
Markerless Radio Frequency Indoor Monitoring for Telemedicine: Gait Analysis, Indoor Positioning, Fall Detection, Tremor Analysis, Vital Signs and Sleep Monitoring
 , ,
, ,  ,
,
Abstract
:1. Global Overview on Current Monitoring Systems
1.1. Inertial Monitoring
1.2. Camera-Based Monitoring
1.3. Radio Frequency Monitoring
1.4. Geomagnetic Monitoring
1.5. IR-UWB: Physical Basis
2. Clinical Applications
2.1. Gait Analysis and Indoor Positioning
2.2. Fall Detection
2.3. Tremor Assessment
2.4. Vital Sign Monitoring
2.5. Sleep Monitoring
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Li, C.; Un, K.F.; Mak, P.I.; Chen, Y.; Muñoz-Ferreras, J.M.; Yang, Z.; Gómez-García, R. Overview of recent development on wireless sensing circuits and systems for healthcare and biomedical applications. IEEE J. Emerg. Sel. Top. Circuits Syst. 2018, 8, 165–177. [Google Scholar] [CrossRef]
- Sánchez-Ferro, Á.; Elshehabi, M.; Godinho, C.; Salkovic, D.; Hobert, M.A.; Domingos, J.; Van Uem, J.M.; Ferreira, J.J.; Maetzler, W. New methods for the assessment of Parkinson’s disease (2005 to 2015): A systematic review. Mov. Disord. 2016, 31, 1283–1292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Summa, S.; Tosi, J.; Taffoni, F.; Di Biase, L.; Marano, M.; Rizzo, A.C.; Tombini, M.; Di Pino, G.; Formica, D. Assessing bradykinesia in Parkinson’s disease using gyroscope signals. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 1556–1561. [Google Scholar]
- Di Biase, L.; Summa, S.; Tosi, J.; Taffoni, F.; Marano, M.; Cascio Rizzo, A.; Vecchio, F.; Formica, D.; Di Lazzaro, V.; Di Pino, G.; et al. Quantitative Analysis of Bradykinesia and Rigidity in Parkinson’s Disease. Front. Neurol. 2018, 9, 121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raiano, L.; di Pino, G.; di Biase, L.; Tombini, M.; Tagliamonte, N.L.; Formica, D. PDMeter: A Wrist Wearable Device for an at-home Assessment of the Parkinson’s Disease Rigidity. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1325–1333. [Google Scholar] [CrossRef]
- Tosi, J.; Summa, S.; Taffoni, F.; di Biase, L.; Marano, M.; Rizzo, A.C.; Tombini, M.; Schena, E.; Formica, D.; Di Pino, G. Feature Extraction in Sit-to-Stand Task Using M-IMU Sensors and Evaluatiton in Parkinson’s Disease. In Proceedings of the 2018 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Rome, Italy, 11–13 June 2018; pp. 1–6. [Google Scholar]
- di Biase, L.; Di Santo, A.; Caminiti, M.L.; De Liso, A.; Shah, S.A.; Ricci, L.; Di Lazzaro, V. Gait Analysis in Parkinson’s Disease: An Overview of the Most Accurate Markers for Diagnosis and Symptoms Monitoring. Sensors 2020, 20, 3529. [Google Scholar] [CrossRef]
- di Biase, L.; Raiano, L.; Caminiti, M.L.; Pecoraro, P.M.; Di Lazzaroo, V. Artificial intelligence in Parkinson’s disease—Symptoms identification and monitoring. In Augmenting Neurological Disorder Prediction and Rehabilitation Using Artificial Intelligence; Pillai, A.S., Menon, B., Eds.; Elsevier: Amsterdam, The Netherlands, 2022; pp. 35–52. [Google Scholar]
- di Biase, L.; Di Santo, A.; Caminiti, M.L.; Pecoraro, P.M.; Di Lazzaro, V. Classification of Dystonia. Life 2022, 12, 206. [Google Scholar] [CrossRef]
- di Biase, L.; Di Santo, A.; Caminiti, M.L.; Pecoraro, P.M.; Carbone, S.P.; Di Lazzaro, V. Dystonia Diagnosis: Clinical Neurophysiology and Genetics. J. Clin. Med. 2022, 11, 4184. [Google Scholar] [CrossRef]
- Piña-Fuentes, D.; Beudel, M.; Little, S.; van Zijl, J.; Elting, J.W.; Oterdoom, D.M.; van Egmond, M.E.; van Dijk, J.M.C.; Tijssen, M.A. Toward adaptive deep brain stimulation for dystonia. Neurosurg. Focus 2018, 45, E3. [Google Scholar] [CrossRef] [Green Version]
- Deuschl, G.; Krack, P.; Lauk, M.; Timmer, J. Clinical neurophysiology of tremor. J. Clin. Neurophysiol. 1996, 13, 110–121. [Google Scholar] [CrossRef]
- Di Pino, G.; Formica, D.; Melgari, J.M.; Taffoni, F.; Salomone, G.; di Biase, L.; Caimo, E.; Vernieri, F.; Guglielmelli, E. Neurophysiological bases of tremors and accelerometric parameters analysis. In Proceedings of the 2012 4th IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics (BioRob), Rome, Italy, 24–27 June 2012; pp. 1820–1825. [Google Scholar]
- Di Biase, L.; Brittain, J.S.; Shah, S.A.; Pedrosa, D.J.; Cagnan, H.; Mathy, A.; Chen, C.C.; Martín-Rodríguez, J.F.; Mir, P.; Timmerman, L.; et al. Tremor stability index: A new tool for differential diagnosis in tremor syndromes. Brain 2017, 140, 1977–1986. [Google Scholar] [CrossRef]
- Di Biase, L.; Brittain, J.S.; Peter, B.; Di Lazzaro, V.; Shah, S.A. Methods and System for Characterising Tremors. U.S. Patent 16/478,545, 13 February 2020. [Google Scholar]
- di Biase, L.; Tinkhauser, G.; Martin Moraud, E.; Caminiti, M.L.; Pecoraro, P.M.; Di Lazzaro, V. Adaptive, personalized closed-loop therapy for Parkinson’s disease: Biochemical, neurophysiological, and wearable sensing systems. Expert Rev. Neurother. 2021, 21, 1371–1388. [Google Scholar] [CrossRef] [PubMed]
- Hamad, R.A.; Hidalgo, A.S.; Bouguelia, M.R.; Estevez, M.E.; Quero, J.M. Efficient activity recognition in smart homes using delayed fuzzy temporal windows on binary sensors. IEEE J. Biomed. Health Inform. 2019, 24, 387–395. [Google Scholar] [CrossRef] [PubMed]
- Cippitelli, E.; Fioranelli, F.; Gambi, E.; Spinsante, S. Radar and RGB-depth sensors for fall detection: A review. IEEE Sens. J. 2017, 17, 3585–3604. [Google Scholar] [CrossRef] [Green Version]
- König, A.; Crispim Junior, C.F.; Derreumaux, A.; Bensadoun, G.; Petit, P.D.; Bremond, F.; David, R.; Verhey, F.; Aalten, P.; Robert, P. Validation of an automatic video monitoring system for the detection of instrumental activities of daily living in dementia patients. J. Alzheimers Dis. 2015, 44, 675–685. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalal, A.; Quaid, M.A.K.; Tahir, S.B.U.D.; Kim, K. A study of accelerometer and gyroscope measurements in physical life-log activities detection systems. Sensors 2020, 20, 6670. [Google Scholar] [CrossRef]
- Lin, C.L.; Chiu, W.C.; Chu, T.C.; Ho, Y.H.; Chen, F.H.; Hsu, C.C.; Hsieh, P.H.; Chen, C.H.; Lin, C.C.K.; Sung, P.S.; et al. Innovative head-mounted system based on inertial sensors and magnetometer for detecting falling movements. Sensors 2020, 20, 5774. [Google Scholar] [CrossRef]
- Jarchi, D.; Pope, J.; Lee, T.K.; Tamjidi, L.; Mirzaei, A.; Sanei, S. A review on accelerometry-based gait analysis and emerging clinical applications. IEEE Rev. Biomed. Eng. 2018, 11, 177–194. [Google Scholar] [CrossRef]
- Greene, B.R.; O’Donovan, A.; Romero-Ortuno, R.; Cogan, L.; Scanaill, C.N.; Kenny, R.A. Quantitative falls risk assessment using the timed up and go test. IEEE Trans. Biomed. Eng. 2010, 57, 2918–2926. [Google Scholar] [CrossRef]
