Pilot evaluation of a novel clinical test of reaction time in national collegiate athletic association division I football players. J. Athl. Train. 2010, 45, 327–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckner, J.T.; Richardson, J.K.; Kim, H.; Joshi, M.S.; Oh, Y.K.; Ashton-Miller, J.A. Reliability and Criterion Validity of a Novel Clinical Test of Simple and Complex Reaction Time in Athletes. Percept. Mot. Ski. 2015, 120, 841–859. [Google Scholar] [CrossRef] [Green Version]
- MacDonald, J.; Wilson, J.; Young, J.; Duerson, D.; Swisher, G.; Collins, C.L.; Meehan, W.P., 3rd. Evaluation of a simple test of reaction time for baseline concussion testing in a population of high school athletes. Clin. J. Sport Med. 2015, 25, 43–48. [Google Scholar] [CrossRef]
- Fritz, N.E.; Cheek, F.M.; Nichols-Larsen, D.S. Motor-Cognitive Dual-Task Training in Persons With Neurologic Disorders: A Systematic Review. J. Neurol. Phys. 2015, 39, 142–153. [Google Scholar] [CrossRef] [Green Version]
- Amboni, M.; Barone, P.; Hausdorff, J.M. Cognitive contributions to gait and falls: Evidence and implications. Mov. Disord. 2013, 28, 1520–1533. [Google Scholar] [CrossRef]
- Montero-Odasso, M.; Bherer, L.; Studenski, S.; Gopaul, K.; Oteng-Amoako, A.; Woolmore-Goodwin, S.; Stoole, P.; Wells, J.; Doherty, T.; Zecevic, A.A.; et al. Mobility and Cognition in Seniors. Report from the 2008 Institute of Aging (CIHR) Mobility and Cognition Workshop. Can. Geriatr. J. 2015, 18, 159–167. [Google Scholar] [CrossRef]
