
Noninvasive Detection of Bacterial Infection in Children Using Piezoelectric E-Nose

Abstract
:1. Introduction
2. Materials and Methods
2.1. Collection of Biosamples and Study Design
2.1.1. Urine Sample Analysis
2.1.2. Biomaterial Analysis
2.2. Analysis of Volatile Compounds
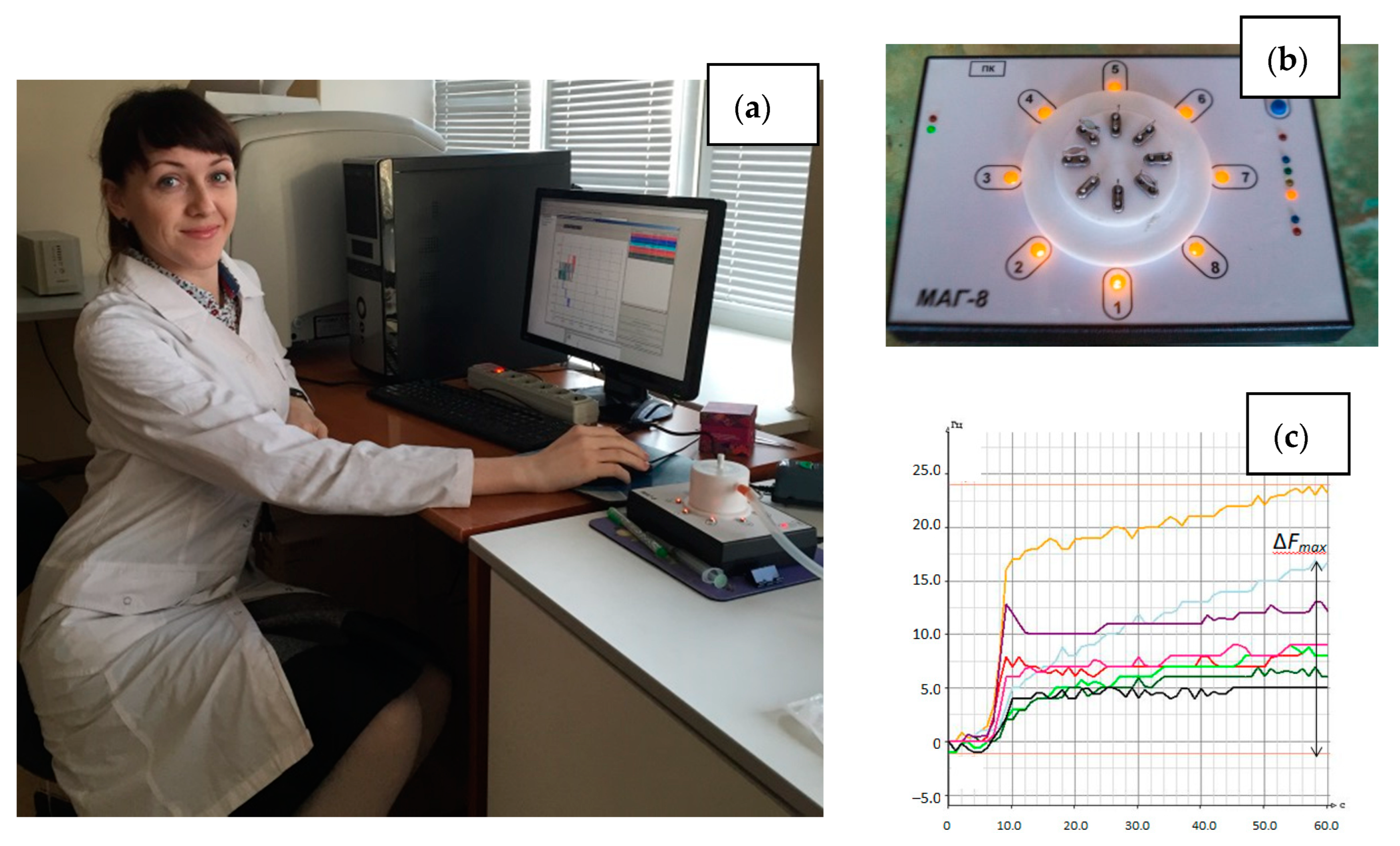
2.2.1. Device and Sensor Array
2.2.2. Technique of Measurement
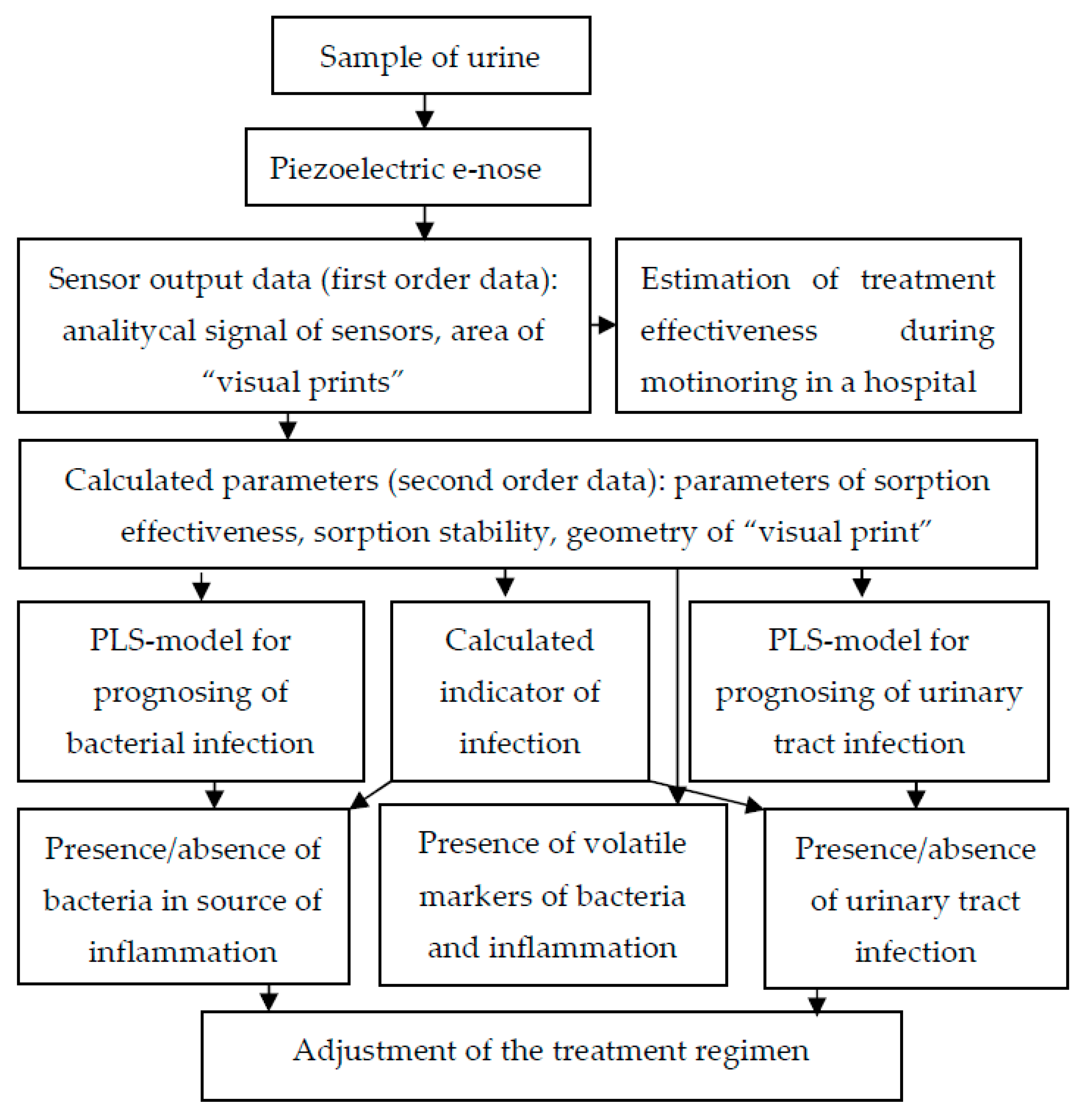
2.2.3. Sensor Data Processing
3. Results
3.1. The Results of the General Analysis of Urine and Bacteriological Culture
3.2. The Results of the Identification of Volatile Substances in the Equilibrium Gas Phase of Urine Samples
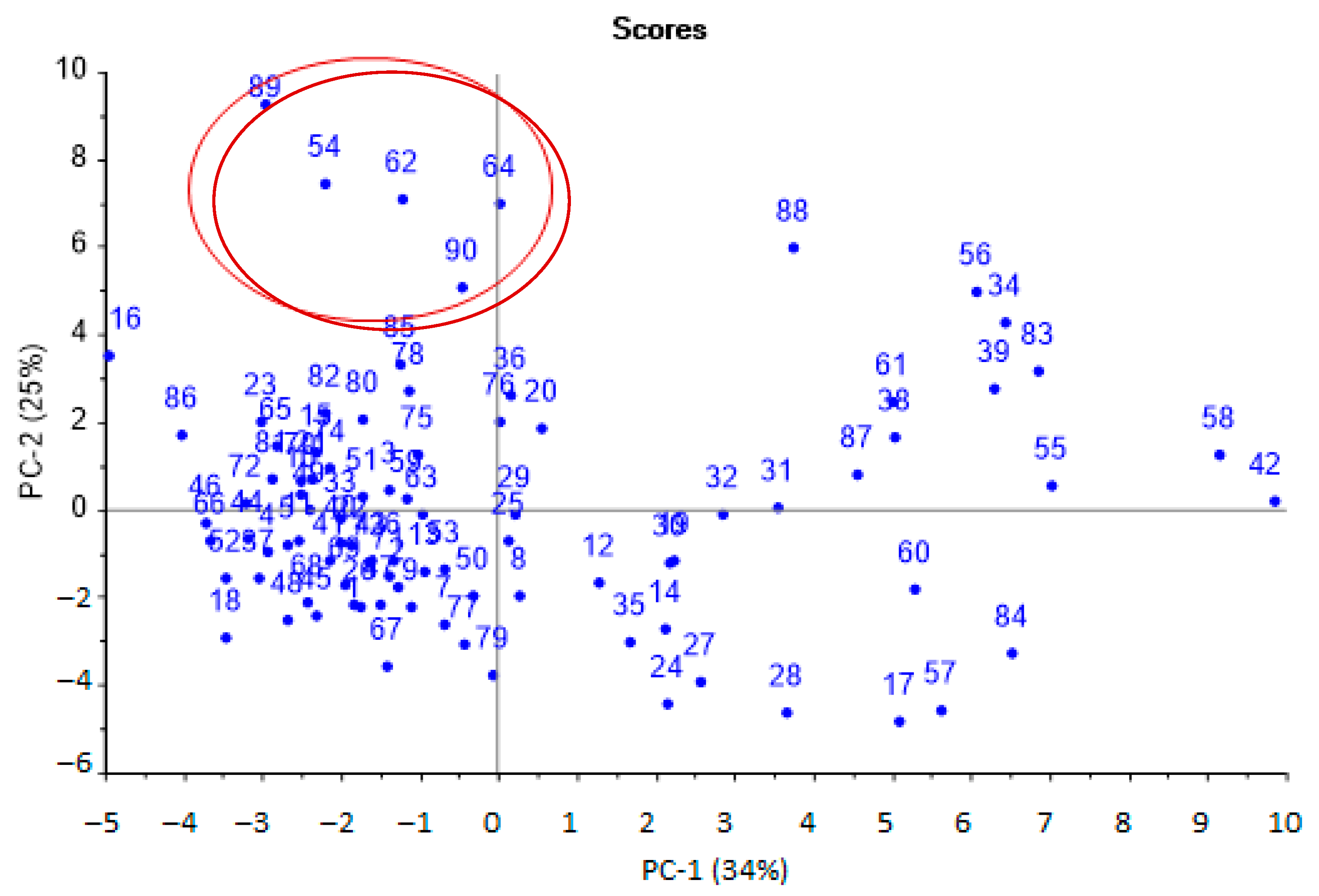