- Liu, Y.; Hu, Y.H.; Pan, Q. Distributed, robust acoustic source localization in a wireless sensor network. IEEE Trans. Signal Process. 2012, 60, 4350–4359. [Google Scholar] [CrossRef]
- Milosevic, M.; Jovanov, E.; Milenković, A. Quantifying Timed-Up-and-Go test: A smartphone implementation. In Proceedings of the 2013 IEEE International Conference on Body Sensor Networks, Cambridge, MA, USA, 6–9 May 2013; IEEE: Piscataway, NJ, USA, 2013. [Google Scholar]
- Dai, J.; Bai, X.; Yang, Z.; Shen, Z.; Xuan, D. A pervasive fall detection system using mobile phones. In Proceedings of the 2010 8th IEEE International Conference on Pervasive Computing and Communications Workshops (PERCOM Workshops), Mannheim, Germany, 29 March 2010–2 April 2010. [Google Scholar]
- Lee, X.G.; Low, K.S.; Taher, T. Unrestrained measurement of arm motion based on a wearable wireless sensor network. IEEE Trans. Instrum. Meas. 2010, 59, 1309–1317. [Google Scholar] [CrossRef]
- Geman, O.; Costin, H. Automatic assessing of tremor severity using nonlinear dynamics, artificial neural networks and neuro-fuzzy classifier. Adv. Electr. Comput. Eng. 2014, 14, 133–139. [Google Scholar] [CrossRef]
- Tsanas, A.; Little, M.A.; McSharry, P.E.; Spielman, J.; Ramig, L.O. Novel speech signal processing algorithms for high-accuracy classification of Parkinson’s disease. IEEE Trans. Biomed. Eng. 2012, 59, 1264–1271. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hariharan, M.; Polat, K.; Sindhu, R. A new hybrid intelligent system for accurate detection of Parkinson’s disease. Comput. Methods Programs Biomed. 2014, 113, 904–913. [Google Scholar] [CrossRef] [PubMed]
- Bachlin, M.; Plotnik, M.; Roggen, D.; Maidan, I.; Hausdorff, J.M.; Giladi, N.; Troster, G. Wearable assistant for Parkinson’s disease patients with the freezing of gait symptom. IEEE Trans. Inf. Technol. Biomed. 2009, 14, 436–446. [Google Scholar] [CrossRef]
- Tripoliti, E.E.; Tzallas, A.T.; Tsipouras, M.G.; Rigas, G.; Bougia, P.; Leontiou, M.; Konitsiotis, S.; Chondrogiorgi, M.; Tsouli, S.; Fotiadis, D.I. Automatic detection of freezing of gait events in patients with Parkinson’s disease. Comput. Methods Programs Biomed. 2013, 110, 12–26. [Google Scholar] [CrossRef]
- Jovanov, E.; Wang, E.; Verhagen, L.; Fredrickson, M.; Fratangelo, R. deFOG—A real time system for detection and unfreezing of gait of Parkinson’s patients. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; IEEE: Piscataway, NJ, USA, 2009. [Google Scholar]
- Khan, S.S.; Hoey, J. Review of fall detection techniques: A data availability perspective. Med. Eng. Phys. 2017, 39, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Grydeland, M.; Hansen, B.H.; Ried-Larsen, M.; Kolle, E.; Anderssen, S.A. Comparison of three generations of ActiGraph activity monitors under free-living conditions: Do they provide comparable assessments of overall physical activity in 9-year old children? BMC Sport. Sci. Med. Rehabil. 2014, 6, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Hegde, N.; Bries, M.; Sazonov, E. A comparative review of footwear-based wearable systems. Electronics 2016, 5, 48. [Google Scholar] [CrossRef]
- Sun, S.; Zhao, X.; Tan, M. Fast and Robust RGB-D Multiple Human Tracking Based on Part Model for Mobile Robots. In Proceedings of the 2019 Chinese Control Conference (CCC), Guangzhou, China, 27–30 July 2019; IEEE: Piscataway, NJ, USA, 2019. [Google Scholar]
- Panahi, L.; Ghods, V. Human fall detection using machine vision techniques on RGB–D images. Biomed. Signal Process. Control 2018, 44, 146–153. [Google Scholar] [CrossRef]
- D’Orazio, T.; Marani, R.; Renò, V.; Cicirelli, G. Recent trends in gesture recognition: How depth data has improved classical approaches. Image Vis. Comput. 2016, 52, 56–72. [Google Scholar] [CrossRef]
- Camplani, M.; Paiement, A.; Mirmehdi, M.; Damen, D.; Hannuna, S.; Burghardt, T.; Tao, L. Multiple human tracking in RGB-depth data: A survey. IET Comput. Vis. 2017, 11, 265–285. [Google Scholar] [CrossRef] [Green Version]
- Diraco, G.; Leone, A.; Siciliano, P. A radar-based smart sensor for unobtrusive elderly monitoring in ambient assisted living applications. Biosensors 2017, 7, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morita, P.P.; Rocha, A.S.; Shaker, G.; Lee, D.; Wei, J.; Fong, B.; Thatte, A.; Karimi, A.; Xu, L.; Ma, A.; et al. Comparative Analysis of Gait Speed Estimation Using Wideband and Narrowband Radars, Thermal Camera, and Motion Tracking Suit Technologies. J. Healthc. Inform. Res. 2020, 4, 215–237. [Google Scholar] [CrossRef] [PubMed]
- Zhang, H.; Zhang, Z.; Gao, N.; Xiao, Y.; Meng, Z.; Li, Z. Cost-effective wearable indoor localization and motion analysis via the integration of UWB and IMU. Sensors 2020, 20, 344. [Google Scholar] [CrossRef] [Green Version]
- He, S.; Chan, S.-H.G. Wi-Fi fingerprint-based indoor positioning: Recent advances and comparisons. IEEE Commun. Surv. Tutor. 2015, 18, 466–490. [Google Scholar] [CrossRef]
- Lashkari, A.H.; Parhizkar, B.; Ngan, M.N.A. WIFI-based indoor positioning system. In Proceedings of the 2010 Second International Conference on Computer and Network Technology, Washington, DC, USA, 23–25 April 2010; IEEE: Piscataway, NJ, USA, 2010. [Google Scholar]
- Alrajeh, N.A.; Bashir, M.; Shams, M. Localization techniques in wireless sensor networks. Int. J. Distrib. Sens. Netw. 2013, 9, 304628. [Google Scholar] [CrossRef] [Green Version]
- Wang, W.; Chen, J.; Hong, T.; Zhu, N. Occupancy prediction through Markov based feedback recurrent neural network (M-FRNN) algorithm with WiFi probe technology. Build. Environ. 2018, 138, 160–170. [Google Scholar] [CrossRef] [Green Version]
- Pecoraro, G.; Di Domenico, S.; Cianca, E.; De Sanctis, M. LTE signal fingerprinting localization based on CSI. In Proceedings of the 2017 IEEE 13th International Conference on Wireless and Mobile Computing, Networking and Communications (WiMob), Rome, Italy, 9–11 October 2017; IEEE: Piscataway, NJ, USA, 2017. [Google Scholar]
- Pecoraro, G.; Cianca, E.; Di Domenico, S.; De Sanctis, M. LTE Signal Fingerprinting Device-Free Passive Localization Robust to Environment Changes. In Proceedings of the 2018 Global Wireless Summit (GWS), Chiang Rai, Thailand, 25–28 November 2018; IEEE: Piscataway, NJ, USA, 2018. [Google Scholar]
- Pecoraro, G.; Di Domenico, S.; Cianca, E.; De Sanctis, M. CSI-based fingerprinting for indoor localization using LTE signals. EURASIP J. Adv. Signal Process. 2018, 2018, 49. [Google Scholar] [CrossRef] [Green Version]
- Cianca, E.; Pecoraro, G.; De Sanctis, M.; Di Domenico, S. LTE signal fingerprinting device-free passive localization in changing environments. J. Mob. Multimed. 2019, 15, 141–162. [Google Scholar] [CrossRef]