- Rosano, C.; Brach, J.; Studenski, S.; Longstreth, W.T., Jr.; Newman, A.B. Gait variability is associated with subclinical brain vascular abnormalities in high-functioning older adults. Neuroepidemiology 2007, 29, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavanaugh, J.T.; Guskiewicz, K.M.; Giuliani, C.; Marshall, S.; Mercer, V.; Stergiou, N. Detecting altered postural control after cerebral concussion in athletes with normal postural stability. Br. J. Sport Med. 2005, 39, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Lord, S.; Galna, B.; Rochester, L. Moving forward on gait measurement: Toward a more refined approach. Mov. Disord. 2013, 28, 1534–1543. [Google Scholar] [CrossRef]
- Lord, S.; Galna, B.; Verghese, J.; Coleman, S.; Burn, D.; Rochester, L. Independent domains of gait in older adults and associated motor and nonmotor attributes: Validation of a factor analysis approach. J. Gerontol. A Biol. Sci. Med. Sci. 2013, 68, 820–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiang, C.; Liu, C.; Hao, C.; Wang, Z.; Che, L.; Zhou, X. A self-powered acceleration sensor with flexible materials based on triboelectric effect. Nano. Energy 2017, 31, 469–477. [Google Scholar] [CrossRef]
- Liu, C.; Fang, L.; Zou, H.; Wang, Y.; Chi, J.; Che, L.; Zhou, X.; Wang, Z.; Wang, T.; Dong, L.; et al. Theoretical investigation and experimental verification of the self-powered acceleration sensor based on triboelectric nanogenerators (TENGs). Extrem. Mech. Lett. 2021, 42, 101021. [Google Scholar] [CrossRef]
- Galetta, K.M.; Liu, M.; Leong, D.F.; Ventura, R.E.; Galetta, S.L.; Balcer, L.J. The King-Devick test of rapid number naming for concussion detection: Meta-analysis and systematic review of the literature. Concussion 2016, 1. [Google Scholar] [CrossRef] [Green Version]
