
How Does Added Mass Affect the Gait of Middle-Aged Adults? An Assessment Using Statistical Parametric Mapping




Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection and Processing
2.3. Data Analysis
2.3.1. Joint Kinematics and Kinetics
2.3.2. Muscle Activity
2.3.3. Statistical Parametric Mapping
3. Results
3.1. Overall Response of Young Adults to Pelvis Mass Increases
3.2. Overall Response of Middle-Aged Adults to Pelvis Mass Increases
3.3. Overall Response of Young Adults to Thigh Mass Increases
3.4. Overall Response of Middle-Aged Adults to Thigh Mass Increases
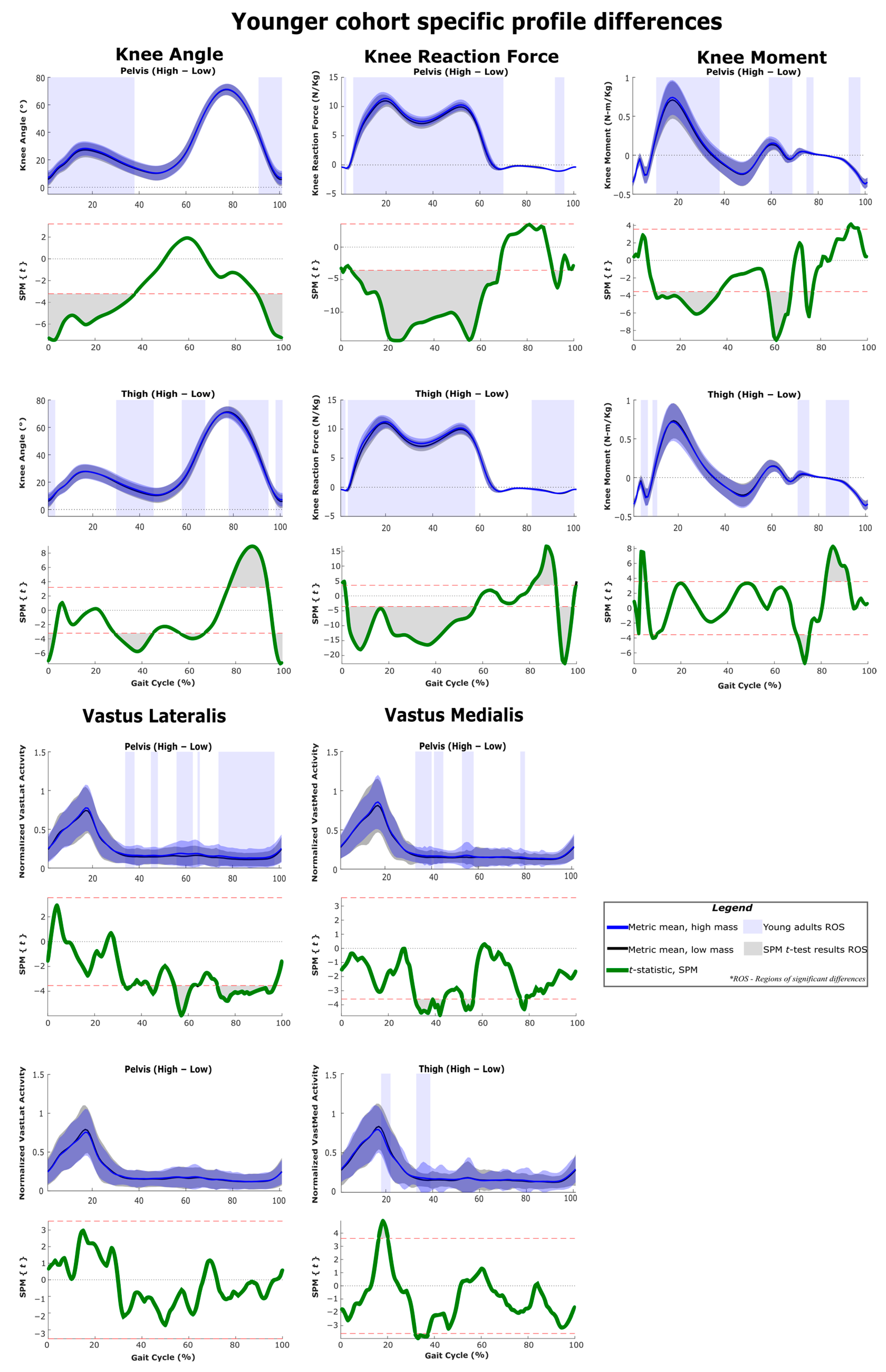
3.5. Profile Differences across the Three Considered Joints
3.6. Age Related Differences in Gait Metrics
4. Discussion
4.1. Characterizing Response Signatures for Added Mass at Pelvis and Thigh
4.2. Comparing to Studies with Other Mass Magnitudes or Increments
4.3. Response to Pelvis Loading during Stance
4.3.1. Young Group
4.3.2. Middle-Aged Group
4.3.3. Weight Acceptance Behaviors
4.3.4. Ankle Joint Responses
4.4. Response to Pelvis Loading during Swing
4.5. Response to Thigh Loading during Stance
4.5.1. Response at Low Thigh Loads
4.5.2. Weight Acceptance Behaviors
4.5.3. Mid-Stance Kinematics
4.5.4. Ankle Joint Responses
4.5.5. Joint Moments and Muscle Activity
4.6. Response to Thigh Loading during Toe-Off
4.6.1. Impact of Temporal Shifts
4.6.2. Joint Moments
4.7. Response to Thigh Loading during Swing
Kinematics and Clearance
4.8. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhang, T.; Tran, M.; Huang, H. Design and experimental verification of hip exoskeleton with balance capacities for walking assistance. IEEE/ASME Trans. Mechatron. 2018, 23, 274–285. [Google Scholar] [CrossRef]
- Yan, T.; Cempini, M.; Oddo, C.M.; Vitiello, N. Review of assistive strategies in powered lower-limb orthoses and exoskeletons. Robot. Auton. Syst. 2015, 64, 120–136. [Google Scholar] [CrossRef]
- Baud, R.; Manzoori, A.R.; Ijspeert, A.; Bouri, M. Review of control strategies for lower-limb exoskeletons to assist gait. J. NeuroEng. Rehabil. 2021, 18, 119. [Google Scholar] [CrossRef]
- Grimmer, M.; Riener, R.; Walsh, C.J.; Seyfarth, A. Mobility related physical and functional losses due to aging and disease—A motivation for lower limb exoskeletons. J. NeuroEng. Rehabil. 2019, 16, 2. [Google Scholar] [CrossRef]