- Li, N.; Becerik-Gerber, B. Performance-based evaluation of RFID-based indoor location sensing solutions for the built environment. Adv. Eng. Inform. 2011, 25, 535–546. [Google Scholar] [CrossRef]
- Filippoupolitis, A.; Oliff, W.; Loukas, G. Bluetooth low energy based occupancy detection for emergency management. In Proceedings of the 2016 15th International Conference on Ubiquitous Computing and Communications and 2016 International Symposium on Cyberspace and Security (IUCC-CSS), Granada, Spain, 14–16 December 2016; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar]
- Santoso, F.; Redmond, S.J. Indoor location-aware medical systems for smart homecare and telehealth monitoring: State-of-the-art. Physiol. Meas. 2015, 36, R53. [Google Scholar] [CrossRef] [PubMed]
- Sugino, K.; Katayama, S.; Niwa, Y.; Shiramatsu, S.; Ozono, T.; Shintani, T. A bluetooth-based device-free motion detector for a remote elder care support system. In Proceedings of the 2015 IIAI 4th International Congress on Advanced Applied Informatics, Okayama, Japan, 12–16 July 2015; IEEE: Piscataway, NJ, USA, 2015. [Google Scholar]
- Fujihara, A.; Yanagizawa, T. Proposing an extended iBeacon system for indoor route guidance. In Proceedings of the 2015 International Conference on Intelligent Networking and Collaborative Systems, Taipei, Taiwan, 2–4 September 2015; IEEE: Piscataway, NJ, USA, 2015. [Google Scholar]
- Alam, M.A.U.; Pathak, N.; Roy, N. Mobeacon: An iBeacon-Assisted SmartphoneBased Real Time Activity Recognition Framework. UMBC Stud. Collect. 2015, 130–139. [Google Scholar] [CrossRef] [Green Version]
- Filippoupolitis, A.; Oliff, W.; Loukas, G. Occupancy detection for building emergency management using BLE beacons. In International Symposium on Computer and Information Sciences; Czachórski, T., Gelenbe, E., Grochla, K., Lent, R., Eds.; Springer: Cham, Switzerland, 2016. [Google Scholar]
- Tekler, Z.D.; Low, R.; Gunay, B.; Andersen, R.K.; Blessing, L. A scalable Bluetooth Low Energy approach to identify occupancy patterns and profiles in office spaces. Build. Environ. 2020, 171, 106681. [Google Scholar] [CrossRef]
- Tekler, Z.D.; Low, R.; Blessing, L. An alternative approach to monitor occupancy using bluetooth low energy technology in an office environment. In Journal of Physics: Conference Series; IOP Publishing: Bristol, UK, 2019. [Google Scholar]
- Zhang, G.; Vahia, I.V.; Liu, Y.; Yang, Y.; May, R.; Cray, H.V.; McGrory, W.; Katabi, D. Contactless In-Home Monitoring of the Long-Term Respiratory and Behavioral Phenotypes in Older Adults With COVID-19: A Case Series. Front. Psychiatry 2021, 12, 754169. [Google Scholar] [CrossRef]
- Adib, F.; Kabelac, Z.; Katabi, D. Multi-Person Localization via RF Body Reflections. In Proceedings of the 12th USENIX Symposium on Networked Systems Design and Implementation (NSDI 15), Oakland, CA, USA, 4–6 May 2015. [Google Scholar]
- Adib, F.; Mao, H.; Kabelac, Z.; Katabi, D.; Miller, R.C. adibadi breathing and heart rate. In Proceedings of the 33rd Annual ACM Conference on Human Factors in Computing Systems, Seoul, Korea, 18 April 2015. [Google Scholar]
- Shaban, H.A.; El-Nasr, M.A.; Buehrer, R.M. Toward a highly accurate ambulatory system for clinical gait analysis via UWB radios. IEEE Trans. Inf. Technol. Biomed. 2009, 14, 284–291. [Google Scholar] [CrossRef]
- Hsu, C.Y.; Ahuja, A.; Yue, S.; Hristov, R.; Kabelac, Z.; Katabi, D. Zero-effort in-home sleep and insomnia monitoring using radio signals. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2017, 1, 1–18. [Google Scholar] [CrossRef]
- Li, C.; Lubecke, V.M.; Boric-Lubecke, O.; Lin, J. A review on recent advances in Doppler radar sensors for noncontact healthcare monitoring. IEEE Trans. Microw. Theory Tech. 2013, 61, 2046–2060. [Google Scholar] [CrossRef]
- Yue, S.; He, H.; Wang, H.; Rahul, H.; Katabi, D. Extracting multi-person respiration from entangled RF signals. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2018, 2, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Zou, Y.; Wang, G.; Wu, K.; Ni, L.M. SmartScanner: Know more in walls with your smartphone! IEEE Trans. Mob. Comput. 2015, 15, 2865–2877. [Google Scholar] [CrossRef]
- He, S.; Shin, K.G. Geomagnetism for smartphone-based indoor localization: Challenges, advances, and comparisons. ACM Comput. Surv. 2017, 50, 1–37. [Google Scholar] [CrossRef]
- Santos, R.; Barandas, M.; Leonardo, R.; Gamboa, H. Fingerprints and Floor Plans Construction for Indoor Localisation Based on Crowdsourcing. Sensors 2019, 19, 919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, C.; Subbu, K.P.; Luo, J.; Wu, J. GROPING: Geomagnetism and crowdsensing powered indoor navigation. IEEE Trans. Mob. Comput. 2014, 14, 387–400. [Google Scholar] [CrossRef]
- Shu, Y.; Bo, C.; Shen, G.; Zhao, C.; Li, L.; Zhao, F. Magicol: Indoor localization using pervasive magnetic field and opportunistic WiFi sensing. IEEE J. Sel. Areas Commun. 2015, 33, 1443–1457. [Google Scholar] [CrossRef]
- Davidson, P.; Takala, J. Algorithm for pedestrian navigation combining IMU measurements and gait models. Gyroscopy Navig. 2013, 4, 79–84. [Google Scholar] [CrossRef]
- Zheng, L.; Zhou, W.; Tang, W.; Zheng, X.; Peng, A.; Zheng, H. A 3D indoor positioning system based on low-cost MEMS sensors. Simul. Model. Pract. Theory 2016, 65, 45–56. [Google Scholar] [CrossRef]
- Chung, J.; Donahoe, M.; Schmandt, C.; Kim, I.J.; Razavai, P.; Wiseman, M. Indoor location sensing using geo-magnetism. In Proceedings of the 9th International Conference on Mobile Systems, Applications, and Services, Bethesda, MD, USA, 28 June 2011. [Google Scholar]
- Infrastructure, L.E.C.; Layer, M.L.P. Ieee Standard for Low-Rate Wireless Networks. IEEE Stand. 2015, 2015, 1–708. [Google Scholar]
- Pirch, H.-J.; Global, H.; Leong, F. Introduction to Impulse Radio UWB Seamless Access Systems. In Proceedings of the Fraunhofer SIT ID:SMART Worksho, Darmstadt, Germany, 19–20 February 2020. [Google Scholar]
- Rüdiger, M.; Maria, F.; Rodney, C.; Adele, G.; Kari, J.; Carmela, M.; Richard, S.; Karl, S.; Pier, S.; Stuck, B.E.; et al. (International Commission on Non-Ionizing Radiation Protection). ICNIRP Guidelines for Limiting Exposure to Electric Fields Induced by Movement of the Human Body in a Static Magnetic Field and by Time-Varying Magnetic Fields below 1 Hz. Health Phys. 2014, 106, 418–425. [Google Scholar]
- Federal Communications Commission. FCC 02-48—Revision of Part 15 of the Commission’s Rules Regarding Ultra-Wideband Transmission Systems, FIRST REPORT AND ORDER. 2002. Available online: http://www.fcc.gov/Bureaus/Engineering_Technology/Orders/2002/fcc02048.pdf (accessed on 1 October 2022).