- Aron, A.; Harper, B.; Andrews, R.; Boggs, E.; Stanley, A. The Effect of Whole-Body Fatigue on King-Devick Test and Balance. Res. Q Exerc. Sport 2021, 1–7. [Google Scholar] [CrossRef]
- Galetta, K.M.; Morganroth, J.; Moehringer, N.; Mueller, B.; Hasanaj, L.; Webb, N.; Civitano, C.; Cardone, D.A.; Silverio, A.; Galetta, S.L.; et al. Adding Vision to Concussion Testing: A Prospective Study of Sideline Testing in Youth and Collegiate Athletes. J. Neuroophthalmol. 2015, 35, 235–241. [Google Scholar] [CrossRef]
- Marinides, Z.; Galetta, K.M.; Andrews, C.N.; Wilson, J.A.; Herman, D.C.; Robinson, C.D.; Smith, M.S.; Bentley, B.C.; Galetta, S.L.; Balcer, L.J.; et al. Vision testing is additive to the sideline assessment of sports-related concussion. Neurol. Clin. Pract. 2015, 5, 25–34. [Google Scholar] [CrossRef] [Green Version]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 2016, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Ludbrook, J. Confidence in Altman-Bland plots: A critical review of the method of differences. Clin. Exp. Pharmacol. Physiol. 2010, 37, 143–149. [Google Scholar] [CrossRef]
- Trinidad-Fernandez, M.; Beckwee, D.; Cuesta-Vargas, A.; Gonzalez-Sanchez, M.; Moreno, F.A.; Gonzalez-Jimenez, J.; Joos, E.; Vaes, P. Validation, Reliability, and Responsiveness Outcomes of Kinematic Assessment with An RGB-D Camera to Analyze Movement in Subacute and Chronic Low Back Pain. Sensors 2020, 20, 689. [Google Scholar] [CrossRef] [Green Version]
- Harper, B.; Aron, A.; John, E. The Role of Pre-Season Health Characteristics As Injury Risk Factors in Female Adolescent Soccer Players. J. Phys. Ther. Sci. 2021, 33, 429–443. [Google Scholar] [CrossRef] [PubMed]