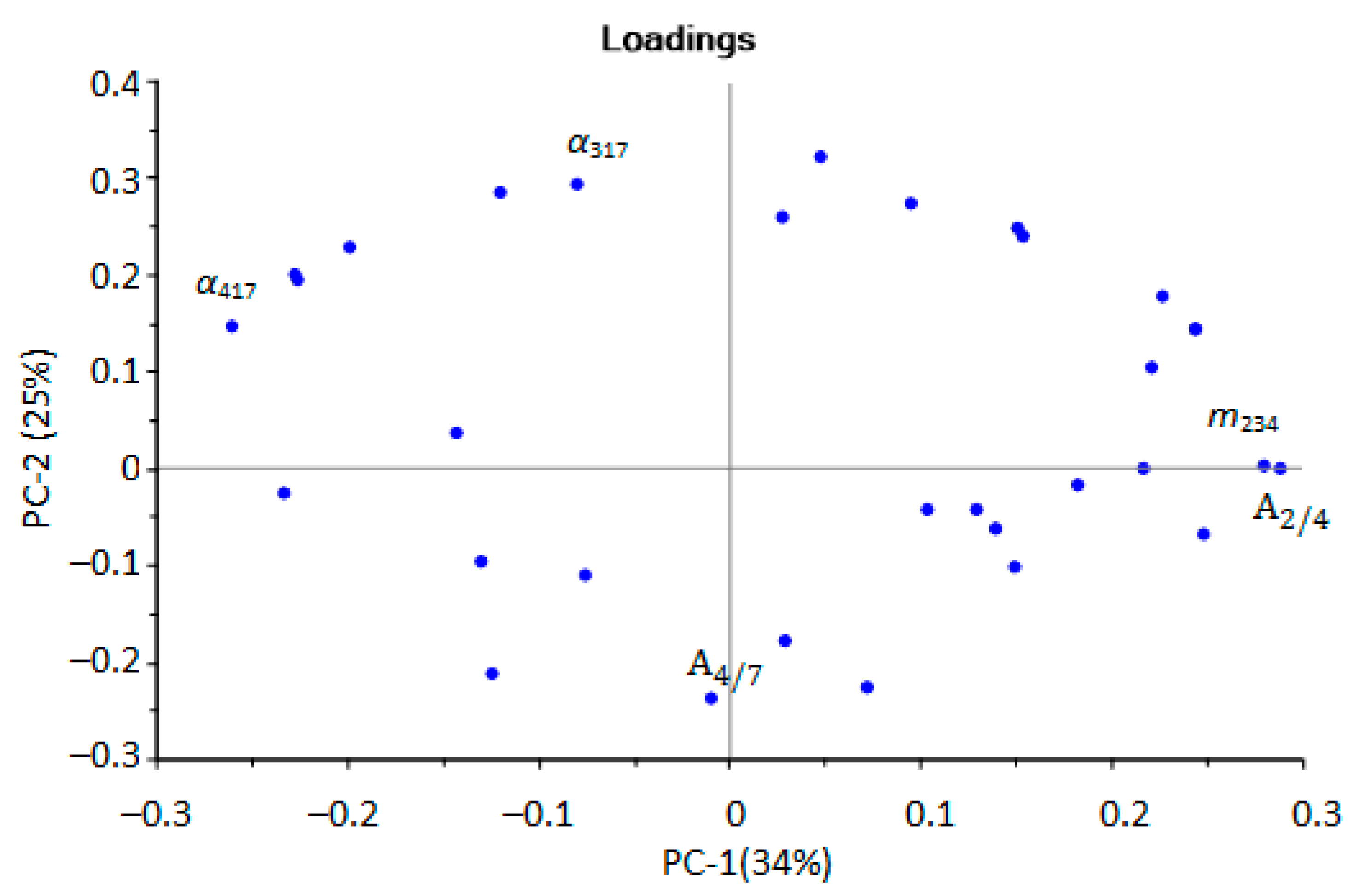
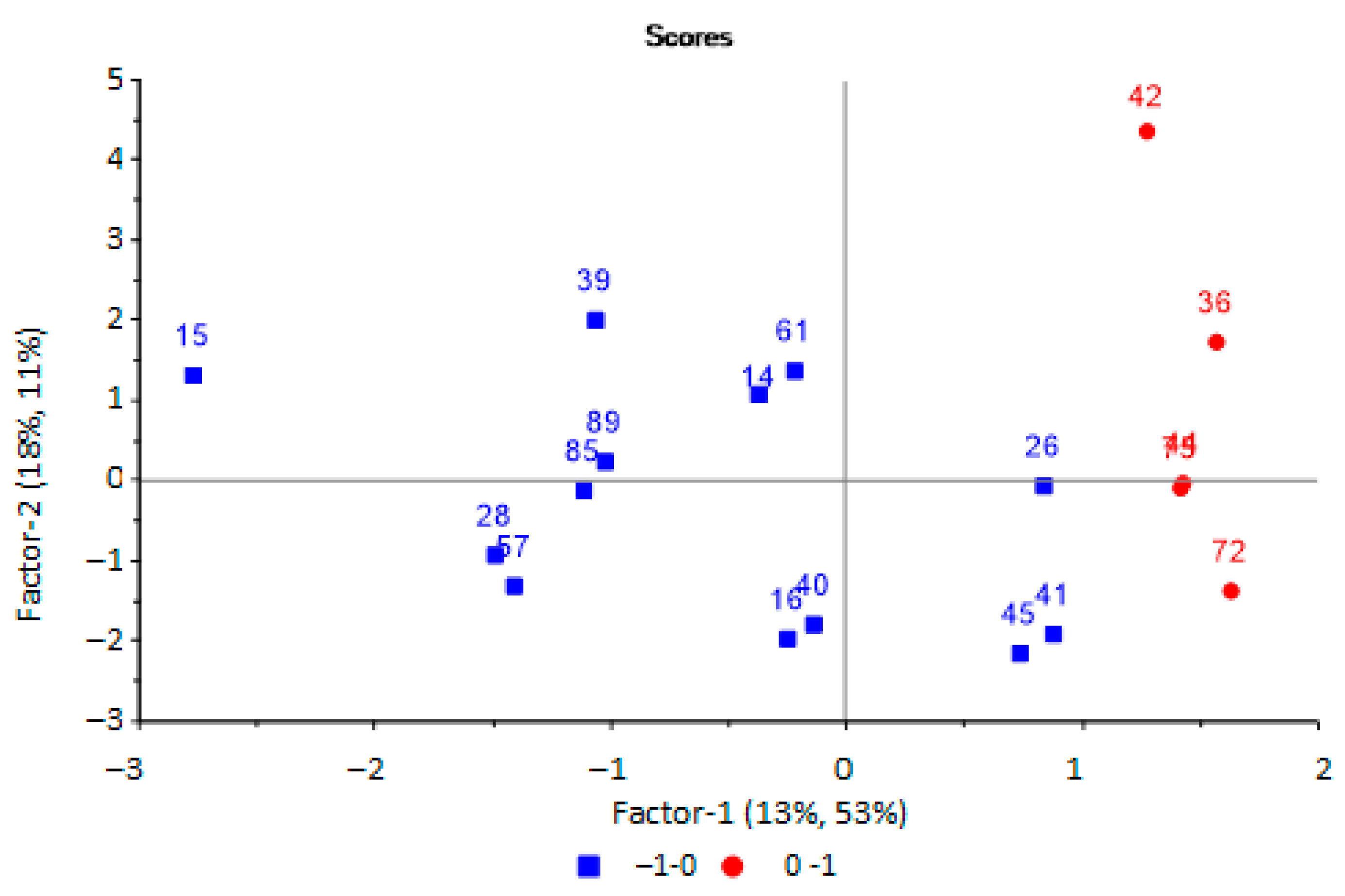
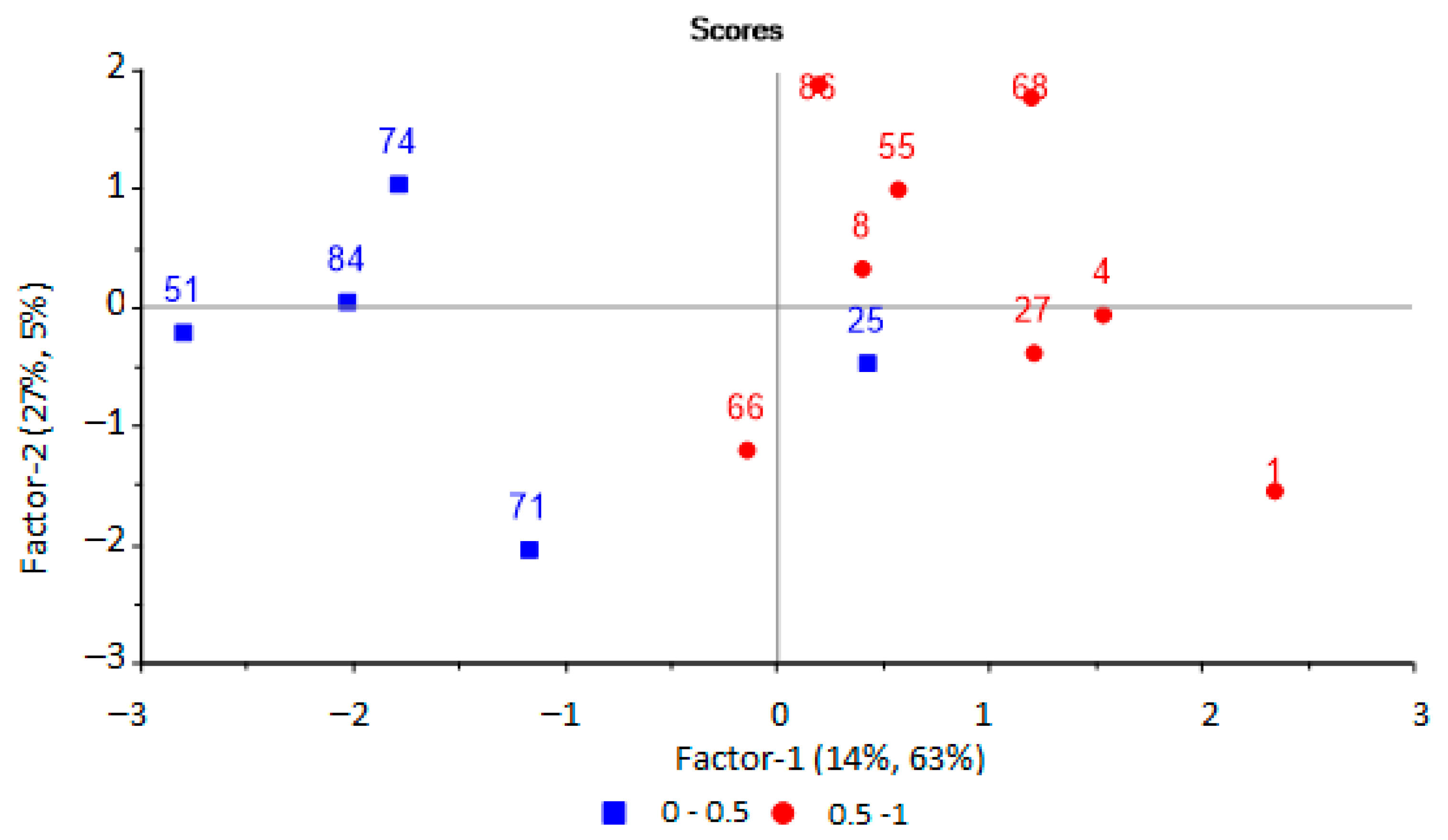
3.3. Selection of Informative Sensor Output Data by Principal Component Analysis
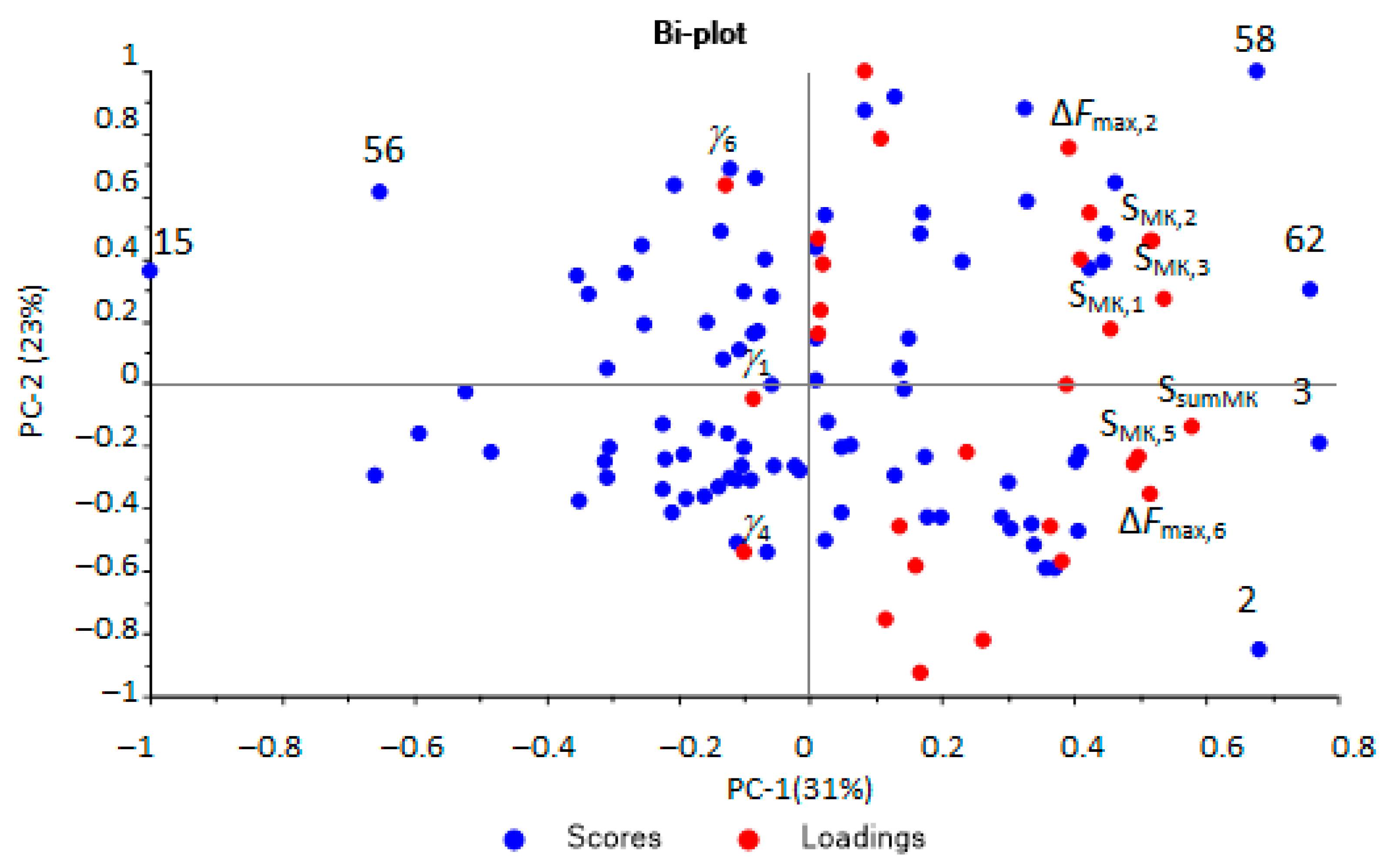
3.4. Prediction of Bacterial Infection by Sensor Data Using Multivariate Partial Least Squares
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Ellett, J.; Prasad, M.M.; Purves, J.T.; Stec, A.A. Post-surgical infections and perioperative antibiotics usage in pediatric genitourinary procedures. J. Pediatr. Urol. 2015, 11, 358.e1–358.e6. [Google Scholar] [CrossRef] [PubMed]