- Cavagnaro, M.; Pisa, S.; Pittella, E. Safety aspects of human exposure to ultra wideband radar fields. In Proceedings of the International Symposium on Electromagnetic Compatibility-EMC EUROPE, Rome, Italy, 17–21 September 2012; IEEE: Piscataway, NJ, USA, 2012. [Google Scholar]
- Ali, A.M.; Al Ghamdi, M.A.; Iqbal, M.M.; Khalid, S.; Aldabbas, H.; Saeed, S. Next-generation UWB antennas gadgets for human health care using SAR. EURASIP J. Wirel. Commun. Netw. 2021, 2021, 33. [Google Scholar] [CrossRef]
- Mahmood, T.; Mahmood, O.A.; L-Qaysi, H.K.A. An Improvement the Channel Characteristics Performance of Ultra-Wideband (UWB) by Controlling the Main Channel Parameters. Des. Eng. 2021, 2021, 1329–1340. [Google Scholar]
- Halder, S.; Ghosal, A. A survey on mobility-assisted localization techniques in wireless sensor networks. J. Netw. Comput. Appl. 2016, 60, 82–94. [Google Scholar]
- Oguntala, G.; Abd-Alhameed, R.; Jones, S.; Noras, J.; Patwary, M.; Rodriguez, J. Indoor location identification technologies for real-time IoT-based applications: An inclusive survey. Comput. Sci. Rev. 2018, 30, 55–79. [Google Scholar] [CrossRef]
- Alarifi, A.; Al-Salman, A.; Alsaleh, M.; Alnafessah, A.; Al-Hadhrami, S.; Al-Ammar, M.A.; Al-Khalifa, H.S. Ultra wideband indoor positioning technologies: Analysis and recent advances. Sensors 2016, 16, 707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gigl, T.; Janssen, G.J.; Dizdarevic, V.; Witrisal, K.; Irahhauten, Z. Analysis of a UWB indoor positioning system based on received signal strength. In Proceedings of the 2007 4th Workshop on Positioning, Navigation and Communication, Hannover, Germany, 22 March 2007; IEEE: Piscataway, NJ, USA, 2007. [Google Scholar]
- Cheng, G. Accurate TOA-based UWB localization system in coal mine based on WSN. Phys. Procedia 2012, 24, 534–540. [Google Scholar] [CrossRef] [Green Version]
- Segura, M.; Mut, V.; Sisterna, C. Ultra wideband indoor navigation system. IET Radar Sonar Navig. 2012, 6, 402–411. [Google Scholar] [CrossRef]
- Fischer, G.; Klymenko, O.; Martynenko, D.; Luediger, H. An impulse radio UWB transceiver with high-precision TOA measurement unit. In Proceedings of the 2010 International Conference on Indoor Positioning and Indoor Navigation, Zurich, Switzerland, 15–17 September 2010; IEEE: Piscataway, NJ, USA, 2010. [Google Scholar]
- Krishnan, S.; Sharma, P.; Guoping, Z.; Woon, O.H. A UWB based localization system for indoor robot navigation. In Proceedings of the 2007 IEEE International Conference on Ultra-Wideband, Singapore, 24–26 September 2007; IEEE: Piscataway, NJ, USA, 2007. [Google Scholar]
- Rowe, N.C.; Fathy, A.E.; Kuhn, M.J.; Mahfouz, M.R. A UWB transmit-only based scheme for multi-tag support in a millimeter accuracy localization system. In Proceedings of the 2013 IEEE Topical Conference on Wireless Sensors and Sensor Networks (WiSNet), Austin, TX, USA, 20–23 January 2013; IEEE: Piscataway, NJ, USA, 2013. [Google Scholar]
- Lee, Y.U. Weighted-average based aoa parameter estimations for LR-UWB wireless positioning system. IEICE Trans. Commun. 2011, 94, 3599–3602. [Google Scholar] [CrossRef]
- Subramanian, A. UWB linear quadratic frequency domain frequency invariant beamforming and angle of arrival estimation. In Proceedings of the 2007 IEEE 65th Vehicular Technology Conference-VTC2007-Spring, Dublin, Ireland, 22–25 April 2007; IEEE: Piscataway, NJ, USA, 2007. [Google Scholar]
- Gezici, S.; Tian, Z.; Giannakis, G.B.; Kobayashi, H.; Molisch, A.F.; Poor, H.V.; Sahinoglu, Z. Localization via ultra-wideband radios: A look at positioning aspects for future sensor networks. IEEE Signal Process. Mag. 2005, 22, 70–84. [Google Scholar] [CrossRef]
- Chong, C.-C.; Watanabe, F.; Win, M.Z. Effect of bandwidth on UWB ranging error. In Proceedings of the 2007 IEEE Wireless Communications and Networking Conference, Hong Kong, China, 11–15 March 2007; IEEE: Piscataway, NJ, USA, 2007. [Google Scholar]
- Win, Z.M.; Scholtz, R.A. Impulse radio: How it works. IEEE Commun. Lett. 1998, 2, 36–38. [Google Scholar] [CrossRef]
- Molisch, A.F. Ultra-wide-band propagation channels. Proc. IEEE 2009, 97, 353–371. [Google Scholar] [CrossRef]
- Yang, X. NLOS mitigation for UWB localization based on sparse pseudo-input Gaussian process. IEEE Sens. J. 2018, 18, 4311–4316. [Google Scholar] [CrossRef]
- Xu, Y.; Shmaliy, Y.S.; Ahn, C.K.; Tian, G.; Chen, X. Robust and accurate UWB-based indoor robot localisation using integrated EKF/EFIR filtering. IET Radar Sonar Navig. 2018, 12, 750–756. [Google Scholar] [CrossRef]
- Ridolfi, M.; Vandermeeren, S.; Defraye, J.; Steendam, H.; Gerlo, J.; De Clercq, D.; Hoebeke, J.; De Poorter, E. Experimental evaluation of UWB indoor positioning for sport postures. Sensors 2018, 18, 168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Minne, K.; Macoir, N.; Rossey, J.; Van den Brande, Q.; Lemey, S.; Hoebeke, J.; De Poorter, E. Experimental evaluation of UWB indoor positioning for indoor track cycling. Sensors 2019, 19, 2041. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Sanctis, M.; Conte, A.; Rossi, T.; Di Domenico, S.; Cianca, E. CIR-Based Device-Free People Counting via UWB Signals. Sensors 2021, 21, 3296. [Google Scholar] [CrossRef] [PubMed]