- Jung, M.M.; Ludden, G.D.S. What Do Older Adults and Clinicians Think About Traditional Mobility Aids and Exoskeleton Technology? ACM Trans. Hum.-Robot. Interact. 2019, 8, 1–17. [Google Scholar] [CrossRef]
- Czaja, S.J.; Charness, N.; Fisk, A.D.; Hertzog, C.; Nair, S.N.; Rogers, W.A.; Sharit, J. Factors Predicting the Use of Technology: Findings from the Center for Research and Education on Aging and Technology Enhancement (CREATE). Psychol. Aging 2006, 21, 333. [Google Scholar] [CrossRef]
- Herssens, N.; Verbecque, E.; Hallemans, A.; Vereeck, L.; van Rompaey, V.; Saeys, W. Do spatiotemporal parameters and gait variability differ across the lifespan of healthy adults? A systematic review. Gait Posture 2018, 64, 181–190. [Google Scholar] [CrossRef]
- Guimaraes, R.M.; Isaacs, B. Characteristics of the gait in old people who fall. Int. Rehabil. Med. 1980, 2, 177–180. [Google Scholar] [CrossRef]
- Poggensee, K.L.; Collins, S.H. How adaptation, training, and customization contribute to benefits from exoskeleton assistance. Sci. Robot. 2021, 6, eabf1078. [Google Scholar] [CrossRef]
- Van Asseldonk, E.H.F.; Ekkelenkamp, R.; Veneman, J.F.; van der Helm, F.C.T.; van der Kooij, H. Selective control of a subtask of walking in a robotic gait trainer (LOPES). In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; IEEE: New York, NY, USA, 2007; pp. 841–848. [Google Scholar] [CrossRef]
- Naghavi, N.; Akbarzadeh, A.; Tahamipour-Z, S.M.; Kardan, I. Assist-As-Needed control of a hip exoskeleton based on a novel strength index. Robot. Auton. Syst. 2020, 134, 103667. [Google Scholar] [CrossRef]
- Browning, R.C.; Modica, J.R.; Kram, R.; Goswami, A. The effects of adding mass to the legs on the energetics and biomechanics of walking. Med. Sci. Sports Exerc. 2007, 39, 515–525. [Google Scholar] [CrossRef] [PubMed]
- McGowan, C.P.; Neptune, R.R.; Kram, R. Independent effects of weight and mass on plantar flexor activity during walking: Implications for their contributions to body support and forward propulsion. J. Appl. Physiol. 2008, 105, 486–494. [Google Scholar] [CrossRef]
- Vijayan, V.; Fang, S.; Reissman, T.; Kinney, A.L.; Reissman, M.E. Spatiotemporal and muscle activation adaptations during overground walking in response to lower body added mass. Gait Posture 2022, 92, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Chen, B.; Ma, H.; Qin, L.Y.; Gao, F.; Chan, K.M.; Law, S.W.; Qin, L.; Liao, W.H. Recent developments and challenges of lower extremity exoskeletons. J. Orthop. Transl. 2016, 5, 26–37. [Google Scholar] [CrossRef] [PubMed]