- Forrester, J.D.; Wolff, C.J.; Choi, J.; Colling, K.P.; Huston, J.M. Surgical Infection Society Guidelines for Antibiotic Use in Patients with Traumatic Facial Fractures. Surg. Infect. 2021, 22, 274–282. [Google Scholar] [CrossRef] [PubMed]
- Mollitt, D.L. Pediatric surgical infection and antibiotic usage. Pediatr. Infect. Dis. J. 1985, 4, 326–329. [Google Scholar] [CrossRef] [PubMed]
- Rangel, S.J.; Fung, M.; Graham, D.A.; Lin, M.; Nelson, G.P.; Sandora, T.J. Recent trends in the use of antibiotic prophylaxis in pediatric surgery. J. Pediatr. Surg. 2010, 46, 366–371. [Google Scholar] [CrossRef]
- Polk, H.C., Jr.; Christmas, A.B. Prophylactic antibiotics in surgery and surgical wound infections. Am. Surg. 2000, 66, 105–111. [Google Scholar]
- Williams, G.; Craig, J.C. Long-term antibiotics for preventing recurrent urinary tract infection in children. Cochrane Database Syst. Rev. 2019, 4, CD001534. [Google Scholar] [CrossRef]
- Powell, C.A.; Mealey, B.L.; Deas, D.E.; McDonnell, H.T.; Moritz, A.J. Post-Surgical Infections: Prevalence Associated with Various Periodontal Surgical Procedures. J. Periodontol. 2005, 76, 329–333. [Google Scholar] [CrossRef]
- WHO’s First Global Report on Antibiotic Resistance Reveals Serious, Worldwide Threat to Public Health. Available online: https://www.who.int/ru/news/item/30-04-2014-who-s-first-global-report-on-antibiotic-resistance-reveals-serious-worldwide-threat-to-public-health (accessed on 4 October 2022).