- Di Domenico, S.; Pecoraro, G.; Cianca, E.; De Sanctis, M. Trained-once device-free crowd counting and occupancy estimation using WiFi: A Doppler spectrum based approach. In Proceedings of the 2016 IEEE 12th International Conference on Wireless and Mobile Computing, Networking and Communications (WiMob), New York, NY, USA, 17–19 October 2016; IEEE: Piscataway, NJ, USA, 2016. [Google Scholar]
- Kilic, Y.; Wymeersch, H.; Meijerink, A.; Bentum, M.J.; Scanlon, W.G. Device-free person detection and ranging in UWB networks. IEEE J. Sel. Top. Signal Process. 2013, 8, 43–54. [Google Scholar] [CrossRef]
- Nguyen, V.-H.; Pyun, J.-Y. Location detection and tracking of moving targets by a 2D IR-UWB radar system. Sensors 2015, 15, 6740–6762. [Google Scholar] [CrossRef] [Green Version]
- Cimdins, M.; Schmidt, S.O.; Hellbrück, H. MAMPI-UWB—Multipath-assisted device-free localization with magnitude and phase information with UWB transceivers. Sensors 2020, 20, 7090. [Google Scholar] [CrossRef]
- Bregar, K.; Hrovat, A.; Mohorčič, M.; Javornik, T. Self-Calibrated UWB based device-free indoor localization and activity detection approach. In Proceedings of the 2020 European Conference on Networks and Communications (EuCNC), Dubrovnik, Croatia, 15–18 June 2020; pp. 176–181. [Google Scholar]
- Choi, J.W.; Yim, D.H.; Cho, S.H. People counting based on an IR-UWB radar sensor. IEEE Sens. J. 2017, 17, 5717–5727. [Google Scholar] [CrossRef]
- Bartoletti, S.; Conti, A.; Win, M.Z. Device-free counting via wideband signals. IEEE J. Sel. Areas Commun. 2017, 35, 1163–1174. [Google Scholar] [CrossRef]
- Yang, X.; Yin, W.; Li, L.; Zhang, L. Dense people counting using IR-UWB radar with a hybrid feature extraction method. IEEE Geosci. Remote Sens. Lett. 2018, 16, 30–34. [Google Scholar] [CrossRef] [Green Version]
- Mohammadmoradi, H.; Yin, S.; Gnawali, O. Room occupancy estimation through WiFi, UWB, and light sensors mounted on doorways. In Proceedings of the 2017 International Conference on Smart Digital Environment, Rabat, Morocco, 21 July 2017; pp. 27–34. [Google Scholar]
- Bouchard, K.; Maitre, J.; Bertuglia, C.; Gaboury, S. Activity recognition in smart homes using UWB radars. Procedia Comput. Sci. 2020, 170, 10–17. [Google Scholar] [CrossRef]
- Ahmed, S.; Cho, S.H. Hand gesture recognition using an IR-UWB radar with an inception module-based classifier. Sensors 2020, 20, 564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallesen, S.; Grønli, J.; Myhre, K.; Moen, F.; Bjorvatn, B.; Hanssen, I.; Heglum, H.S.A. A pilot study of impulse radio ultra wideband radar technology as a new tool for sleep assessment. J. Clin. Sleep Med. 2018, 14, 1249–1254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nathanson, F.E.; Reilly, J.P.; Cohen, M.N. Radar design principles-Signal processing and the Environment. NASA STI/Recon Tech. Rep. A 1991, 91, 46747. [Google Scholar]
- Corrales, J.A.; Candelas, F.A.; Torres, F. Hybrid tracking of human operators using IMU/UWB data fusion by a Kalman filter. In Proceedings of the 2008 3rd ACM/IEEE International Conference on Human-Robot Interaction (HRI), Amsterdam, The Netherlands, 12–15 March 2008; pp. 193–200. [Google Scholar]
- Wang, Y.; Li, X. The IMU/UWB fusion positioning algorithm based on a particle filter. ISPRS Int. J. Geo-Inf. 2017, 6, 235. [Google Scholar] [CrossRef] [Green Version]
- Ayena, J.C.; Chioukh, L.; Otis, M.J.-D.; Deslandes, D. Risk of falling in a timed up and go test using an UWB radar and an instrumented insole. Sensors 2021, 21, 722. [Google Scholar] [CrossRef]
- Murata, M.; Ahmetovic, D.; Sato, D.; Takagi, H.; Kitani, K.M.; Asakawa, C. Smartphone-based localization for blind navigation in building-scale indoor environments. Pervasive Mob. Comput. 2019, 57, 14–32. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Zhao, Q.; Li, Y.; Niu, X.; Zhuang, Y.; Liu, J. Collaborative WiFi fingerprinting using sensor-based navigation on smartphones. Sensors 2015, 15, 17534–17557. [Google Scholar] [CrossRef]
- Shi, Q.; Zhao, S.; Cui, X.; Lu, M.; Jia, M. Anchor self-localization algorithm based on UWB ranging and inertial measurements. Tsinghua Sci. Technol. 2019, 24, 728–737. [Google Scholar]
- Zhong, S.; Zhang, K.; Zhu, G.; Liu, S. UWB-Inertial Fusion Location Algorithm Based on Kalman Filtering. In Proceedings of the 2018 15th International Conference on Control, Automation, Robotics and Vision (ICARCV), Singapore, 18–21 November 2018; pp. 574–578. [Google Scholar]
- Chen, S.W.; Lin, S.H.; Liao, L.D.; Lai, H.Y.; Pei, Y.C.; Kuo, T.S.; Lin, C.T.; Chang, J.Y.; Chen, Y.Y.; Lo, Y.C.; et al. Quantification and recognition of parkinsonian gait from monocular video imaging using kernel-based principal component analysis. Biomed. Eng. Online 2011, 10, 99. [Google Scholar] [CrossRef] [Green Version]
- Mahfouz, M.R.; Kuhn, M.J.; To, G.; Fathy, A.E. Integration of UWB and wireless pressure mapping in surgical navigation. IEEE Trans. Microw. Theory Tech. 2009, 57, 2550–2564. [Google Scholar]
- Qi, Y.; Soh, C.B.; Gunawan, E.; Low, K.-S.; Maskooki, A. Using wearable UWB radios to measure foot clearance during walking. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 5199–5202. [Google Scholar]
- Rana, S.P.; Dey, M.; Ghavami, M.; Dudley, S. ITERATOR: A 3D gait identification from IR-UWB technology. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 782–787. [Google Scholar]