- Lempke, L.B.; Johnson, R.S.; Schmidt, J.D.; Lynall, R.C. Clinical versus Functional Reaction Time: Implications for Postconcussion Management. Med. Sci. Sport Exerc. 2020, 52, 1650–1657. [Google Scholar] [CrossRef]
- Soangra, R.; Lockhart, T.E. A comparative study for performance evaluation of sit-to-stand task with body worn sensor and existing laboratory methods. Biomed. Sci. Instrum. 2012, 48, 407–414. [Google Scholar] [PubMed]
- Soangra, R.; Lockhart, T.E.; Lach, J.; Abdel-Rahman, E.M. Effects of hemodialysis therapy on sit-to-walk characteristics in end stage renal disease patients. Ann. Biomed. Eng. 2013, 41, 795–805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spierer, D.K.; Petersen, R.A.; Duffy, K.; Corcoran, B.M.; Rawls-Martin, T. Gender influence on response time to sensory stimuli. J. Strength Cond. Res. 2010, 24, 957–963. [Google Scholar] [CrossRef]
- Jha, R.K.; Thapa, S.; Kasti, R.; Nepal, O. Influence of Body Mass Index, Handedness and Gender on Ruler Drop Method Reaction Time among Adults. J. Nepal. Health Res. Counc. 2020, 18, 108–111. [Google Scholar] [CrossRef]
- Lynall, R.C.; Johnson, R.S.; Lempke, L.B.; Schmidt, J.D. Test-Retest Reliability of a Functional Reaction Time Assessment Battery. J. Sport Rehabil. 2021, 30, 1237–1241. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, G.B.; Nabhan, D.C.; Prusmack, C.J.; Moreau, W.J. Detection of Persisting Concussion Effects on Neuromechanical Responsiveness. Med. Sci. Sport Exerc. 2018, 50, 1750–1756. [Google Scholar] [CrossRef] [PubMed]
- Del Rossi, G. Evaluating the Recovery Curve for Clinically Assessed Reaction Time After Concussion. J. Athl. Train. 2017, 52, 766–770. [Google Scholar] [CrossRef] [Green Version]