- Usupbaev, A.C.; Kabaev, B.A.; Imankulova, A.S.; Sadyrbekov, N.Z.; Cholponbaev, K.S.; Usupbaeva, A.A. Postoperative infectious complications in patients with urinary disease. Res. Pract. Med. J. 2018, 5, 30–37. [Google Scholar] [CrossRef] [Green Version]
- Wakeman, D.; Livingston, M.H.; Levatino, E.; Juviler, P.; Gleason, C.; Tesini, B.; Wilson, N.A.; Pegoli, W., Jr.; Arca, M.J. Reduction of surgical site infections in pediatric patients with complicated appendicitis: Utilization of antibiotic stewardship principles and quality improvement methodology. J. Pediatr. Surg. 2022, 57, 63–73. [Google Scholar] [CrossRef]
- Ploegmakers, I.B.M.; Olde Damink, S.W.M.; Breukink, S.O. Alternatives to antibiotics for prevention of surgical infection. Br. J. Surg. 2017, 104, e24–e33. [Google Scholar] [CrossRef] [Green Version]
- Zakharova, I.N.; Osmanov, I.M.; Machneva, E.B.; Mamuladze, E.B.; Gavelia, N.V.; Brazhnikova, O.V.; Lupan, I.N. Clinical analysis of urine: Historical significance for the development of medicine. Пeдиaтpия. Cons. Med. 2019, 1, 83–88. [Google Scholar] [CrossRef]
- De Lacy Costello, B.; Ratcliffe, N.M.; Amann, A.; Smith, D. Volatile organic compounds (VOCs) found in urine and stool. In Volatile Biomarkers: Non-Invasive Diagnosis in Physiology and Medicine, 1st ed.; Amann, A., Smith, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; pp. 405–462. [Google Scholar]
- De Lacy Costello, B.; Gould, O.; Ratcliffe, N.M. Biomarkers in urine and stool. In Breathborne Biomarkers and the Human Volatilome, 2nd ed.; Beauchamp, J., Davis, C., Pleil, J., Eds.; Elsevier: Amsterdam, The Netherlands, 2020; pp. 379–408. [Google Scholar] [CrossRef]
- Mills, G.A.; Walker, V. Headspace solid-phase microextraction profiling of volatile compounds in urine: Application to metabolic investigations. J. Chromatogr. B Biomed. Sci. Appl. 2001, 753, 259–268. [Google Scholar] [CrossRef]
- Smith, S.; Burden, H.; Persad, R.; Whittington, K.; de Lacy Costello, B.; Ratcliffe, N.M.; Probert, C.S. A comparative study of the analysis of human urine headspace using gas chromatographymass spectrometry. J. Breath Res. 2008, 2, 37022. [Google Scholar] [CrossRef] [PubMed]
- Ratui, I.-A.; Bocos-Bintintan, V.; Monedeiro, F.; Milanowski, M.; Ligor, T.; Buszewski, B. An Optimistic Vision of Future: Diagnosis of Bacterial Infections by Sensing Their Associated Volatile Organic Compounds. Crit. Rev. Anal. Chem. 2020, 50, 501–512. [Google Scholar] [CrossRef] [PubMed]
- Kwak, J.; Preti, G. Challenges in the Investigation of Volatile Disease Biomarkers in Urine. In Volatile Biomarkers: Non-Invasive Diagnosis in Physiology and Medicine, 1st ed.; Amann, A., Smith, D., Eds.; Elsevier: Amsterdam, The Netherlands, 2013; pp. 395–404. [Google Scholar] [CrossRef]
- Ratui, I.-A.; Ligor, T.; Monedeiro, F.; Al-Suod, H.; Bocos-Bintintan, V.; Szeliga, J.; Jackowski, M.; Buszewski, B. Features of infected versus uninfected chemical profiles released from human exudates. Stud. Univ. Babes-Bolyai Chem. 2019, 64, 207–216. [Google Scholar] [CrossRef]
- Bermejoa, J.; Gianelloa, M.; Pascalea, M.L.; Borda, N.; Freije, J.; Notario, R. Significado clínico del aislamiento de Staphylococcus aureus en muestras de orina. Enferm. Infecc. Microbiol. Clin. 2013, 31, 389–391. [Google Scholar] [CrossRef] [PubMed]
- Sethi, S.; Nanda, R.; Chakraborty, T. Clinical application of volatile organic compound analysis for detecting infectious diseases. Clin. Microbiol. Rev. 2013, 26, 462–475. [Google Scholar] [CrossRef] [Green Version]
- Aathithan, S.; Plant, J.C.; Chaudry, A.N.; French, G.L. Diagnosis of bacteriuria by detection of volatile organic compounds in urine using an automated headspace analyzer with multiple conducting polymer sensors. J. Clin. Microbiol. 2001, 39, 2590–2593. [Google Scholar] [CrossRef] [Green Version]
- Guernion, N.; Ratcliffe, N.M.; Spencer-Phillips, P.T.; Howe, R.A. Identifying bacteria in human urine: Current practice and the potential for rapid, near-patient diagnosis by sensing volatile organic compounds. Clin. Chem. Lab. Med. 2001, 39, 893. [Google Scholar] [CrossRef]
- Hayward, N.J.; Jeavons, T.H.; Nicholson, A.J.; Thornton, A.G. Development of specific tests for rapid detection of Escherichia coli and all species of Proteus in urine. J. Clin. Microbiol. 1977, 6, 195–201. [Google Scholar] [CrossRef]
- Kuchmenko, T.A.; Shuba, A.A.; Menzhulina, D.A.; Volkova, A.A.; Vecherkin, V.A.; Tueros, J.V.C. On a Correlation between the Results of In-Hospital Analysis of Biosamples from Children Performed Using Standard Methods and an Array of Piezosensors. J. Anal. Chem. 2022, 77, 376–387. [Google Scholar] [CrossRef]
- Capelli, L.; Taverna, G.; Bellini, A.; Eusebio, L.; Buffi, N.; Lazzeri, M.; Guazzoni, G.; Bozzini, G.; Seveso, M.; Mandressi, A.; et al. Application and Uses of Electronic Noses for Clinical Diagnosis on Urine Samples: A Review. Sensors 2016, 16, 1708. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrola, J.; Rocha, C.M.; Barros, A.S.; Gil, A.M.; Goodfellow, B.J.; Carreira, I.M.; Bernardo, J.; Gomes, A.; Sousa, V.; Carvalho, L.; et al. Metabolic signatures of lung cancer in biofluids: NMR-based metabonomics of urine. J. Proteome Res. 2011, 10, 221–230. [Google Scholar] [CrossRef] [PubMed]