- Pfister, A.; West, A.M.; Bronner, S.; Noah, J.A. Comparative abilities of Microsoft Kinect and Vicon 3D motion capture for gait analysis. J. Med. Eng. Technol. 2014, 38, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Koo, Y.S.; Ren, L.; Wang, Y.; Fathy, A.E. UWB MicroDoppler Radar for human Gait analysis, tracking more than one person, and vital sign detection of moving persons. In Proceedings of the 2013 IEEE MTT-S International Microwave Symposium Digest (MTT), Seattle, WA, USA, 2–7 June 2013; pp. 1–4. [Google Scholar]
- Wang, F.; Skubic, M.; Rantz, M.; Cuddihy, P.E. Quantitative gait measurement with pulse-Doppler radar for passive in-home gait assessment. IEEE Trans. Biomed. Eng. 2014, 61, 2434–2443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saho, K.; Uemura, K.; Sugano, K.; Matsumoto, M. Using micro-Doppler radar to measure gait features associated with cognitive functions in elderly adults. IEEE Access 2019, 7, 24122–24131. [Google Scholar] [CrossRef]
- Hsu, C.-Y.; Liu, Y.; Kabelac, Z.; Hristov, R.; Katabi, D.; Liu, C. Extracting gait velocity and stride length from surrounding radio signals. In Proceedings of the 2017 CHI Conference on Human Factors in Computing Systems, Denver, CA, USA, 6–11 May 2017; pp. 2116–2126. [Google Scholar]
- Fan, L.; Li, T.; Yuan, Y.; Katabi, D. In-home daily-life captioning using radio signals. In Proceedings of the European Conference on Computer Vision, Glasgow, UK, 23–28 August 2020; Springer: Berlin/Heidelberg, Germany, 2020; pp. 105–123. [Google Scholar]
- Zhao, M.; Li, T.; Abu Alsheikh, M.; Tian, Y.; Zhao, H.; Torralba, A.; Katabi, D. Through-wall human pose estimation using radio signals. In Proceedings of the IEEE Conference on Computer Vision and Pattern Recognition, Salt Lake City, UT, USA, 18–23 June 2018; pp. 7356–7365. [Google Scholar]
- Zhao, M.; Tian, Y.; Zhao, H.; Alsheikh, M.A.; Li, T.; Hristov, R.; Kabelac, Z.; Katabi, D.; Torralba, A. RF-based 3D skeletons. In Proceedings of the 2018 Conference of the ACM Special Interest Group on Data Communication, Budapest, Hungary, 7 August 2018; pp. 267–281. [Google Scholar]
- Li, T.; Fan, L.; Zhao, M.; Liu, Y.; Katabi, D. Making the invisible visible: Action recognition through walls and occlusions. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Seoul, Korea, 27–28 October 2019; pp. 872–881. [Google Scholar]
- Zhao, M.; Liu, Y.; Raghu, A.; Li, T.; Zhao, H.; Torralba, A.; Katabi, D. Through-wall human mesh recovery using radio signals. In Proceedings of the IEEE/CVF International Conference on Computer Vision, Seoul, Korea, 27 October 2019–2 November 2019; pp. 10113–10122. [Google Scholar]
- Sun, M.; Wang, Y.; Xu, S.; Cao, H.; Si, M. Indoor positioning integrating PDR/geomagnetic positioning based on the genetic-particle filter. Appl. Sci. 2020, 10, 668. [Google Scholar]
- Ashraf, I.; Hur, S.; Shafiq, M.; Park, Y. Floor identification using magnetic field data with smartphone sensors. Sensors 2019, 19, 2538. [Google Scholar]
- Mastorakis, G.; Makris, D. Fall detection system using Kinect’s infrared sensor. J. Real-Time Image Process. 2014, 9, 635–646. [Google Scholar] [CrossRef]
- Bevilacqua, V.; Nuzzolese, N.; Barone, D.; Pantaleo, M.; Suma, M.; D’Ambruoso, D.; Volpe, A.; Loconsole, C.; Stroppa, F. Fall detection in indoor environment with kinect sensor. In Proceedings of the 2014 IEEE International Symposium on Innovations in Intelligent Systems and Applications (INISTA) Proceedings, Alberobello, Italy, 23–25 June 2014; pp. 319–324. [Google Scholar]
- Nghiem, A.T.; Auvinet, E.; Meunier, J. Head detection using kinect camera and its application to fall detection. In Proceedings of the 2012 11th International Conference on Information Science, Signal Processing and Their Applications (ISSPA), Montreal, QC, Canada, 2–5 July 2015; pp. 164–169. [Google Scholar]
- Zhang, Z.; Liu, W.; Metsis, V.; Athitsos, V. A viewpoint-independent statistical method for fall detection. In Proceedings of the 21st International Conference on Pattern Recognition (ICPR2012), Tsukuba, Japan, 11–15 November 2012; pp. 3626–3630. [Google Scholar]
- Dubois, A.; Charpillet, F. Human activities recognition with RGB-Depth camera using HMM. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 4666–4669. [Google Scholar]
- Planinc, R.; Kampel, M. Introducing the use of depth data for fall detection. Pers. Ubiquitous Comput. 2013, 17, 1063–1072. [Google Scholar]
- Feng, G.; Mai, J.; Ban, Z.; Guo, X.; Wang, G. Floor pressure imaging for fall detection with fiber-optic sensors. IEEE Pervasive Comput. 2016, 15, 40–47. [Google Scholar] [CrossRef]
- Droghini, D.; Ferretti, D.; Principi, E.; Squartini, S.; Piazza, F. A combined one-class SVM and template-matching approach for user-aided human fall detection by means of floor acoustic features. Comput. Intell. Neurosci. 2017, 2017, 1512670. [Google Scholar]
- Mokhtari, G.; Aminikhanghahi, S.; Zhang, Q.; Cook, D.J. Fall detection in smart home environments using UWB sensors and unsupervised change detection. J. Reliab. Intell. Environ. 2018, 4, 131–139. [Google Scholar] [CrossRef]
- Han, T.; Kang, W.; Choi, G. IR-UWB sensor based fall detection method using CNN algorithm. Sensors 2020, 20, 5948. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Liu, M.; Wang, N.; Wang, L.; Yang, Y.; Wang, H. Room-level fall detection based on ultra-wideband (UWB) monostatic radar and convolutional long short-term memory (LSTM). Sensors 2020, 20, 1105. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salarian, A.; Russmann, H.; Wider, C.; Burkhard, P.R.; Vingerhoets, F.J.; Aminian, K. Quantification of tremor and bradykinesia in Parkinson’s disease using a novel ambulatory monitoring system. IEEE Trans. Biomed. Eng. 2007, 54, 313–322. [Google Scholar] [CrossRef] [PubMed]