- Lempke, L.B.; Howell, D.R.; Eckner, J.T.; Lynall, R.C. Examination of Reaction Time Deficits Following Concussion: A Systematic Review and Meta-analysis. Sport Med. 2020, 50, 1341–1359. [Google Scholar] [CrossRef] [PubMed]
- Wilkerson, G.B.; Grooms, D.R.; Acocello, S.N. Neuromechanical Considerations for Postconcussion Musculoskeletal Injury Risk Management. Curr. Sport Med. Rep. 2017, 16, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Gessel, L.M.; Fields, S.K.; Collins, C.L.; Dick, R.W.; Comstock, R.D. Concussions among United States high school and collegiate athletes. J. Athl. Train. 2007, 42, 495–503. [Google Scholar] [PubMed]
- Subotic, A.; Ting, W.K.; Cusimano, M.D. Characteristics of the King-Devick test in the assessment of concussed patients in the subacute and later stages after injury. PLoS ONE 2017, 12, e0183092. [Google Scholar]
- Clugston, J.R.; Chrisman, S.P.D.; Houck, Z.M.; Asken, B.M.; Boone, J.K.; Buckley, T.A.; Hoffman, N.L.; Schmidt, J.D.; Kontos, A.P.; Jaffee, M.S.; et al. King-Devick Test Time Varies by Testing Modality. Clin. J. Sport Med. 2020, 30, e139–e142. [Google Scholar] [CrossRef]
- Nguyen, M.Q.; King, D.; Pearce, A.J. A Reliability and Comparative Analysis of the New Randomized King-Devick Test. J. Neuroophthalmol. 2020, 40, 207–212. [Google Scholar] [CrossRef]
- Eckner, J.T.; Richardson, J.K.; Kim, H.; Lipps, D.B.; Ashton-Miller, J.A. A novel clinical test of recognition reaction time in healthy adults. Psychol. Assess. 2012, 24, 249–254. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Consistency | Absolute Agreement | ||||