- Riener, R.; Lünenburger, L.; Jezernik, S.; Anderschitz, M.; Colombo, G.; Dietz, V. Patient-cooperative strategies for robot-aided treadmill training: First experimental results. IEEE Trans. Neural Syst. Rehabil. Eng. 2005, 13, 380–394. [Google Scholar] [CrossRef]
- Young, A.J.; Gannon, H.; Ferris, D.P. A Biomechanical Comparison of Proportional Electromyography Control to Biological Torque Control Using a Powered Hip Exoskeleton. Front. Bioeng. Biotechnol. 2017, 5, 37. [Google Scholar] [CrossRef]
- Mooney, L.M.; Herr, H.M. Biomechanical walking mechanisms underlying the metabolic reduction caused by an autonomous exoskeleton. J. NeuroEng. Rehabil. 2016, 13, 4. [Google Scholar] [CrossRef]
- Fang, S.; Kinney, A.L.; Reissman, M.E.; Reissman, T. Simulation on the Effect of Gait Variability, Delays, and Inertia with Respect to Wearer Energy Savings with Exoskeleton Assistance. In Proceedings of the IEEE 16th International Conference on Rehabilitation Robotics (ICORR), Toronto, ON, Canada, 24–28 June 2019. [Google Scholar]
- Dames, K.D.; Smith, J.D. Effects of load carriage and footwear on lower extremity kinetics and kinematics during overground walking. Gait Posture 2016, 50, 207–211. [Google Scholar] [CrossRef]
- Jin, X.; Cai, Y.; Prado, A.; Agrawal, S.K. Effects of exoskeleton weight and inertia on human walking. In Proceedings of the IEEE International Conference on Robotics and Automation, Singapore, 29 May–3 June 2017; pp. 1772–1777. [Google Scholar] [CrossRef]
- Nüesch, C.; Roos, E.; Egloff, C.; Pagenstert, G.; Mündermann, A. The effect of different running shoes on treadmill running mechanics and muscle activity assessed using statistical parametric mapping (SPM). Gait Posture 2019, 69, 1–7. [Google Scholar] [CrossRef]
- Pataky, T.C. One-dimensional statistical parametric mapping in Python. Comput. Methods Biomech. Biomed. Eng. 2012, 15, 295–301. [Google Scholar] [CrossRef]
- Van Sint Jan, S. Color Atlas of Skeletal Landmark Definitions: Guidelines for Reproducible Manual and Virtual Palpations, 1st ed.; Churchill Livingstone: London, UK, 2007. [Google Scholar]
- Sensor Locations, (n.d.). Available online: http://seniam.org/sensor_location.htm (accessed on 26 September 2021).