- Uhríková, Z.; Šprdlík, O.; Hoskovcová, M.; Komárek, A.; Ulmanová, O.; Hlaváč, V.; Nugent, C.D.; Růžička, E. Validation of a new tool for automatic assessment of tremor frequency from video recordings. J. Neurosci. Methods 2011, 198, 110–113. [Google Scholar] [CrossRef]
- Bortone, I.; Buongiorno, D.; Lelli, G.; Di Candia, A.; Cascarano, G.D.; Trotta, G.F.; Fiore, P.; Bevilacqua, V. Gait analysis and parkinson’s disease: Recent trends on main applications in healthcare. In Proceedings of the International Conference on NeuroRehabilitation, Pisa, Italy, 16–20 October 2018; Springer: Cham, Switzerland, 2018; pp. 1121–1125. [Google Scholar]
- Green, R.D.; Guan, L. Quantifying and recognizing human movement patterns from monocular video images-part I: A new framework for modeling human motion. IEEE Trans. Circuits Syst. Video Technol. 2004, 14, 179–190. [Google Scholar] [CrossRef]
- Jobbagy, A.; Hamar, G. PAM: Passive marker-based analyzer to test patients with neural diseases. In Proceedings of the 26th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, San Francisco, CA, USA, 1–5 September 2004; pp. 4751–4754. [Google Scholar]
- Peikon, I.D.; Fitzsimmons, N.A.; Lebedev, M.A.; Nicolelis, M.A. Three-dimensional, automated, real-time video system for tracking limb motion in brain–machine interface studies. J. Neurosci. Methods 2009, 180, 224–233. [Google Scholar] [CrossRef]
- Uhríková, Z.; Sprdlik, O.; Hlavác, V.; Ruzicka, E. Action tremor analysis from ordinary video sequence. In Proceedings of the 2009 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009; pp. 6123–6126. [Google Scholar]
- Oikonomidis, I.; Kyriazis, N.; Argyros, A.A. Efficient model-based 3D tracking of hand articulations using Kinect. In Proceedings of the British Machine Vision Conference, University of Dundee, Scotland, UK, 29 August 2011–2 September 2011; BMVA Press: Durham, UK, 2011; p. 3. [Google Scholar]
- Grimaldi, G.; Manto, M. Neurological tremor: Sensors, signal processing and emerging applications. Sensors 2010, 10, 1399–1422. [Google Scholar] [CrossRef]
- Djurić-Jovičić, M.D.; Jovičić, N.S.; Popović, D.B. Kinematics of gait: New method for angle estimation based on accelerometers. Sensors 2011, 11, 10571–10585. [Google Scholar] [CrossRef] [Green Version]
- Du, H.; Henry, P.; Ren, X.; Cheng, M.; Goldman, D.B.; Seitz, S.M.; Fox, D. Interactive 3D modeling of indoor environments with a consumer depth camera. In Proceedings of the 13th International Conference on Ubiquitous Computing, Beijing, China, 17–21 September 2011; pp. 75–84. [Google Scholar]
- Blumrosen, G.; Uziel, M.; Rubinsky, B.; Porrat, D. Tremor acquisition system based on UWB Wireless Sensor Network. In Proceedings of the 2010 International Conference on Body Sensor Networks, Singapore, 7–9 June 2010; pp. 187–193. [Google Scholar]
- Blumrosen, G.; Uziel, M.; Rubinsky, B.; Porrat, D. Noncontact tremor characterization using low-power wideband radar technology. IEEE Trans. Biomed. Eng. 2011, 59, 674–686. [Google Scholar] [CrossRef]
- Schleicher, B.; Nasr, I.; Trasser, A.; Schumacher, H. IR-UWB radar demonstrator for ultra-fine movement detection and vital-sign monitoring. IEEE Trans. Microw. Theory Tech. 2013, 61, 2076–2085. [Google Scholar] [CrossRef] [Green Version]
- Regev, N.; Wulich, D. Multi-modal, remote breathing monitor. Sensors 2020, 20, 1229. [Google Scholar] [CrossRef] [PubMed]
- Khan, F.; Ghaffar, A.; Khan, N.; Cho, S.H. An overview of signal processing techniques for remote health monitoring using impulse radio UWB transceiver. Sensors 2020, 20, 2479. [Google Scholar] [CrossRef] [PubMed]
- Caro, C.; Bloice, J. Contactless apnoea detector based on radar. Lancet 1971, 298, 959–961. [Google Scholar] [CrossRef]
- Lin, J.C. Noninvasive microwave measurement of respiration. Proc. IEEE 1975, 63, 1530. [Google Scholar] [CrossRef]
- Staderini, E.M. UWB radars in medicine. IEEE Aerosp. Electron. Syst. Mag. 2002, 17, 13–18. [Google Scholar]
- Lin, J.C. Microwave sensing of physiological movement and volume change: A review. Bioelectromagnetics 1992, 13, 557–565. [Google Scholar] [CrossRef]
- Li, C.; Lin, J. Random body movement cancellation in Doppler radar vital sign detection. IEEE Trans. Microw. Theory Tech. 2008, 56, 3143–3152. [Google Scholar]
- Hu, X.; Jin, T. Short-range vital signs sensing based on EEMD and CWT using IR-UWB radar. Sensors 2016, 16, 2025. [Google Scholar]
- Kranjec, J.; Beguš, S.; Geršak, G.; Drnovšek, J. Non-contact heart rate and heart rate variability measurements: A review. Biomed. Signal Process. Control 2014, 13, 102–112. [Google Scholar] [CrossRef]
- Li, F.; Valero, M.; Shahriar, H.; Khan, R.A.; Ahamed, S.I. Wi-COVID: A COVID-19 symptom detection and patient monitoring framework using WiFi. Smart Health 2021, 19, 100147. [Google Scholar] [CrossRef]
- Saeed, U.; Shah, S.Y.; Ahmad, J.; Imran, M.A.; Abbasi, Q.H.; Shah, S.A. Machine learning empowered COVID-19 patient monitoring using non-contact sensing: An extensive review. J. Pharm. Anal. 2022, 12, 193–204. [Google Scholar] [CrossRef]
- Zhao, M.; Yue, S.; Katabi, D.; Jaakkola, T.S.; Bianchi, M.T. Learning sleep stages from radio signals: A conditional adversarial architecture. In Proceedings of the International Conference on Machine Learning, Sydney, Australia, 6–11 August 2017; pp. 4100–4109. [Google Scholar]