|---|---|---|---|---|---|---|
| ICC | ICC Confidence Interval 95% | ICC | ICC Confidence Interval 95% | Datapoints | Pearson Correlation Coefficient | |
| Overall | 0.82 | [0.78 to 0.85] | 0.71 | [0.14 to 0.86] | 480 | 0.69 |
| Standing | 0.78 | [0.71 to 0.83] | 0.66 | [0.10 to 0.84] | 190 | 0.64 |
| Sitting | 0.70 | [0.56 to 0.80] | 0.57 | [0.02 to 0.78] | 100 | 0.55 |
| Single Task | 0.79 | [0.75 to 0.83] | 0.65 | [−0.03 to 0.84] | 370 | 0.66 |
| Dual Task | 0.75 | [0.64 to 0.83] | 0.69 | [0.42 to 0.82] | 110 | 0.61 |
| Foam Standing | 0.88 | [0.84 to 0.91] | 0.79 | [0.18 to 0.91] | 190 | 0.79 |
| Firm Standing | 0.78 | [0.71 to 0.83] | 0.66 | [0.10 to 0.84] | 190 | 0.64 |
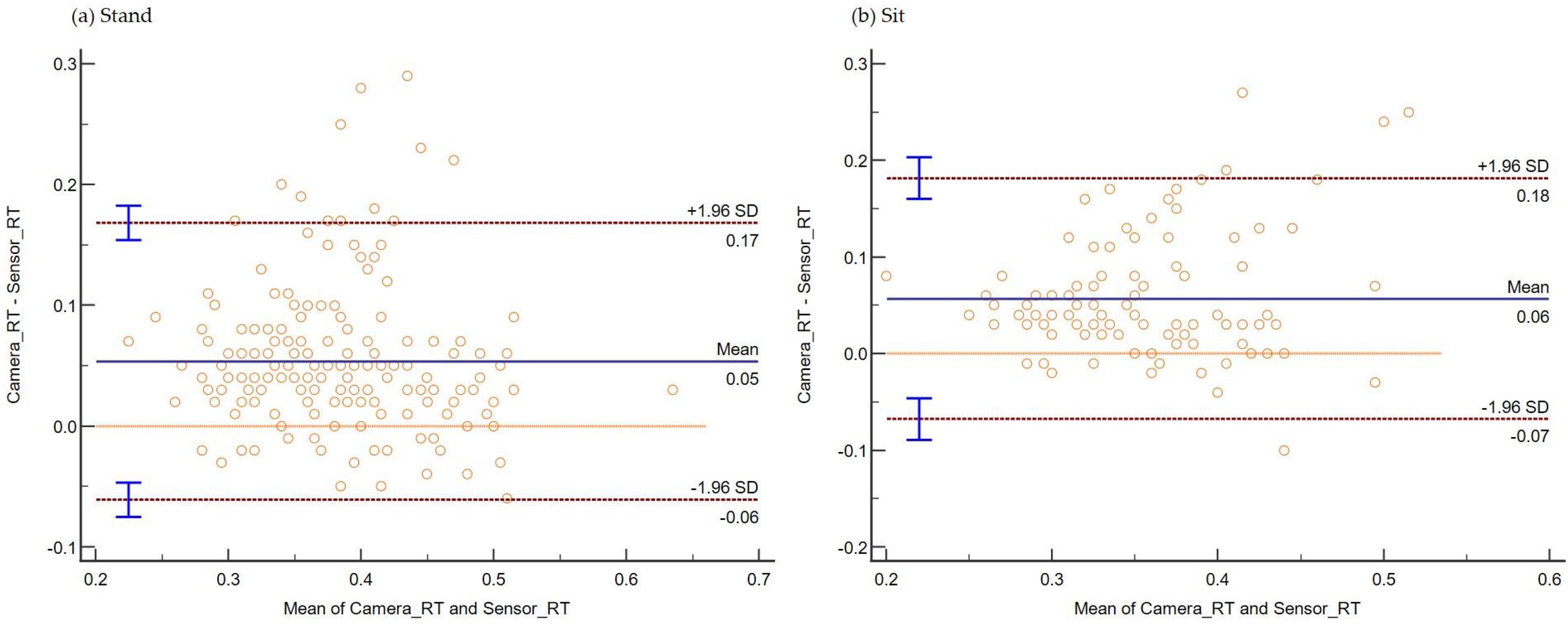
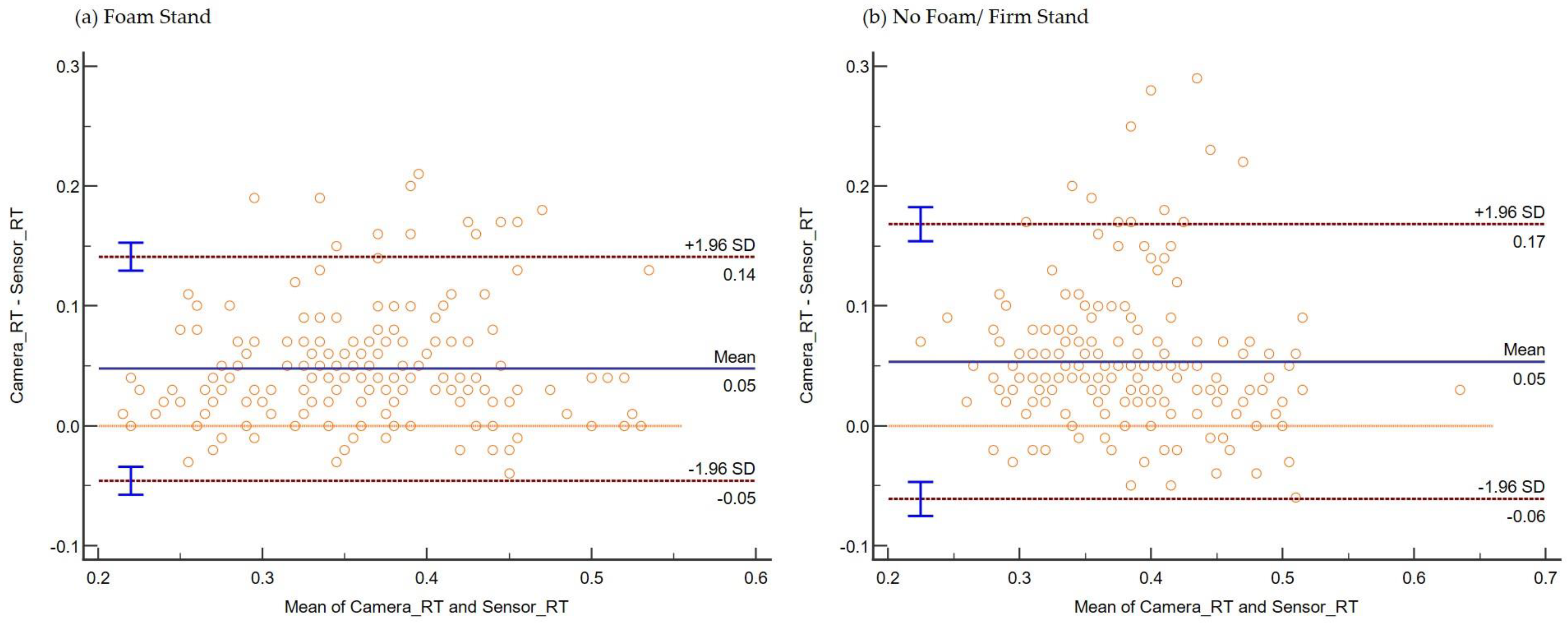
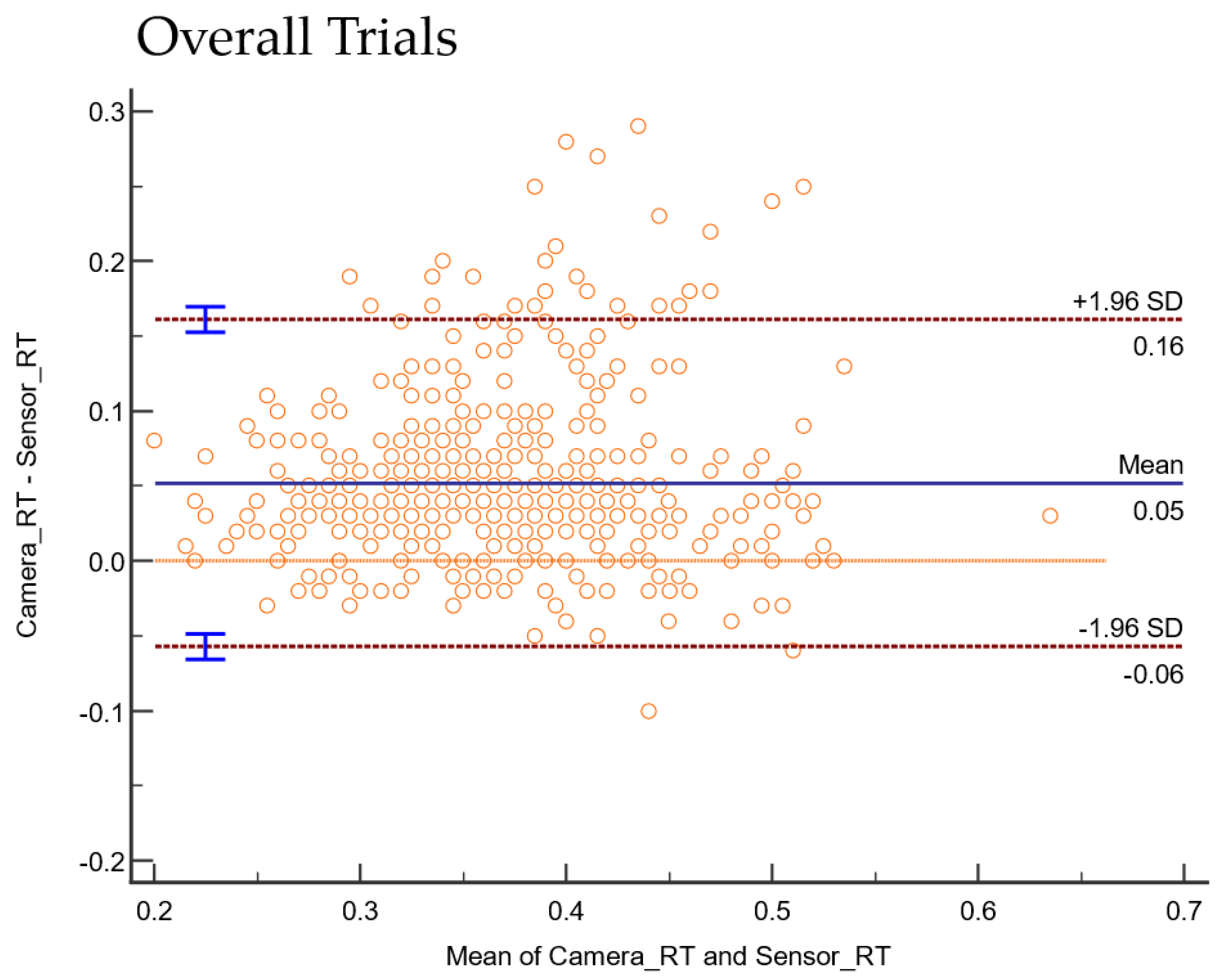
| Condition | Bias | 95% CI bias | Lower LOA | 95% CI of Lower LOA | Upper LOA | 95% CI of Upper LOA |
|---|---|---|---|---|---|---|
| Overall | 0.05 | [0.04 to 0.05] | −0.05 | [−0.06 to −0.04] | 0.16 | [0.15 to 0.16] |
| Standing | 0.05 | [0.04 to 0.06] | −0.06 | [−0.07 to −0.04] | 0.16 | [0.15 to 0.18] |
| Sitting | 0.05 | [0.04 to 0.06] | −0.06 | [−0.08 to −0.04] | 0.18 | [0.16 to 0.20] |
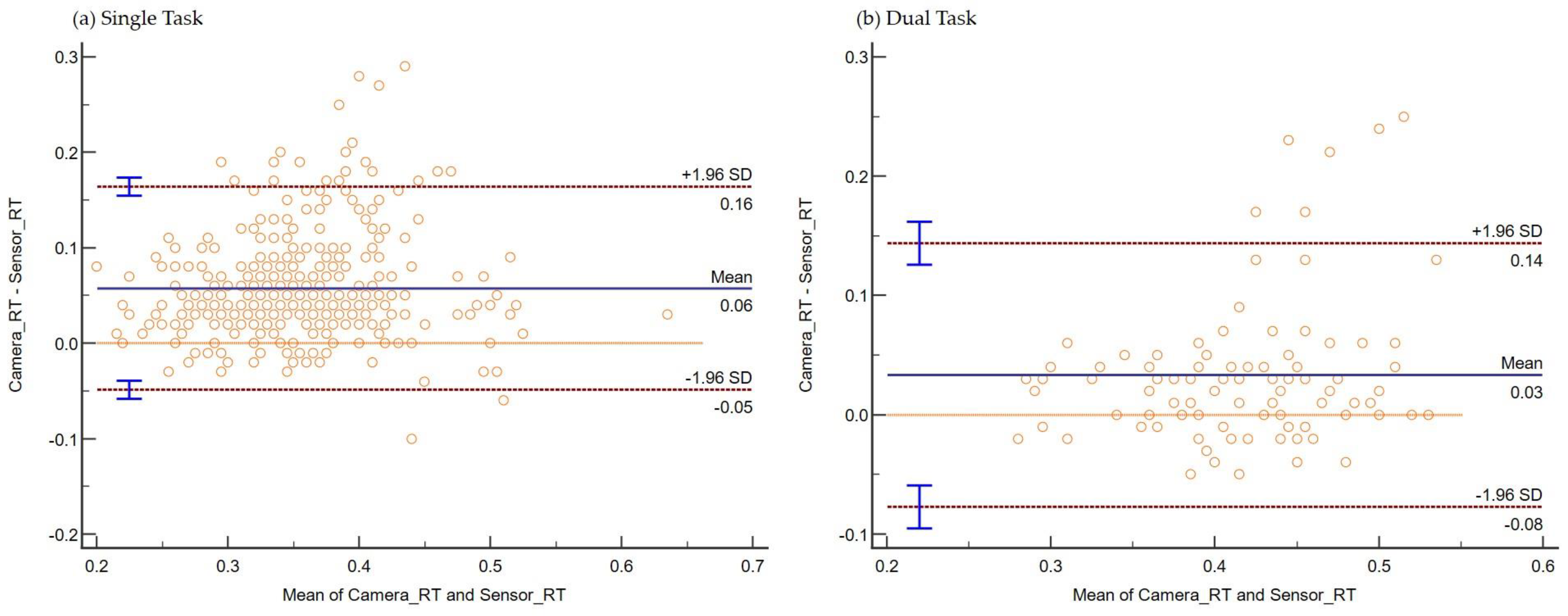
| Single Task | 0.05 | [0.05 to 0.06] | −0.04 | [−0.05 to −0.03] | 0.16 | [0.15 to 0.17] |
| Dual Task | 0.03 | [0.02 to 0.04] | −0.07 | [−0.09 to −0.05] | 0.14 | [0.12 to 0.16] |
| Foam Standing | 0.04 | [0.04 to 0.05] | −0.04 | [−0.05 to −0.03] | 0.14 | [0.12 to 0.15] |
| No Foam Standing | 0.05 | [0.04 to 0.06] | −0.06 | [−0.07 to −0.04] | 0.16 | [0.15 to 0.18] |