- Chen, B.; Zi, B.; Qin, L.; Pan, Q. State-of-the-art research in robotic hip exoskeletons: A general review. J. Orthop. Transl. 2020, 20, 4–13. [Google Scholar] [CrossRef] [PubMed]
- Bisseling, R.W.; Hof, A.L. Handling of impact forces in inverse dynamics. J. Biomech. 2006, 39, 2438–2444. [Google Scholar] [CrossRef] [PubMed]
- Kristianslund, E.; Krosshaug, T.; van den Bogert, A.J. Effect of low pass filtering on joint moments from inverse dynamics: Implications for injury prevention. J. Biomech. 2012, 45, 666–671. [Google Scholar] [CrossRef]
- Edwards, W.B.; Troy, K.L.; Derrick, T.R. On the filtering of intersegmental loads during running. Gait Posture 2011, 34, 435–438. [Google Scholar] [CrossRef]
- C-Motion, Segments, WIKI Documentation. 2018. Available online: https://www.c-motion.com/v3dwiki/index.php?title=Segments (accessed on 28 July 2022).
- Schwartz, M.H.; Rozumalski, A. A new method for estimating joint parameters from motion data. J. Biomech. 2005, 38, 107–116. [Google Scholar] [CrossRef]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E. Measurement of lower extremity kinematics during level walking. J. Orthop. Res. 1990, 8, 383–392. [Google Scholar] [CrossRef]
- Dempster, W.T. Space Requirements of the Seated Operator, Geometrical, Kinematic, and Mechanical Aspects of the Body with Special Reference to the Limbs; Michigan State University: East Lansing, MI, USA, 1955. [Google Scholar]
- Yeadon, M.R. The simulation of aerial movement—II. A mathematical inertia model of the human body. J. Biomech. 1990, 23, 67–74. [Google Scholar] [CrossRef]
- Hanavan, E.P. A Mathematical Model of the Human Body; Air Force Aerospace Medical Research Lab, Wright-Patterson AFB: Dayton, OH, USA, 1964. [Google Scholar]
- Stegeman, D.; Hermens, H. Standards for Surface Electromyography: The European Project Surface EMG for Non-Invasive Assessment of Muscles (SENIAM), Línea). Available online: http://www.seniam.org/%5Cnhttp://www.med.uni-jena.de/motorik/pdf/stegeman.pdf (accessed on 28 January 2022).
- Meuleman, J.H.; van Asseldonk, E.H.F.; van der Kooij, H. The effect of directional inertias added to pelvis and ankle on gait. J. NeuroEng. Rehabil. 2013, 10, 1–12. [Google Scholar] [CrossRef]
- Sloot, L.H.; van der Krogt, M.M. Interpreting Joint Moments and Powers in Gait. In Handbook of Human Motion; Springer International Publishing: Cham, Switzerland, 2018; pp. 625–643. [Google Scholar] [CrossRef]
- Shamael, K.; Dollar, A.M. On the Mechanics of the Knee during the Stance Phase of the Gait. In Proceedings of the 2011 IEEE International Conference on Rehabilitation Robotics, Zurich, Switzerland, 29 June–1 July 2011; IEEE: New York, NY, USA, 2011. [Google Scholar]
- Bell, R.D.; Hoshizaki, T.B. Relationships of age and sex with range of motion of seventeen joint actions in humans. J. Can. Des Sci. Appl. Sport 1981, 6, 202–206. [Google Scholar]
- Hortobágyi, T.; Mizelle, C.; Beam, S.; Devita, P. Old Adults Perform Activities of Daily Living Near Their Maximal Capabilities. 2003. Available online: https://academic.oup.com/biomedgerontology/article/58/5/M453/536222 (accessed on 28 January 2022).