- Chang, K.-M.; Liu, S.-H. Wireless portable electrocardiogram and a tri-axis accelerometer implementation and application on sleep activity monitoring. Telemed. E-Health 2011, 17, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H.J.; Hwang, S.H.; Lee, S.M.; Lim, Y.G.; Park, K.S. Estimation of body postures on bed using unconstrained ECG measurements. IEEE J. Biomed. Health Inform. 2013, 17, 985–993. [Google Scholar] [PubMed]
- Yoon, H.; Hwang, S.; Jung, D.; Choi, S.; Joo, K.; Choi, J.; Lee, Y.; Jeong, D.-U.; Park, K. Estimation of sleep posture using a patch-type accelerometer based device. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 4942–4945. [Google Scholar]
- Akbarian, S.; Delfi, G.; Zhu, K.; Yadollahi, A.; Taati, B. Automated non-contact detection of head and body positions during sleep. IEEE Access 2019, 7, 72826–72834. [Google Scholar] [CrossRef]
- Grimm, T.; Martinez, M.; Benz, A.; Stiefelhagen, R. Sleep position classification from a depth camera using bed aligned maps. In Proceedings of the 2016 23rd International Conference on Pattern Recognition (ICPR), Cancun, Mexico, 4–8 December 2016; IEEE: Piscataway, NJ, USA, 2016; pp. 319–324. [Google Scholar]
- Liu, S.; Ostadabbas, S. A vision-based system for in-bed posture tracking. In Proceedings of the IEEE International Conference on Computer Vision Workshops, Venice, Italy, 22–29 October 2017; pp. 1373–1382. [Google Scholar]
- Barsocchi, P. Position recognition to support bedsores prevention. IEEE J. Biomed. Health Inform. 2012, 17, 53–59. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Chen, Y.; Wang, Y.; Chen, X.; Cheng, J.; Yang, J. Monitoring vital signs and postures during sleep using WiFi signals. IEEE Internet Things J. 2018, 5, 2071–2084. [Google Scholar] [CrossRef]
- Liu, X.; Cao, J.; Tang, S.; Wen, J. Wi-Sleep: Contactless sleep monitoring via WiFi signals. In Proceedings of the 2014 IEEE Real-Time Systems Symposium, Rome, Italy, 2–5 December 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 346–355. [Google Scholar]
- Long, X.; Yang, J.; Weysen, T.; Haakma, R.; Foussier, J.; Fonseca, P.; Aarts, R.M. Measuring dissimilarity between respiratory effort signals based on uniform scaling for sleep staging. Physiol. Meas. 2014, 35, 2529. [Google Scholar] [CrossRef] [Green Version]
- Várady, P.; Bongár, S.; Benyó, Z. Detection of airway obstructions and sleep apnea by analyzing the phase relation of respiration movement signals. IEEE Trans. Instrum. Meas. 2003, 52, 2–6. [Google Scholar]
- Almazaydeh, L.; Elleithy, K.; Faezipour, M.; Abushakra, A. Apnea detection based on respiratory signal classification. Procedia Comput. Sci. 2013, 21, 310–316. [Google Scholar]
- Yue, S.; Yang, Y.; Wang, H.; Rahul, H.; Katabi, D. Bodycompass: Monitoring sleep posture with wireless signals. Proc. ACM Interact. Mob. Wearable Ubiquitous Technol. 2020, 4, 1–25. [Google Scholar] [CrossRef]
- Carskadon, M. Normal Human Sleep: An Overview. In Principles and Practice of Sleep Medicine; Kryger, M.H., Roth, T., Dement, W.C., Eds.; Elsevier: St Louis, MO, USA, 2011. [Google Scholar]
- Lichstein, K.L.; Stone, K.C.; Donaldson, J.; Nau, S.D.; Soeffing, J.P.; Murray, D.; Lester, K.W.; Aguillard, R.N. Actigraphy validation with insomnia. Sleep 2006, 29, 232–239. [Google Scholar] [PubMed]
- Adib, F.; Kabelac, Z.; Katabi, D.; Miller, R.C. 3D tracking via body radio reflections. In Proceedings of the 11th USENIX Symposium on Networked Systems Design and Implementation (NSDI 14), Seattle, WA, USA, 2–4 April 2014; pp. 317–329. [Google Scholar]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
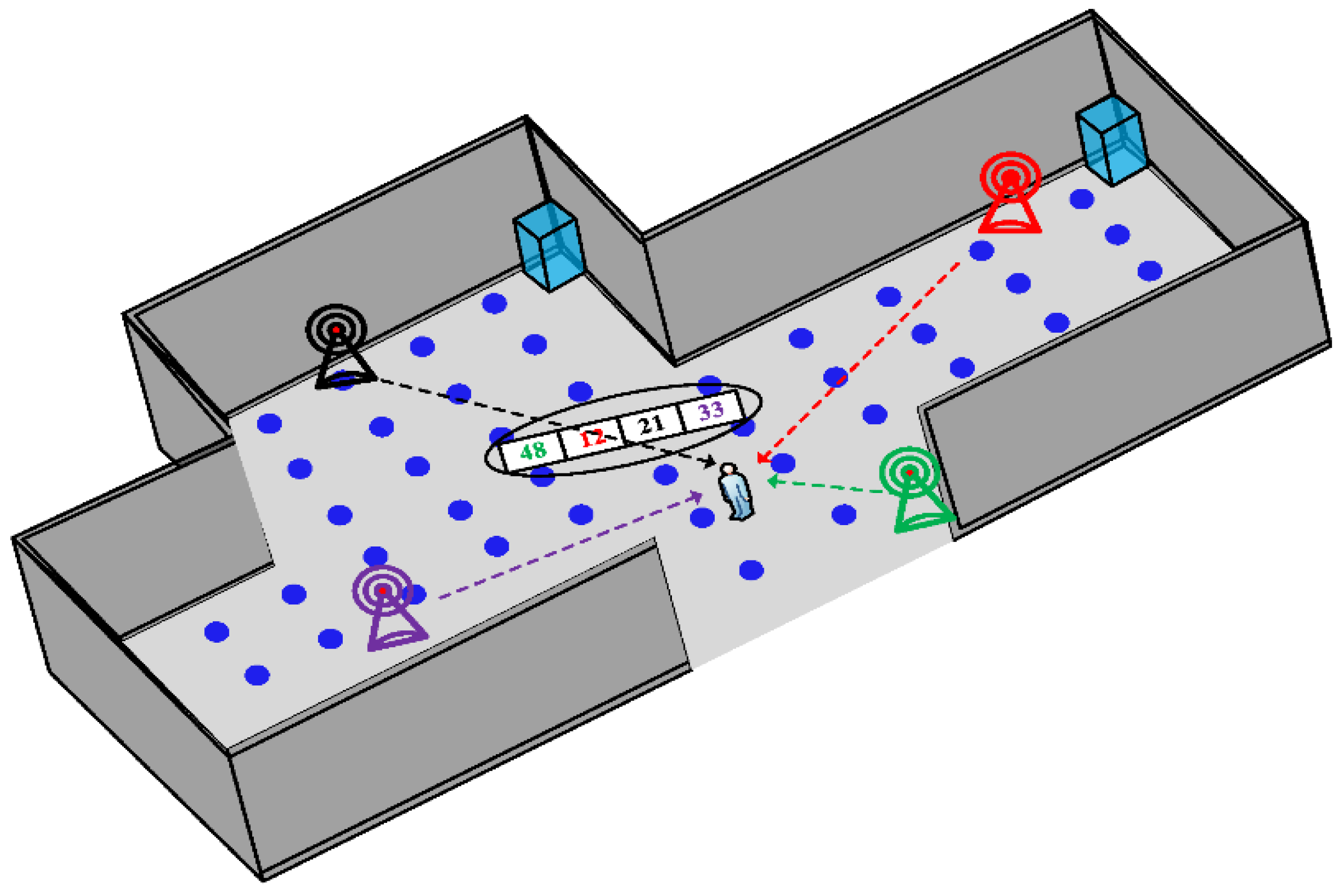
| IR-UWB Positioning Metric | Definition |
|---|---|
| Signal Strength (SS) | The target measures the signal strength for received signals from reference nodes in order to use signal strength as an estimator of the distance from them [86] |
| Time of Arrival (ToA) | The location is the intersection of circles with radius equal to the distance between the target and reference nodes and calculated as the one-way propagation time between them [87,88,89]. |
| Time Difference of Arrival (TDoA) | It is based on comparing the time difference between the target and at least three reference nodes [90,91]. |
| Angle of Arrival (AoA): | The location can be found from the intersection of the angle line for each reference node [92,93,94]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
di Biase, L.; Pecoraro, P.M.; Pecoraro, G.; Caminiti, M.L.; Di Lazzaro, V. Markerless Radio Frequency Indoor Monitoring for Telemedicine: Gait Analysis, Indoor Positioning, Fall Detection, Tremor Analysis, Vital Signs and Sleep Monitoring. Sensors 2022, 22, 8486. https://doi.org/10.3390/s22218486
di Biase L, Pecoraro PM, Pecoraro G, Caminiti ML, Di Lazzaro V. Markerless Radio Frequency Indoor Monitoring for Telemedicine: Gait Analysis, Indoor Positioning, Fall Detection, Tremor Analysis, Vital Signs and Sleep Monitoring. Sensors. 2022; 22(21):8486. https://doi.org/10.3390/s22218486
Chicago/Turabian Styledi Biase, Lazzaro, Pasquale Maria Pecoraro, Giovanni Pecoraro, Maria Letizia Caminiti, and Vincenzo Di Lazzaro. 2022. "Markerless Radio Frequency Indoor Monitoring for Telemedicine: Gait Analysis, Indoor Positioning, Fall Detection, Tremor Analysis, Vital Signs and Sleep Monitoring" Sensors 22, no. 21: 8486. https://doi.org/10.3390/s22218486