| Time Interval (SX1-SX2) | Time Interval (SX1-SX3) | Time Interval (SX1-SX4) | Time Interval (SX1-SX5) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Condition | Task | Mean | SD | SE | Mean | SD | SE | Mean | SD | SE | Mean | SD | SE |
| Foam Stand | Dual Task | 0.047 | 0.021 | 0.003 | 0.341 | 0.055 | 0.008 | 0.410 | 0.058 | 0.009 | 0.547 | 0.103 | 0.016 |
| Foam Stand | Single Task | 0.060 | 0.025 | 0.002 | 0.231 | 0.055 | 0.005 | 0.315 | 0.061 | 0.005 | 0.430 | 0.112 | 0.009 |
| Sit | Dual Task | 0.057 | 0.040 | 0.009 | 0.308 | 0.049 | 0.011 | 0.368 | 0.041 | 0.009 | 0.462 | 0.044 | 0.010 |
| Sit | Single Task | 0.057 | 0.030 | 0.003 | 0.233 | 0.052 | 0.006 | 0.317 | 0.061 | 0.007 | 0.404 | 0.083 | 0.009 |
| Stand | Dual Task | 0.057 | 0.032 | 0.005 | 0.332 | 0.065 | 0.009 | 0.404 | 0.060 | 0.008 | 0.535 | 0.098 | 0.014 |
| Stand | Single Task | 0.063 | 0.025 | 0.002 | 0.240 | 0.057 | 0.005 | 0.332 | 0.065 | 0.005 | 0.443 | 0.135 | 0.011 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harper, B.; Shiraishi, M.; Soangra, R. Reliability and Validity of Inertial Sensor Assisted Reaction Time Measurement Tools among Healthy Young Adults. Sensors 2022, 22, 8555. https://doi.org/10.3390/s22218555
Harper B, Shiraishi M, Soangra R. Reliability and Validity of Inertial Sensor Assisted Reaction Time Measurement Tools among Healthy Young Adults. Sensors. 2022; 22(21):8555. https://doi.org/10.3390/s22218555
Chicago/Turabian StyleHarper, Brent, Michael Shiraishi, and Rahul Soangra. 2022. "Reliability and Validity of Inertial Sensor Assisted Reaction Time Measurement Tools among Healthy Young Adults" Sensors 22, no. 21: 8555. https://doi.org/10.3390/s22218555