- Liebich, H.M.; Al-Babbili, O.; Zlatkis, A.; Kim, K. Gas-chromatographic and massspectrometric detection of low-molecular-weight aliphatic alcohols in urine of normal individuals and patients with diabetes mellitus. Clin. Chem. 1975, 21, 1294–1296. [Google Scholar] [CrossRef] [PubMed]
- Podebrad, F.; Heil, M.; Reichert, S.; Mosandl, A.; Sewell, A.C.; Bohles, H. 4,5-Dimethyl-3-hydroxy-2[5H]-furanone (sotolone)—The odour of maple syrup urine disease. J. Inherit. Metab. Dis. 1999, 22, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Essler, J.L.; Kane, S.A.; Nolan, P.; Akaho, E.H.; Berna, A.Z.; DeAngelo, A.; Berk, R.A.; Kaynaroglu, P.; Plymouth, V.L.; Frank, I.D.; et al. Discrimination of SARS-CoV-2 infected patient samples by detection dogs: A proof of concept study. PLoS ONE 2021, 16, e0250158. [Google Scholar] [CrossRef]
- Banday, K.M.; Pasikanti, K.K.; Chan, E.C.; Singla, R.; Rao, K.V.; Chauhan, V.S.; Nanda, R.K. Use of urine volatile organic compounds to discriminate tuberculosis patients from healthy subjects. Anal. Chem. 2011, 83, 5526–5534. [Google Scholar] [CrossRef]
- Lim, S.H.; Martino, R.; Anikst, V.; Xu, Z.; Mix, S.; Benjamin, R.; Schub, H.; Eiden, M.; Rhodes, P.A.; Banaei, N. Rapid Diagnosis of Tuberculosis from Analysis of Urine Volatile Organic Compounds. ACS Sens. 2016, 1, 852–856. [Google Scholar] [CrossRef] [Green Version]
- Liebich, H.M.; Buelow, H.J.; Kallmayer, R. Quantification of endogenous aliphatic alcohols in serum and urine. J. Chromatogr. 1982, 239, 343–349. [Google Scholar] [CrossRef]
- Cummings, J.H.; Hill, M.J.; Bone, E.S.; Branch, W.J.; Jenkins, D.J. The effect of meat protein and dietary fiber on colonic function and metabolism. II. Bacterial metabolites in feces and urine. Am. J. Clin. Nutr. 1979, 32, 2094–2101. [Google Scholar] [CrossRef]
- Davies, T.; Hayward, N.J. Volatile products from acetylcholine as markers in the rapid urine test using head-space gas-liquid chromatography. J. Chromatogr. 1984, 307, 11–21. [Google Scholar] [CrossRef]
- Meng, W.; Zhao, C.; Gao, Y. Comparison of urine proteome among rat models by intraperitoneal injection with single bacteria and co-injection with two bacteria. PLoS ONE 2021, 16, e0261488. [Google Scholar] [CrossRef] [PubMed]
- Wintjens, A.G.W.E.; Hintzen, K.F.H.; Engelen, S.M.E.; Lubbers, T.; Savelkoul, P.H.M.; Wesseling, G.; van der Palen, J.A.M.; Bouvy, N.D. Applying the electronic nose for pre-operative SARS-CoV-2 screening. Surg. Endosc. 2021, 35, 6671–6678. [Google Scholar] [CrossRef]
- Wilson, A.D. Noninvasive Early Disease Diagnosis by Electronic-Nose and Related VOC-Detection Devices. Biosensors 2020, 10, 73. [Google Scholar] [CrossRef] [PubMed]
- Meraj, M.; Alvi, S.A.M.; Quasim, M.T.; Haidar, S.W. A Critical Review of Detection and Prediction of Infectious Disease using IOT Sensors. In Proceedings of the Second International Conference on Electronics and Sustainable Communication Systems (ICESC), Coimbatore, India, 4–6 August 2021; pp. 679–684. [Google Scholar] [CrossRef]
- Yatesa, J.W.T.; Chappella, M.J.; Gardnera, J.W.; Dowb, C.S.; Dowsonb, C.; Hamoodb, A.; Boltb, F.; Beebyb, L. Data reduction in headspace analysis of blood and urine samples for robust bacterial identification. Comput. Methods Programs Biomed. 2005, 79, 259–271. [Google Scholar] [CrossRef] [PubMed]
- Mironova, I.I.; Romanova, L.A.; Sosnin, D.Y. General clinical (chemical-microscopic) studies. In Clinical Laboratory Diagnostics; Dolgov, V.V., Ed.; FGBOU DPO RMANPO: Moscow, Russia, 2016; pp. 368–404. ISBN 978-5-7249-2608-9. [Google Scholar]
- Mironova, I.I.; Romanova, L.A.; Dolgov, V.V. General Clinical Studies: Urine, Feces, Cerebrospinal Fluid, Sputum, 3rd ed.; Triada: Tver, Russia, 2012; 420p, ISBN 978-5-94789-560-5. [Google Scholar]
- Alieva, E.V.; Kaftyreva, L.A.; Makarova, M.A.; Tartakovskiy, I.S. Practical recommendations for the preanalytical stage of microbiological research. Lab. Serv. 2020, 9, 45–66. [Google Scholar] [CrossRef]
- Order of the Ministry of Health of the USSR dated April 22, 1985 N 535 “On the unification of microbiological (bacteriological) research methods, used in clinical diagnostic laboratories of medical institutions” (together with “Guidelines for the use of unified microbiological (bacteriological) research methods in clinical diagnostic laboratories”). Available online: https://docs.cntd.ru/document/420245293 (accessed on 22 October 2022).
- Kuchmenko, T.A.; Selmanshchuk, V.A. Multichannel “Electronic Nose” on Piezosensors. RF Patent No. 2327984. Application 2007106335/28, 19 February 2007. publ. 06/27/2008. [Google Scholar]
- Kuchmenko, T.; Shuba, A.; Umarkhanov, R.; Menzulina, D.; Chernitskiy, A. New Way and Sensor Device for Investigation of Biosamples and Health Status of Humans and Animals. Int. J. Adv. Life Sci. 2021, 13, 1–13. Available online: http://www.thinkmind.org/index.php?view=article&articleid=lifsci_v13_n12_2021_1 (accessed on 22 October 2022).