- Umberger, B.R.; Martin, P.E. Mechanical power and efficiency of level walking with different stride rates. J. Exp. Biol. 2007, 210, 3255–3265. [Google Scholar] [CrossRef]
- Schwartz, M.H.; Rozumalski, A.; Trost, J.P. The effect of walking speed on the gait of typically developing children. J. Biomech. 2008, 41, 1639–1650. [Google Scholar] [CrossRef] [PubMed]
- Bovi, G.; Rabuffetti, M.; Mazzoleni, P.; Ferrarin, M. A multiple-task gait analysis approach: Kinematic, kinetic and EMG reference data for healthy young and adult subjects. Gait Posture 2011, 33, 6–13. [Google Scholar] [CrossRef]
- Maharaj, J.N.; Cresswell, A.G.; Lichtwark, G.A. Tibialis anterior tendinous tissue plays a key role in energy absorption during human walking. J. Exp. Biol. 2019, 222, jeb191247. [Google Scholar] [CrossRef] [PubMed]
- Herzog, W.; Longino, D.; Clark, A. The role of muscles in joint adaptation and degeneration. Langenbeck’s Arch. Surg. 2003, 388, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Francis, C.A.; Lenz, A.L.; Lenhart, R.L.; Thelen, D.G. The modulation of forward propulsion, vertical support, and center of pressure by the plantarflexors during human walking. Gait Posture 2013, 38, 993–997. [Google Scholar] [CrossRef]
- Kharb, A.; Saini, V.; Jain, Y.K.; Dhiman, S. A Review of Gait Cycle and Its Parameters. 2011. Available online: https://www.ijcem.org/papers72011/72011_14.pdf (accessed on 28 January 2022).
- Cruz, T.H.; Dhaher, Y.Y. Impact of ankle-foot-orthosis on frontal plane behaviors post-stroke. Gait Posture 2009, 30, 312–316. [Google Scholar] [CrossRef]
- Luciano, F.; Ruggiero, L.; Pavei, G. Sample size estimation in locomotion kinematics and electromyography for statistical parametric mapping. J. Biomech. 2021, 122, 110481. [Google Scholar] [CrossRef]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Condition | Thigh Mass | Pelvis Mass |
|---|---|---|
| 1 | Low | Low |
| 2 | Low | Medium |
| 3 | Low | High |
| 4 | Medium | Low |
| 5 | Medium | Medium |
| 6 | Medium | High |
| 7 | High | Low |
| 8 | High | Medium |
| 9 | High | High |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vijayan, V.; Fang, S.; Reissman, T.; Reissman, M.E.; Kinney, A.L. How Does Added Mass Affect the Gait of Middle-Aged Adults? An Assessment Using Statistical Parametric Mapping. Sensors 2022, 22, 6154. https://doi.org/10.3390/s22166154
Vijayan V, Fang S, Reissman T, Reissman ME, Kinney AL. How Does Added Mass Affect the Gait of Middle-Aged Adults? An Assessment Using Statistical Parametric Mapping. Sensors. 2022; 22(16):6154. https://doi.org/10.3390/s22166154
Chicago/Turabian StyleVijayan, Vinayak, Shanpu Fang, Timothy Reissman, Megan E. Reissman, and Allison L. Kinney. 2022. "How Does Added Mass Affect the Gait of Middle-Aged Adults? An Assessment Using Statistical Parametric Mapping" Sensors 22, no. 16: 6154. https://doi.org/10.3390/s22166154