- Korenman, Y.I.; Popova, N.N.; Kuchmenko, T.A. Determination of C1–C3 carboxylic acids in air using a sensor. J. Anal. Chem. 2008, 63, 85–89. [Google Scholar] [CrossRef]
- Shuba, A.A.; Kuchmenko, T.A.; Samoilova, E.I.; Bel’skikh, N.V. Selection of a Piezoelectric Sensor Array for Detecting Volatile Organic Substances in Water. Mosc. Univ. Chem. Bull. 2016, 71, 68–75. [Google Scholar] [CrossRef]
- Kuchmenko, T.A.; Mishina, A.A. Sorption specifics of volatile amines on thin films of acid-base indicators. J. Anal. Chem. 2011, 66, 701–708. [Google Scholar] [CrossRef]
- Kuchmenko, T.A.; Umarkhanov, R.U.; Kochetova, Z.Y.; Bel’skikh, N.V. Development of a piezosensor-based transducer, gas analyzer and ammonia detector. J. Anal. Chem. 2012, 67, 930–939. [Google Scholar] [CrossRef]
- Kuchmenko, T.A.; Umarkhanov, R.U. Peculiarities of microweighing of trace quantities of alkylamines on polymer and solid–state thin films. J. Anal. Chem. 2013, 68, 368–377. [Google Scholar] [CrossRef]
- Korenman, Y.I.; Popova, N.N.; Kuchmenko, T.A.; Suleimanov, S.M. Effect of the morphology of polyethylene glycol esters on the distribution of C-1-C-4 carboxylic acids in the gas phase-sorbent system. Russ. J. Phys. Chem. 2006, 80, 1993–1998. [Google Scholar] [CrossRef]
- Kuchmenko, T.A.; Shuba, A.A.; Drozdova, E.V. Substantiation of the operating life of gas piezosensors in detection of vapors of organic compounds. Russ. J. Appl. Chem. 2015, 88, 1997–2006. [Google Scholar] [CrossRef]
- Kuchmenko, T.A.; Kochetova, Z.Y.; Silina, Y.E.; Korenman, Y.I.; Kulin, L.A.; Lapitskii, I.V. Determination of trace amounts of hydrogen sulfide in a gas flow using a piezoelectric detector. J. Anal. Chem. 2007, 62, 781–790. [Google Scholar] [CrossRef]
- Kuchmenko, T.A.; Lvova, L.B. A Perspective on Recent Advances in Piezoelectric Chemical Sensors for Environmental Monitoring and Foodstuffs Analysis. Chemosensors 2019, 7, 39. [Google Scholar] [CrossRef] [Green Version]
- Kuchmenko, T.A.; Shuba, A.A.; Belskikh, N.V. The identification parameters of organic substances in multisensors piezoquartz microbalance. Anal. Kontrol 2012, 16, 151–161. [Google Scholar]
- Kuchmenko, T.A. Innovative solutions in analytical control: Textbook. In Voronezh: Voronezh State Technological Academy; SenTech LLC: Voronezh, Russia, 2009; p. 252. ISBN 978-5-89448-596-6. [Google Scholar]
- Kuchmenko, T.; Shuba, A.; Umarkhanov, R.; Chernitskiy, A. Portable Electronic Nose for Analyzing the Smell of Nasal Secretions in Calves: Toward Noninvasive Diagnosis of Infectious Bronchopneumonia. Vet. Sci. 2021, 8, 74. [Google Scholar] [CrossRef]
- Kuchmenko, T.A.; Shuba, A.A. Informative nature of the electronic nose output signals based on the piezoelectric sensors. Anal. Kontrol 2017, 21, 72–84. [Google Scholar] [CrossRef] [Green Version]
- Kuchmenko, T.A.; Shuba, A.A.; Bityukova, V.V.; Matveeva, N.A. Application of a Chemical Sensor Array to Assessing the Presence of Neoplasms by Blood Smell. J. Anal. Chem. 2018, 73, 91–101. [Google Scholar] [CrossRef]
- Kholin, Y.V.; Nikitina, N.A.; Panteleimonov, A.V.; Reshetnyak, E.A.; Bugaevsky, A.A.; Loginova, L.P. Metrological Characteristics of Detection Methods with a Binary Response; Timchenko: Kharkov, Ukraine, 2008; p. 128. ISBN 9789668661358. [Google Scholar]
- Sharkey, L. Urine analysis. In Interpretation of Equine Laboratory Diagnostics, 1st ed.; Pusterla, N., Higgins, J., Eds.; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2017; pp. 383–386. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Indicators of GUA | Isolated Microorganism from Specimen for Biopsy | ||
|---|---|---|---|---|
| Mucus | Leukocytes | Bacteria | ||
| 1 | ~0 | 2 | ~0 | Staphylococcus aureus |
| 2 | + | 9 | ~0 | – |
| 3 | ~0 | 2 | ~0 | – 1 |
| 4 | ~0 | 2 | ~0 | Streptococcus b-haemophylus; Candida albicans |
| 5 | ~0 | 2 | ~0 | – |
| 6 | ~0 | 2 | ~0 | E. coli, Streptococcus b-haemophylus |
| 7 | ~0 | 16 | ~0 | E. coli |
| 8 | ~0 | 3 | ~0 | Staphylococcus aureus |
| 9 | ~0 | 4 | ~0 | – |
| 10 | ~0 | 7 | + | – |
| 11 | ~0 | 3 | ~0 | Staphylococcus aureus |
| 12 | ~0 | 3 | ~0 | – |
| 13 | + | 2 | ~0 | – |
| 14 | ~0 | 4 | ~0 | – |
| 15 | ~0 | 16 | + | – |
| 16 | ~0 | 2 | ~0 | – |
| 17 | ~0 | 4 | ~0 | – |
| 18 | ~0 | 3 | ~0 | – |
| 19 | ~0 | 4 | ~0 | – |
| 20 | ~0 | 5 | ~0 | – |
| 21 | ++ | 8 | + | – |
| 22 | ~0 | 6 | ~0 | – |
| 23 | ~0 | 5 | ~0 | – |
| 24 | ~0 | 4 | ~0 | – |
| 25 | ~0 | 2 | ~0 | Not determined |
| 26 | ++ | 8 | ~0 | – |
| 27 | ~0 | 2 | – | E. coli |
| 28 | ~0 | 2 | – | – |
| 29 | + | 9 | ~0 | Staphylococcus gallinarum |
| 30 | ++ | 1 | ~0 | – |
| 31 | ~0 | 4 | + | – |
| 32 | ~0 | 6 | + | – |
| 33 | + | 2 | + | – |
| 34 | + | 2 | + | – |
| 35 | +++ | 10 | + | – |
| 36 | +++ | 1 | + | Staphylococcus aureus |
| 37 | ~0 | 1 | ~0 | – |
| 38 | ~0 | 1 | ~0 | – |
| 39 | + | 1 | ~0 | – |
| 40 | ~0 | 3 | ~0 | – |
| 41 | + | 2 | ~0 | – |
| 42 | ++ | 10 | + | – |
| 43 | ~0 | 1 | ~0 | – |
| 44 | + | 1 | + | – |
| 45 | ~0 | 1 | ~0 | – |
| 46 | +++ | 1 | + | – |
| 47 | ~0 | 2 | ~0 | – |
| 48 | + | 3 | ++ | – |
| 49 | + | 2 | + | – |
| 50 | + | 2 | ~0 | – |
| 51 | ++ | 10 | ~0 | Not determined |
| 52 | ++ | 7 | ~0 | – |
| 53 | + | 3 | ~0 | – |
| 54 | + | 3 | ~0 | Staphylococcus aureus |
| 55 | + | 4 | ++ | Staphylococcus saprophysicus |
| 56 | ++ | 2 | ~0 | – |
| 57 | ++ | 1 | ~0 | Staphylococcus aureus |
| 58 | ++ | 1 | ~0 | Streptococcus jaccicum |
| 59 | ++ | 1 | + | – |
| 60 | + | 25 | + | – |
| 61 | ~0 | 1 | ~0 | – |
| 62 | ~0 | 1 | ~0 | – |
| 63 | ~0 | 2 | ~0 | – |
| 64 | + | 2 | + | – |
| 65 | ~0 | 1 | ~0 | Streptococcus viridans |
| 66 | ++ | 1 | ~0 | Streptococcus b-haemophylus |
| 67 | ++ | 20 | +++ | – |
| 68 | + | 1 | ~0 | Staphylococcus aureus |
| 69 | + | 1 | ~0 | – |
| 70 | +++ | 4 | + | – |
| 71 | ~0 | 7 | ~0 | Not determined |
| 72 | +++ | 4 | ++ | Not determined |
| 73 | ~0 | 1 | ~0 | – |
| 74 | ++ | 4 | + | Not determined |
| 75 | ~0 | 1 | ++ | Not determined |
| 76 | ++ | 1 | + | – |
| 77 | ++ | 4 | ~0 | – |
| 78 | +++ | 6 | + | – |
| 79 | ++ | 1 | + | – |
| 80 | + | 2 | ~0 | – |
| 81 | +++ | 1 | ~0 | Staphylococcus epidermidis |
| 82 | ~0 | 3 | ~0 | Streptococcus b-haemophylus |
| 83 | ++ | 1 | ~0 | Klebsiella pneumoniae |
| 84 | ++ | 5 | + | Not determined |
| 85 | ~0 | 2 | ~0 | – |
| 86 | + | 5 | ~0 | Staphylococcus haemolyticus |
| 87 | ++ | 1 | ~0 | Streptococcus viridans |
| 88 | +++ | 3 | ++ | – |
| 89 | +++ | 2 | + | – |
| 90 | + | 4 | ~0 | – |
| Coating | Ammonia | Diethylamine | Butyric Acid | Ethanol | Acetone | Sr* |
|---|---|---|---|---|---|---|
| PEGSb | 5.00 | 7.82 | 15.0 | 7.72 | 1.41 | 0.04–0.13 |
| TX-100 | 4.37 | 29.4 | 27.5 | 1.43 | 1.44 | 0.03–0.12 |
| 18C6 | 6.17 | 1.90 | 77.5 | 0.98 | 1.27 | 0.12–0.20 |
| Tween | 2.51 | 1.52 | 71.3 | 1.52 | 1.21 | 0.05–0.15 |
| MR | 13.4 | 4.00 | 6.72 | 1.39 | 0.65 | 0.02–0.17 |
| BCB | 16.4 | 10.2 | 7.12 | 1.16 | 0.83 | 0.05–0.20 |
| MCNT | 14.3 | 3.74 | 7.52 | 0.98 | 0.39 | 0.07–0.17 |
| Substances | Maxillofacial Surgery | General Surgery | Traumatology | Burn | Neurosurgery | Purulent-Septic | Orthopedic |
|---|---|---|---|---|---|---|---|
| Ethanol | 85 | 100 | 83 | 100 | 100 | 100 | 75 |
| Buthanol-1 | 85 | 100 | 83 | 100 | 100 | 100 | 75 |
| Acetone | 32 | 39 | 22 | 33 | 83 | 75 | 50 |
| Hydrogen sulfide | 15 | 22 | 13 | – | – | – | 25 |
| Phenol | 76 | 72 | 56 | 66 | 83 | 75 | 50 |
| Ethyl acetate | 20 | 28 | 17 | 33 | 83 | 75 | 50 |
| Acetic acid | 76 | 94 | 83 | 100 | 100 | 100 | 75 |
| Butyric acid | 76 | 94 | 83 | 100 | 100 | 100 | 75 |
| Dimethylacetal dimethylformamide | 76 | 89 | 70 | – | 100 | 50 | 50 |
| Piperidine | 89 | 11 | 39 | 33 | – | 25 | – |
| Diethylamine | 70 | 67 | 39 | 66 | 50 | 100 | 50 |
| Ammonia | – * | 67 | 52 | 100 | 33 | 100 | 100 |
| Amines | 100 | 67 | 52 | 100 | 33 | 100 | 75 |
| Valeric acid | 50 | 61 | 52 | 33 | 100 | 75 | 50 |
| Isovaleric acid | 50 | 61 | 52 | 33 | 100 | 75 | 50 |
| Sample No. | Predicted Value | Deviation | Reference Value |
|---|---|---|---|
| 5 | −0.21 | 0.47 | −1 |
| 10 | 0.29 | 0.47 | 1 |
| 20 | −0.29 | 0.57 | −1 |
| 21 | −1.38 | 0.64 | 1 |
| 34 | 0.15 | 0.68 | 1 |
| 46 | −0.56 | 0.52 | 1 |
| 48 | 0.26 | 0.65 | 1 |
| 54 | −1.55 | 0.78 | −1 |
| 55 | 0.14 | 0.62 | 1 |
| 71 | 0.24 | 0.80 | −1 |
| 79 | 1.17 | 0.66 | 1 |
| 80 | −0.78 | 0.40 | −1 |
| 85 | −1.04 | 0.71 | −1 |
| 90 | −1.14 | 0.44 | −1 |
| Sample No. | Predicted Value | Deviation | Reference Value |
|---|---|---|---|
| 36 | 0.94 | 0.44 | 1 |
| 57 | 0.55 | 0.35 | 1 |
| 58 | 0.56 | 0.38 | 1 |
| 71 | 0.34 | 0.32 | 0 |
| 75 | 0.70 | 0.50 | 0 |
| 83 | 0.57 | 0.31 | 1 |
| Sample No. | InfI | No. | InfI | No. | InfI | No. | InfI | No. | InfI |
|---|---|---|---|---|---|---|---|---|---|
| 1 | 1.48 | 19 | 1.45 | 37 | 1.57 | 55 | 1.84 | 73 | 1.42 |
| 2 | 1.42 | 20 | 1.51 | 38 | 2.09 | 56 | 1.45 | 74 | 1.60 |
| 3 | 1.59 | 21 | 1.69 | 39 | 1.99 | 57 | 1.94 | 75 | 1.45 |
| 4 | 1.60 | 22 | 1.43 | 40 | 1.52 | 58 | 2.03 | 76 | 1.78 |
| 5 | 1.53 | 23 | 1.56 | 41 | 1.47 | 59 | 1.81 | 77 | 1.22 |
| 6 | 1.59 | 24 | 1.29 | 42 | 1.88 | 60 | 1.98 | 78 | 1.68 |
| 7 | 1.58 | 25 | 1.50 | 43 | 1.61 | 61 | 1.87 | 79 | 1.14 |
| 8 | 1.48 | 26 | 1.42 | 44 | 1.54 | 62 | 1.80 | 80 | 1.78 |
| 9 | 1.32 | 27 | 1.64 | 45 | 1.56 | 63 | 1.45 | 81 | 1.59 |
| 10 | 1.57 | 28 | 1.49 | 46 | 1.57 | 64 | 2.10 | 82 | 1.81 |
| 11 | 1.54 | 29 | 1.57 | 47 | 1.58 | 65 | 1.59 | 83 | 1.72 |
| 12 | 1.42 | 30 | 1.26 | 48 | 1.50 | 66 | 1.63 | 84 | 1.95 |
| 13 | 1.50 | 31 | 1.51 | 49 | 1.87 | 67 | 1.34 | 85 | 1.62 |
| 14 | 1.26 | 32 | 1.55 | 50 | 1.42 | 68 | 1.57 | 86 | 1.78 |
| 15 | 1.99 | 33 | 1.70 | 51 | 1.45 | 69 | 1.54 | 87 | 1.89 |
| 16 | 1.45 | 34 | 2.45 | 52 | 1.61 | 70 | 1.72 | 88 | 1.95 |
| 17 | 1.52 | 35 | 1.63 | 53 | 1.28 | 71 | 1.42 | 89 | 1.61 |
| 18 | 1.73 | 36 | 1.75 | 54 | 1.79 | 72 | 1.63 | 90 | 1.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuchmenko, T.; Menzhulina, D.; Shuba, A. Noninvasive Detection of Bacterial Infection in Children Using Piezoelectric E-Nose. Sensors 2022, 22, 8496. https://doi.org/10.3390/s22218496
Kuchmenko T, Menzhulina D, Shuba A. Noninvasive Detection of Bacterial Infection in Children Using Piezoelectric E-Nose. Sensors. 2022; 22(21):8496. https://doi.org/10.3390/s22218496
Chicago/Turabian StyleKuchmenko, Tatiana, Daria Menzhulina, and Anastasiia Shuba. 2022. "Noninvasive Detection of Bacterial Infection in Children Using Piezoelectric E-Nose" Sensors 22, no. 21: 8496. https://doi.org/10.3390/s22218496